
Abstract
Background:
Although undernutrition and sarcopenia are common among older adults and both result in worse health outcomes, data concerning the burden of these conditions in Portuguese community-dwelling older adults are scarce.
Objective:
The aim of this study was to firstly describe the occurrence of sarcopenia and undernutrition among a nationwide community-dwelling sample of older adults.
Methods:
Using a cross-sectional analysis, 1493 Portuguese older adults age ≥65 years from the Nutrition UP 65 study were evaluated. Sarcopenia was defined according to the European Working Group on Sarcopenia in Older People, and undernutrition status was evaluated by Mini-Nutritional Assessment-Short Form.
Results:
Sarcopenia frequency was 11.6%, and of these, 4.4% were classified with severe sarcopenia. Furthermore, 0.8% presented sarcopenic obesity. Undernutrition frequency was 1.3%, and 14.7% of the older adults were classified as being at undernutrition risk.
Conclusion:
Sarcopenia is present in one-tenth of the sample. This frequency taken together with undernutrition data warrants further study and preventive measures.
Introduction
Age decline in physical performance and especially in muscle strength were shown to be significantly higher than the decline in muscle mass. Moreover, the onset of this decline can occur earlier, between the age of 40 and 50. 1, 2 Sarcopenia can be identified as the presence of low muscle mass plus low muscle function (strength or performance) with a risk of adverse outcomes such as physical disability, poor quality of life, and death. 3 Sarcopenia has multifactorial causes, namely, lack of exercise, endocrine dysfunction, chronic diseases, inflammation, insulin resistance, and nutritional deficiencies. 4
The aging process involves a deterioration in some functions that can result in reduced appetite, difficulty in chewing, inflammation of the gums, and a poor diet quality, which can negatively impact nutritional status. 4 Undernutrition status is associated with a decline in muscle mass, impaired muscle function, decreased bone mass, immune dysfunction, anemia, reduced cognitive function, and even higher mortality. 5,6 In Portugal, the frequency of sarcopenia and undernutrition was estimated in adult day care center facilities and in hospitalized older adults 7,8 ; however, results regarding the community are still inexistent. Therefore, it is important to acknowledge the frequency of these conditions in the community. The purpose of this study was to evaluate the occurrence of sarcopenia and undernutrition in Portuguese older adults from the Nutrition UP 65 study.
Materials and Methods
The present study is based on data from a cross-sectional observational study conducted in Portugal. A detailed description of the methods was published previously. 9 Briefly, the Nutrition UP 65 included a cluster sample of 1500 older Portuguese, ≥65 years old, representative of the Portuguese older population in terms of age, sex, education, and regional area. In each regional area, 3 or more town councils with >250 inhabitants were randomly selected, and potential community-dwelling participants were contacted via home approach, telephone, or via institutions, such as town councils and parish centers. Individuals presenting any condition that precluded the collection of venous blood samples or urine (eg, dementia or urinary incontinence) were excluded from the study. Individuals with missing values for triceps skinfold thickness and physical performance measures, which did not enable sarcopenia classification (n = 7), were excluded from the present analysis, and a total of 1493 older adults were included in this study. Muscle mass was estimated, as suggested by Landi et al 10 , by the mid-arm muscle circumference (MAMC), calculated using the following formula: MAMC = mid-arm circumference − 3.14 × triceps skinfold thickness.
A calibrated Jamar® Plus+ Digital Hand Dynamometer (Sammons Preston Inc, Bolingbrook, Illinois) was used to assess muscle strength. Nondominant handgrip strength (HGS) was measured with individuals sitting in a chair without an arm rest, with their shoulders adducted, their elbows flexed 90°, and their forearms in neutral position, as recommended by the American Society of Hand Therapists. 11 Each participant performed 3 measurements with a 1-minute pause between measurements and the higher value was used for the analysis. When the individual was unable to perform the measurement with the nondominant hand, the dominant hand was used. Gait speed was quantified over a distance of 4.6 m. Participants were asked to walk at usual pace in an unobstructed corridor and walking time in seconds was recorded by a chronometer (School electronic stopwatch, Dive049, Topgim, Portugal).
Sarcopenia was identified using the European Working Group on Sarcopenia in Older People (EWGSOP) criteria as the presence of low muscle mass plus low muscle strength (measured by HGS) or low physical performance (measured by usual gait speed). 3 Low muscle mass was classified as MAMC less than 21.1 cm or 19.2 cm in men or women, respectively. 10 Low muscle strength was classified as grip strength <20 kg in women and <30 kg in men, and a gait speed of ≤0.8 m/s identified participants with poorer physical performance. 3 Individuals who were unable to perform gait speed test due to mobility or balance limitations (n = 29) were considered to have this criterion. Sarcopenic obesity was diagnosed by the coexistence of both sarcopenia using the EWGSOP criteria and obesity, identified by World Health Organization body mass index (BMI) classification.
The Portuguese version of the Mini-Nutritional Assessment®-Short Form (MNA-SF) was applied. A participant scoring ≤7 out of 14 points was classified as undernourished, one who scores between 8 and 11 was at risk of undernutrition, and one who scores between 12 and 14 points was considered well-nourished. 12
Ethics
This research was conducted according to the guidelines established by the Declaration of Helsinki, and the study protocol was approved by the ethics committee of the Department of Ciências Sociais e Saúde (Social Sciences and Health) from the Faculdade de Medicina da Universidade do Porto (PCEDCSS—FMUP 15/2015) and by the Portuguese National Commission of Data Protection (9427/2015). All study participants (or 2 representatives if the participant was deemed to be cognitively impaired) signed an informed consent form.
Statistical Analyses
All statistical analyses were performed using IBM SPSS Statistics 23 (SPSS, Inc, an IBM Company, Chicago, Illinois). Descriptive analyses were conducted to show the characteristics of the study sample according to sex, and comparison between the groups was conducted using χ2 test or Fisher's exact test. Confidence intervals were computed at 95%, and statistical significance was defined by P < .05.
Results
The main characteristics of the 1493 participants are presented in Table 1. Age ranged from 65 to 100 years, and the median age was 74.0 (interquartile range: 11.0) years. Women represented 59.7% of the sample. Regarding sarcopenia status, 108 were classified as sarcopenic (7.2%) and 66 as severely sarcopenic (4.4%), resulting in a total frequency of 11.6% of this syndrome. Sarcopenic obesity was present in 0.8% of the older adults (n = 12).
Characteristics of Participants, according to sex.
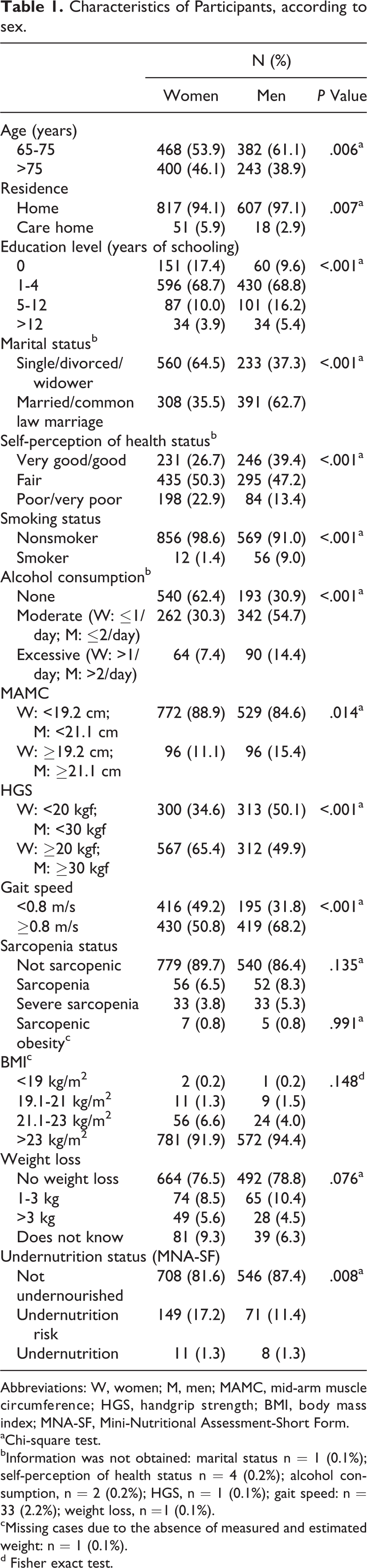
Abbreviations: W, women; M, men; MAMC, mid-arm muscle circumference; HGS, handgrip strength; BMI, body mass index; MNA-SF, Mini-Nutritional Assessment-Short Form.
aChi-square test.
bInformation was not obtained: marital status n = 1 (0.1%); self-perception of health status n = 4 (0.2%); alcohol consumption, n = 2 (0.2%); HGS, n = 1 (0.1%); gait speed: n = 33 (2.2%); weight loss, n =1 (0.1%).
cMissing cases due to the absence of measured and estimated weight: n = 1 (0.1%).
d Fisher exact test.
Concerning undernutrition status, evaluated by the MNA-SF, 19 (1.3%) older adults were classified as undernourished and 220 (14.7%) at undernutrition risk. Women and men differed in all the studied characteristics, except for sarcopenia status (P = .135), sarcopenic obesity (P = .991), BMI (P = .148), and weight loss (P = .076). The frequency of each criterion which was used to diagnose sarcopenia was evaluated. Low muscle mass was present in 12.9% of all older adults. Higher frequencies were observed for low handgrip strength and low gait speed criteria, respectively, the first 58.9% and the second 56.9%.
Discussion
This study describes the burden of sarcopenia and undernutrition in a nationwide sample of community-dwelling older adults. Sarcopenia occurrence (11.6%) is within the values previously described in a systematic review that estimated the prevalence of sarcopenia in studies conducted in community-dwelling older adults (1%-29%). 13 However, it should be referred that sarcopenia prevalence is highly dependent on the applied diagnostic criteria. 14 Even though the EWGSOP definition was used in all studies included in this systematic review, methodologic differences can be noted, because MAMC was applied in only 2 studies to estimate muscle mass. 10,15 In the latter studies, the frequency of sarcopenia was considerably higher than the current one and this may be due to the fact that their samples were also older. Despite not being recommended, 3 anthropometric measures are easily applied in large population surveys and clinical practice, due to its simplicity. 16 Furthermore, there is lack of data comparing MAMC with the gold standard for assessing muscle mass in the identification of sarcopenia.
The HGS values within Nutrition UP 65 study have been previously discussed. 17 Similarly, a high frequency of low gait speed (56.9%) was observed in this study, but a much lower frequency of low muscle mass was present (12.9%). These results are in line with previous longitudinal research where these indicators were evaluated during the life course. Indeed, muscle strength and physical performance suffer a greater decline than muscle mass and this decline may start as early as middle age. 1,2
Undernutrition status values can vary significantly in accordance with inclusion criteria and the assessment tool chosen by the studies. When the MNA-SF was applied to older adults in the community setting, undernutrition and undernutrition risk were estimated to range from 8% to 29.6%. 18 In a Portuguese city, higher frequencies of undernutrition and undernutrition risk were observed comparing with the present study (2.1% and 31.8% vs 1.3% and 14.7%, respectively), notwithstanding the sample of that study included individuals of day care center facilities who are expected to have greater decline in nutrition status. 7
Some weaknesses can be discussed. First, from the initial sample, 7 individuals were excluded from this study, and also the database has some missing values. Second, in order to be included, participants (or 2 representatives if the participant was deemed to be cognitively impaired) had to sign an informed consent form, which may have created a participation bias and led to a lower frequency of the conditions in this study. Additionally, low muscle mass criterion was measured by means of MAMC, which may underestimate the older adults at risk of sarcopenia and hamper the comparison with previous studies which used bioelectrical impedance analysis (BIA) or dual-energy X-ray absorptiometry (DXA). In contrast, this study has several strengths. It was the first to advance knowledge on the frequency of sarcopenia and undernutrition in the Portuguese community-dwelling older adults. Additionally, undernutrition status was evaluated using MNA-SF, which is a well-recognized tool to assess nutritional status.
In conclusion, sarcopenia is present in approximately one-tenth of Portuguese older adults included in this sample (11.6%). Moreover, 16% were undernourished or at risk of undernutrition. These results are of major relevance to plan public health interventions.
Footnotes
Authors’ Note
ARSS and TFA designed this research; CA, NB, AS, PP, PM, and TFA contributed to the Nutrition UP 65 study design. ARSS and TFA analyzed the data. All authors contributed to manuscript preparation and approved the final version of the manuscript submitted for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: The present project was granted in 85% by the Public Health Initiatives Programme (PT06), financed by EEA Grants Financial Mechanism 2009 to 2014 and in 15% by Faculdade de Ciências da Nutrição e Alimentação da Universidade do Porto.