
Abstract
Background:
Understanding the context of infant and young child feeding (IYCF) is recognized as essential for designing appropriate complementary feeding interventions.
Objective:
Our objective was to study household IYCF behaviors in 2 districts in southern and northern Ghana to identify opportunities to improve existing nutrition programs.
Methods:
We interviewed 80 caregivers of children aged 6 to 23 months using ethnographic methods, including free listing, guided discussions and cognitive mapping techniques, and 24-hour dietary recall. Descriptive statistics and thematic content analysis were used to analyze quantitative and qualitative data.
Results:
In both settings, children’s diets were predominantly maize based. Fish, the main animal source food, was consumed daily but in very small quantities. Milk was consumed by only a few children, in tea and porridge. Fruits were seldom consumed. Household food production did not meet requirements, and the markets were heavily relied on for staples and other key ingredients. Most caregivers demonstrated basic knowledge and understanding of key health and nutrition concepts. Barriers to optimal child feeding identified were lack of money to purchase the nutritious foods recommended for children, seasonal food insecurity, and some caregiver beliefs, practices, and nutrition knowledge gaps. Positive contextual features include caregiver recognition of the dietary needs of young children and commitment to provide foods to meet these needs.
Conclusion:
Our findings suggest that complementary feeding in these rural settings can be improved through reinforcement or modification of strategic components of local health and nutrition education in light of existing barriers and enablers to optimal IYCF.
Introduction
Childhood undernutrition remains a major public health problem in much of the developing world, contributing to high prevalence of stunting, poor cognitive development, increased morbidity, and 35% of deaths of children younger than 5 years. 1 For most of the past 2 decades, prevalence of stunting in Ghana has hovered around 30%, leading to the country’s inclusion in the list of 36 high-burden countries for malnutrition. 2 The 2014 Ghana Demographic and Health Survey shows a reduction in stunting from 30% in 2008 to 19%, 3,4 suggesting some gains in efforts to address the problem. Despite these gains, poor feeding practices and inadequate diets still persist. Only 13% of children aged 6 to 23 months meet the criteria for minimum acceptable diet, with infants aged 6 to 11 months being the most vulnerable. 4 Furthermore, marked regional and socioeconomic variations in both stunting and optimal infant and young child feeding (IYCF) remain, as shown in other countries. 5 –7 There is, therefore, a need to better understand the contexts of IYCF in order to develop effective strategies to improve the nutrition of children, especially in resource-poor settings.
Formative research is recognized as a tool that provides context-specific data to inform evidence-based decisions for nutrition and public health interventions. 8 –11 It is particularly valuable in identifying suitable interventions or potential barriers that are likely to affect the success of an intervention.
In line with this, the Global Alliance for Improved Nutrition (GAIN) has supported the development of a formative research tool, the “Focused Ethnographic Study for Infant and Young Child Feeding 6 to 23 Months: Behaviors, Beliefs, Contexts, and Environments” (FES-IYCF) to identify key context factors that influence IYC feeding practices, 12 and has been applied in different country settings for GAIN’s IYC nutrition programming. 13
The GAIN and the US Agency for International Development (USAID) have since conducted collaborative FES-IYCF research in conjunction with dietary intake surveys and Optifood linear programming analysis 14 to identify context-specific food-based recommendations for IYC diets in Kenya 11,15 and Ghana (Armar-Klemesu et al [unpublished data] note1, Brouwer et al [unpublished data] note 2). This article reports on the FES carried out in 2 rural districts in Ghana to identify the main constraints and facilitators to optimal IYCF. As a result of stakeholder consultations (Lee, personal communication [note 3]), a secondary objective was to identify areas where the community-IYCF (C-IYCF) Counselling Package 16 messages could be made more locally relevant and strengthened for maximum impact.
Materials and Methods
The Study Settings
The studies were conducted in Karaga District in the Northern Region, and Gomoa East District in the Central Region of Ghana. Karaga District, one of the newest administrative districts in the northern region, is in the USAID Feed the Future program area in the northern regions. Gomoa East was selected as a southern comparison and on the basis of it also being one of the newest administrative districts in the Central Region. The districts are situated in 2 distinct agroecological zones, which may influence agriculture, food availability, and consumption, including IYCF.
Karaga District is in the Guinea Savannah vegetation zone, with a single farming season and agriculture employing 95% of the workforce. The major traditional crops include maize, sorghum (guinea corn), millet, groundnuts, cowpeas, cassava, rice, and yam. As in other parts of northern Ghana, seasonal food insecurity is a major problem mainly due to the erratic rainfall pattern as well as other factors such as poor storage, high postharvest losses, and high food prices during the lean season. The Dagomba are the dominant ethnic group and the majority are Muslims (83% compared to 13% for traditionalists and 4% for Christians). 17
Gomoa East District spans 2 ecological zones (dry coastal savannah and moist semi-deciduous forest), experiences 2 rainfall seasons, and employs about 63% of the active population in agriculture. Major crops include maize, cassava, yam, plantain, vegetables (tomatoes, pepper, garden eggs, and okra), and fruits (citrus, pineapple, pawpaw, and banana). Although classified as a food basket area, chronic food insecurity is prevalent among the poor and vulnerable due to limited production resulting from limited access to land, an unpredictable rainfall pattern, and lack of access to financial capital to support farming activities. The Gomoa are the dominant ethnic group and the majority are Christians (82% compared to 11% for Muslims and less than 1% for traditionalists). 18
Karaga is the more disadvantaged of the 2 districts with very poor infrastructure (including poor water and sanitation facilities, transportation, and market infrastructure) and lower literacy rates (22% of persons ≥11 years described as literate compared to 82% in Gomoa East). 17,18
Study Participants
The study targeted caregivers of infants and young children aged 6 to 23 months, divided into 4 groups: 6 to 8 months, 9 to 11 months, 12 to 23 months (breastfed), and 12 to 23 months (non–breastfed). Forty caregivers were selected from each district for the study. A multistage cluster randomized design was used to select the communities and participants included in the survey (note 2). At the first stage, 1 subdistrict was randomly selected from each district (Gomoa Buduatta in Gomoa East District and Karaga in Karaga District). The communities in the selected subdistrict were then clustered geographically into 3 clusters comprising 10 to 15 communities, representing the north, central, and south locations within the subdistrict. The sampling frame of all listed households with children aged 6 to 23 months was then divided into subframes to correspond with the age-groups of interest. Within each subframe, the required number of eligible children was randomly selected from each cluster for the dietary survey (note 2). For the FES, 2 to 3 communities were randomly selected from each of the 3 clusters in each subdistrict, and primary caregivers were randomly selected from the dietary survey census database by filling a sampling grid based on clusters and child age and breastfeeding status to cover the 4 subgroups noted above. Those who had already participated in the dietary survey were excluded. The caregivers, categorized as key informants (n = 8 per district) and respondents (n = 32 per district), were interviewed in their homes by trained qualitative interviewers. The sample sizes are predetermined to be adequate for the FES methodology 12 as applied in previous studies. 13,15
Data Collection and Analysis
The FES-IYC tool is based on a cultural–ecological framework that ensures collection of data on all the domains that have been shown to influence IYC feeding. The FES-IYC manual 12 gives a detailed description of the structure of the FES (also summarized in Table 1). The FES data collection and analysis are structured into protocols, each consisting of a set of individual modules focusing on specific areas of interest in understanding IYC feeding practices and child health and development. The modules were administered through in-depth one-on-one interviews that employ open-ended and guided questions as well as a precoded structured questionnaire. Some modules use formal ethnographic techniques including “free listing” or rating and ranking tasks to elicit respondents’ cognitive or cultural models. 19,20 Data collection was conducted in 2 phases. Phase I involved interviews with caregiver key informants, the results of which were used to fine-tune the modules for the phase II of interviews with caregiver respondents, which are designed to confirm and expand the initial picture that emerged from the key informant interviews. Interviews ranged 2 to 3 hours and were often conducted in 1 session.
Summary of FES-IYC Modules and Their Purpose.
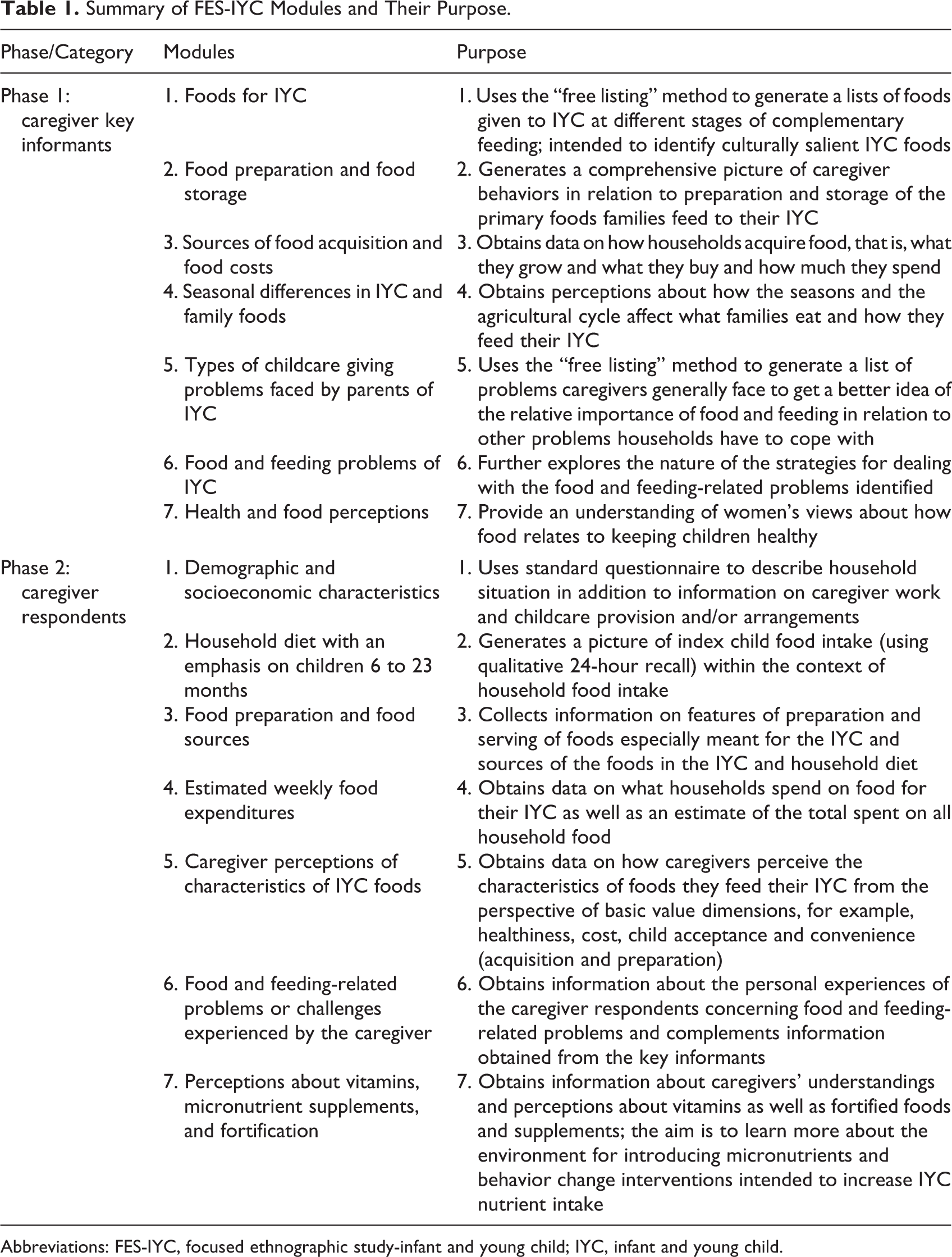
Abbreviations: FES-IYC, focused ethnographic study-infant and young child; IYC, infant and young child.
Demographic and socioeconomic data were analyzed using Stata 12 21 and other quantitative data using Excel spreadsheets. Thematic analysis of the transcribed and translated recordings of the interviews followed basic principles of qualitative text analysis. 22 The findings were initially organized and presented following the FES-IYC cultural–ecological framework, 12 in the study of Armar-Klemesu et al (note 1). For the purposes of this article, relevant themes relating to barriers and facilitators to optimal IYC in the corpus of data generated by the FES were then identified and coded. The study was approved by the institutional review board of the Noguchi Memorial Institute for Medical Research. Informed consent (written and thumb printed as appropriate) was obtained from all study participants. Permission was also granted by the Ghana Health Service.
Results
Demographic and Socioeconomic Characteristics
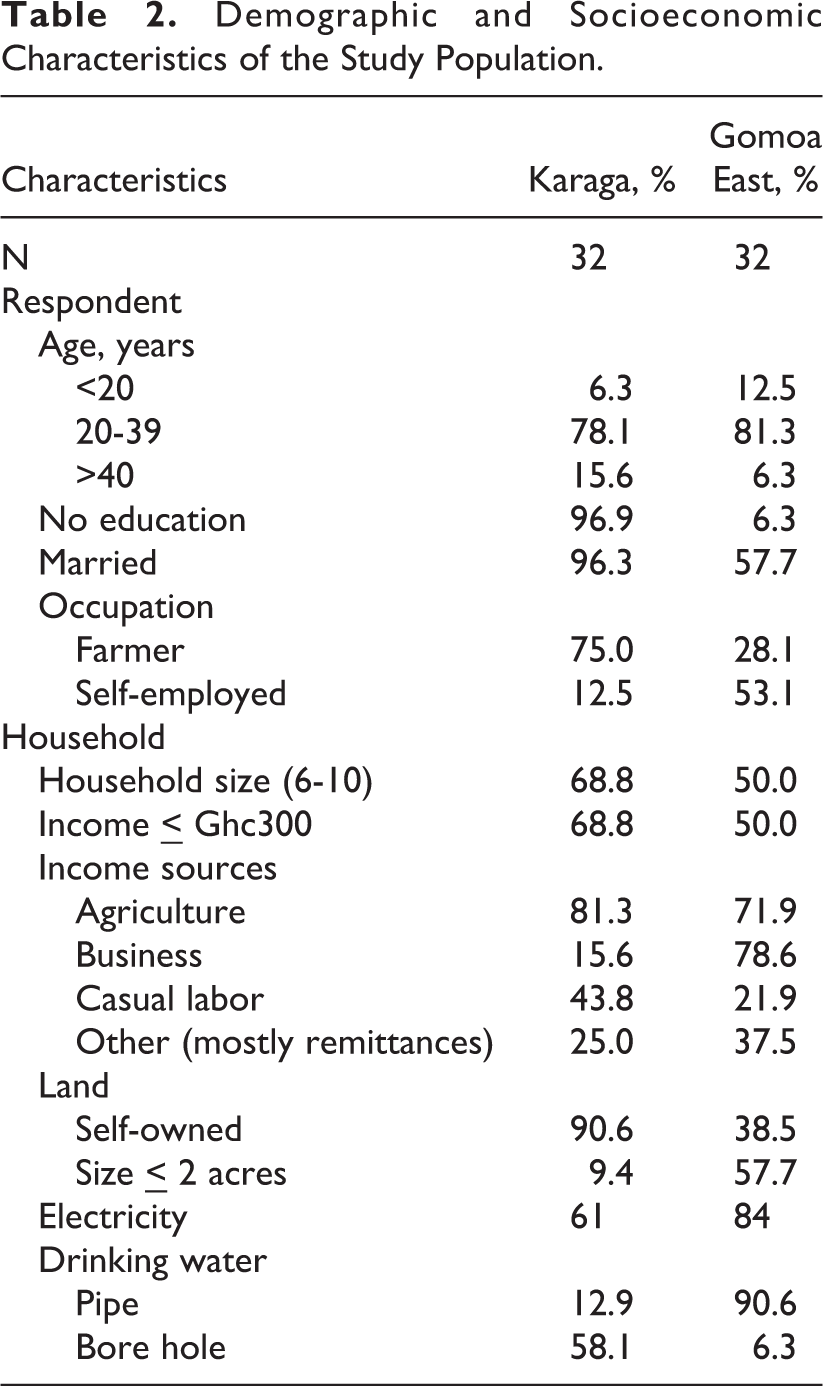
Table 2 shows the key demographic and socioeconomic characteristics of the 64 caregiver respondents who participated in phase 2 of the study. The majority of respondents were aged between 20 and 39 years. Respondents from the 2 districts differed in that in Karaga, most were married but had no formal schooling, were engaged in agriculture for employment and had access to agricultural land that was owned, and most lived in larger households. In contrast, in Gomoa East, fewer respondents reported to be married, most had some education, and more reported to be self-employed drawing income from business, with fewer owning land.
Demographic and Socioeconomic Characteristics of the Study Population.
Characteristics of the IYC Diet
The concept of core foods has been used to describe the differences among cultures or societies in the foods that are the basis of preferred local diets. 23 We used the caregiver key informant free list of foods fed to IYC (ie, culturally salient IYC foods), and the caregiver respondent 24-hour recall of foods actually fed to the index child to generate the core foods that characterize the IYC diet in Karaga and Gomoa East, based on the frequency of mentions and proportion of children consuming food, respectively. Generally, the cultural core foods corresponded closely with the foods reportedly consumed. However, some cultural core foods were hardly consumed and conversely some foods not mentioned as part of the cultural core were consumed by a considerable proportion of IYC. From this observation and applying similar criteria described in Goode, 23 the foods presented in Table 3 were considered to form the IYC core in Karaga and Gomoa East.
Core Foods for Infants and Young Children in Karaga and Gomoa East Districts.
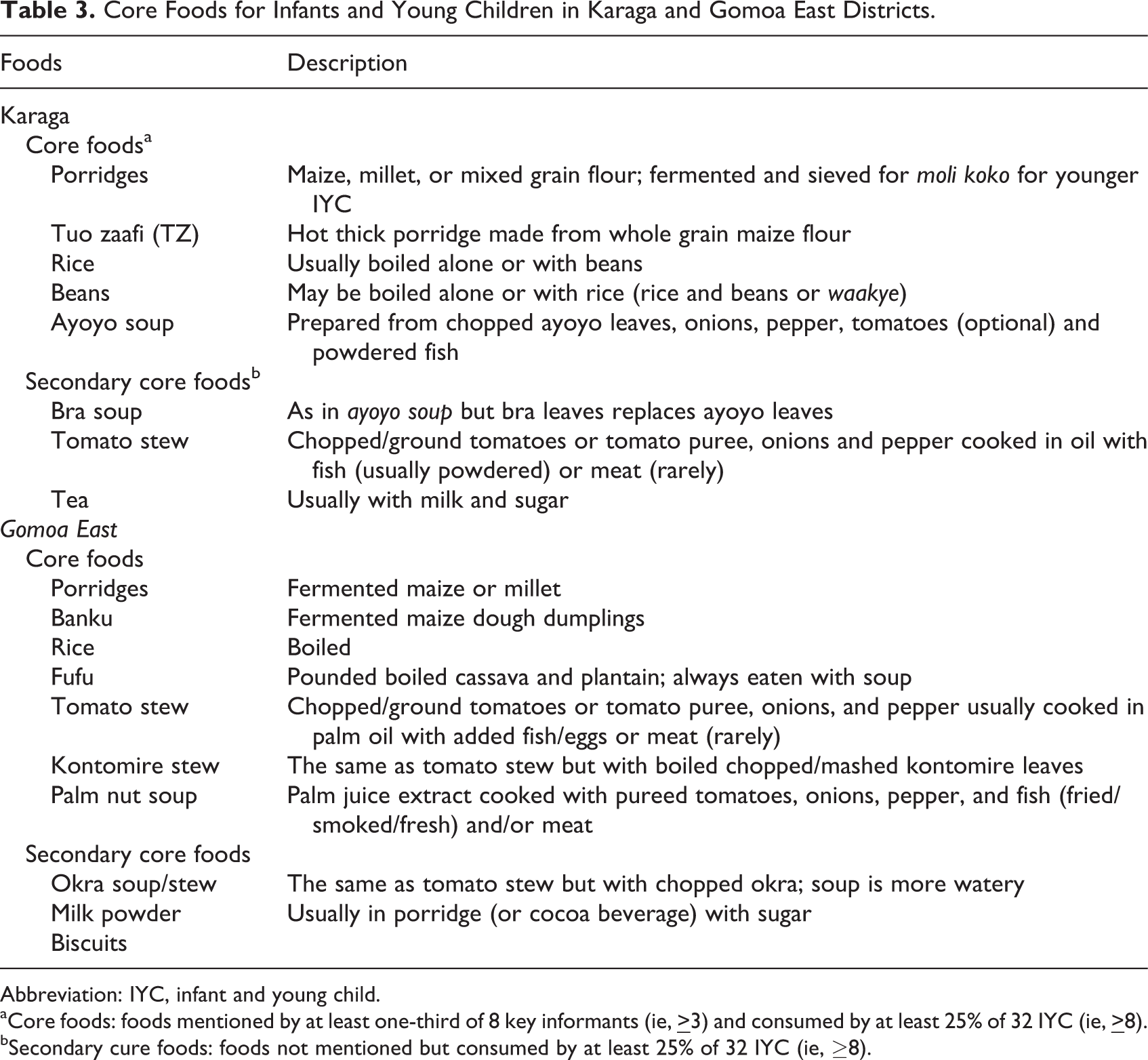
Abbreviation: IYC, infant and young child.
aCore foods: foods mentioned by at least one-third of 8 key informants (ie,
bSecondary cure foods: foods not mentioned but consumed by at least 25% of 32 IYC (ie, ≥8).
Cereals and especially maize-based foods are the predominant core foods in the IYC diet in both locations. Porridges are consumed on a daily basis by nearly all children, whereas most other core foods enter the IYC diet at about 1 year of age. The core staples are normally paired with vegetable soups and stews in which fish is the predominant and often the only animal source ingredient, especially in Karaga. Notable differences in core IYC foods between Karaga and Gomoa East districts are the variety and types of porridges in Karaga, whereas Gomoa East has somewhat more variety in both the staple dishes (ie, inclusion of cassava and plantain in the form of fufu) and the accompanying soups and stews. The variety and forms of fish consumed in Gomoa East are also greater and include smoked mackerel, herrings and tuna, frozen fish, and dried fish powder (used only in recipes specially prepared for IYC). This is in contrast to Karaga where dried powdered anchovies or herrings are the main form in which fish is generally used even for household food preparation. Milk and fruits were not listed as foods fed to IYC. Milk was only consumed in tea in Karaga and in porridges in Gomoa East by about a third of IYC. Consumption of fruit was seldom reported in either district.
Identifying the Barriers and Facilitators to Optimal IYC Feeding
Three main themes contributed to the barriers and facilitators to optimum IYC feeding: food acquisition and preparation, seasonal fluctuations in food availability, and caregiver knowledge, beliefs, and practices.
IYC food acquisition and preparation
Three main barriers to acquiring and sourcing foods for IYC were identified in both Karaga and Gomoa East. First, household dependence on own production for its food needs was limited by low productivity and seasonal fluctuations in staple reserves. Secondly, some key ingredients used in preparing the soups and stews that accompany the staple dishes are solely purchased. These include fish, red palm oil, cooking oil, canned tomato puree, and bouillon cubes. Tea, cocoa beverages, sugar, and powdered milk for the porridges and beverages fed to the IYC are also purchased, often in small single-use packets or small repackaged quantities knotted into polythene bags, reflecting caregivers’ purchasing patterns.
These findings suggest that having cash in hand is vital for IYC feeding and more importantly for implementing IYC feeding recommendations. The cognitive mapping exercise carried out by caregivers to rate common IYC foods across selected value dimensions (Table 4) showed that foods rated as the healthiest were generally also rated least accessible due to cost. Many caregivers were aware that the plain porridge (koko) provides insufficient nourishment to their infant, yet they consider it unaffordable to add milk to the porridge, or to add meat to food, as illustrated by this Karaga caregiver:
Caregivers’ Ratings of Foods They Feed Their IYC.a,b
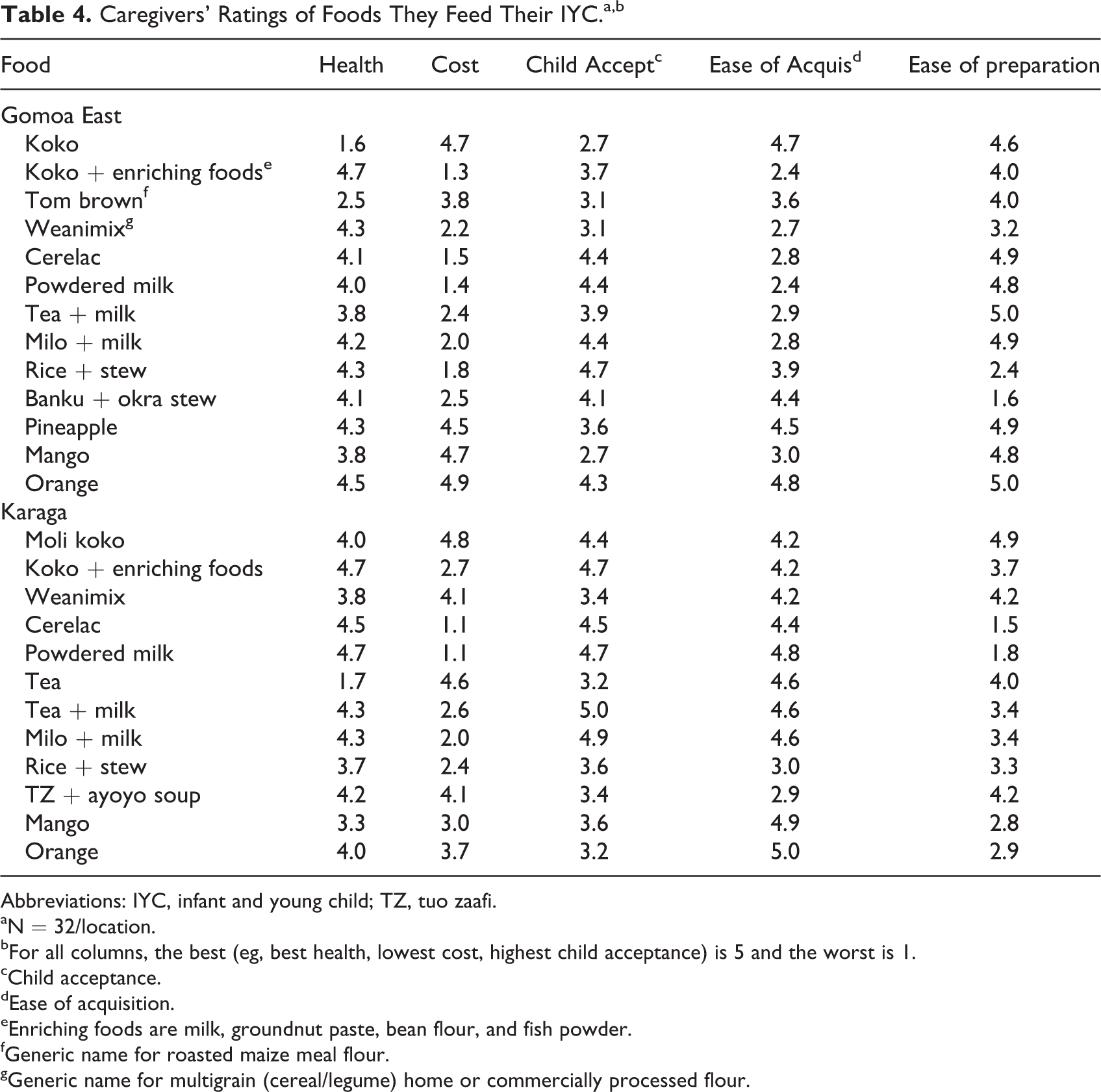
Abbreviations: IYC, infant and young child; TZ, tuo zaafi.
aN = 32/location.
bFor all columns, the best (eg, best health, lowest cost, highest child acceptance) is 5 and the worst is 1.
cChild acceptance.
dEase of acquisition.
eEnriching foods are milk, groundnut paste, bean flour, and fish powder.
fGeneric name for roasted maize meal flour.
gGeneric name for multigrain (cereal/legume) home or commercially processed flour.
We are told what to feed our children with by health workers at times when we visit them. But the fact is if you don’t have money, what they say will not really count. You will just feed the child on what is affordable and available. If I had money, I would have prepared the food better for her to eat. I will buy more sugar and Nido (powdered milk) and add to the moli koko for her to eat. But because I don’t have, I add only sugar and even with that it is not always that I’m able to buy. Every child likes porridges especially if there is milk in it but I can’t afford the milk.
Cost or access to money was therefore considered a very important determinant of what can be provided and may be the most significant barrier to wider use of several key nutrient-dense foods in the IYC diet.
Caregivers’ strategy for coping with lack of cash was to borrow or buy food on credit from vendors within their neighborhoods, the latter being more evident in Gomoa East than in Karaga. However, in both locations, foods bought on credit are mainly foods that caregivers claim children prefer, such as rice and stew (often purchased ready prepared), and milk and sugar, which make porridges and beverages more nutritious and acceptable.
Two main findings relating to IYC food preparation were identified. First was the recognition by caregivers that infants and young children have different dietary needs compared to older children and adults. In Karaga and Gomoa East, some foods were specially prepared and fed to IYC that were not consumed by other family members. In Karaga, these included moli koko (unspiced fermented porridge), rice and stew and beans with palm oil, and in Gomoa East, these included rice or soft banku and stew prepared with powdered fish or eggs. Caregivers’ detailed accounts of how foods are specially prepared for IYC show distinct differences from those prepared for the whole family. Moli koko, unlike family koko, is prepared from sieved, fermented, sun-dried maize flour, and family foods such as tuo zaafi (TZ), banku, or rice are cooked to a softer texture for IYC.
Second, caregivers recognize that child acceptance of food is facilitated by appealing to their senses of taste, sight, and smell. For most caregivers, it is a combination of the key attributes of pleasant or sweet taste, smooth or soft textures, and colorful visual appeal that make food acceptable, and achieving these through food preparation processes, and ingredients used was considered important. When available and affordable, meat, fish, and eggs are added to food to enhance taste, visual appeal, and as incentives to encourage food acceptance. Bouillon stock cubes are also used to enhance the taste of stews and soups, sugar and milk to make beverages and porridges more acceptable, and red palm oil to make food attractive.
Effects of seasonality on IYC feeding and IYC diets
Seasonal fluctuations in own staple reserves and vegetable ingredients and the need to access these from markets had a dual impact: increases in cost of out-of-season foods and transport to acquire them further put additional strain on limited household food budgets. Despite the fact that different degrees of market accessibility were reported, many of the coping strategies for household diets described by caregivers in Karaga and Gomoa East were similar and suggested there would be implications for the diversity and nutritional quality of the diet.
Three main findings were identified with respect to lean season adjustments made to food preparation and consumption. First is the substitutions of more readily available but less preferred ingredients, such as gathered “wild bra” for bra leaves in Karaga and in Gomoa East, and gathered dandelion is substituted for kontomire and kokonte (dried cassava flour dumpling) for fresh cassava and plantain fufu. Second is the alterations made to the fundamental structure of common dishes. In Karaga, TZ may be eliminated and maize flour limited to thickening soup dishes or other “one pot meals.” In Gomoa East, where dishes are more elaborate and lack of money may be more of a challenge, this may be the “dry” consumption of staples without the usual soups and stews. This is a radical adjustment that omits vegetables, oils, and fish, the most nutritious ingredients. Third, in extreme circumstances, caregivers in both locations reported reductions in meal frequency and portion sizes. The impact of seasonality and its cost implication on food is described by this Karaga caregiver: When it comes to foods that are cheap, TZ is less costly because we produce maize on the farm. Ayoyo and bra too are cheap at this time of the year when the rains are still coming. However, when it gets to the dry season, we stop cooking these soups because they become very expensive and if you want to cook them, you would have to buy the ingredients.
The role of caregiver knowledge, beliefs, and practices
Two findings relating to this theme were identified. First is caregivers’ ideas about the attributes of healthy IYC foods and diets which include a sense of the importance of balancing dietary components, a notion of the preventive power of certain foods, and the ability of certain foods to supply energy and support growth, in the view of caregivers by “building” or “making blood.” The specific foods mentioned in connection with these attributes varied between Karaga and Gomoa East, but the beliefs are broadly consistent with contemporary nutrition knowledge and recommendations. Leafy vegetables, fish, and eggs, for example, are believed to “give” blood which ensures good growth and health in children and makes them active and not prone to sickness. Similarly, “heavy” foods such as staple dishes with accompaniments (eg, TZ and ayoyo soup, rice, and stew) are thought to build strength and promote growth. A second finding is the awareness of the importance of the contextual elements of IYC feeding which was more evident among Gomoa East caregivers, who cited child-centered feeding practices, such as a congenial feeding environment and devoting time and attention during feeding as important to promoting child acceptance of food. Among Karaga caregivers, however, the idea that the feeding environment might play a role in child food acceptance did not emerge spontaneously from the discussions.
Despite these positive attributes, 3 areas of concern relating to beliefs, knowledge, and practices that may limit the nutritional quality of IYC diets were identified. First is a strongly held belief, more evident in Karaga than in Gomoa East, that it is unwise to feed children “heavy” foods before they are 1 year old or begin to walk. The reason offered was that feeding foods such as TZ, fufu, and banku, during this period will retard the child’s ability to walk. The following narrative from the mother of an 8-month-old child in Karaga is illustrative: In our locality, we believe that a child who is less than 1 year must not eat TZ or fufu…our elders say that, when you give a child such food at that age, it retards the child’s development. The child does not walk early as she would have.
A third area of concern around gaps in knowledge, particularly among Karaga caregivers, is the limited specific knowledge relating to vitamins and food fortification. Although Karaga caregivers are well informed about the health-giving properties of fruits and vegetables for instance, the majority were unfamiliar with the term “vitamins” and none could identify any individual vitamin. Among the small minority who recognized it, vitamins were likened to a medicine that can restore appetite and IYC health. By contrast, more than two-thirds of Gomoa East caregivers were familiar with the term “vitamin,” although they similarly associated vitamins with treatments prescribed by doctors and nurses. Gomoa East caregivers were also more familiar with the concept of fortification of foods with vitamins to improve their nutritional value, with about 50% showing awareness compared to only 10% of Karaga caregivers.
Discussion
Our findings corroborate those of other studies 8 –11,15 that underscore the importance of the role of context in designing IYCF interventions. However, as in the FES in Kenya, 11,15 these studies not only identified 2 major sets of barriers and challenges to the adequacy of IYCF, they also revealed several positive elements of caregiver beliefs and behaviors, presenting opportunities to adapt or introduce context appropriate interventions to improve IYCF in these distinct agrarian Ghanaian populations. The primary challenges were the limited accessibility of nutrient-dense foods due to cost which was further compounded by limited availability and access during the lean season, certain beliefs that may limit provision of nutrient-dense foods especially in the second half of infancy and knowledge gaps that present missed opportunities for increased nutrient intakes from fruits and potentially from fortified foods. Our findings also suggest that compared to Gomoa East, Karaga may be at a higher risk of IYCF inadequacy, as has been observed for the northern region in general. 6
Notwithstanding the significant barriers to IYC dietary adequacy, the FES findings indicate there may be a positive environment for the adoption of several nutrition-specific interventions that can be supported by behavior change communication (BCC) messages to increase consumption of nutritious IYC foods. Opportunities to build on positive practices include a cultural commitment to the concept of specially prepared foods for IYC and adding value to IYC foods. Further, BCC may appeal to caregiver desires to feed their children well and the importance placed on child acceptance of foods through improving taste, color, and texture of IYC foods.
Implications for Nutrition-Specific Actions
Nutrition-specific actions should prioritize 2 key IYCF strategies: reinforcing the promotion of nutritionally improved IYC porridges and promoting increased use of existing nutrient-dense foods in the IYC diet with more innovative BCC messaging channeled through Ghana’s C-IYCF counseling package, the main vehicle for nutrition education in the rural setting.
Porridges are central in the IYC diet and are consumed on a daily basis by the majority of IYC. As the first complementary food fed to infants for much of the first year, the plain porridges (koko) have historically been linked to malnutrition in young children. 24 Despite awareness of their poor nutritional quality, they are preferred because they are perceived to be cheap and convenient (note 1). 25 Recognition of the importance of porridges in the IYC diet is demonstrated by efforts made over the years at improving their nutritional quality. Addition of nutrient-dense foods such as milk, groundnut paste, fish powder, and palm oil to porridges is a widely promoted strategy. Our findings show that mothers recognize the healthiness value of adding these foods, as shown by past evaluations of their impact, 26 and there may still be value in renewed BCC messaging that addresses other motivations in addition to the health dividend, including improved child acceptance of foods. The culture of adding value to porridges also offers an opportunity to use specific interventions including the use of fortified foods as ingredients and, when appropriate, the introduction of micronutrient powders or food supplements such as KOKO Plus, which is a soy-based product, undergoing research to assess effective distribution channels in Ghana. 27
Another prominent strategy is the promotion of industry-manufactured fortified complementary foods, as, for example, Weanimix, (a 4:1 cereal–legume blend) that is being distributed by the Ministry of Health and United Nations Children’s Fund (UNICEF) dating back to the late 1980s. Our study and others, 13,25,28 however, suggest that Weanimix-type porridges are not much patronized and do not feature much in IYCF in low-income households due to their limited availability and cost. Indeed according to Pelto et al. 13 Weanimix-type porridges (whether made at home from recipes, or from mixes obtained from clinics, or purchased as commercial products) were not well regarded, as they did not have the qualities women were interested in; “they were seen as moderately healthy, not inexpensive and most seriously, carrying a heavy burden of time costs, including the time required to secure and prepare them and presenting challenges of storing them safely.” Nevertheless promotion of these blends should be maintained, especially in the Northern Region. Nevertheless promotion of these blends should be maintained especially in the Northern Region (and generally the northern regions), where a potentially more receptive environment exists since Karaga caregivers, in contrast to their Gomoa East counterparts, rated Weanimix more favorably (Table 4). Additionally, the presence of fortified beverages in the IYC diet suggests a place for other types of fortified foods such as the fortified instant cereal/legume porridge produced by a local agro-processing company. 29
The national IYCN program, with innovative BCC messaging, offers opportunities for promoting increased consumption of existing nutrient-dense foods in the IYC diet. At the district level, the community-based health planning and services program 30 is the main link with families and the C-IYCF counseling package is the main conduit for IYCF messages. Based largely on generic guidelines developed by UNICEF for Africa, 16 the C-IYCF counseling package has been adapted to specific settings in Ghana and relies on the communication of key messages in a manner consistent with existing practices and culture. For the most part, the C-IYCF materials are highly appropriate, and their emphasis is consistent with the IYC feeding landscape of Karaga and Gomoa East revealed in our studies. However, some specific observations were made that may be considered by GHS and its partners to further strengthen the IYCF messages and thereby increase their applicability and effectiveness in the context of these and similar settings as discussed below.
Ensuring timely introduction of solid and semi-solid foods
There is an urgent need for targeted BCC messaging to address the prevalent belief that too early introduction of solid or “heavy” foods will retard physical development, manifesting as failure to walk. The concern here is that since these foods are usually consumed with soups and stews, it seems plausible that consumption of some nutritious ingredients is being delayed. Specific assurances about the safety of family foods particularly for 7 to 12 months old children who are most likely to be adversely affected by this proscription will need to be introduced. The finding that late introduction of complementary foods is associated with non-Christian mothers, such as the predominantly Muslim Karaga caregivers, in Ghana and not other West African countries with similar large Muslim populations 6 is instructive and an indication that this culturally embedded belief can only be effectively addressed with the engagement of the wider community, especially fathers, grandparents, community elders, and religious leaders.
Animal source foods
The C-IYCF counseling tools describe the importance of adding animal source foods to the IYC diet using meat, chicken, fish, liver, eggs, milk, and milk products as examples. However, our results indicate that currently fish and powdered milk are the only items consumed by IYC with any frequency. Notably meat was virtually absent from both IYC and family diets. This finding is corroborated by other studies that have identified major constraints on the use of animal source foods in rural communities and despite the ubiquity of fish in the IYC diet, amounts consumed ranged from only 1.5 to 6 g per day (note 2). 31,32 Collectively, these studies indicate that fish may be the most viable animal source food to promote and adapting the C-IYCF messages to put specific emphasis on fish in the many forms that it takes in the local diet may present a more attainable option for caregivers in Karaga, Gomoa East, and similar settings and achieve results in the immediate term.
Modifying family foods to increase nutrient density of IYC diets
The cultural recognition of “special foods for infants” is a relevant concept for improving IYC diets. Dewey and Brown 33 have hypothesized that it is easier to introduce IYC-specific interventions if families already have a concept of special infant foods. Our studies show that once IYC are introduced to family foods, soups and stews (the main sources of vegetables and fish) become integral parts of the IYC diet. The common practice of separating out the IYC portion during the cooking process offers an opportunity to promote the habit of preparing an IYC portion with additional fish and mashed (rather than chopped) ingredients such as leafy vegetables by including specific guidance in the C-IYC materials for increased feeding frequency or portion size. Behavior change communication will need to address the reasons why IYC particularly need this nourishment by building on the concept of “special IYC foods” already held by caregivers.
Consumption of fruits
Community-IYCF messages for the 12- to 24-month age-group include specific emphasis on consuming vitamin A–rich fruits and vegetables. Although IYC regularly consume dark green leafy vegetables when introduced to family foods, regular consumption of fruit is much less common. In our study, caregivers rated fruit favorably on all dimensions suggesting a potential receptive environment for increasing fruits in the IYC diet. Community-IYCF messages could expand the importance of fruits beyond the therapeutic use by adding language about the benefits of daily consumption, incorporating local ideas about the power of fruits but linking them to their preventive properties in a similar fashion as the western concept of “an apple a day keeps the doctor away”.
Responsive feeding and care practices
The C-IYCF messages place strong emphasis on feeding children in a stress-free and conducive environment. The importance of these contextual elements of IYC feeding is well documented 34 –36 and was more evident among Gomoa East caregivers compared to their Karaga counterparts. Although mothers who have to manage dual roles as caregivers and income earners may struggle to devote the time they would like to feed their IYC, awareness raising of these contextual elements of IYC feeding, especially among caregivers in Karaga, as a means of ensuring adequate food intake particularly during the transition period to family foods needs to be emphasized.
The effectiveness of the above nutrition-specific actions can further be enhanced if the problem of poverty and lack of money are also addressed. The Livelihood Empowerment Against Poverty (LEAP) cash transfer program is Ghana’s flagship program of the National Social Protection Strategy which was launched in March 2008, reaching 71 000 households in all 10 regions as of June 2013. 37 Expansion and better targeting of beneficiaries under LEAP may support increased accessibility of nutrient-dense foods in local markets. Impact evaluation reports suggest that LEAP has enabled poor families to meet their food needs and allowed for improvements in the diets of beneficiaries, who are now able to prepare meals of better quality, cooking with fish, oil, and Maggi (seasoning), without incurring much debt. 37 This clearly resonates with our findings and recommendations.
Finally, concerted efforts must be made to engage all sectors in developing strategies and activities to broaden the audience for nutrition messages beyond mothers, who can more effectively take actions to improve child nutrition if they are supported by other segments of the rural society.
Conclusion
The results from these studies provide a holistic perspective from the point of view of caregivers on their beliefs and practices around IYCF, providing insights into how this might be improved within the current context of IYCF in Karaga and Gomoa East and similar rural settings. Despite the obvious restrictions for caregivers in improving the adequacy of IYC diets due to poverty and seasonal food scarcity, we have identified several culturally specific issues that could be addressed through innovative BCC messaging and contextualization of the C-IYCF guidelines. These studies also highlight the need to engage relevant segments of rural society and for other interventions, such as social safety net programs to contribute to improved IYCF.
Footnotes
Authors’ Note
M. A. K. and A. T. designed the study. M. A. K., S. O. M., and S. Z. A. led data collection. M. A. K., S. O. M., S. Z. A., and J. L. analyzed the data and wrote the background reports. All authors contributed to interpretation of results. M. A. K. and C. H. drafted the manuscript and all authors reviewed, contributed to, and approved the manuscript.
Acknowledgments
The authors wish to thank Professor KA Koram and the Office of Research Support of the Noguchi Memorial Institute for Medical Research for administrative and logistics support for the study. The authors thank Bonnie McClafferty (GAIN) for the support and opportunity to apply the Focused Ethnography Study (FES) methodology in another setting and context. The authors are grateful to all those who contributed in diverse ways to the success of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was made possible by the generous support of the American people through the support of the Office of Health, Infectious Diseases and Nutrition, Bureau for Global Health, US Agency for International Development (USAID) under the terms of Grant No. GHA-G-00-06-00002 to GAIN. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the US Government.