
Abstract
Background:
Iodine deficiency is the world’s single most important cause of preventable mental retardation. In Ethiopia, the knowledge and perception of food handlers toward the iodized salt consumption (ISC) was very low.
Objective:
To assess knowledge and perception of food handlers toward consumption of iodized salt in Wolaita Sodo town and Sodo Zuria woreda, 2014.
Methods:
The community-based cross-sectional study design was done from May 10 to May 30, 2014 in Sodo town and Sodo Zuria woreda (district), Wolaita zone, southern Ethiopia. Systematic sampling techniques were used to identify study participants. Data entered into the software Epi Info version 3.5.3 and analyzed using the software SPSS version 16. To assess an association, odds ratio was used at 95% confidence interval, whereas confounding was controlled by employing multivariate logistic regression.
Results:
Lower knowledge and perception on iodine deficiency was observed. About 239 (44.7%) of the respondents had good knowledge and 228 (42.6%) had positive attitude toward consumption of iodized salt. Most (346, 64.7%) of the participants had heard about goiter, whereas only 170 (31.8%) of them associated it with iodine deficiency. About 46.4% of respondents heard about iodized salt. Respondents’ age, education, family income, place of residence, and occupation had significant association with good knowledge and positive attitude toward consumption of iodized salt.
Conclusion:
The study revealed the existence of knowledge and perception gap in iodine deficiency disorder and ISC. Household income, education of respondents, and place of residence were determinant factors for poor knowledge and perception of iodized salt. Therefore, efforts to scale-up the knowledge and perception toward ISC should focus on households with low income, educational level, and rural residence.
Introduction
Iodine deficiency is the world’s single most important cause of preventable mental retardation in children. 1 About 2 billion people would be affected by iodine deficiency disorders (IDDs) in the absence of iodized salt in developing countries. 2,3 In addition, about 38 million newborns in developing countries yearly remain at risk of the brain damage related to IDDs. 2 These IDDs affect a child’s ability to learn and later life via preventing children, communities, and nations from fulfilling their potential. 4
Iodine deficiency is a serious public health problem in Ethiopia. According to the International Council for the Control of Iodine Deficiency Disorders (ICCIDD), Ethiopia is one of the top iodine-deficient countries in the world where about 66 million of its people are apt to the risk of IDDs; about 12 million school-age children live with inadequate iodine in Ethiopia. 5
To solve the problem of IDD, correction of iodine deficiency is the most important and simplest method. 6 And this is achieved through universal salt iodization (USI)—the addition of suitable amounts of potassium iodate to all salt for human and livestock consumption and that all age, socioeconomic, cultural, and religious groups throughout the year utilize salt universally. Iodized salt is both a preventive and curative means for iodine deficiency and is the most effective, low-cost, long-term solution to a foremost community problem. 4,7
Endemic goiter, one of the visible manifestation of IDD, 3,4 was the major health problem in Ethiopia that the national prevalence of goiter rate was 36% in woman and 35% in children. 8,9 The South Nations Nationalities and Peoples Region (SNNPR) had the highest (71%) proportion of goiter prevalence rate compared to other regions of Ethiopia, 8 though there are some areas with medium goiter prevalence. 10,11 The problem of goiter was significant in Wolaita Sodo town, the current study area where about 50.5% of school children were having goiter, 12 whereas World Health Organization (WHO) stated that a goiter rate of more than 5% represent a public health problems. 7
In Ethiopia, according to Ethiopian Public Health Institute 2014 survey report, availability of iodized salt at the household level was very high (95%) but less than half (43%) of these were adequately iodized. 13 Therefore, the country is at risk of IDDs and elimination of IDDs is a critical development issues and should be given the highest priority by governments and international agencies. 3
In addition to USI, the ICCIDD recommends an advocacy plan and a communication strategy designed to support elimination and sustain the change it brings to address iodine deficiency at national level. The creation of awareness to public authorities and general public includes sustaining knowledge and information about the values of iodine in the diet and the dangers of its absence. 2,3
Several community-based surveys conducted elsewhere on knowledge and perception of iodized salt consumption (ISC) show variation from country to country. In Kazakhstan, only 33% of urban and 24% of rural women were aware that the use of iodized salt could prevent IDD, although almost 70% had heard of iodized salt. 14 In India, study conducted among the poor and the disadvantaged district shows very low (15%) participants knew the benefits of iodized salt. 15 In Ghana, only one-third of the respondents indicated that the intake of iodized salt is important to cure goiter. 16 Studies conducted in rural Sidama zone, southern Ethiopia, 17,18 and north Gondar of Ethiopia 19 revealed that only 6%, 12%, and 25% of the participants knew the benefits of iodized salt, respectively. Moreover, the same studies showed that knowledge on cause and prevention of IDDs was very low. 17 –19 Similarly, the reasons mentioned for not using iodized salt was mainly lack of knowledge according to the study done in Ghana and northern Ethiopia. 16,19
As stated, above studies in the southern part of Ethiopia showed little knowledge on IDD and ISC and the absence of information from the current study areas on their important aspects and evidence of high prevalence of goiter among school children; the current study aimed at filling this gap. Thus, the current study assessed knowledge and perception of food handlers toward consumption of iodized salt and its associated factors.
Materials and Methods
Study Setting and Context
The study was conducted from May 10 to May 30, 2014 in Wolaita Sodo town and Sodo Zuria (surrounding) woreda located in Wolaita zone, one of the 14 zones in the SNNP Region, Ethiopia. Wolaita Sodo town is located at 360 km south of the capital, Addis Ababa. The total population of the study area in 2015/2016 as projected based on the 2007 census data was 303 063 with the total household of 61 832 (40 283 Sodo Zuria and 21 549 Sodo town). 20 Wolaita zone is composed of 3 agroecological zones; highland (Dega) accounts 9%, midland temperate (Woinadega) accounts 56%, and the rest 35% is lowland (Kolla). The livelihood of the rural population depends on subsistence farming. Regarding the health facilities of the study area, there are 2 public hospitals, 7 health centers, and 39 health posts.
Study Design and Population
A community-based cross-sectional study design was employed. The study population was members of the selected households who were responsible for food preparation aged 18 years or older. The sample size was determined using single-population proportion formula considering the following assumptions: 12% proportion of households who knew the benefit of ISC, 17 95% confidence level, and 3% margin of error. The required sample size for this study was 483; after adding 15% for nonresponse, the final sample size was 556 households.
Sampling Procedure
The study area is divided into 35 rural (31 rural and 4 subcity kebeles [small administrative units]) and 11 town kebeles. A total of 556 households were selected using systematic sampling techniques after 12 (9 rural and 3 town) kebeles had been identified by the lottery method out of 46 total kebeles. The study kebeles and households were allocated proportionally for each stratum (town and rural residence). Members of the household who were responsible for purchasing food items and mostly involved in food preparation in the selected households were interviewed. When study participants were absent in the selected households, revisits were arranged for 2 to 3 times and the next house was considered still if the participant was absent.
Data Quality Management
Structured questionnaires were primarily developed in English and then translated into local language, Amharic, and retranslated into English by another translator for checking consistency before data collection. Finally, the pretest was performed on 5% of the study participants out of the study area, in Areka. Twelve diploma nurses for data collection and 3 BSc professionals for supervision of the study were trained for 2 days, particularly on the data collection tool, interview method, and enrollment of the study participants. Data were collected using structured questionnaire containing information on sociodemographic characteristics, income, education, and knowledge and attitude/perception factors on consumption of iodized salt at household level by face-to-face interview technique.
Definitions
Knowledge on IDD/ISC: measured among respondents using 3 items—(1) ever heard about iodine deficiency; (2) having information on goiter; and (3) ever heard about iodized salts. Accordingly, those who responded “yes” were given a value of “1,” whereas those cited “no” were given “0” and summed up. Those who scored mean or more value were considered as having good knowledge, whereas those scored below mean value were categorized as poor knowledge.
Perception on IDD/ISC: this part measured among food handlers using 3 items—(1) “In your opinion, do all types of salt have iodine?”; (2) “In your opinion, is iodized salt differing from noniodized one?”; and (3) “In your opinion, does iodine changes taste of the salt?” Accordingly, those who responded “yes” were given a value of “1,” whereas those cited “no” were given “0” and summed up. Those who scored mean or more value were considered as having good perception, whereas those scored below mean value were categorized as poor perception.
Statistical Analysis
After data were collected clearly, code and entry were performed using the Epi Info software version 3 and then analyzed with SPSS software version 16. Codebook, analysis, and tabulation plans were developed in advance. Data analysis ranges from the basic description to identification of potential predicators. Associations between dependent and independent variables were assessed and presented using odds ratios (ORs) at 95% confidence intervals. Bivariate analyses were carried out for categorical variables, and ORs were used to quantify the strength of association between dependent and independent variables. Multivariate logistic regressions were utilized to manage the confounding effect of different variables as assessing the effect of each variable.
Ethical Considerations
Ethical clearance was obtained after the proposal was reviewed and approved by the research and ethical committee of the School of Public Health of Wolaita Sodo University. Permission was obtained to commence this study from every relevant authority at all levels (zonal and woreda health offices), and informed verbal consent from every respondent was obtained.
Results
Sociodemographic Characteristics of Respondents
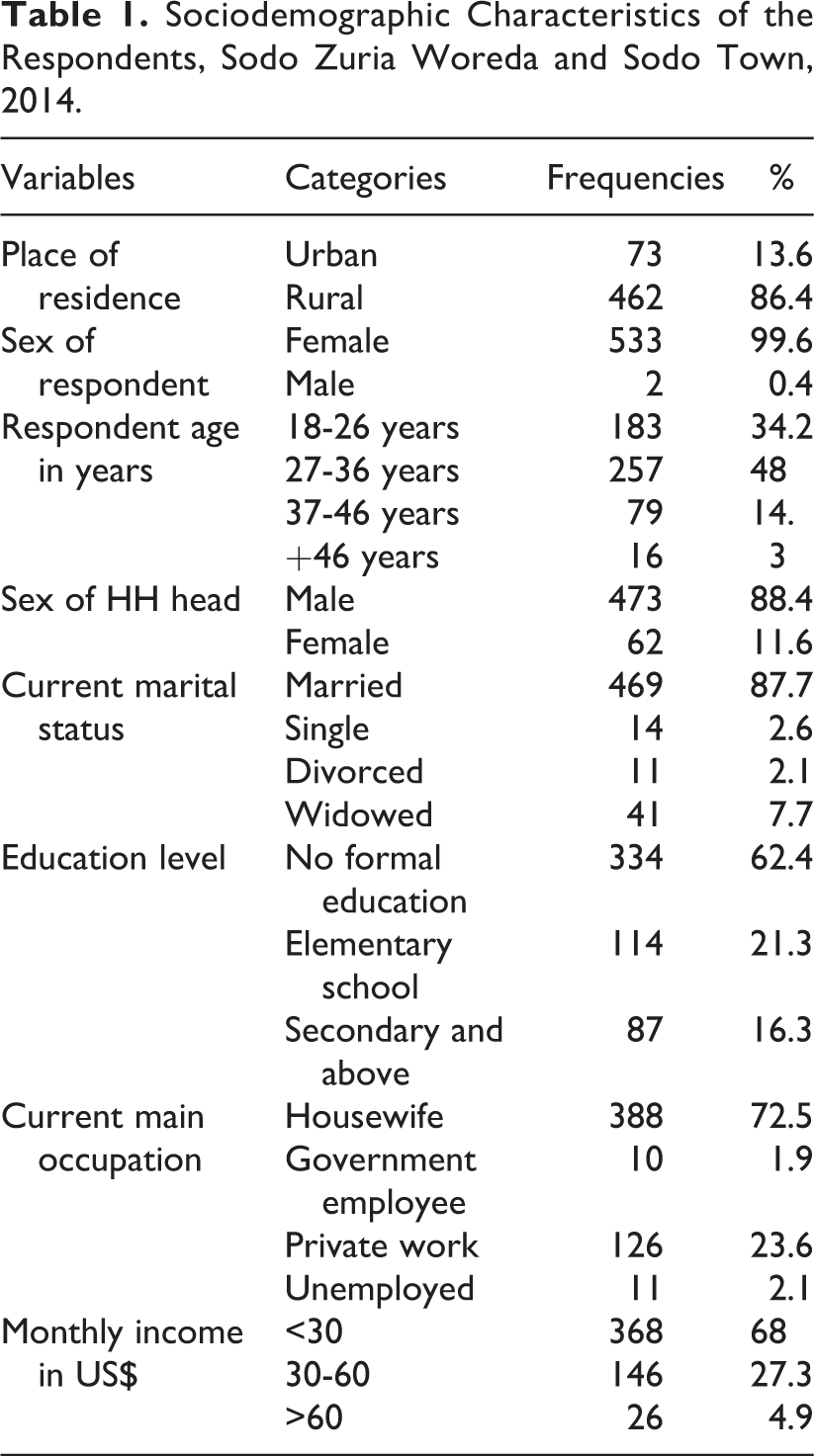
The study revealed that a total of 556 respondents who met the set criteria were enrolled, of which 96% (n = 535) were interviewed. Nearly all (533, 99.6%) of participants were females and the majority (462, 86%) of them were from rural, whereas 73 (14%) were from urban areas (Table 1). Nearly half were in the age category of 25 to 34 years with the mean age and standard deviation of 30.2 ± 7.3 years. Most (334, 62.4%) of the respondents had no formal education and majority (88%) of them were married. Nearly, all (88%) households were headed by males (Table 1).
Sociodemographic Characteristics of the Respondents, Sodo Zuria Woreda and Sodo Town, 2014.
Knowledge Toward IDD and ISC
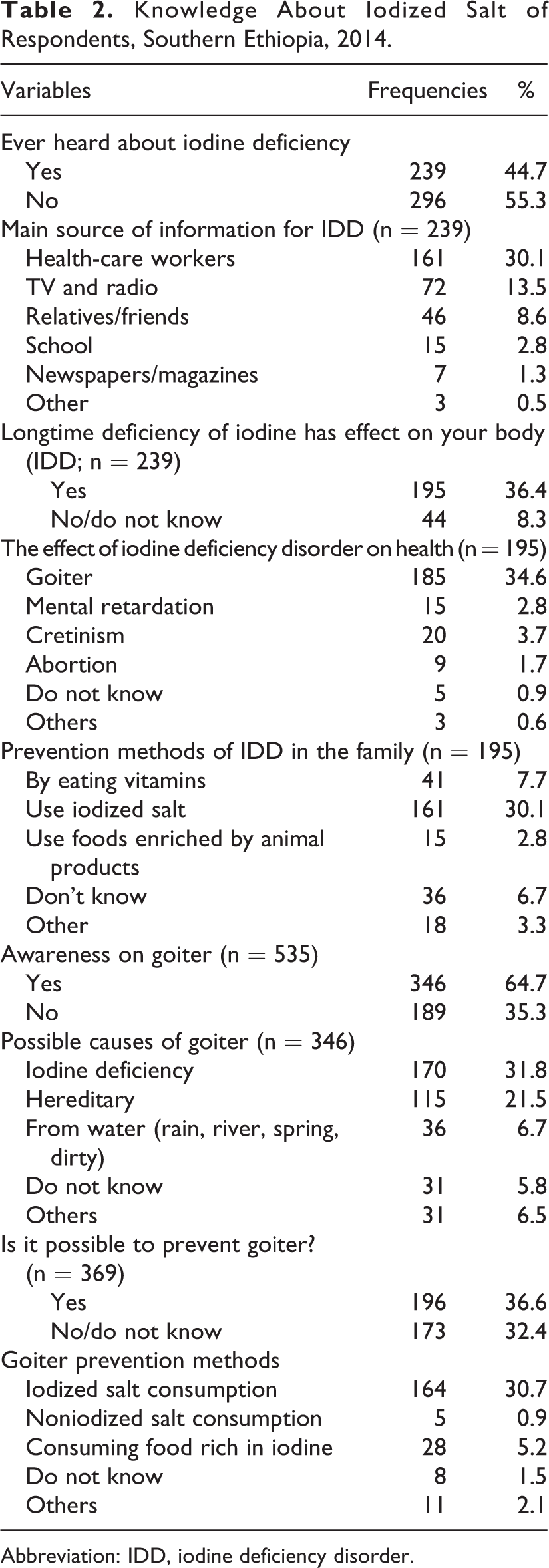
Overall, 239 (44.7%) of the respondents had good knowledge about IDD and ISC, whereas 296 (55.3%) did not. The participants were asked whether they heard about iodine deficiency and only 239 (45%) had heard, whereas more than half (55%) did not. Health-care workers were their main source of information for those who heard about iodine deficiency (Table 2). The use of iodized salt was mentioned by 166 (69.4%) participants for the prevention of iodine deficiency, whereas others preferred to use vitamins, food rich in iodine, clean surroundings, avoiding eating of cabbage and “boyye,” a goiterogenic food, and do not know was mentioned by 166 (69%)…41 (17%), 15 (6%), 9 (4%), 4 (1.6%) and 41 (17%), respectively. Among participants who inquired about the effect of IDD on our body, 185 (35%) were associated it with goiter while few of them linked it with mental retardation, cretinism, and abortion. One hundred sixty-one (30%) mentioned the use of iodized salt as prevention methods of IDD in the family whereas eating vitamins and the use of foods enriched with animal products was stated by 8% and 3%, respectively (Table 2).
Knowledge About Iodized Salt of Respondents, Southern Ethiopia, 2014.
Abbreviation: IDD, iodine deficiency disorder.
Knowledge About Goiter
Most (346, 65%) of participants heard about goiter, whereas only 170 (32%) of them associated it with iodine deficiency, 115 (22%) of them linked it with hereditary, and others associated it with infection, evil, poisoning, rain (ashanda) water, river water, dirty water, and so on. Of 346 participants who heard about goiter, 161 (31%) mentioned ISC and few (28, 5%) mentioned consuming food rich in iodine to prevent goiter (Table 2).
Knowledge and Utilization of Iodized Salt
Table 3 shows about knowledge and utilization of iodized salt at the household level. Of 535 respondents inquired, 248 (46.4%) had heard about iodized salt. The sources of information were mainly health-care workers, 182/248 (73.4%) followed by radio 85/248 (34.2%), relatives 70/248 (28.2%), television 44/248 (17.7%), and school 11/248 (4.4%). Of those who heard about goiter, 171 perceived goiter as a common health problem in their area, and in 48 of the households, there was a goiter in females accounting for the majority.
Community Awareness on Iodized Salt Utilization, Sodo Zuria Woreda and Sodo Town, 2014.
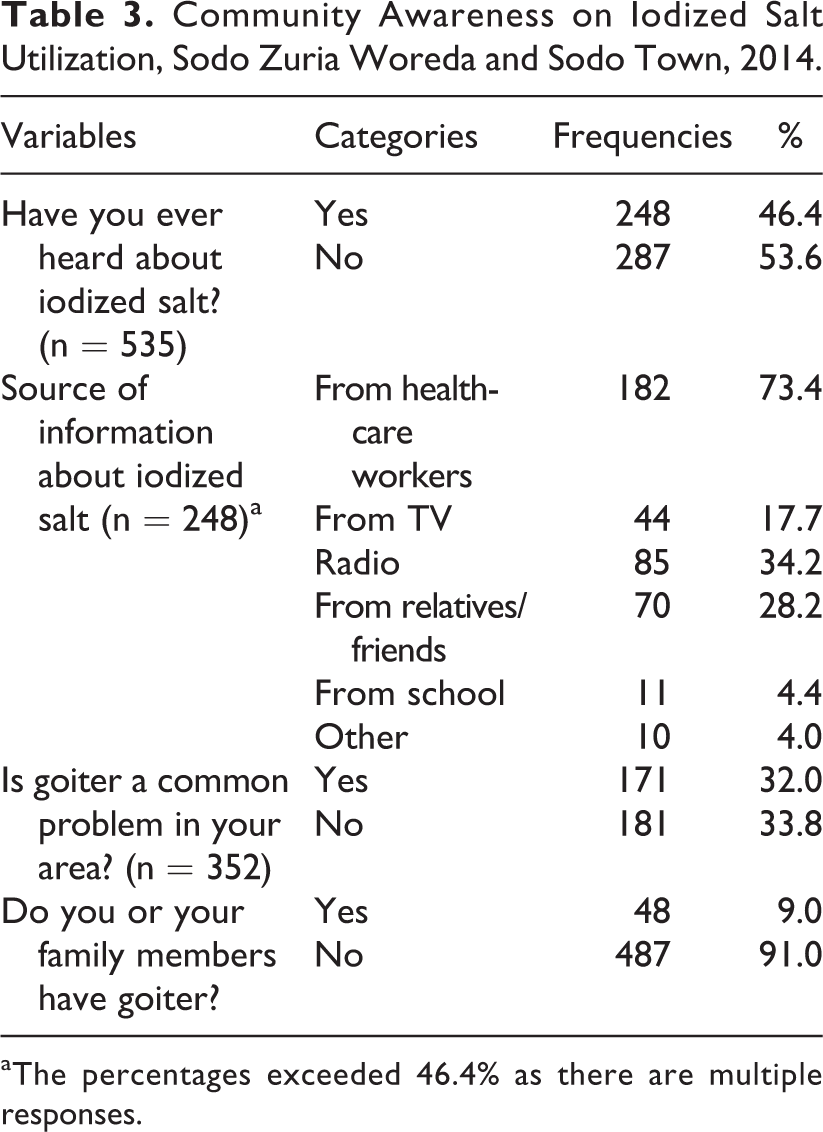
aThe percentages exceeded 46.4% as there are multiple responses.
Perception Toward ISC
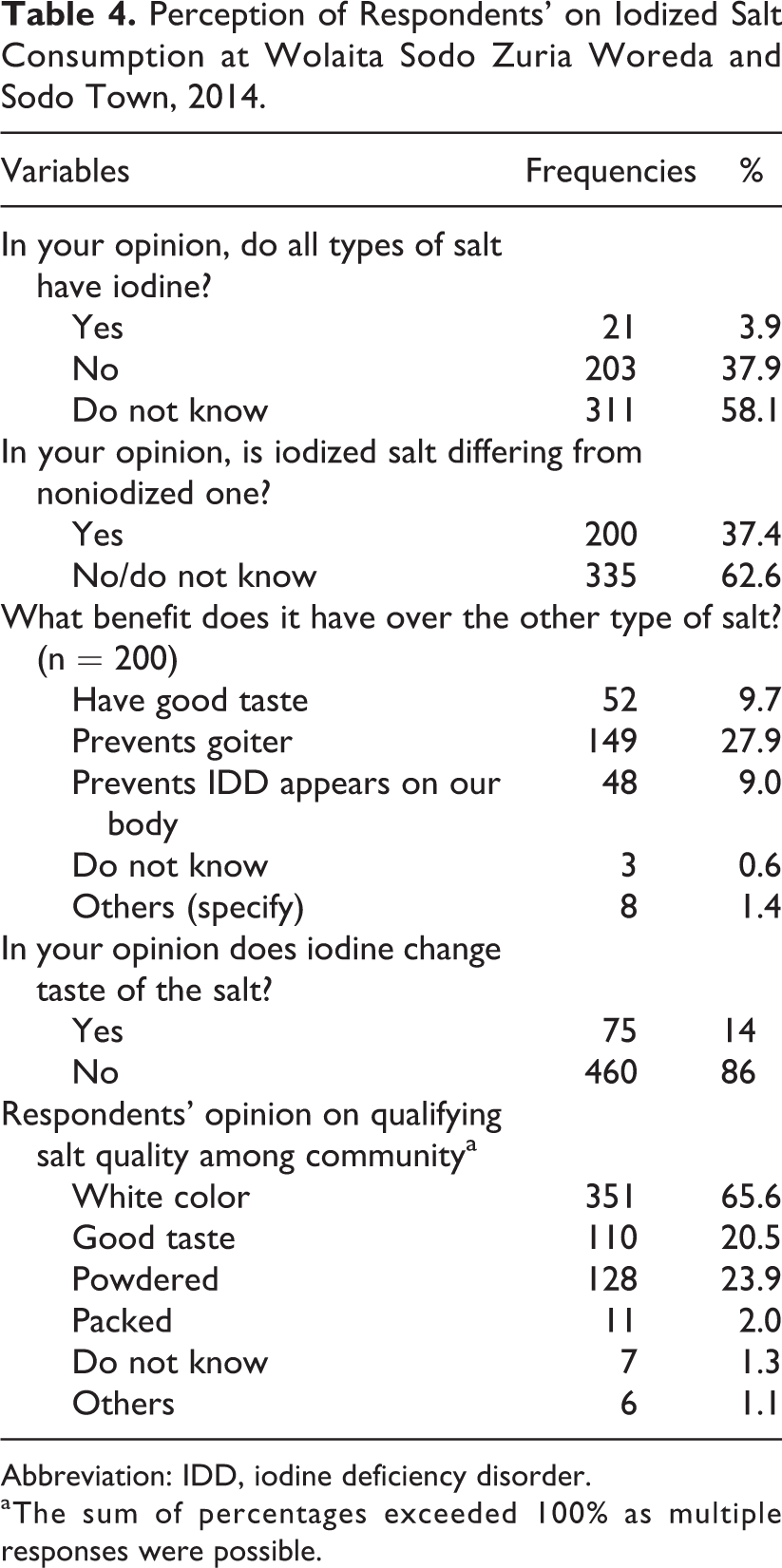
Generally, 228 (42.6%) participants had positive attitude toward ISC, whereas 307 (57.4%) had negative attitude. Participants were asked as to whether all types of salt have iodine, and more than half, 203 (58%), said “did not know,” and 203 (38%) cited “no,” whereas only 21 (4%) responded “yes.” Of the total participants, 200 (37.4%) of respondents had a belief that iodized salt differs from noniodized one, whereas the rest (335, 62.6%) of them said no difference between the 2 types of salts or did not know at all (Table 4).
Perception of Respondents’ on Iodized Salt Consumption at Wolaita Sodo Zuria Woreda and Sodo Town, 2014.
Abbreviation: IDD, iodine deficiency disorder.
aThe sum of percentages exceeded 100% as multiple responses were possible.
Concerning the opinion of respondents in verifying salt quality, about 351 (66%) of them said whitish color of the salt followed by powdered (24%) and good taste (21%), whereas only 2% of them mentioned packing to verify quality of the salt (Table 4). Regarding salt preference, respondents were inquired: “If you had a choice which salt would you buy?” 38% responded that they would buy iodized salt, nearly half of them had no preference, whereas 9% did not know the type of salt they would buy but few of them cited to buy noniodized salt. As to the criteria used to choose the type of salt, respondents cited salt neatness, salt color, price, and its being packed in 36%, 39%, 30%, and 22%, respectively.
Factors Associated With Knowledge and Perception of ISC
Regarding factors associated with knowledge and perception, variables that were statistically significant in the binary logistic regression model were reentered into multivariate logistic regression models to identify the independent effect of association. The following variables: respondents’ age, education, family incomes, place of residence, and occupation of the respondents, had significant association with respondents’ knowledge toward consumption of iodized salt. Variables such as family size and marital status were not significantly associated with knowledge and perception toward ISC and IDD in the bivariate analysis (Tables 5 and 6).
Factors Associated With Respondents’ Knowledge Toward Utilization of Iodized Salt in Wolaita Zone, 2014.
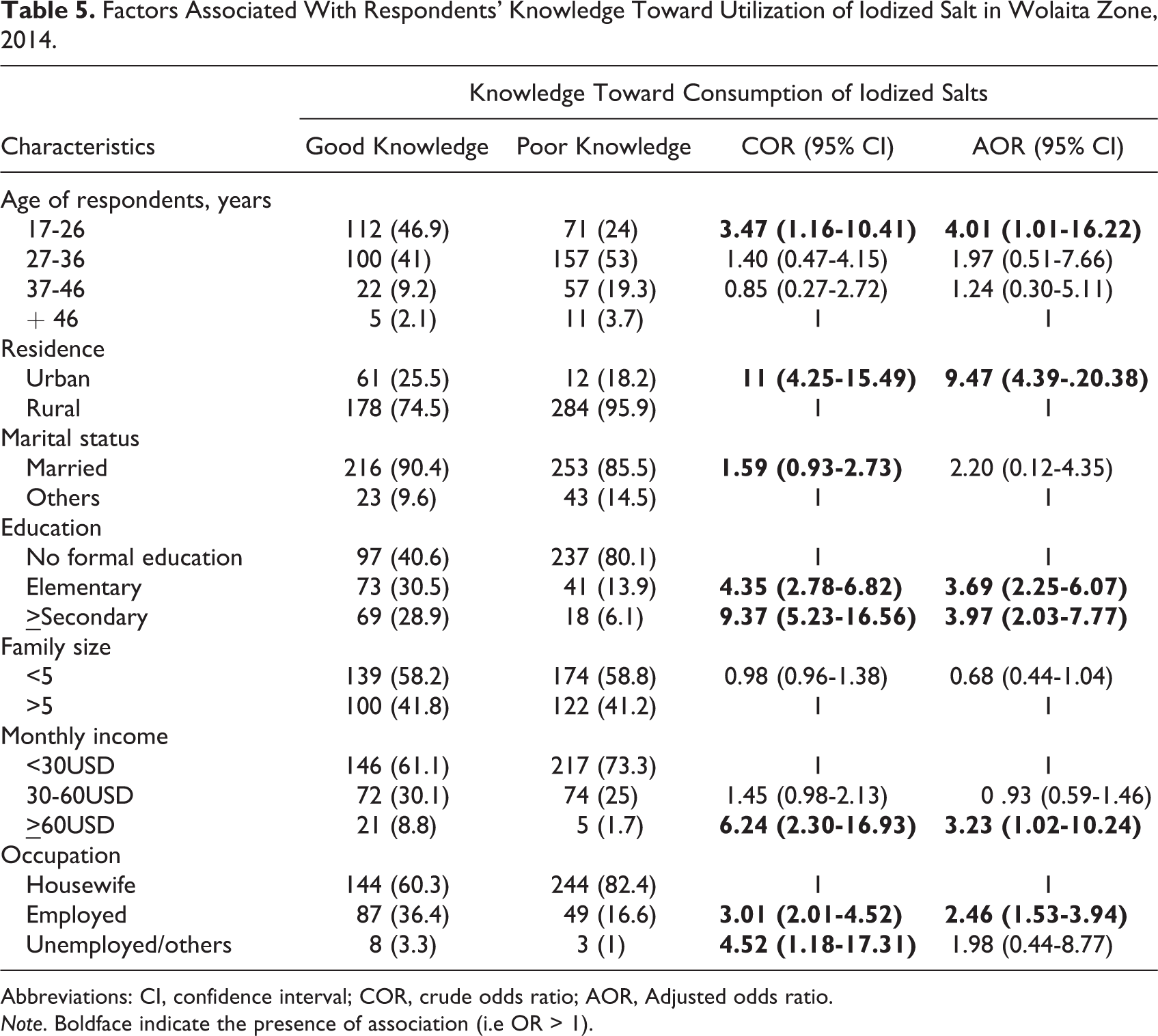
Abbreviations: CI, confidence interval; COR, crude odds ratio; AOR, Adjusted odds ratio.
Note. Boldface indicate the presence of association (i.e OR > 1).
Factors Associated With Respondents’ Perception Toward Utilization of Iodized Salt in Wolaita Zone, May, 2014.
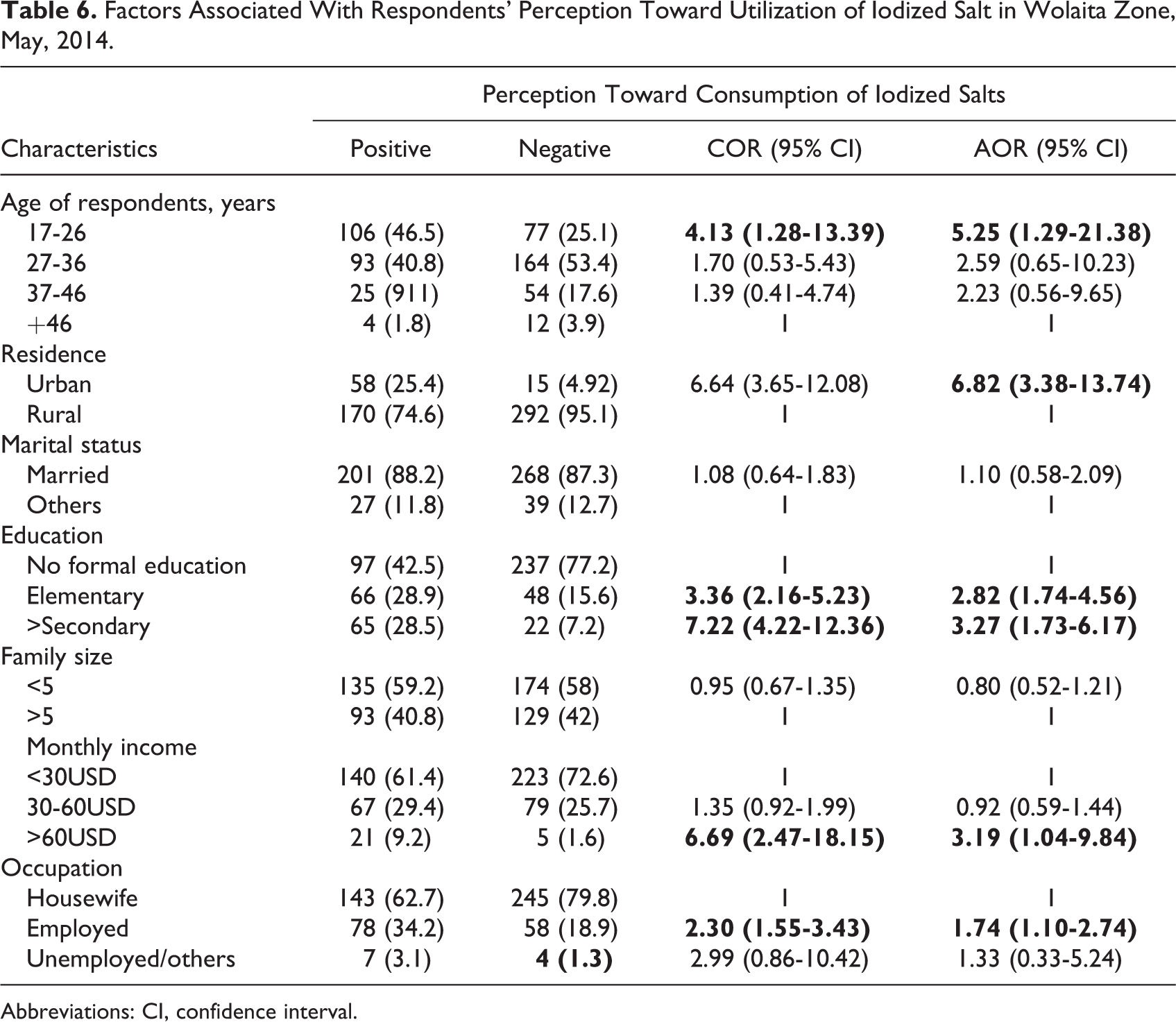
Abbreviations: CI, confidence interval.
In multivariate analysis, respondents’ educational status was a stronger predictor of knowledge toward ISC and IDD, respondents whose educational status was elementary and secondary school and above were about 4 times more likely to have good knowledge than respondents with no formal education. Younger age, higher income earners, and urban resident respondents had better knowledge than the counterpart about the consumption of iodized salt for the prevention of IDD (Table 5). Another important factor predicting the knowledge of consuming iodized salt at household level was occupation that employed respondents were 2 times higher than that of housewives in having good knowledge (Table 5).
In multivariate analysis, place of respondents, educational level, and monthly income were associated factors toward positive attitude on ISC by food handlers. In addition, being young age and employed were factors found to be associated with positive perception toward ISC (Table 6).
Discussion
In Ethiopia, just as many countries of developing world, one of the most effective, feasible, safe, and economical public health intervention strategies for elimination of IDDs is salt iodization, which was recommended by the WHO/United Nations Children’s Fund/ICCIDD. 2,7,21,22 Despite a proclamation in 2011 that states all salt for human consumption should be iodized, IDD still remains a public health problem in Ethiopia. 23 –25
This community-based study has attempted to identify the knowledge and perception of food handlers toward ISC in Sodo town and Sodo Zuria woreda, Wolaita zone, SNNPR, southern Ethiopia. Information on sociodemographic characteristics, income, education, place of residence, and knowledge and attitudes about ISC, were collected.
The results of the current study revealed that knowledge and perception about ISC of the food handlers was significantly influenced by the level of education, place of residence, and income of the respondents in this study area. According to study done in southern Ethiopia, education and monitoring programs are required to combat IDD. 18 Similarly, it is consistent with our study where respondents whose educational status is elementary and secondary school and above are about 5 times more knowledgeable about ISC than respondents with no formal education.
Participants from urban households are more likely to have good knowledge and positive attitude toward ISC. This may be related to information exposure differences between the 2 communities in that urban households have better access to educational media, which is consistent with the study conducted in Pakistan, Sindh, and Punjab provinces where the urban households have better knowledge toward ISC than their counterparts. 26 Hence, broadcasting of specific information targeting the particular population group and geographical areas through mass media and health professionals is needed.
Moreover, younger age groups and employed participants are also determinant factors for knowledge and perception on ISC. This may be due to the younger age groups and employed participants had better exposure to knowledge and more concerned about their health.
The result of the current study shows a considerable gap in knowledge and attitude toward IDD and ISC among the participants who greatly influence consumption of iodized salt that in turn may result in various health problems: mental retardation, abortions, stillbirths, congenital anomalies, increased infant mortality, and so on. 3,4,7
Our study results revealed that awareness of iodized salt is about 46% in the study area. Our finding is lower to the study conducted in northern Ethiopia 19 (59%), Pakistan 26 (85%), and Ghana 16 (90%). This is due to the fact that our study commonly (86%) conducted on rural community where the level of education and exposure to media is low as compared to other studies stated above. However, our findings shows higher awareness level about iodized salt as compared to similar studies conducted in southern and northern Ethiopia. For example, the study conducted among pregnant women in rural Sidama, south Ethiopia, reported only 9% awareness 17 ; another study from Sidama, among rural women reported 28% of food caterers heard about iodized salt. 18 Though increasing consumer awareness and demand for adequately iodized salt has been proven to be one of the most effective intervention strategies to promote USI globally, community still in need of raising awareness/knowledge to develop positive views for change. 7
The results of our study show that the participants were not well informed about the importance of using iodized salt in the prevention of IDDs. In this study, nearly 45% of respondents heard about iodine deficiency. The finding of this study is very low compared to the study conducted in rural households of Ghana where most (72% to 95%) of the respondents knew about iodized salt and IDD. 16 This may be due to cultural and educational differences existed between the 2 studies. However, it shows better knowledge in contrast to the 2 studies conducted in Sidam zone, southern Ethiopia, where only 6% and 12% of respondents heard about IDD, respectively. 17,18 This is possible because our study focus on community as a whole regardless of place of residence, whereas these studies exclusively conducted among rural women.
So, it is important for developing better awareness through campaigns to increase uptake of iodized salt through home to home delivering message by health professionals (health extension workers) since those who have no TV and radio are primary beneficiaries.
Goiter prevalence is one of the prominent indicators of IDDs, and assessing community’s awareness about goiter is a top priority area. 3,7 Hence, the current study revealed that about two-third of the participants heard about goiter but only 32% of them related it to iodine deficiency. This finding is in contrast to the Indian 15 study citing 50%, Bosnian 27 study reporting 62%, and Afghanistan 28 study revealing 70% of participants knew that goiter is the common problem associated with IDDs. This shows that the community has large gap in preventing IDDs as low association between goiters or IDDs and ISC reported and requires behavior change communication.
Nearly, 21% of the respondents associated goiter/IDDs with hereditary, whereas 7% of them linked it with drinking water (rain, river, spring, and dirty). This is consistent with the study conducted on risk factors for goiter among school children in southern Ethiopia, which revealed the presence of goiter is notably associated with drinking river water. 12
In this study, most (58%) of the participants do not know whether all salts have iodine or not whereas, only 38% of them perceived not all types of salt have iodine, this is much lower to study conducted in Ghana where about 72% of respondents believed not all salts have iodine. 16 As to the prevention of the IDDs, 43% of the respondents considered they have positive attitude toward ISC for the prevention of IDDs and goiter. However, only 28% and 9% of the respondents perceived that ISC prevent goiter and IDDs, respectively. This is very low compared with study conducted in Albania where most of the respondents believed they are preventable. 29 In our study area, majority of the respondents have no positive attitude toward ISC for the prevention of IDDs and goiter, which require mitigation strategies to enhance their attitude. Interestingly, this shows a wide knowledge and perception gaps in the current study among meal preparing women toward ISC, and the variation may be due to differences in educational level, income, and place of residence.
In conclusion, results of our study showed a considerable gap in knowledge and attitude about IDDs and ISC among the food handlers, which may significantly influence the consumption of iodized salt in the study area. The knowledge and perception level was significantly related to the educational status, income level, place of residence, and younger age of the respondents.
It is often asserted that lack of awareness on benefit of iodized salt and low income/cash prevents families from buying iodized salt. There is a need to focus on behavior change communication to increase knowledge, bringing positive attitude toward utilization of iodized salt via health extension workers, currently working on preventive aspects of diseases in a home to home basis and mass media in scaling up knowledge and attitude toward ISC by households. The officials should promote TV and FM (local radio) for broadcasting message on the benefit of ISC. Particularly, due emphasis should be given to unemployed and less educated, as well as to the low socioeconomic food handlers.
Footnotes
Authors’ Note
Y.H. prepared the proposal, designed the study, participated in coordination, supervision, and the overall implementation of the project, analyzed the data, and drafted and finalized the manuscript. A.J. and P.W. were involved in all stages of the study and revised the manuscript. All authors read and approved the final version of the manuscript.
Acknowledgments
The authors are grateful to Wolaita Sodo University for funding the study. Data collectors and study participants, who had full support in realizing the successes of the study, are honorably acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Wolaita Sodo University.