
Abstract
Background:
Despite varying serum levels of 25(OH)D among schoolchildren in Ethiopia, data are lacking whether this affects their muscle function as measured by handgrip strength of these children. Handgrip strength may be used as a proxy indicator of muscle strength and function. This study evaluated the association between serum levels of 25(OH)D and handgrip strength among schoolchildren in Ethiopia.
Methods:
The study used a data set from a school-based cross-sectional study conducted on a total of 174 randomly selected schoolchildren from urban (N = 89) and rural (N = 85) settings of Adama Town and Adama Woreda, respectively. Handgrip strength, serum 25(OH)D levels, and anthropometry were measured for each child following standard procedures, while data on demographic characteristics of children and their parents were collected using a structured interviewer-administered questionnaire. A multivariable linear regression model was used to determine the association between serum vitamin D level and handgrip strength after adjusting for other predictors.
Results:
The mean handgrip muscle strength of the students was 17.6 ± 6.9 kg. The average serum 25(OH)D for the group was 54.5 ± 15.8 nmol/L. On multivariable linear regression model, serum 25(OH)D level was significantly associated with handgrip strength (β = 0.06, P = .008) of the children after controlling for potential confounders. Other variables, female gender (β = −2.20, P = .004), age (β = 1.97, P < .001), height (β = .22, P < .001), weight (β = 0.33, P < .001), and triceps skinfold thickness (β = −0.19, P = .023), were identified to have significant association with handgrip strength of schoolchildren.
Conclusion:
Serum 25(OH)D levels had significant positive association with handgrip strength of Ethiopian schoolchildren. The results imply the need for incorporating school nutrition education on consumption of foods rich in important nutrients including vitamin D-rich foods in the school curricula and also enhancing behavioral change communication toward exposure to sunlight in the school to produce adequate vitamin D. Further longitudinal study involving a larger sample is recommended to confirm the findings.
Background
Vitamin D deficiency and insufficiency are still reported as frequent problems in children and adolescents worldwide. 1 Deficiency of this vitamin is a global health challenge, with well-known impacts on calcium metabolism and bone health, as the classical action of vitamin D is regulating absorption of calcium and bone mineralization. 2 -4
Vitamin D has many forms; while the most common is vitamin D3 produced from cholesterol in the skin upon exposure to sun light, it can also be obtained from foods. 5 There are 3 forms of vitamin D3: cholecalciferol–the inactive form; calcifediol (25-hydroxyvitamin D), abbreviated as 25(OH)D), which is the best indicator of vitamin D status of individuals; and calcitriol (1, 25(OH)2D3)—the active form which is formed in the kidney after hydroxylation processes. 5,6 The active form (1, 25(OH)2D3) has intestine, bone, and kidney as its traditional target tissues for its classical action in calcium and phosphorus balance and bone structure. 6 The other form of this vitamin is vitamin D2 or ergocalciferol, a provitamin found in foods of plant sources such as sun light–exposed mushrooms. 5 -7 Foods that naturally contain significant amounts of vitamin D3 are mainly of animal origin including liver, oily fish, fish liver oil, and egg yolk. In humans, vitamin D3 is more effective than vitamin D2 at raising serum 25(OH)D concentrations. 7 Although it can be obtained from foods, the primary source of vitamin D for humans is exposure to sunlight. However, its production in the skin depends on season, latitude, time of a day, aging, skin covering clothes, the use of sun block, glass windows, body fatness, and skin pigmentation. 8 -12
Besides its known effects on bone and mineral homeostasis, growing body of evidence suggests that vitamin D exerts a range of effects on skeletal muscle cells. For instance, research findings show that muscle weakness, myopathy, and myalgia are prominent features of individuals with vitamin D deficiency that respond to its replacement. 13,14 Handgrip strength has gained attention as a simple and noninvasive marker of muscle strength and function both in epidemiological and in clinical studies. 15 Schoolchildren are prone to vitamin D deficiency due to reduced exposure to sunlight as they spend most of their day time indoors. Hence, decreased synthesis of vitamin D3 in the skin could put them at increased risk of developing vitamin D deficiency and related health problems including muscle weakness. This effect might be exacerbated by consumption of low vitamin D, especially in settings like Ethiopia where commonly consumed foods contain naturally inadequate vitamin D. This is demonstrated by our previous findings that showed a high prevalence of vitamin D deficiency among Ethiopian schoolchildren in urban (61.8%) and rural (21.2%) settings. 16 Studies on other age-groups also indicated that vitamin D deficiency and insufficiency are commonly prevalent in Ethiopia. 17 -19 There is evidence showing existence of the association between serum vitamin D levels and handgrip strength among adolescent girls in China. 20 However, there are no data on the association between serum 25(OH) D levels and handgrip strength among Ethiopian population including schoolchildren. In this study, we set out to investigate the association between serum levels of 25(OH) D and handgrip strength among schoolchildren aged 11 to 18years in Ethiopia.
Methods
Study Design and Participants
Data for this analysis are taken from the school-based cross-sectional study conducted in Adama Town (N = 89) and Rural Adama woreda (N = 85) from May 20 to June 22, 2013, to determine vitamin D deficiency and its predictors among Ethiopian schoolchildren. Sample size was calculated using formula for estimating 2 population proportions using a power of 80%. Multistage stratified random sampling procedures were used to select study participants from each study setting. Further details including sampling procedure, inclusion/exclusion criteria, and protocol approval and ethics statements have been described elsewhere. 16
Analysis of Serum 25(OH)D Levels
After obtaining informed written consent from the parents/guardians and verbal assent from the children, each child had a finger prick by trained health workers, from which free-flowing blood drops were collected on blood spot cards per ZRT laboratory instructions (www.zrtlab.com). At least 2 such usable (nonoverlapping) drops were collected per participant. After air drying for at least 30 minutes, flaps were closed and placed in the sealed Ziploc bags with desiccant and moisture indicators and taken to Oromia Public Health Research, Capacity Building and Quality Assurance Laboratory by principal investigator for storage at −80°C. Samples were then sent for analysis to ZRT laboratory (Oregon), within 4 days. Circulating serum 25(OH)D was analyzed from dried blood spots, using a standard liquid chromatography/tandem mass spectrometry (LC-MS/MS) assay having intra-assay and interassay coefficients of variation (CVs) of 8.1% to 9.2% and 12% to 13%, respectively. The ZRT Laboratory participates in DEQAS, the Vitamin D Quality Assessment Scheme, which provides control samples to ensure assay accuracy, and the blood spot 25(OH)D determination is deemed equivalent to serum, as stability of 25(OH)D in serum or plasma is high. 21 Cutoffs for deficiency and normal of <50 nmol/L and ≥50 nmol/L were based on consideration of the Institute of Medicine’s Recommended Dietary Allowance). 22 In addition, Holick reported that 25(OH)D levels of 50 to 75 nmol/L represent insufficiency, while levels below 50 and 25 nmol/L represent deficiency and severe deficiency, respectively. Serum 25(OH)D levels of ≥75 nmol/L are generally accepted as sufficient levels. 23
Muscle Strength and Anthropometric Measurements
Muscle strength of the study participants as determined by forearms handgrip strength was measured on both dominant and nondominant hands by well-trained data collector using a BASELINE hydraulic hand dynamometer (model 10602; White Plains, New York, NY) with adjustable widths. Measurements were taken per American Society of Hand therapists’ standardized procedure with the participants in the sitting position on chair and both feet flat and against floor, with their shoulders adducted, their elbows flexed at 90°, and their forearms in neutral position, a methodology that is associated with high intratest and intertest reliability. Finally, the measurements were taken in kilograms and rounded to the nearest 0.1 kg. The standard test protocol uses the mean of 3 strength tests per adjusted width for both hands as the resultant score. 24 Body weight and height were measured using a precision digital scale (model: HD-318; TANITA; Tokyo, Japan) and portable stadiometer, respectively. Children removed their shoes and jackets for height and weight measurements. Weight and height were measured 3 times, and the means were used for analyses. Every morning and prior to each measurement, the weight scale was calibrated with a standard weight, and instruments were calibrated according to the manufacturer’s recommendations.
Socioeconomic Index
Socioeconomic index was developed as follows: First, all study participants were asked about the ownership of fixed assets by their respective households with a score “1” given to those who own the asset and score of “0” given to those who did not own. Then, all items asked were assessed for internal consistency and showed to be reliable with a Cronbach α value of .82. Then, principal component analysis was used to develop wealth index. The first factor was taken and rank ordered into tertiles to give low, middle, and high socioeconomic status.
Statistical Analysis
Data were checked for missing values and outliers and analyzed using SPSS for window (IBM SPSS statistics version 20; Chicago, Illinois). Normality of the continuous variables including age of children, handgrip strength, and serum 25(OH) D levels was checked visually using inspection of the skewness and kurtosis measures of their respective standard errors, histograms, and Q-Q plots of residuals against the predicted values. Measurement values for both handgrip strength and serum 25 (OH) D levels of the students were normally distributed, while age and triceps skinfold thickness (TSF) of children did not have normal distribution. Height and weight of children also had normal distribution. Mean values between groups were compared using independent sample t test and 1-way analysis of variance for normally distributed data. Chi-square tests were used to compare categorical data between groups. After checking all necessary assumptions, we fitted a linear regression model to identify predictors of handgrip muscle strength. We first carried out bivariate analyses to identify candidate variables for the multivariable linear regression model. Then, variables that had P < .25 in the bivariate analyses were entered into multivariable linear regression model using enter method to identify the significant independent predictors of handgrip muscle strength at significance level of .05. All tests were 2-sided, and P values <.05 were considered statistically significant. The results were reported as β coefficients and 95% confidence intervals.
Results
A total of 174 study participants from the schools in 2 settings in Adama Town 89 (51.1%) and rural kebeles of Adama Woreda 85 (48.9%) participated in the study, yielding a response rate of 98%. The median (range) age of the students was 15 (11-18) years. Higher proportions of students were females (56.9%) and in the age-group 15 to 18 years (55.7%) and most (79.9%) of them were Christian by religion. The majority of mothers and fathers had attended a formal education (69% and 55.4%, respectively). Only a small proportion of mothers and fathers were employed (14.9% and 28.7%, respectively). Almost equal proportions of the study participants were from households in low (34.5%) and high (35.1%) socioeconomic status (Table 1).
Characteristics of Schoolchildren in Central Ethiopia.
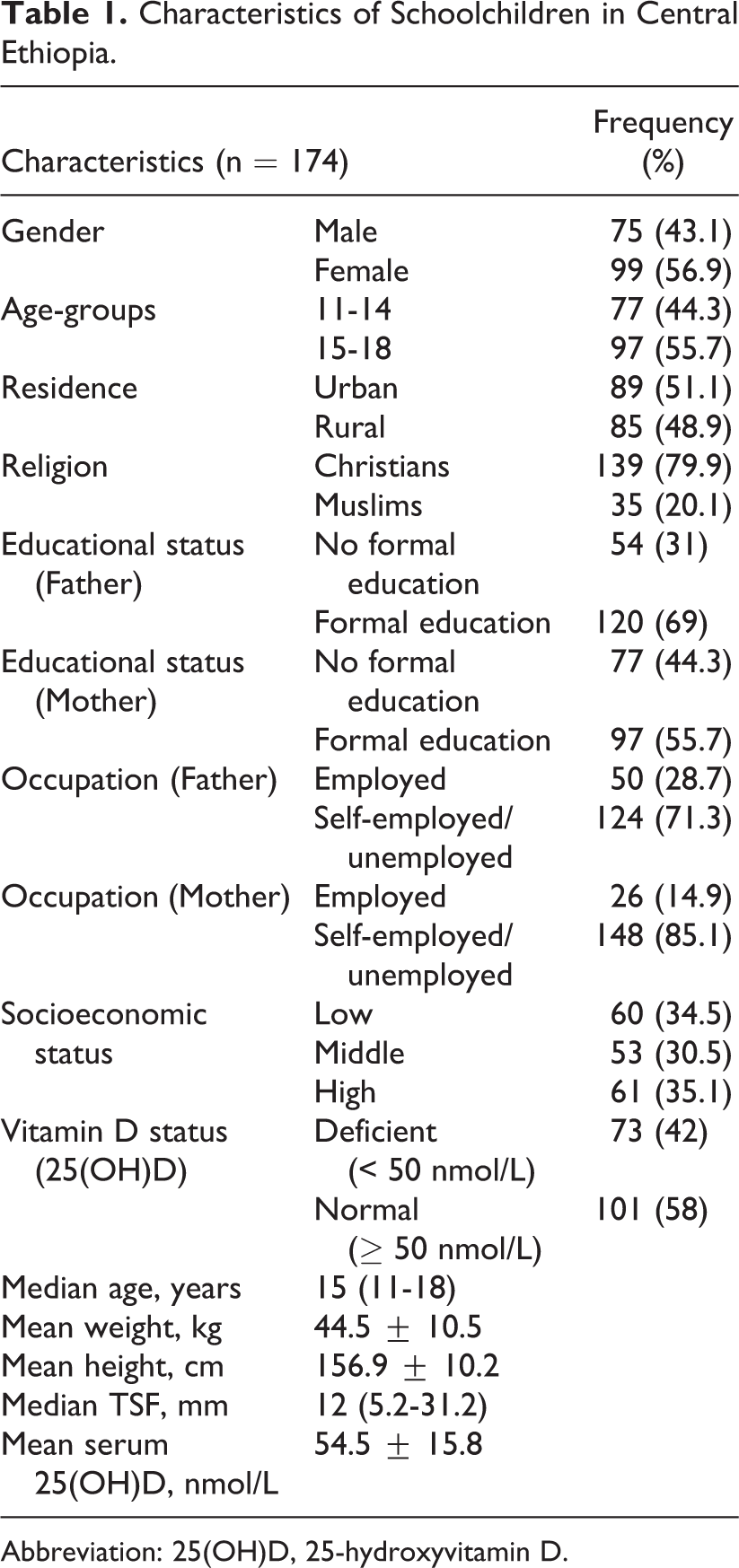
Abbreviation: 25(OH)D, 25-hydroxyvitamin D.
As shown in Table 1, mean values for weight and height of the children were 44.5 ± 10.5 kg and 156.9 ± 10.2 cm, respectively. Their median TSF value was 12 (5.2-31.2 mm). Average serum 25(OH)D for the group was 54.5 ± 15.8 nmol/L.
We also undertook subgroup analysis to characterize vitamin D status among female students (n = 99), where they were classified into 3 different groups. Group I (n = 45) comprised of girls from the schools located in a rural setting, group II (n = 48) included girls from schools located in an urban setting, and group III (n = 6) included girls from religious schools in an urban setting in which Muslim girls wore Hijab as a regular school uniform for a religious purpose. Overall, 51 (51.5%) girls had vitamin D deficiency (serum 25(OH)D <50 nmol/L). Almost all of the girls in group III, 5 (83.3%), had severe vitamin D deficiency (serum 25(OH)D <25 nmol/L), and only 1 girl from this group had serum 25(OH)D level above 50 nmol/L. About one-third and three-fourth of girls from group I and group II had vitamin D deficiency (Table 2).
The Proportion of Vitamin D Deficiency in Female Students Who Live in Rural (Group I) or Urban Areas and Do (Group III) or Do Not Wear Hijab (Group II), Adama Town and Adama Woreda, Ethiopia.
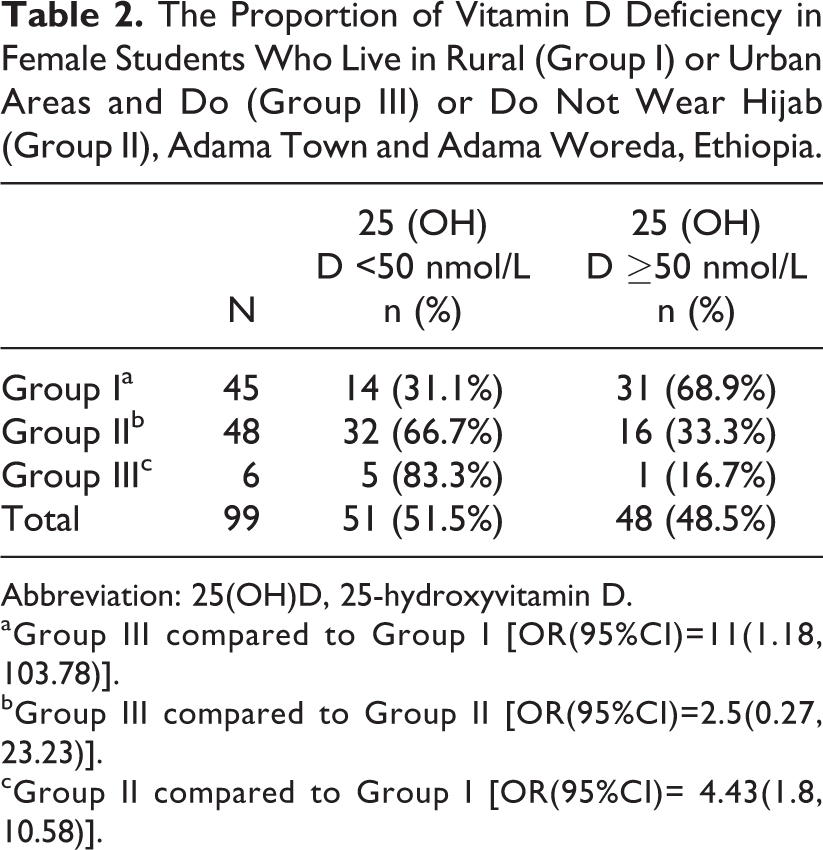
Abbreviation: 25(OH)D, 25-hydroxyvitamin D.
aGroup III compared to Group I [OR(95%CI)=11(1.18, 103.78)].
bGroup III compared to Group II [OR(95%CI)=2.5(0.27, 23.23)].
cGroup II compared to Group I [OR(95%CI)= 4.43(1.8, 10.58)].
When we compare mean serum 25(OH)D concentrations of all 99 females (28 Muslims and 71 non-Muslims) according to their religion, Muslim females had significantly lower serum 25(OH)D levels (40.79 ± 12.61) than serum 25(OH)D levels (53.68 ± 12.08) of non-Muslims (P < .001). We found marginal significance level of 0.06 when we see the association between religion of the girls and their vitamin D status (crude odds ratio [OR] = 2.53 [0.91, 7.02]).
Furthermore, we compared mean serum 25 (OH)D levels of girls in group III with Muslim girls from nonreligious schools and those who did not wear Hijab as regular school uniform (22 female students) but wore school uniform covering forearms and legs during school time. The mean serum 25(OH)D concentration of girls in group III was significantly lower than their counterparts (27.33 ± 13 vs 43.86 ± 9.24; P < .001). The overall severe vitamin D deficiency (serum 25(OH)D <25 nmol/L) was detected only in 6 (3.4%) of the study participants, and almost all of these were Muslim girls from religious schools where the girls wore Hijab as a regular school uniform.
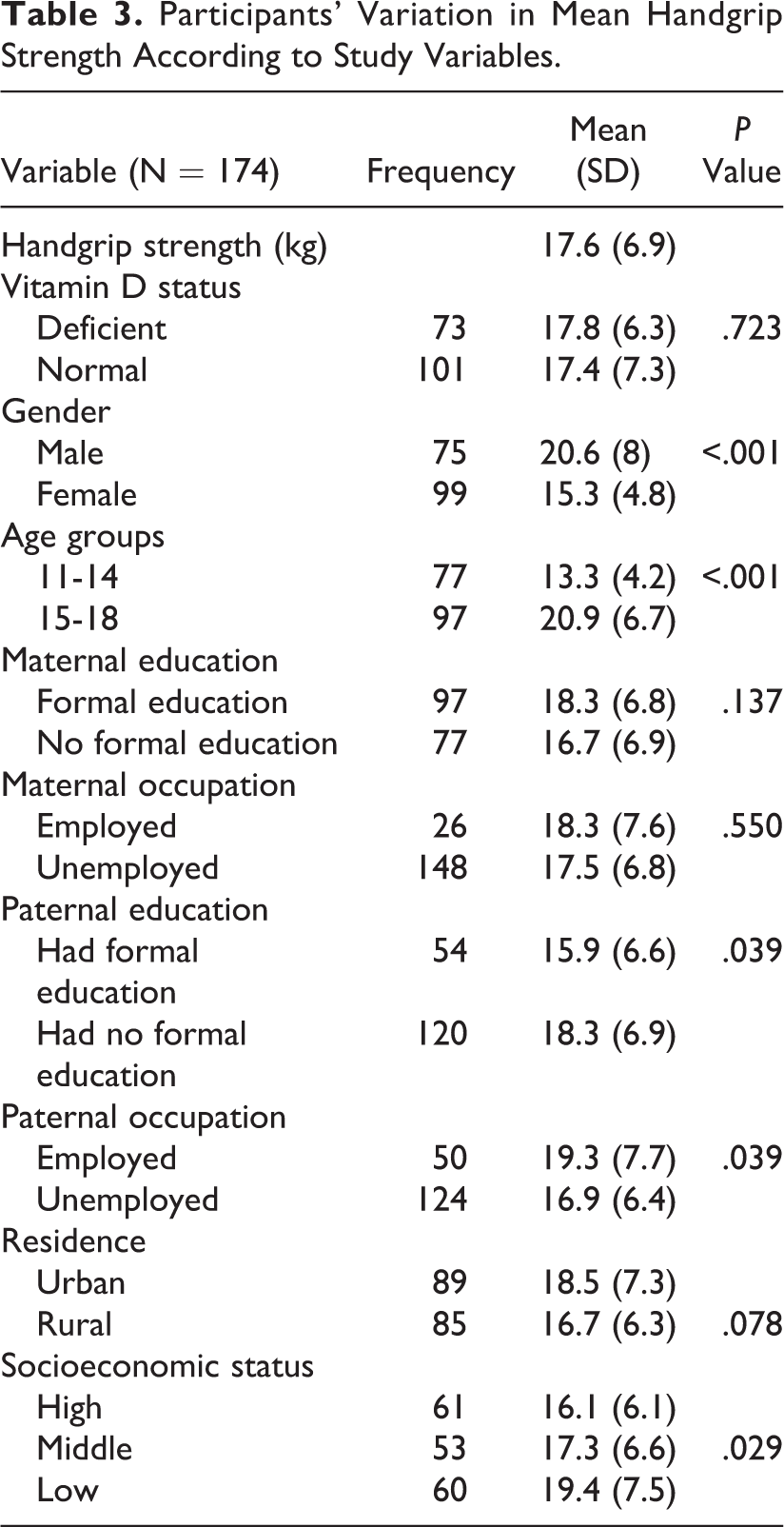
The mean handgrip strength of the students was 17.6 ± 6.9 kg. There were no significant differences in mean handgrip strengths between groups according to their vitamin D status (P = .723). However, significant differences in mean handgrip strength were observed between gender and age-groups of children and their fathers’ education and occupation groups, where children from female gender and lower age-groups and whose fathers had formal education and were unemployed had lower handgrip strength. Mean handgrip strength also varied significantly according to household socioeconomic status of the study participants. Tukey post hoc tests showed that these results were driven by the significantly lower handgrip strength in the high socioeconomic group compared to low socioeconomic group (P = .029); no such significant pairwise differences in mean handgrip strength were found between children from low and middle socioeconomic status groups and high and middle socioeconomic status groups (P = .617 and P = .234, respectively). In addition, differences in handgrip strength of children by maternal education and occupation were not significant (P > .05). There was a trend toward significant difference in handgrip strength according to residence of the study participants (P = .078; Table 3). Serum 25(OH)D level was positively correlated with handgrip strength although the observed correlation was not statistically significant (r = .087; P = .256).
Participants’ Variation in Mean Handgrip Strength According to Study Variables.
In multivariable linear regression analyses, serum 25(OHD) levels, female gender, age, height, weight, and TSF of children were significantly associated with their handgrip strength. Fathers’ occupation of being employed appeared to show a trend toward significant association with handgrip strength of their children after controlling for potential confounders (Table 4).
Multivariable Linear Regression Model Predicting Handgrip Strength Among Ethiopian Schoolchildren.a
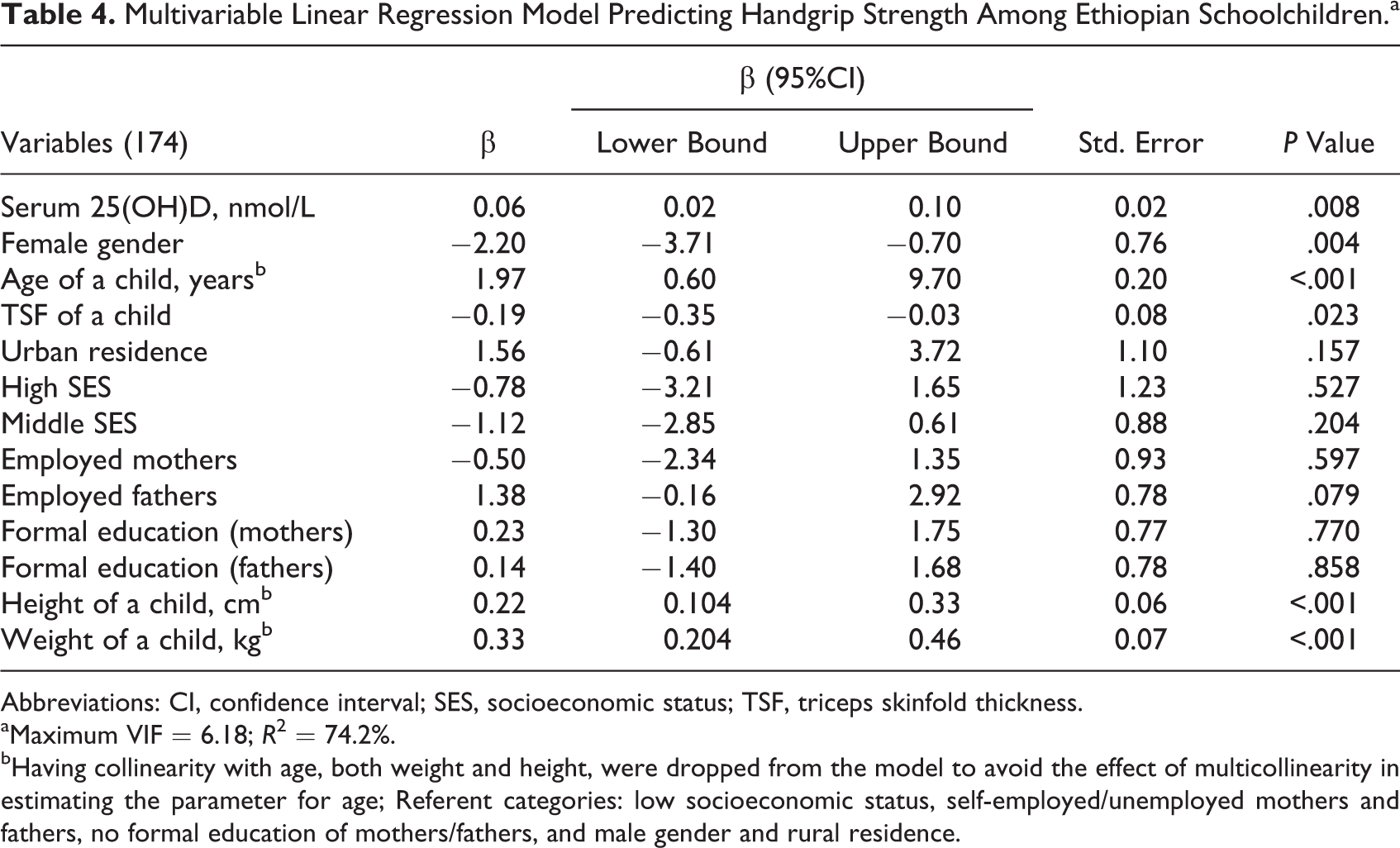
Abbreviations: CI, confidence interval; SES, socioeconomic status; TSF, triceps skinfold thickness.
aMaximum VIF = 6.18; R 2 = 74.2%.
bHaving collinearity with age, both weight and height, were dropped from the model to avoid the effect of multicollinearity in estimating the parameter for age; Referent categories: low socioeconomic status, self-employed/unemployed mothers and fathers, no formal education of mothers/fathers, and male gender and rural residence.
This study showed that serum 25(OH)D was significantly associated with handgrip strength among schoolchildren in Ethiopia. As serum 25(OH)D level of a child increased by 1 nmol/L, child’s handgrip strength increased by 0.06 (β = 0.06; P = .008). Conversely, body fatness was negatively associated with handgrip strength of children; a unit increase in TSF reduced handgrip strength by 0.19 (β = −0.19; P = .023). In addition, sociodemographic factors also had statistically significant association with handgrip strength of children under the study. Being female had negative association with handgrip strength (β = −2.20; P = 0.004), while a unit increase in age increased handgrip strength by 1.97 (β = 1.97; P < .001), showing positive association between age and handgrip strength. Furthermore, height and weight of children had significant association with handgrip strength (P < .001). For a unit increase in height and weight of children, their handgrip strength increased by 0.22 cm and 0.33 kg, respectively (β = 0.22, P < .001 and β = 0.33, P < .001, respectively). Having employed fathers had a trend toward significant association with handgrip strength of their children under the study (P = .079).
Discussion
This study indicated that serum 25(OH)D level had a positive significant association with muscle strength as measured by handgrip strength among schoolchildren in Ethiopia. For a unit increase in serum 25(OH)D level, handgrip strength increased by 0.06 (0.02-0.10) kg adjusting for possible potential confounders on multivariable linear regression model. This association was independent of adiposity, age, gender, weight, and height of children. The modest effect size observed in this study may be due to having subjects with 25(OH)D levels greater than 50 nmol/L (20).
The mechanism through which vitamin D affects muscle tissue is controversial. A growing body of evidence suggests that the active form of vitamin D, 1,25(OH)2D3, exerts its classical actions of regulatory control of mineral homeostasis on cells other than the intestine, bone, and kidney; these other cells include muscle cells. 25,26
Vitamin D exerts its action on target cells through expression of vitamin D receptor (VDR) gene which modulates its actions. 25 -28 The vitamin D receptor (VDR) gene is expressed in human skeletal muscle cell, demonstrating its ability to regulate transcription at this site to influence muscle function. 25,26,29,30 This is further supported by findings from animal model studies confirming the presence of VDR and its expression in muscle tissue in mice where it modulated the uptake of vitamin D by muscle cells. 31,32 Further, vitamin D had the direct effects on the proliferation and differentiation of human skeletal muscle precursor cells, suggesting beneficial effects of vitamin D on muscle performance and strength in humans. 26
It was also reported that VDR knockout mice had significantly weaker grip strength than their controls in animal model studies, possibly showing impaired function of vitamin D in VDR knockout mice. 31 In this study, a similar finding where vitamin D-deficient mice had significantly weaker grip strength than their controls was also reported. 31 On the other hand, VDR polymorphism could have a direct effect on muscle strength may be via modulating vitamin D levels. Bozsodi et al reported a positive association between VDR gene variants and muscle strength among Caucasian schoolchildren. 28 Although we didn’t assess VDR polymorphism in our study participants, evidence shows that variants of the VDR gene were associated with lower vitamin D levels, 33 possibly suggesting that VDR gene polymorphisms might have been linked to varying vitamin D levels and related variation in muscle strength in our study population. 32
Notably, several cross-sectional studies involving adults and younger humans indicate that adequate vitamin D levels positively affect muscle strength. 20,34,35 Hurst et al reported a significant positive association between vitamin D status and handgrip strength in adult women from India. 34 Similarly, a positive association between adequate vitamin D status and higher handgrip muscle strength was reported in the study involving adolescent girls, indicating girls with adequate vitamin D status had significantly higher handgrip muscle strength compared to those with poor vitamin D status. 20 Another cross-sectional study investigating the relationship between baseline vitamin D level and muscle power and force among postmenarchal adolescent girls showed a significant association. 35 The girls were further included in a randomized controlled trial of vitamin D supplementation indicating that muscle function was improved in the vitamin D-treated group and the effect was even greater in girls with the lowest baseline vitamin D levels. 36 Similarly, Gupta et al found a significant positive effect of vitamin D supplementation on muscle strength of young Indians with baseline vitamin D deficiency randomized to either oral cholecalciferol with elemental calcium or dual placebos. 37 On the contrary, some studies fail to demonstrate a significant effect of vitamin D on muscle function in randomized controlled trials of young adults. 38,39 Goswami et al did not find a difference in skeletal muscle strength among young females randomized to vitamin D and/or calcium supplementation in randomized placebo controlled trial. 38 Knutsen et al also reported a similar finding showing supplementation of vitamin D had no effect on muscle strength or power as measured by the handgrip test, jump test, or chair-rising test in the adult population with low baseline vitamin D status. 39 The observed disagreements may be partly explained by the differences in the amount, type, and duration of vitamin D supplementation and discrepancies in the cutoffs to define vitamin D status. Nonetheless, the pooled data from meta-analysis of randomized controlled trials indicates that vitamin D supplementation increases upper and lower limb strength in healthy adult population, suggesting vitamin D could have a significant positive effect on overall muscle function in humans. 5
On the other hand, age, height, and weight of children had significant positive associations with handgrip strength, while this association was negative for adiposity and for being female in our study. These findings are in line with other study findings. In the study by Ploegmakers et al that included large sample of schoolchildren from the northern provinces of the Netherlands, grip strength had a significant association with age, height, weight, and gender of the children. These associations were positive for age, height, and weight; however, a trend in grip strength for boys was found to be stronger than girls showing a negative association between grip strength and being female. 40 The fact that adipose deposition predominates in girls while muscle mass increases in boys during adolescence could explain the observed difference in hand grip strength between the 2 groups. 41 In fact, we reported in our previous finding on the same study population that there was higher likelihood for girls to have higher adiposity that might reduce their grip strength. 42 Similar results have been reported by Souza et al in that grip strength of children increased with their age. 43 In addition, grip strength had positive correlation with fat-free mass and height in this study. 43 A similar finding was reported in older age-group, where grip strength was positively associated with age, height, and weight among study participants aged 20 to 25 years. 44 Moreover, the observed negative association between adiposity as measured by TSF and grip strength in our study could be due to higher degree of fat infiltration in muscle tissue resulting in lower grip strength. 45,46
As shown in Table 2, some participants had severe vitamin D deficiency. These were Muslim adolescent girls attending schools where Hijab was the school uniform. Given our sample size for this subgroup analysis was small (n = 6), further research with larger sample size should be undertaken to examine the association between wearing style and vitamin D deficiency and its subsequent effect on growth among school adolescent girls in Ethiopia.
This is the first study to assess the association of serum vitamin D levels with handgrip strength among Ethiopian population including schoolchildren. In addition, using a standard liquid chromatography (LC-MS/MS) assay to determine serum vitamin D levels could add strength to our study. However, our study has some limitations. The cross-sectional nature of the study limits establishing causal relationship between serum vitamin D levels and handgrip strength in our study participants. Furthermore, lack of adequate data on others important factors that could affect muscle strength including detailed physical activity, calcium, and vitamin D intakes can be considered as limitations of our study.
Conclusion
Serum levels of vitamin D had a significant positive association with handgrip strength among schoolchildren in Ethiopia. The findings imply the need to design preventive strategies to curb the deleterious metabolic effects including muscle weakness that could come due to lower serum vitamin D levels in Ethiopian schoolchildren. This could be done via behavioral change communications among students in the school to have adequate sunlight exposure to produce vitamin D. Furthermore, schools in Ethiopia should incorporate school nutrition education in the curricula to enable students in the school to learn about important nutrition issues including importance of vitamin D to prevent the negative health consequences related to deficiency of this vitamin, including poor muscle development and function, especially in growing children. Further longitudinal study involving larger sample is recommended to confirm the findings.
Footnotes
Authors’ Note
TW and SW equally conceived the idea; TW, SW, and TB designed the study; TW supervised data collection, analyzed and interpreted the data, and drafted the manuscript; SW and TB reviewed the drafted manuscript critically. All authors gave final approval of the manuscript to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.