
Abstract
Background:
Measurements of mid-upper arm circumference (MUAC) may result in measurement error due to incorrect placement along the arm or tight pulling of tape. To reduce the risk of these measurement errors, a new wider tape was developed.
Objective:
To compare the measurement agreement and precision and the ease of use of the standard and wide MUAC tapes.
Methods:
Mid-upper arm circumference was measured in 814 children aged 9 to 32 months with both tapes. The midpoint of the upper arm was measured with the standard tape and estimated with the wide tape. Standardization sessions were implemented to assess intra- and interobserver precision.
Results:
Mid-upper arm circumference with the wide MUAC tape was significantly larger than the standard tape (mean [standard deviation]: 14.3 [1.0] cm vs 13.9 [1.0] cm; P < .001), resulting in a consistent bias of +0.41 cm. Forty-six (5.7%) children were identified with low MUAC <12.5 cm by standard tape compared with 10 (1.2%) by the wide tape (P <.001). Because a new tape could be reproduced by correcting for this bias, we corrected measured results by subtracting 0.41 cm and mean MUAC by tape type was no longer significantly different. Intra- and interobserver technical error of measurement suggested a better precision with the wide MUAC tape.
Conclusions:
Despite simplifying the measurement by approximating the midpoint of the upper arm, the wide MUAC tape tended to have better precision than the standard MUAC tape. However, there was a consistent measurement bias of +0.41 cm in mean MUAC. This first field test yielded promising results and led to further product adjustments.
Introduction
Mid-upper arm circumference (MUAC) is a commonly used screening measure for assessing under- and overnutrition and is considered a useful tool for identifying children 6 months to 5 years of age with moderate or severe acute malnutrition and an elevated risk of mortality. 1 The current definitions of acute malnutrition are based either on the weight-for-length z-score (WLZ) <−2 standard deviations (SDs) of the World Health Organization (WHO) growth standards 2 or a MUAC measurement <12.5 cm. 3 Severe acute malnutrition in children is defined as a WLZ <−3 SD or a MUAC <11.5 cm. 1 These cutoffs are used to estimate the prevalence of acute malnutrition and to identify children who require treatment. Mid-upper arm circumference is also frequently measured in research projects to assess the impact of nutritional interventions.
The standard tape to measure MUAC is low cost, and the measurement is considered simple. Indeed, in a recent study of 103 children, minimally trained mothers were able to perform and identify most children with severe acute and moderate acute malnutrition using the 3-color MUAC tape, which is color-coded to indicate the cutoffs for moderate and severe acute malnutrition. 4 For accurate measurements, it is recommended that anthropometrists, field workers, and community health workers should be rigorously trained and standardized to perform MUAC measurements. Because the MUAC results may vary depending on which arm is measured and where along the arm the tape is applied, recommended steps include (1) measuring the left and not the right arm, (2) identifying and marking the midpoint between the tip of the shoulder and the tip of the elbow of the bent arm, and finally (3) measuring with the tape in the correct midpoint position on the straightened arm. 5,6 Potential sources of inaccuracy of the current MUAC tape include incorrect placement of the tape along the arm, nonperpendicular, placement of the tape, and pulling the tape too tight and thus squeezing the arm. Any of these errors may result in an incorrect MUAC measurement 7 and affect related referral and treatment actions of children with acute malnutrition. Moreover, any measurement error during surveys may result in substantially overestimating the reported prevalence of acute malnutrition. 8
To simplify the MUAC measurement, a new “wide MUAC tape” has been developed by Intellectual Ventures Laboratory Global Good Fund. The team of developers designed the wider tape to eliminate the need to measure the midpoint between the tip of the shoulder and the tip of the elbow, as the wider tape placed at the estimated midpoint would almost certainly include the midpoint. It was also assumed that the wider tape would be less subject to variation in pressure applied by the user. Because of these new features, we hypothesized that the wide MUAC tape would have equal or better precision than the standard MUAC tape and that it would be preferred by anthropometrists because of its ease of use.
The present study describes the first field testing of the new wide MUAC tape. The objectives of the present study were to compare the standard and wide MUAC tapes with regard to (1) measurement agreement, (2) intra- and interobserver precision, and (3) ease of use.
Methods
The present field test of the wide MUAC tape was nested within an ongoing community-based randomized intervention trial, referred to as the Lao Zinc Study. The primary objective of the Lao Zinc Study was to determine the effects of 2 forms of daily preventive zinc supplementation versus therapeutic zinc supplementation for diarrhea on young children’s physical growth and other health outcomes. Ethical approval for the study protocol and the consent procedure was provided by the National Ethics Committee for Health Research (Lao Population’s Democratic Republic [PDR]) and the institutional review board of the University of California, Davis. The trial was registered at www.clinicaltrials.gov (NCT02428647). Written informed consent was obtained from one of the child’s primary caregivers (mother, father, or legal guardian).
The Lao Zinc Study was implemented in rural villages of Khammouane Province in Lao PDR. Briefly, approximately 3400 infants and young children 6 to 23 months of age were enrolled and individually randomized to 1 of 4 intervention groups. In all groups, children were visited weekly for morbidity surveillance and provision of their assigned supplements for 36 weeks. At baseline and after 18 and 32 to 34 weeks, anthropometric measurements were completed following protocols recommended by the Food and Nutrition Technical Assistance Project. 6 Namely, the body weight of unclothed or minimally dressed children was measured on a frequently calibrated electronic balance with 10 g sensitivity (digital Seca scale 383, Hamburg, Germany). Length was measured with 0.1 cm precision using an infantometer (Seca length board 416). Left MUAC was measured with 0.1 cm precision using a standard nonstretchable 0.8-cm-wide insertion tape (range: 0-26.5 cm, calibrated to 0.1 cm, ShorrTape Measuring Tape; Weigh and Measure, Olney, MD, USA). All measurements were collected in duplicate; if measurements differed by more than 0.1 kg (weight) or 0.5 cm (length, MUAC), the measurement was repeated a third time.
During product development, flat and bifold MUAC designs were manufactured using Mylar material to assess the ease of use of alternative fastening and reading mechanisms on the wider tape. After some in-lab assessments and test measurements of an infant’s MUAC, the bifolded tape was selected for use in this study. This 5-cm-wide MUAC tape (range: 0-34 cm, calibrated to 0.1 cm) had a tunnel-like buckle design that ensured correct alignment for reading (Figure 1).

Prototype of wide mid-upper arm circumference (MUAC) tape used in field testing.
Similar to the standard MUAC measurement, the wide MUAC tape was used to measure MUAC in duplicate, and a third measurement was completed, if the 2 measurements differed by >0.5 cm. Due to the timing of the availability of the new tape in relation to the implementation of the main trial, the assessment of the wide tape was implemented at the midpoint and the end line anthropometric screening visits only. Initially, the wide MUAC measurement was done directly under the armpit of the left arm, as this was considered likely to be the easiest measurement approach. Since this was the first field testing of the new tool, we reserved the option to review preliminary results and adapt measurement strategy as needed. After measuring approximately 270 children with the standard tape and the wide tape under the armpit, we noticed a consistent bias with significantly greater measurements with the wide MUAC tape and hypothesized that this was due to the measurement position under the armpit (Supplemental Table S1). Thus, after an internal discussion among the investigators, the wide tape was used to measure MUAC closer to the point of the upper part of the left arm. However, to keep the measurement technique as simple as possible with the wide MUAC tape, the midpoint of the upper arm was not determined by measurement. Instead, the anthropometrists simply estimated the midpoint when conducting the measurement.
Measurements were completed by 3 teams, each consisting of an anthropometrist and an assistant. Each person was trained in their respective role and responsibilities on measurements of length, weight, and MUAC with the standard tape prior to the start of the study. The wide MUAC comparison study was added while the Lao Zinc Study had already been ongoing and was thus implemented in a subgroup of children during the midpoint and end line anthropometric sessions (Figure 2). Anthropometrists were trained briefly on the recommended use of the wide MUAC tape prior to the commencement of the present field test. Scientific field coordinators and coinvestigators frequently visited the screening sites to provide onsite supervision. In addition, regular standardization sessions were implemented to compare the performance of anthropometry teams among themselves and with their supervisors. 7
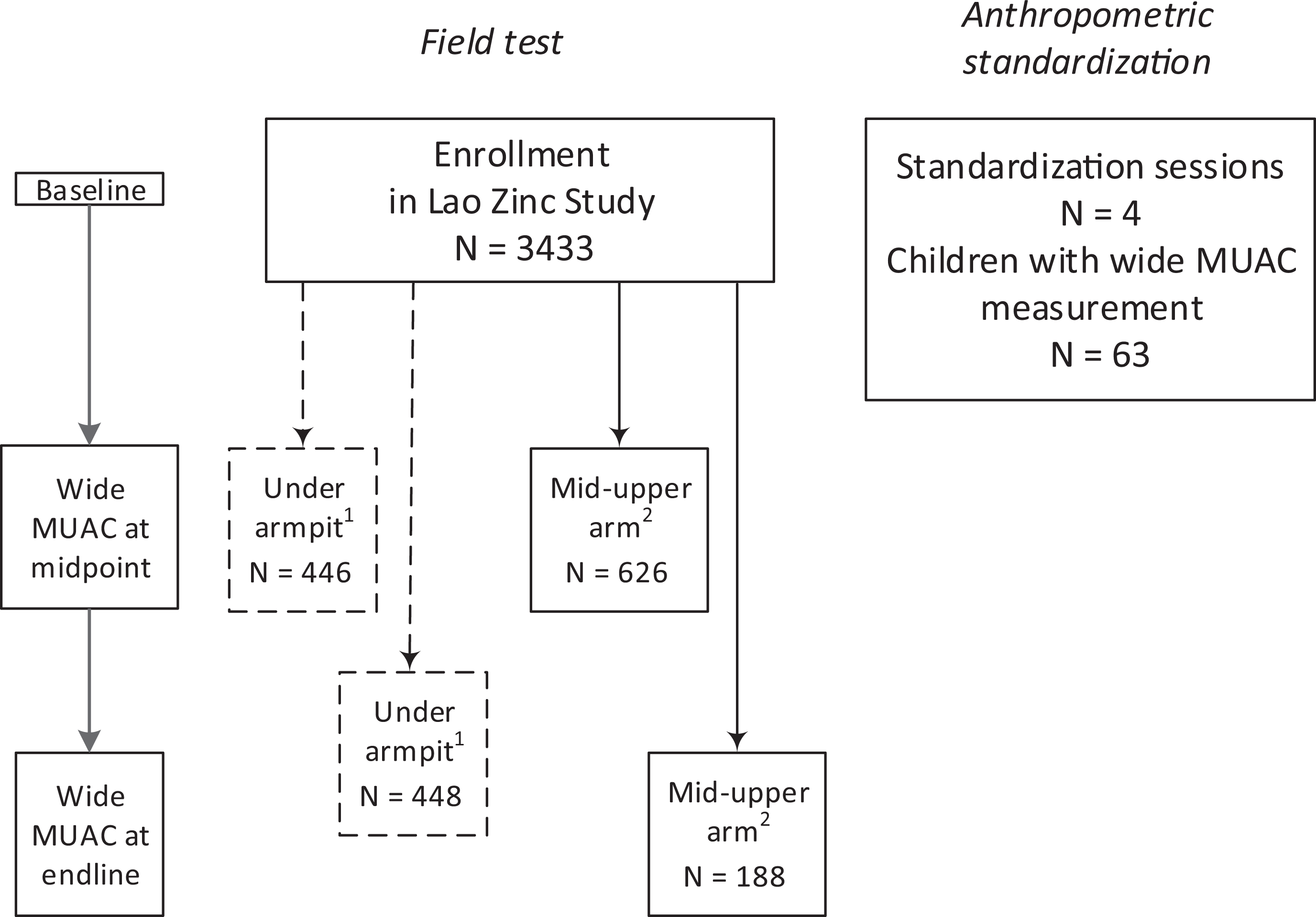
Flowchart of children participating in mid-upper arm circumference measurements with a standard tape and a newly developed wide measuring tape during a field test and anthropometric standardizations. 1 Measurements with the wide tape placed directly under the armpit (results included in Supplemental Material). 2 Measurements with the wide tape placed at the approximate midpoint of the upper arm of the left arm.
For each standardization session, approximately 15 children (range: 9-26 children) were invited, and oral consent by the caregiver was documented on a verbal consent log. Each anthropometry team performed each measurement (ie, length, weight, standard MUAC, wide MUAC under armpit, and/or wide MUAC mid-upper arm) only once and then the child would move on to the next anthropometry team. After completion of 1 round of measurements, the team received a new data collection form for the second round of anthropometric measurements. The purpose of separating the duplicate measurements was to limit the possibility that anthropometry teams would remember and try to match the second measurement to their first measurement. To reduce the participants’ burden, not all anthropometric measurements were performed during all standardization sessions. Thus, the number of sessions varied by anthropometric indices. However, all MUAC measurements were generally performed in the same session and for each child; the order of MUAC measurements (by standard or wide tape) was randomly assigned to reduce possible measurement bias.
A structured questionnaire was developed to collect information from anthropometry staff about their experiences and preferences during the training and use of the MUAC tapes. Prior to conducting the interview, it was emphasized that answering the questionnaire was voluntary. A 5-point scale (eg, 1, not at all easy; 2, slightly easy; 3, somewhat easy; 4, very easy; 5, extremely easy) was used for this questionnaire. The 5-point scale was explained with common examples to ensure that all team members felt confident answering the questionnaire. All members involved in anthropometric measurements agreed to be interviewed (anthropometrists, assistants, and anthropometry supervisors). Because only 8 team members were involved in the MUAC measurements or related supervision, we will present their responses without further statistical analyses.
Statistical Methods
Stata software version 14 (StataCorp [2015], College Station, Texas) was used to complete statistical analyses. The characteristics of the children are presented as mean (SD) or percentage, as appropriate. Length-for-age z-score (LAZ), weight-for-age z-score (WAZ), WLZ, and MUAC-for-age z-score (MUACZ) were calculated according to the WHO growth standards. 2,9 Stunting, underweight, and wasting were defined as <−2 SD LAZ, WAZ and WLZ, respectively. Acute malnutrition (moderate and severe combined) was defined as MUAC measurement <12.5 cm and severe acute malnutrition as MUAC <11.5 cm. 3
In the main analyses, we used a paired t test to test for differences between measurement tapes for continuous variables and a McNemar test for dichotomous variables. Comparisons with P < .05 were considered significant. To examine whether age would modify the results, we repeated the main analyses by age groups for 9- to 15-month-, 16- to 22-month-, and 23- to 32-month-old children. We used Bland-Altman plots to assess the bias and limits of agreement between the wide MUAC placed approximately at the midpoint of the upper arm and the standard MUAC tapes and between the wide MUAC under armpit and the standard MUAC tapes. 10 In another set of analyses, we corrected the wide MUAC results by measurement bias identified by the Bland-Altman analyses to assess whether the tapes would be equally precise after correction.
Technical error of measurement (TEM) and the coefficient of reliability (R) were calculated according to the formulae used in the WHO Multicenter Growth Reference Study. 11 The intraobserver TEM was calculated using 2 measurements per child from the pooled data from standardization sessions and also from the data collected in the field. In standardization sessions, 3 to 5 anthropometric teams measured each child twice. In the field, 2 to 3 measurements were taken per child by 1 anthropometric team and the 2 closest measurements were used for this calculation. The calculation accounts for the different number of children measured by each anthropometric team by allowing the number of children to vary by anthropometric team. The interobserver TEM and R could only be calculated for the pooled standardization sessions. The average of each anthropometric team’s 2 measurements on a child was used for the single measurement for that child. The calculation accounts for the different number of anthropometric teams that measured each child by allowing the number of observers to vary by child.
Results
A total of 814 children with ages 9 to 32 months (mean: 18.0 ± 5.4 months) and a high prevalence of stunting (41.3%) and underweight (28.0%) and a relatively low prevalence of wasting (6.6%) participated in the field testing of the standard and the wide MUAC tape (Table 1). In preliminary studies, we found that for measurements obtained when the wide MUAC tape was placed directly under the armpit, the results were significantly greater than obtained by the standard tape placed exactly at the midpoint (14.9 ± 1.0 cm vs 13.8 ± 0.9 cm; P < .001; Supplemental Table S1).
Baseline Characteristics of Young Laotian Children.
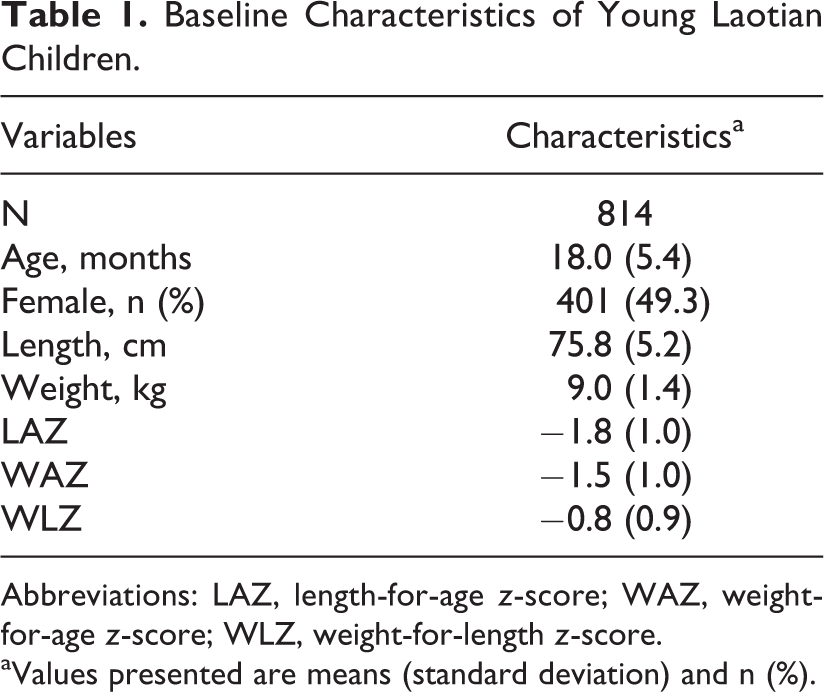
Abbreviations: LAZ, length-for-age z-score; WAZ, weight-for-age z-score; WLZ, weight-for-length z-score.
aValues presented are means (standard deviation) and n (%).
When the wide MUAC tape was placed at the approximate midpoint of the upper arm, measurements with the newly developed wide MUAC tape were still significantly larger than with the standard tape (14.3 ± 1.0 cm vs 13.9 ± 1.0 cm; P < .001; Table 2). However, the difference was less when the wide tape was placed just below the armpit. The Bland-Altman plot indicated a bias of +0.413 cm and 95% limits of agreement were −0.003 to +0.83 cm between the wide tape placed at the approximate midpoint and the standard tape (Figure 3). This difference in mean MUAC was consistent for all age groups (Table 2). Similarly, the ranges in measurements were comparable for both tapes across all age groups. Mean MUACZ for all children was −0.79 ± 0.9 by standard MUAC tape and −0.41 ± 0.8 by wide MUAC (P < .001). All completed duplicate measurements were within the acceptable range of <0.5 cm. In other words, no measurement had to be repeated for a third time, indicating that both tapes were acceptably precise in duplicate measurements.
Mid-Upper Arm Circumference in Young Laotian Children Measured With a Standard Tape and a Newly Developed Wide Measuring Tape, by Age-Group.
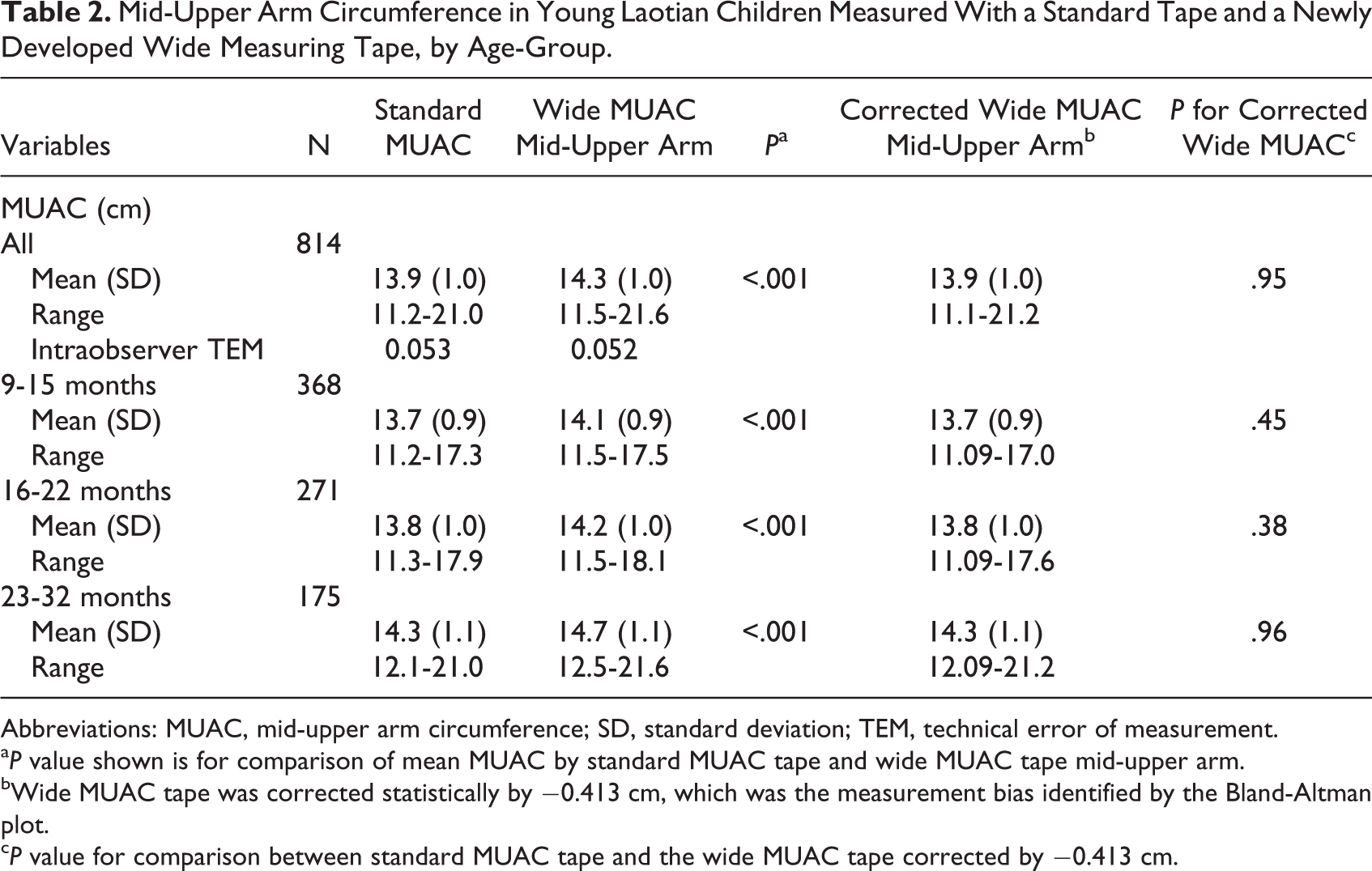
Abbreviations: MUAC, mid-upper arm circumference; SD, standard deviation; TEM, technical error of measurement.
a P value shown is for comparison of mean MUAC by standard MUAC tape and wide MUAC tape mid-upper arm.
bWide MUAC tape was corrected statistically by −0.413 cm, which was the measurement bias identified by the Bland-Altman plot.
c P value for comparison between standard MUAC tape and the wide MUAC tape corrected by −0.413 cm.
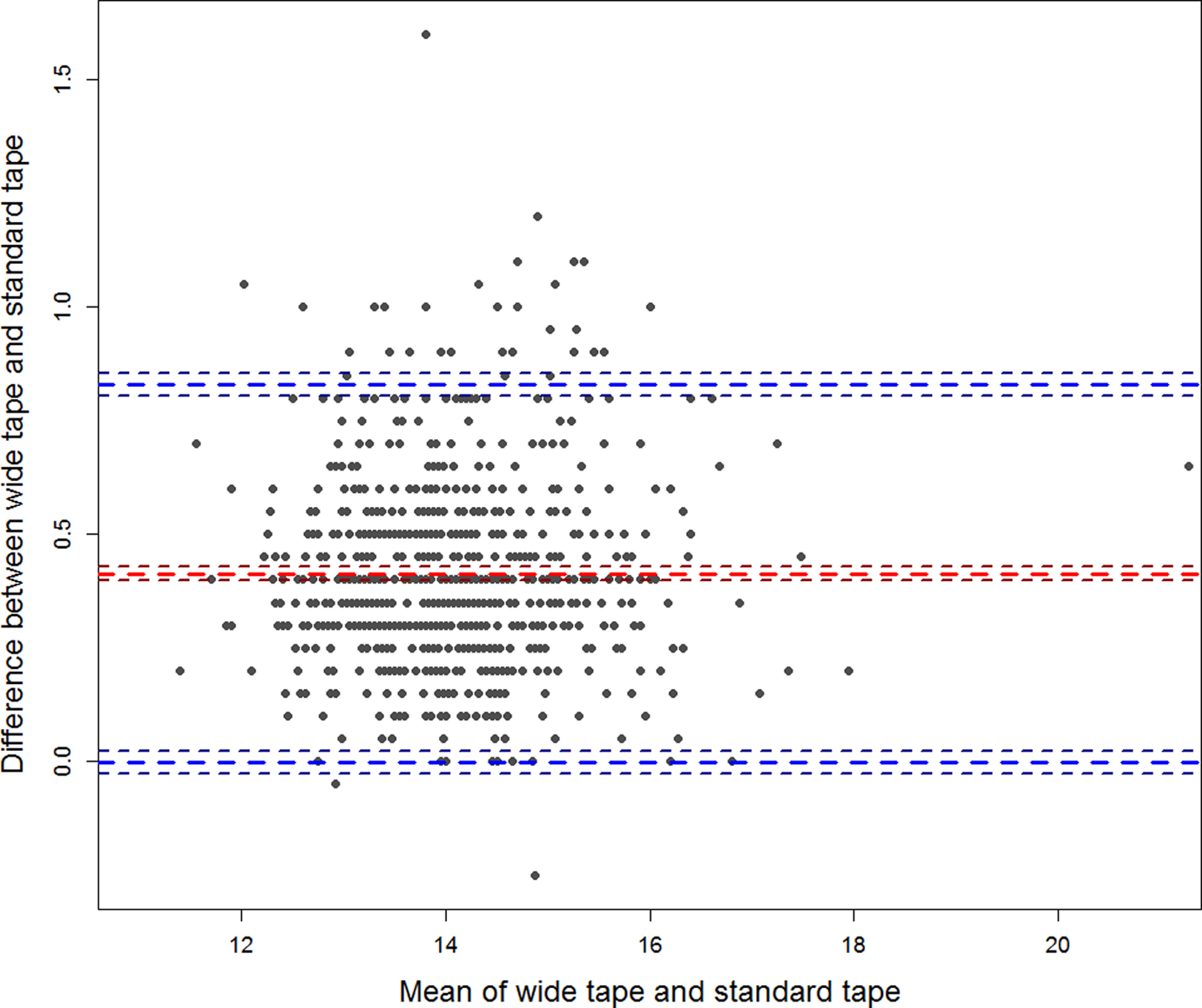
Bland-Altman plot comparing mid-upper arm circumference measured by a standard tape and a newly developed wide tape positioned approximately at the midpoint of the upper arm.
Because the wide MUAC yielded a consistent measurement bias across all age groups and another prototype could be produced to correct for this measurement bias, we also compared the standard MUAC tape with asimulated corrected wide MUAC tape after deducting 0.413 cm from each measurement. After this correction was made, there was no significant difference in mean MUAC between the 2 types of tapes (Table 2).
Forty-six (5.7%) children were identified as acutely malnourished by standard MUAC tape compared with 10 (1.2%) children by the wide MUAC tape (P < .001), and 3 children were identified with severe acute malnutrition by standard tape compared to none by the wide MUAC tape (Table 3). Consequently, sensitivity of the wide MUAC tape was low and specificity was high compared with the standard tape. However, when the wide MUAC tape was corrected by deducting the measurement bias of 0.413 cm, sensitivity and specificity were substantially improved as shown in Table 3. The number of children identified with moderate or severe acute malnutrition was no longer significantly different, except for 1 age-group. In particular, among children 16 to 22 months of age, 13 children were identified with a low MUAC <12.5 cm by standard MUAC tape compared with 19 children by the corrected wide MUAC tape. Thus, more children were identified as malnourished with the corrected wide MUAC tape than with the standard MUAC tape. When we investigated this discrepancy further by exploring the WLZ of differently categorized children, we found that <2% of children with WLZ > −2 SD were identified as malnourished by the corrected wide MUAC tape. Among wasted children (WLZ < −2 SD), the 2 tapes disagreed on a similar number of children. Namely, 4 wasted children were identified as moderately acute malnourished based on MUAC <12.5 cm by wide tape, but not the standard tape, and 3 children were identified with low MUAC <12.5 cm by the standard tape, but not the wide tape.
Percent Children With Low Mid-upper Arm Circumference Measured With a Standard Tape and a Newly Developed Wide Measuring Tape Among Young Laotian Children, by Age-Group.
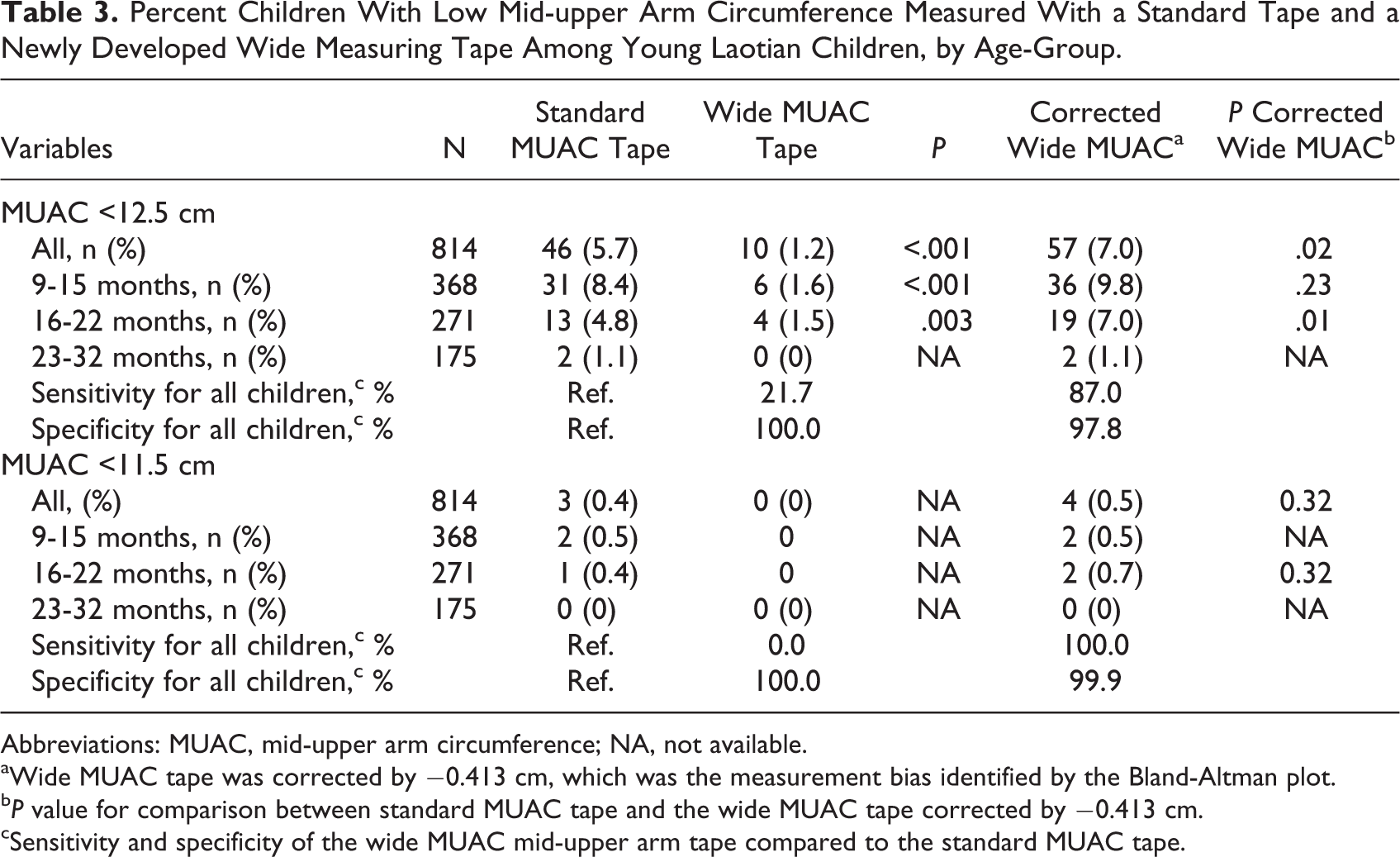
Abbreviations: MUAC, mid-upper arm circumference; NA, not available.
aWide MUAC tape was corrected by −0.413 cm, which was the measurement bias identified by the Bland-Altman plot.
b P value for comparison between standard MUAC tape and the wide MUAC tape corrected by −0.413 cm.
cSensitivity and specificity of the wide MUAC mid-upper arm tape compared to the standard MUAC tape.
Four standardization sessions were organized during the course of the present field testing comparing the standard MUAC tape with the wide MUAC tape measured mid-upper arm. Children had a mean age of 13.8 ± 5.3 months, and 47.6% were boys. The intraobserver TEM (4 sessions; 42 children) for length and weight was 0.38 cm and 0.07 g, respectively, and was considered acceptable. The interobserver and intraobserver TEM for standard MUAC and wide MUAC was also acceptable (Table 4) and suggested that measurements with the wide MUAC tape placed at the approximate midpoint of the upper arm tended to be slightly more precise.
Precision of the Different Mid-Upper Arm Circumference Measuring Tapes When Used by the Different Observers and the Same Observer (Results From Standardization Sessions).
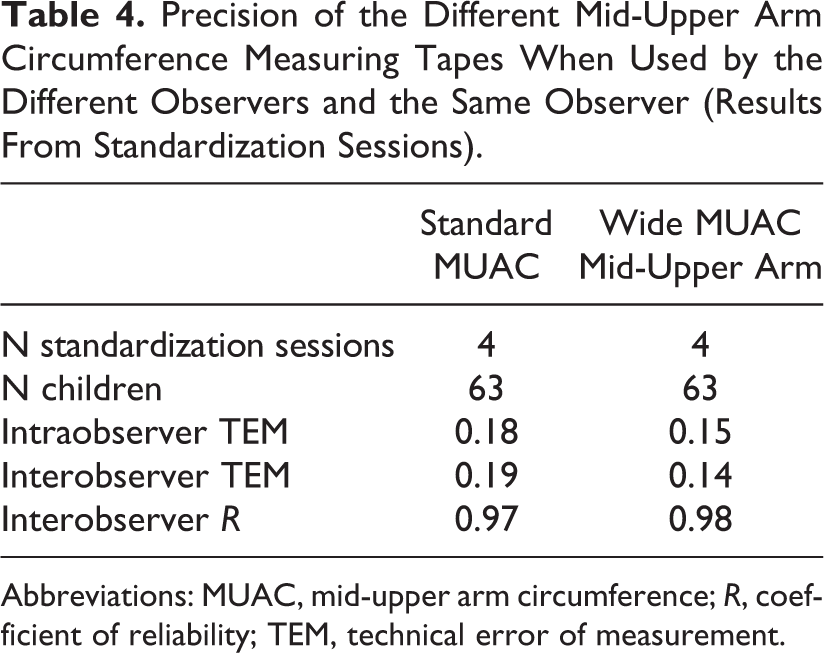
Abbreviations: MUAC, mid-upper arm circumference; R, coefficient of reliability; TEM, technical error of measurement.
Eight team members (3 anthropometrists, 3 anthropometry assistants, and 2 anthropometry supervisors) were involved in the MUAC training, assessments, and/or supervisions and answered a structured questionnaire about their experiences and preferences regarding the 2 types of MUAC tapes. Using a 5-point scale ranging from 1 (not at all easy) to 5 (extremely easy), they tended to find learning and using the wide MUAC tape slightly easier. The mean score for learning was 3.1 for the wide MUAC tape compared to 2.6 for the standard MUAC tape, and similarly, the mean score for ease of work was slightly higher (3.5 vs 3.1, respectively). However, the standard MUAC tape was ranked a little higher with regard to their preference for use (3.5 for standard vs 3.0 for wide MUAC). Interestingly, 6 of 8 team members perceived measurements by the standard MUAC tape as more precise than the wide tape. Some additional insights were gained by the open-ended responses provided by the team members. Although they found the extra step needed to measure the midpoint location of the arm with the standard MUAC tape cumbersome, time-consuming, and irritating for the child, some also perceived this same step as important to ensure precision, although this perception was not confirmed by the study results. Several individuals also raised concerns about the material used for this first prototype of the wide tape and suggested it should be softer. Other common suggestions were to add the 3 colors (red, yellow, and green) to the wide MUAC tape to give it “a friendlier look” and because the colors may distract the child temporarily from the measurement.
Discussion
The present study was the first field test of an innovative 5.0-cm-wide MUAC tape, which was placed at the approximate midpoint of the upper arm without measuring the exact location between the tip of the shoulder and the tip of the elbow. Despite simplifying the measurement by approximating the midpoint of the upper arm, the wide MUAC tape tended to have better precision than the standard MUAC tape, possibly because of less variability in compression of the arm. However, we found a consistent measurement bias of +0.4 cm in mean MUAC of children 9 to 32 months of age with the wide MUAC tape compared with the standard MUAC tape, which was consistent across all age groups. To explore the potential of the wide MUAC tape, we corrected the measurements by deducting the identified measurement bias and found that there was no longer a difference in mean MUAC between the 2 tapes. Thus, the wide MUAC tape has the potential to become a useful tool after further product developments. Independently from our own developments, a consortium including Médecins Sans Frontières, Action Against Hunger, HelpAge International, and the International Committee of the Red Cross made some design improvements to the standard MUAC tape and developed a new medium-width MUAC tape named uniMUAC (2.5 cm width; range: 0-32 cm; calibrated to 0.1 cm). The first field test of mother-led MUAC screening in Kenya showed promising results, and further field tests are ongoing (Angeline Grant, personal communication, June 20, 2017).
The slightly higher precision with the wide MUAC tape may be of particular advantage in program settings, where anthropometric measurements are often done by community health volunteers or individuals with minimal training and supervision. Although a recent methodological report of Demographic and Health Surveys did not include MUAC specifically, the anthropometric data quality of height and weight assessments was considered inadequate in some of the surveys. 12 In their report, Assaf et al pointed to several cases of measurement errors and also highlight the need for more practice in the measurement. Because both length and MUAC measurements are considered challenging in the field, it is likely that similar conclusions would be drawn for MUAC measurements in programmatic settings. Thus, the simplified measurement and higher precision of the wide MUAC tape may prove to be useful in these settings.
Mid-upper arm circumference and WLZ are recommended indicators for identifying children 6 months to 5 years of age with moderate or severe acute malnutrition. 1,3 The uncorrected wide MUAC tape had a low sensitivity and failed to identify the same number of children with moderate or severe acute malnutrition as identified by the standard MUAC. Thus, the current prototype would not be acceptable in community- and clinic-based settings where children with acute malnutrition need to be identified and referred for treatment. However, when measurements done with the wide MUAC tape were corrected for the measurement bias, the sensitivity of the wide MUAC tape improved. In fact, the wide MUAC tape identified slightly more children with moderate acute malnutrition defined as MUAC <12.5 cm. However, some discrepancy remained. Namely, 4 children with WLZ < −2SD were identified as moderately acute malnourished by the wide MUAC tape, but not the standard tape, and 3 children with low WLZ were identified as moderately acute malnourished by the standard tape, but not the wide MUAC tape. Thus, after correction, the wide MUAC tape had the same rate of identifying low MUAC as the standard tape. It is known that MUAC and WLZ do not always overlap, which is why Grellety and Golden have suggested that WLZ and MUAC should be used independently to diagnose acute malnutrition. 13
A limitation for the present field study was that the wide MUAC tape was introduced after anthropometrists had already gained experience with the standard MUAC tape. This may also explain why this team of anthropometrists and anthropometry assistants perceived the standard MUAC tape as more precise, even though the data showed a tendency in the opposite direction. It has to be noted that the present field testing was integrated into a randomized controlled trial with rigorous data collection and supervision. Standardization sessions were implemented frequently; after each session, results were discussed with the anthropometry team and retraining was conducted, if needed. Thus, the current field test was implemented in a research context, and further field tests should be completed in programmatic settings where community health workers often are trained and supervised to a lesser extent. The wide MUAC tape should also be compared in settings of higher rates of severe acute malnutrition to ensure that vulnerable children are identified and referred for treatment appropriately with this new tool. Indeed, the field team’s feedback and suggestions to produce the wide MUAC tape with a softer material were taken into consideration in subsequent product modifications to design and material by the development team at Intellectual Ventures Laboratory Global Good Fund, and more field tests are planned with the new prototype.
An additional weakness of the present study is the lack of a true gold standard. Thus, it is possible that the mean MUAC in the present study population as measured by the wide MUAC tape was indeed correct and would not need to be corrected by 0.4 cm. However, we considered the standard MUAC measurements as the gold standard only because a standard 0.7 cm-width tape was used in the WHO Multicenter Growth Reference Study and the current recommended international growth standards and the recommended cutoffs for moderate and severe acute malnutrition are based on measurements with a standard-width MUAC tape. 1,3,9 Thus, to allow the adoption of an innovative tool like a 5.0-cm-wide MUAC tape, it seems important that it can be used in the context of these same growth standards and cutoffs. Future field tests with slightly revised prototypes will be needed to evaluate this further.
Conclusion
The present field testing was the first to assess an innovative wide-width MUAC tape among young children living in rural communities of Lao PDR. This low-cost tool allowed for simplification of field measurement techniques by estimating the midpoint of the upper arm instead of measuring it. The precision was good, and feedback from the field team was taken into consideration for further product development. Future field tests will be needed to test the accuracy and precision of this modified prototype and ensure that the wider tape reliably identifies children with severe and moderate acute malnutrition.
Footnotes
Authors’ Note
S.Y.H., G.M.H., M.A.B., C.A.D., and S.K. designed research, G.M.H., M.A.B., and B.B. conducted research. D.B. and T.M. provided essential material. G.M.H. and C.A.D. analyzed data. S.Y.H. wrote paper. S.Y.H. had primary responsibility for final content. All authors have read and approved the final manuscript. All data are available at Open Science Framework: ![]() .
.
Acknowledgments
The authors thank K. Ryan Wessells (University of California, Davis) and Kenneth H. Brown (Bill & Melinda Gates Foundation) for technical support throughout the whole project. The authors appreciate valuable comments on the manuscript by Victoria Hunt (Intellectual Ventures Global Good Fund).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.B. and T.M. work for the Intellectual Ventures Global Good Fund. The spouse of S.Y.H. works for the Bill & Melinda Gates Foundation, which supported other aspects of this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided by the Bill & Melinda Gates Foundation Trust through the Intellectual Ventures Global Good Fund I, LLC (201700276). Other aspects of the Lao Zinc study were funded by the Mathile Institute for the Advancement of Human Nutrition and Nutrition International (formerly the Micronutrient Initiative; 10-1347-UCALIF-07) and the Bill & Melinda Gates Foundation (OPP1134272).
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.