
Abstract
Background:
Assessing micronutrient powder (MNP) consumption is the key for monitoring program performance; no gold standard exists for assessing consumption in nutrition programs.
Objective:
To compare estimates of MNP consumption assessed by maternal report versus observed unopened MNP sachets in the household.
Methods:
Cross-sectional household surveys of children aged 6 to 23 months were conducted to assess an MNP project in Nepal; eligible children received 60 sachets per distribution. Mothers reported the number of sachets consumed and showed unused sachets. Directly observed difference (DOD) of MNP consumption was calculated by subtracting the number of observed unopened sachets from 60. Spearman correlation coefficient, categories of MNP consumption, and end digit preference were assessed.
Results:
A total of 205 mothers did not show remaining unopened sachets despite reporting that all were not consumed. For the remaining 605 children, median consumption was 60.0 sachets by DOD and maternal report; the correlation coefficient was 0.91. With consumption grouped into categories of 0 to 14, 15 to 29, 30 to 44, and 45 to 60 sachets, the percent categorized into the same groupings by DOD and maternal report was 100%, 80.6%, 80.7%, and 91.2%, respectively. Excluding those who consumed 60 sachets, 16.9% and 8.0% by report and 14.2% and 6.1% DOD, ended with 0 and 5, respectively.
Conclusion:
Had the observation of unused sachets been used alone to assess MNP consumption, 205 children would not have been assessed. Estimates of MNP consumption by DOD and maternal report were similar in this population with high intake adherence.
Introduction
Micronutrient powders (MNPs) are vitamins and minerals in powder form that can be mixed into any ready to eat semisolid food with an aim to improve the quality of the diet. The World Health Organization recommends the use of MNP to address anemia and iron deficiency in young children aged 6 to 23 months. 1 In 2013, MNPs were distributed in over 60 public health programs in low-income and middle-income countries. 2
Assessing MNP consumption is a key component of monitoring to describe program performance and indicate whether adjustments are needed to support recommended consumption so that participants receive the maximum benefit. 3 There are no biological indicators to assess MNP consumption in program settings. The least costly and most logistically feasible methods include asking participants or their caregivers to report the number of MNP consumed and counting unopened MNP sachets at participant homes. 3 –5 Other methods include directly observed use and saving used sachets. These latter 2 methods are sometimes used in research settings but can be resource intensive for program staff. Additionally, keeping opened sachets can be culturally unacceptable and may result in difficulties with sachet disposal. Thus, these methods are not generally considered for MNP programs. 3,6,7
Limitations of maternal report to assess MNP consumption include the potential for social desirability bias; recall bias, which may increase with a longer recall period; not reporting when MNPs are shared with others, lost, or thrown out; and end digit preference where people have the tendency to round their numeric answers regarding the number of sachets consumed so that they end in a 0 or 5. 5,7 Due to these limitations, Rah et al suggest triangulating reported MNP consumption with observation of MNP sachets 8 when assessing MNP consumption in programs. The purpose of our analysis is to compare mother’s report of the child’s consumption of MNP sachets with observation of unopened sachets in the household, which were collected as part of a monitoring survey in an MNP pilot project in Nepal.
Methods
Setting/Design
Integrated infant and young child feeding and MNP pilot project
As part of an integrated infant and young child feeding (IYCF) and MNP pilot project, 60 MNP sachets were distributed to all children aged 6 to 23 months every 6 months. Mothers were instructed to give their children 1 MNP sachet daily until they consumed all 60 sachets (2 month supply) and then to return in 4 months for the next batch of 60 sachets. If they stopped giving the MNP for any reason, they were encouraged to restart and complete the 60 sachets. Additional details about the pilot program and monitoring surveys are published elsewhere. 9
Survey design
As part of program monitoring, representative cross-sectional household surveys were conducted by an external organization between September and November, 2011. Because of the staggered roll out of the project across districts, data were collected in Rupandehi and Parsa districts (plains ecozones) 3 months after program implementation and in Makwanpur and Palpa districts (hills ecozones) 15 months after program implementation.
Population proportion to size sampling was used to randomly select 30 clusters from rural areas in each of the 4 district and 30 clusters across the urban municipalities of Rupandehi and Parsa districts; no data were collected in urban areas of Makwanpur and Palpa. In each cluster, 12 children aged 6 to 23 months were randomly selected and their mothers were invited to participate in an administered questionnaire interview. All survey participation was voluntary, and women gave informed consent that was witnessed and recorded. The protocol was approved by the Nepal Ministry of Health and Population. We used deidentified data for this secondary analysis.
Assessing consumption of MNP
The survey questionnaire focused on assessing knowledge, attitudes, and practices of the mother of the selected child in relation to the IYCF/MNP pilot program. Among mothers reporting the child ever received a batch of MNP sachets, consumption of MNP was assessed by (1) the interviewer asking the mother to report the number of MNP sachets consumed by the child from the most recent batch of 60 sachets received followed by (2) the interviewer asking to see any MNP sachets in the household and recording the number of unused MNP sachets observed.
Analytic sample
Overall, 1712 children were recruited for assessment; 710 were excluded from this analysis because mothers reported not receiving any MNPs. Of the remaining, 1002 children whose mothers reported that they had ever received MNP; 186 children were excluded because they received the MNP sachets less than 2 months ago, 6 because of missing maternal report of MNP consumption, and 205 because the mother reported the child did not consume all 60 MNP sachets but did not show the remaining MNP sachets in the household. The remaining 605 children were included in the analysis. A total of 330 (55%) of mothers in the analytic sample reported that the child had consumed all 60 sachets; they were still asked to show remaining sachets and 0 was recorded if none was shown. None of these mothers showed any remaining sachets in the household. Compared to the 605 children included in this analysis, the 211 children who had received the MNP 2 months prior but were excluded from the analysis because they did not have complete data were more likely to be older.
Statistical analysis
Data were analyzed using SAS 9.3 (SAS Institute Inc, Cary, North Carolina), accounting for clustering and weighting. The directly observed difference (DOD) of MNP consumption was calculated by subtracting the number of observed unused sachets in the household from 60 sachets (total amount given with each distribution). Since the data on consumption were skewed, the median is presented and median differences between DOD and reported consumption at the individual level are reported. The association between reported consumption and the DOD of MNP was computed using the Spearman correlation coefficient. To further compare reported consumption and DOD, we grouped consumed MNP into the following categories—0 to 14, 15 to 29, 30 to 44, and 45 to 60 sachets. We further compared the percentage of maternal report of sachets consumed and DOD that ended in 0 and 5 to examine potential end digit bias.
Results
Approximately half of the children were male and about half were 12 to 17 months old. Fifty-eight percent of mothers had no education or primary education only, and 35% of mothers belonged to the lowest or second lowest wealth quintiles (Table 1). All mothers reported that they received 60 sachets of MNP in the most recent batch. Median DOD was 60.0 sachets (inter quartile range (IQR): 34-60), and median maternal report of consumption from the last batch was 60.0 sachets (IQR: 44-60). At the individual level, the median difference between DOD and reported consumption was 0 sachets (IQR: 0-0). More than half (54.5%) of mothers reported that the child had consumed all 60 sachets, whereas 58.5% had consumed all 60 sachets by DOD. The correlation coefficient between the DOD and maternal report estimates was 0.91. With MNP consumption grouped into the following categories—0 to 14 sachets, 15 to 29 sachets, 30 to 44 sachets, and 45 to 60 sachets, the percent categorized into the same groupings by the DOD and maternal reported consumption was 100%, 80.6%, 80.7%, and 91.2%, respectively (Table 2). Overall, the number of reported sachets consumed ending in 0 or 5 was 441 (67.9%) and 33 (5.5%), respectively. By DOD, 421 (69.6%) and 25 (4.1%) of sachets consumed ended with 0 and 5, respectively. Since the reported or DOD number of sachets ending in 0 may have been largely driven by children who consumed all 60 sachets, we additionally excluded children whose consumption was 60 sachets by either method; 16.9% and 8.0% reported number of consumed sachets ending with 0 and 5, respectively, whereas by DOD, 14.2% and 6.1% ended with 0 and 5, respectively. Only 14 (2.8%) mothers reported pressure to share the MNP with other children (results not shown).
Characteristics of Nepali Children and Their Mothers.a
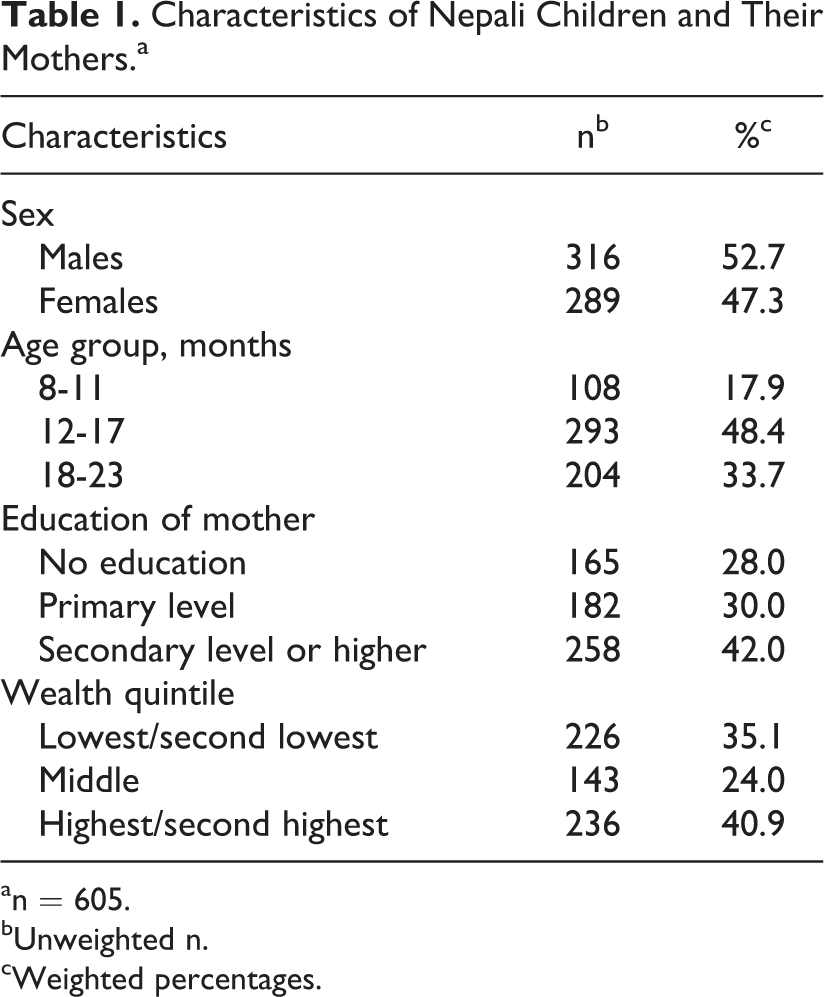
an = 605.
bUnweighted n.
cWeighted percentages.
Comparison of the Directly Observed Difference (DOD) of Micronutrient Powder (MNP) Consumption and Maternal Reported MNP Consumption by Categories of MNP Sachets Consumed.a
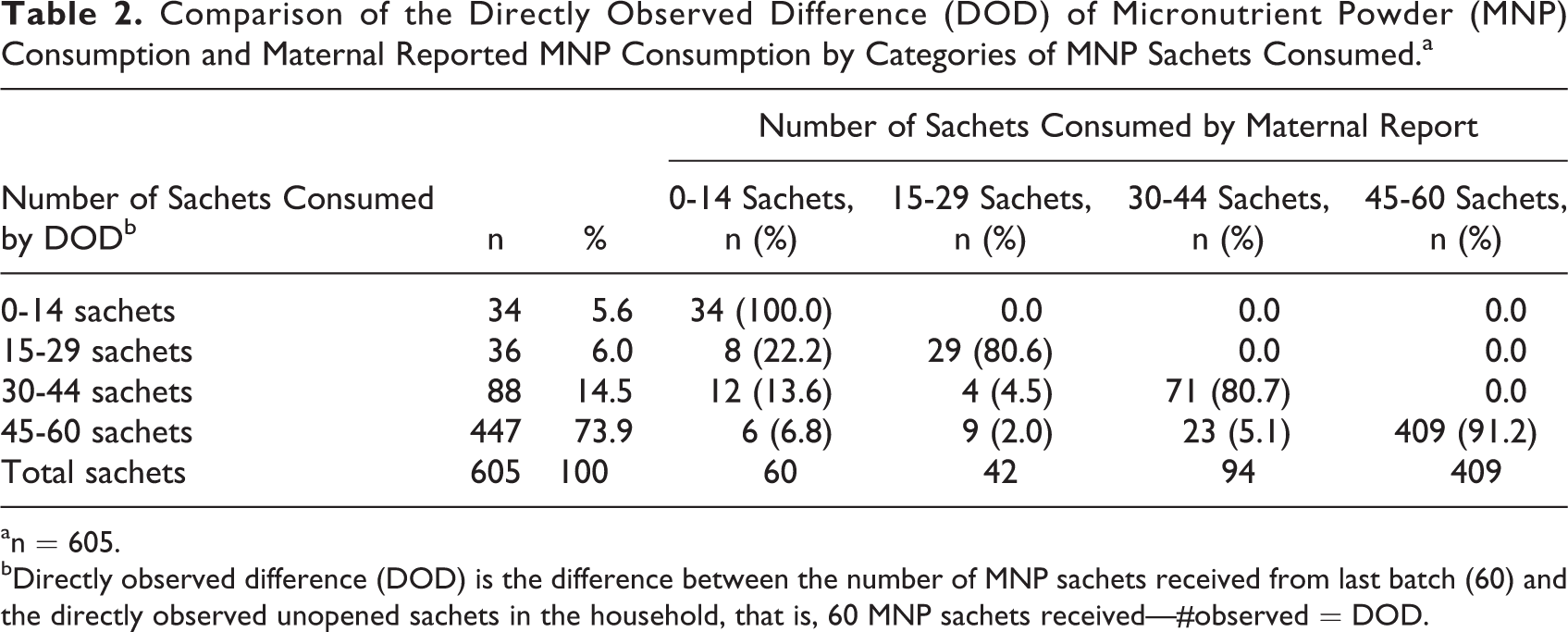
an = 605.
bDirectly observed difference (DOD) is the difference between the number of MNP sachets received from last batch (60) and the directly observed unopened sachets in the household, that is, 60 MNP sachets received—#observed = DOD.
Discussion
Both maternal report and direct observation of unopened sachets are commonly used to assess MNP consumption for young children in public health interventions. All mothers reported that they received the correct number of MNP sachets (60 sachets) during the last MNP distribution, which is critical in the interpretation of both direct observation difference (DOD) as well as reported consumption of MNP. There was no difference in the estimate of median consumption of MNP by maternal report or DOD method when assessing MNP consumption among children 6 to 23 months of age in an IYCF/MNP pilot program in Nepal. There was also a positive correlation between reported consumption and DOD. When we further classified MNP consumption into categories, estimates based on maternal report and DOD generally fell in the same categories. Our estimate of potential end digit reporting bias found that 68% of mothers stated that the child consumed an amount of MNP ending in 0 and 6% reporting a number that ended with 5. After further excluding the children whose mothers had reported consumption of 60 sachets, the proportion of sachets reported consumed that ended with 0 reduced by 51 percentage points; from 67.9% to 16.9% and the resulting estimates of reported consumption that ended with 0 or 5 were similar to those for DOD. This suggests that maternal reported end digit preference may have been minimal since DOD counts of unused sachets are unlikely to be influenced by end digit preference.
A substantial number of mothers could not show the remaining sachets in the household even though they reported that they did not feed their children all 60 sachets. These findings suggest that 205 children or approximately 20% among those reporting MNP coverage of 60 sachets would not have been assessed if consumption of MNP had been assessed by observation of the unused sachets alone. In contrast, only 6 mothers did not report the number of sachets consumed. Although the reasons for not showing the remaining sachets were not collected during the assessments, they may include discarding of or losing the sachets, sharing sachets with someone other than the eligible child, or caregiver unwillingness to show the remaining sachets. Furthermore, we assumed that those mothers who reported that the child consumed all 60 MNP and did not have any sachets to show had given all 60 sachets to the child. In the event that the number of reported sachets was incorrect and that remaining sachets were not shown because they were either lost, misplaced, or because the mother did not want to show the remaining sachets, this may have led to over reporting of reported consumption. Both maternal report and observation of unused sachets in the household are subject to bias if sachets are shared with nontargeted individuals 5 ; however, we found that very few mothers reported that they had pressure to share the MNP with other children who were not the focus of the intervention. The finding that the 2 methods yield similar results and that maternal report was able to assess a large proportion of children may suggest that reported consumption may be used alone in assessing MNP intake without an extra burden on the health-care worker to carry out DOD in MNP programs.
Although our findings suggest a potential use of self-report for monitoring MNP intake in routine program settings, it is important to note that these assessments were carried out through external monitoring surveys and information was collected by trained field data collectors, an approach that is resource intense and that may not be feasible under the regular programmatic conditions. Possible ways of integrating the assessment of MNP intake in regular nutrition programs may include program staff interviewing mothers on intake when they return for a refill of the MNPs. However, this may introduce bias especially if the interviewer is also the health-care worker who counseled the caretaker on MNP use. Further evaluation of the feasibility of integrating self-report of consumption in routine nutrition programs is therefore needed.
Strengths of this study include the large representative sample of children from a public health program setting that allowed us to restrict the analysis to children who had received the intervention for a 2-month period. This study has some limitations. Consumption of MNP was high in this population, and findings may vary in settings where consumption rates are lower. Also there is no gold standard for assessing MNP consumption and we therefore could not assess which of the 2 methods of assessing MNP consumption is more accurate. Another limitation is that in the event that the 710 (41%) whom we excluded incorrectly reported not receiving any MNPs, this may have introduced selection bias. Also, in the comparison of maternal report and DOD, we excluded 205 children whose mothers could not show unopened sachets for counting. Considering that mothers were asked to report the number of MNPs consumed before they provided the remaining sachets for counting, this may have influenced the number of sachets they were willing to show introducing social desirability bias. Had this analysis included these 205 children, we do not know how this would have influenced the results of the estimates of MNP consumption. These data are cross-sectional and therefore we could not assess consumption of MNP at other time points during the intervention. Finally, our findings are not generalizable to other districts of Nepal besides pilot regions. If the program had been implemented on a large scale, the results of the assessment may have yielded different results.
More analyses comparing logistically feasible and low-cost MNP consumption assessment methods are needed to better understand the best ways to assess MNP consumption in public health program settings.
Footnotes
Authors’ Note
This manuscript is the authors’ original work and has not been submitted for publication elsewhere. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention, UNICEF, or the Government of Nepal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Nepal Ministry of Health and Population and UNICEF Nepal Country Office supported the implementation of the pilot intervention. UNICEF Nepal funded an external agency to conduct the monitoring surveys described in this analysis.