
Abstract
Background:
Measuring undernutrition using composite index of anthropometric failure (CIAF) and identifying its determinants in tribal regions is essential to recognize the true burden of undernutrition in these settings.
Objective:
To determine anthropometric failure and its determinants among tribal children younger than 5 years in Palghar, Maharashtra, India.
Methods:
A cross-sectional survey employing CIAF was performed in children <5 years to estimate undernutrition in the tribal district of Palghar in Maharashtra, India. Anthropometric measurements, maternal and child characteristics were recorded from 577 mother–child pairs in 9 villages.
Results:
As per Z score, prevalence of stunting, wasting, and underweight were 48%, 13%, and 43%, respectively. According to CIAF, 66% of children had at least one manifestation of undernutrition and 40% had more than one manifestation of undernutrition. Odds of anthropometric failure were 1.5 times higher among children of mothers who were illiterate (adjusted odds ratio [AOR] =1.57, 95% CI: 1.0-2.3), children who had birth weight >2.5 kg had lesser odds (AOR: 0.63, 95% CI: 0.4-0.9) of anthropometric failure, and children who had initiated early breastfeeding had 1.5 times higher odds of anthropometric failure (crude odds ratio: 1.5, 95% CI: 1.0-2.1). However, when adjusted for other independent variables, the results were not significant.
Conclusion:
The alarming proportion of anthropometric failure among tribal children calls for urgent short-term interventions to correct undernutrition and long-term interventions to improve maternal literacy and awareness to prevent and manage child undernutrition.
Introduction
Studying different dimensions of undernutrition is essential to recognize the true burden and the association between morbidity, undernutrition, and mortality. Studying different geographical settings, cultures, and employing alternate measuring techniques provide novel insights to the science of undernutrition. For instance, trends in prevalence of malnutrition vary with settings. High prevalence of undernutrition has been reported in isolated tribal settings especially among children younger than 5 years, contributing significantly to premature mortality. 1,2
Likewise, employing alternate measurement techniques either over-or underestimates the true burden. Composite index of anthropometric failure (CIAF) is one such measurement that provides a comprehensive measure of undernutrition and simultaneously provides a clear picture of the association between undernutrition and morbidity. 3 In an Indian context, high prevalence of undernutrition among children, unrelenting to tested interventions, often leads to arguments about the type of measurements used and the inferences drawn. 4 Measurements that provide a larger estimate of the burden are often unaccepted, as the reality of the situation leaves India faring poorer than the Sub-Saharan Africa. 5 It is therefore essential to employ measures that provide a comprehensive assessment of the prevailing conditions, to draw the attention of public health fraternity, to these isolated tribal settings, which otherwise is unreflected in national statistics.
The wealthiest state of Maharashtra in India presents an interesting paradox of highest growth and development on one side while housing a large proportion of undernourished children on the other. Despite obtaining the highest gross domestic product, Maharashtra is worse than some of the world’s poorest countries in prevalence of underweight among children such as Bangladesh (33%), Afghanistan (25%), or Mozambique (15%). 6 Maharashtra houses 10 million tribal population who live under conditions that are far from development. And their children are worst affected by undernutrition and its consequences. 7 As per 2016 statistics, Maharashtra is home to >30% stunted, 25% wasted, another 10% severely wasted, and 35% underweight children. 8 Studying prevalence of malnutrition among tribal children where concentration of malnourished children is higher through a measure that identifies any form of undernutrition, either as a single or combined manifestation, that underscores both magnitude and severity, is of larger relevance to prevent childhood mortality.
Palghar district of Maharashtra is predominantly a tribal area, where agriculture provides the primary source of livelihood. 9 In 2017, the prevalence of undernutrition was reportedly 59% stunting, 53% underweight, and 20% wasting and further recorded 600 deaths of children younger than 5 years due to undernutrition. 6 Lower socioeconomic status, less access to amenities, and low levels of literacy increase the vulnerability compared to nontribal settings. The World Health Organization (WHO) 2006 indicators of malnutrition reflect different aspects of undernutrition. Stunting (height-for-age Z score (HAZ)] detects long-term undernutrition with deprivation of food or exposure to infection and other environmental and social factors; wasting (weight-for-height Z score (WHZ)] is a well-known indicator of acute undernutrition or recent weight loss; and underweight (weight-for-age Z score [WAZ]) is used as a composite measure of WHZ and HAZ. 10 Individually these indicators cannot measure the overall prevalence of undernutrition, as an underweight child could also be stunted and/or wasted. To consider all undernourished children including any/all forms of manifestation, an aggregate indicator called CIAF was proposed by Svedberg P., 2000 11 and further modified by Nandy et al. 12 Employing CIAF, we studied undernutrition and its determinants in a tribal setting in Palghar, Maharashtra, where the prevalence of undernutrition in children is a major concern.
Methods
A community-based cross-sectional study was carried out in 2018 in the tribal villages of Mokhada, a tehsil (an administrative division) in Palghar district of Maharashtra, to assess the nutritional status of children aged 0 to 59 months. Palghar district has a total of 8 talukas/tehsils, namely Jawhar, Mokhada, Talasari, Vasai, Vikramgad, Palghar, Dahanu, and Wada. Of these 8 talukas, 1 taluka, that is, Mokhada, was selected as the study area. There are total 59 villages in Mokhada of which 9 (15%) villages (namely Chas, Ghoshali, Khoch, Gonde khurd, Mokhada, Palsunde, Poshera, Shivali, and Washala) were randomly selected for the study. The sampling frame consisted of mother–child pairs from these 9 villages of Mokhada taluka. Mothers with children 0 to 59 months of age were included and children with any major illness were excluded from the study.
Sample size was calculated using the prevalence of wasting among children younger than 5 years in National Family Health Survey 4. 8 Considering the prevalence of wasting as 25.6%, a desired precision and CI of 4% and 95% each, an additional 10% nonresponse, and 0.1 design effect, the estimated sample size was n = 554. To achieve this sample size, 600 mother–child pairs were enrolled, of which 577 provided complete details. A population proportion sample was drawn based on the number of children in 0 to 59 months of age from the selected villages. In each village, a list of children aged 0 to 59 months registered in the anganwadi centers (government preschools) were obtained from the anganwadi workers. Mother–child pairs were enrolled through household visits.
Data were collected using a semistructured questionnaire administered through a tablet version of “EpiCollect 5,” from each of the 9 selected villages. 13 The households from each village were randomly selected following the inclusion criteria. The institutional ethics committee of Savitribai Phule Pune University (SPPU/IEC/2018/04) approved this work. Informed consent was obtained from every participant prior to the interview. The purpose of research was explained to the participants, and confidentiality of data was assured with the freedom to withdraw at any time during the study period.
Data of 40 participants were collected from Talegaon, Pune, for pilot test. For validation, the questionnaire was checked for the flow of questions, usage of relevant terminologies, and whether the questions elicited the intended response.
Anthropometric Measurements
Two researchers with formal training in public health nutrition and trained in anthropometry recorded anthropometric measurements. Instruments were standardized using known weights and measures. Also, height and weight measurements were standardized for validity.
Length/height: Seca Infantometer (Model No: 416) (Positive Dynamics, Mumbai) was used to record length of children younger than 2 years in a reclined position. The fixed head piece touched the crown of the toddler and the feet touched the movable piece of the infantometer. Care was taken to keep the head, knees, and feet in position while the measurement was recorded. Standing height of children was recorded using a portable stadiometer (Seca Model No: 213). The head, back, and feet were aligned to the scale, and Frankfort plane was adjusted to measure maximum height. The movable head piece rested above the head while the measurement was recorded. Measurements were recorded to the nearest 0.1 cm.
Weight: Combined weight of the mother and child was recorded using portable, digital weighing scales (Omron model no: HN 283), while the mothers held their children. Following this, mother’s weight was recorded and subtracted from the earlier weight of the mother and child. The measurements were recorded to the nearest 0.1 kg.
All measurements were recorded in duplicates, and the average was obtained. Technical error of measurements were kept within standard limits (<0.1).
Definitions
Stunting (HAZ): Height-for-age is a measure of linear growth retardation and cumulative growth deficits. Moderate stunting is defined as Z score <−2 standard deviation (SD), while severe stunting is defined as Z score <−3 SD. 8
Wasting (WHZ): Wasting is a reduction or loss of body weight in relation to height. Moderate wasting is defined as Z score <−2 SD, while severe wasting is defined as Z score <−3 SD. 8
Underweight (WAZ): Weight-for-age is a composite index of height-for-age and weight-for-height. It considers both acute and chronic undernutrition. Moderate underweight is defined as Z score <−2 SD, while severe underweight is defined as Z score <−3 SD. 8
Composite Index of Anthropometric Failure
To measure undernutrition collectively, CIAF was used. According to CIAF classification, children were divided into the following 7 groups: Group A: no failure; Group B: wasting only; Group C: wasting and underweight; Group D: wasting, stunting, and underweight; Group E: stunting and underweight; Group F: stunting only; and Group Y: underweight only.
14
From the above-mentioned classification, total prevalence of undernutrition is measured by summation of all the groups except group A.
Data analysis was performed using statistical packages for social sciences (SPSS) version 19. To convert the anthropometric data into Z scores of the indices, WHO Anthro version 3.2.2, 2011 software 15 was used for stunting, wasting, and underweight and exported to SPSS 19 for further analysis. Descriptive statistics such as frequency, percentage, mean, and SD were used to organize distribution of demographic and socioeconomic, maternal, and environmental characteristics.
Statistical significance of associations was assessed using chi-square tests. Logistic regression was performed and adjusted odds ratio (AOR) and unadjusted odds ratio with 95% CI were calculated to determine the independent effect of those variables that were found significant through univariate analysis. A P value of <0.05 was considered as statistically significant. All P values reported are 2 tailed.
Results
Distribution of sociodemographic characteristics of the participants is presented in Table 1. Reported mean age of the mothers was 26.7 ± 2.91 years and that of the children was 30.6 ± 16.5 months. The mean weight at birth of the children was 2.48 ± 0.36 kg.
Distribution of Sociodemographic Variables.a
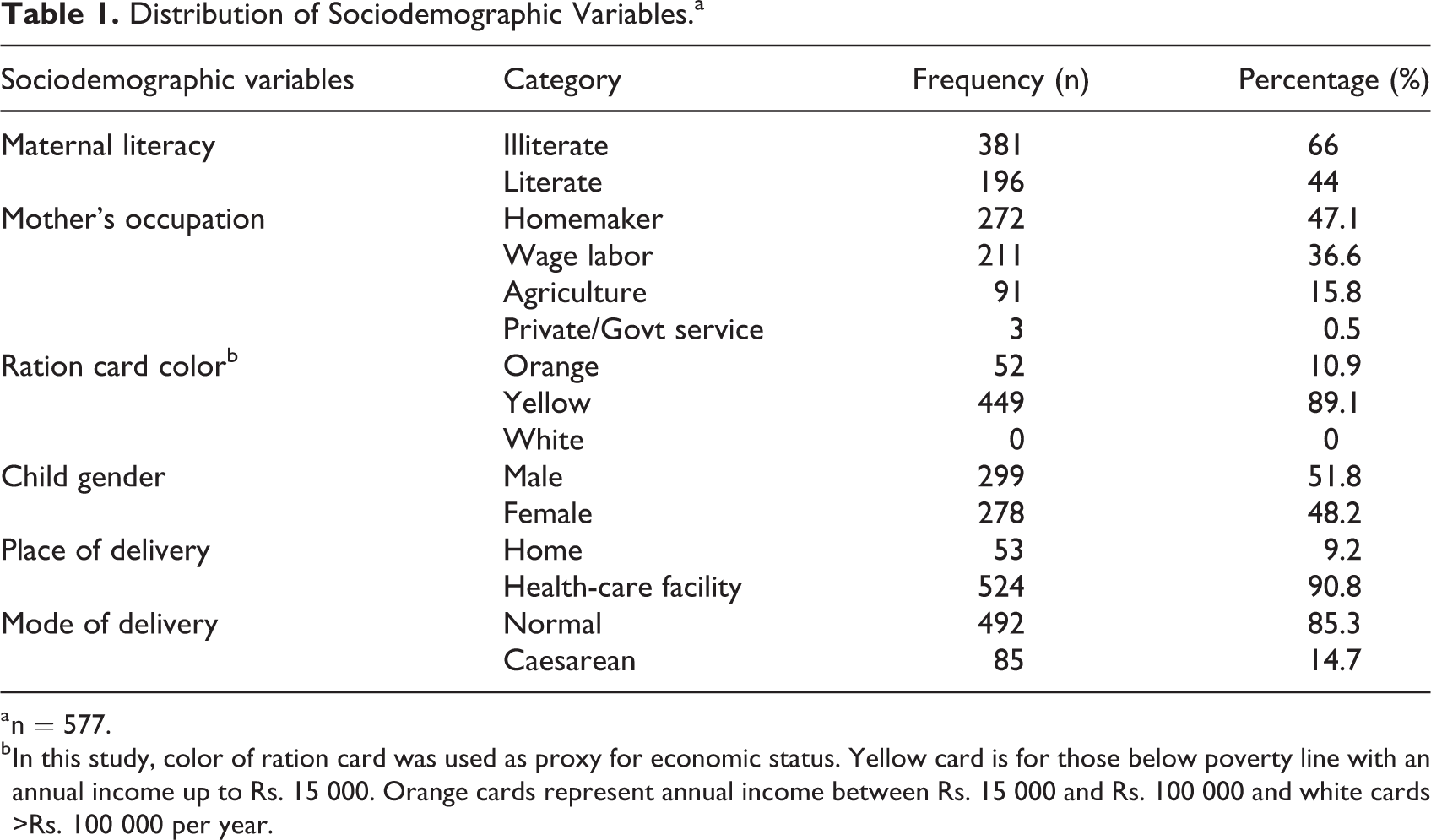
a n = 577.
b In this study, color of ration card was used as proxy for economic status. Yellow card is for those below poverty line with an annual income up to Rs. 15 000. Orange cards represent annual income between Rs. 15 000 and Rs. 100 000 and white cards >Rs. 100 000 per year.
Prevalence of undernutrition among children according to Z scores identified that among the manifestations of undernutrition, 30% were moderately underweight followed by a higher presentation of moderate and severe form of stunting accounting to >20% each. Overall prevalence of wasting was 13%. All manifestations showing >10% prevalence indicate the seriousness of the public health issue (Table 2). 16
Prevalence of Undernutrition Using Z Score.a
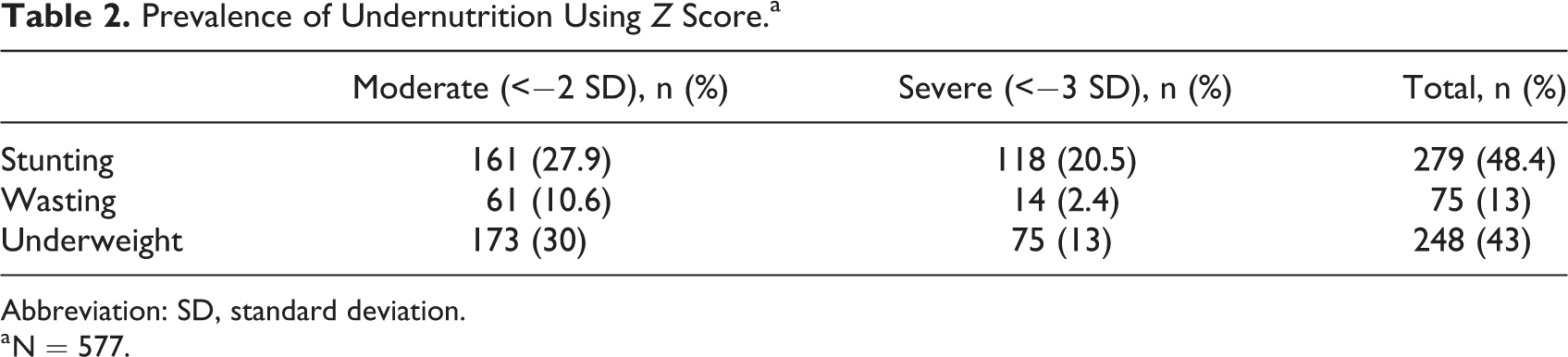
Abbreviation: SD, standard deviation.
a N = 577.
Table 3 shows the sex-specific prevalence of the children having single and multiple failures of the CIAF (groups B-Y). Of 577 children, 41.2% of the children were anthropometrically normal; 58.2% of children had one or more form of anthropometric failure. Among the single manifestations, greater percentage of children were wasted (14.9%) as compared to stunting (5%) or underweight (1.6%). As per CIAF categories of multiple failures, more than one-fourth (25.8%) of undernourished children were concentrated in group E (stunting + underweight). Low birth weight children comprised 43.5% of the total sample (Table 4).
Prevalence of Undernutrition Using Different Categories of Anthropometric Failure (CIAF) in Children.a
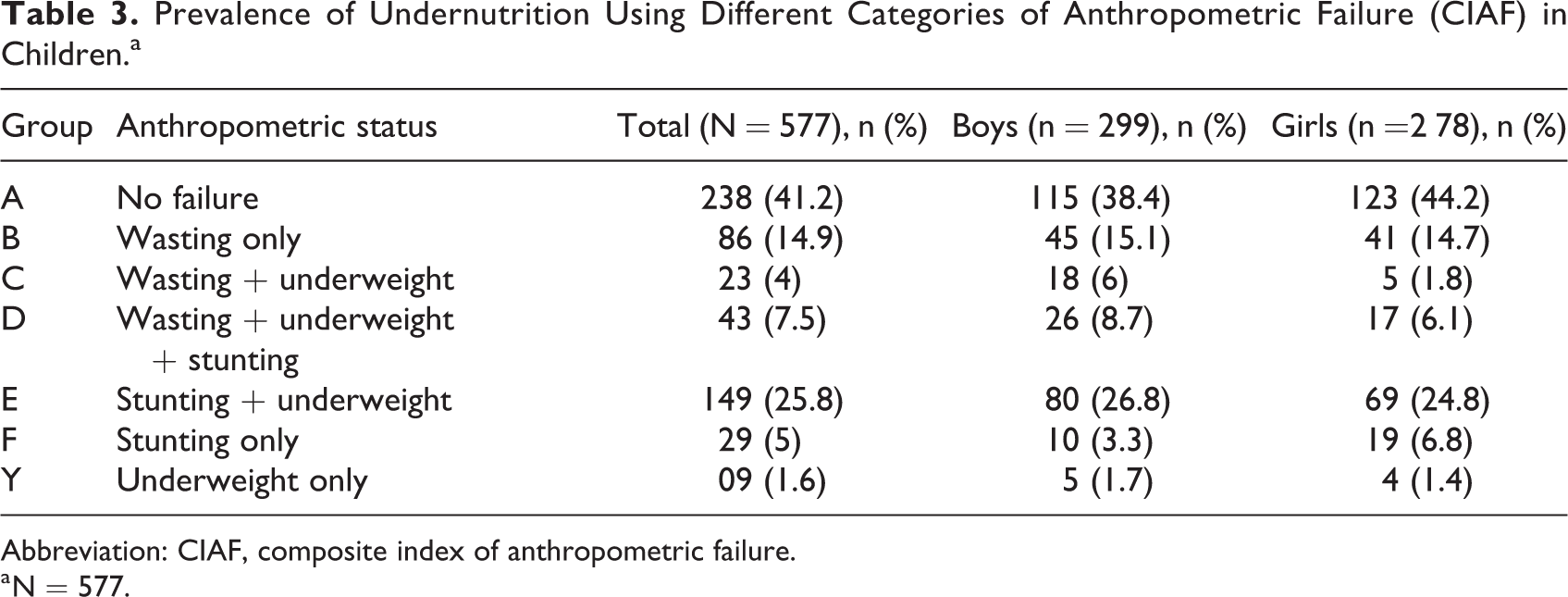
Abbreviation: CIAF, composite index of anthropometric failure.
a N = 577.
Binary Logistic Regression of Adjusted and Unadjusted Determinants of CIAF.
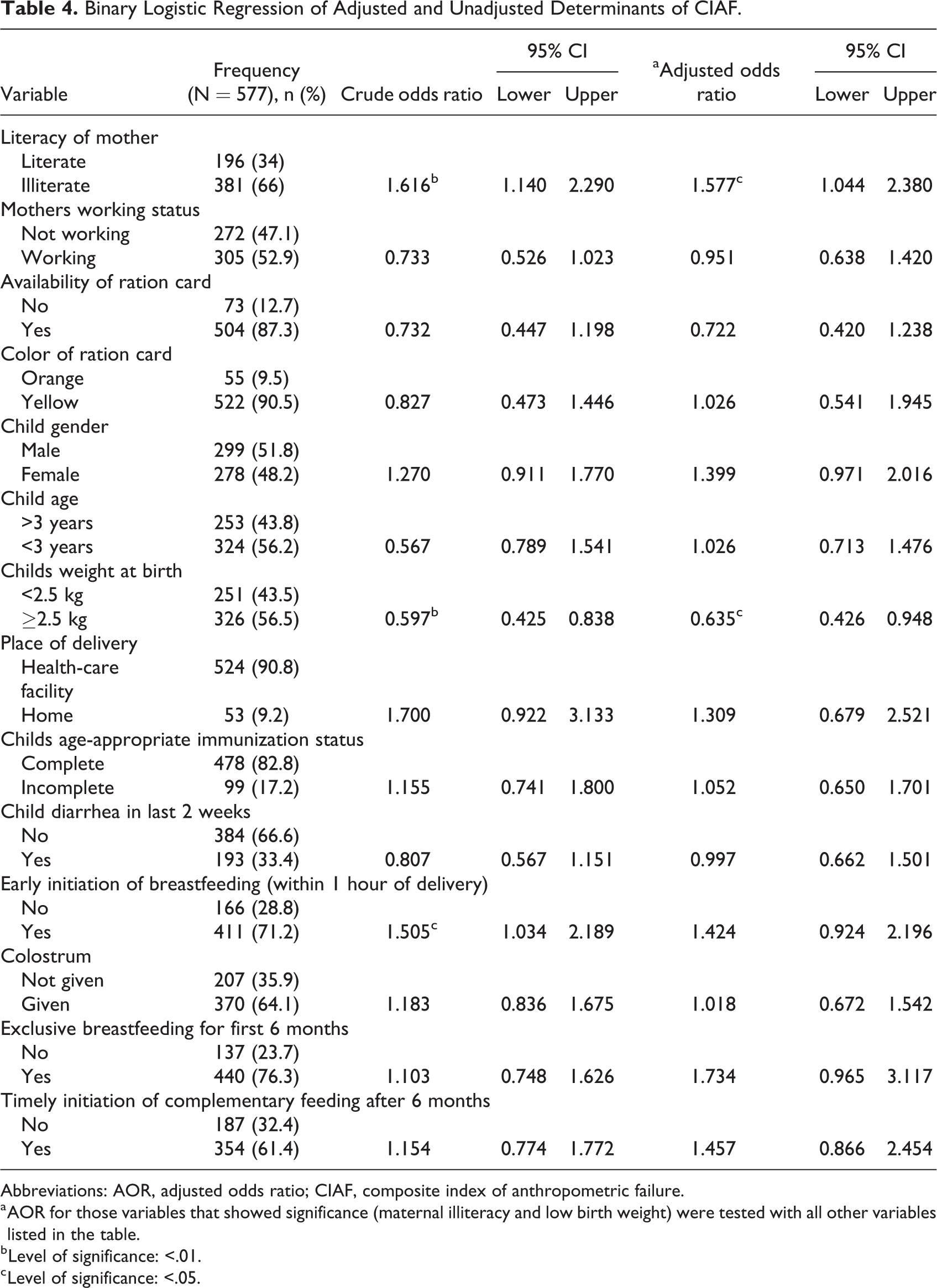
Abbreviations: AOR, adjusted odds ratio; CIAF, composite index of anthropometric failure.
a AOR for those variables that showed significance (maternal illiteracy and low birth weight) were tested with all other variables listed in the table.
b Level of significance: <.01.
c Level of significance: <.05.
Among the variables tested as risk factors for anthropometric failure, maternal illiteracy (crude odds ratio [COR] = 1.6 [1.1-2.2]), low-birth weight (COR = 0.5 [0.4-0.8]), and early initiation of breastfeeding (COR = 1.5 [1-2.1]) were significantly associated. Strength of association of variables such as socioeconomic status; working status of the mother; place of delivery; and child characteristics such as age, gender, immunization status, diarrhea, and breastfeeding practices, when adjusted with other variables maternal illiteracy (AOR = 1.5 [1-2.3]), and low birth weight (AOR = 0.6 [0.4-0.9]) stayed significant in the multivariable model (Table 4). The positive association found between early initiation and CIAF was not significant when adjusted with other variables.
Discussion
Ours is among the few studies that have assessed CIAF and its determinants in a tribal setting. Palghar in Maharashtra often attracts media attention for its high concentration of undernourished children and infant and child deaths. Background characteristics of the population in our study identified a higher percentage of women to be illiterate, compared to urban settings, 17,18 despite significant allocation of resources by the Ministry of Tribal Affairs have contributed to an overall increase in the literacy rates, nevertheless a decline in literacy rates among certain sections of the tribal population has been reported. 19,20 Similar is the situation in women’s participation in agriculture, where our study identified a small percentage of women engaged in agriculture, although subsidy ceiling specifically for women in tribal regions had been increased. 19 With much reliance on daily wages in nonagricultural sectors, 90% of the population studied were below the poverty line. Our study identified that a significant proportion of women utilized the government health care facilities for institutional deliveries. These observations are consistent with the national statistics where the overall utilization rates are higher in tribal regions but the increase in numbers is slow due to regional differences where some pockets still underutilize government antenatal care services. 21,22 Thus, a situation analysis of this tribal setting identified a transition phase where there is receding agricultural involvement, better utilization of maternity services, and yet little or no change in economic and literacy status.
Using Z scores, our study showed lesser prevalence of stunting, wasting, and underweight as compared to national surveys and other regional studies. 6,8,23 Work in Melghat, another tribal region in Maharashtra, showed a lesser prevalence as compared to our results. Varying levels of development in different tribal regions contribute to this variation. Nevertheless, as per WHO criteria of public health significance, all the above tribal regions have a population prevalence >15% and are categorized as regions with critical levels of undernutrition. Despite concentrated efforts, the change is slow as there is lack of development, poor roads, extremes of climatic conditions such as drought and migration for work that contribute to poor living conditions, food insecurity, and undernutrition. 24,25 Our study did not show gender differences in nutritional status indicative of nonexistence of gender bias in feeding or child care practices. This is similar to observations by Gosh and Varekar. 6 In our effort to study CIAF, we identified 60% to have any form of undernutrition, of which 40% had a combination of manifestations, such as wasting in combination with stunting or underweight. This identifies a huge proportion of critically undernourished children who need immediate intervention compared to single manifestation. Our earlier work among children aged 12 to 23 months has identified 75% prevalence of CIAF compared to the 60% in the present study. 26 This underscores that children in the critical age-group contribute to high burden of undernutrition among children younger than 5 years. Work done by Bharali et al 27 identified 51% CIAF among tribal children aged 2 to 5 years, lesser compared to our estimate, while Mandal and Bose 28 reported more than 70% manifestation of CIAF. In comparison to Z scores, CIAF draws attention to the greater proportion of the population who suffer from multiple manifestations of undernutrition. Thus, the advantage of measuring any public health event using composite indices provides an overall estimate of the problem of concern, while individual measurements may underestimate the magnitude and severity. 29 Studying the underlying biology of different manifestations of undernutrition and designing specific protocols based on specific predictors for CIAF would provide novel approaches to control undernutrition. 30
Predictors of CIAF identify risk factors of any form of undernutrition. Our study identified mother’s education and birth weight as predictors of CIAF. Among the limited existing literature of the determinants of CIAF, work done in urban Jammu identified morbidity and early weaning, 31 while number of children and mothers nutritional status emerged in a Bangladesh study. 32 Work in Ethiopia further identified birth order and age of children as critical factors. 33 The common predictors such as mother’s literacy and birth weight that emerged in these studies are in consonance with our results. Early initiation of breastfeeding emerged as a risk factor for growth failure in our results. However, when adjusted with other variables, it was not significant.
Besides the above-mentioned risk factors, impact of social environment on height has been studied in human auxology. According to this theory, children will not remain stunted due to starvation in early years. A stimulating environment or setting enabled achievement of adult height. 33 It is well established that nutrition alone does not bring about desired improvement in nutritional status 34 emphasizing the need to address non-nutritional factors to improve growth and development throughout the growing phase. Although some studies show association between background characteristics, ours did not. For instance, associations between economic status and immunization status were not evident. Our study utilized color of ration card as proxy indicator for economic status and not actual income, and the sample was a homogenous one, which could have contributed to these results. Considering immunization and undernutrition, it is quite evident from literature that with increasing age, immunization has little effect 35 on nutritional status and our study considered children younger than 5 years compared to few others that studied children younger than 2 years. Further, such associations are likely to emerge when studied with severity of undernutrition. 36
Thus, to address undernutrition in any of its form, emphasis on maternal nutrition, literacy, and economic well-being need to be prioritized. In tribal settings, health care services, apart from being inadequate, are also poor in quality and are often inappropriate for the geographical setting as they are replicated as in other settings and lack relevance. As observed in our study, current interventions have improved nutritional status marginally with no improvement in economic status. These results identify the need for a comprehensive approach to improve the living conditions and food security in these settings to improve nutritional status of children.
The results of the study need to be interpreted with care as it comes with the following limitations. Although CIAF identifies a greater percentage of children as malnourished, it does not address wasting masked by edema. Thus, it would be appropriate to combine clinical assessment along with CIAF. Further, the prevalence and risk factors vary according to age and settings, which needs consideration while planning intervention.
Conclusion
Economic growth in the nation despite alarming levels of prevailing of undernutrition in tribal regions highlights inequality in economic development. Higher prevalence of undernutrition as per CIAF underscores the critical conditions in tribal settings that necessitates immediate intervention. Policies aimed at improving literacy of mothers, creating awareness on infant and young child feeding practices, and empowering women to increase household income are key factors to address any form of undernutrition in these tribal settings.
Footnotes
Acknowledgments
We thank DBT for funding the project, the authorities who provided the necessary permissions to work in Palghar and the participants of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Department of Biotechnology (DBT) under Grant—BT/IN/Indo-US/Foldscope/39/2015, India.