
Abstract
Objective:
There is a significant evidence gap on the long-term educational benefits of longer breastfeeding in low- and middle-income countries. We estimated the association between duration of (any) breastfeeding and educational outcomes of Indian children.
Methods:
We used regression analysis to examine the association between the length of breastfeeding (in months) and future education outcomes on the basis of 2 data sets: (1) data from a follow-up survey known as the Andhra Pradesh Children and Parents Study (APCAPS, 2003-2005) of 1165 children aged 13 to 18 years from a controlled nutrition trial originally conducted in South India during the period of 1987 to 1990; and (2) nationally representative data from the India Human Development Survey (IHDS-2, 2011-2012) of 6121 children aged 6 to 12 years.
Results:
In APCAPS, children with >36 months of breastfeeding scored 0.28 (95% confidence interval [95% CI]: 0.00-0.56; P < .05) higher on tests than those with up to 12 months of breastfeeding. In the nationally representative IHDS-2 data, above-median breastfeeding duration was associated with 0.1 year (95% CI: 0.04-0.16; P < .01) higher educational attainment. In IHDS-2, >12 to 24 months and >24 months of breastfeeding were associated with 0.12 (95% CI: 0.01-0.23; P < .05) and 0.19 years of (95% CI: 0.05-0.34; P < .05) higher educational attainment, respectively, than for those with up to 6 months of breastfeeding. In additional analyses by sex, we found that the benefits of breastfeeding accrued primarily to boys.
Conclusion:
Breastfeeding duration was associated with small gains in educational outcomes for boys but not for girls in India.
Introduction
A sizable literature has confirmed that breastfeeding improves infants’ health and survival. 1 –3 The effect is particularly strong when access to clean drinking water is limited, and poverty pressures mothers to dilute costly substitutes for breast milk. 1 –3 In line with these findings, the World Health Organization (WHO) recommends 6 months of exclusive breastfeeding for newborns and continued breastfeeding with appropriate complementary foods for 2 years or more worldwide. 1,4,5 Long-term effects of breastfeeding, either exclusive or any, on the health of mothers and their offspring are also increasingly well studied. 2,6 –9
The nutrients in breast milk, such as docosahexaenoic acid and arachidonic acid, may support rapid brain development in infants, thereby improving cognition in the long term. 7,10 –12 A pooled analysis of 9 studies, adjusted for both home stimulation and maternal intelligence, 7 found a 2.6 increase in IQ points (95% confidence interval [95% CI]: 1.3-4.0) associated with any breastfeeding. The most compelling evidence for a causal effect of breastfeeding on cognition comes from a single cluster-randomized trial of breastfeeding promotion in Belarus, in which 6.5-year-old children whose mothers originally received the intervention during the period of 1996 to 1997 had 7.5 (95% CI: 0.8-14.3), 2.9 (95% CI: −3.3-9.1), and 5.9 (95% CI: −1.0-12.8) higher verbal, performance, and full-scale IQ points, respectively. 13
The effect of breastfeeding on cognitive performance could be expected to extend to improvements in academic outcomes—such as school enrollment, grade attainment, and test scores—through its effect on IQ or cognition. However, the association between breastfeeding and education has not been widely studied, especially in the context of low- and middle-income countries. 7 A few small-scale studies from the United States, United Kingdom, New Zealand, and Brazil showed positive links between any (not necessarily exclusive) breastfeeding and educational attainment, but no association was seen in Guatemala and South Africa, and a negative association was found in the Philippines. 7,14 –16
In this study, we evaluated the association between breastfeeding duration and academic outcomes in India. Rates of child undernutrition in India are among the highest in the world. In 2014, 39% and 30% of Indian children under age 5 were stunted and underweight, with large disparities across socioeconomic groups and regions. 17,18 Undernutrition in early life may also worsen future educational outcomes. 19,20 A staggering 42% of all school-going Indian children drop out before completing grade 8, and 64% of girls and 62% of socioeconomically disadvantaged tribal children drop out before grade 10. 21 –23
The potential long-term effects of breastfeeding in India are poorly understood. Most studies focus on the socioeconomic determinants of breastfeeding rates and patterns in India. 24 –28 A community-based randomized trial of promotion of exclusive breastfeeding during the period of 1998 to 2002 in the state of Haryana found lower diarrhea rates among exclusively breastfed children but no associations with weight-for-height or height-for-age Z scores. 29 An observational study also found no significant association between breastfeeding initiation and exclusive breastfeeding with child growth metrics in national data. 30 However, a cluster-randomized trial study from Andhra Pradesh found that providing mothers with information on WHO recommendations of exclusive breastfeeding and complementary feeding was associated with higher intakes of calorie, protein, and micronutrients, and lower stunting among children under the age of 2 years. 31 To the best of our knowledge, no study has examined the association between breastfeeding duration and the cognitive or educational outcomes of children in India.
Methods
Analysis of Andhra Pradesh Children and Parents Study
We used 2 data sources of breastfeeding and future academic outcomes. One set of data came from the Andhra Pradesh Children and Parents Study (APCAPS), a community-based trial of nutritional supplementation integrated with other public health programs and its follow-up surveys. The trial was conducted during the period of 1987 to 1990 under India’s Integrated Child Development Services (ICDS), which is a national program of providing free supplemental nutrition, preschool education, health checkups and referral, immunization, and nutrition and health education to pregnant women and young children below the age of 6 years. 32 –34
First, 2 adjacent subdistricts—one each as intervention and control areas—near the city of Hyderabad in the state of Andhra Pradesh (now in Telangana) were selected for the study. Then, within each subdistrict, a group of villages around a village centrally located in the subdistrict was included in the trial—resulting in 15 intervention and 14 control villages. Under the ICDS, a balanced protein–calorie supplement, made from locally available corn–soya ingredients called “upma,” was offered daily over a period of 3 years to pregnant women and children below 6 years of age living in 15 intervention villages. The intervention was delayed in 14 control villages and introduced after the trial ended. Access to other public health programs, such as primary healthcare, child immunization, and anemia control in pregnancy by providing iron and folic acid tablets, were similar in intervention and control villages. A short abstract describing the trial was published, but no other documents are available. 35
Children born during the original trial period (1987-1990) were resurveyed during the period of 2003 to 2005, followed by further surveys in 2009 to 2010 and 2010 to 2012. Data from these surveys have been used to examine the association between exposure to the nutritional supplement and adolescent height, lean body mass, muscle strength, cardiovascular health, and educational outcomes. 20,35 –37 Information on the intake of the supplement by participants during the original trial is not available. As a result, exposure to the supplement has been measured as intention to treat, that is, birth in an intervention village during the trial period, in these studies.
For the current study, we used data from the 2003 to 2005 follow-up survey of the APCAPS cohort. Among the 8246 children born since the beginning of the trial, 11.5% had died before the follow-up survey. Of the surviving children, 2601 were born during the trial period and are therefore eligible for follow-up. Among them, 654 intervention and 511 control group children with historical records participated in the survey (801 and 691 were invited to participate, respectively). 35 We used retrospective data on breastfeeding collected from their mothers by the 2003 to 2005 survey, when the children were 13 to 18 years (see Table 1). Breastfeeding initiation was nearly universal (99.4% of children), and the median reported duration of any breastfeeding was 24 months (standard deviation [SD] = 14.2). Information on the exclusivity of breastfeeding was not collected by the survey, which asked only for the number of months before introducing solid food (with no details on the type of food). Self-reported data on whether currently enrolled in school, highest schooling grade completed, and scores on the most recent test at school for each 13- to 18-year-old study participant were collected. 38
Comparison of Breastfeeding-Related Questions in APCAPS and IHDS Surveys With WHO.
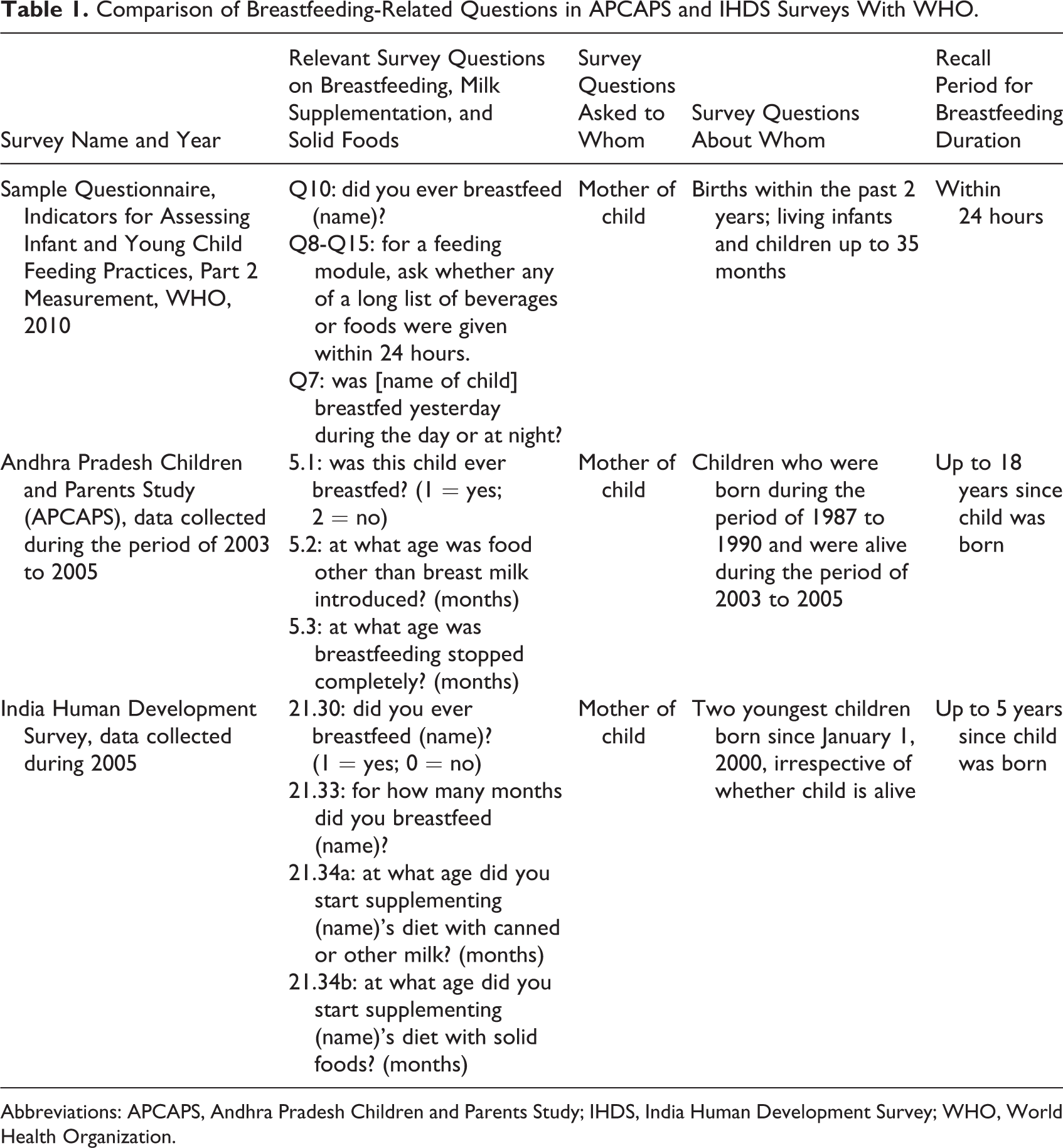
Abbreviations: APCAPS, Andhra Pradesh Children and Parents Study; IHDS, India Human Development Survey; WHO, World Health Organization.
We used Stata version 14 (StataCorp LLC) for analysis and considered P < .05 statistically significant. We used probit regression to estimate the association between explanatory variables and school enrollment and ordered probit regression for schooling grade and test score. The schooling grade was on a scale of 0 to 12, and test scores were measured as follows: distinction = 5, first class = 4, second class = 3, third class = 2, and fail = 1.
The main explanatory variable of our regression model was months of any breastfeeding. Since other foods, either as complementary to or as a substitute for breast milk, may affect breastfeeding duration, we also included months before the introduction of solid food as a covariate. Other covariates were household caste (scheduled caste or scheduled tribe, other backward class), religion (Hindu or other), household standard of living—measured by the quintiles of a composite wealth index 20,39 —indicators of education of the father and mother (literate, completed primary, or completed secondary or above, in comparison with illiterate), and child’s age, sex (whether female), and birth order. Because preterm birth may adversely affect the future educational outcomes of a child, 40,41 we included an indicator of premature birth among our covariates.
There are large gaps in child human capital investment and outcomes in India between boys and girls. Boys are breastfed at a higher rate and for a longer duration than girls. 42 To capture the sex-specific association between breastfeeding and future outcomes, we included an interaction between sex and breastfeeding duration in our model. Finally, in order to capture any links between the nutrition trial and breastfeeding duration, we included an indicator of whether the child was born in an intervention village among the covariates. We clustered standard errors of all regression models at the village level.
Analysis of IHDS
We further examined the link between breastfeeding and educational outcomes in the nationally representative India Human Development Surveys (IHDS) of 2004 to 2005 and 2011 to 2012 (IHDS-2) data. India Human Development Survey-2 covered 42 152 Indian households, of which 83% were resurveys from IHDS. We used IHDS breastfeeding information collected for the 2 youngest children born to each mother since 2000 (see Table 1). From IHDS-2, we used data on the socioeconomic status of households and the demographic characteristics and educational attainment of individuals.
Because of attrition between IHDS and IHDS-2, only a subsample of children could be matched between the 2 survey rounds. Self-reported information on educational attainment in years, based on standard national schooling curriculum, was available for all matched children (6 to 12 years old in IHDS-2). For children aged 8 to 11 years in IHDS-2, the survey administered standardized tests in reading, writing, and mathematics. Children were given a choice of the test language (1 of 13 languages). The reading test, involving a short story, was scored on the following scale: can’t read = 0, letter = 1, word = 2, paragraph = 2, and story = 4. The writing test was scored as follows: cannot write = 0, writes with 2 or less mistakes = 1, and writes with no mistakes = 2. The mathematics test, involving calculations, was scored as follows: cannot recognize number = 0, number = 1, subtraction = 2, and division = 3. These tests were very similar to those used in other internationally recognized surveys of adolescent children, including the Pratham Foundation’s Annual Status of Education Report surveys and the Young Lives Surveys. 43,44
Breastfeeding initiation was nearly universal (99%) among children who could be matched between the 2 rounds. The median reported duration of any breastfeeding was 17 months (SD = 9.5). Among matched children in the 8- to 11-year-old age-group (ie, those with test scores), the median reported duration of any breastfeeding was 16 months (SD = 9.3). Information on the month of introducing liquids and solid food (but not the type of liquid or solid) was collected by the survey. However, information on child feeding during the 24 hours preceding the survey—as per the WHO standard for gathering data on breastfeeding exclusivity—was not collected. Summary statistics of the APCAPS and IHDS samples are shown in Table 2.
Summary Statistics of APCAPS and IHDS Samples.a
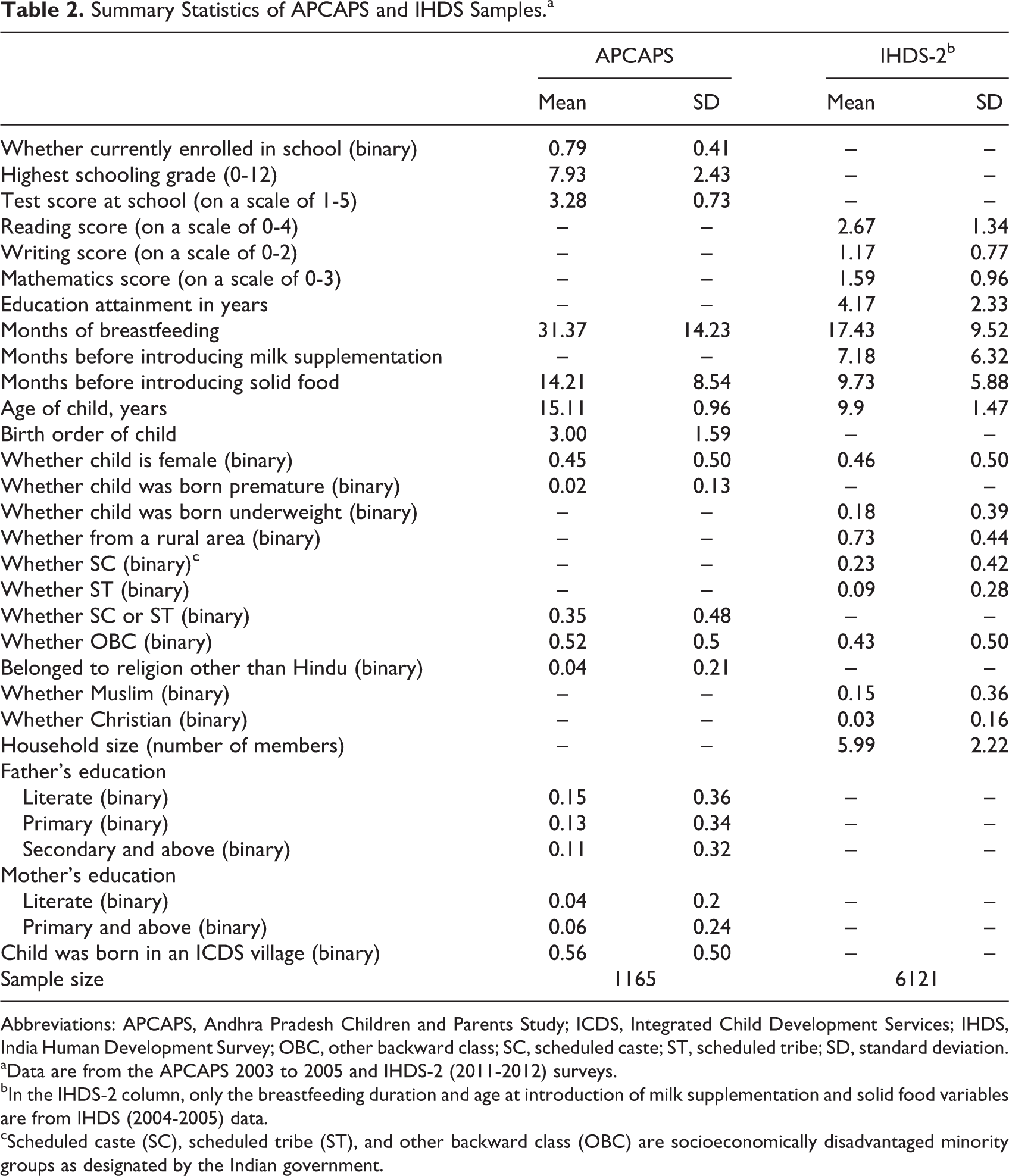
Abbreviations: APCAPS, Andhra Pradesh Children and Parents Study; ICDS, Integrated Child Development Services; IHDS, India Human Development Survey; OBC, other backward class; SC, scheduled caste; ST, scheduled tribe; SD, standard deviation.
aData are from the APCAPS 2003 to 2005 and IHDS-2 (2011-2012) surveys.
bIn the IHDS-2 column, only the breastfeeding duration and age at introduction of milk supplementation and solid food variables are from IHDS (2004-2005) data.
cScheduled caste (SC), scheduled tribe (ST), and other backward class (OBC) are socioeconomically disadvantaged minority groups as designated by the Indian government.
Using the IHDS-2 data, we employed ordered probit regression models to examine the association between breastfeeding duration and later life outcomes: (1) educational attainment in years and (2) test scores (only for 8- to 11-year-old children) in reading, writing, and mathematics. We obtained the main explanatory variables—months of breastfeeding and months before introducing liquids and solid food—from the IHDS survey. Other covariates (from IHDS-2) included age and sex of the child (whether female), whether the child was underweight (as perceived by the mother), interaction between sex of the child and breastfeeding duration, household size, and indicators of caste (scheduled caste, scheduled tribe, or other backward class) and religion (Muslim or Christian, in comparison with Hindu). We captured the standard of living of the household by quintiles of monthly per capita household expenditure (in Indian rupees). We adjusted for state indicators in all regression models and clustered the standard errors at the state level.
Additional Analyses Using Categorized Values of Breastfeeding Duration
Figure 1 shows the kernel density distributions of duration of breastfeeding in APCAPS and IHDS data, respectively. In both, reported breastfeeding duration was significantly clustered around the half-yearly or annual values (eg, 12, 18, and 24 months). The clustering was more pronounced in the APCAPS data, possibly because of recall error arising from the long gap between the 1987 and 1990 trial period, when the children were breastfed, and 2003 to 2005, when breastfeeding data were collected from their mothers.
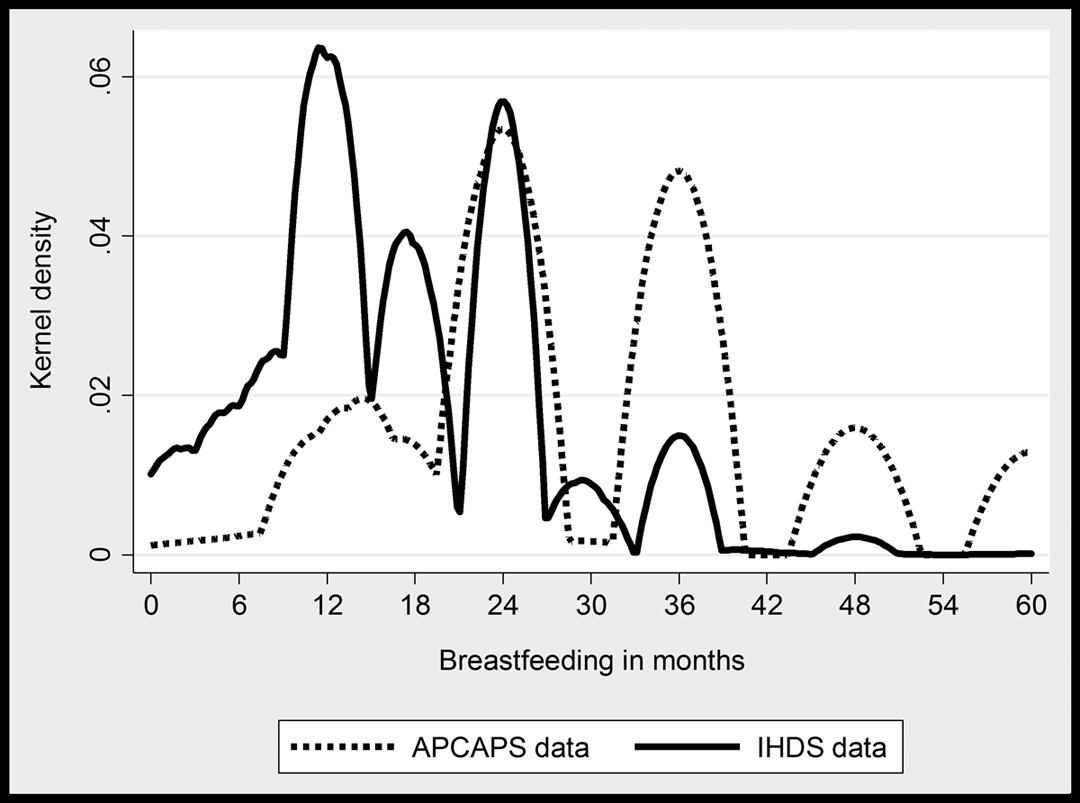
Kernel density distribution of duration of any breastfeeding in Andhra Pradesh Children and Parents Study (APCAPS) 2003 to 2005 survey and India Human Development Survey (IHDS) 2004 to 2005. The IHDS sample includes children born since year 2000 who could be matched with IHDS-2.
The measurement error in breastfeeding duration could widen the CIs of the estimated relationship between breastfeeding duration and child outcomes. We improved precision by replacing the breastfeeding duration in months with categorized values in additional regression models. In one set of models, we used a binary indicator of above-median duration (as compared with at or below median) instead of duration in months. In another set of models, we categorized the breastfeeding duration in APCAPS into the following groups: (1) up to 12 months of breastfeeding, (2) more than 12 but less than 24 months of breastfeeding, (3) more than 24 but less than 36 months of breastfeeding, and (4) over 36 months of breastfeeding. In IHDS, we categorized breastfeeding duration into the following groups: (1) up to 6 months of breastfeeding, (2) more than 6 but less than 12 months of breastfeeding, (3) more than 12 but less 24 months of breastfeeding, and (4) over 24 months of breastfeeding. We included indicators of each category in the regression models (using the lowest category as the comparison group) instead of the duration in months. This approach ignored a child’s exact location, which may be imprecise, on the breastfeeding duration distribution.
We report the estimated association between breastfeeding duration and educational outcomes in the overall sample (ie, by excluding the interaction between duration and female child indicator from regression) of APCAPS in the top half of Table 3. We then included the interaction term in the model and report its estimated coefficient in the bottom half of Table 3. Full regression results are available in Supplemental Tables 1–3.
Regression of Educational Outcomes for Study Participants, APCAPS 2003-2005 Follow-Up.a
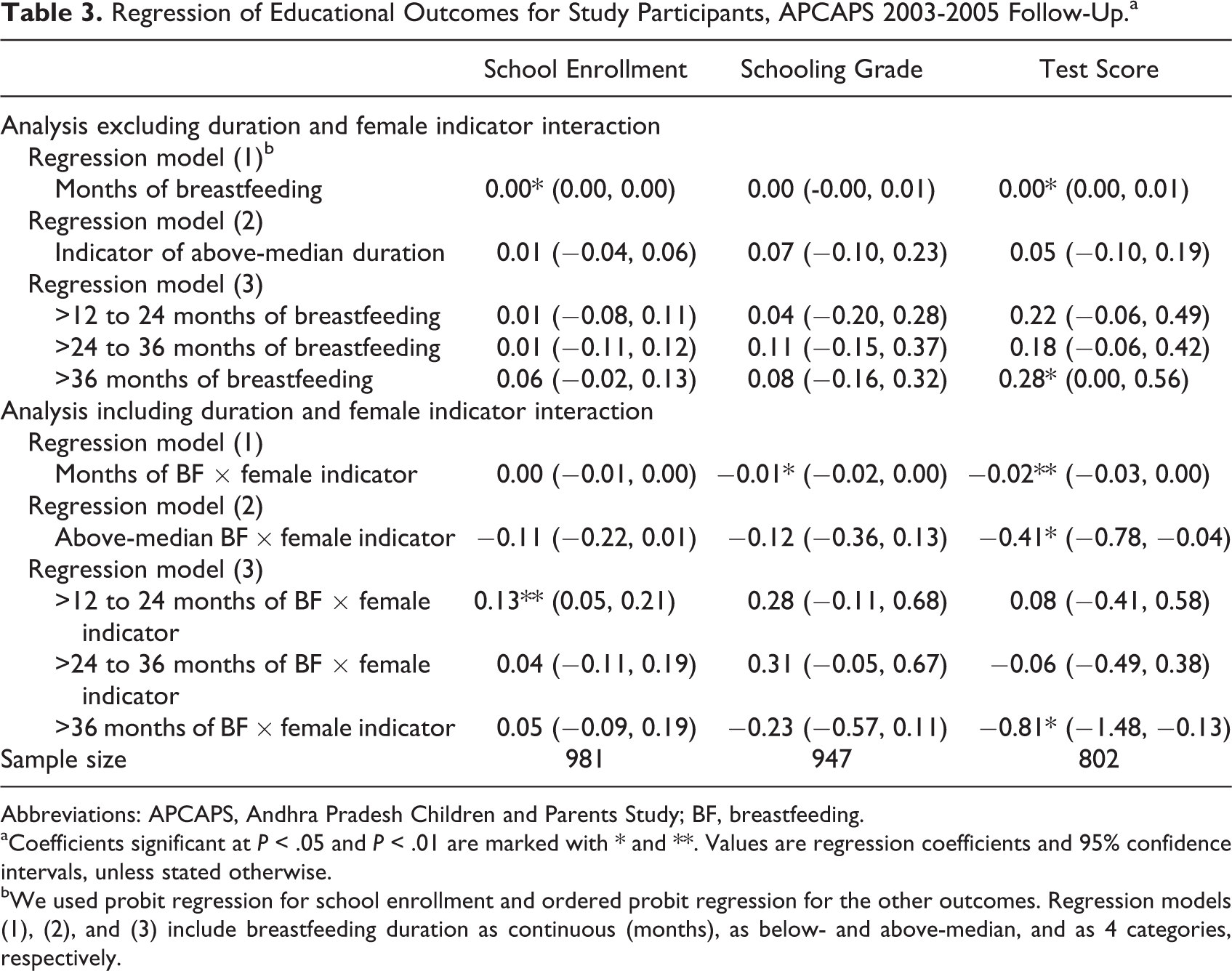
Abbreviations: APCAPS, Andhra Pradesh Children and Parents Study; BF, breastfeeding.
aCoefficients significant at P < .05 and P < .01 are marked with * and **. Values are regression coefficients and 95% confidence intervals, unless stated otherwise.
bWe used probit regression for school enrollment and ordered probit regression for the other outcomes. Regression models (1), (2), and (3) include breastfeeding duration as continuous (months), as below- and above-median, and as 4 categories, respectively.
We present the estimated regression coefficients of breastfeeding duration (excluding interaction with the female child indicator from covariates) from IHDS data in the top half of Table 4. After including the interaction term in the regression, we report its estimated coefficients in the bottom half of Table 4. Full regression results are shown in Supplemental Tables 4–6.
Regression of Educational Outcomes for Study Participants, IHDS-2 (2011-2012).a
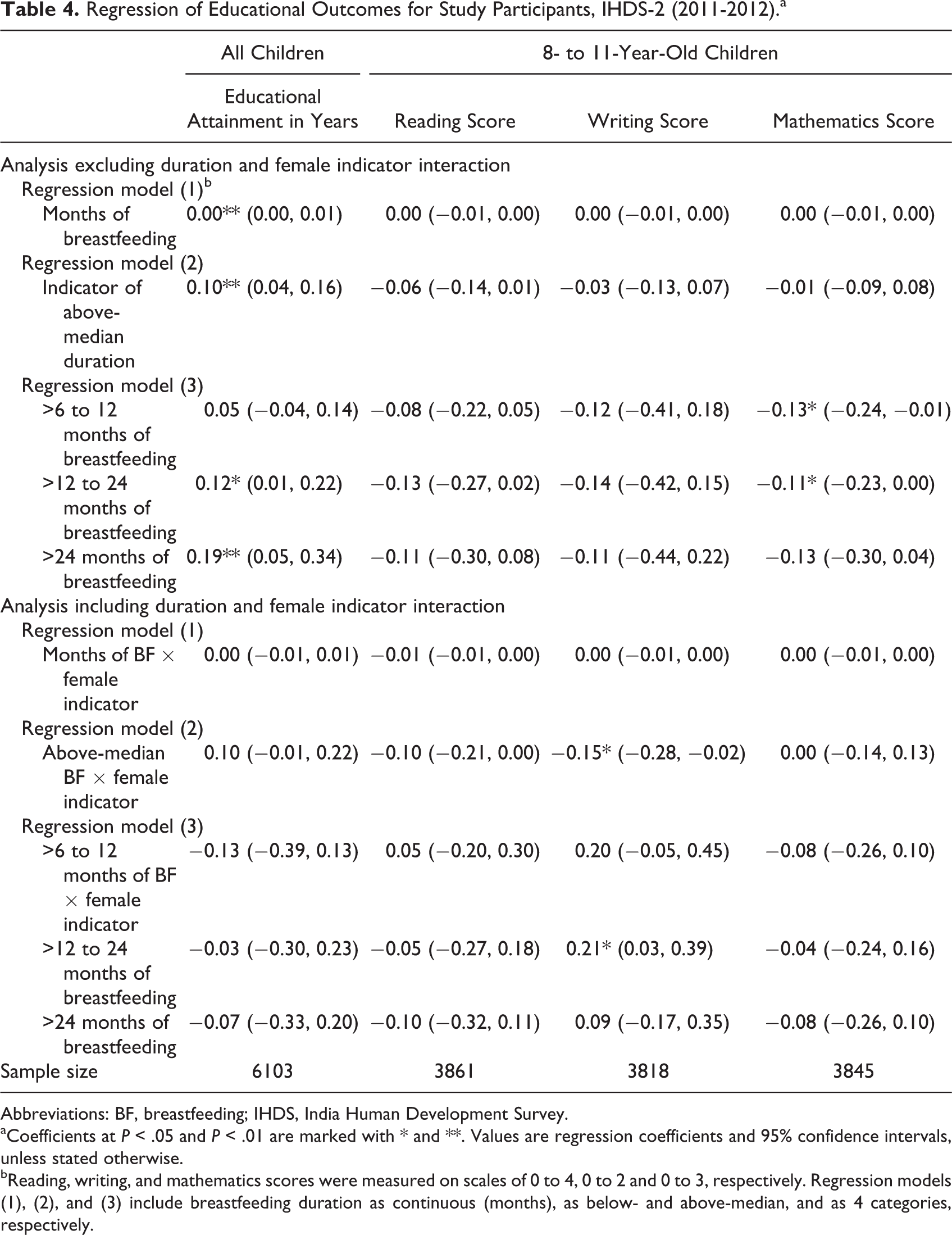
Abbreviations: BF, breastfeeding; IHDS, India Human Development Survey.
aCoefficients at P < .05 and P < .01 are marked with * and **. Values are regression coefficients and 95% confidence intervals, unless stated otherwise.
bReading, writing, and mathematics scores were measured on scales of 0 to 4, 0 to 2 and 0 to 3, respectively. Regression models (1), (2), and (3) include breastfeeding duration as continuous (months), as below- and above-median, and as 4 categories, respectively.
In order to explore the sex-specific differences more, we also estimated the regressions with continuous and binary indicator of above-median duration of breastfeeding separately for boys and girls (results are reported in Supplemental Table 7-14). Because sample sizes were low, we could not reliably estimate regressions with finer categories of breastfeeding duration separately by sex.
Results
Households in APCAPS were all from rural areas; 96% of them were Hindu and 87% belonged to socioeconomically disadvantaged caste groups. Among children in the data, 79% were enrolled in school and attained 8th grade at school on average. Households in the IHDS data were 73% from rural areas, 80% were Hindu, and 75% belonging to socioeconomically disadvantaged caste groups. Children in these households had completed 4 years of education on average.
In APCAPS, we found no significant association between the duration of breastfeeding—either in months or as below and above median—and educational outcomes in the overall sample. When we categorized the values of breastfeeding duration, >36 months of breastfeeding was associated with 0.28 points (95% CI: 0-0.56; P < .05) higher test scores as compared with up to 12 months of breastfeeding.
Boys benefited more from breastfeeding in APCAPS data, as breastfeeding duration among girls was associated with 0.01 (95% CI: −0.02 to 0; P < .05) lower schooling grade and 0.02 points (95% CI: −0.03 to 0; P < .01) lower test scores. Above-median duration and >36 months of breastfeeding were associated with 0.41 points (95% CI: −0.78 to −0.04; P < .05) and 0.81 points (95% CI: −1.48 to −0.13; P < .05) lower test scores for girls than boys. Only in 1 case, >12 to 24 months of breastfeeding was associated with 13 percentage points (95% CI: 5-21; P < .01) higher school enrolment among girls than boys, when compared with up to 12 months of breastfeeding.
In IHDS, we found no significant association between breastfeeding duration and educational outcomes in the overall sample. However, the above-median breastfeeding duration was associated with 0.1 (95% CI: 0.04-0.16; P < .01) higher educational attainment in years. Similarly, >12 to 24 months and >24 months of breastfeeding were associated with 0.12 (95% CI: 0.01-0.22; P < .05) and 0.19 (95% CI: 0.05-0.34; P < .01) extra years of educational attainment as compared with up to 6 months of breastfeeding. The durations of >6 to 12 months and >12 to 24 months of breastfeeding were associated with 0.13 (95% CI: −0.24 to −0.01; P < .05) and 0.11 (95% CI: −0.23 to 0.00; P < .05) points lower mathematics test scores.
The interaction between breastfeeding duration and female indicator was not statistically significant in IHDS except in 2 cases. Above-median duration was associated with 0.15 points (95% CI: −0.28 to −0.02; P < .05) lower writing scores among girls as compared with boys. The duration of >12 to 24 months of breastfeeding was associated with 0.21 points (95% CI: 0.03-0.39; P < .05) higher writing scores among girls than boys, when compared with up to 6 months of breastfeeding.
In the APCAPS data, months of breastfeeding was associated with 0.01 points (95% CI: 0.01-0.02; P < .01) increase and 0.01 points (95% CI: −0.02 to 0; P < .05) decrease in test scores of boys and girls, respectively. Above-median duration of breastfeeding was associated with a 0.24 points increase (95% CI: 0.01-0.46; P < .05) in test score for boys. In the IHDS-2 data, months of breastfeeding were associated with 0.01 (95% CI: 0-0.01; P < .05) more years of education among boys. Above-median breastfeeding duration was associated with 0.18 (95% CI: 0.12-0.24; P < .001) extra years of education and 0.11 points (95% CI: –0.22, –0.01; P < .05) lower test score in writing for girls. There were no other significant associations.
Discussion
We examined the association between the duration of breastfeeding of Indian children and their future educational outcomes. We mitigated possible measurement errors by dividing breastfeeding duration into 2 or 4 categories. In APCAPS data, >36 months of breastfeeding was associated positively with test scores. In IHDS-2 data, above median, >12 to 24 months, and >24 months of breastfeeding were associated with more years of educational attainment. Breastfeeding durations of >6 to 12 months and >12 to 24 months were also associated with very small (less than one-seventh of an SD), and therefore negligible, reductions in mathematics test scores in IHDS-2.
Boys received greater educational benefits than girls in both data sets. When conducting regressions separately by sex, above-median duration of breastfeeding was associated with higher test scores for boys in APCAPS. In IHDS-2 data, above-median breastfeeding was associated with more years of education but lower writing scores for girls. However, the reduction in writing score was equivalent to about one-seventh of an SD and is therefore negligible.
Longer breastfeeding duration has been associated with improved educational outcomes in a few other countries. A study using long-term data on approximately 1000 children born in 1977 in New Zealand found that those breastfed for at least 8 months postbirth were 62% more likely to complete schooling and had standardized test scores up to 0.59 SDs higher at age 18 than non-breastfed children. 45 A cohort study of 8226 nine-year-old Irish children found that breastfeeding was associated with 3.24 and 2.23 percentage points higher reading and mathematics scores. 46 A longitudinal study of 1739 men and women born in 1946 in England, Wales, and Scotland found that breastfeeding duration was positively associated with educational attainment by age 26 and the ability to read 2 additional words on the 50-word National Adult Reading Test at age 53. 47 Another study followed 2094 children born in 1982 in Pelotas, Brazil, for 18 years and found that those breastfed for 9 or more months in childhood attained 0.5 to 0.8 more grades of schooling than those breastfed for less than 1 month. 48 A follow-on study that revisited the cohort when the participants were 30 years old reported that breastfeeding for at least 12 months was associated with 0.9 more years of education relative to those breastfed for less than 1 month. 49
Our finding of a sex difference in educational outcomes associated with breastfeeding is consistent with the findings of previous studies of breastfeeding patterns in India. A recent study estimated that mothers on average breastfed daughters for 0.9 fewer months than they did sons. 42 Another study showed not only that girls were breastfed for 0.45 fewer months than boys but also that the amounts of breast milk and other milk consumed by them were 21% and 14% lower, respectively. 50 Health and educational resources such as vaccinations and nutrition are also provided more to boys. 51 –53 The sex difference in the intensity of breastfeeding may explain the stronger positive association between breastfeeding and educational outcomes among boys in our data.
Possible explanations on the differences in findings from the APCAPS and IHDS data sets and also between our study and the previous literature include lengthy recall periods (in APCAPS) and differences in the methods of collecting breastfeeding data.
We first address recall periods. In the APCAPS survey, historical data on breastfeeding during early childhood of 13- to 18-year-old children were collected from their mothers. Similarly, IHDS 2004 to 2005 collected historical data on breastfeeding of children born since the year 2000. As a result, reported breastfeeding duration data were highly clustered around certain values. The measurement error likely attenuated our regression estimates, especially in case of the APCAPS data, in which recall periods are long.
In additional analyses, we examined the association between breastfeeding duration and outcomes separately for children who were between 6 and 9 years old in the IHDS-2 data. The recall period for breastfeeding was shorter for these younger children, yet the estimated links between breastfeeding and outcomes from these regression models were not statistically significant.
As shown in Table 1, both APCAPS and IHDS surveys deviated significantly from the WHO guidelines for collecting breastfeeding data. Although the questions related to whether children were ever breastfed and total duration (in months) of breastfeeding were the same, there were significant differences in how data on exclusive breastfeeding were collected. In particular, neither APCAPS nor IHDS included detailed questions on breastfeeding and liquids or food given the day before the survey. As a result, the nature and quantity of liquids and solid food given to children are unknown. The duration of exclusive breastfeeding in these data cannot be reliably compared with international standards. As discussed earlier, the background characteristics of the APCAPS and IHDS samples were also different. India Human Development Survey presents an average estimated relationship between breastfeeding duration and education across the country, which could be considerably different from the local findings of APCAPS.
Although we incorporate in our analysis child characteristics such as sex, birth order, and the incidence of premature or underweight birth, which could all affect the duration of breastfeeding, there may be confounding effects from residual unobserved factors. Attrition between consecutive rounds of data may be selective and distort our findings. For example, IHDS-2 households that cannot be matched with IHDS data have higher per capita monthly expenditures than households that can be matched, and their children are breastfed for 1.2 fewer months. Also, a mother may selectively breastfeed certain children more based on their or her own unobserved characteristics. For example, Indian mothers with higher levels of financial autonomy in the household or those who receive more prenatal care are likely to breastfeed at a higher rate, 54,55 whereas Sri Lankan children who are born by cesarean delivery are initiated to breastfeeding late. 56 Information on maternal IQ, which might affect children’s cognition, was also unavailable in our data.
In addition, if mothers who breastfeed for longer durations also provide additional educational resources to their children, any estimated positive association between breastfeeding duration and academic outcomes will be inflated. This may affect a child’s future healthcare and education resources, such as availability of vaccinations, school quality, and public versus private schooling, and could play a role in a child’s decision to withdraw from school—all of which could affect educational outcomes. The socioeconomic and educational environment surrounding a child also may change over time, thereby affecting the relationship between breastfeeding in early life and future academic outcomes. Because of a lack of data, these unobserved factors are beyond the scope of our analysis.
Finally, the underlying mechanisms through which cognition or IQ may be related to educational achievements in India have been studied inadequately. As a result, our findings are limited in providing a theoretical understanding of the relationship between breastfeeding and academic outcomes.
Conclusion
Longer breastfeeding duration, in addition to having well-established positive health benefits, has been associated with improved longer-term cognitive and educational outcomes in a few country case studies. Using long-term data from a regional trial and a nationally representative household survey, we found small positive associations between breastfeeding duration and a few educational outcomes for adolescent males but not females in India. However, household surveys that collected data on breastfeeding in India have not always followed the WHO guidelines. Although our findings suggest the potential importance of breastfeeding promotion as a policy tool for improving future educational outcomes, further research using higher-quality breastfeeding duration data is necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Bill & Melinda Gates Foundation, which provided a grant to the University of Virginia. The authors are solely responsible for all views expressed in this paper, which are not necessarily those of the funder or any other organization. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.