
Abstract
Background:
Hidden hunger affects individuals who chronically consume an inadequate intake of at least 1 micronutrient and is associated with low dietary diversity. Little data are available on dietary intake or status assessment of B vitamins among preschool children in Zambia.
Objectives:
The aim of this study was to assess 24-hour dietary recall records obtained from Zambian children aged 3 to 7 years for B vitamin intake in relation to adequacy and change over time in the same community.
Methods:
Twenty-four-hour dietary recalls were collected from 2 studies that were 2 years apart in the same district of Zambia. Data were retrospectively analyzed for B vitamin intake, that is, biotin, vitamin B12, folate, niacin, pantothenic acid, vitamin B6, riboflavin, and thiamin. The estimated average requirement (EAR) cut point method was used to assess inadequacy prevalence for EARs established by the Institute of Medicine in the United States.
Results:
For all B vitamins, mean values were below the EARs established for children 4 to 8 years old. Relative to the EAR, children had the highest intakes of vitamin B6 with inadequacies of 77.9% and 60.1% in 2010 and 2012, respectively. The highest prevalence of inadequate intake was associated with folate, where ≥95% of the children had intakes below the EAR in both studies.
Conclusions:
All median vitamin B intakes were inadequate among these young children in rural Zambia. Future researchers and policy makers may need to consider B vitamin status in resource-poor areas of the country.
Introduction
Hidden hunger results from regularly lacking adequate consumption of at least 1 micronutrient and is estimated to affect 2 billion people globally. 1 This occurs in areas with low dietary diversity and can be confounded by processing, cooking, and storage techniques resulting in loss of nutrients. It is estimated that maize contributes one-third of the calories available in the food supply in Southern African countries and up to half in countries such as Lesotho and Zambia. 2 Maize is naturally low in bioaccessible niacin and the essential amino acid tryptophan, which places populations that consume maize as a staple food at risk of pellagra. 3 Furthermore, maize is a poor source of folate, and high dependence as a staple has been associated with neural tube defects. 2 Micronutrients from maize are further restricted in many countries due to consumer preferences for white maize, 4 which is a poor source of provitamin A carotenoids, 5 and for “super” maize meal which is highly refined, thus reduced in B vitamins and minerals due to bran and germ removal. 6
Zambia is included in the top 20 countries with a high Hidden Hunger Index, 1 where low dietary diversity is a major contributor to inadequate micronutrient intakes. 7 Schmaelzle et al reported that preschool Zambian children had macronutrient intakes that met dietary recommended intakes according to dietary recall (n = 1048), but many minerals including calcium, iron, and zinc were below recommendations. 8 Another analysis of 24-hour dietary recall records (n = 928) from 4- to 8-year-old Zambian children indicated that mean intakes of vitamin B12, folate, and calcium were below the recommended daily allowance (RDA), but other B vitamins were adequate. 9 Vitamin B12 deficiency has been documented in 87% and 95% of Zambian children under 5 years and women, respectively. 10 Mondloch et al measured serum alanine aminotransferase (ALT) activity to assess liver function in Zambian children with elevated liver retinol stores and serum retinyl esters and found this activity to be low. 11 Follow-up analysis of serum pyridoxal-5’-phosphate (PLP), essential for ALT activity, revealed deficient vitamin B6 status in 79% of these children. While there are efforts to improve status of micronutrients such as vitamin A and iodine, 12 these findings suggest that B vitamin intake and status may be an overlooked public health issue in Zambia.
The aim of this short communication is to assess 24-hour dietary recall records obtained from Zambian children during previous studies 8,13 for B vitamin intakes (ie, biotin, vitamin B12, folate, niacin, pantothenic acid, vitamin B6, riboflavin, and thiamin) in relation to the prevalence of inadequacy and examine differences among younger and older children.
Materials and Methods
Participants and Food Record Analysis
As part of 2 biofortified maize intervention studies, 24-hour recalls were conducted with Zambian children and analyzed primarily for vitamin A and macronutrient intakes. 8,13 All human participants' procedures were approved by the Tropical Diseases Research Center Ethics Review Committee (Ndola, Zambia) and the University of Wisconsin’s Health Sciences Human Subjects Institutional Review Board. The first trial was solely a food intervention and thus was not registered. The second trial in the older children included a daily preformed vitamin A supplement in the positive control group and therefore was registered at National Institutes of Health (NIH) Clinical Trials (registry number NCT01814891). Written informed consent was obtained from parents or caregivers, who were instructed to be present on Mondays when full 24-hour recalls from Sundays were performed.
In both studies, children were recruited from the same rural villages in the Eastern Province of Zambia, but represented different age groups in 2010 (3-5 years) and 2012 (5-7 years). These communities had expressed interest in participating following sensitization efforts related to biofortified orange maize by HarvestPlus nutritionists, the principal investigator (S.A.T.), and a representative from the National Food and Nutrition Commission (Lusaka, Zambia). Subsequent findings of low serum retinol concentrations in 2009 confirmed targeting this province. 14 After household listings of eligible children in the desired age range were obtained, recruited children were screened. Exclusions included children with severe anemia (<70 g/L), undernutrition (weight-for-age and weight-for-height z scores <−3), or presence of clinical infection causing fever. Those determined to be relatively healthy were enrolled; the first study enrolled 195 children and the second 140 (Figure 1). The main vitamin A efficacy details have been published for both studies. 15,16
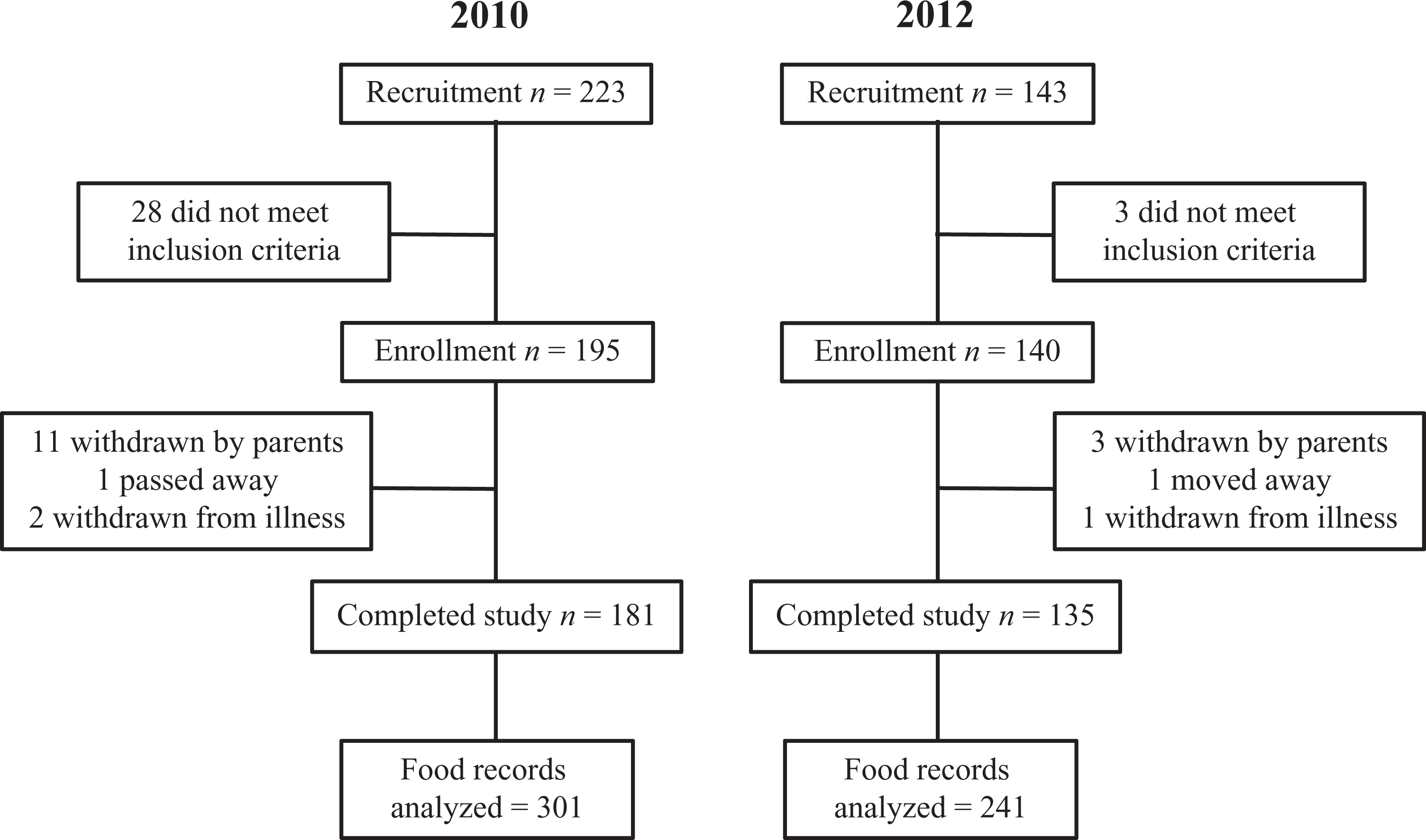
CONSORT flow diagram of participant recruitment, enrollment, study completion, and analyzed food records for the 2010 and the 2012 studies.
After finding deficient vitamin B6 status in the older children, 11 compiled dietary intake data from the 24-hour recalls were further investigated for all B vitamin intakes. Data for biotin, vitamin B12, folate, niacin, pantothenic acid, vitamin B6, riboflavin, and thiamin were retrieved from the food recalls analyzed with Nutritionist Pro software (Axxya Systems v 7.0.0) during the previous studies 8,13 and retrospectively evaluated. The previous studies provided treatment diets 6 days a week, leaving participants to consume their normal meals on Sundays. Values were analyzed from food records on nontreatment Sundays from the previous studies to access usual intake, and then compared with the recommended requirements for the appropriate age group (Table 1). 17
Recommended Intakes for B Vitamins From the Institute of Medicinea and Food and Agriculture Organizationb for Children.
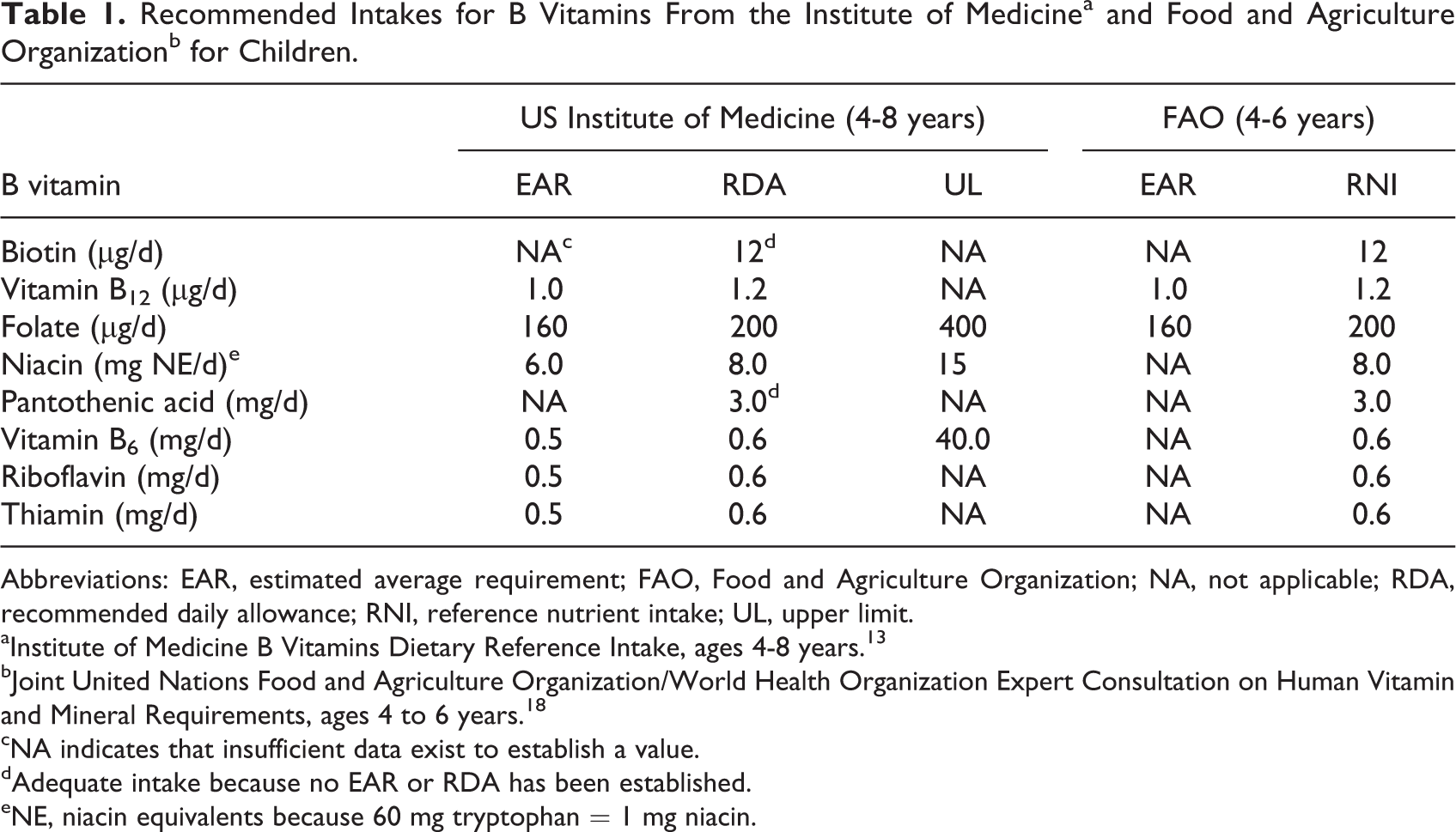
Abbreviations: EAR, estimated average requirement; FAO, Food and Agriculture Organization; NA, not applicable; RDA, recommended daily allowance; RNI, reference nutrient intake; UL, upper limit.
aInstitute of Medicine B Vitamins Dietary Reference Intake, ages 4-8 years. 13
bJoint United Nations Food and Agriculture Organization/World Health Organization Expert Consultation on Human Vitamin and Mineral Requirements, ages 4 to 6 years. 18
cNA indicates that insufficient data exist to establish a value.
dAdequate intake because no EAR or RDA has been established.
eNE, niacin equivalents because 60 mg tryptophan = 1 mg niacin.
Assessing Prevalence of Nutrient Inadequacy
The estimated average requirement (EAR) cut point method is used to estimate nutrient inadequacy in a population by evaluating the distribution of intakes below the EAR as a percent at any given time. 19 The EAR cut point method accounts for variation in requirements of a population and is more appropriate than simply comparing means or using RDAs, 20 which are meant to cover requirements for 97.5% of healthy individuals. In the 2010 and 2012 Zambian children studies, 68% and 75% of participants had 2 days of 24-hour dietary recall, respectively, while the remaining had 1 day of complete records. To remove dependent variables and adjust for day-to-day variation, midpoint values were used within participants for those who had 2 days of dietary recall. Statistics were calculated from the adjusted data, which included the midpoints and data from participants who completed 1 complete 24-hour dietary recall. Estimated average requirement cut point was determined from adjusted values with the NORM.DIST (adjusted mean intake, EAR, adjusted intake standard deviation [SD], false) function (Microsoft Excel 2016) for vitamin B12, folate, niacin, vitamin B6, riboflavin, and thiamin. The EAR for niacin includes niacin equivalents from tryptophan where 60 mg tryptophan equals 1 mg niacin, 17 thus tryptophan intake was also recorded and included in niacin cut point assessment. All records were compared with the EAR for 4- to 8-year-olds of the respective vitamins even though the 2010 study included 3-year-old children. The difference between the EAR of 1- to 3-year-old and 4- to 8-year-old children is about 80% for the B vitamins.
Statistical Analysis
Means, medians, and SDs of intakes were calculated for each nutrient separately for each study. For B vitamins lacking an established EAR (ie, biotin and pantothenic acid), means, medians, and SDs were calculated as described above but prevalence of inadequacy was not assessed. Changes in intake between the 2 studies, which represented different age groups, were assessed with 2-sample t tests.
Results
Study characteristics are summarized in Table 2. In these preschool children from rural Zambia, retrospective dietary record analysis by EAR cut point method revealed intakes of all B vitamins were significantly below the respective EAR during both the 2010 and 2012 studies (Table 3). Calculation of prevalence of inadequacy for biotin and pantothenic acid was not possible due to lack of an established EAR. For biotin and vitamin B12, primarily obtained from animal-sourced foods, medians were below means due to many extremely low intakes. Animal-sourced foods are limited in resource-poor areas of Zambia. In both groups of children, vitamin B6 was the most adequately consumed B vitamin with 22% and 40% of intakes meeting the EAR in 2010 and 2012, respectively. Folate had the poorest intake, with ≥95% inadequate intake from both sets of records.
Study Participant Characteristics and Dietary Recall Records.
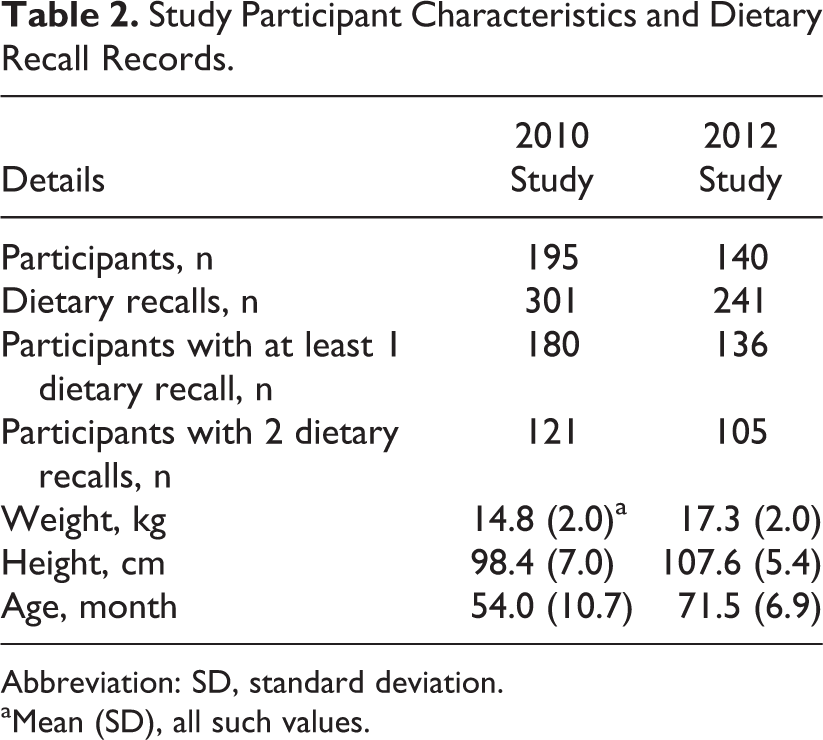
Abbreviation: SD, standard deviation.
aMean (SD), all such values.
Vitamin B Intakes of Zambian Children From 24-Hour Dietary Recall Records.a
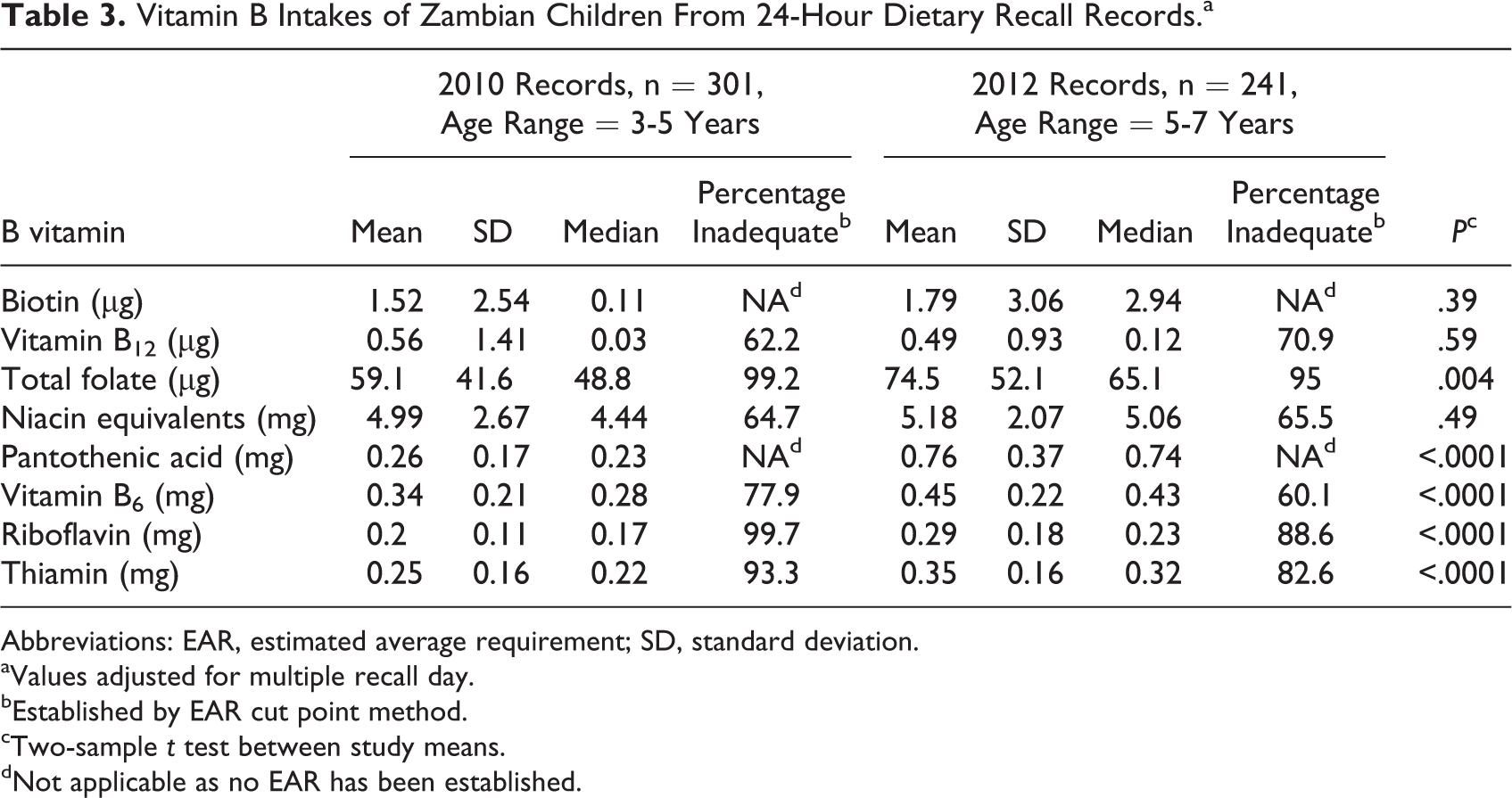
Abbreviations: EAR, estimated average requirement; SD, standard deviation.
aValues adjusted for multiple recall day.
bEstablished by EAR cut point method.
cTwo-sample t test between study means.
dNot applicable as no EAR has been established.
Many B vitamin mean intakes increased from 2010 to 2012 (Figure 2), except for vitamin B12, which did not change from 0.56 to 0.49 μg/d (P = .59). The increases were expected due to increased food intake related to growth and the age differences in the children (Table 2). Of note, the intakes of folate (P = .004), pantothenic acid (P < .0001), vitamin B6 (P < .0001), riboflavin (P < .0001), and thiamin (P < .0001) significantly increased, while mean intakes of biotin and niacin were not different.
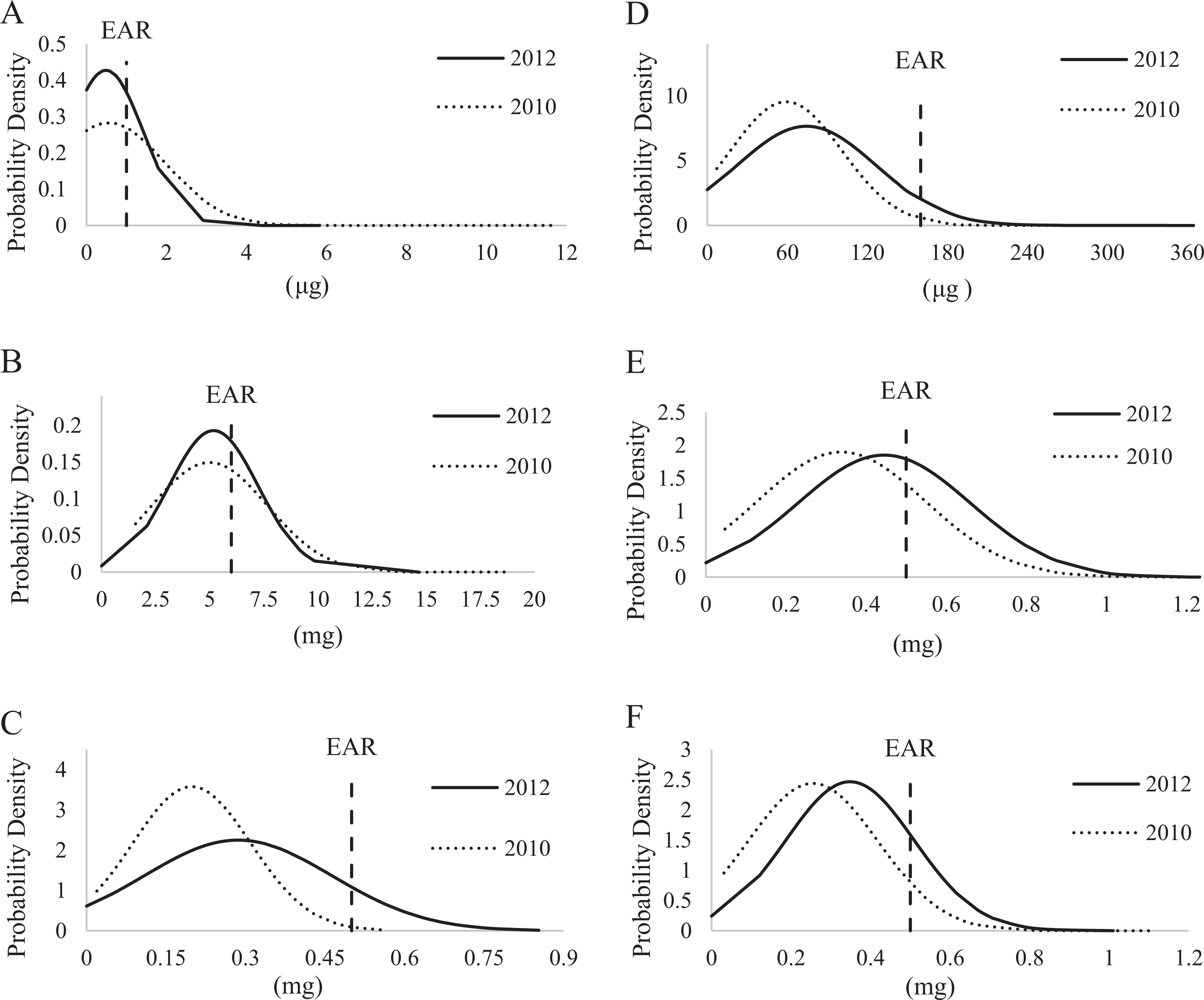
Overlaid vitamin B intake distributions from 2010 and 2012 studies assessed by 24-hour dietary recall for vitamins with estimated average requirements (EARs): A, vitamin B12; B, niacin; C, riboflavin; D, folate; E, vitamin B6; and F, thiamin.
Discussion
This analysis demonstrated a 60% or higher prevalence of inadequate intakes of all B vitamins among young children enrolled in 2 studies in rural Zambia. In prior studies, Zambian children had prevalent indicators of hidden hunger and micronutrient malnutrition, with reports of 40% stunting and 15% underweight. 21 Furthermore, 15% of children under 5 years are estimated to be zinc-deficient, 20% are vitamin A-deficient based on serum retinol concentrations, 21% are iron deficient (56% anemic), and 87% are deficient in vitamin B12. 10 The Zambian government mandates fortification of salt with iodine, margarine with vitamins A and D, and sugar with vitamin A. 12 Folic acid and iron fortification of maize meal gained support in 2006, but concerns over an association with increased malaria mortality 22 lead to governmental rejection. Given these data and the observed lack in dietary diversity, 7 other nutrients, including B vitamins, need further assessment in Zambian children before fortification should move forward.
Niacin deficiency causes pellagra, which was observed in the Southern province of Zambia after a drought in the early 1990s. 23 Malawi, a country neighboring Zambia that is dependent on maize as a staple food, more recently experienced an increased incidence of pellagra. 24 Niacin deficiency is associated with other deficiencies, including protein, riboflavin, vitamin B6, thiamin, folic acid, vitamin A, magnesium, potassium, iron, and zinc. 3 There have been reports of high liver retinol stores, elevated serum retinyl esters, 11 and hypercarotenodermia 25 in some Zambian children, which conflicts with other reports of vitamin A deficiency established with low serum retinol. 26 Niacin-derived compounds, especially nicotinamide adenine dinucleotide (NAD), are cofactors for vitamin A metabolic enzymes. 27 Given prior niacin deficiency problems and the dependence on maize as a staple food, niacin status assessment may be needed in Zambia.
The analysis of the 2012 study dietary recall records revealed a 60.1% vitamin B6 dietary inadequacy and a mean intake of 0.45 mg/d, which is below the established EAR. In this same cohort, low serum PLP (the functional biomarker of vitamin B6) values were found, with 79% of children below the serum PLP cutoff for deficiency (ie, 20 nmol/L). 11 Considering that vitamin B6 intakes were actually one of the highest in relationship to the EAR compared with the other B vitamins evaluated, biochemical determination of all B vitamins in Zambian children is warranted. Furthermore, due to the reported widespread iron deficiency and anemia, 10 vitamin B6 deficiency is troublesome due to its need for heme synthesis. 17 It is worth noting that the children with the low serum PLP also had elevated C-reactive protein, 11 which has been associated with low serum PLP due to compartmental shifts to tissues with higher demands in times of inflammation. 28 However, this does not negate concern, as it has also been reported that dietary vitamin B6 requirements are increased during times of inflammation. 29
Vitamin B6 in the form of PLP and riboflavin in the form of flavin adenine dinucleotide, along with iron, are required as cofactors in the pathway to convert tryptophan into NAD. 30 This analysis included niacin equivalents from tryptophan conversion by the kynurenine pathway as outlined by the Institute of Medicine at 60 mg tryptophan to 1 mg niacin. 17 Because this pathway requires PLP as a cofactor, it is uncertain if the flux of this pathway would be unchanged in the presence of vitamin B6 deficiency, such as that observed in the 2012 study. Niacin intake accounted for 62% and 67% of total niacin equivalents in 2010 (3.10 mg/ d) and 2012 (3.46 mg/d), respectively. Inadequacy, if assessed by using niacin alone, was 89.3% and 93.3% in 2010 and 2012, respectively, so the true niacin inadequacy is likely between these values and the 64.7% and 65.5% found when niacin equivalents were used.
Riboflavin deficiency was suggested to be protective against malaria infection, 31 but studies using more sophisticated analytical techniques have questioned this assertion. 32 Riboflavin supplementation increased hemoglobin response to iron supplements in anemic participants with deficiency in Gambia. 33 Whole grain maize contains more riboflavin, and B vitamins in general, than refined maize. Whole grain contains 0.2 mg riboflavin/100 g maize, 2 which is 40% the EAR for children, 17 whereas refined grain contains between 0.08 and 0.1 mg/100 g or 16% to 20% the EAR for children. Although all whole grain maize contains more total B vitamin content, processing can increase bioaccessibility, especially for thiamin and niacin. 2 Some countries, especially those located in the Americas, that rely on maize have avoided niacin deficiency by nixtamalizing maize with base, which releases bound niacin. 2 This process has not been adopted in traditional Zambian cuisine.
Inadequate intake of thiamin may be of particular concern in this region. Beriberi, caused by severe thiamin deficiency, can present with a variety of symptoms, including peripheral neuropathy and muscle weakness, myocardial dysfunction and edema, encephalopathy and cognitive impairments, and hypoglycemia and lactic acidosis. Of concern is the potential relationship of malaria infection and nonberiberi thiamin deficiency as observed in patients from Thailand 34 and Laos. 35 From the available evidence, it is not possible to determine whether this is a causal relationship, but it is thought that thiamin deficiency may contribute to the acidosis caused by the increased need for glucose and lactate disposal of malaria.
These findings are limited because they are based on data from 24-hour dietary recalls and not weighed food records, and day-to-day variation was not quantified. It is also likely that the available nutrient data for some of the traditional foods entered into the Nutritionist Pro Software do not truly represent those consumed in these Zambian communities. For example, it is common to consume small dried whole fish, locally called kapenta, which were entered as herring into the program. While protein and fat may be accurate, the micronutrients in kapenta are likely underrepresented because bones and organs are consumed in these whole fish. The 24-hour dietary recall does not reflect long-term intake and may be susceptible to recall bias. 36
These data are from eastern rural Zambian children who were involved in intervention studies and may not represent other areas of the country. However, the universally low B vitamin content of the monotonous diets in these children in addition to the biochemical finding of deficient serum concentrations of PLP 11 should be of concern. Further research is needed to evaluate the degree of B vitamin deficiency in Zambian children and the risks and benefits of increased B vitamin intake to determine which interventions should be recommended.
Footnotes
Authors’ Note
The 2012 trial is registered with NIH Clinical Trial registry number NCT01814891. T.J.T. looked critically on the B vitamin intakes and wrote the first draft of the manuscript. S.T.S. entered all data for the trial in 2012, and E.T.N. did the same for the 2010 trial. J.F.G. performed the serum analysis of PLP and had intellectual input into the manuscript. S.A.T. conceived the idea of evaluating B vitamin intakes and revised the manuscript.
Acknowledgments
The authors would like to thank Devika Suri for the consultations about implementing and interpreting the EAR cut point method.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by HarvestPlus contract numbers 8217 and 8256, which were partially funded by the Bill and Melinda Gates Foundation number OPP27510; an endowment to S.A.T. entitled “Friday Chair for Vegetable Processing Research.” HarvestPlus (![]() ) is a global alliance of agriculture and nutrition research institutions working to increase the micronutrient density of staple food crops through biofortification. The views expressed do not necessarily reflect those of HarvestPlus.
) is a global alliance of agriculture and nutrition research institutions working to increase the micronutrient density of staple food crops through biofortification. The views expressed do not necessarily reflect those of HarvestPlus.