
Abstract
Background:
The role of fathers in proper nutrition of young children has not been a frequent topic of studies. Mothers are usually the primary caregivers for young children. However, the father is often responsible for the financial choices of the household, especially in developing countries; we wondered to what extent fathers were involved in child feeding.
Objective:
This study aimed to investigate the extent of perceptions, practices, and challenges of fathers from low-income settings in routine child care, particularly in relation to child-feeding practices.
Methods:
A qualitative study was conducted in northern Ethiopia. Ten fathers, who had children between 6 and 23 months, were participated in the study. To validate fathers’ comments, 10 mothers (from different households) also participated. In-depth interviews and focus group discussions were carried out. A thematic analysis was completed to identify emergent themes within the data.
Results:
In general, traditional fathers, fathers in transition, and modern fathers are the 3 types of fathers identified based on their perception, practice, and challenges of routine child care and feeding.
Conclusion:
Our findings provide new insight to the literature in describing fathers’ roles and challenges in routine child-care and feeding practices. We have developed a model that could help researchers, programmers, policy makers, and health workers to approach fathers in different child intervention research and plans. Our findings suggest that targeting fathers may be a worthwhile approach and that it seems justifiable to plan interventions involving fathers.
Introduction
The way in which people feed their children has been an important topic in both high- and low-income countries in order to prevent child malnutrition. 1,2 This is especially important in developing countries where child undernutrition remains a serious public health problem—child feeding is not only a matter of having healthy food but also of fulfilling the basic needs of a child. 2 –6
Many governmental and nongovernmental organizations have invested in programs that inform the public about the importance of appropriate child feeding. 7 –13 These programs will often be received by mothers, as they are most often the primary caregivers for young children. However, a previous study of our group suggested that fathers could have a crucial role in the successful implementation of such advice. 14 If, for example, the father is responsible for financial choices of the household, the decision to buy nutrient-rich foods for the baby also depends on him. Therefore, we wondered to what extent fathers were involved in raising the children.
The role of the father in proper nutrition of young children has not been a frequent topic of studies. Several studies emphasize that mothers play a crucial role in children’s life, whereas the fathers’ role often comes after and is usually addressed quite superficially by merely emphasizing the impact of the fathers’ socioeconomic status on child health outcomes. 15 –17 Socioeconomic status often was found to be the important predictor of child health and related outcomes.
Few studies have looked at other aspects of fathers’ involvement in children’s life, and most often these studies concerned fathers of children with specific and serious health problems such as autism, obesity, or psychological or behavioral problems. 18 –22 These studies stressed the importance of the father in reducing child health problems. Different studies have highlighted the fathers’ influence when it comes to motivating children for education and school readiness, 23 –25 whereas other studies showed the positive influence of fathers’ supportiveness in breast-feeding, such as verbal encouragement and active involvement in breast-feeding activities. 26 A systematic review of longitudinal studies and 1 cross-sectional study showed that mothers usually adopt the primary caregiver role and that the father usually supports the mother. 22,27
Although the available research agrees on the importance of the involvement of fathers in child care, research has largely focused on high-income populations, which is not translatable to the practices and challenges of those in low-income settings. Therefore, data from these bodies of research cannot be used to develop programs for low-income populations. With this knowledge deficit in mind, our study aimed to investigate the perceptions, practices, and challenges of fathers from low-income settings in routine child care, particularly in relation to child-feeding practices.
Materials and Methods
Design and Study Participant
The study was conducted in the rural Tigray Region of northern Ethiopia and used a qualitative approach. Ten in-depth interviews and 1 focus group discussion (FGD) were carried out among 10 fathers who had children between 6 and 23 months. To validate fathers’ comments, 10 mothers (from different households) also participated in the study, and 1 in-depth interview and 1 FGD were conducted among these mothers.
Data Collection
The following questions were addressed during the interviews and FGDs (Table 1). The in-depth interviews and FGDs were conducted using the local language, Tigrigna, at the nearest health center. All participants were interviewed for the sociodemographic characteristics after we got their consent. The duration of each interview and discussion were between 60 and 120 minutes. Both the FGDs and in-depth interviews were held at locations that were accessible to participants such as at health posts and health centers. The FGD discussion and interviews were carried out by trained moderator and interviewers. Considering the rural fathers’ wrong gender perception, male moderators were assigned to run the FGDs among fathers. A purposive sampling technique 28 was applied to select the study participants. There were no formal exclusion criteria to select fathers and mothers. The participants were selected based on the recommendation of community health workers, who selected fathers and mothers, who they thought would be able to provide useful information about their experiences on child-care and feeding practices.
Interview Guides for In-depth Interviews and FGD.
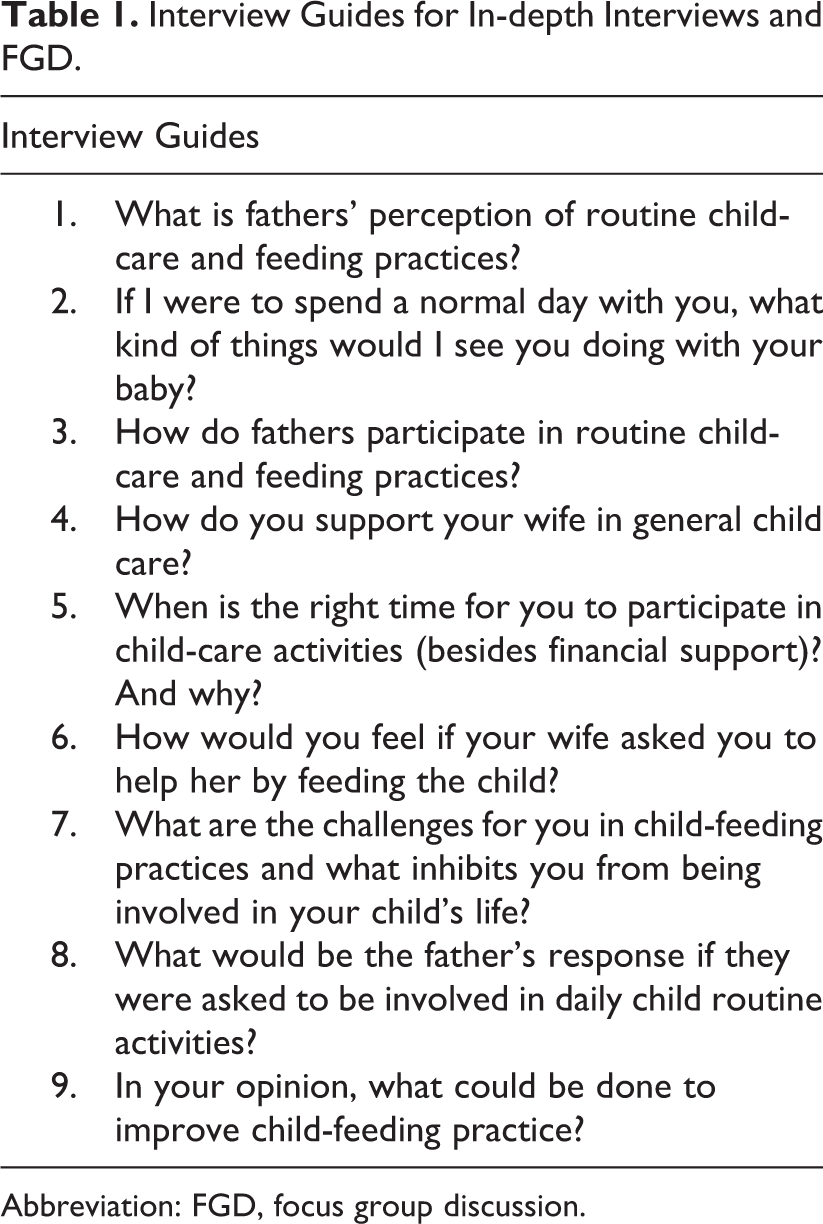
Abbreviation: FGD, focus group discussion.
Open coding was used during the interviews and then elaborated later. As new concepts appeared, the researcher revisited the participants with the questions (with some amendments and additional question). The interview and discussion process lasted until saturation point, when no new information was provided. 29 The interviews were conducted by trained moderators and interviewers who were native speakers of the Tigrigna language and able to speak and write in English. For the in-depth interviews and FGD, semistructured open-ended interview guidelines were prepared.
Data Analysis
The study applied a thematic analysis 30 to a careful examination to identify, analyze, and extract emerging themes from the data. This technique minimally organizes and describes the data set in rich detail. Ongoing data analysis took place throughout the study. Early involvement in the analysis phase was helpful to move back and forth between development of themes and data collection and direct the subsequent data collection toward sources that were more useful for answering the research questions. The researchers first familiarized themselves with the data where upon initial codes were developed. The open codes were then assigned to identify and categorize the phenomena found in the text. Axial coding was then performed by fitting themes into a basic frame of generic relationships. Finally, a single story line constituted using selective coding. We continued analyzing the categories in great detail until saturation. 29 ATLAS.ti50 software was used to support the analysis. 31
Trustworthiness
According to Lincoln and Guba, the quality of qualitative research should be assured by meeting standards of trustworthiness through addressing credibility and transferability. 28 To meet credibility, we included mothers from different districts. Additionally, in-depth interviews, FGDs, and field notes were used in the analysis. Two investigators also participated to collect and analyze the data. To strengthen the transferability of the findings to different settings and contexts, our study provided descriptions of the setting, sampling, sample size, inclusion and exclusion criteria, interview procedures, and findings.
Ethics
Ethical approval was obtained from the ethical review committee of Mekelle University and the Tigray Regional Health Bureau (registration number: CHS/0136/PH-05). Participants who were literate were provided written information about the aim of the study, benefits, and confidentiality. A written consent was subsequently obtained from these participants. For those participants who were illiterate, the purpose of the study and confidentiality were explained by the interviewer/moderator and then verbal consent was obtained. This procedure was tape-recorded.
Results
The average age of fathers who were involved in this research was 40 years, and all fathers were capable of reading and writing. All fathers except 1 had attended formal education. Farming was the occupation of all fathers and the main source of their income was, on average, US$601 per year. The mean age of their children was 13 months, and half of the children were female. The mean age for mothers was 26 years, and the majority were housewives with no formal education. Based on the thematic data analysis, 4 major themes emerged from the data: (1) fathers’ perception of routine child care and feeding, (2) fathers’ practice of routine child care and feeding, (3) challenges of fathers’ involvement in routine child-care and feeding practices, and (4) model for the extent fathers’ perception, practice, and challenge of routine child care and feeding.
Fathers’ Perception of Routine Child Care and Feeding
Some fathers did not perceive routine child-care practice as their responsibility. They considered all child-care responsibilities, from morning to evening, as the mothers’ responsibility, so for some men it seemed that mothers were the only responsible caregivers in the child’s daily life. These men were very distant from the routine life of their family, and they only felt responsible for income-generating activities. In this role, they perceived that they were giving full priority to their family because they were fulfilling their responsibility as needed. These fathers usually spent their time outside their home, and, if there was any leisure or free time, they often preferred to spend it with friends rather than their family.
The majority of the fathers still perceived child care mainly as a responsibility of mothers, however, they were also involved in routine child-care activities, although this was often mentioned in a way of helping the mother. For example, “… majority of the activity is that of the mother, but I help her when she is involved in some other activities …” Their role was often conditional on several factors, such as the age of the children (between 6 and 8 months was considered as the right time for fathers to be involved in child-care activities). Some fathers also mentioned 5 years or more as a right time for them to be involved in child-care activities. I wash her body after eight months just after she is comfortable to be hold. Before that age, it is difficult to hold the baby body, even to change their cloths … during this age; it is the mother who takes care of the baby. …, I meet my child only few hours per day. But the child spends many hours with her mother whereas with me just very few.… for example I go to work in the morning leaving my child behind and I meet her in the evening. But when I get home, I help my wife … The one who will be responsible is the one who spends most of the time with the family. From the time of birth until he/she starts to lead his/her own life independently, he/she needs the care of his father and his mother. Full involvement might be difficult but sharing it could be acceptable especially by the new generation. However, I can’t say that it would be fully accepted.… In the past, all household chores were considered to be the responsibility of the mother, but now I can say almost half of the community husbands are helping the mother. As long as she is involved in different activities of the father, he should also be involved in mothers’ activities… … Traditional and cultural influence favours for males. Therefore, almost all activities related to child care, feeding and food preparation are considered to be the responsibility of mothers.
Fathers’ Practice of Routine Child Care and Feeding
Playing with the child was the first thing that came to fathers’ mind when asked about the kind of activities that we would see them doing with their baby, if we were to spend a normal day with them. Playing activities were described in different ways, for example, “physical playing,” “tricking while feeding,” and “making different musical sounds.” Preparing the child’s food, feeding the child, giving money to the mother to buy food or other things for the child, bringing food from the garden, and buying food and other child needs from the market/town were other activities that were often mentioned by fathers. Oh, regarding food preparation … I have nothing to do with that, I only bring the items. In addition, I feed him, entertain and trick him. Especially, playing with the child is my job
Additional discussion points in relation to child feeding included decisions on what food to buy from the market/town, what food to bring from the garden, and the foods that were available at home. Other discussions points between mothers and fathers concerned other child needs and child health educations that were provided by health-care workers. Regarding other health-related activities, few fathers attended the health education even if it was given in their homes. Taking the child for vaccination/immunization or any child health–related activity was seldom mentioned by fathers.
Mothers also confirmed that common activities of fathers in relation to routine child care and child feeding included playing with the child, giving money to the mothers to buy necessary things, and providing food from the garden. Buying food and other child needs from the market/town were other activities mentioned as typical fathers’ activities. Mothers also confirmed that attending child health–related education, taking the child to vaccination, or other child-care visits were rarely done by fathers. In general, all mothers agreed that compared to their past experience, fathers’ practice in routine child care and feeding has shown some improvement.
Challenges to Fathers’ Involvement in Routine Child-Care and Feeding Practices
Being busy with work activities (such as farming and other income generation activities) made it difficult for fathers to spend time with their child, being involved in their child’s life and to attend child health–related education. I meet my child only for few hours … my child spends many hours with her mother because I go to work in the morning and I come back home and meet her in the evening. … for some of the fathers, economical/financial problems were huge challenges even if they have plenty of knowledge about feeding practices. On the other hand, there were other groups who have the money but do not have the knowledge … There were also some extravagant individuals who waste the money on non-essential issues or they simply save the money without spending it on their child’s needs. And there were fathers who have the knowledge as well as the money but they do not want to buy anything for their children.
The majority of mothers confirmed the challenges of the fathers’ perceptions and cultural and traditional beliefs that indicated child care is only the mother’s responsibility. They also mentioned the knowledge and information gap between mothers and fathers, because the fathers are not participating in child health–related education. They also emphasized that this knowledge gap indirectly affected mothers’ financial capacity and hindered them from providing all the necessary care, foods, and materials for their children.
Model for the Extent Level of Fathers’ Perception, Practice, and Challenge of Routine Child Care and Feeding
This study identified 3 general types of fathers (Figure 1). The first group is fathers who do not feel part of routine child care, and they fully believe child care is only the mothers’ responsibility. They consider making money and/or farming to be their responsibility for their family. Their knowledge on child care and child needs is very poor and they are largely unaware of the challenges that the mother and child face every day. Therefore, the entire burden of taking care of the baby weighs on the mothers’ shoulder. These fathers are very traditional and believe that they are fulfilling their child-care responsibilities as needed. Therefore, it might be very difficult to change this group’s behaviors and will probably be very difficult to involve them in any innovative program on child-related issues. We should tell the truth. It is not because I do not have time, but we both should do our part, so it is better if the mother do her part, take care of the child, and I do my part, farming, rather than leaving my activities undone.
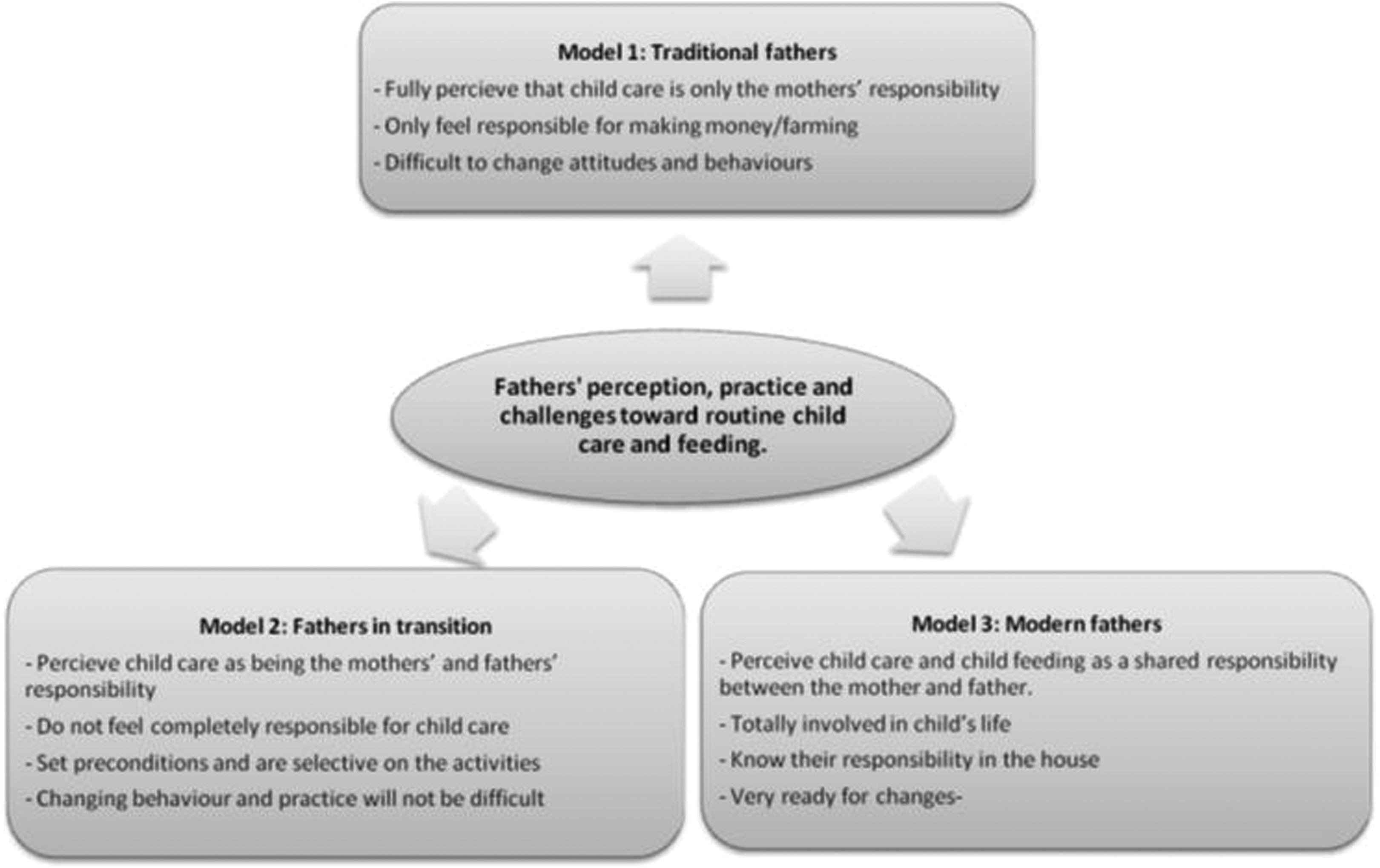
A model to describe fathers’ perception, beliefs, practice, and challenges toward routine child care and feeding.
The second group of fathers perceive child care as being both the mothers’ and fathers’ responsibility. However, they do not feel completely responsible for child care but set preconditions such as: “if I am free,” “if I do not have other activities to do,” “if I am at home,” or “when the mother is busy with other household activities.” This group of people understand the need to help the mother. They are, however, selective on the activities they do. As this group of fathers also have other priorities, they may be reluctant to attend any education on child care, resulting in a knowledge gap on this issue. However, they seem happy to respond to the mothers’ needs in relation to routine child care, and they are helpful and open for child-related innovations and changes. Therefore, this group of fathers require a good approach or system, considering their time and interests, to boost their knowledge and help them feel responsible for their children. Targeting this group to implement changes in behaviors and beliefs thus could prove less challenging. Buying food is her responsibility and it is the mother who should prepare the food. But I can feed her if I come home while the child is being fed, but it is her mother who feeds the child most of the time. Because it is her mother who spends much time with her. But I can be involved in buying (supporting financially) the food. … If you had spent a day with me, you could see me giving all the care for my daughter. We all help each other equally, the only difference between the mother and me is that she carried and delivered the baby …
Discussion
Our study showed that fathers’ perceptions and practices of routine child care and feeding seem to be improved from the past. However, except for income generation and providing necessary things for the child, the majority of fathers still fully or partially perceived routine child-care and feeding practice as being the mothers’ responsibility. Besides income generation activities, playing with the child seemed the only interesting activity for the fathers. Attending child health–related education and taking the child for immunization or any child health–related visits seemed insignificant activities in the fathers’ minds. Common setbacks that held fathers back from practicing routine child care and feeding included being busy with work, lack of knowledge, traditional beliefs, and financial reasons. In general, 3 types of fathers (traditional fathers, fathers in transition, and modern fathers) identified based on their perception, practice, and challenges of routine child care and feeding.
There were very few fathers who fully perceived that child care was a shared responsibility between mothers and fathers, however, the majority fell into the category of fathers who felt partially responsible and who were only involved in the activities that interested them. Even though it was difficult to find studies similar to our topic of interest, these results are generally consistent with our expectations and with other related studies that showed that work, lack of information, poor knowledge, economic issues, absence of recognition of their role, lack of engagement during the education process, and lack of commitment from health professionals to engage fathers are common challenges that inhibit fathers from being fully involved in routine child care. 25,27,32,33 Therefore, in order to increase their engagement in children’s life, we required much stronger interventions that could overcome these setbacks.
For many fathers, their involvement in child care appeared to extend only to making money for the family. This is a reason why many researchers often address household income to indirectly address fathers’ roles in child health–related outcomes or issues. 15 –17 Fathers who consider income generation as their only responsibility are very traditional and it could be very challenging to engage them in their child’s daily life, in areas other than financial support. The very limited involvement of this group of fathers in their children’s life could directly affect their knowledge toward child care and their support in decision-making and financial support in the family. This might increase the economic burden toward mothers. Therefore, approaching this group of fathers is not only a matter of introducing a strong system about child care but it also needs more work to break the chain of traditional beliefs and perception toward child care and family value.
In line with our finding, fathers to go to the health centers seems a universal problem. 34 –36 Parental discussions seem to be the source of information for fathers. Most fathers rely on second-hand information passed only by their wives. Fathers are neither attending health education nor visiting child health-care centers. Therefore, we suspect that fathers’ child-care practices and their appeal to mothers’ needs in relation to the child can be misguided. More research is needed to assess fathers’ engagement and challenges in different child health–related education programs.
Some limitations of this study should be mentioned. The data from mothers were weak as there is a deep cultural belief that mothers should not talk badly about their partners. We experienced that mothers’ disclosure of their partners’ ill perceptions and poor practice of child care in front of other mothers during the FGD was difficult. The majority of mothers preferred to remain quiet during the discussion or only gave very short responses by referring to the comments of others. As a result, the data obtained were mainly dominated by the fathers’ opinion. Again almost all fathers were literate and this might skew the representativeness. However, the majority of mothers were housewives with no formal education and this might increase the credibility of the data. Again, having interviews and FGDs with fathers about this issue in detail in a low-income setting is hard to find, therefore, we consider the data we obtained to be highly valuable.
Our finding added new insight to the current literature describing fathers’ roles and challenges of routine child-care and feeding practices. We have developed a model that could provide further insight to help researchers, programmers, policy makers, and health workers to approach fathers in different modalities in relation to the design, research, and planning of child-care and feeding interventions. For that reason, in order to engage fathers in childrens’ lives, knowing their perceptions, practices, and challenges and customizing approaches toward them based on the model the fathers fit into could be a more effective way to reach fathers.
Targeting fathers as much as we target mothers in house-to-house education programs through improving fathers’ knowledge toward child care and feeding could be a worthwhile approach for meeting all appropriate child-feeding practices. Developing checklists to level fathers in the model and identifying education and practices that suit each category of the model would be appropriate steps to start planning the intervention program. Then house-to-house education about child care and feeding should be designed for each category of fathers (traditional fathers, fathers in transition, and modern fathers). Therefore, every father should get the education that is targeted to their level of beliefs, perceptions, and practice of child care and feeding.
For instance, traditional fathers strongly perceive that child care is only the responsibilities of mothers, and they only feel responsible for making money. We believe that traditional fathers should receive basic education that could challenge their strong beliefs and perception of child care and could help them to start being involved in child-care practices. For example, teaching them how being involved in their child’s life on a routine basis could help them to understand their child’s needs and challenges. Further, being more involved in their child’s life could stimulate fathers to work more to provide the child with necessary items. This group of fathers need an easy pathway to start being involved in child-care practices.
Fathers in transition perceive child care as being both the mothers’ and fathers’ responsibility. They are, however, selective on the activities they do and make excuses for the very limited involvement in their children’s lives. This group should receive education that could strengthen their positive perception toward child care and generate opportunities to increase their involvement in child-care practices.
Modern fathers are the most advanced in terms of fathers’ involvement in child care. They perceive child care as a shared responsibility between mothers and fathers, although they have minor challenges to put their knowledge into practice. This group should not receive basic education about child-care responsibility, and they do not need pressure to participate in child care on a daily basis. They already have a good perception and knowledge about child care and feeding and are also very involved in their child’s life. Therefore, they should only receive education to advance their knowledge or provide professional support to solve any minor challenges faced in practicing child care and feeding.
In line with other studies and our expectations, this study suggests that targeting fathers may be a worthwhile approach and it seems justifiable to plan interventions that involve fathers. However, assessing their engagement and experiences in child health–related education programs is an important prerequisite for any intervention plan.
Footnotes
Acknowledgments
The authors would like to extend our sincere appreciation to the mothers and fathers who shared their time and information with us, thereby contributing to the success of the data collection and to our colleagues and staff in the College of Health and Public Health Department of Mekelle University for the use of their facilities, for consultations and participation in the data collection process, and for moral support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research is funded by an AECID PhD scholarship from Spain.