
Abstract
Background:
The Integrating Orange Project promotes production and consumption of orange-fleshed sweet potato (OFSP) to address vitamin A deficiency among rural populations of Zambia since 2011.
Objective:
This study assessed household production and consumption of OFSP and identified factors associated with consumption thereof in Integrating Orange Project areas in Chipata district, Zambia.
Methods:
Respondents of 295 randomly selected households were interviewed using a structured questionnaire during the sweet potato harvest season. Associations between OFSP consumption and household factors were assessed using χ2 tests.
Results:
Frequency of OFSP consumption was categorized as ≥4 days during the last 7 days (30.2%), 1 to 3 days during the last 7 days (49.5%), eats OFSP but not during the last 7 days (7.1%), and never (13.2%). In total, 60.3% of households planted OFSP, and 40.0% bought OFSP, mostly from farmers within the community. Orange-fleshed sweet potato consumption was associated with the presence of children aged less than 5 years in the household (P = .018), production of OFSP (P < .001), purchasing of OFSP (P < .001), and respondent having knowledge on health benefits of OFSP (P = .014). Age and sex of the household head and household size had no association with OFSP consumption (P > .05).
Conclusion:
A high percentage of households consumed OFSP during the harvesting season in Integrating Orange Project areas. Programs promoting OFSP consumption should thus focus on OFSP production and sensitizing households on nutritional benefits of OFSP and target households with children aged less than 5 years as entry point.
Introduction
Vitamin A deficiency (VAD) affects 190 million preschool children and 19 million pregnant women, with regions in Africa and South-East Asia being affected the most. 1 Zambia has no current nationally representative data on VAD; the only national assessment done was in 2003, and this showed that 54% of children aged less than 5 years and 13% of women of childbearing age were vitamin A deficient. 2 More recently, cross-sectional data for rural populations in the Eastern and Central Provinces in Zambia showed similar results, with 54% of children aged 2 to 5 years being vitamin A deficient (based on low serum retinol concentrations), despite adequate dietary vitamin A intake, high coverage of vitamin A supplementation, and access to vitamin A fortified sugar. 3 On the contrary, a micronutrient and food consumption survey that was done in 2014 in 2 of the 3 ecological zones in Zambia showed that 25.8% of children aged 6 to 59 months were vitamin A deficient. 4 In addition, the baseline data for a randomized controlled trial assessing the efficacy of biofortified orange maize reported a lower (12.1%) prevalence of VAD in slightly older (4-8 years) children in a rural farming district in Zambia. 5
Biofortification is a feasible and cost-effective complementary strategy of delivering micronutrients to rural populations that may have limited access to diverse diets and other micronutrient interventions, such as supplementation and food fortification. 6,7 Biofortification refers to the breeding of staple crops, including sweet potato, for increased micronutrient content. From 2011 to 2014, sweet potato production in Zambia ranged between 43 211 and 45 677 tons, 8 which is low compared to Eastern African countries where sweet potato is one of the main staple foods. Aimed at improving food security and livelihoods of poor families in Sub-Saharan Africa, the Sweetpotato Action for Security and Health in Africa, through the International Potato Center (CIP) and in collaboration with the rural poor, embarked on a 5-year initiative to increase production and consumption of sweet potato. In Zambia, this initiative implements various interventions in the orange-fleshed sweet potato (OFSP) value chain to ensure that production, productivity, and utilization of OFSP result in improved health and nutrition and economic upliftment of the rural poor communities. 9 To date, OFSP is considered the single most successful example of biofortification. 6 Promotion of OFSP is an intervention especially suitable for rural communities that have limited access to vitamin A-rich foods, and consume mostly locally produced staple foods. 10,11 Evidence has shown that consumption of OFSP can significantly improve vitamin A intake and status among vulnerable populations. 11,12 In Mozambique, OFSP accounted for 78% of total vitamin A intake among women and children who participated in a large-scale intervention that promoted OFSP. 12 According to Low and coworkers, 13 100 to 125 g of OFSP can supply the recommended dietary allowance of vitamin A for children aged less than 5 years. A randomized controlled trial in South Africa showed that the consumption of 125 g of OFSP over a period of 53 school days improved liver vitamin A stores in 5- to 10-year-old children. 14 In Mozambique, a 50% reduction in VAD 13 and reduced prevalence and duration of diarrhea episodes 15 were reported in children aged less than 5 years in areas where OFSP was promoted. A recent systematic review on OFSP studies in Mozambique reported that although various studies have shown a positive impact on vitamin A status due to the introduction of OFSP, various challenges for the large-scale adoption of this intervention remain. 16
Studies in Mozambique, Uganda, and Kenya have shown that adoption of OFSP is associated with various factors such as, for example, the size of land dedicated to the production of OFSP, 17,18 the type of variety of sweet potato, 19 market potential of the crop, 18 cost, 20 knowledge on the nutritional value of OFSP, 18,21 and the presence of a young child in the household. 21
In Zambia, a US Agency for International Development–funded project named the Integrating Orange Project was implemented by the CIP in collaboration with the Zambia Agriculture Research Institute in 2011, whereby OFSP is being promoted in rural farming communities in the Eastern and Central Provinces as one of the interventions to control VAD. The target was to reach 15 000 rural households, prioritizing women with children younger than 5 years. 22 Baseline data for this project showed that only 0.2% of households in the Chipata district cultivated OFSP, covering a total of only 3.67 ha of land. 23 Since then, a number of strategies have been implemented in the target areas, such as provision of high-quality OFSP vines to rural households; training of communities on good agronomic practices, multiplication, and conservation of vines; providing nutritional knowledge related to VAD, OFSP, childcare, and dietary diversity; developing promotion and education messages; and building capacity. 24 Recipes were promoted through community cooking demonstrations. Results of preference tastes done in all communities showed that more than 80% of the community members liked the OFSP products and were willing to consume them in their homes. 22 However, the consumption of OFSP at household level in Integrating Orange Project areas and the factors associated with its consumption are unknown. The aim of this study was therefore to establish the consumption of OFSP and identify factors associated with consumption thereof in rural households from the Chipata district in Zambia.
Methods
A cross-sectional study was conducted among the rural populations of Chipata district. Only communities that were part of the Integrating Orange Project were included and these were located in Chipangali, Chipata Central, Kasenengwa, and Luangeni agricultural camps. People residing outside these areas were not included in the study.
The required sample size was calculated using a 95% confidence level and 3.5% precision and based on the assumption that an estimated 11% of households consumed OFSP. 25 The required sample size of 307 households was adjusted to allow for a 15% nonresponse rate. Thus, the final sample size was 353 households.
A systematic random sampling approach was used to select households from a main sampling frame of the list of all households (n = 2 790) in the project area. Households that were not available were visited 3 times and those that could not be reached after the third nonresponse visit were not replaced. Some of the sampled households were unavailable and could not be reached through 3 visits as they were participating in the community agricultural shows which were ongoing for 1 month. As a result, the final study sample consisted of 295 households, which was 12 short of the required 307 households.
Data Collection
Data were collected using an interviewer-administered structured questionnaire that was designed to collect information on household sociodemographics; production, procurement, and consumption of OFSP; and knowledge on the nutritional benefits of OFSP. Prior to the survey, the questionnaire was pretested in 20 households in another community with similar characteristics as the study population. Survey data were collected for the 295 randomly selected households in June 2015. The head of the household (or their spouse) were interviewed by male and female agricultural officers who were trained in data collection. Data collection was closely monitored and completed questionnaires were checked daily.
The study protocol was approved by the research ethics committee of the University of the Western Cape (reference number 15/3/22). Prior to data collection, the community was informed about the study through social mobilization meetings. Informed written consent was obtained from each respondent prior to data collection.
Data Analysis
Data were entered using EpiData 26 and analyzed using SPSS version 20. Data on whether the household eats OFSP when available and the number of days eaten during the past 7 days were used to categorize households into 4 groups according to OFSP consumption, that is, at least 4 days during the last 7 days, 1 to 3 days during the last 7 days, seldom (eats OFSP but not in the last 7 days), and never. Descriptive statistics were done, and data are presented as frequencies and percentages. Associations between household consumption of OFSP and sociodemographic variables and the factors that might be associated with OFSP consumption were determined using cross-tabulations and a χ2 test, with a P value ≤.05 considered statistically significant.
Results
Respondent and Household Characteristics
In total (n = 295), 184 (62.4%) males and 111 (37.6%) females were interviewed. For 210 (71.2%) households, the household head was male, with an average age of 43.7 ± 12.2 years, and for 85 (28.8%) households, the household head was female, with an average age of 47.3 ± 4.1 years. The number of individuals per household ranged from 1 to 18, with an overall mean of 6.6 ± 3.0 individuals per household. Of the 295 households, 183 (62.0%) had children less than 5 years old with a median of 2 children (interquartile range 1) per household. Farming, reported by 251 (85.1%) households, was the modal livelihood means of survival.
Production of OFSP
In total, 282 (95.6%) households grew different types of crops, of whom 161 (57.1%) cultivated more than 1 ha of land. Orange-fleshed sweet potato was usually planted by 178 (60.3%) households, of whom 167 (93.8%) planted OFSP during the 2014/2015 planting season, accounting for 56.6% of the total number of households included in the study. For households that grew crops but not OFSP (n = 104), 57 (54.8%) had no specific reason for not planting OFSP; for the remainder, lack of planting materials (n = 26; 25.0%) and lack of money to buy planting materials (n = 13; 12.5%) were the main reasons for not growing OFSP. Information on production practices for households who planted OFSP is shown in Table 1. For those households who planted OFSP during the 2014/2015 season (n = 167), the majority planted less than a hectare of land for OFSP. Planting materials were mainly sourced from the CIP project (50.0%) and own stock from previous seasons (39.9%). The main problems encountered were a lack of market (20.4%) and plant pests and diseases (12.0%), whereas 46.1% did not experience any problems. Of the 178 households that usually grew OFSP, 69.7% sold some of their OFSP, of whom 78.2% sold them within their communities.
Information on Cultivation of OFSP for Those Households that Planted OFSP.a
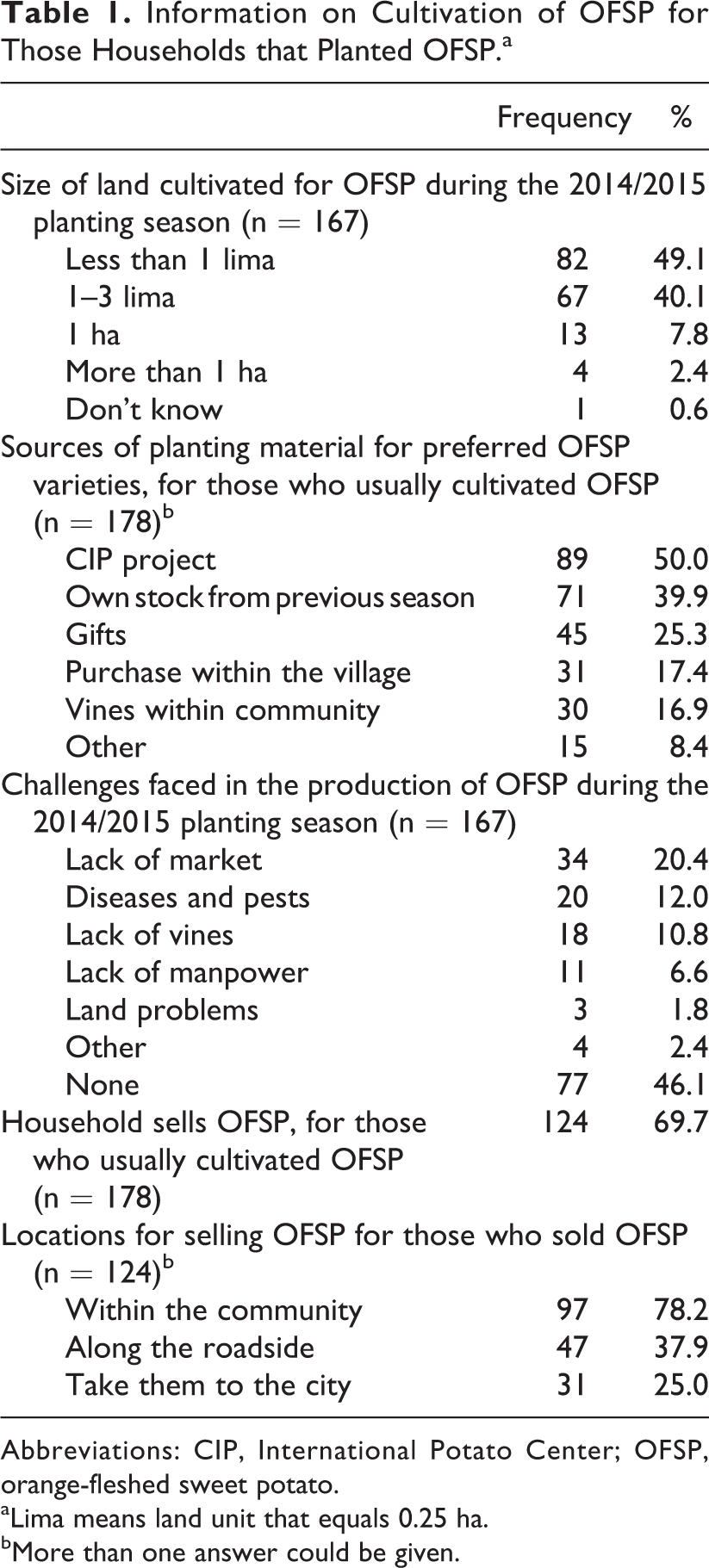
Abbreviations: CIP, International Potato Center; OFSP, orange-fleshed sweet potato.
aLima means land unit that equals 0.25 ha.
bMore than one answer could be given.
Procurement of OFSP
Information on procurement of OFSP for household consumption is given in Table 2. Forty percent of the households usually bought OFSP, of whom 85.6% did so within their communities and 30.5% bought from farms in another community. The study further showed that 46.1% of all households (n = 295) faced challenges in procuring OFSP.
Household Procurement of OFSP.
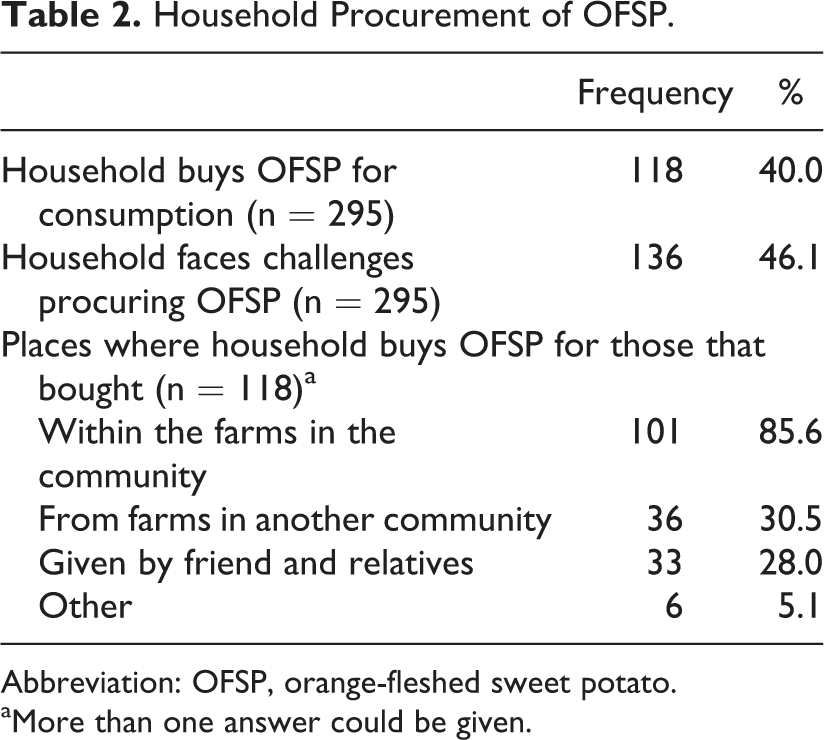
Abbreviation: OFSP, orange-fleshed sweet potato.
aMore than one answer could be given.
Knowledge of VAD, Prevention of Vitamin A Deficiency, and Benefits of OFSP
Knowledge on VAD and the benefits of OFSP are shown in Table 3. Results showed that 78.0% of respondents said they knew something about VAD, and 76.9% said that something could be done to prevent it; these included eating vegetables (93.0%), eating OFSP (89.0%), and eating vitamin A-rich foods (87.7%). Sources of information on VAD, prevention of VAD, and OFSP benefits were mostly staff at the health facilities (34.6%) and agricultural officers (33.6%). When asked about the benefits of eating OFSP, 87.1% agreed that OFSP had health benefits; these included controlling VAD (83.6%) and making the body healthy (51.0%). For 91 (30.8%) of the households, there was at least one household member who has been trained in value addition preparation methods, of whom 81 (89.0%) used these skills to prepare OFSP in their households.
Respondent’s Knowledge on VAD, Suggested Preventive Actions, and Perceived Health Benefits of Eating OFSP.
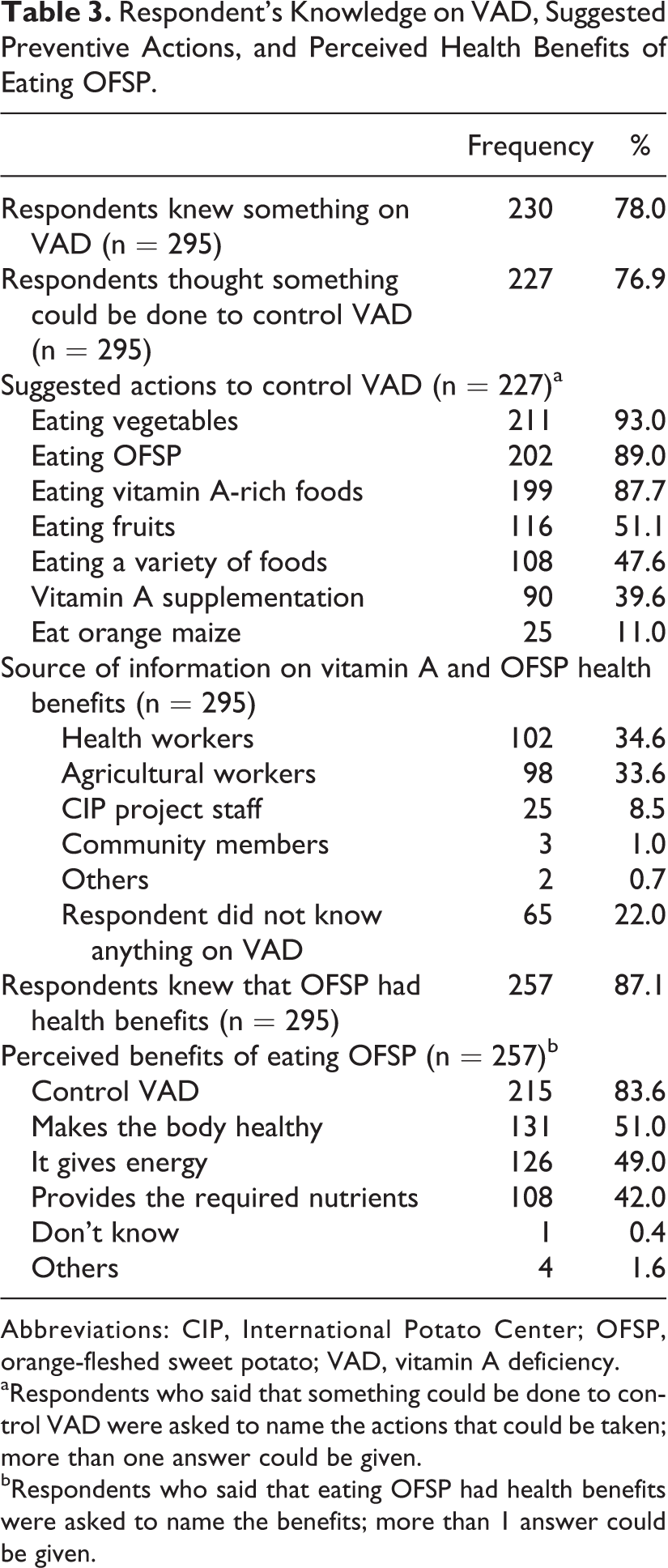
Abbreviations: CIP, International Potato Center; OFSP, orange-fleshed sweet potato; VAD, vitamin A deficiency.
aRespondents who said that something could be done to control VAD were asked to name the actions that could be taken; more than one answer could be given.
bRespondents who said that eating OFSP had health benefits were asked to name the benefits; more than 1 answer could be given.
Household Consumption of OFSP and Factors Associated Therewith
Of the 295 households, 89 (30.2%) ate OFSP on ≥4 days during the past 7 days; 146 (49.5%) ate OFSP on 1 to 3 days during the past 7 days; 21 (7.1%) ate OFSP but not in past 7 days; and 39 (13.2%) never ate OFSP. For households that ate OFSP (n = 256), 69.1% preferred orange-fleshed varieties (vs 30.9% who preferred non–orange-fleshed varieties), and 45.2% preferred value addition preparation methods (mixing OFSP with other foods or processing the OFSP root in a way other than eating it as a root) versus 16.3% who preferred traditional preparation methods, that is, washing the tubers, eating it raw, or boiling it.
Sex and age of the household head, and household size had no relationship with household consumption of OFSP (P > .05) A summary of the other factors associated with OFSP consumption is shown in Table 4, namely, children in household; production, purchasing, and procurement challenges; and respondent’s knowledge on benefits of OFSP and VAD. Households with children younger than 5 years reported consuming OSFP more frequently than households without children (P = .018), with the largest differences being the categories of never (8.7% and 20.5%, respectively) and 1 to 3 days within the last 7 days (54.6% and 41.1%, respectively). Households that produced OFSP reported consuming OSFP more frequently than households that did not produce OFSP (P < .001), with the largest differences being the categories of never (1.1% and 31.6%, respectively) and ≥4 days within the last 7 days (40.4% and 14.5%, respectively). Purchasing of OFSP was associated with the consumption of OFSP (P < .001), with the largest differences being the categories of 1 to 3 days within the last 7 days (69.5% and 36.2%, respectively) and ≥4 days within the past 7 days (20.3% and 36.7%, respectively). Respondents who were aware of the benefits of OFSP reported consuming OSFP more frequently than respondents who were not aware of the benefits (P = .014), with the largest differences being the categories of never (7.8% and 50.0%, respectively) and ≥4 days within the last 7 days (33.5% and 7.9%, respectively). Similarly, respondents who claimed to have knowledge of VAD reported consuming OSFP more frequently than respondents who were not aware of VAD (P = .014), with the largest differences being the categories never (8.3% and 30.8%, respectively) and ≥4 days within the last 7 days (34.3% and 15.4%, respectively).
Factors Associated with Household Consumption of OFSP.
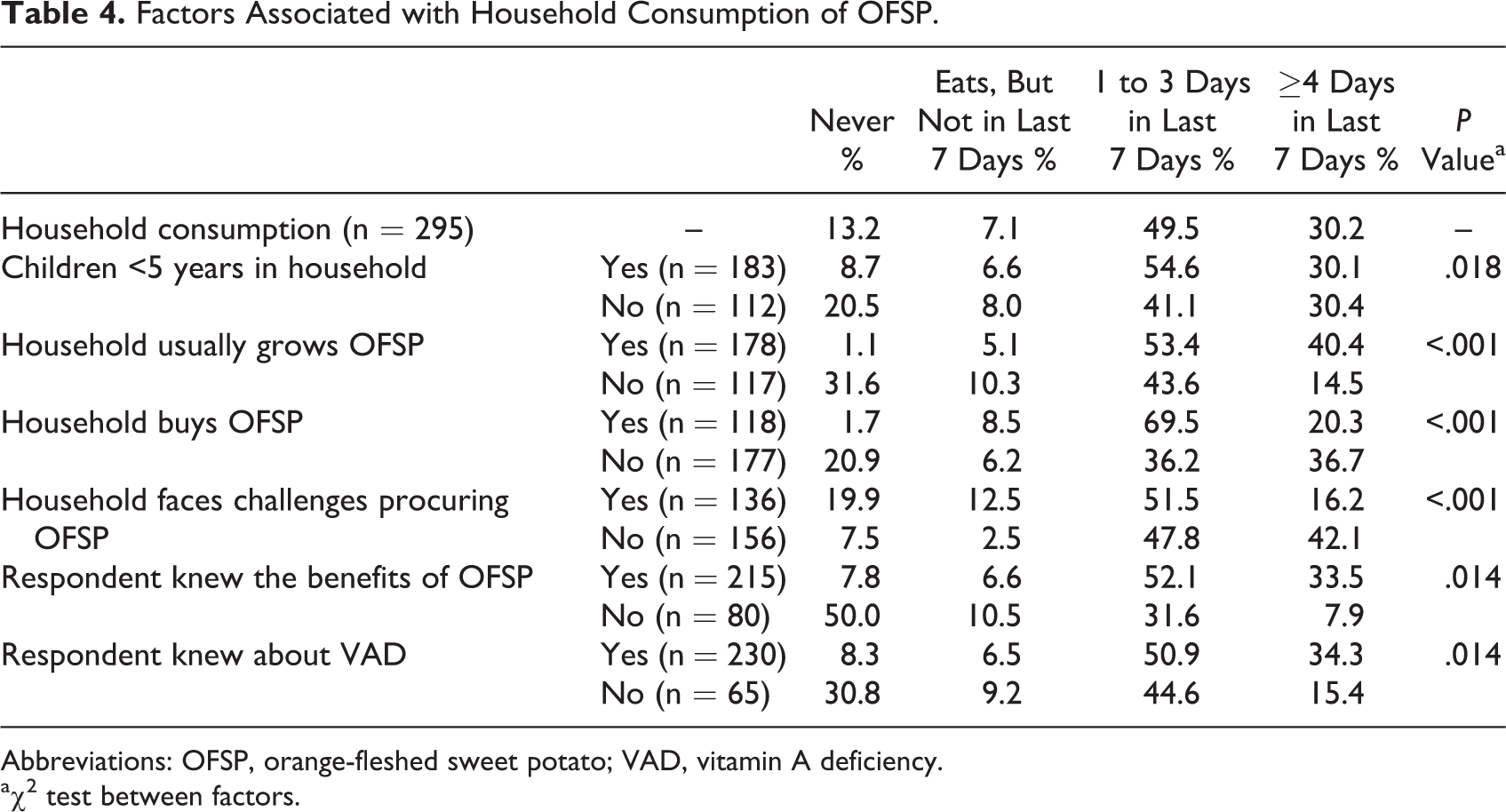
Abbreviations: OFSP, orange-fleshed sweet potato; VAD, vitamin A deficiency.
aχ2 test between factors.
Discussion
The study was done during the harvest season in the Chipata district of Zambia where production and consumption of OFSP is promoted since 2011 through the Integrating Orange Project which targets rural households, prioritizing women with children younger than 5 years. Sixty percent of the households produced OFSP, and two-thirds of these households sold some of their produce, mostly within the community. Forty percent of the households bought OFSP, mostly from growers within the community. A high percentage (86.8%) of households consumed OFSP. Household production of OFSP, the presence of children younger than 5 years in the household, and knowledge on benefits of OFSP and VAD were associated with a more frequent consumption of OFSP.
There was an association between household production of OFSP and consumption thereof. For most of the households in the study area that planted OFSP, the size of the area under cultivation was less than 1 ha. In a study in rural Mozambique, size of the plot was associated with consumption, with households with bigger farm plots of OFSP consuming more OFSP than those with smaller plots. 17 Various factors may affect production, 16 which may limit the availability of OFSP and thereby affect consumption. Availability of vines is an important factor influencing adoption of OFSP. 21 The Integrating Orange project was the major source for planting material for households, and access to clean vines may be problematic once project funding ends. In Tanzania, projects supplied farmers with planting materials, but the seed systems were not viable after project funding ended. 27 The review by Jenkins and coworkers 16 identified lack of access to quality vines as one of the greatest challenges facing OFSP interventions that promote local production. A current approach in OFSP interventions is to create functional linkages between trained vine multipliers and national programs providing planting material, and efforts are underway to design and implement business plans to ensure that seed systems are viable when project support ends. 28
Only 8.7% of households with children less than 5 years old never ate OFSP, compared to 20.5% of households without children. This association may reflect the effect of sensitizations of mothers during the “under five clinics” as a collaborative effort between the Ministry of Health and CIP in the study area, 29 as providing nutrition information helps to ensure that biofortified foods are integrated into children’s diets. 30 In Malawi, mothers who were sensitized on the health benefits of OFSP, considered them to be good for babies and were willing to feed them to their children. 31
Individuals with knowledge of the benefits of an intervention are usually more likely to adopt the practices that are promoted, in order to prevent the known consequences of not doing so. 32 This was reflected in a study in Kenya, which showed that knowledge on the nutritional value of OFSP was associated with both adoption and intensity of adoption of an OFSP intervention in terms of production. 21 In a study in Tanzania, farmers who were sensitized about the benefits of OFSP were more positive about its superior nutritional value and its popularity among children, indicating that perceptions on OFSP seem to be influenced by awareness and knowledge of OFSP. 33
The observed association between knowledge of the benefits of OFSP and consumption thereof could be attributed to extensive OFSP promotion that was going on in the area. 22 Knowledge on health benefits of foods is an important motivational factor to the dietary choices that individuals make, 32 and knowledge of important attributes of food increases consumers’ choice of the food in their diets. 34 Results of the study showed a sharp increase in the consumption and production of OFSP among the households compared to previous years. The respondents’ knowledge of the benefits of OFSP probably played an important role in enabling them to prioritize consumption of OFSP. However, the type of knowledge and how it affected their decision to produce and/or consume OFSP were not determined in this study. Further research is needed to assess the quality of knowledge that households have and understand the attitudes and practices of households on OFSP.
As could be expected, purchasing of OFSP was associated with the consumption of OFSP. Households that faced challenges in procuring OFSP ate OFSP less frequently than those that did not face challenges. The lack of purchasing power may be a possible challenge that households may have faced, taking into consideration that 40.7% of the people in rural Zambia are very poor. 35
Household demographic characteristics such as household size, age of the household head, and sex of the household head were not related to the consumption of OFSP. This might be because consumption patterns in most households in Zambia are similar, and a previous study has reported that food consumption patterns in Zambia do not vary according to gender of the household head. 4 With regard to the consumption of OFSP per se, a study by Mmasa and Mlambiti 36 established no association between household size and OFSP consumption.
The study was done in an area where OFSP consumption was promoted through the Integrating Orange Project. Although the findings may not be representative of OFSP consumption within the districts, it may be reflective of areas where OFSP are being promoted within similar settings. Assessing meaningful associations with OFSP consumption was limited by the low number of households that did not consume OFSP. Another limitation of the study is that the amounts consumed were not determined. The results do however provide important information on the consumption of OFSP and factors that were associated with the consumption thereof within the Integrated Orange Project, which has been lacking. Due to the cross-sectional design of the study, causality cannot be inferred. The findings of this study can be useful in designing nutritional interventions to increase and maintain an increased consumption of OFSP.
In conclusion, a large percentage of households produced and/or consumed OFSP, reflecting a positive outcome of the Integrating Orange Project that promoted production and consumption of OFSP. The survey was done during the harvesting season, which contributes to the high production and consumption observed. Awareness of VAD, knowledge on the benefits of OFSP consumption, household production of OFSP, purchasing OFSP, and the presence of children less than 5 years in the household were related to consumption of OFSP. Programs promoting OFSP consumption should thus focus on OFSP production and sensitizing households on nutritional benefits of OFSP, and target households with children less than 5 years old as entry point. The challenge will be to maintain the production and consumption of OFSP, and for this promotional strategies focusing on production, marketing and value addition techniques related to OFSP are needed.
Footnotes
Acknowledgments
The authors thank colleagues at the National Food and Nutrition Commission as well as Dr Chipungu and her team at the International Potato Center (CIP) involved in the Integrating Orange Project in Chipata district for their assistance and support during the data collection. The authors thank the enumerators who collected the data and the families in Chipata district who agreed to participate in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.