
Abstract
Background:
Anemia is a global public health concern. Its devastating consequences include impaired cognitive and motor development, reduced work productivity, and adverse birth outcomes, all of which apply to adolescents, as well as adults and children.
Objective:
This study aimed to examine the determinants of anemia in Indonesian adolescent girls and boys from Klaten and Lombok Barat districts.
Methods:
A total of 2150 adolescents who participated in a cross-sectional household survey were included in the analysis. The dietary intake of adolescents was assessed using a 7-day food frequency questionnaire. The relationship between anemia status, dietary intake, and other hypothesized determinants was assessed for adolescent girls and boys on a separate basis, using complex samples Cox regression analysis. Variables were selected for inclusion in multivariate models if they were significantly associated with the dependent variable in univariate models (P < .05).
Results:
The prevalence of anemia among adolescent girls and boys was 19% and 5%, respectively. In multivariate analyses, frequent consumption of animal-based iron-rich foods was significantly associated with a lower risk of anemia (prevalence ratio [PR]: 0.59; 95% CI: 0.36-0.97) among adolescent girls, whereas a higher intake of vitamin A-rich fruits and vegetables was associated with a reduced risk of anemia (PR: 0.41; 95% CI: 0.20-0.85) among adolescent boys, after adjustment for all potential confounders.
Conclusions:
Increased consumption of iron- and vitamin A-rich foods through the implementation of gender-responsive Social Behaviour Change Communication (SBCC) interventions is warranted. This should be coupled with improved coverage and quality of iron and folic acid supplementation programs in adolescents.
Introduction
Anemia is a global public health concern, and one to which children younger than 5 years and pregnant mothers are most vulnerable. 1 However, evidence suggests that the prevalence of anemia among adolescent girls in South-East Asia is also considerable, and ranges between 17% and 90%. 2 In Indonesia, approximately 23% and 12% of adolescent girls and boys, respectively, were estimated to be anemic in 2013, which has made anemia a moderate public health problem, with particular reference to adolescent girls. 3,4
Determinants of anemia have been studied widely among women of reproductive age. Anemia is largely attributed to iron deficiency 5,6 but is also related to deficiencies of other micronutrients, such as vitamin A, folic acid, and vitamin B-12. 6 In addition, non-nutritional factors, such as parasitic infections, malaria, HIV, and hemoglobinopathies, and some demographic factors, such as age, gender, and household sanitation facilities, contribute to the development of anemia. 7,8 Adolescents are vulnerable to anemia due to their concomitant increase in iron requirements to support rapid pubertal growth and the onset of menstruation. 2,9 Few studies, however, have researched the risk factors of anemia specifically among adolescent girls and boys in a South-East Asian context.
In developing countries, adolescence often coincides with the time when many girls drop out of school, enter marriage, and have their first pregnancy. 10,11 This is concerning, as prepregnancy maternal undernutrition and anemia increase the risk of adverse birth outcomes, and subsequent stunting during early childhood within offspring. 12 -14 For adolescent girls and boys, the consequences of anemia include impaired cognitive and motor development, and reduced physical fitness, school performance, and work productivity. 8,15,16
This study aimed to assess the determinants of anemia among Indonesian adolescent girls and boys aged 12 to 18 years from the districts of Klaten and Lombok Barat. Few studies have explored the risk factors for anemia among Indonesian adolescents, especially with reference to boys. Given that adolescents make up a population group that is rapidly growing and of vital importance to break the intergenerational cycle of malnutrition, there is a clear need to reach them with the appropriate nutrition interventions. 17,18 This research will enrich existing knowledge on adolescent anemia and relevant risk factors and help guide the design and planning of future program and policy decisions to address the burden of anemia in this age group.
Methods
Study Design and Participants
A cross-sectional household survey was conducted in April and May 2017 in Klaten District in Central Java Province, and Lombok Barat District in West Nusa Tenggara Province. Klaten is 1 of the 35 districts in Central Java; its total population in 2015 was 1.2 million, of whom 15% were aged 10 to 19 years. 19 In 2016, the school participation rate of adolescents aged 13 to 15 years and 16 to 18 years was 99% and 76%, respectively. 19 Lombok Barat is 1 of the 10 districts in West Nusa Tenggara; the total population in 2015 was 654 892, of whom 12% were aged 13 to 18 years. 19 Data from the District Office of Education Youth and Sport showed that in the 2015/2016 academic year, there were 174 out-of-school children. 19
The study sample comprised adolescent girls and boys aged 12 to 18 years and their parents or guardians, where appropriate. All adolescents younger than 12 and older than 19 years of age at the time of interview were excluded, and those who were not physically living in the selected village and/or those with any mental and/or physical disability which may impede their ability to answer questions. Interviews and assessments were only conducted after written consent was obtained from both the adolescent and parents/guardian. The survey was approved by the Ethical Committee of Gadjah Mada University in Yogyakarta, Indonesia.
A multistage sampling strategy was employed to obtain a representative sample of adolescent girls and boys living across all subdistricts. A sample size of 2160 was determined to be sufficient to detect a 5% difference in healthy eating behaviors across the whole sample. First, 45 clusters in each district were selected using a probability proportionate to size sampling strategy, to ensure that more clusters were selected in subdistricts with more villages. Second, one or more subvillages were selected using simple random sampling to attain at least 12 adolescent boys and 12 adolescent girls aged 12 to 18 years from each cluster. If there were more than 12 of either gender, they were randomly sampled. If there were fewer than 12 adolescent boys and 12 adolescent girls, a second, and potentially a third, subvillage in the same village was randomly selected. This process was repeated until the required sample size (n = 2160) was obtained. Only one adolescent from each household was included in the sample.
Data Collection
All selected eligible adolescents were visited by 2-person field teams for home-based interviews and measurements. Data were collected using standardized digital questionnaires on a mobile data collection system, using CSPro on Android-based tablets. Interviews were conducted in either Indonesian or the local language (Javanese or Sasak). For adolescents and their parents/guardians, interviews were conducted independent of each other so as to minimize the parents’/guardians’ influence on the adolescent’s answers.
Adolescents were requested to provide information on their demographic characteristics, education, morbidity in the past week, dietary intake, sources and use of pocket money, and health-seeking and hygiene behaviors. Specifically, dietary intake was collected using a 7-day food frequency questionnaire (FFQ), for which the list of food items was developed in line with the food groups used in the Minimum Dietary Diversity for Women measurement guideline. 20 Information on the adolescent’s intake of micronutrient supplement was also collected. The parents and/or guardians of adolescents were asked about their household composition, demography, socioeconomic status, source of drinking water, and access to sanitation facilities.
Anthropometric measurements, including the height and weight of the adolescents, were assessed following standard procedures. 21 The adolescent’s height was measured to the nearest 0.1 cm using a SECA 206 Mechanical Measuring Tape (Microtoise), and weight was assessed (to the nearest 0.1 kg) using SECA 874 flat digital weighing scales. Hemoglobin concentrations were assessed using HemoCue 201+ (HemoCue). All equipment was calibrated regularly. The adolescent’s date of birth was collected from his or her birth certificate, family/ID card, or other official documents to the extent possible or, if these were not available the adolescent’s self-reported date of birth was used.
The data collectors were trained according to the study protocols and were regularly monitored and supervised throughout the data collection. Survey nonresponse and refusal to participate were both negligible.
Statistical Analyses
All data entered in the digital questionnaire were double-checked by enumerators and supervisors, all anthropometric and hemoglobin data were double-entered, and appropriate data-cleaning procedures were conducted. The analyses were weighted according to the total population size and adjusted for the multistage sampling design.
The adolescents’ dietary diversity was assessed following the recommended methodology for determining the Minimum Dietary Diversity for Women. 20 A dichotomous variable for dietary diversity was created to classify adolescents into inadequate and adequate diversity using the following cutoffs: inadequate (<5 food groups) or adequate (≥5 food groups). 20 In addition, for each food group, the median and accompanying interquartile range (IQR) were assessed, and tertiles of intake were created to categorize adolescents into low-, average-, and high-consumption categories. Different cutoffs were applied for different food groups and genders.
Anemia status was defined in accordance with the World Health Organization (WHO) guidelines. 1,4 Body mass index (BMI) (kg/m2) was defined as weight (kg)/height (m2). Using the WHO growth standards, stunting and thinness were defined as having z-scores less than −2 for both height for age and BMI for age, respectively. Overweight was defined as a z-score above 1 for BMI for age.
Household food security was assessed using the Household Food Insecurity Access Scale, 22 and household wealth quintiles were created using the approach outlined by the Demographic Health Surveys. 23 Appropriate cutoffs were applied to create dichotomous or categorical variables for a few variables.
Household sanitation facilities were dichotomized into improved (private facility with/without septic tank) or unimproved sources (shared/public latrine, pit latrine without slab, yard/bush/forest, river/stream/creek, and others). 24 Household drinking water sources were also categorized into improved (piped water, well with pump, protected well, protected spring, and rain) or unimproved sources (unprotected well, unprotected spring, bottled water, refilled water, river/lake/pond/irrigation/dam, and others). 24
Descriptive analyses were employed to examine the distribution of the full range of variables. Adolescent girls who reported that they were pregnant at the time of interview, or who had ever been pregnant (n = 10), were excluded from any further analyses.
Determinants of anemia were assessed for adolescent girls and boys separately, using a complex samples Cox regression analysis with constant time at risk. Separate univariate complex samples Cox regression models were used to examine the relationship between anemia status, dietary intake, and other hypothesized determinants, including household, parental, and adolescent characteristics. The determinant analysis was guided by the adolescent nutrition conceptual framework (Figure 1) and other relevant literature. 5,8
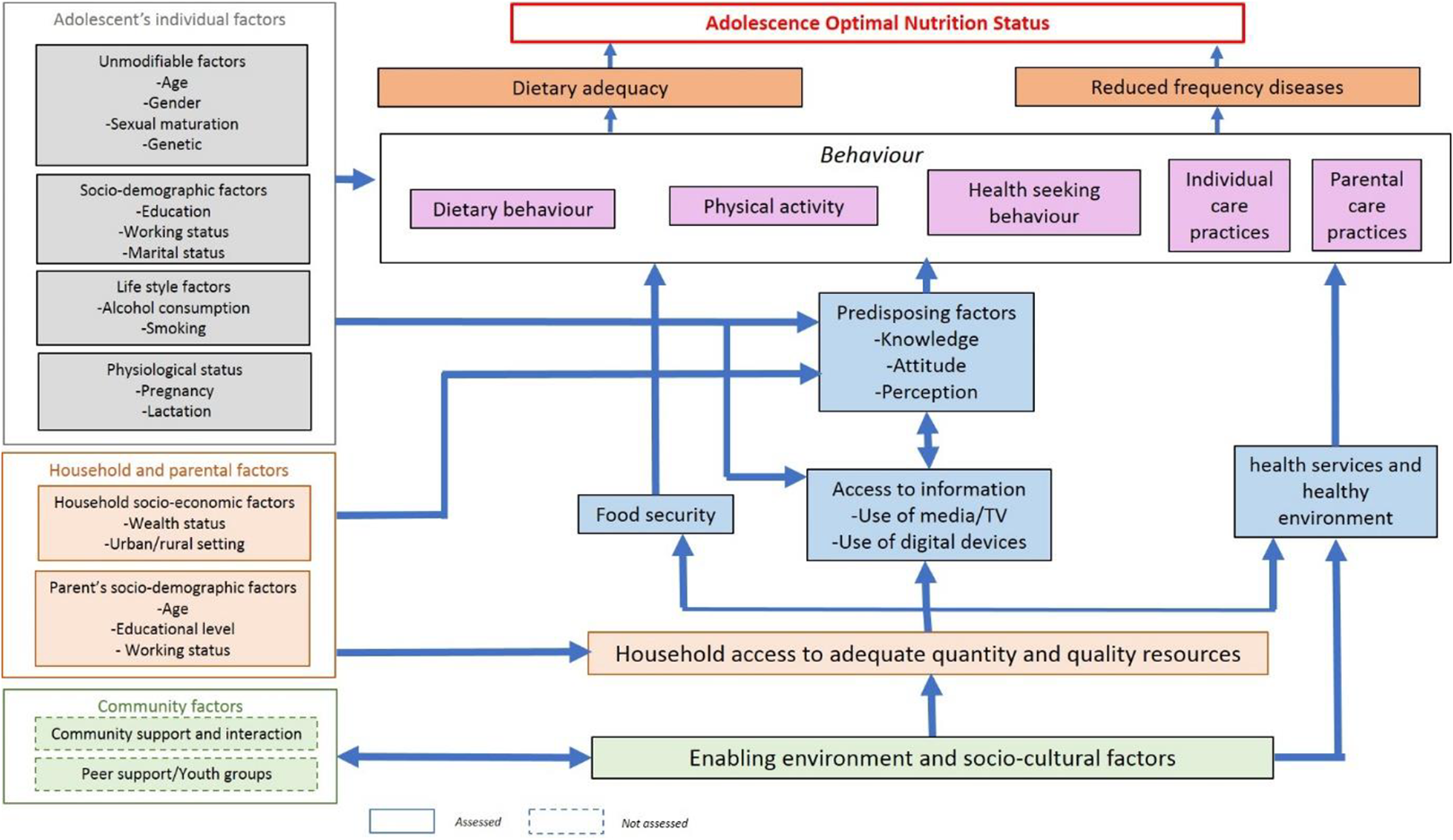
Conceptual framework of nutritional status among adolescents.
Variables were selected for inclusion in the multivariate models if they had a statistically significant association with the dependent variable in the univariate models (defined as P < .05). District and adolescent age were included in the multivariable Cox regression models, irrespective of statistical significance. Multicollinearity was assessed on the basis of a variance inflation factor <10 to determine whether it was appropriate to include all variables in the multivariate models. No multicollinearity was observed. In multivariate models, an α of <.05 was considered statistically significant. All analyses were performed using SPSS Statistics 24 (IBM Corporation).
Results
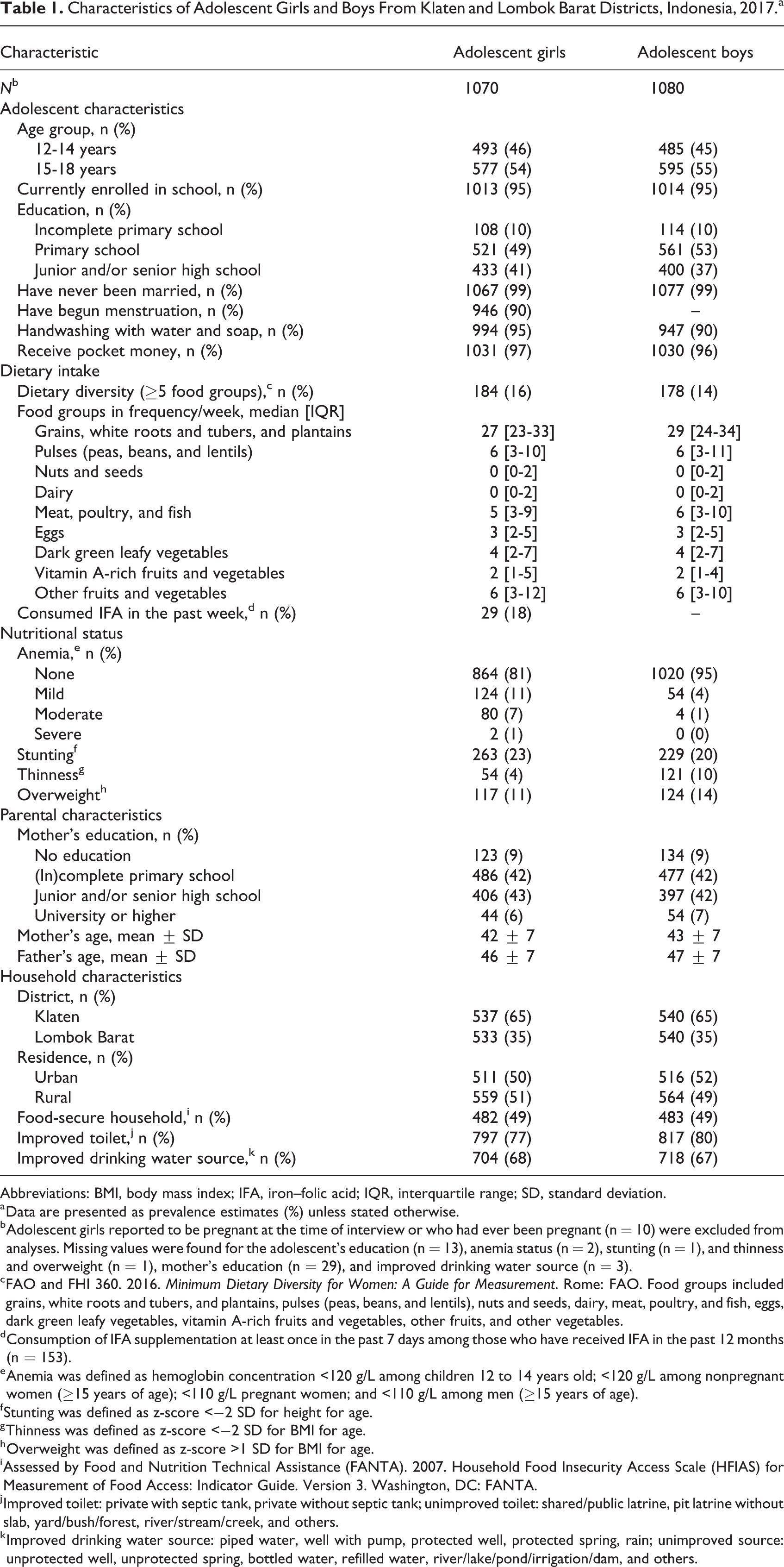
The mean (±standard deviation [SD]) age of adolescents included in the analysis was 15 (±2); 48% were girls (n = 1070; Table 1). About two-thirds of the adolescents lived in the district of Klaten, and the majority of them were enrolled at school at the time of interview (95%). Hardly any adolescents reported being married, and most adolescent girls had experienced their first menstruation (90%). Approximately 23% and 20% of adolescent girls (n = 263) and boys (n = 229) were stunted, respectively. About 4% and 10% of adolescent girls and boys were thin, and another 11% and 14% were overweight or obese.
Characteristics of Adolescent Girls and Boys From Klaten and Lombok Barat Districts, Indonesia, 2017.a
Abbreviations: BMI, body mass index; IFA, iron–folic acid; IQR, interquartile range; SD, standard deviation.
a Data are presented as prevalence estimates (%) unless stated otherwise.
b Adolescent girls reported to be pregnant at the time of interview or who had ever been pregnant (n = 10) were excluded from analyses. Missing values were found for the adolescent’s education (n = 13), anemia status (n = 2), stunting (n = 1), and thinness and overweight (n = 1), mother’s education (n = 29), and improved drinking water source (n = 3).
c FAO and FHI 360. 2016. Minimum Dietary Diversity for Women: A Guide for Measurement. Rome: FAO. Food groups included grains, white roots and tubers, and plantains, pulses (peas, beans, and lentils), nuts and seeds, dairy, meat, poultry, and fish, eggs, dark green leafy vegetables, vitamin A-rich fruits and vegetables, other fruits, and other vegetables.
d Consumption of IFA supplementation at least once in the past 7 days among those who have received IFA in the past 12 months (n = 153).
e Anemia was defined as hemoglobin concentration <120 g/L among children 12 to 14 years old; <120 g/L among nonpregnant women (≥15 years of age); <110 g/L pregnant women; and <110 g/L among men (≥15 years of age).
f Stunting was defined as z-score <−2 SD for height for age.
g Thinness was defined as z-score <−2 SD for BMI for age.
h Overweight was defined as z-score >1 SD for BMI for age.
i Assessed by Food and Nutrition Technical Assistance (FANTA). 2007. Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: Indicator Guide. Version 3. Washington, DC: FANTA.
j Improved toilet: private with septic tank, private without septic tank; unimproved toilet: shared/public latrine, pit latrine without slab, yard/bush/forest, river/stream/creek, and others.
k Improved drinking water source: piped water, well with pump, protected well, protected spring, rain; unimproved source: unprotected well, unprotected spring, bottled water, refilled water, river/lake/pond/irrigation/dam, and others.
Approximately 19% of adolescent girls were anemic (n = 206), whereas 5% of boys were anemic (n = 58). Most anemic adolescents had mild anemia (Table 1).
About half of the households were reported to have food insecurity (51%), and most adolescents were reported to have inadequate dietary diversity (85%; Table 1). High consumption of grains, white roots and tubers, and plantains was observed among both adolescent girls and boys, while consumption of micronutrient-rich foods such as fruits and vegetables, nuts and legumes, dairy, meat, poultry, and fish was low. The consumption of iron–folic acid (IFA) supplements was reported to be low, with less than 20% of adolescent girls having consumed it in the past week (n = 29, 18%).
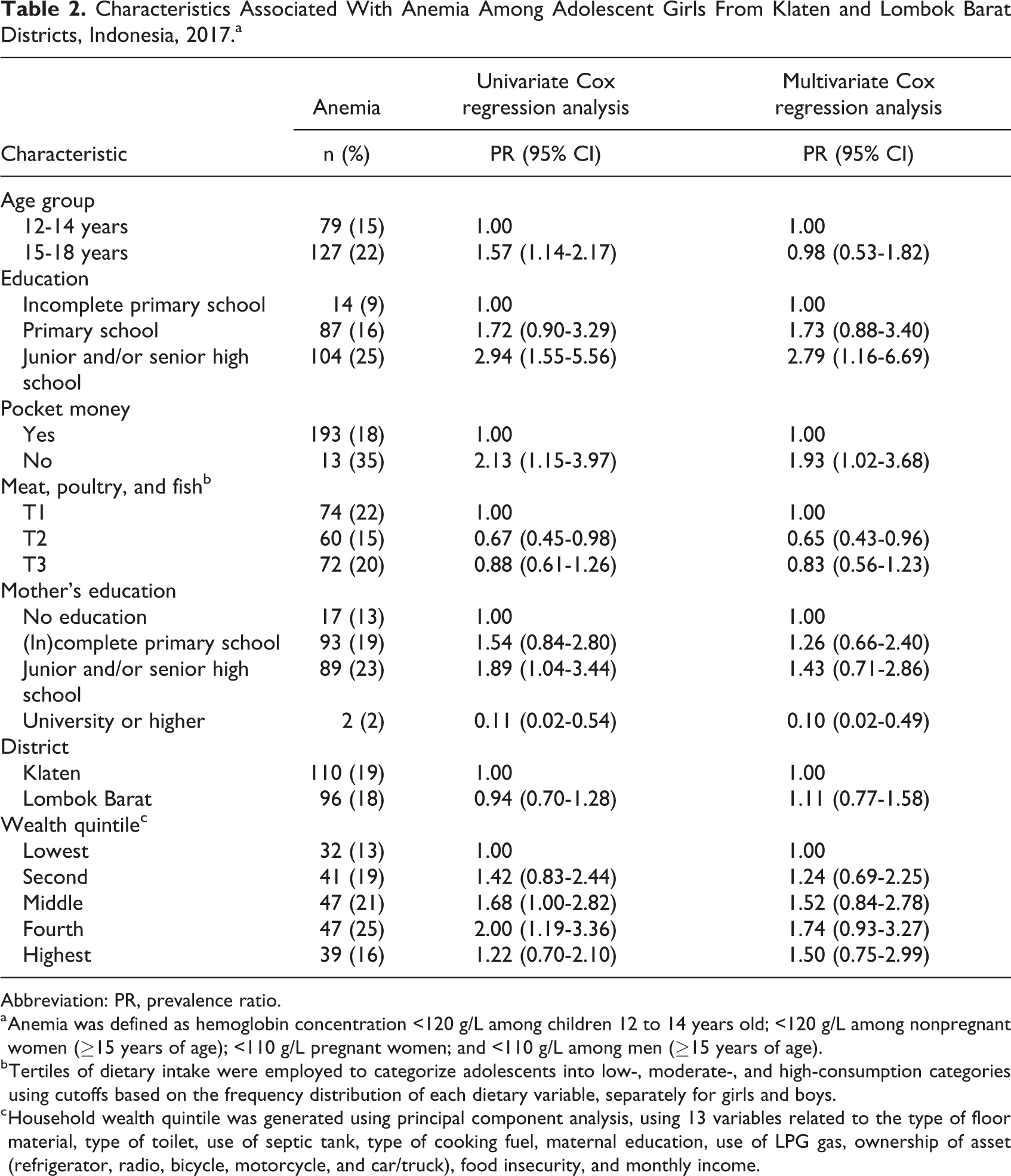
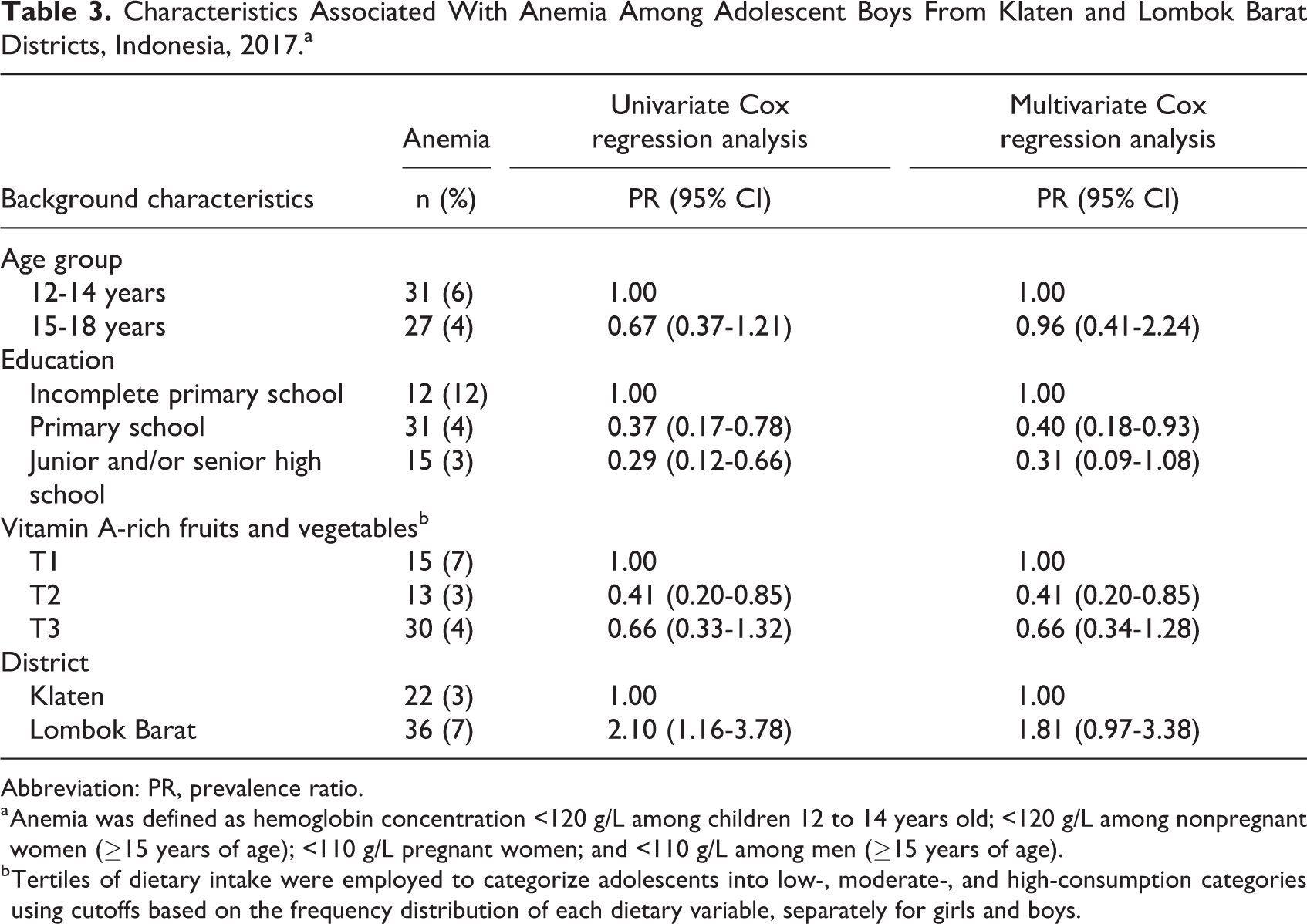
In the multivariate analysis for adolescent girls, a lower prevalence of anemia was associated with frequent consumption of animal-based iron-rich foods, such as meat, poultry, and fish (prevalence ratio [PR]: 0.65; 95% CI: 0.43-0.96), and the mother’s education (PR: 0.10; 95% CI: 0.02-0.49), while a higher prevalence of anemia was associated with not receiving pocket money (PR: 1.93; 95% CI: 1.02-3.68) and education (PR: 2.79; 95% CI: 1.16-6.69), controlling for all potential confounders such as age, district, and wealth quintile (Table 2). Among adolescent boys, frequent consumption of vitamin A-rich fruits and vegetables (PR: 0.41; 95% CI: 0.20-0.85) and education (PR: 0.40; 95% CI: 0.18-0.93) were associated with a lower prevalence of anemia, while adjusting for all potential confounders such as age and district (Table 3). No association was found between the risk of anemia and the overall dietary diversity of adolescent girls and boys (data not shown).
Characteristics Associated With Anemia Among Adolescent Girls From Klaten and Lombok Barat Districts, Indonesia, 2017.a
Abbreviation: PR, prevalence ratio.
a Anemia was defined as hemoglobin concentration <120 g/L among children 12 to 14 years old; <120 g/L among nonpregnant women (≥15 years of age); <110 g/L pregnant women; and <110 g/L among men (≥15 years of age).
b Tertiles of dietary intake were employed to categorize adolescents into low-, moderate-, and high-consumption categories using cutoffs based on the frequency distribution of each dietary variable, separately for girls and boys.
c Household wealth quintile was generated using principal component analysis, using 13 variables related to the type of floor material, type of toilet, use of septic tank, type of cooking fuel, maternal education, use of LPG gas, ownership of asset (refrigerator, radio, bicycle, motorcycle, and car/truck), food insecurity, and monthly income.
Characteristics Associated With Anemia Among Adolescent Boys From Klaten and Lombok Barat Districts, Indonesia, 2017.a
Abbreviation: PR, prevalence ratio.
a Anemia was defined as hemoglobin concentration <120 g/L among children 12 to 14 years old; <120 g/L among nonpregnant women (≥15 years of age); <110 g/L pregnant women; and <110 g/L among men (≥15 years of age).
b Tertiles of dietary intake were employed to categorize adolescents into low-, moderate-, and high-consumption categories using cutoffs based on the frequency distribution of each dietary variable, separately for girls and boys.
Discussion
In this cross-sectional analysis of a survey conducted in a representative sample of adolescents from 2 districts in Indonesia, frequent intake of micronutrient-rich foods emerged as an important determinant of anemia among adolescent girls and boys, reinforcing the crucial link between anemia and dietary intake. More specifically, a higher consumption of animal-based iron-rich foods, such as meat, poultry, and fish, and vitamin A-rich fruits and vegetables, was associated with a 35% and 59% reduced prevalence of anemia among adolescent girls and boys, respectively. The consumption of animal-based iron-rich foods had lower impact in reducing the anemia prevalence among adolescent girls than that among boys may be due to iron loss during menstruation among girls.
Overall, approximately 19% of adolescent girls and 5% of adolescent boys were found to be anemic in our study. This is lower than the national estimates of anemia prevalence reported in the 2013 Basic Health Research Survey. The discrepancies may reflect geographical variations in anemia prevalence among adolescents in different parts of the country. Studies conducted in different regions in Indonesia reported anemia prevalence estimates ranging between 9% and 57% for adolescent girls, and 12% and 17% for adolescent boys. 25 -27 Alternatively, the reduced prevalence of anemia reported in our study may reflect the declining trend of anemia in Indonesia 3,28 and could perhaps be attributed to higher quality diets, decreased food insecurity, better access to safe water and sanitation, improved health care, and other determinants. 29 Still, more research is required to investigate this phenomenon and its associative factors.
Among adolescent girls, anemia was significantly associated with the consumption of animal-based iron-rich foods such as meat, poultry, and fish, education, mother’s education, and pocket money. Iron deficiency is a well-known cause of anemia, 5 so a diet rich in iron is usually recommended to prevent anemia. It is well established that animal-based foods have a higher iron content and bioavailability than plant-based foods. 6 In developing countries, however, the majority of people consume a plant-based diet that is rich in nonheme iron, and its absorption is often less than 10%. 30,31 The absorption of nonheme iron is increased by meat and ascorbic acid, but inhibited by phytates and polyphenols—substances commonly found in plant-based foods. 31 Our findings are similar to those from a study performed in participants aged 16 to 24 years from the United Kingdom, which found a direct link between red meat intake and increased iron and hemoglobin concentrations. 32 Equivalently, the infrequent intake of meat was shown to correlate with anemia in women of reproductive age from Vietnam. 33 In contrast, a study among Indonesian girls aged 10 to 12 years found that those with iron deficiency anemia had iron intakes significantly higher than those who were not iron deficient. It should be mentioned, however, that total iron intake was also much lower than the Indonesian Recommended Daily Allowance, meaning that any difference in iron intake could not have had a significant effect. 34 Our findings go beyond previous reports, being among the first to demonstrate the association between anemia and the consumption of iron-rich foods among Indonesian adolescent girls.
We speculate that those adolescent girls who do not receive pocket money have decreased access to the purchase of animal-based foods rich in iron, and as a consequence, might consume a more plant-based diet, thereby increasing their risk of anemia. The latter could perhaps also be true for those adolescent girls with a higher education, though the reasons for this result are not yet understood.
Among adolescent boys, anemia was significantly associated with the consumption of vitamin A-rich fruits and vegetables and education. Prior studies have suggested that vitamin A and β-carotene can enhance the absorption of nonheme iron, and thereby contribute to an increase in hemoglobin concentrations. 35,36 This is confirmed by previous findings in the literature that serum vitamin A and the intake of fruit were significantly related to hemoglobin concentrations among pregnant women from Bangladesh. 37 Likewise, a trial among pregnant Indonesian women showed that supplementation with vitamin-A-enhanced hemoglobin levels resulted in a decreased prevalence of anemia; the results were even better when vitamin A supplementation was combined with iron supplementation. 38 Our research is unique, in the sense that it showed the association between anemia and the consumption of vitamin A-rich fruits and vegetables specifically among adolescent boys.
At present, there is an IFA supplementation program in place in Indonesia, which is operated through a school-based delivery system. The national guideline was published in 2016 but, up until the time of writing, IFA tablets have only been distributed to adolescent girls at junior and senior high schools, and geographical coverage remains limited. 39 At the time of data collection, the districts of Klaten and Lombok Barat had not yet commenced IFA distribution; thus, the low intake of IFA supplementation in this study was not remarkable. Despite declines in anemia over the past few years, the prevalence of anemia among adolescent girls remains fairly high (19%), and although not as considerable, we found that a substantial portion of adolescent boys suffer from anemia (5%). Thus, IFA supplementation remains an important intervention strategy for the further reduction of anemia prevalence rates among adolescent girls as well as adolescent boys. 40 In addition, the implementation of a gender-responsive Social Behavior Change Communication (SBCC) program would be a suitable accompaniment for the IFA supplementation program, in order to guide appropriate dietary intake and other behavioral changes, and to ultimately bring about a decrease in the prevalence of anemia among both adolescent girls and boys. Moreover, the assessment of helminth infection will be of importance in future studies, as helminths are an important risk factor for anemia, since they can cause a decrease in hemoglobin concentrations. Pairing IFA supplementation with deworming programs for adolescents has been shown to effectively reduce anemia. 41
Overall, little research has been conducted in Indonesia which focuses on adolescent nutrition and its determinants. Our report adds to the existing knowledge by providing the most recent estimates of nutritional status of both adolescent girls and boys, representative of the district level, and by demonstrating the importance of a healthy diet rich in iron and vitamin A for the prevention and control of anemia. Several limitations need to be considered. Due to the cross-sectional nature of the data, observed associations cannot be interpreted as causal, and reverse causation could be a possibility. Our dietary intake assessment was restricted to the frequency of consumption. Information on portion size and/or the amount of intake was not available. The use of an FFQ comes with certain biases, which include response bias (eg, social desirability answering) and recall bias (eg, not remembering eating behavior), the latter leading to possible misclassification. As questions related to pregnancy status were only asked of adolescents who reported being married, adolescent pregnancy may be underestimated in this survey. In addition, most adolescents in this study were enrolled in school, which could have led to a response bias as those out-of-school may have refused to join the study.
Conclusion
Our study demonstrated that frequent consumption of food rich in micronutrients such as iron and vitamin A is associated with a decreased prevalence of anemia among adolescent girls and boys in Indonesia, after controlling for all potential confounders. This reinforces the growing evidence of the association between dietary intake and adolescent nutritional status. Increasing consumption of iron- and vitamin A-rich foods, specifically, as well as the improvement and scaling up of IFA supplementation programs, complemented with gender-responsive SBCC interventions, may be essential to the improvement of adolescent anemia status. Further research is needed to explore the observed association using longitudinal data, thereupon incorporating the assessment of helminth infection and the utilization of a semiquantitative FFQ, which includes portion sizes in addition to frequency.
Footnotes
Authors’ Note
M.K. wrote the paper and conducted the analysis, J.H.R. and A.R. conceptualized the paper and provided a significant contribution to the writing and review of analysis, and J.S. led the data collection. All authors have reviewed and approved the draft. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Ethical approval was obtained from the Ethical Committee of Gadjah Mada University in Yogyakarta, Indonesia (Ke/FK/0200/EC/2017). Written informed consent was obtained from all adolescents and their parents/guardians. If the parent/guardian of the respondent was illiterate, the consent form was read aloud, and a fingerprint was taken as consent to take part in the study in lieu of a signature. In addition to ethical clearance, formal approvals were sought from the central government, provincial governments, and local authorities in both districts prior to the start of the data collection activities.
Acknowledgments
The authors wish to acknowledge Ms Masumi Maehara for her kind support in reviewing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by The Government of Canada, the Canadian UNICEF Committee, and the 25th Team for the project “Addressing MNCH gaps to create scalable investments for the future” implemented by UNICEF Indonesia Country Office and the Ministry of Health Republic of Indonesia.