
Abstract
Background:
Designing effective nutrition interventions for infants and young children requires knowledge about the population to which the intervention is directed, including insights into the cognitive systems and values that inform caregiver feeding practices.
Objective:
To apply cultural domain analysis techniques in the context of implementation research for the purpose of understanding caregivers’ knowledge frameworks in Northern Senegal with respect to infant and young child (IYC) feeding. This study was intended to inform decisions for interventions to improve infant and young child nutrition.
Methods:
Modules from the Focused Ethnographic Study for Infant and Young Child Feeding Manual were employed in interviews with a sample of 126 key informants and caregivers from rural and peri-urban sites in the Saint-Louis region of northern Senegal. Descriptive statistics, cluster analysis, and qualitative thematic analysis were used to analyze the data.
Results:
Cluster analysis showed that caregivers identified 6 food clusters: heavy foods, light foods, snack foods, foraged foods, packaged foods, and foods that are good for the body. The study also revealed similarities and differences between the 2 study sites in caregivers’ knowledge frameworks.
Conclusions:
The demonstration of differences between biomedical concepts of nutrition and the knowledge frameworks of northern Senegalese women with regard to IYC feeding highlights the value of knowledge about emic perspectives of local communities to help guide decisions about interventions to improve nutrition.
Keywords
Introduction
Infant and young child (IYC) feeding and care practices play a critical role in global nutrition and health outcomes for children. 1 These practices are deeply contextual, reflecting the knowledge structures that are embedded in the local culture and customs of communities. 2 Given the central role of knowledge frameworks in caregiving behaviors, a prerequisite for designing interventions to improve IYC nutrition is understanding the insider, or emic, cognitive models that underlie caregivers’ feeding and care behaviors regarding their children. This study of caregiver knowledge and perspectives about IYC foods and feeding in northern Senegal was undertaken as part of a larger research effort to identify and guide the development of nutrition interventions that would be appropriate for local Senegalese contexts. It aimed specifically to understand how caregivers in northern Senegal structure their knowledge of and perspectives on foods for IYC feeding. The article presents the results of a focused ethnographic study that employed cognitive mapping techniques, in conjunction with qualitative interviews, to understand the cognitive systems of caregivers with respect to IYC feeding.
Identifying and selecting appropriate research methods is a critical challenge for investigators who need to examine the knowledge systems and structures. A number of techniques and methodologies are available, including in-depth individual interviews, focus groups, and surveys. Among the available methods, each has benefits and limitations. For this study, we used “cultural domain analysis,” a form of cognitive mapping. This technique has the advantage of providing an efficient means of examining the cognitive, social, and cultural domains—or categories—by which individuals organize their knowledge, and it does not require literacy. 2,3 As a component of mixed methods research, cultural domain analysis can offer useful insight into the cognitive systems of caregivers by melding quantitative measurements with qualitative interview data.
Pile sorting is a technique for cultural domain analysis that is commonly used in cognitive anthropology. During a pile sorting exercise, participants organize and evaluate their cultural domains using visual aids, such as cards or pictures. 4,5 They sort cards that contain visual representations and/or text of “items” and group them into piles based on their perceived similarities or differences. This method provides information from the perspective of the target population, without the risk of undue influence or bias inadvertently introduced by imposing the external knowledge system of the investigator. Pile sorting reveals relationships among items that might not be explicitly articulated by respondents in qualitative interviews alone and provides quantifiable results that can be used for comparison across groups. Thus, it provides insight into values, societal norms, and cultural expectations in the community. 3 Additionally, another advantage of pile sorting is that it is more efficient than traditional cultural domain interviewing procedures that require complex, iterative questioning frames.
Investigators can draw from several alternative pile sorting techniques. A more structured version may use terms derived from previously conducted “free listing” exercises, which are used to create a standardized card deck. In less structured versions, each participant may be asked first to freely list all terms related to a specific topic. 6,7 Respondents may be directed to sort cards into piles based solely on their individual preferences or into piles based on predetermined categories. 6,8 The physical act of sorting cards creates a visual representation of how elements of interest are thought about and the perceived similarities and differences between them. In addition to the sorting results, respondents’ discussions with interviewers during the process (a form of qualitative interviewing) provides invaluable insights to augment the quantifiable pile sorting results.
Pile sorting has been used to reveal perceptions on many different topics, including gender norms, 8 HIV, 9,10 malaria, 11 and diabetes. 12 It has been particularly useful in nutrition research for illuminating the conceptual frameworks that underpin nutritional knowledge, including emic perspectives that contribute to food decision-making processes. 3,13 –17 As efforts to address malnutrition among infants and young children continue to evolve, pile sorting has emerged as an innovative tool for understanding caregiver decisions about complementary feeding. For example, Rodriguez-Oliveros and colleagues 3 used this technique in their study of complementary feeding in Mexico to understand how mothers perceived local foods. The utility of emic perspectives for designing and implementing interventions that are responsive to the cultural context and local behaviors has been reviewed within the larger context of using ethnography in nutrition and public health. 18 –20
Methods
Study Setting
Two sites in the Saint-Louis Region of northern Senegal were selected for this study: the rural community of Didjiery and the larger, peri-urban community of Gaé. Both sites fall within the Dagana district of Saint-Louis, located along the Mauritanian border, roughly 400 km north of Dakar, the capital city. Rates of stunting (13.2%), wasting (8.4%), underweight (13.7%), and anemia (56.9%) among children in Saint-Louis emphasize the importance of formative research to inform nutrition interventions in this region. 21
Study Design
The study was framed with protocols from the Focused Ethnographic Study for Infant and Young Child Feeding Manual 22 and was organized into 2 phases. In phase 1, a sample of key informants participated in a free listing exercise that identified the foods selected for the subsequent phase. In phase 2, caregiver respondents completed a pile sorting activity. During both phases, recorded interviews yielded extensive text for analysis with standard qualitative techniques.
Phase 1: Free listing
In phase 1, 80 key informants (40 in each study site) were asked to “free list” foods that are appropriate for IYC in various age categories. Free listing is a technique used to initiate an exploration of a cultural domain. 5,23 –25 The free listing exercise began with a neutral question: “First, I would like to ask you about how infants are fed. I would like to know the types of foods that are given to infants (about 6-8 months) when they begin to eat solid food in addition to breast milk. While you’re thinking, you can begin by telling me about the food you give (gave) to your own infant.” Next, the interviewer asked the same question for other age-groups: 9 to 12 months, 13 to 18 months, 19 to 24 months, and 25 to 59 months. The interviewer also asked key informants to describe foods that are not appropriate for IYC in each age category, along with their perceptions of the feeding practices of other mothers and caregivers from their communities.
Phase 2: Pile sorting
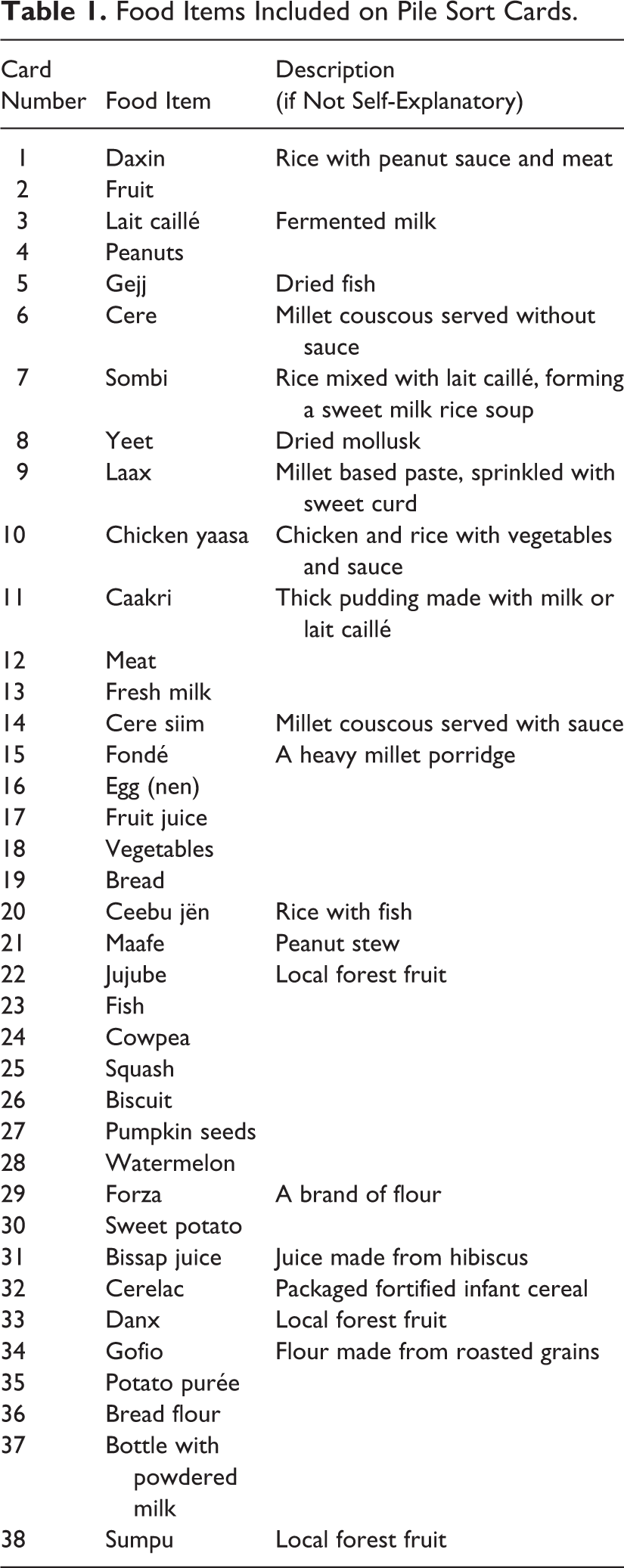
In phase 2, 22 caregivers in Didjiery and 24 in Gaé participated in cognitive mapping interviews. They were presented with a set of 38 cards displaying images of food items that were selected based on the results of the free-listing exercise (Table 1). In order to avoid respondent fatigue, the complete list of food items elicited in phase 1 was reduced by identifying food items that were most commonly listed at each study site as well as across both study sites. These reduced lists were used to create the food cards for phase 2. In order to maintain consistency with local context, the research team used photos of food items taken in local markets on the food cards where possible. When that was not possible, the local research team used images from the Internet. Although this iterative approach to data collection facilitated the use of community perspectives to guide the research process, it is not without limitations. As Blake et al note, “the inclusion or exclusion of selected foods or the decision to represent multiple levels of categorization on the food cards may [result] in the emphasis and inhibition of some categories.” 14 (p508)
Food Items Included on Pile Sort Cards.
Following the procedure recommended by Pelto and Armar-Klemesu, 22 we asked caregivers to sort the cards into piles of foods that they felt “belonged together” (Pulaar: “mo yadata”; Wolof: “yu annd”). No a priori categories were imposed by the researchers, and the respondents were free to organize the piles as they wished, based on their own criteria. The researchers then asked caregivers about the rationale for each of the piles they had created, and the results were audio-recorded.
Data Collection
Data collection took place during July 2015. Following training on the study protocol, interviewers visited the 2 study sites and conducted all interviews in the local languages, Wolof and Pulaar, according to the preferences of participants. All key informants and caregivers provided written informed consent, and a Senegalese ethics committee (Comité National d’Éthique pour la Recherche en Santé, Ministére de la Santé et de l’Action Sociale, Sénégal) provided ethical approval for the study. All interviews were audio-recorded with respondent permission.
Samples
A total of 126 key informants and caregivers were interviewed. The key informants were community members who were considered knowledgeable and experienced with regard to IYC feeding and care practices. They were primarily mothers of infants and young children (64 of 80) but also included community health workers and grandmothers (16 of 80). The caregiver respondents were mothers or other individuals responsible for the feeding and care of an infant or child between 6 months and 5 years of age. Caregivers of children with disabilities or chronic illnesses were excluded from the sample. Respondents were purposively selected to represent a diversity of child age-groups and economic statuses. Specifically, for each study site, the investigators aimed to select at least 12 caregivers with children between 2 and 5 years as well as 3 caregiver respondents for each of the following child age categories: 6 to 8 months, 9 to 12 months, 13 to 18 months, and 19 to 24 months. Local health facility workers assisted with the identification of key informant and caregiver respondents and facilitated introductions between the data collection team, village chiefs, and community members. The sample size for this study was driven by recommendations from Pelto and Armar-Klemesu’s Focused Ethnographic Study of Infant and Young Child Feeding Manual 22 as well as considerations regarding saturation sampling. The researchers continued to interview key informants and caregivers in both study phases until thematic redundancy had been achieved. Saturation was determined through consistent review of the transcripts for emergent themes and regular meetings for discussion among the research team.
Data Analysis
Audio-recordings from interviews were checked for quality, transcribed, and translated from the Wolof and Pulaar languages into French by Helite. Investigators coded qualitative data in NVivo (version 10) according to standard qualitative analytical practices. 26
The quantitative data from the pile sorting exercise were analyzed using the software R-Cmap, a concept mapping package for R. 27 The data from each participant’s piles were analyzed according to the methodology described by Kane and Trochim. 28 The software first created a similarity matrix for each respondent’s piles by converting each pile into a 1-0 co-occurrence. Next, the similarity matrix was used for a multidimensional scaling (MDS) analysis. The purpose of MDS is to provide a visual representation of patterns among items—in this case, different food items—that are considered to be similar to one another by respondents. 29 This analytical process produced a graphical output of the clusters that represents the proximities between individual items in the aggregated matrix. Accordingly, items that are often grouped together appear closer on the spatial R-CMap output, whereas those that are grouped together less frequently are further apart. Stress values were calculated to capture the degree to which the map represents the original input similarity matrix data. For this study, stress values below 0.205 were considered low given that studies estimate that 95% of concept mapping projects likely yield stress values between 0.205 and 0.365. 28
As with factor analysis or other types of cluster analysis, the investigators select descriptive labels for the clusters. We used several steps to do this. First, the research team considered the physical characteristics of the food items in each of the clusters. Next, these initial observations were supplemented with qualitative analysis of the discussions recorded during the pile sorting exercise, which had been conducted to provide an understanding of the respondents’ rationales for the piles that they created but also facilitated the labeling of the piles. Finally, the food group clusters were shared with the field team and PATH researchers. They were asked to independently assign their own names to the clusters based on their personal contextual knowledge, including experiences with the data and study participants. To arrive at the final cluster names, the study team synthesized this information to create the names used in this article.
Results
Characteristics of the Sample
Interviews were conducted with 80 key informants (phase 1) and 46 caregivers (phase 2), sampled such that each of the 5 child age-groups was represented. Because of low population numbers in Didjiery, it was possible to locate only 1 caregiver respondent with a child 13 to 18 months old. Table 2 shows the characteristics of the sample by site and type of respondent (key informant or caregiver). All respondents were women and represented a wide range of ages—and consequently, degrees of childcare experience. Of note, most respondents (68%) declined to provide an average monthly income. Differences in household characteristics reflect the more rural status of Didjiery compared to peri-urban Gaé.
Characteristics of the Sample, According to Location and Type of Respondent.
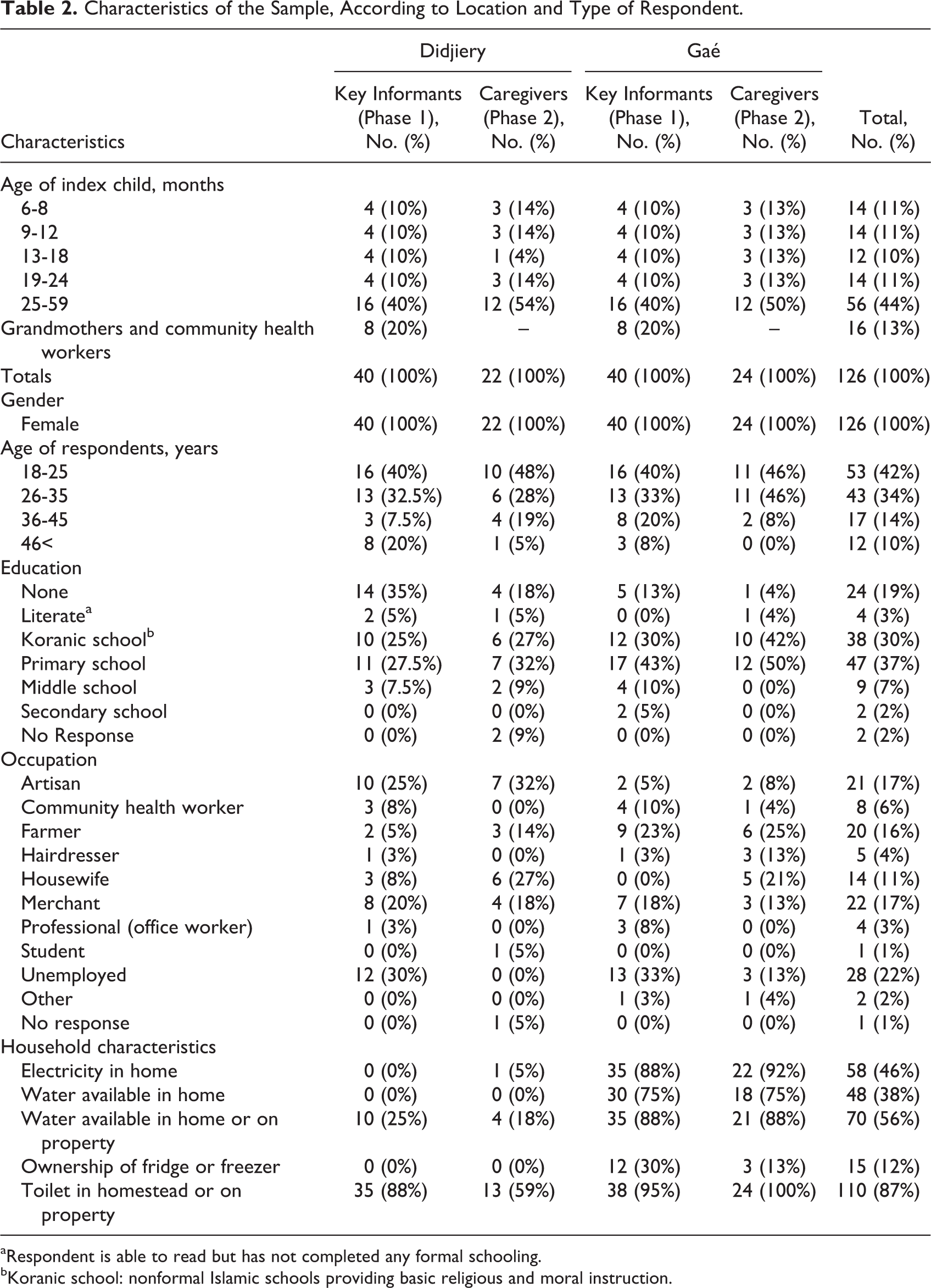
aRespondent is able to read but has not completed any formal schooling.
bKoranic school: nonformal Islamic schools providing basic religious and moral instruction.
Results of the Free-Listing Exercise: Age of Introduction of Foods for Infants and Young Children
During phase 1, key informants from Didjiery spontaneously listed 69 different food items that are appropriate to feed to IYC between 6 and 59 months of age. In peri-urban Gaé, 92 foods were named. Table 3 lists the food items mentioned by at least 5 respondents as being appropriate for IYC feeding in each child age category.
Food Items Mentioned During the Free Listing Exercise by At Least 5 Respondents as Being Appropriate for Infants and Young Children, According to Location and Child Age Group.
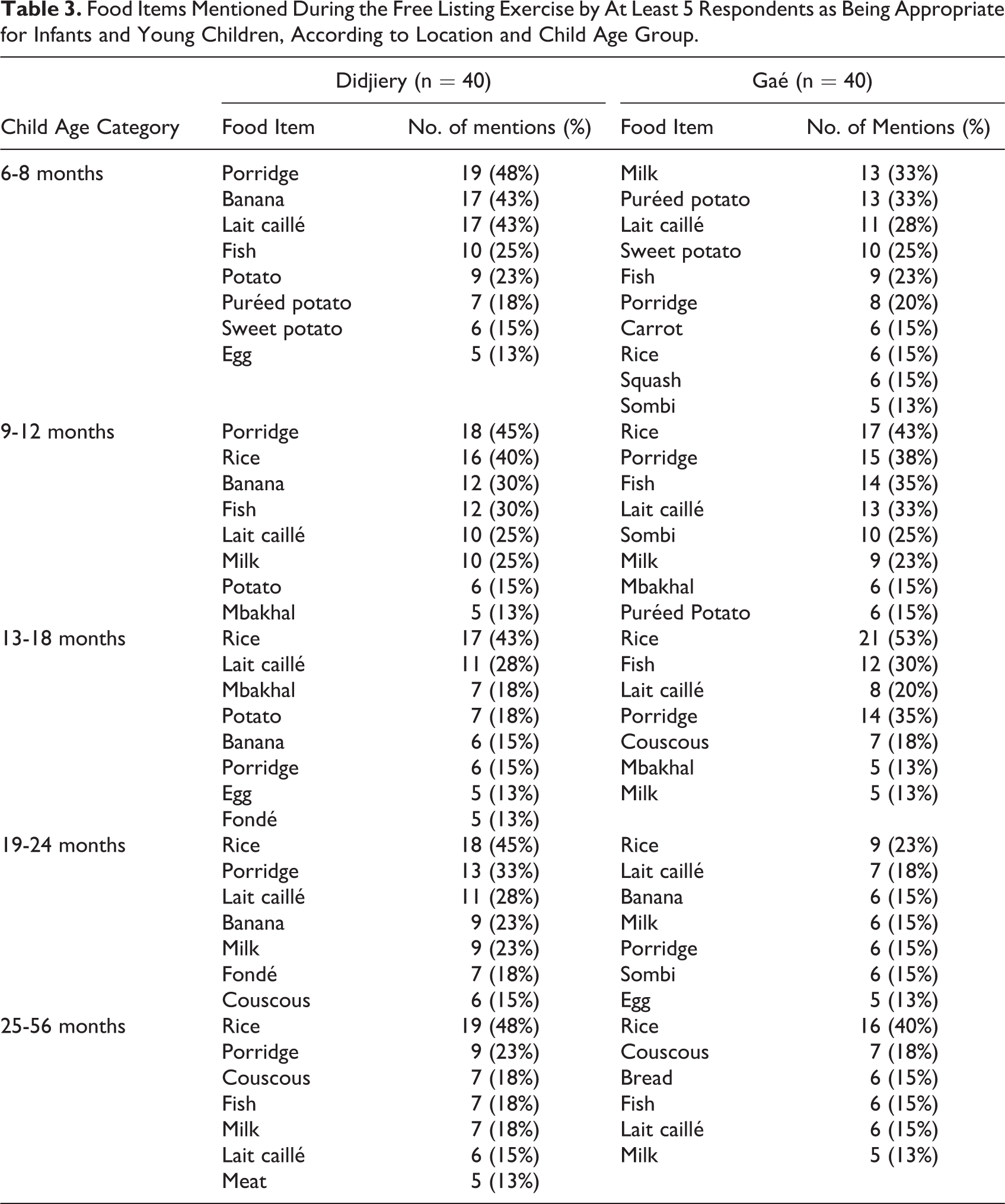
For infants aged between 6 and 8 months, key informants listed soft food items, such as porridges, milks, and purées of potatoes or other vegetables. For infants 9 to 12 months of age, key informants reported more solid food items, such as rice, and suggested larger quantities of foods. For children between 13 and 18 months of age, 33% of key informants mentioned that children eat “what the family eats.” These more substantial meals might include rice, couscous, and sauces served with or without meat. For children more than 2 years old (25-59 months), 54% of key informants mentioned feeding children the same foods as the rest of the family.
While key informants in both communities listed soft animal source foods that can easily be consumed by IYC—such as milk products and eggs—as being appropriate for various child age-groups, more “chewy” animal source proteins (ie, meat from cows, chickens, or goats) were listed for older age-groups. Specifically, in rural Didjiery, meat was commonly listed as being appropriate for the older age-group (25-56 months), but it was not listed by more than 5 key informants in Gaé for any of the child age-groups.
Cluster Analysis of Pile Sorting Results
Table 4 shows the results of the cluster analysis, documenting at an aggregate level how the 38 food cards tended to be sorted in each of the 2 locations during phase 2. As discussed in the Methods section, we used an iterative procedure to name these clusters. In Didjiery, the clusters were heavy foods, light foods, snack foods, and foraged foods. In Gaé, the clusters were heavy foods, light foods, snack foods, packaged foods, and foods that are good for the body.
Food Clusters Identified by Caregivers during the Pile Sorting Exercise, Together With Corresponding Cluster, According to Location.
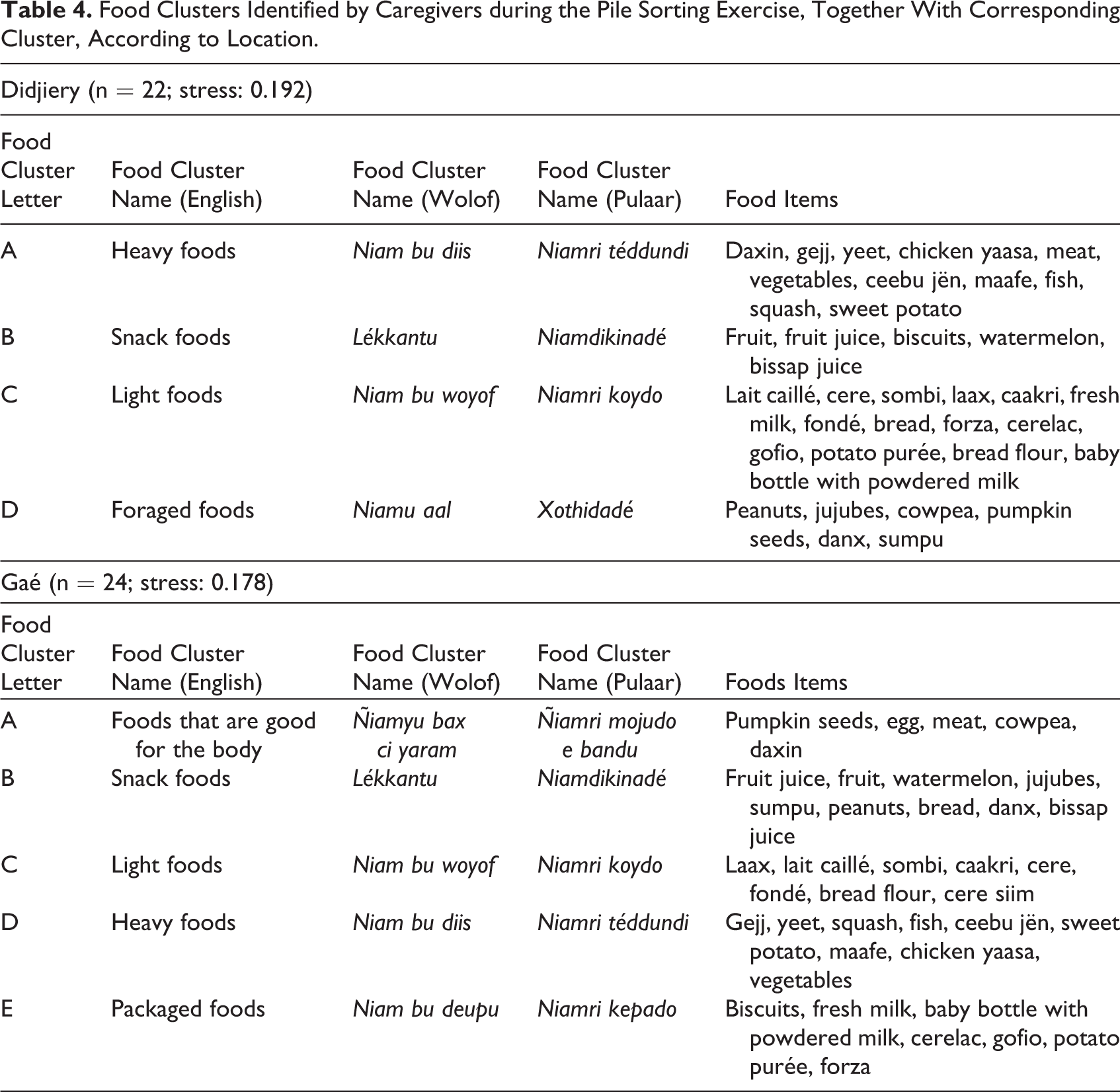
Heavy foods
Certain similarities in food groupings emerged in both communities. In both Gaé and Didjiery, caregivers identified a cluster that we refer to as “heavy foods” (Pulaar: “Niamri téddundi”; Wolof: “Niam bu diis”). This group contains traditional family meals, such as chicken yassa and mafé, or ingredients commonly used to make those meals, for example, vegetables, fish, and squash. Further, the concept of “heaviness” also imbues these food items with specific qualities: They are considered harder to digest and so are eaten during the day rather than in the evening before sleeping. Additionally, the “heavy” food items in these clusters were generally described as being less appropriate for children, particularly those younger than 2 years of age. For example, 1 caregiver from Gaé noted: “There are foods that are not good for the child. I can say foods such as potato, which is a bit heavy for the child…a child should not eat it.”
The results of the free-listing activity are also instructive for interpreting the pile sorting results. With respect to the “heavy foods” cluster, many key informants said “heavy” foods were appropriate for the older child age categories but less suitable for infants—particularly those between 6 and 9 months of age. For example, 1 key informant from Gaé explained: “I believe that my child who has no teeth cannot eat rice. I do not give my child rice at this age because it is too heavy for him. As his body cannot handle it, I will not give him rice. I give my children light foods until they are one year old.”
Light foods
In both Didjiery and Gaé, another cluster consisted of “light foods” (Pulaar: “Niamri koydo”; Wolof: “Niam bu woyof”). This cluster includes milk- or porridge-based foods, such as lait caillé, caakri, and fondé. A caregiver from Gaé succinctly explained her rationale for placing these types of foods together in a pile:
“Why have you put milk and caakri together in this pile?”
“These are light foods.”
Light foods are softer or less substantial meals or food items that are considered easy to digest and better for young children. As one caregiver from Gaé suggested, “Food that is not light is not recommended for children.” Another caregiver from Gaé noted, “These are the foods that are lighter for children. They are lighter in their stomachs and they digest quickly.”
Key informants identified light foods as appropriate for IYC in all age categories, especially for children younger than 12 months of age. Food items from the “light” clusters were more frequently listed as being appropriate for IYC in younger age categories and were used as complementary foods along with breastfeeding. As 1 key informant from Gaé said, “In my opinion, until a child reaches his first year, one must give him food that is somewhat light.”
Snack foods
Another category that emerged in both the rural and the peri-urban locations is one that we have labeled “snack foods” (Pulaar: “Niamdikinadé”; Wolof: “lékkantu”). These are foods that need little or no preparation and can easily be given to children between meals or while they play outside. Food items in this cluster include fruits and juices. According to one mother from Didjiery, foods like these “go together” because “there is nothing that one cooks: you peel and give it to the child.” Similarly, a mother from Gaé explained the rationale for one of her piles by stating: “These are snack foods and they have the same origin. This is why I have put them together.”
Foraged foods and packaged foods
The categories of foraged foods and packaged foods are particularly interesting because each of them only occurred at one of the study sites and not the other. Thus, foraged foods (Pulaar: “Xothidadé”; Wolof: “Niamu aal”) was a category in Didjiery but not in Gaé, and packaged foods (Pulaar: “Niamri kepado”; Wolof: “Niam bu deupu”) was a separate category in Gaé but not in Didjiery. In Didjiery, respondents created a group that contained foraged foods and foods taken from fields that are generally available without the need for market transactions. This cluster includes food items such as fruits, nuts, and legumes. Respondents’ comments about this pile included statements such as “they come from trees and can be picked” or “they are picked in the same manner.” Foraging is more likely to be part of the household livelihood strategy in rural Didjiery. By contrast, in Gaé, packaged foods fell into a cluster that included Cerelac, Gofio, and Forza—all of which are commercial brands of infant cereal or flour. Additionally, powdered milk, biscuits, and potato purée are also sold in packaging. As one caregiver from Gaé explained, “These are the foods that one buys.” In Didjiery, these foods were placed in other clusters rather than sorted into their own specific cluster. However, the qualitative interview data reveal that foods in both the “foraged foods” and “packaged foods” clusters were spoken about in quite similar ways: They have the advantage of being ready—or almost ready—to eat. In other words, these are foods that are convenient to prepare. As such, they may actually serve similar functions in the different local contexts.
Foods that are good for the body
Another cluster, “foods that are good for the body” (Pulaar: “Ñiamri mojudo e bandu”; Wolof: “Ñiamyu bax ci yaram”), appeared only in the peri-urban location. Food items in this cluster were pumpkin seeds, egg, meat, cowpea, and daxin (a local meal made with rice, peanut sauce, and meat). In contrast to the other groupings, this classification is not based on the type of food or where it comes from. Instead, the common factor is the effect that this food has on the body—for instance, helping children to grow well and be healthy. From an etic perspective, these are all foods that are rich in protein and other nutrients. While the word “protein” was not used verbatim by respondents, the fact that residents of Gaé categorized these seemingly disparate foods together may indicate a degree of understanding about nutritional qualities of certain foods and their physiological effects. For example, 1 caregiver from Gaé explained her rationale as follows:
“And why have you put the following foods together? Cowpea, meat, and egg?”
“If someone falls ill, they say that you should give them meat. Sometimes they also tell you to buy cowpea, and if you don’t have the means, you can buy some eggs to give them.”
The results from the key informant interviews are similarly supportive of caregivers’ motivations for sorting these foods together. For example, when discussing the appropriateness of cowpea for IYC between 25 and 56 months, one key informant from Gaé said: “Sometimes if I have cowpea, I boil it and feed it to him [the child]. Cowpeas give him strength. A child should eat foods that give him strength.”
Spatial map of food clusters
Figures 1 and 2 represent the food clusters in the form of geometric shapes. These are the outputs from the proximity analysis in which shape indicates the consensus strength for the food items in a group; thus, a smaller size indicates a stronger (or “tighter”) consensus among respondents. The proximity of each dot to the center of the shape signifies the degree of consensus for that individual food item; foods closer to the center of the shape have a stronger consensus among respondents for “belonging with” the group.
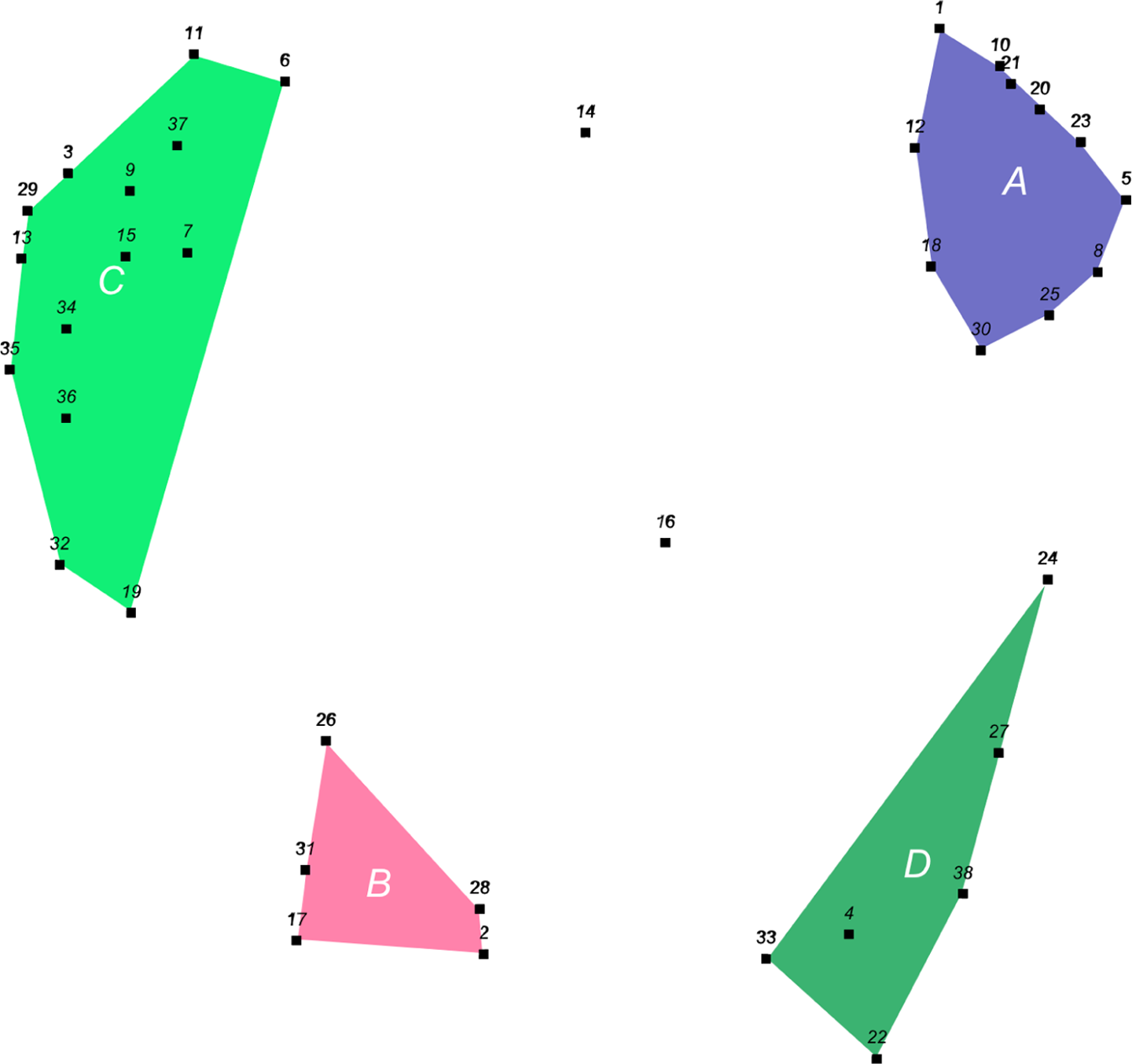
Spatial representation of food groups identified by caregivers of infants and young children in Didjiery (n = 22; stress = 19.2%). 1The shape size in the figure indicates the consensus strength for the food items in a group (ie, a smaller size indicates a stronger, or “tighter,” consensus among respondents regarding which food items should be grouped together). The proximity of each dot to the center of the shape signifies the degree of consensus for that individual food item; foods closer to the center of the shape have a stronger consensus among respondents for “belonging with” the group. Stress values are reported at the bottom of the figure. 2 Refer to Table 1 for the corresponding food items that are represented by numbers in the figure shapes. Refer to Table 4 for the names of the food clusters represented by letters on the figure shapes.
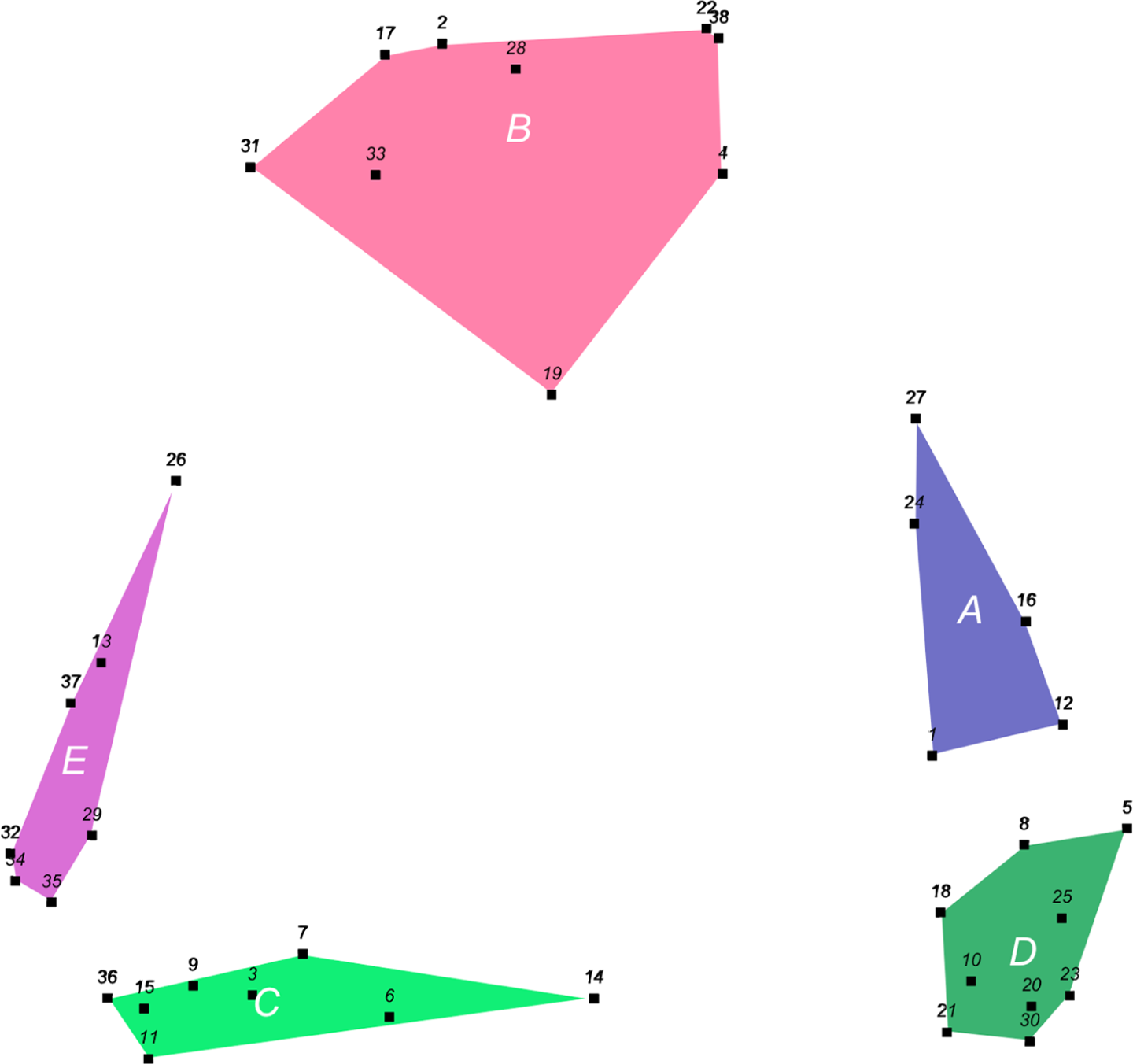
Spatial representation of food groups identified by caregivers of infants and young children in Gaé (n = 24; stress = 17.8%). 1The shape size in the figure indicates the consensus strength for the food items in a group (ie, a smaller size indicates a stronger, or “tighter,” consensus among respondents regarding which food items should be grouped together). The proximity of each dot to the center of the shape signifies the degree of consensus for that individual food item; foods closer to the center of the shape have a stronger consensus among respondents for “belonging with” the group. Stress values are reported at the bottom of the figure. 2Refer to Table 1 for the corresponding food items that are represented by numbers in the figure shapes. Refer to Table 4 for the names of the food clusters represented by letters on the figure shapes.
In Didjiery, there is significant consensus about the clusters for heavy foods, snack foods, and foraged foods. The items in the light foods cluster are relatively more dispersed in Didjiery, suggesting less agreement here in the way that these foods were sorted. In Gaé, there is a relatively strong consensus around all of the clusters, with the exception of the snack foods group. The overall stress values are 0.192 and 0.178 for Didjiery and Gaé, respectively.
Discussion
The purpose of this study was to use cultural domain analysis exercises, augmented by qualitative interviews, to describe the knowledge frameworks of northern Senegalese caregivers with respect to foods and feeding. This descriptive study was one component of a larger implementation research effort, which included investigations into other factors (particularly barriers and challenges to good IYC feeding practices, as well as issues related to food safety and food production). Taken together, these data and insights would be used to inform the selection and design of nutrition interventions to improve IYC nutrition.
The results reveal cultural features of caregivers’ knowledge frameworks and document both commonalities and differences between the rural and the urban communities. Caregivers in both communities created clusters for “heavy” and “light” foods, indicating the centrality of these concepts in their knowledge frameworks. The notion that foods have heavy or light characteristics is one that finds resonance in the anthropological literature on dietary choices and beliefs, where these concepts have emerged as common cultural attributions. 3,30 –32 In northern Senegal, these concepts are clearly relevant in the domain of IYC feeding. Foods that are considered light, or easy to eat and digest, are also the ones that are thought to be particularly suitable as complementary foods for infants and young children younger than 12 months of age. Also, as Sukkary-Stolba 31 observed, when demands on caregiver time and resources are high, “light” foods are often preferred because they require less work to be made. Recognizing that heavy family foods contain the necessary nutrition for children but that light foods are more acceptable, one implication for nutrition interventions is the potential value of introduction of handheld infant food grinders to turn stewed meats into thick pastes for young children to eat. Additionally, some of the staple foods that are regarded as “light” have a soft consistency that makes them particularly amenable candidates for home fortification interventions. These foods include lait caillé, fondé, laax, sombi, and caakri.
Related to caregivers’ perspective on the time savings of light foods, the larger issue of convenience also emerged in our study, but it appears indirectly and differently in the 2 locations. Cross-culturally, there is growing attention to the significance of convenience as a basic factor in women’s IYC feeding decisions. 33 Here, we find a situation of rural/urban differences that has significance with respect to intervention design. In the rural area, “packaged foods” are not conceptually a part of caregiver knowledge frameworks. In other words, they are not a part of local culture. An intervention that involves new, packaged foods is likely to be more readily acceptable in urban or peri-urban areas compared to rural areas. However, if convenience is an important underlying value of foraged foods (the category that was only found in rural Didjiery), this feature can also be stressed with respect to foods that are similar to foraged foods or foods that are planted in gardens and fields alongside of staple foods. Therefore, it is probable that the concept will also be useful in communicating with rural caregivers.
At the same time, the meaning of the cluster we have named “foods that are good for the body” is notable. This conceptual category was found only in peri-urban Gaé. That occurrence, coupled with the absence of a corresponding cluster in rural Didjiery, may reflect a type of culture change that is associated with greater education and/or greater exposure to nutrition messages, including exposure to such messages in health-care facilities. 34 The presence of this cluster in the knowledge frameworks of caregivers provides a foundation for communicating directly about new foods from the perspective of their nutritional qualities and benefits. In rural areas, providing caregivers with understandable information about nutritional concepts may be a prerequisite before one employs the concept of “being good for the body” to promote new foods or food preparations.
With respect to the issue of community consensus, the statistical findings on “stress values” are noteworthy. For Didjiery and Gaé, the stress values were 0.192 and 0.178, respectively. These stress values are low, which indicates a reasonable statistical fit and a moderately strong degree of consensus within each community. This finding is important not only for intervention planning for northern Senegal; it also contributes to the need for broader empirical knowledge about the more general issue of intracultural diversity and the design of nutrition interventions. 35,36
We have suggested previously that the degree and nature of intracultural diversity should be examined as part of implementation research to assist program development. 37 In developing the behavior change communication component to support IYC interventions for northern Senegal, further investigation is warranted to better understand the intracategory variation with respect to how caregivers perceive food clusters. Both the similarities and the differences in the clusters created by caregivers in Gaé and Didjiery can be harnessed to structure these messages. We have indicated previously how the concepts of “heavy” and “light” foods, snacks, and “good for the body” could be used to shape message content.
The study results demonstrate that caregiver cognitive frameworks, which comprise an important aspect of their broader “knowledge frameworks,” diverge from the ways in which foods are usually conceptualized from a western, biomedical perspective, wherein nutritional scientists typically organize foods according to their taxonomic, nutrient, or biological properties. 38,39 Evidence of the biomedical paradigm can be seen in the US Department of Agriculture’s Food Guide Pyramid—a common and widely recognized symbol of this approach to food categorization. 38,39 Rather than grouping foods into categories such as fruits, vegetables, carbohydrates, or proteins, for example, caregivers in this study discussed foods in terms of their origins, packaging, purpose, convenience, and classifications as “heavy” or “light.” Clearly, multiple knowledge frameworks influence how individuals in different contexts and cultures organize information about food.
As is the case for all methods that attempt to understand the “cognition” of others, particularly the cognitive models of people who speak a different language and live in a different culture, the cultural domain analysis techniques we employed have significant limitations. For example, the necessity for the translation of words to images is a limitation of pile sorting. In doing so, the researchers assume that the photos on the food cards map straightforwardly onto the verbal signifier given in the free listing exercise. However, this is an assumption. To minimize the potential for bias from this limitation, when possible, we used photos from local markets to represent the food items.
Another limitation is respondent fatigue. Participating in these exercises is demanding and it is possible that respondents may become less focused on the exercise as time progresses. This could result in rushed or less thoughtful responses at the end of the interview compared to the beginning.
The data revealed some differences between Didjiery and Gaé. These differences may stem from differences in the cognitive maps of the peri-urban people in Gaé compared to those of the Peuhl people in Didjiery who have pastoralist lifestyles and culture. A limitation of our study is that we do not have sufficient data to definitively determine the magnitude of significance of the differences for intervention planning. At a different level of concern is the more general theoretical problem of how broadly the results from 2 field sites can be generalized to other communities in Northern Senegal. In other words, additional research is needed to assess the generalizability of our findings for different communities and contexts.
Our intention in this article has been to illustrate the application of cultural domain analysis as a feasible method for obtaining emic data on caregiver perceptions and “knowledge systems” within the context of implementation research to develop appropriate interventions to improve IYC nutrition. The use of cultural domain methods, together with the more classic approach of open-ended interviewing and exploration of meanings, provides extended opportunities to understand how caregivers organize and structure their knowledge. Applying these insights in the development of interventions is the next step. For these communities in northern Senegal, our findings suggest that more nuanced and differentiated interventions, as opposed to a “one-size fits all” approach, are likely to be more appropriate. 16 –18
Footnotes
Authors’ Note
GP, MP, PM, and IW contributed to the study design. IW, TN, AMD, and MP coordinated the study and managed the data collection. SZ, NK, and BW analyzed the data. SZ, NK, GP, MP, and BW drafted the report. All authors contributed to manuscript revisions.
Acknowledgments
The authors thank Helite and their staff who collected the data in local languages (Wolof and Pulaar). Special thanks also go to Fatou Wéllé and Maimouna Ba for their efforts in communicating with the local communities to arrange participant interviews. Many thanks to Elizabeth Fox for the statistical analysis of the pile sorting results and for introducing us to the RStudio program for pile sorting. Also, thanks to Dr Haim Bar for creating the R-Cmap program and graciously making it available as shareware. Finally, the authors thank the many participants and community members who contributed their time to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a grant from the Bill & Melinda Gates Foundation, Seattle, WA.