
Abstract
Background:
The COVID pandemic and subsequent lockdown has disrupted food supplies across large parts of India, where even prior to the pandemic, food insecurity and malnutrition were widely prevalent. Tribal populations in southern Rajasthan, India, live in extreme scarcity, rely mainly on outward migration for sustenance, and have been significantly affected by the pandemic. In this study, we assess the availability of foodstuffs at the household level and community experiences about satiety and hunger during lockdown.
Methodology:
We conducted a rapid assessment of food security in rural southern Rajasthan, India, using a structured questionnaire. Trained interviewers conducted telephonic interviews using KoBoToolbox, an open-source tool. A total of 211 respondents including community volunteers, family members of tuberculosis patients and malnourished children, pregnant women, and influential members in the villages participated in the study.
Results:
A cereal was reported to be present by 97% of the respondents, two-thirds had pulses, and nearly half had milk. The amount of cereals available was adequate for about 5 months and that of pulses, oil/ ghee, and sugar for about 1 to 2 weeks. Two-thirds of the respondents reported that food in their households was sometimes not sufficient for the amount they wanted to eat, and 97% of these mentioned not having money to buy food as the reason for not having sufficient food.
Conclusion:
This study highlights widespread food insecurity among tribal communities in southern Rajasthan, and the scenario is likely to be similar in other tribal migration dependent areas of the country.
Introduction
The COVID pandemic, subsequent lockdown, halting of employment and incomes has affected almost the entire country, with those working in the informal sector being affected the most. Lack of food created panic and unrest after the lockdown was announced, and fragility of the communities was visible clearly, with a large number of families having no food to eat. Grains from the previous harvest had been used up, the current crop was not yet ready, food supplies from the public distribution system (PDS) had not yet reached, and other sources of income had abruptly halted. The global scenario is equally worrying, with the Food and Agriculture Organization estimating the number of people with food insecurity to double by the end of 2020. 1
Food security of population requires all the time access, both physical and economic, to sufficient, safe, and nutritious food that meets their dietary needs and food preferences for an active and healthy life. 2 The relationship between food security and malnutrition is best understood for children—for whom insufficient food intake is recognized as 1 of the 2 key determinants of malnutrition. 3 In India, malnutrition was deeply entrenched even prior to the pandemic. Over one-third of the children are stunted, and 1 in 5 of them is wasted. 4 The adults too are not spared, with 1 in 5 women as well as men being malnourished. 4 Such high levels of malnutrition point toward a widespread food insecurity. A further cause for concern is the evidence which suggested that the consumption of nutritious foods in rural population, had actually declined in the past 3 decades. 5
Rural, tribal communities in southern Rajasthan rely predominantly on outward migration for sustenance. In these areas, availability of nutritious food items such as pulses, oil, milk, vegetables, and fruits in the region has been extremely poor, which is also reflected in much higher levels of malnutrition as compared to the national, as well as the state average. 6 The food crisis mobilized organizations, individuals and the government, that came together, and provided immediate (though short term) relief. This situation also prompted us to delve into an enquiry on availability of foodstuff in households, and community experiences about satiety and hunger.
Methodology
We conducted individual interviews to ascertain food availability in their household, and their perceptions on adequacy of food, during the lockdown. The sample included patients visiting AMRIT Clinics (not-for-profit clinics) and a Primary Health Center (PHC) that we manage in partnership with government, and other community members, all of whom possessed a mobile phone.
The patients included those suffering from tuberculosis (TB), parents of children with severe acute malnutrition, and pregnant women seeking treatment at AMRIT clinics and PHC Nithauwa. Community members included those from the clinic advisory committees, and community volunteers. As mobility was severely restricted, the interviews were conducted telephonically. Trained and experienced interviewers administered a structured questionnaire, developed in “Kobotoolbox”—an open-source tool for field data collection. All respondents were above the age of 18 years. The respondents were explained about the study and their verbal consent was sought at beginning of the interview.
Results and Discussion
Lockdown was announced in the region on March 22. The survey began on May 12 and ended on June 10. We reached out to 269 respondents and could conduct the interviews with 211 of them. We were unable to connect to 58 respondents either due to poor connectivity or because the phone number was wrong or was switched off. All the respondents provided verbal informed consent. The respondents included community volunteers (72), family members of TB patients and severely malnourished children (38), pregnant women (53), and influential members in the villages (48). Of all respondents, 97% were tribals. There were 67 men and 144 women. All but 3 reported having a ration card, 41% had cards meant for families that are below poverty line, and 9% had an Antyodaya card, meant for destitute and vulnerable. The mean family size was 5. The findings from the study are shared below:
Functioning of PDS
Although 99% of the respondents possessed a ration card, only 82% received wheat and pulses through the scheme. Families were denied food grains for not possessing an Aadhar card (national unique ID card), or if their name did not appear in the online list even when they did have an Aadhar card, or if their fingerprints did not match those in the database—the last seen specially among the elderly. Many families who did have a ration card, including several of our own health workers, reported being given smaller amounts than what was due to them.
Availability of Food Items in the Households
Cereals were available in almost all the households—97% reported availability of wheat, 49% had maize, and 48% had both wheat and maize (Figure 1). Only 21% of the households had other cereals such as rice, bajra (pearl millet), and semolina. The cereals came both from their own yield as well as that provided through PDS. Pulses were present in 65% of the households, and 43% of them reported having only one pulse. Of the respondents, 78% reported having one or more vegetables. When, however, onion, potato, green chillies, and garlic, vegetables with relatively lower nutritional value, were removed from the list, only 34% of the respondents were left with having one or more vegetables. Fruits were reported to be present by 45% of the respondents. About half (49%) reported availability of any milk, and another 15% reported some milk-product, most commonly buttermilk.
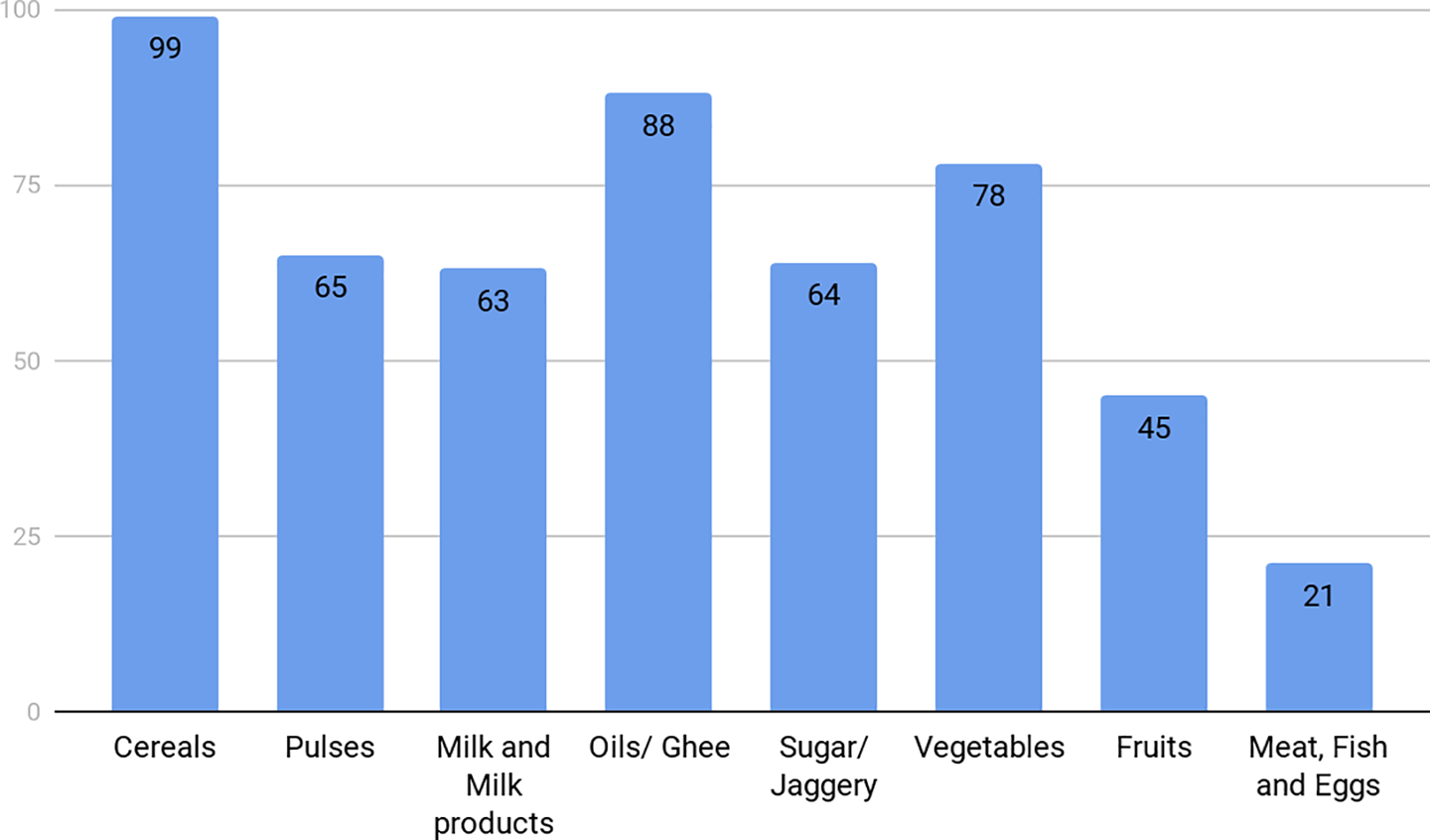
Availability of foodstuffs (percentage).
Most of the vegetables and fruits came from their own kitchen gardens or the locally grown trees. Travel to the nearest markets was difficult as these were still far (15-20 km or more), public transport was not available, and police restricted movement of villagers. People also stopped buying from vendors coming to the villages, due to fear that these could spread COVID. Nonperishable items such as pulses, oil, and spices were sourced from the small grocery shops in the villages, which were fast running out of supplies due to disruption of supply chain. These started raising the prices, which went up by 30% to 50%. At the same time, people had little liquid cash, and started bartering wheat from the recent harvest to buy these items. Wheat was sold at a price around Rs. 15 (∼0.2 USD) per kg, the lowest for several years. Many families which were not able to trade their wheat survived on a mainly cereal-based diet together with small amount of spices, most often chillies or garlic.
Respondents’ Experience on Satiety and Hunger
We shared 4 scenarios with the respondents regarding their perceptions on the adequacy of food in their households and asked them to choose which of these described their situation best. These included the following: food in the household is sufficient for the amount they want to eat, or the food is sometimes not adequate, or it is mostly not adequate, or that they do not know. Only a third of respondents reported that they have sufficient food for the amount they want to eat, while nearly two-third reported that sometimes food is not adequate for how much they want to eat (Figure 2). Almost all (97%) the respondents reported not having sufficient money for buying food as the reason for not having as much food as they would want.
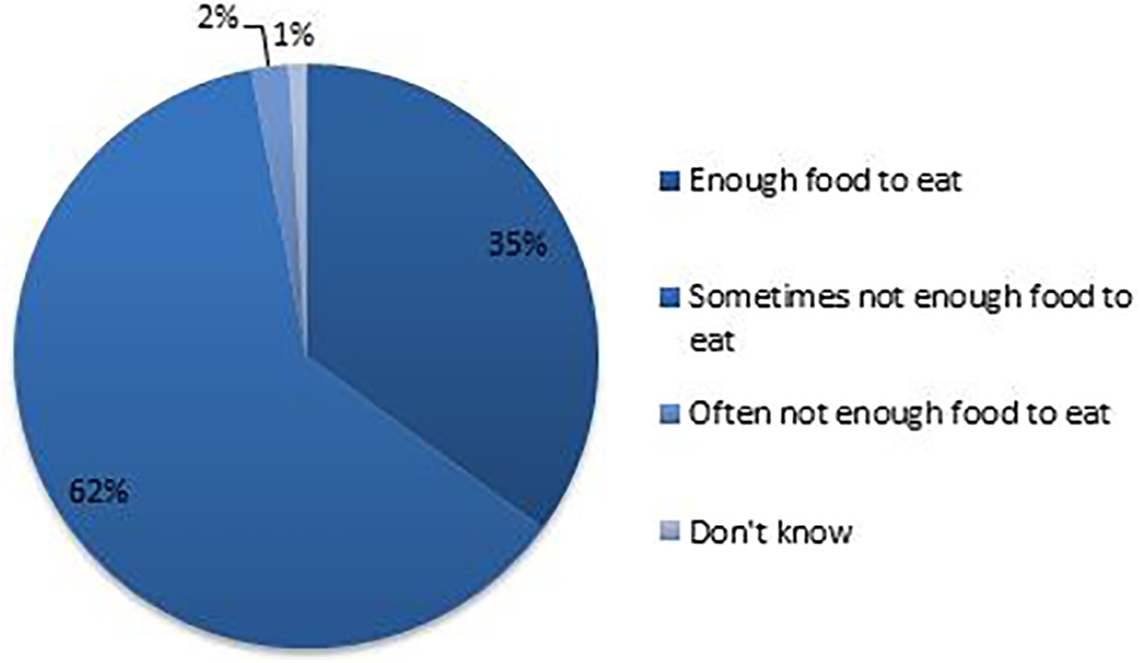
Perception on adequacy of food in the household (N = 211).
Nearly half of the respondents (47%) reported cutting down on a meal or skipping a meal altogether in the last one month as they did not have sufficient money. Half of them reported that this happened 1 to 2 times in the month, while the others shared that this happened more frequently. Two (1%) persons reported not having food for the entire day, on account of not having enough money.
How Long Will the Food Supplies Last
We could ascertain detailed information on actual amounts of nonperishable items (cereals, pulses, oil and ghee, and sugars) available in the households for 155 respondents. Although families had a fair amount of cereals (median amount approximately 240 kgs), the amount of other items was very sparse, with pulses, oil/ghee, and sugar being 1 kg each (median). We also estimated how long the available supplies would last (Figure 3), using the following assumptions—that each household had 2 adults (as families in the region are predominantly nuclear) and the remaining family members were children, and that the adults indulged in moderately strenuous activity. 7 We calculated the amount of food items required per day in each household, and expected duration for which supplies would last, also for each household. We finally calculated the median duration for which supplies would suffice, across the respondents. Although the amount of cereals available in the households seemed sufficient for a period of 5 months, pulses and sugar were enough for just over a week, and oil or ghee (clarified butter) for a fortnight.
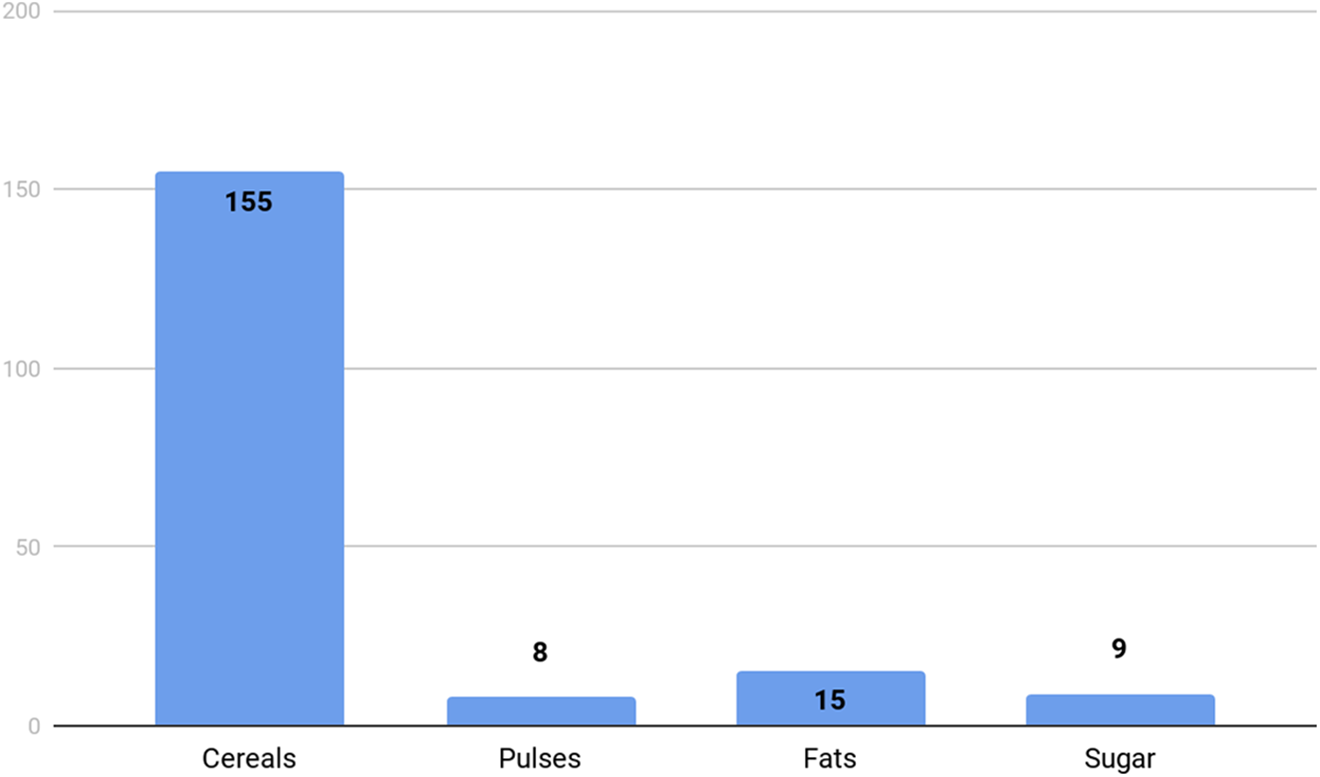
Median number of days each food ingredient will last.
Conclusions
The study highlights the widespread food insecurity in tribal communities in southern Rajasthan. Although cereals were reportedly present in all households, only two-thirds had any pulses, half had milk, and about one-third of them had a nutritious vegetable. The supplies of all items except cereals were also very small, just enough for 1 to 2 weeks. It must also be mentioned that at least some foodstuff was reported to be present in almost all the households.
All the respondents in the study possessed a mobile phone. At the time the study was carried out, travel in the field was severely restricted and conducting it over phone was the only option possible. It is likely that availability of food, and self-reported inadequacy of food, in the general population may be even worse than what we observed among those who participated in the study.
Findings from the study call for urgent measures to promote household food security. It may be noted that tribal populations in southern Rajasthan are among the most vulnerable in the country, and findings from these areas may not hold true for the country as a whole. These would however hold true for India’s tribal populations, which make up almost 9% of the population of the country (over 100 million). 8
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.