
Abstract
Background:
Zinc is an essential micronutrient for human health. Approximately 1.4% of deaths worldwide are related to zinc deficiency. In Mexico, 33% of children younger than 5 years are zinc deficient.
Objective:
To give an overview of zinc supplementation and fortification in children younger than 5 years through the analysis of current regulations in Mexico, the availability of these products, and the opinion of Mexican experts in this field.
Methods:
We gave an overview of zinc supplementation and fortification strategies in the Mexican pediatric population by conducting a literature review of Mexican studies and national standards concerning zinc supplementation and fortification. Semistructured interviews were conducted with personnel from the main producers of zinc supplements and fortified products and from social assistance programs in Mexico.
Results:
Zinc supplementation in Mexico has been associated with reduction in the duration and incidence of diarrhea. Through interviews with experts, we identified several barriers in achieving adequate zinc consumption such as problems in social assistance programs that distribute zinc-fortified foods, lack of specific dietary recommendations regarding the intake of zinc, lack of regulation of nonpatented zinc supplements, and inconsistencies in public health actions due to political and administrative changes.
Conclusion:
Despite current regulation and efforts made by social assistance programs, zinc deficiency continues to be a prevalent public health issue. Mexico requires an in-depth analysis of existing barriers and alternatives in order to reduce zinc deficiency.
Introduction
Zinc plays an important role in the immune system, as it participates in the activation of transcription factors, acts as an antioxidant and anti-inflammatory agent, and participates in the maintenance of skin and mucous membranes. Additionally, zinc has been implicated in multiple phases of cellular metabolism and is essential for the action of more than 100 enzymes. 1,2 Zinc deficiency is a large public health issue among children. Zinc deficiency may lead to stunting, alterations in cognitive development, and morbidity and mortality due to infectious diseases. 3 Globally, it is estimated that zinc deficiency is associated with 16% of lower respiratory tract infections, 18% of malaria, and 10% of diarrheal disease, being responsible for 800 000 deaths. 4
Zinc deficiency may be attributed to inadequate intake of zinc, malabsorption due to high intake of fiber and phytates, and loss due to diarrhea. 4 Supplementation and food fortification in children are some of the most common strategies used to improve diet quality and increase the consumption of certain nutrients. 5 Interventions aimed at increasing the intake or bioavailability of zinc in children have aimed to reduce the incidence of infections, their duration, and promote linear growth and reduce mortality.
Systematic reviews have shown that zinc supplementation and fortification have a positive effect on serum zinc levels, 6 anemia, weight gain, 7 and during pregnancy has been found to not modify the risk of low birth weight, but it did modify the risk of preterm delivery. 8
In general, zinc fortification has been documented to have significant impact on serum zinc concentration. With respect to linear growth and height velocity, zinc fortification studies show nonsignificant effects. However, the subgroup analysis showed significant improvement in height velocity among newborns with very low birth weight. About the food fortification effect on weight gain, no significant impact was observed, although subgroup analyses have suggested a positive trend in weight gain among newborn infants, low birth weight infants, and infants at risk of stunting. 6
However, these results have been inconsistent regarding linear growth, as zinc promotes a greater linear growth rate in very low birth weight infants, but not in healthy newborns. 6
Oral administration of zinc (≥5 mg/d) in children older than 6 months shortened the duration of diarrhea by half a day in the intervention groups with normal weight, and by a day in children with malnutrition, when compared to the controls. 9 Additionally, zinc supplementation in children aged 6 months to 12 years has been associated with a significant reduction in mortality risk associated with diarrhea, and lower incidence of respiratory tract infection, malaria, and all-cause mortality, as well as a reduction in the incidence of diarrhea. 10 In contrast, in children aged 2 to 59 months with pneumonia who received zinc supplements combined with traditional antibiotic treatment, they found no significant differences in clinical recovery time, tachypnea, time to hospital discharge, or thoracic retractions. 11 Also, zinc supplements have been found to cause no effects in reducing the incidence of middle ear infections in healthy children; however, they may reduce the incidence of these events in children with severe malnutrition. 12 On the other hand, zinc supplementation in children younger than 5 years did not show differences in mental and psychomotor development indexes when compared to controls. 13 Therefore, in the present study, we aim to give an overview of zinc supplementation and fortification in children younger than 5 years through the analysis of: (1) the research conducted in Mexico on zinc supplementation and fortification trials and nutritional assistance programs with preschool children, (2) current regulations in Mexico related to zinc supplementation and fortification in preschoolers, and (3) interviews with Mexican experts on zinc supplementation and fortification.
Methods
We conducted a literature search on zinc supplementation and fortification in the pediatric population using PubMed, Ovid, Cochrane Database of Systematic Reviews, Lilacs, and Google Scholar databases. The keywords used were (zinc or Zn) and (children or child or infant or adolescent). We considered clinical trials published between 1990 and 2017 in both Spanish and English for the following interventions: zinc supplementation alone or in addition to other nutrients and fortified food with zinc. Studies in the non-Mexican population and older than 5 years old were not included.
In addition, an independent review of the Mexican national standards concerning products supplemented with zinc and the commercial availability of zinc supplements and zinc-fortified products for children was conducted using supermarket and pharmacy websites. Multivitamin supplements were excluded.
Furthermore, a qualitative study was carried out through 8 semistructured interviews of approximately 10 open-ended questions to personnel representing a range of main producers of zinc supplements and fortified products and the most important nutrition assistance programs in Mexico. Interviews were conducted for approximately 30 minutes in closed spaces where privacy and confidentiality could be maintained.
Finally, interviews were recorded with prior oral authorization for its subsequent transcription, or were received in written form via e-mail. The content of the interviews was analyzed through the qualitative analysis software (QDA) ATLAS.ti version 8.4.
Results
In the context of the present study, the results are divided as follows: (1) literature review of clinical trials and nutritional assistance programs in Mexico in preschool children, (2) national standards and regulations of zinc supplementation and fortification in Mexico in preschoolers, and (3) interviews with experts about the main barriers that obstruct access to zinc-fortified products and supplements.
Literature Review: Clinical Trials and Nutritional Assistance Programs in Mexico
Clinical Trials
In 2016, a double-blinded randomized factorial clinical trial was performed that included children 6 to 15 months of age from the community “La Magdalena Atlicpac” in the State of Mexico. Children were assigned to 1 of 4 groups: (1) 20 000 IU of retinol every 2 months in children ≤1 year old, or 45 000 IU in children >1 year; (2) 20 mg/d of elemental zinc (zinc methionine); (3) combined supplementation with vitamin A and zinc; and (4) placebo. The children were monitored for 1 year. In this study, they found that zinc supplementation reduced diarrhea in children whose homes had a dirt floor and whose mothers were more educated. 14 Additionally, children from the vitamin A and zinc group had lower prevalence of Giardia intestinalis and Ascaris infections, and lower risk of diarrhea due to Ascaris lumbricoides. The group supplemented only with zinc showed increased prevalence of infection by A lumbricoides and a longer duration of Entamoeba histolytica infections, but a reduction in the incidence of diarrhea associated with E histolytica. In addition, reductions in the duration of Giardia infections were observed in all 3 intervention groups, compared to the placebo group. 15
Another study was conducted in 4 communities near Querétaro city in 266 children aged 6 to 43 months with anemia (Hb < 11.7 g/dL), and who had been breastfed exclusively. Children were randomized into 5 intervention groups for 4 months: (1) 20 mg/d iron supplement; (2) 12 mg/d of iron plus 50 μg/d of folic acid; (3) multivitamin (10 mg of iron and 10 mg of zinc/d, among others); (4) a micronutrient fortified complementary food as porridge powder (10 mg of iron and 10 mg of zinc/d, among others); (5) and fortified water (5.6 mg/d of zinc, 6.7 mg/d of iron, and 44.4 mg/d of ascorbic acid). The study concluded that the supplements promoted greater increases in hemoglobin levels and greater reductions in the prevalence of anemia than the micronutrient fortified complementary food group; however, only groups 2 and 3 presented significant differences with respect to baseline measurements. It should also be noted that fortified food strategies, groups 4 and 5, had greater acceptance than did supplements. 16
Nutritional Assistance Programs to Reduce Zinc Deficiency in Mexico
According to the National Nutrition Survey of 1999 and the National Health and Nutrition Surveys (ENSANUT, by its Spanish acronym) 2006 and 2012, a reduction in the prevalence of zinc deficiency in children younger than 5 years (1999, 33.1%; 2006, 27.5%; and 2012, 17.7%) was observed, probably due to interventions at the federal level such as the LICONSA Milk Supply Social Program (PASL, by its Spanish acronym) and the PROSPERA Program that provides fortified foods and zinc supplements to children, pregnant women, and infants. 17
PROSPERA
Since the 1970s, the Federal Government of Mexico has enacted social programs focused on assisting impoverished populations such as the Investment Program for Rural Development (PIDER, 1970-1982), the General Coordination of the National Plan for Depressed Areas and Marginalized Groups (COPLAMAR, by its Spanish acronym, 1976-1983), the National Solidarity Program (PRONASOL, by its Spanish acronym, 1988-1995), and the Education, Health and Nutrition Program (PROGRESA, by its Spanish acronym, 1997-2002). PROGRESA changed its name to Oportunidades (2002-2014) and then to Social Inclusion Program (PROSPERA, by its Spanish acronym) from 2014 to date. 18
PROSPERA was implemented to end the intergenerational transmission of poverty through various actions such as cash transfers to improve household diets, dietary supplements for children from 6 to 59 months, and pregnant women, education in health and nutrition, and access to primary medical care. Currently, PROSPERA has 3 different food supplements (Nutrisano, Nutricrece, and Vitaniño) presentations (Table 1) for rural and urban children aged 6 to 59 months, that are designed to provide 5 to 10 mg of zinc per day. 19
Zinc Availability in Supplements and Fortified Foods From Nutritional Assistance Programs.
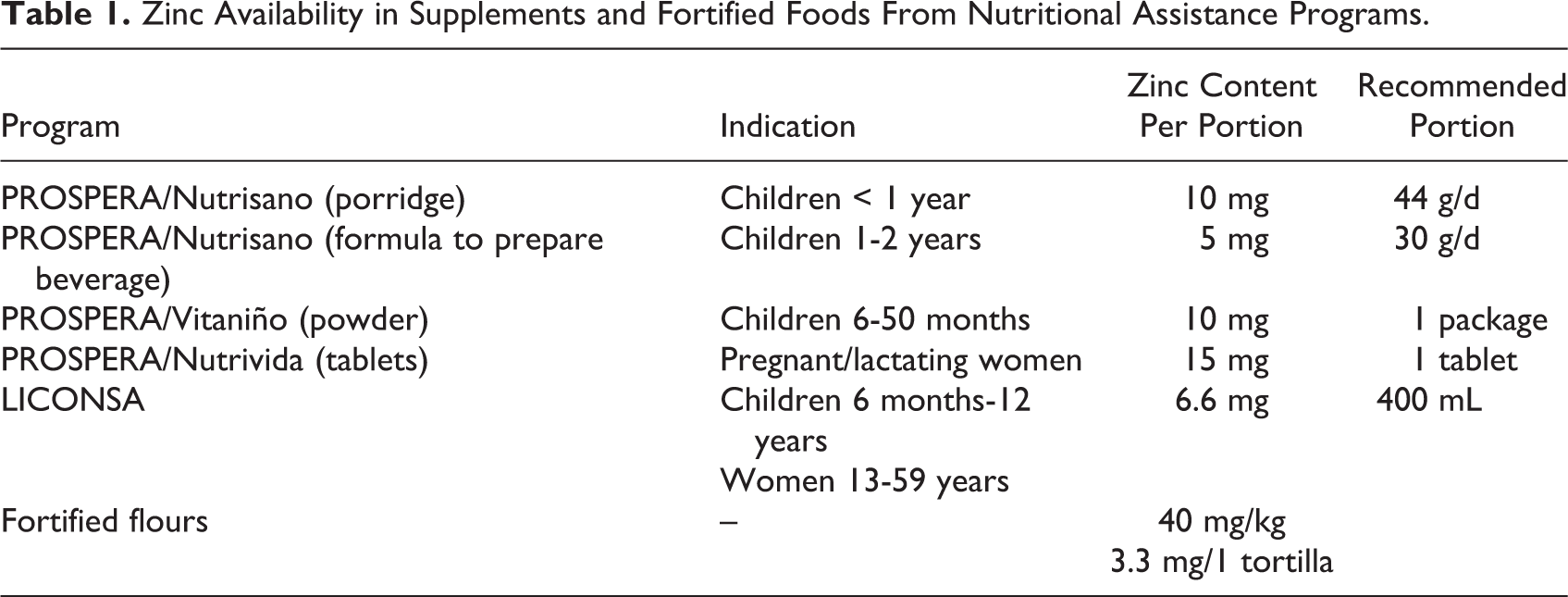
In a randomized sample of rural communities in 6 states of Mexico, children younger than 5 years were randomized to be enrolled in PROSPERA or to the control group for 1 year. Daily consumption of zinc was higher in the intervention group than in the control group (2.96 mg/d and 2.65 mg/d, respectively). 20 PROSPERA also reported improvements in the incidence of anemia and a higher linear growth rate in children younger than 2 years; yet, this population still continue to face nutritional challenges. 21
LICONSA Milk Supply Social Program
The PASL benefits almost 6.5 million Mexicans, through the production and distribution of 3.4 million liters of milk per day, mainly in rural areas. Milk is sold at affordable prices ranging from $1.00 to $5.50 22 Mexican pesos to households with children aged 6 months to 12 years, women from 13 to 59 years, adults >60 years and individuals with chronic diseases and/or disabilities. The recommended dose for children aged 6 months to 12 years is 400 mL/d (5.28 mg zinc/d). Several studies in Mexico have shown that PASL improves zinc and iron concentrations in children. In a clinical trial, which included children from 10 to 30 months of age, from a community of low socioeconomic level in the state of Puebla, they observed that those randomized (n = 58) to take 2 portions of 400 mL/d (a portion) of LICONSA milk fortified with iron (5.28 mg/400 mL, as ferrous gluconate), zinc (5.28 mg/400 mL, as zinc oxide), and ascorbic acid (48 mg/400 mL) for 6 months showed no differences in serum zinc levels; but, improvements in hemoglobin levels were observed when compared to children who received whole unfortified milk. 23
Another study carried out in the marginalized neighborhoods of Hermosillo, with children aged 3 to 5 years observed that children who were part of the PASL for 6 months (n = 54) presented a statistically significant increase in serum zinc levels of 45.2 μg/dL, in hemoglobin of 1.13 g/dL and ferritin of 5.83 μg/L, in comparison with the group that consumed unfortified whole milk (n = 23), in which no significant changes were observed. 24
Fortified Wheat and Corn Flours Project
The fortified wheat and corn flours project was inaugurated in 2005 with national coverage. This program ensured the fortification of nixtamalized (lime-treated) corn flour and of wheat flour with 2 mg/kg of folic acid, 40 mg/kg of iron, 40 mg/kg of zinc, and that they would contain thiamine (vitamin B1), riboflavin (vitamin B2), and niacin (vitamin B3) in accordance with the standard NOM-247-SSA1-2008 (NOM, 2008). 25 National wheat flour fortification levels increased from 52% in 2010 to 76% in 2017, whereas the fortification of corn flour has been less widespread, from 18% in 2010 to 35% in 2017. 26
“Zinc Saves Kids,” United Nations International Children’s Emergency Fund Mexico
In August 2016, United Nations International Children’s Emergency Fund (UNICEF) announced an agreement with the International Zinc Association in Mexico called “Zinc saves kids.” It was established to reduce the incidence, duration, and severity of acute diarrheal diseases and respiratory infections, in addition to promoting zinc intake in children younger than 6 years. This program began in Mexico in 2016 with affiliates of the Mexican Social Security Institute (IMSS, by its Spanish acronym) training physicians, promoting educational activities with the families, providing visual demonstrations on the importance of zinc supplements for children younger than 6 years, and developing a proposal to modify the Mexican official standards for the treatment of diarrheal and acute respiratory diseases in children younger than 6 years. 27
National Standards: Regulation of Zinc Supplementation and Fortification in Mexico
Fortification and Enrichment of Foods and Nonalcoholic Beverages
The Mexican Official Standard-NOM-086-SSA1-1994-: Goods and services. Food and nonalcoholic beverages with modified composition establishes 5% to 100% of the recommended dietary allowance (RDA) per serving as the limit range for the addition, fortification, and enrichment of foods and nonalcoholic beverages, as long as that the nutrient consumption in usual conditions does not exceed the RDA (5 mg/d, of zinc for children aged 0-5 years). It also indicates that gluten-free products used to replace staple foods, such as flour or bread, should provide approximately the same amount of vitamins and minerals as the original. 28
Fortification of Corn and Wheat Flours
Initially, the Mexican Ministry of Health mandatorily required fortifying wheat flour with 2 mg of folic acid/kg of flour and 35 mg of iron (as ferrous ion)/kg of flour. 29 However, the standard NOM-247-SSA1-2008: Products and services. Cereals and their products, 30 also considered the fortification of corn flour and the addition of zinc to flours; indicating that each kilogram of nixtamalized corn flour and wheat must be fortified with 40 mg of zinc (as zinc oxide), 2 mg of folic acid, and 40 mg of iron (as ferrous sulfate or fumarate). In addition, each kilogram of flour must be replaced with 5 mg of thiamine (as thiamine mononitrate), 3 mg of riboflavin, and 35 mg of niacin (as nicotinamide). Finally, for durum and semolina flour, the nutrient restitution and addition may be made when preparing pasta using the same amounts. Then it comes to the pasta flours, approximately 80% of the standard zinc oxide will suffice. 30
Recommended Daily Intakes and Labeling of Products With Zinc Content
NOM-051-SCFI/SSA1-2010: General labeling specifications for pre-packaged foods and nonalcoholic beverages-Commercial and health information established a mandatory declaration of important nutrient information (by 100 g, 100 mL, per serving or per container) or with declared nutritional properties for the labeling of prepackaged foods and nonalcoholic beverages. Vitamin and mineral content may be reported. If the product contains dairy, the Mexican RDA and dietary reference intakes (DRI) included in this standard is encouraged to be used. The suggested daily intake of zinc is 10 mg/d based on a 2000 kcal diet. 31
Similarly, standard NOM-247-SSA1-2008 (NOM, 2008) 30 states that grains and their by-products must declare the number of servings contained in the package and nutritional information in numerical form (per 100 g, 100 mL or per serving or per container). Complementary nutritional information may refer to micronutrients (such as zinc) only if DRI exists and nutrient content per portion is ≥5% of the DRI. The zinc DRI for the Mexican population is 10 mg/d. For prepackaged wheat and nixtamalized corn flours, the content of various micronutrients, including zinc, in milligrams per 100 g of the product, and its source are labeled. 30
The NOM-131-SSA1-2012: Products and services. Infant formulas, continuation and special nutritional needs formulas. Food and non-alcoholic beverages for infants and young children, indicates the following zinc reference values for the Mexican pediatric population to be used to report (as a percentage) on the labeling of food products for infants and young children: for infants from 0 to 6 months. This standard does not specify a recommendation due to insufficient information needed to establish an RDA; and for 7 to 12 months and 1 to 3 years of age, RDAs of 3.8 mg/d and 4 mg/d are indicated. In addition, this standard considers zinc acetate, zinc carbonate, zinc chloride, zinc gluconate, zinc lactate, zinc oxide, and zinc sulfate as acceptable zinc sources. 32
In contrast, the document “Technical Bases for the Supplementation of Vitamins and Minerals in Childhood and Adolescence” 33 considers the following DRI for zinc: 3 mg/d for 6 to 11 months, 5 mg/d for 1 to 9 years, and 8 to 11 mg/d for ≥10 years. Finally, as mentioned above, the standard NOM-086-SSA1-1994 (NOM, 1994) 28 reports the zinc DRI as 5 mg/d for 0 to 11 months and 15 mg/d for 1 to 3 years of age.
The Official Mexican Standard, NOM-043-SSA2-2012: Basic health services. Nutrition promotion and education stipulates the adequate intake of iron and zinc during complementary feeding through the daily consumption of meat and other animal foods (1-2 ounces) from 6 months of age. They also list other important sources of zinc: animal source foods (dairy, meat, eggs, and seafood), legumes (beans), vegetables (wheat sprouts) and nuts, among others. 34
In 2003, the Ministry of Health published the Technical Bases for the Supplementation of Vitamins and Minerals in Childhood and Adolescence providing guidelines for the treatment of anemia with 2 mL/d of an oral solution (1.0 g of elemental zinc/100 mL) for 6 months, indiscriminately for children aged 4 to 23 months and 1 to 9 years if clinically diagnosed with anemia. 33
United Nations International Children’s Emergency Fund and the World Health Organization (WHO) published a recommendation for the treatment of diarrheal infection in which they suggested to provide 10 mg of zinc in children younger than 6 months, and 20 mg in children between 6 months and 5 years for 10 to 14 days, in addition to the administration of oral rehydration solution until diarrheal cessation. 35
These WHO guidelines are reflected in other official Mexican publications such as the Official Mexican Standard PROY-NOM-031-SSA2-2014 Project: For child healthcare, which recommends zinc supplementation during diarrheal infections and up to 10 to 14 days after the episode, with 10 mg in children younger than 6 months and 20 mg in children older than 6 months. In this particular document, they recommend zinc supplementation regardless of the type of salt: sulfate, acetate, or gluconate. 36
Also, in the Guidelines for vaccination and frequent diseases in disasters and displaced populations 37 of the National Center for Health of Children and Adolescents (CeNSIA, by its Spanish acronym) of the Ministry of Health, we found a recommendation for zinc supplementation for 10 to 14 days with 10 mg/d in children younger than 6 months and with 20 mg/d in older than 6 months in cases of acute diarrheal diseases without dehydration and in acute respiratory infections, without specifying the dose. Additionally, the WHO dosage recommendations are also included in the Manual for Acute Diarrheal Diseases, Prevention, Control and Treatment of the Ministry of Health 38 indicating that currently in Mexico “zinc supplement availability is in process, and will soon be included in the recommendations for the management of diarrhea.”
However, the Official Mexican Standard NOM-031-SSA2-1999-For child healthcare does not establish guidelines for zinc supplementation in the prevention and control of acute diarrheal or respiratory infections. It also does not establish any recommendation of zinc supplementation for the prevention and control of acute diarrheal and respiratory infections. 39
Finally, the Guidelines for Prevention, Diagnosis and Treatment of Acute Diarrhea in Children aged 2 months to 5 years in the first and second level of care 40 address WHO guidelines stating there is not enough evidence to justify the use of zinc in well-nourished children with gastroenteritis. We now know this statement to be inaccurate, as children with normal weight who receive supplementation with zinc have been seen to have reductions in diarrhea duration by half a day when compared to controls. 9
The Program for Specific Actions 2007-2012: Prevention of infant mortality did not include zinc supplementation as part of its objectives. 41 While the program Mexico without Hunger 2014-2018 42 mentioned it as part of its objectives (1) to reduce acute and chronic child malnutrition, and improve the weight and height indicators of childhood, and (2) to supplement the pediatric population, pregnant and lactating women, as well as older adults with micronutrients (zinc, vitamin A, and iron) to prevent malnutrition.
Additionally, the program “Healthcare sector program” and the National Development Plan 2013-2018 established strategies to reduce child morbidity and mortality for those younger than 5 years, especially in marginalized communities, though different lines of action, such as assisting in the provision of food and food supplements to ensure adequate nutrition. Furthermore, it employed as a main strategy the promotion, prevention, and action on overlooked disease. One of the lines of action included the development of public health programs focused on improving weight and height and treating acute malnutrition in childhood. 43
Despite the technical complications for zinc fortification (eg, altered palatability), 44 there is great availability of these products in the Mexican market; for example, multiple products made with corn are among the most common products fortified with zinc. Unfortunately, a great proportion of zinc-supplemented products, such as beverages and cereals, have a high sugar content.
In 2013, the Federal Attorney’s Office of Consumer (PROFECO, by its Spanish acronym), published a study that analyzed the nutritional content of several fortified foods with micronutrients, such as zinc. In this analysis, they found that all the cereal bars were fortified with zinc and that 5 of the cookies evaluated also included zinc; it was also found that some milk drinks stand out for their high zinc content. A particular brand of baby cereals, among the products for children up to 3 years old analyzed by PROFECO, had a significant zinc content. 45
In relation to zinc supplements, we observed that in Mexico, the only available presentation is tablets of 20 mg, 30 mg, and 50 mg of zinc, intended for adult population consumption. The availability of these supplements is greater online than in pharmacies and supermarkets, this restricts its accessibility.
Interviews: Barriers Regarding Zinc Supplementation and Fortification in Mexico
We conducted 8 interviews with experts from 8 participating companies and institutions on the operation of social assistance programs and the supplements and fortified foods market in Mexico. Among these participating entities were (1) 2 large-scale fortified food producers, (2) one large scale supplement producer, (3) PROSPERA, (4) PASL, (5) 2 interviews to past and current CeNSIA personnel, and (6) a researcher from the National Institute of Public Health of Mexico (INSP).
These interviews allowed us to identify common barriers that hinder access to zinc-fortified products and supplements: Problems with the distribution of PROSPERA fortified foods which are poorly adhered to since families share the fortified foods during meals: “There is distribution of the porridge inside the families…and sometimes the Ministry of Health does not distribute them adequately, it takes them long time to get here and when the delivery arrives, they hand out all the packages, so, the people are not going to use it one by one, instead they use it to make corn gruel, to do whatever, to distribute it among the family.” (INSP researcher) Lack of specific dietary recommendations about the intake and absorption of zinc in nutritional assistance programs such as PROSPERA. Despite the distribution of zinc-fortified foods through these programs, the diet in rural areas and the southern region of the country is still low in zinc,
17,46,47
and has a high phytic acid consumption, which inhibits the absorption of zinc.
46
For example, in a previous study conducted in Mexican children, the bioavailability of zinc was 22%.
48
The lack of a zinc supplement presentation (according to the WHO recommendations for the treatment of diarrhea)
35
included in the Basic Chart and Drug Catalog (BCDC, drug catalog used by public institutions in Mexico) was unanimously identified as one of the problems to treat zinc deficiency in children. Among the reasons contributing to this problem we found: 3.1 Zinc supplementation may not be an attractive or profitable business to the pharmaceutical industry; however, interviewees reported the existence of several isolated attempts to include this supplement in the BCDC: “…I think it is not…a business that has being interesting to a company…I think that if it was regulated, then somebody would be forced to do it.” (Food producer) 3.2 The use of nonregistered or nonpatented zinc supplements in hospitals due to the lack of a regulated supply in the BCDC: “When I worked in (the hospital) “La Raza,” we used zinc supplements supplied by the pharmacy in little sachets … The pharmacy bought it in bulk, well, buys it, because I think they still do.” … I thought it was a bad idea to continue using a product that is not regulated, has no patent or registration number.” (Pediatric Gastroenterologist and Consultant of the American Society of Gastroenterology, Hepatology and Pediatric Nutrition) 3.3 The interviewees identified administrative or political issues as impediments to the inclusion of the zinc supplement to the BCDC: “(the problem of the) supplementation in diarrhea is nothing more than political will. If this has been tried, for example by CeNSIA, it has not progressed because there has not been enough political will for it to be included (in the BCDC).” (INSP researcher). 3.4 The current existence of multivitamin supplement presentation (code 2709) containing zinc in the BCDC. 3.5 And the lack of certain professional profiles in the Health General Council, such as those responsible for childhood health: “…unfortunately, in the past, CeNSIA had a representative on the council…now, when they have presented the zinc proposal, most say: ‘but there are micronutrients (in the BCDC),’ and there is no one there who can explain to them that do we need them….”
Discussion
Our review suggests that, in Mexico, zinc supplementation has been associated with reduced risk of diarrhea in preschool children. Additionally, different nutritional assistance programs to reduce zinc deficiency, like PROSPERA, LICONSA, fortified wheat and corn flours project, and “zinc saves kids,” have reported improvements in the prevalence of anemia, linear growth, and zinc concentrations in the population of children younger than 5 years. According to the national standards and regulation of zinc supplementation and fortification in Mexico, we found that multiple official Mexican standards about fortification and enrichment of foods, fortification of corn and wheat flours, daily intakes and labeling of products with zinc content have been published in order to establish guidelines for child health care. Finally, the interviews with experts suggest that problems with the distribution of supplements, lack of specific dietary recommendations about the intake and absorption of zinc in nutritional assistance programs, and lack of a zinc supplement presentation are the main barriers that obstruct access to zinc-fortified products and supplements.
In general, global scientific evidence shows that zinc supplementation promotes higher linear growth rate in very low birth weight infants, 6 a reduction in the duration and incidence of diarrhea, 10 reduced risk of preterm delivery, 8 and a reduction in general mortality, including the association with diarrhea and lower respiratory tract infections. 10 In addition, zinc fortification has been documented to have significant effect on serum zinc concentration. With respect to linear growth, the subgroup analysis showed significant improvement in height velocity among newborns with very low birth weight. 6 For these reasons, the administration of supplements and food fortification with zinc in children should be integrated into public health strategies that aim to reduce morbidity and mortality in children. 5
The WHO recommends the indistinct use of zinc gluconate, sulfate, or acetate for the supplement manufacture 35 ; however, new evidence indicates that zinc citrate is also a viable option to be considered when designing zinc supplements, due to its comparable absorption with sulfate and its good palatability. 49 In addition, it is important to consider certain packaging and distribution characteristics of these supplements to improve their acceptance in the population 50 : (1) flavor to mask the taste and improve palatability, (2) more attractive packaging, (3) packaging that serves as a container to measure the dose, (4) the inclusion of instructions with images, and (5) copackaging of the zinc supplement and oral rehydration salts.
Despite that fact that, in Mexico, zinc deficiency is still prevalent among children, that scientific evidence demonstrates the positive effects of zinc reducing morbidity and mortality in this age-group, and that zinc supplementation is included in some national standards as part of the treatment of acute diarrheal disease, 36 -38 to date its use in our country is not sufficient and hindered by the lack of adequate presentation for its administration in pediatric population.
Finally, it is necessary to generate a comprehensive strategy to achieve the inclusion of zinc supplement in the BCDC, through the inclusion of CeNSIA personnel and other centers in the decision-making of the Health General Council; to regulate the use of nonpatented zinc supplements in hospitals and specialty pharmacies, and generate scientific evidence that reduces the disparities between the administration of the multivitamins included in the BCDC with the interventions recommended by the WHO for acute diarrhea.
35
In addition, we believe that other actions may be carried out to increase zinc blood levels in children younger than 5 years: Guarantee that all children younger than 5 years have access to zinc-fortified foods, by improving the distribution processes of fortified foods from programs such as PROSPERA, independent of their affiliation to a social program. For this purpose, it is important that the corresponding regulations contemplate the universal coverage of zinc-fortified foods for children. Additionally, is important that this issue is considered a priority in the public health agenda by the decision-makers. Evaluate strategies aimed to reduce the prevalence of zinc deficiency in the infant population and in marginalized areas. Through innovation, manufactured fortified foods with zinc and other minerals with good palatability and nutritionally adequate (eg, low in added sugars) to promote better acceptability and reduce the consumption of foods with added sugars, which are currently abundant in the market. Consider the inclusion of biofortification programs in order to increase the amount of zinc in vegetables or reduce the phytic acid content. This strategy not only is potentially more cost-effective but would also increase the intake of zinc in the rest of the population. Raise awareness within the medical community and among primary care doctors regarding the importance of adequate zinc intake during childhood and especially in cases of malnutrition and acute diarrheal diseases. Promote food preparation strategies to increase the bioavailability of zinc in the infant population, including the PROSPERA beneficiaries. Consolidate the Official Mexican Standard PROY-NOM-031-SSA2-2014 Project: For child healthcare, which recommends supplementing with zinc in case of diarrheal infections during the episodes and for 10 to 14 days more, with 10 mg for children younger than 6 months and 20 mg for children 6 months and older.
36
Conclusion
Despite the efforts of national programs and regulations, zinc deficiency continues to be a public health problem. Currently, in Mexico, there are no supplement presentations targeted toward children to encourage compliance with international and national recommendations for the management of infectious diseases. Finally, comprehensive actions by decision makers are required, supported by scientific evidence to evaluate different alternatives to reduce zinc deficiency in preschool children.
Footnotes
Authors' Note
Yanelli Rodríguez-Carmona is currently affiliated with the Department of Nutritional Sciences, University of Michigan School of Public Health, Ann Arbor, USA
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.