
Abstract
Background:
India has made important strides in reducing nutritional deficiencies over the past several decades. However, for micronutrients such as zinc, previous studies have suggested a worsening situation, contrary to most other dietary indicators. Adding to this burden, higher carbon dioxide (CO2) levels of 550 ppm, projected to potentially occur within decades, could reduce the zinc content of many staple crops.
Objective:
To assess the historical prevalence of inadequate zinc intake, as well as to estimate the future prevalence attributable to rising CO2.
Methods:
Seven household food consumption surveys between 1983 and 2012 were used to calculate total dietary zinc, phytate, and absorbable zinc intakes and to assess the prevalence of historic inadequacy in zinc intake. The added nutritional effect of elevated CO2 on zinc intake is then modeled.
Results:
Prevalence of inadequate absorbable zinc intake has increased from 17.1% (15.3%-19.0%) in 1983 to 24.6% (22.3%-27.1%) in 2011-12, corresponding to an additional 82 million people consuming inadequate zinc than would have otherwise if 1983 rates had persisted. These increases in inadequacy have been driven by a relatively constant zinc intake being increasingly insufficient to meet a 5% growth in zinc requirements due to the aging of the population. Reaching 550 ppm CO2 by 2050 could potentially increase the prevalence of inadequate zinc intake by another 3.9 percentage points (2.1-5.8), corresponding to 65 million additional people having inadequate zinc intake.
Conclusions:
The persistently worsening trend for zinc—opposite most other measures of human nutrition—shows that it may pose an ongoing risk unless addressed.
Introduction
For much of the past century, nutritional health in India has lagged relative to the rest of the world, especially important given its large proportion of the global population. In 1985, nearly 40% of children younger than 5 years were estimated to be severely stunted, the fourth highest prevalence of any country globally. 1 Likewise, Indian children in 1985 endured the second-worst prevalence of wasting, with over 25% severely wasted. 1 Other nutritional burdens included 62% of children younger than 5 years were vitamin A deficient in 2001 to 2013 (12th worst globally), 2 74% of children younger than 5 years were considered anemic in 1998 to 1999 (19th worst), 3 and 52% of reproductive-aged women were anemic (24th worst). 3
Consistent with global trends, there have been significant improvements in recent years. Under-5 severe stunting has fallen to 17% in 2011, 1 severe wasting is now 7.4%, 4 and vitamin A deficiency has dropped to 45% in 2016 coinciding with a near-doubling of coverage for supplementation. 4 Anemia rates have also declined steadily for children (59% in 2016), though have held steady for reproductive-aged women (53%). 4 However, though household incomes have continued to rise and propel some progress in nutrition-related health outcomes, undernutrition is still relatively high in India compared to similar developing countries.
Zinc intake has stood in contrast to these other, mostly positive trends. Previous work looking into inadequate dietary zinc intakes globally using the UN Food and Agriculture Organization’s (FAO) food balance sheets estimated that India had a 28% prevalence of dietary inadequacy in 1990, which increased to 31% by 2005, contrasted with a globally averaged decrease from 20.7% to 19.6% over the same time. 5 Though zinc deficiency is only responsible for 0.2% of the disability-adjusted life-years lost in India last year (attributable to its role in increasing the severity of diarrheal disease, lower respiratory infection, and malaria 6 ), the upward trend remains worrisome.
In addition to dietary shifts away from micronutrient-rich coarse cereals in the Indian diet, anthropogenic CO2 emissions are likely to exacerbate these trends in the future. A global CO2 concentration of 550 ppm—which is predicted to occur around 2050 on our current trajectory—has been shown to reduce the content of zinc, iron, and protein in a range of food crops. 7 Though the mechanism of how higher CO2 leads to lower crop nutrition is not clear, it has been shown empirically to lower the nutrition density in many grains (wheat, rice, barley, maize) and legumes by 3% to 17%. Specifically, for zinc, these food crops could see losses of 5% to 11% of their overall zinc content under higher CO2 relative to current conditions, particularly in cereals. A global analysis of this effect that focused on zinc indicated that India could be particularly hard-hit, with an additional 4.2% of its population placed at risk of inadequate zinc intake compared to baseline, given its high reliance on grain crops for dietary zinc. 8
The purpose of our study is to investigate both past and future trends in dietary intake of absorbable zinc to elucidate the magnitude, scope, and cause of these trends. We use nationally representative household-level data to study in detail how the prevalence of inadequate dietary zinc intake has changed over the past 30 years by state, rural and urban, and by income. We then forecast future changes to the nutrient density of foods to examine the potential impact of elevated CO2 levels on absorbable zinc intake and prevalence of dietary inadequacy. Finally, we model intervention scenarios to explore ways to mitigate current and future harm.
Methods
Total per capita food consumption at the household level was extracted from the following 7 rounds of the National Sample Survey of Consumption Expenditure: 1983 (round 38), 1987 to 1988 (round 43), 1993 to 1994 (round 50), 1999 to 2000 (round 55), 2004 to 2005 (round 61), 2009 to 2010 (round 66), and 2011 to 2012 (round 68). 9 These surveys represent only the rounds where dietary information was collected. Intake data were paired with Indian food composition tables 10 (summarized in Table S1) to estimate per capita dietary zinc and phytate intake and then converted to absorbable (or bioavailable) zinc using the Miller equation. 11,12 Some recent studies have shown that absorption may be less or more than prescribed by the Miller equation in some specific groups: children aged 1 to 4, pregnant women, and lactating women. 13 -15 However, we are unable to account for these differences in absorption as we do not have any specific data on zinc or phytate intake by age or sex group. Regardless, we believe the effect of our assumption of the Miller equation across all demographic groups to have a relatively minor effect on our results, as discussed further in Supplemental Methods.
Aggregated data on zinc and phytate intake at the state and rural/urban levels, as well as by income quartile, were also compiled with household weights provided from the National Sample Survey. The intraindividual distributions of intakes around the mean were estimated using the technique described in Supplemental Methods.
To determine the prevalence of inadequate dietary zinc, absorbable zinc intakes were compared with population-weighted estimated average requirements (EARs), calculated for each level of aggregation (state, income, and rural/urban) using age- /sex-specific requirements 16 and the demographic distributions in each survey year using decadal census data, 17 -20 linearly interpolated to coincide with dietary survey years . The prevalence of inadequate intakes was estimated using the EAR cut-point method. 21,22
Here, we use the term “prevalence of inadequate zinc intake,” which is intended to describe the proportion of the population that is eating too little zinc to meet their estimated bodily needs. This is distinct from the term “zinc deficiency,” which is a clinical measure of one’s serum zinc being below a medically designated threshold. Though inadequate dietary zinc is the main cause of zinc deficiency, there are other mediating factors—inadequate absorption, high loss rate in the body, and increased utilization by body systems—that may intervene between the two, making them not directly interchangeable.
The effect of elevated CO2 (550 ppm) on the zinc content of each crop was taken from a recent meta-analysis by Myers et al 7 and applied using a similar method as previous studies. 8 For each individual crop that shows a response to elevated CO2, as well as for broader food categories (eg, C3 legumes), percentage losses of zinc are shown in Table S2. Zinc and phytate losses of crops under 550 ppm were multiplied by the amount supplied by each food group to estimate both future zinc intake and the future prevalence of inadequate zinc. Population size and requirements in 2050 were estimated based on population projections. 23,24 Due to high uncertainty in projecting future diets, we assume that diets remain constant, not as a prediction, but merely as a simple and transparent assumption. Additional justification for this assumption may be found in Supplemental Methods, and implications are explored in “Discussion” section.
We also model two scenarios to help improve absorbable zinc under current and future diets; both were previously proposed in a study published last year in this journal aimed at improving iron in Indian diets. 25 The first, scenario 1, maintains the current amount of grain consumption, but returns to the 1983 mix of grains, which is higher in coarse cereals (millet and sorghum) and lower in wheat. The second, scenario 2, restores both the 1983 mix of grains and the higher amount of grains consumed in 1983 while holding the rest of the diet constant.
A full description of the methodology and data sets may be found in Supplemental Methods.
Results
The prevalence of inadequate zinc intake has risen from 17.1% (95% confidence interval: 15.3%-19.0%) to 24.6% in 2011/12 (22.3%-27.1%), reaching a maximum of 26.3% (23.9%-28.6%) in 2009/10 (Figure 1). The increase in inadequate zinc intake over the span of nearly 3 decades amounts to a growth of 7.5 percentage points (4.4%-10.8%), corresponding to an additional 82 million people (47-119 million) consuming inadequate zinc compared to if 1983 rates had persisted to 2011-12. This rise in inadequacy is primarily not attributable to a decrease in the per capita consumption of absorbable zinc. More precisely, total dietary zinc and phytate have both fallen over time, though phytate has fallen more rapidly, reducing the molar phytate-to-zinc ratio and improving the absorbability of zinc due to the reduction of the inhibitory action of phytate in the gut. The confluence of these factors has served to keep the per capita absorbable zinc remarkably constant, only varying within ±2% over the past 3 decades (Figure 2).
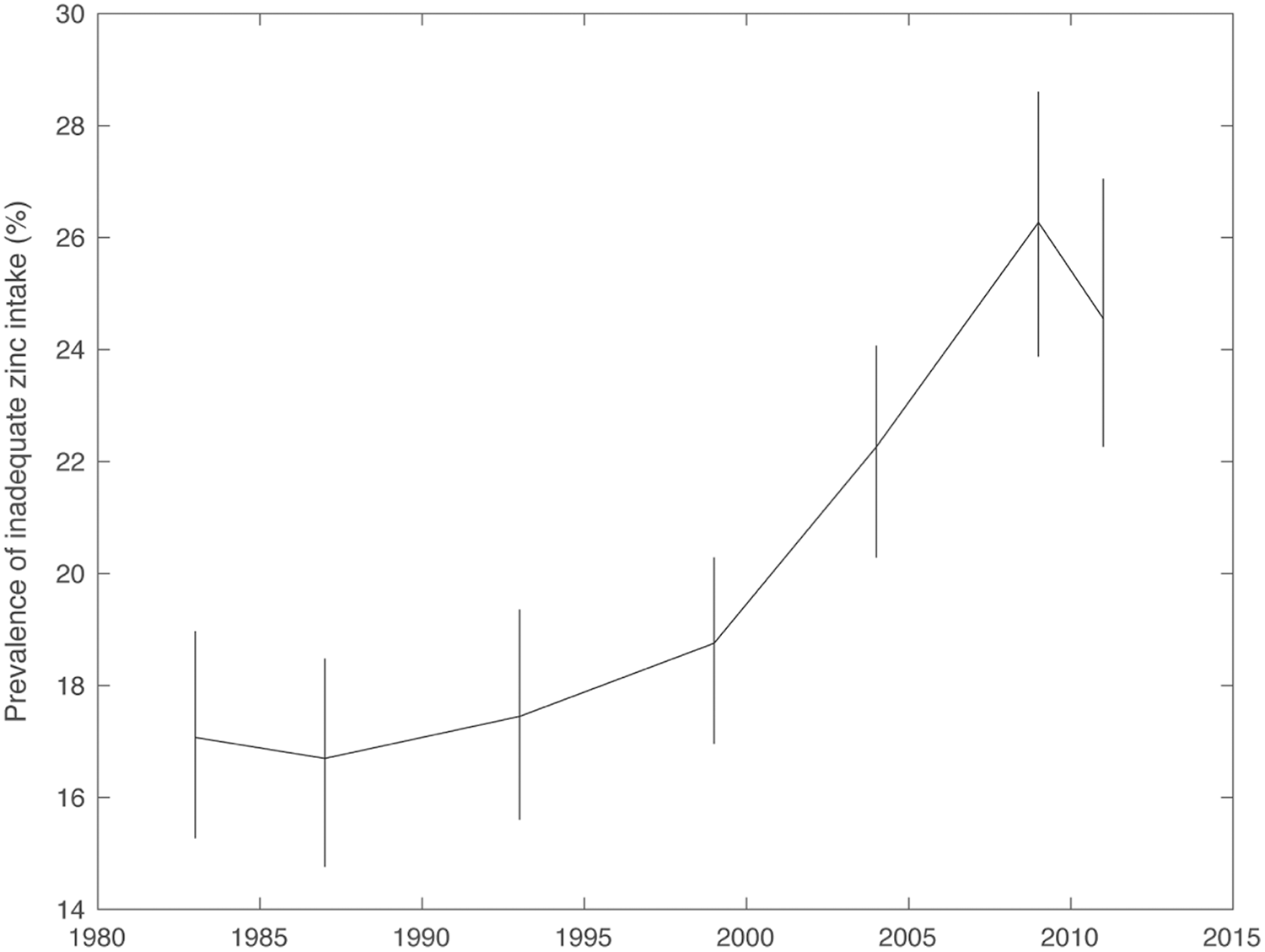
Prevalence of inadequate zinc intakes from 1983 to 2011-12 for all India.
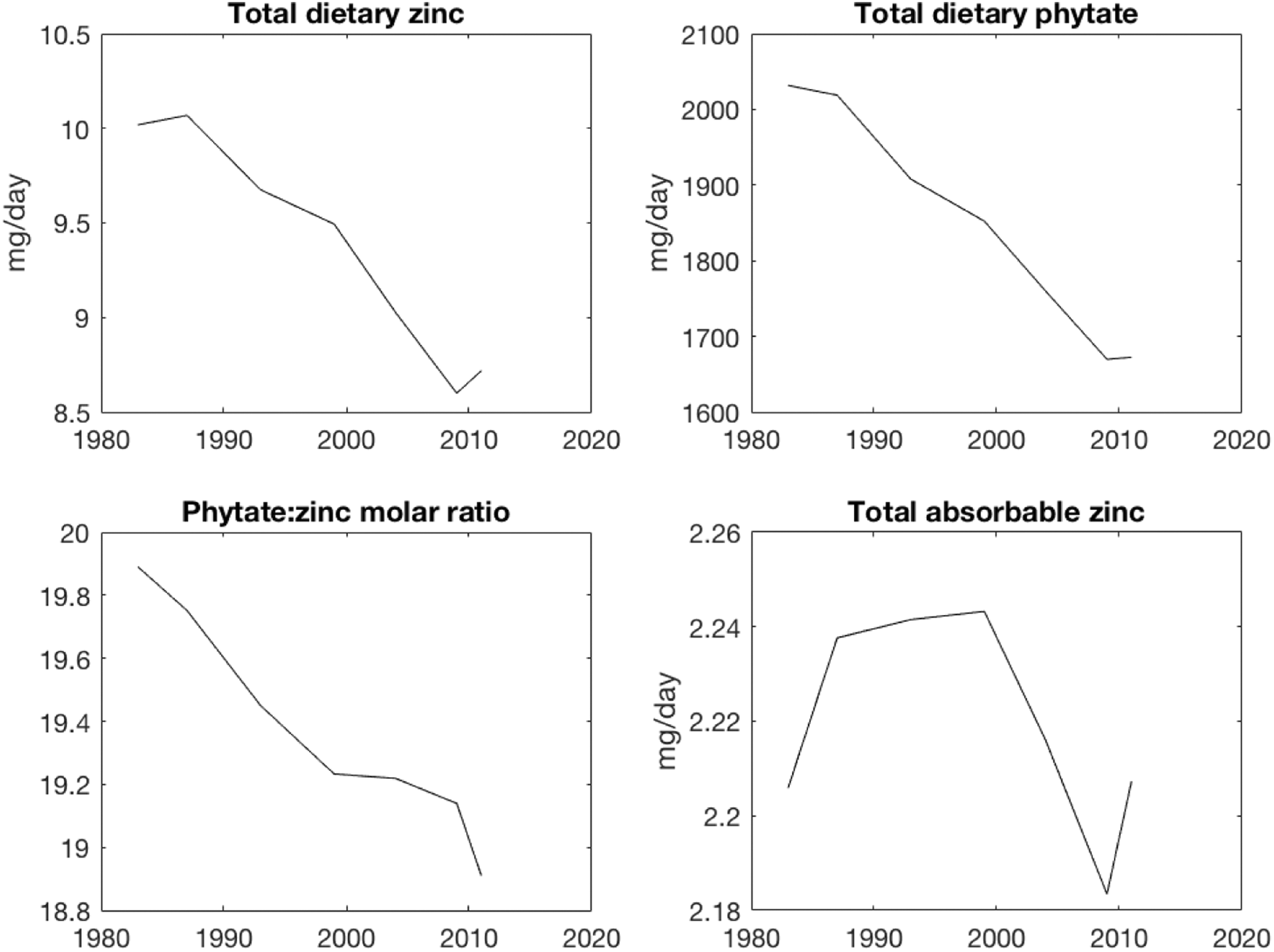
Trends in Indian zinc, phytate, phytate-to-zinc molar ratio, and total absorbable zinc for all India.
Instead, the steady absorbable zinc intake has proven increasingly inadequate to meet the growing needs of a slowly aging Indian population. Figure 3A shows the contribution of individual foods to total absorbable zinc compared to the population-weighted national EAR, which has increased 5% over the measured period. Figure 3 also showcases the dietary shifts that have taken place in the intervening decades, with dietary zinc moving away from coarse cereals (such as millets and sorghum) toward wheat, and a growing contribution from noncereal sources such as animal-source foods and C3 plants (mainly fruits, vegetables, and vegetal oils). Panels B and C of Figure 3 also show how the contributions of cereals to both total zinc and phytate have decreased over time, which has buffered the effect of the overall zinc decline on absorbable zinc.
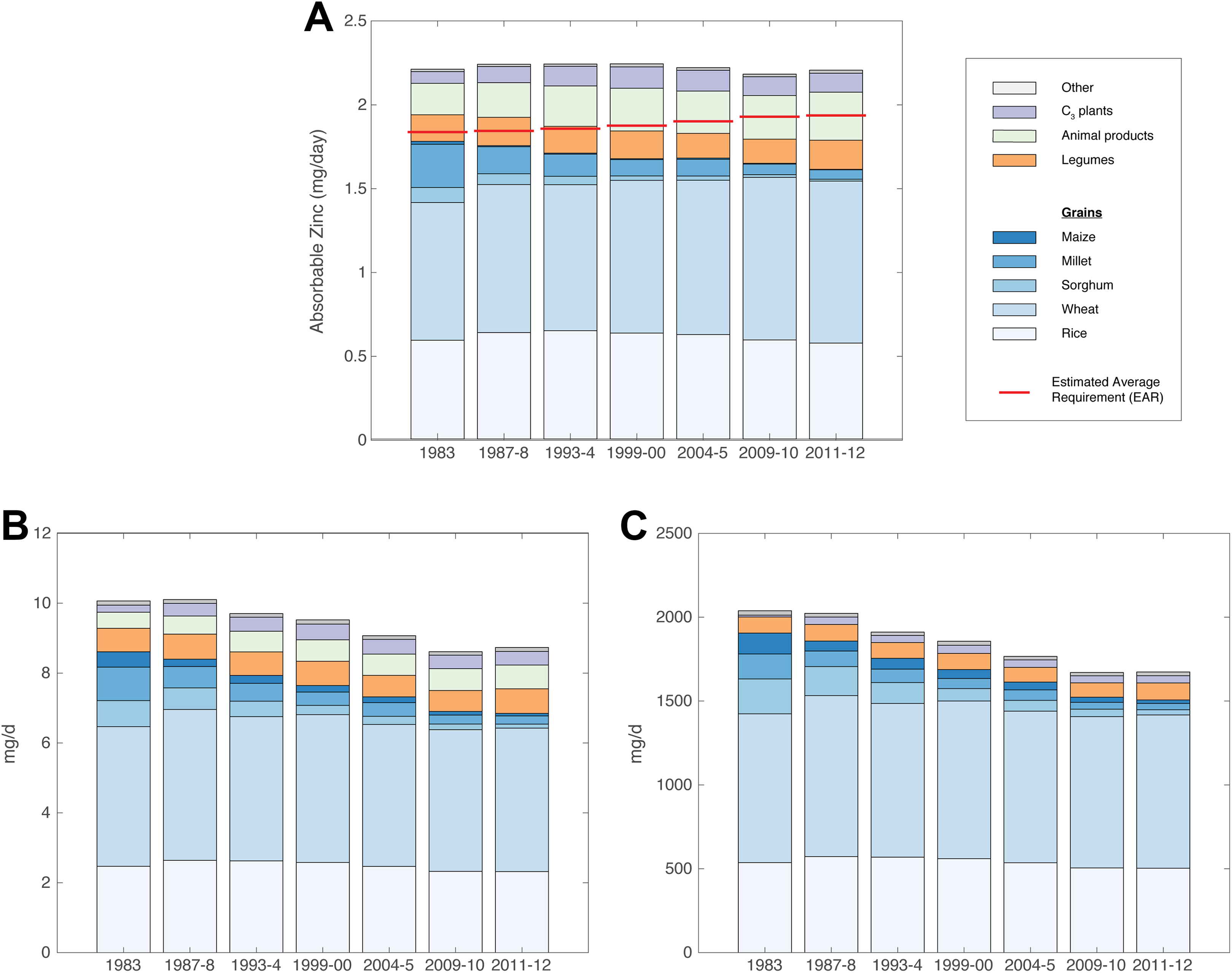
Contributions of individual foods to dietary zinc. (A) Total absorbable zinc in the diet compared with nationally averaged requirements; also for (B) total dietary zinc and (C) phytate. Methodology for calculating individual per-food contributions to absorbable zinc is described in Supplemental Methods.
Rural and urban rates of inadequate zinc intake have increased by roughly the same amount (6.0% and 5.5%) over the past several decades (Figure 4), corresponding to an average of 59 and 21 million people, respectively. However, urban populations have a much higher average rate of inadequate zinc intake overall (40% in 2011-2012), compared with rural populations (18%). This discrepancy is driven by two factors. First, there is a difference in diets between the two: Urban populations eat 7% fewer calories overall compared with rural populations, driven by a much lower consumption of grains, though a greater consumption of C3 plants, oils, and some animal-source foods. Second, urban populations are older and more male than rural populations, requiring 4% to 5% more zinc. The median age in 2011 for urban areas was 26 compared to 23 in rural areas, and males were 7.6% more prevalent than females in 2011 within urban areas compared with 5.4% for rural areas. The combination of these two factors, combined with the growth of the urban population, from 24% of total population in 1983 to 31% in 2011 to 2012, has also contributed to a greater share of the country consuming inadequate zinc.
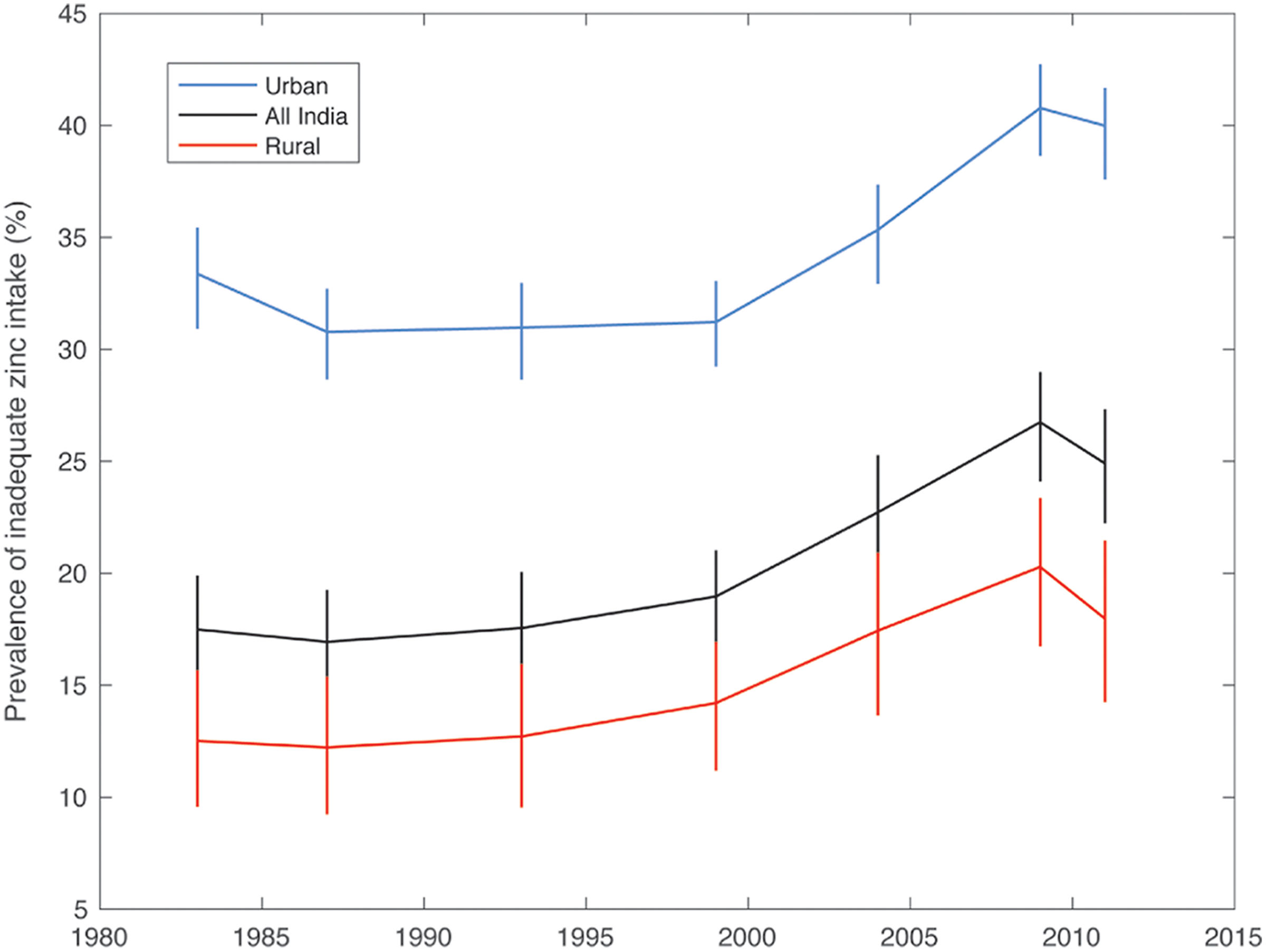
Prevalence of inadequate zinc intake for all India divided into rural, urban, and total population. The rural population comprises 76% of the total population in 1983 and 69% in 2011-12.
Regional-level results reveal a diversity of susceptibilities to inadequate zinc intake based on local eating patterns (Figures 5 and 6). Full state-level results are shown in Table 1 and Figures S2-S3. Rice-eating states in the south and northeast have a much higher prevalence of inadequate zinc intake (38%) than the predominantly wheat-eating states of north, east, central, and western India (17%). Furthermore, states that have seen the most dramatic rise in inadequacy rates were also once major consumers of millet and sorghum, predominantly in the south and west. Of the 8 states that derived greater than 10% of their absorbable zinc from millet and sorghum in 1983, all except one also had a 10% or greater increase in the prevalence of inadequate zinc intake by 2011 to 2012. The lone exception, Rajasthan, had the highest zinc intake of any state, buffering against these losses.
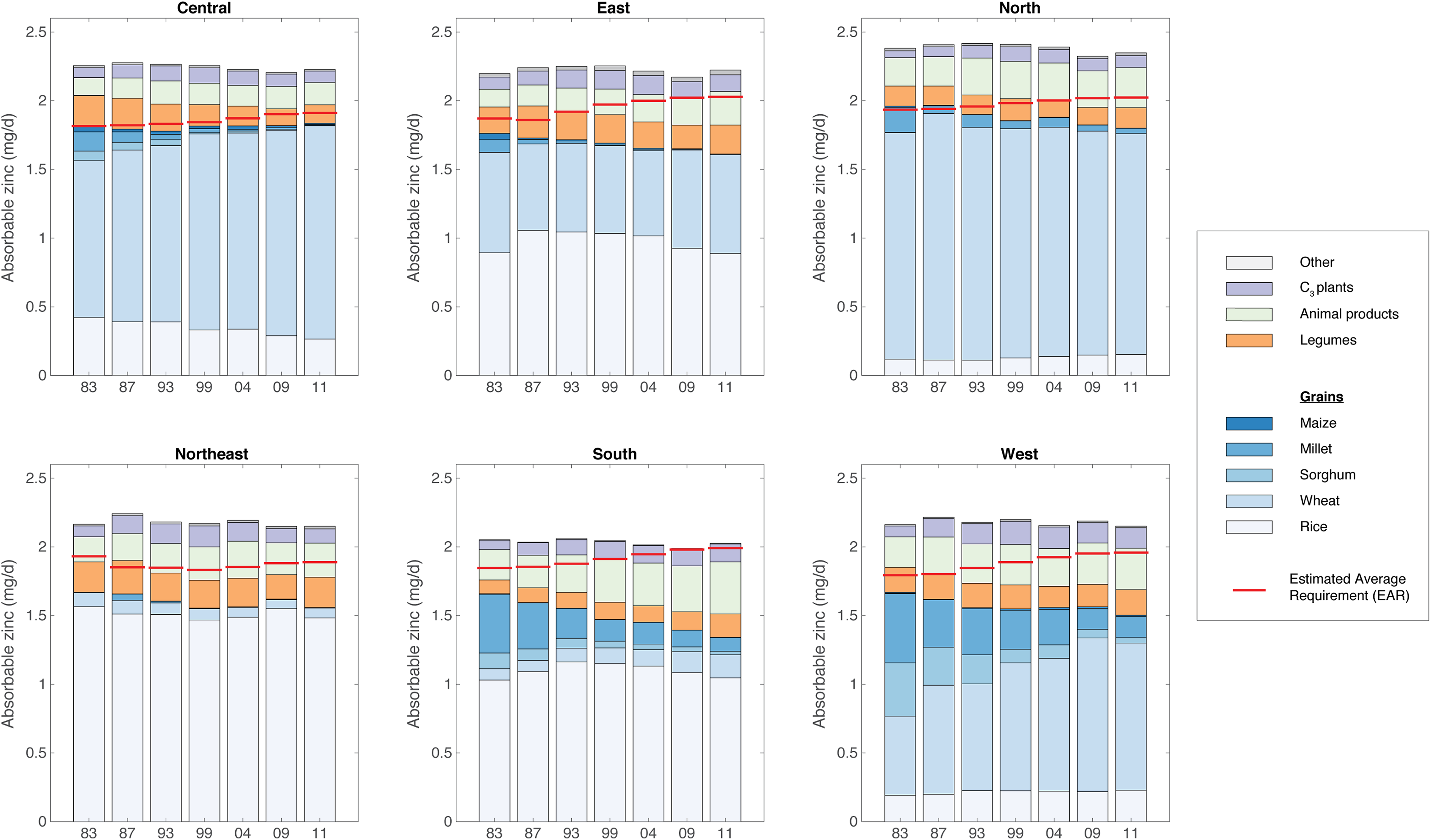
Per-food contribution to total absorbable zinc by region. States and territories comprising each region are described in Table 1.
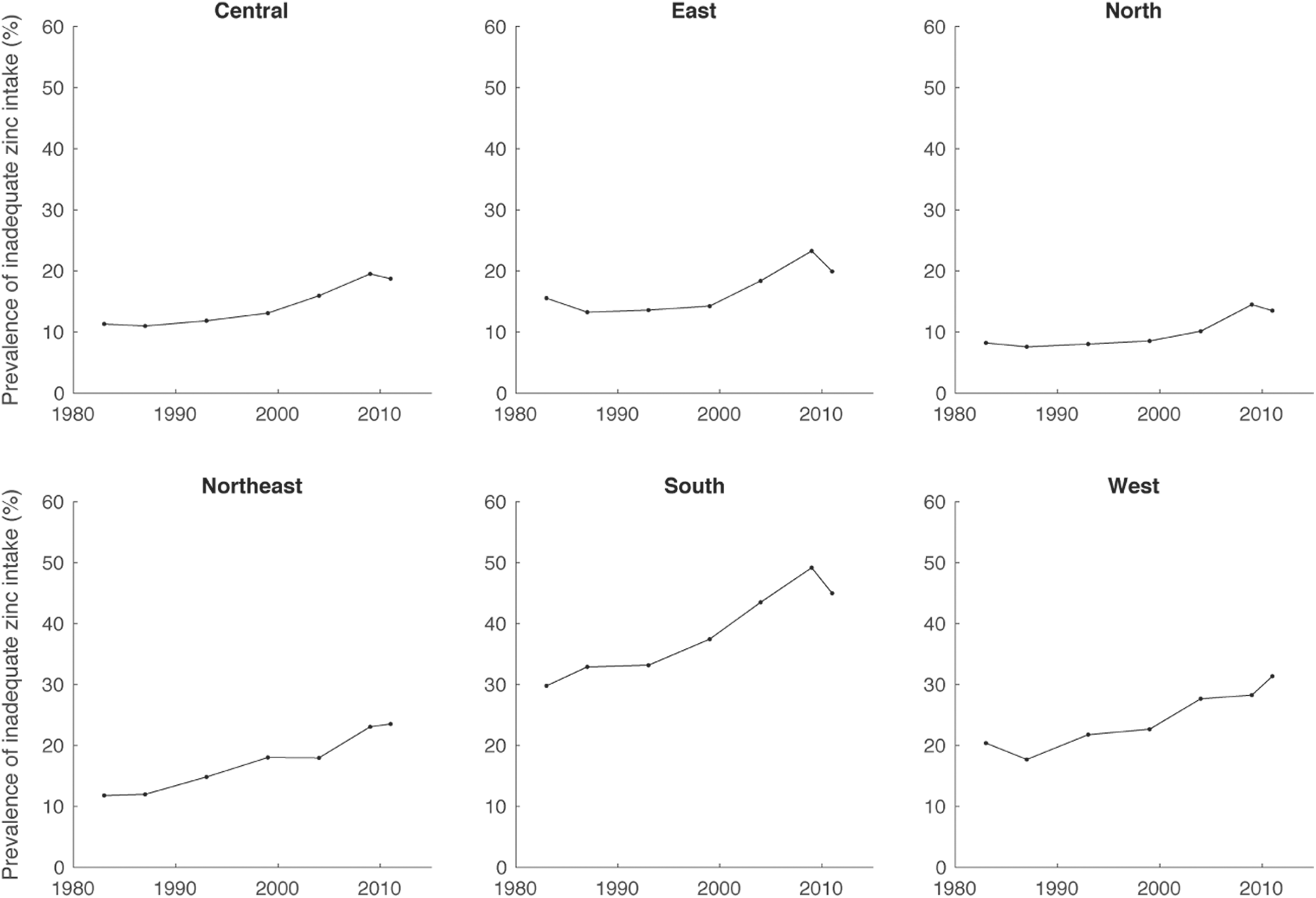
Prevalence of inadequate zinc intake by region. States and territories comprising each region are described in Table 1.
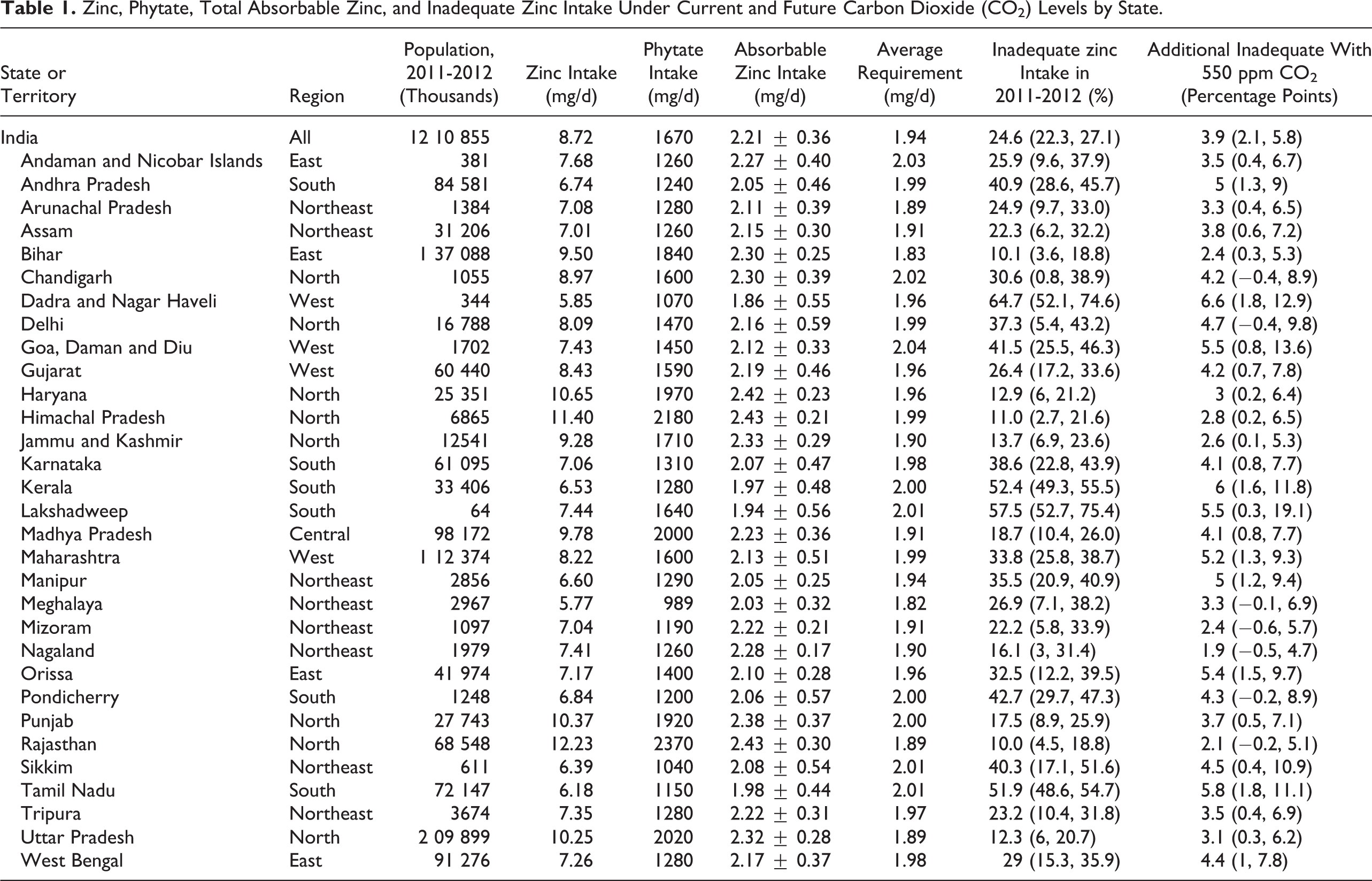
Zinc, Phytate, Total Absorbable Zinc, and Inadequate Zinc Intake Under Current and Future Carbon Dioxide (CO2) Levels by State.
Trends in inadequate zinc intake by income quartile present a more complicated picture (Figure 7). Among rural populations, income appears to have little to no impact on zinc inadequacy. Poor rural households are equally likely to be consuming inadequate zinc as the wealthiest ones for most of the study period; only in the last 2 rounds does the highest quartile show slightly greater inadequacy relative to others. Among urban populations, the highest income quartile has the highest prevalence of inadequate zinc intake and has also seen the largest increase over the study period. The third quartile is the next-most inadequate and the bottom 2 quartiles are statistically indistinguishable for most of the study period. These trends are related to the intersection of zinc intake and requirement (Figure 8). For rural populations, zinc intake is observed to mostly increase with income. However, their requirements also increase with income because wealthier households are often smaller, have fewer children, and have a greater male-to-female ratio. Therefore, the prevalence of inadequate intake is roughly the same and relatively low (∼5%-15%) for all quartiles. For urban populations, the requirements follow the same correlation with income as with rural households, but intakes do not, with the top 3 quartiles eating nearly the same amount of zinc over much of the study period. This results in higher income households being more susceptible to inadequate intakes overall.
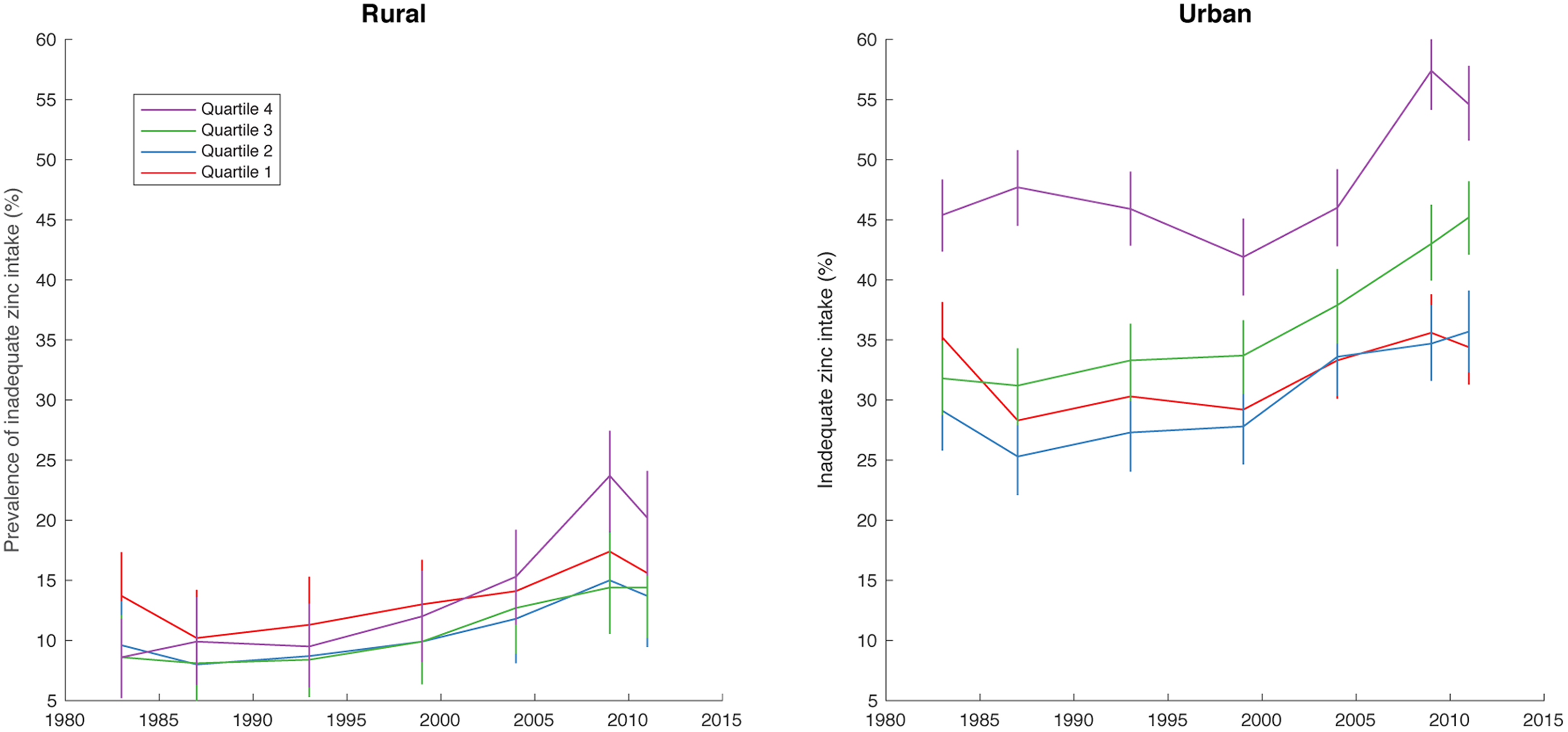
Inadequate zinc intake for all India divided by income quartile and by rural/urban.
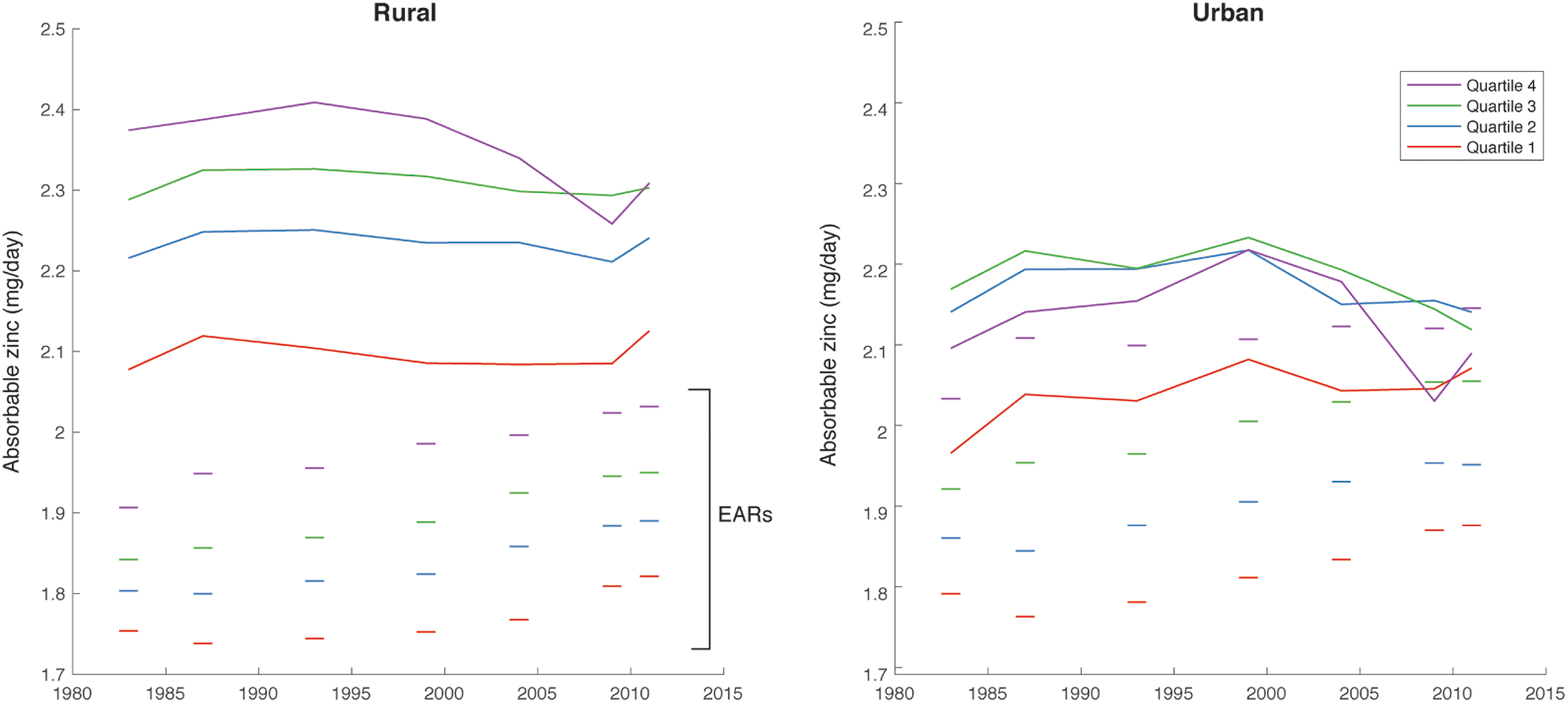
Absorbable zinc and physiological requirements by income quartile and rural/urban.
Elevated CO2 and the Future of Zinc
The effect of elevated CO2 on Indian diets is especially pernicious because it affects the grain crops upon which Indians base their diet most heavily. The effect of raising CO2 to 550 ppm would be to increase the prevalence of inadequate intake by 3.9 percentage points (2.1-5.8) relative to 2011-12 (Table 1), corresponding to 65 million (37-100 million) additional people with inadequate intake. This effect is felt most strongly in states that already experience a high rate of inadequate zinc intakes (Figure S4). Nearly all regions derive a high proportion of their zinc from CO2-susceptible crops, and a similarly sized decrease in zinc intake would affect a more deficient state more heavily than one that has greater sufficiency due to the normally distributed intakes.
Scenarios for Alleviating Inadequate Dietary Zinc Intakes
Implementing scenario 1—same cereal intake, mix of cereals at 1983 levels—to alleviate the risk of inadequate zinc intake today or in the future has a modest effect (Table 2). In the context of 2011 diets, the prevalence of inadequate zinc intake under scenario 1 is expected to be reduced by 0.7 percentage points (−0.1 to 1.4) relative to baseline. Extending this to look at its impact on inadequate zinc intakes in 2050 under elevated CO2, we would expect to see only a reduction by 0.9 percentage points (−0.4 to 2.3) relative to a no-intervention scenario. These modest effects are related to the size of the shift in diets, which constitute roughly a 10% shift in cereals from millet and sorghum to wheat. This leads to a slight improvement (decrease) in the phytate to zinc ratio of the diet, increasing the amount of absorbable zinc.
Implications of Different Intervention Scenarios for Improving Those Consuming an Inadequate Amount of Zinc Now and in the Future.
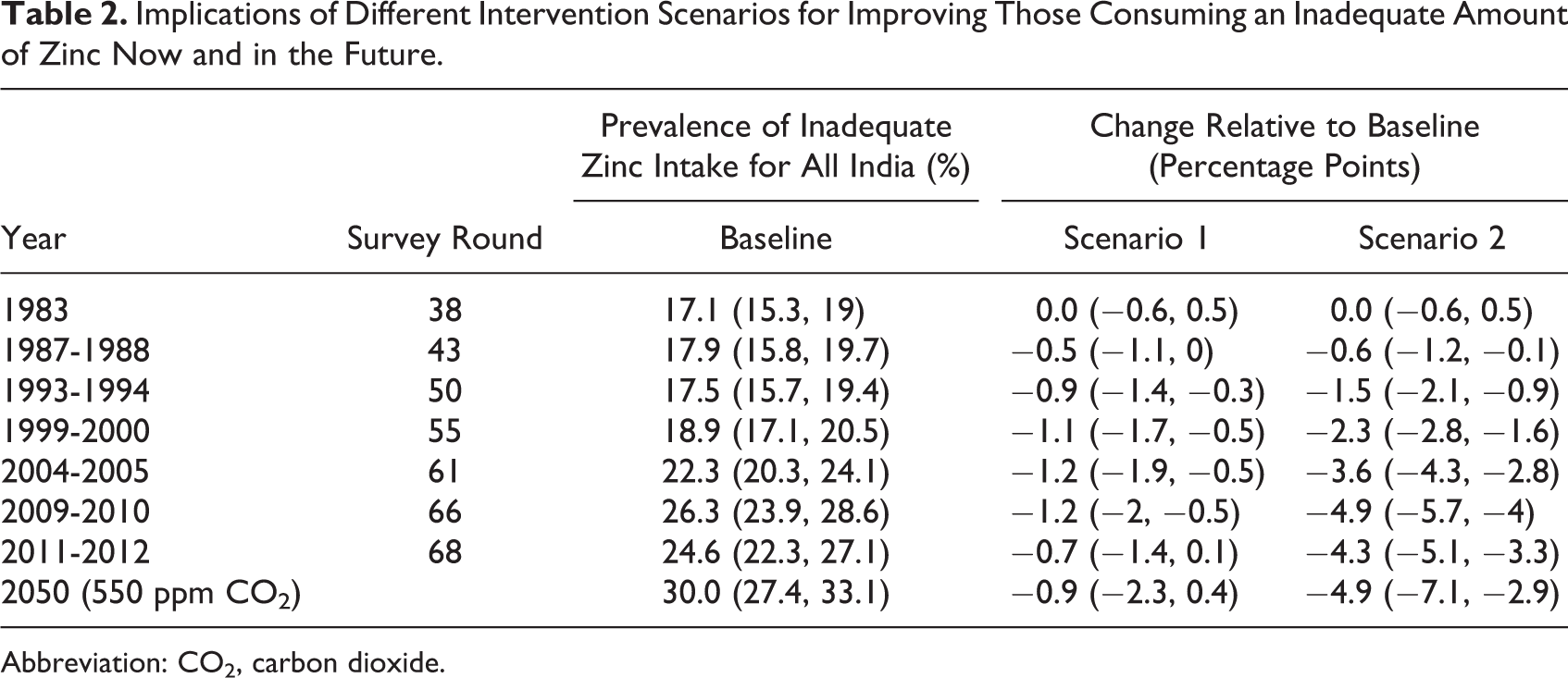
Abbreviation: CO2, carbon dioxide.
Scenario 2—replacing today’s cereal consumption with 1983 levels and proportions—leads to even better outcomes today and in the future. Under 2011 diets, scenario 2 would lead to a reduction of the prevalence of inadequate zinc intake of roughly 4.3 percentage points (3.3-5.1), and 4.9 points (2.9-7.1) under elevated CO2. The shift and growth in cereal consumption under scenario 2 would offset nearly all of the impact of increased CO2 by 2050.
Discussion
The increase in national inadequate zinc intakes appears to be attributable to at least two factors. First, zinc intakes have gone down relative to the average Indian requirements, whose median age has increased from 20 to 24 over the time period of these surveys. 17,20 A higher median age means a greater proportion of adults relative to children, which has resulted in the population as a whole requiring 5% higher zinc now than in 1983 despite nearly steady absorbable zinc intake over that time frame. Second, urbanization has driven more people to consume a zinc-inadequate diet. We find that urban diets have remained poorer in zinc, and the proportion of India’s population living in cities has grown from 24% to 31% over this time. Combined, these trends have conspired to drive inadequate zinc intake higher despite otherwise stable or improving health.
However, this trend toward greater inadequacy has not been felt uniformly around the country. Rice-eating states—those that derive greater than 50% of the cereal calories from rice—in the south and northeast have seen a disproportionate share of the health burden of inadequate zinc intake, primarily due to the poor zinc content of white rice. Rice-eating states have similar overall caloric intake compared with wheat-eating or mixed-grain-eating states and have a similar proportion of calories derived from cereals. However, rice-eating states eat nearly 8% less absorbable zinc on average than other states because white rice has less than half the total zinc compared with wheat. Rice also contains less phytate, but this is not sufficient to significantly offset the lower zinc content to maintain absorbable zinc. The relationship between rice content of the diet and total absorbable zinc is shown in Figure S5.
One of the causes of this rise in inadequacy has been a gradual rise in requirements relative to intake, driven by a lower fertility rate and a raising of the median age. This would mean that those groups who are most susceptible to the worst health burdens of inadequate zinc intake—children and pregnant women—have declined as a proportion of the population while overall inadequacy has risen. Therefore, this demographic trend of fewer children and mothers may have been able to countervail some of the broader nutritional trends and lessen its full health effect.
The relationship between inadequate zinc intake and income, at first glance, appears odd. In rural settings, prevalence of inadequate zinc intake is roughly the same across all income categories, while in urban populations the prevalence of inadequate intake actually increases with income. This somewhat counterintuitive observation can be squared by looking at previous work that has studied the food choices made by high-income groups. High-income Indians, particularly in urban settings, have chosen to use their higher purchasing power on higher cost calories from fats and sugars at the expense of cheaper cereals. 26 This trade is particularly obvious in the observation that rural and urban groups in India eat roughly the same number of calories, but urban population consume nearly one-third more fat. 26 Furthermore, other work has corroborated these findings for urban groups, showing that high-income groups consume nearly double the amount of fat as low-income groups. 27 Oils consumed in India—soybean, mustard, groundnut, coconut, ghee, and margarine 28 —contain little zinc despite their high caloric density, leaving high-income groups quite often eating less zinc compared with those that derive more of their diet from cereals. Sugars are similarly calorie rich and nutrient poor, further widening the gap.
In the face of these challenges, it is useful to ask what can be done. Dietary diversification as a long-term sustainable strategy to address adequate zinc intake may be further explored. For a developing country like India which has predominantly a cereal- and pulse-based vegetarian diet with minimal amounts of flesh foods (a rich source of zinc), cereals appear to be the major source of zinc with its contribution going up to 60% of total dietary zinc, owing to the sheer volume of intake. Nonetheless, other foods that are traditionally part of Indian diets such as milk, legumes, eggs, nuts, and vegetables in a diverse diet can contribute to improved zinc intake. 29 However, within the context of the current grain-dominant diet, we focused on possible intervention scenarios that simply involved adjusting grain intake by investigating 2 that would reintroduce varying amounts of coarse cereals back into the diet. The most logistically plausible, scenario 1, which would keep cereal levels as-is but reintroduce the proportion of cereals back as it was in 1983, has only a modest effect at ameliorating the current trend of inadequate zinc intake and at staving off future CO2-related effects. Scenario 2—reintroducing the 1983 amount and proportion of grains—makes more significant progress on both fronts but is likely to be more difficult to implement. Increasing cereal production and consumption by ∼25% would require significant agricultural improvements and would countervail the current cultural preferences toward fewer cereals in the diet. Furthermore, India is already an outlier in the proportion of cereals in the diet (72% of total calories), and introducing another 4% under scenario 2 has the potential to increase the risk of other nutritionally mediated diseases.
Despite the lack of effectiveness or feasibility of these modeled solutions, several established strategies at improving zinc status have already proven effective. The World Health Organization recommends direct supplementation with zinc to avert severe deficiency, and this strategy has been shown to be highly effective in avoiding adverse health outcomes related to zinc deficiency in children. 30 However, supplementation would not be a feasible long-term sustainable solution, given the cost and complexity of maintaining a steady supply of zinc supplements to a broad Indian population. Alternately, fortification of staple foods with zinc has been demonstrated to improve serum zinc levels and requires less targeted methods to enable population-level coverage. 31 Currently, India engages in voluntary fortification of wheat flour and milled rice at a level of 30 mg/kg, though it is estimated that only 2% of industrially milled wheat and 0.25% of rice are fortified according to these guidelines. 32 Were India to fortify these major grains nationally at a much lower level of 2.1 mg/kg, which is less than any other fortifying country globally, they would be able to reverse the increase in zinc inadequacy incurred since 1983. An additional 1.2 mg/kg would avoid the harmful effects of nutritional inadequacy from rising CO2 in 2050. Other interventions—shifting diets toward high-zinc foods or biofortification of crops—have shown some promise but currently lack research demonstrating feasibility at large scale. 33,34
This study has several limitations that may affect the precision of its findings. First, because we are using household-level data, we are unable to identify true distributions of intakes taking into account the full spread of intrahousehold variability. This is likely to make our estimates of the prevalence of inadequate intake rather conservative because increasing the spread of the intake distribution would have the mathematical effect of more people consuming inadequate zinc. Second, we make a rather large assumption that diets will not change in the future. Because of the tremendous model uncertainty surrounding the impact of future economic and environmental changes on global diets, let alone India’s previously noted unique behavioral response to rising incomes, it would be highly unreliable to try and model the impact of elevated CO2 on the predicted trajectory of future diets. Therefore, we have chosen to take the unlikely but transparent assumption, in line with previous modeling efforts of the kind, that diets remain stable. 8,35 Thirdly, estimates of inadequate zinc intake would ideally be compared to a more direct measure of physiologic deficiency, such as serum zinc, to corroborate our findings. However, no national- or state-representative estimates of the kind exist. We hope that future data will enable this type of comparison to help bolster our modeling efforts and empower policy makers to take action to head off future problems. Finally, as we discuss in more detail in Supplemental Methods, we are only able to capture some sources of uncertainty in our inputs: those related to the intraindividual population distributions of zinc intake, as well as the impact of rising carbon dioxide on the nutrient density of many major foods in the diet. However, although considerable care was taken to standardize and correct for shifts in sampling methodology and district boundaries across survey rounds, the estimated measurement error of each survey is not recorded within the data provided by the Ministry of Statistics and Programme Implementation. Without knowing the full size of the uncertainty, it is unclear how this unknown source of error would influence our findings. Yet despite our inability to account for this layer of uncertainty in our estimates, the magnitude of our finding of rising inadequacy concords with the only previous study that attempted a countrywide assessment of dietary zinc adequacy using a different data source 5 —FAO food balance sheets—which lends confidence to our estimates of the overall worsening trend for the country.
In conclusion, we find that the prevalence of inadequate zinc intake is growing in India and is likely to continue to do so if current trends persist. Furthermore, the effect of ongoing and accelerating carbon dioxide emissions will likely exacerbate these trends as crops lose zinc under elevated CO2. Unless major shifts begin to take hold, it is unlikely that the current trajectory of Indian diets will ameliorate these issues on its own without intervention. We model 2 scenarios aimed at improving the zinc situation and find that only one—returning dietary cereals back to 1983 levels and proportions—is likely to have a meaningful effect, though its practical implementation may be difficult. However, other zinc interventions have already proven effective (direct supplementation, fortification) or show promise (biofortification, advocating for high-zinc diets through dietary diversification). In sum, zinc deficiency may remain an ongoing public health issue in India though significant impact may still be made by devising a targeted program toward high-risk states and populations.
Supplemental Material
Supplemental_Material_clean - Inadequate Zinc Intake in India: Past, Present, and Future
Supplemental_Material_clean for Inadequate Zinc Intake in India: Past, Present, and Future by Matthew R. Smith, Ruth DeFries, Ashwini Chhatre, Suparna Ghosh-Jerath and Samuel S. Myers in Food and Nutrition Bulletin
Footnotes
Authors’ Note
MRS, SSM, and RD designed the study. AC, MRS, and RD analyzed the data with assistance from SSM and SGJ. All authors interpreted the data and wrote the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MRS was funded by a fellowship from Weston Foods US, Inc.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.