
Abstract
Background and objectives:
Initiation and adherence are both critical challenges for micronutrient supplementation programs, especially during the preconceptional period. This study examines factors influencing initiation of supplement use and continued adherence among women participating in PRECONCEPT, a double-blind randomized controlled trial of preconception micronutrient supplementation.
Methods:
In-depth interviews were conducted with 39 participants during different periods (prepregnancy [n = 15], pregnancy [n = 8], postpartum [n = 8], and dropouts [n = 8]). We examined participants’ knowledge about nutritional needs and micronutrient deficiencies, individual experience with nutritional supplements, and perceived benefits and side effects of supplements. Four focus groups were conducted with 24 village health workers (VHWs) to collect information on VHWs’ perceptions of factors influencing participants’ adherence and logistics of supplement distribution. Influences on initiation and adherence were examined within the Health Belief Model framework.
Results:
Primary barriers to initiation of supplement use were low perceptions of severity of nutrient deficiencies and personal susceptibility. These are associated with low knowledge and awareness around deficiencies. Perceived seriousness and susceptibility varied by nutrient: high for iron during pregnancy but low for all other micronutrient deficiencies, including iron outside pregnancy. Continued maintained adherence to an initiated regimen was influenced by the woman’s perceptions of the health benefits of, and barriers to, regular supplement use.
Conclusion:
Initiation of supplement use was influenced by perceived susceptibility and severity of nutrient deficiencies, while maintained adherence to consistent use was influenced by perceived benefits and barriers. Recognizing the influences on each stage may help improve adherence and maximize positive effects of future interventions.
Keywords
Introduction
Maternal nutritional status during pregnancy is essential to supporting fetal development and reducing the risk of adverse health outcomes. 1 –3 Iron and folic acid (IFA) supplements are widely recommended during pregnancy and have been shown to reduce the incidence of low birth weight babies, neural tube defects, and infant and maternal mortality. 4 –6 More recently, prenatal multiple micronutrient supplementation has been recommended, which may have an additional positive impact on pregnancy outcomes beyond that of traditional iron–folate supplements. 7 –9
Research suggests that a woman’s nutrient status entering pregnancy is critical to fetal development in the first month of gestation. 10,11 In many low- and middle-income countries, women do not know their pregnancy status until the second trimester; therefore, traditional prenatal supplementation may be inadequate to meet the needs of women who begin pregnancy with deficient nutrient status. In areas where micronutrient deficiencies are common, prepregnancy supplementation with multiple micronutrients among women of reproductive age (WRA) may be a crucial component of efforts to reduce adverse pregnancy outcomes. 12
While antenatal IFA supplements have been successful in preventing and treating anemia deficiencies, supplementation programs delivered at scale often suffer from poor adherence. 13,14 Low adherence rates may be due to a variety of contextualized personal, sociocultural, and/or logistical factors that may differentially affect whether a woman initiates and then sustains the supplementation regimen over the recommended period 15 ; identification of these factors is a necessary step toward improving program effectiveness.
The current study uses the health belief model (HBM) as a framework to aid in understanding the factors that influence initiation and adherence to supplement use. The HBM is one of the most widely used theoretical frameworks for understanding behavioral change. 16 The model holds that an individual’s likelihood of adopting and maintaining a new behavior is heavily influenced by their perceptions around the health threat and the behavior being proposed to address that threat (Figure 1).
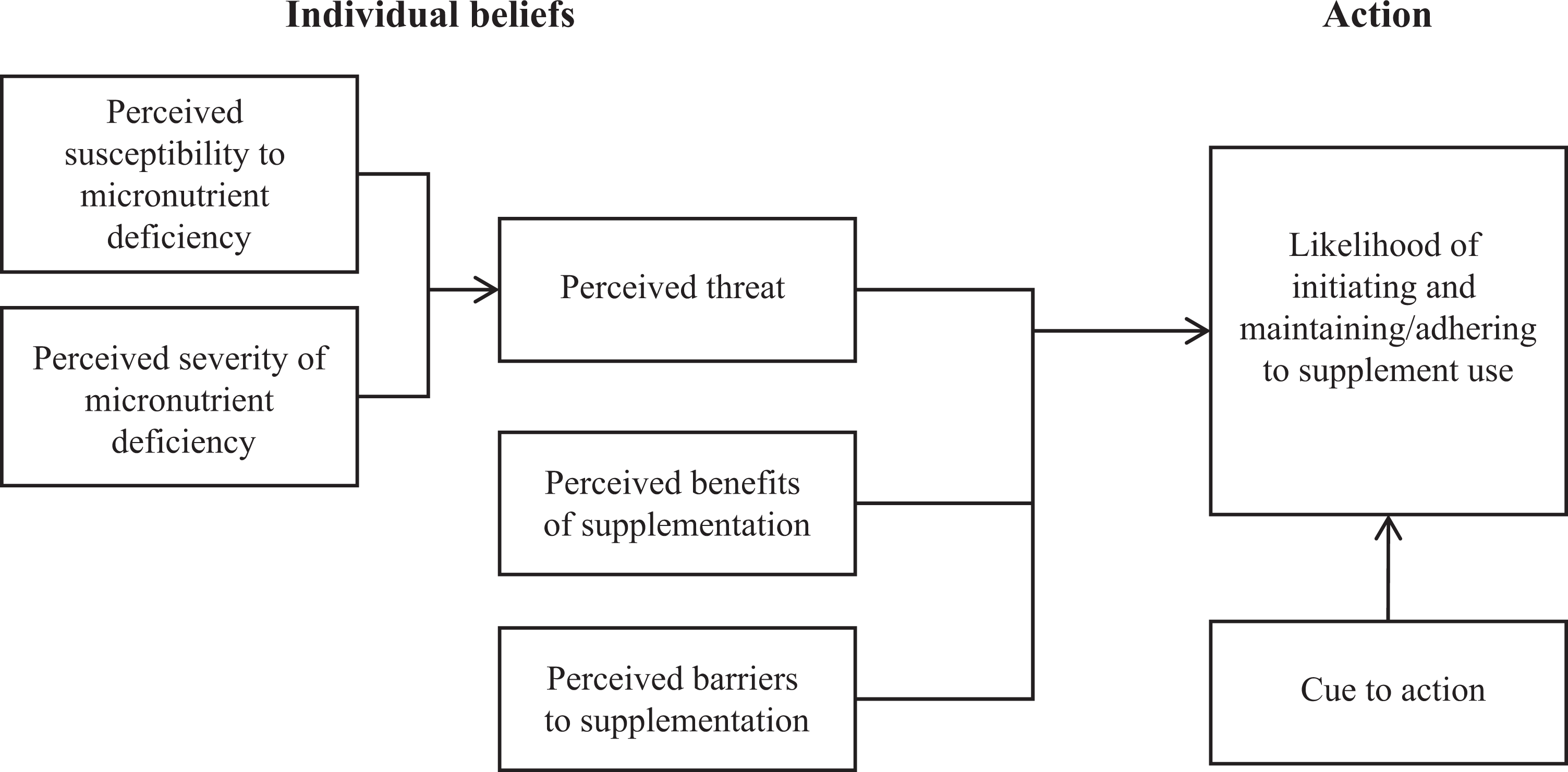
Health belief model. Adapted from Champion and Skinner. 24
For long-term health behaviors such as supplement consumption, a complete understanding of the factors that influence both initial adoption and continued adherence to the practice is critical. These distinct stages may be influenced by different facets of the HBM framework and require different strategies for improvement. Previous research on factors affecting prenatal iron supplementation have identified the barriers of negative side effects and forgetting as having a negative impact on adherence, 3,17 –20 while others have found a positive association between high perceived health benefits of supplements and consistent adherence. 1,3,16,18,19 In contrast, much less is known about initiation of supplementation regimens among WRA, an exception being 2 studies of school-based supplementation programs for adolescents. 21,22 Initiation is a particularly critical issue among nonpregnant women who lack the defined start and end points for supplementation provided by a pregnancy. As countries increasingly move to adopt preventative micronutrient supplementation programs for all WRA, research that identifies barriers and facilitators to both initiation and adherence among nonpregnant women will be crucial to designing effective programs.
Therefore, for the purposes of this study, we focused on the potential factors that influence supplementation in these 2 stages: the decision to begin supplementation (“initiation”) and the ongoing decision to continue with the supplementation regimen (“adherence/maintenance”). Following the HBM framework, we proposed that the initiation and adherence of supplementation among WRA may depend on a woman’s perceptions of her susceptibility to micronutrient deficiency before and during pregnancy, her perceptions of the severity of micronutrient deficiency and its effects on her own and her infant’s health, and her perceived benefits and barriers of consistent supplement use. Under this framework, a woman would be more likely to initiate and adhere to a supplementation regimen if she believes that she is personally susceptible to micronutrient deficiency, that the health effects of such deficiency would be severe, and that the health benefits of consistent supplement use outweigh any barriers to that use. 23 She may additionally require a cue to action to initiate and sustain use. 24 The current study examined these potential influences on initiation and adherence to micronutrient supplementation among WRA in Vietnam, a population at risk of nutritional deficiencies.
Methods
Parent Study
This cross-sectional qualitative study was conducted within a larger double-blind randomized controlled trial (RCT) known as the PRECONCEPT (double-blind RCT of preconception micronutrient supplementation on maternal and birth outcomes in Vietnam) study, a collaboration between Emory University and the Thai Nguyen University of Medicine and Pharmacy (TUMP). The PRECONCEPT study seeks to assess the impact of weekly preconceptual micronutrient supplements on pregnancy outcomes and early childhood development. 25 The PRECONCEPT study participants were married nonpregnant women (n = 5011) between the ages of 18 and 40, who planned to become pregnant in the next year. Most participants were farmers and lived in 20 rural communes located in 4 districts in Thai Nguyen, a mountainous province in northern Vietnam.
Participants for the parent study were recruited from 20 communes in Thai Nguyen province from October 2011 to April 2012. Village health workers (VHWs) identified and invited currently married women aged 18 to 35 years who were planning to become pregnant, based on lists of WRA that were obtained for each commune from the commune health center (CHC). 25 Following screening and obtaining written informed consent, all eligible women were randomly assigned to 1 of the 3 weekly oral supplements: folic acid, iron–folic acid, or multiple micronutrients. The VHWs visited women every 2 weeks to deliver the supplements and also recorded the number of supplements women did not consume and any symptoms or side effects women experienced. The consumption of the first supplement was observed in person by the VHWs. For the second week, they used phone messaging to remind women and confirmed consumption at the next biweekly visit by the presence of the open blister package. Women were also encouraged to consume supplements on an empty stomach at the same time each week to enhance absorption and minimize side effects. 25 Women were also counseled to take these supplements until they became pregnant, at which point they were switched to daily iron–folic acid supplements for the duration of their pregnancy.
Current Study
Study site and population
This qualitative study on initiation of and adherence to supplementation targeted women and VHWs who were involved in the PRECONCEPT study before or during the summer of 2013. Data collection was conducted in 4 communes that were randomly selected from the 20 communes in 4 districts (1 commune per district). All interview and focus group participants were purposively recruited for the different groups described subsequently by CHC staff and the TUMP liaison for each commune.
Semistructured in-depth interviews were conducted with current and former PRECONCEPT participants, including nonpregnant women currently taking 1 of the 3 PRECONCEPT supplements, pregnant women taking daily IFA, postpartum women who had completed the PRECONCEPT and antenatal regimens, and women who had dropped out of the study (Table 1). These subgroups were selected to assess whether women’s attitudes toward supplements were affected by their level of perceived “success” with the PRECONCEPT supplement regimen, as determined by whether they had conceived, carried a healthy pregnancy to term, and/or continued participating in the study.
Summary of Study Methods, Participants, and Domains of Interest.
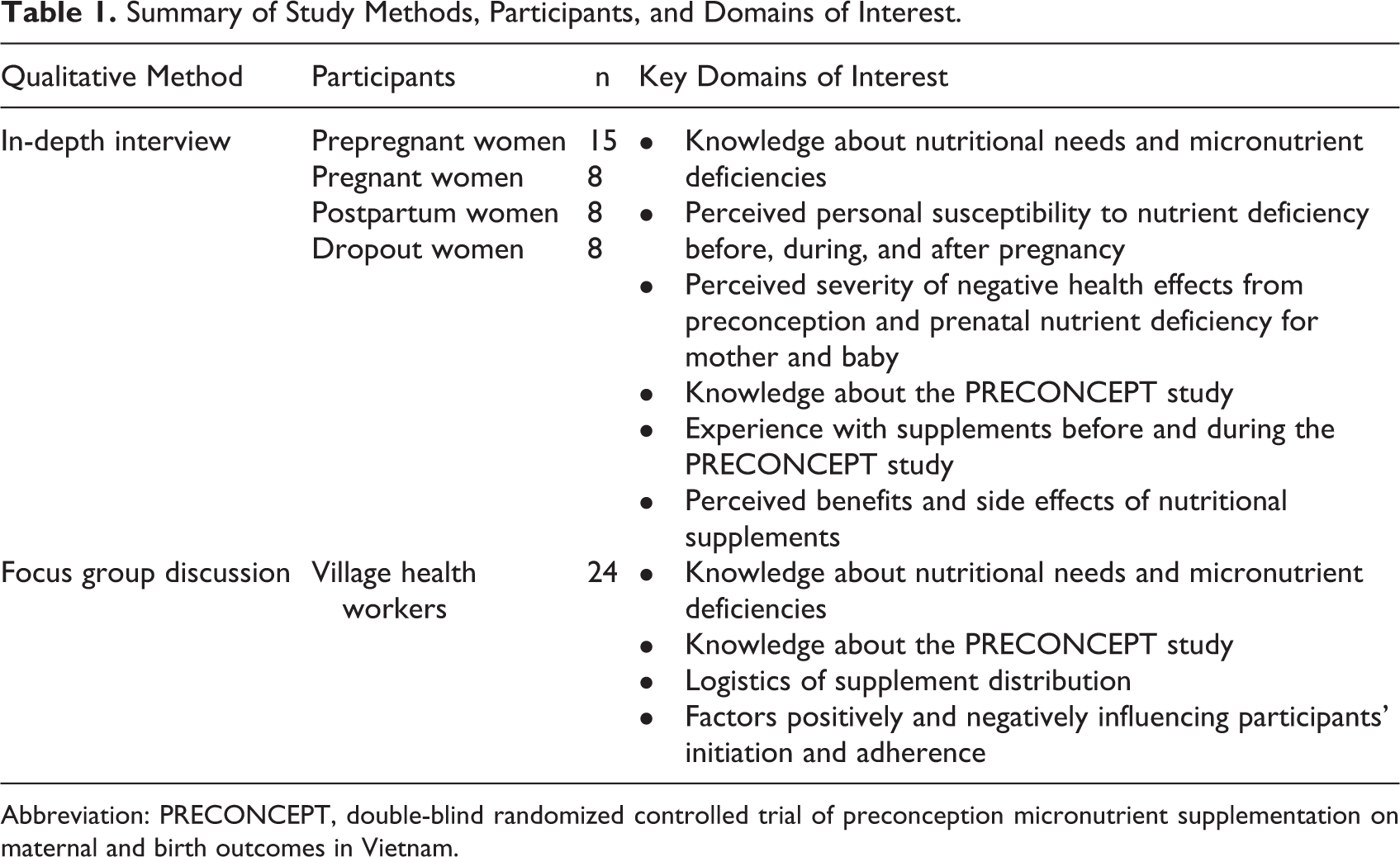
Abbreviation: PRECONCEPT, double-blind randomized controlled trial of preconception micronutrient supplementation on maternal and birth outcomes in Vietnam.
In addition, 4 focus group discussions were conducted, 1 per commune, with 6 participating VHWs each. All participating VHWs were responsible for PRECONCEPT supplement distribution, counseling participants, and participant follow-up.
Study instruments
One focus group discussion guide and 4 in-depth interview guides (tailored to each subgroup of participants) were developed in collaboration with the PRECONCEPT study team. The interview guides shared a base of common questions and included additional questions based on participation status. Interviews with participants focused on each woman’s individual experience with supplement use and her perceptions around nutrition, prepregnancy and prenatal health, and supplements. Domains of interests were designed to assess participants’ perceptions of micronutrient deficiency as a threat to their health and their views of supplementation as an answer to that threat, with a focus on perceived barriers and facilitators of continued adherence. To complement these individual histories and perceptions, the domains of interest for the focus groups were designed to elicit broader perceptions of the facilitators and barriers to initiation and sustained adherence of supplement use among the study population, building from the VHWs’ experience supporting multiple participants in a diverse range of villages.
Procedures
All interviews and focus groups were conducted by trained research assistants in Vietnamese in private rooms at the CHC. Interviews and focus groups were digitally recorded with the consent of participants. These recordings were later transcribed verbatim and translated by trained TUMP staff into English prior to analysis. The accuracy of the translations was verified by the second author (P. N.) who is bilingual (English and Vietnamese).
Translated transcripts were coded using MAXQDA10 software and analyzed according to the principles of grounded theory. 26 Comparative analysis was conducted across commune and participation status as well as by inductive subgroups identified during the coding process. Several strategies were used to ensure the reliability and validity of the analysis. The first author (M. N.), who was responsible for the coding scheme and conducting the analyses, clarified the meanings of categorizations by working closely with team members in the study site in Vietnam. The themes of the coding scheme were also further validated by the coinvestigator/second author (P. N.) who is from Vietnam.
Ethical considerations
This study was approved by the institutional review board (IRB) of Emory University as closely aligned with the goals and aims of the previously approved PRECONCEPT study and was added as an amendment to that study (IRB #51384). Written informed consent was secured from participants before all interviews and focus group discussions. Informed consent was also obtained for digital recording of the interviews.
Results
A total of 39 in-depth interviews were conducted with current and former PRECONCEPT participants, including 15 nonpregnant women currently taking 1 of the 3 PRECONCEPT supplements, 8 pregnant women taking daily IFA, 8 postpartum women who had completed the PRECONCEPT and antenatal regimens, and 8 women who had dropped out of the study. Several themes were identified during analysis and related to (1) perceived susceptibility to anemia and awareness of iron supplementation, (2) perceptions of other nutrient deficiencies as health threats and supplements as a treatment for these, and (3) initiation and maintenance behaviors. These themes are described subsequently, beginning with impacts on initiation, followed by implications for adherence. Women expressed high perceived susceptibility to anemia and benefits of iron–folic acid supplements during pregnancy.
Awareness of the causes, consequences, and preventive strategies for anemia in pregnancy was high across all categories of participants. Anemia was universally understood as a consequence of iron deficiency, and most women understood that iron was needed to produce blood, that their bodies needed to produce more blood during pregnancy, and that not having enough blood could harm themselves and their babies. Other causes of anemia were not mentioned by women. Iron supplements were considered the primary means of both prevention and treatment of anemia and were believed by most participants to be highly effective. Most participants reported taking iron supplements during a previous pregnancy. Many explicitly stated that they took iron in response to the threat of gestational anemia, whether of their own initiative or on the advice of friends or health workers. I knew that during pregnancy, I had to take iron supplements [ …] to replenish my blood. We lose a lot of blood during pregnancy and delivery. (A9—Prepregnant woman, Phan Me) Iron supplies nutrients for the blood, so the body has enough blood. [ …] I took iron to have enough blood during my last pregnancy. (D9—Dropout, Lam Vy) When I went to the Commune Health Center [during my previous pregnancy], they told me to buy and take iron supplements so I would have enough blood. (B6—Postpartum woman, Binh Long) [Women] should take supplements because most women are anemic. No one isn’t—only a few. (C1—Postpartum, Khoi Ky, previously diagnosed with anemia) Women expressed low perceived awareness of severity and susceptibility to micronutrient deficiencies other than iron.
Following iron, the most common supplements women had taken previously, either during pregnancy or outside pregnancy, were vitamin C and a range of B vitamins, particularly B1, B6, and B12. Despite being a component of antenatal supplements, awareness of folic acid was very low. While many women recognized a general association between the mother’s nutritional status and her child’s health, they could not describe specific ways that micronutrient deficiencies other than iron could affect their own health or fetal or early childhood development. Unlike iron, which participants noted could serve both to prevent and to treat anemia, B and C vitamins were considered to serve an exclusively curative purpose. Consistent with low awareness, women appeared to have very low perceived susceptibility to micronutrient deficiencies other than iron. Although some respondents reported taking “Obimin,” a common prenatal multivitamin containing iron and other micronutrients, during a previous pregnancy, such use of multiple micronutrient supplements during pregnancy was reportedly not common in these communities; when it was reported, women typically referred to it simply as “iron” and were not aware of the other micronutrients in the supplement. In general, during pregnancy in rural areas, we just go to the pharmacy for iron supplements. Nothing else.” (C7—Prepregnant woman, Khoi Ky) I didn’t take any supplements before joining this project. [ …] I just took iron when I was pregnant. Besides that, I didn’t take anything. (B3—Prepregnant, Bing Long) Before coming to this project, I only took iron pills. [ …] It was in the Obimin bottle. I only took it when I was pregnant. (C9—Prepregnant woman, Khoi Ky) Before pregnancy, we don’t need iron. Just during pregnancy. (D1—Postpartum woman, Lam Vy) Interviewer: You said in the future, you would take iron supplements only when you were pregnant. Why don’t you want them before this period? Participant: Because I think my child should be provided with sufficient nutrients during the pregnancy. My body has sufficient nutrients before I am pregnant, so I don’t need those tablets. (D4—Pregnant woman, Lam Vy)
Most women agreed that they would initiate use of iron supplements once they knew they were pregnant, whether or not they showed symptoms of anemia. In the absence of pregnancy, however, women relied on symptoms such as dizziness, fatigue, and/or weakness as a cue to seek out supplements, namely C and B vitamins. In the absence of these symptomatic cues, women considered themselves healthy and not susceptible to deficiencies. I won’t take supplements before pregnancy. My health is already good, so it isn’t necessary to take supplements. If my health is weak, I will take them as needed. (B2—Prepregnant woman, Binh Long) In the past, I sometimes took vitamin 3B [a supplement which includes B1, B6, and B12]. [ …] Whenever I felt ill or tired or in pain, I would take this supplement. I bought it myself, or went to the Commune Health Center to ask for advice. When I felt that I had my strength back, I stopped. (A10—Prepregnant, Phan Me) Interviewer: When you took vitamin B1, did you think that was a nutrient? Participant: No, I didn’t. I think it’s a kind of medicine. A medicine for better appetite, to become healthier and less tired. (B8—Prepregnant, Binh Long) I think [Vitamin B and C] are necessary for ill women. I would take them too if I were sick. Normally, they are not that important. (D4—Pregnant woman, Lam Vy) When I’m not pregnant, I won’t take supplements. [ …] I can have better use of that money.” (D9—Dropout, Lam Vy) Once initiated, adherence to micronutrient supplementation regimens was a balancing act between perceived barriers and benefits.
While initiation of supplement use was largely dependent on the perceived severity of and/or susceptibility to nutrient deficiencies and specific cues to action, adherence to an initiated regimen appeared to be influenced by women’s capacity to overcome perceived barriers. Both PRECONCEPT study participants and VHWs identified 2 primary barriers to regular supplement use: forgetting and side effects. These barriers were reported across all communes and participation status groups.
The majority of participants reported having forgotten to take their assigned prepregnancy supplement at least once, with some forgetting repeatedly. Roughly half of these women said they took the supplement when they remembered, and the other half omitted the tablet for that week. Participants who considered the dosing schedule to be very strict tended to omit that week’s supplement if they forgot, while women who viewed the schedule as more flexible were likely to take the supplement when they remembered. Many women felt that the weekly prepregnancy supplement was harder to remember than a daily one, as a daily supplement became part of their routine. For instance, if I forgot one night, I would remember it and take it the following day. I didn’t forget for several days. ( …) I didn’t take it on a scheduled day or hour. For example, today is Saturday and I am supposed to take the supplement. This week I might take it in the morning, but next week I will take it at noon, since whenever I see it, I remember and take it. (A9—Prepregnant, Phan Me) I skip a week [when I forget]. I was told to take the supplement at the exact time every week. I’m afraid that taking it at the wrong time is not good. (B8—Prepregnant, Binh Long) I took [the daily prenatal supplement] every day, I didn’t forget. I remembered very well, since I had to take it every day. I took the prepregnancy supplement every week, so it was easier to forget. (C1—Postpartum, Khoi Ky) Interviewer: What was your main reason for dropping out of the project? Participant: I didn’t remember the schedule of taking the medicine. It wasn’t taken continuously, just one tablet per week, so I didn’t remember. […] If I were taking the medicine continuously, I could remember. (B9—Dropout, Binh Long) I leave the supplements right next to my bed. […] It is good to take the supplements regularly, because they provide enough nutrients for us, provides the nutrients that we lack. (B4—Pregnant woman, Binh Long) We must take the supplements regularly. It is good for our health. I can’t forget any tablets. I must take one tablet a week, and can’t miss it. [… ] Before taking the supplements, I felt weaker. Now I feel much healthier. I can eat more, and work for a long time without getting tired. (A8—Prepregnant woman, Phan Me) I have never forgotten because I have a reminder in my phone. I take my supplements every Thursday. [ …] In the past, I got dizzy all the time. Since I’ve been taking the supplements, I feel less dizzy. (A10—Prepregnant woman, Phan Me) I have never forgotten to take the supplement. […] I felt stronger after taking the supplement. It wasn’t until after I started taking them that I stopped becoming dizzy. (D6—Prepregnant woman, Lam Vy) I didn’t take it on a scheduled day or hour. [The VHW] told me, “You must take it at a regular time,” but I couldn’t remember it. Some days I forgot, some days I remembered. [ …] I haven’t noticed any good effects yet. Maybe I have to wait until I give birth. (A9—Prepregnant woman, Phan Me) My health worker said that it didn’t matter, maybe my body was not used to the supplement at first. I believed her. After taking the supplement, I ate some kind of fruit to avoid the nausea, and after lying down I felt better. [ …] It disappeared naturally. (C8—Prepregnant woman, Khoi Ky) I felt uncomfortable and bloated, but just for a little while. [ …] The VHW said that it was nothing to worry about, those pills were good and there was nothing wrong with them. So I just took them. It was just the side effect. (A2—Pregnant woman, Phan Me)
Discussion
We applied the HBM to better understand barriers and facilitators to the initiation of and adherence to multiple micronutrient supplements among WRA in rural Vietnam. According to the HBM framework, an individual’s decisions to initiate and adhere to a new behavior are influenced by their perceptions of the health threat (in this case, micronutrient deficiency) and of the proposed behavior (oral supplementation). Potentially influential factors include perceived severity of and personal susceptibility to the threat, perceived benefits of and barriers to the new behavior, and the presence of a cue to action to prompt initiation.
Because the research was conducted in the context of an RCT, we did not assess supply issues, which have been identified as a barrier to uptake and adherence in programmatic settings in multiple countries. 27 Our findings indicated that rural WRA in the PRECONCEPT study sites had high perceived susceptibility to anemia during pregnancy and were aware of the consequences of anemia. Women also had strong positive beliefs on the benefits of iron supplementation for the prevention and/or treatment of anemia. Not surprisingly, pregnancy served as a critical cue for initiating IFA supplementation. However, beyond iron and outside pregnancy, we observed low perceived susceptibility to other micronutrient deficiencies, limited awareness of health effects of micronutrient deficiencies, and reliance on physical symptoms as cues to action for initiation of micronutrient supplementation.
These beliefs, combined with the ease of remembering a daily supplement compared to a weekly supplement, may have contributed to the higher adherence to the prenatal daily iron supplementation regimen compared to the prepregnancy weekly multiple micronutrient supplementation regimen. More than three-quarters of women in the PRECONCEPT trial consumed 100% of the daily IFA tablets provided during pregnancy and 20% consumed 80% to 99% of received tablets. 28 However, <60% consumed 100% of the prepregnancy weekly supplements. Such high adherence to IFA supplements during pregnancy is not uncommon in Vietnam, where supply and delivery are ensured. A 3-arm RCT of antenatal iron or multiple micronutrients in Ha Nam province reported compliance as high as 96% of provided supplements consumed. 29 Recent operations research of an antenatal IFA supplementation program in Nghe An province in Vietnam reported that over 95% of women consumed at least some iron tablets in their most recent pregnancy, with the mean duration of supplementation approaching 5 months. 18
The national nutrition survey in 2010 found that anemia affected 29% of nonpregnant women and 36.5% of pregnant women. 30 The PRECONCEPT baseline survey data 31 indicated that prevalence of anemia varied greatly across participating communes, ranging from a low of 9% to a high of 36%. However, interview participants across all 4 communes expressed a similar and high level of perceived personal susceptibility to anemia during pregnancy, suggesting that perceived susceptibility may not be dependent on personal experience with or exposure to the condition, though we cannot rule out that women may have had relatives or neighbors with anemia, which may have increased personal perceived susceptibility. The high awareness of gestational anemia and self-reporting of previous prenatal iron supplementation indicate success in the Ministry of Health’s campaign to improve knowledge and awareness of gestational iron deficiency and to increase coverage of iron supplementation during pregnancy. 32 However, national trends are not known, as uptake of IFA supplements during pregnancy was not reported in recent population-based nutrition surveys. 30,33
The belief that, outside pregnancy, micronutrients are medicines and used only in response to a typology of symptoms is a potential barrier to programs that promote prepregnancy preventative micronutrient supplementation, especially in light of low perceived susceptibility to and consequences of deficiency. Because physical symptoms served as the cue to action for most women, women who may have subclinical or asymptomatic deficiencies are unlikely to view nutrient deficiency as a serious health threat or to initiate supplement use as a means to address it. Results from a meta-synthesis 15 identified a similar medicalization of iron supplements as a barrier to antenatal iron supplementation programs. Changing social norms about the beneficial role of micronutrient supplements as preventative as opposed to curative and increasing perceptions of susceptibility to and severity of deficiency likely requires contextualized social marketing efforts. Such community-based social marketing strategies have been successful for weekly IFA supplements in WRA in Vietnam. 34 Similar lessons from that and other work should be considered if governments elect to scale up preventative multiple micronutrient supplements for nonpregnant women.
As has been reported in other qualitative work, 15 adherence to supplementation regimens was influenced by women’s beliefs in the positive attributes of the supplements, which were reinforced if they noticed positive physical changes in themselves. Forgetting and side effects were the 2 most commonly cited barriers to adherence; women overcame these by developing strategies to remember and from the counseling they received from VHWs. These findings corroborate and extend previous research on supplementation adherence. Negative side effects and forgetting have been consistently recognized as significant barriers to adherence of antenatal micronutrient supplementation regimens, 3,17 –20,35 –37 and more broadly for medication adherence, including patient adherence to HIV and tuberculosis treatment. 38 –43 Perceived health benefits of supplements, including those actually experienced by users, have been found to facilitate continued maintenance of a supplementation regimen. 1,3,16,18,19
Based on these findings, we can identify several strategies to facilitate adherence once supplement use has been initiated. The first is flexible dosing schedules. Women who perceived the weekly dosing schedule as very rigid (ie, same day/time of day) were more likely to not take their weekly dose after forgetting, whereas women who perceived a more flexible dosing schedule would take it as soon as they remembered. More flexible dosing schedules have been shown to be as effective as more rigid schedules for both antenatal IFA supplementation 44,45 and micronutrient supplementation in children. 46 The second strategy would be to utilize formulations that minimize side effects; for example, using alternative forms of iron or the use of micronutrient powders (MNPs) instead of tablets. The iron in MNPs is lipid encapsulated, which aids digestion and reduces gastrointestinal side effects when prepared correctly. 47 Furthermore, because MNPs are added to food, they may have higher acceptability among women who view tablet supplements as medicine and thus taken only on a curative basis. Finally, adequate counseling and social support mechanisms, consistently identified in other studies as essential to increasing adherence, 15,48 –50 should be considered to reduce forgetting and improve women’s capacity to manage side effects. Women reported feeling encouraged by the support and counseling they received from VHWs and CHC staff, particularly reassurance about the health benefits of the supplements, as well as strategies to overcome the barriers of forgetting and side effects. However, health workers in Vietnam and elsewhere are frequently overburdened 49 and may have limited skills or training in interpersonal counseling 50 ; thus, community health workers may prioritize provision of curative care over more preventative strategies such as nutrition counseling. 48 –50 Scale-up of a supplementation program for nonpregnant women, which would be an additional activity for VHWs, will require alternative community-based sources of support, such as the establishment of support groups for WRA. There is evidence that peer support may improve adherence to self-managed treatment regimens 23 through the mechanism of “functional support based on sharing of information and experience, mutual counseling, and exchange among peers.” 24
Other commonly identified barriers to adherence were not observed in this setting. Participants in this study and the larger RCT self-reported high levels of attendance to antenatal care and use of some prenatal IFA supplements during a previous pregnancy, 25 suggesting that coverage and access were not significant barriers. There was no mention among participants of the fear of delivering a large baby which has been noted in other contexts. 51 While these potential barriers were not cited as such by this population, research in other countries has found that, when present, they can present significant roadblocks to adherence. 13,17
Strengths and Limitations
This study is the first qualitative exploration of factors that may influence both initiation of and adherence to micronutrient supplementation among nonpregnant WRA in a developing country. Using the framework of the HBM, the authors were able to more systematically examine important factors related to supplementation uptake in this population. As a substudy of a long-term trial operating in multiple sites, the researchers had the opportunity to assess influences on initiation of and adherence to supplementation at various stages of participation and across a range of demographics and nutritional statuses. The diversity of the participant pool provided unique insight into women’s perceptions of supplement effectiveness and challenges to adherence.
It is important to note that PRECONCEPT was an efficacy trial with relatively high individual support, monitoring, and incentives for compliance, and adherence was consequently higher than might be expected among the general population. Adherence has been repeatedly shown to suffer in the scale-up from such efficacy trials to regional or national supplementation programs. 13,14 Issues related to costs and sustainability that were not barriers in the present study also need to be considered. The role of food-based approaches, which may be viewed as a more sustainable approach to improving micronutrient intakes, needs to be compared to supplements, which may be more highly valued and more effective in selected settings and/or for subgroups at greatest risk. Therefore, it is particularly crucial to consider how this study’s findings may help improve the effectiveness of future programming both in Vietnam and elsewhere.
Conclusion
Initiation and continued adherence are 2 of the foremost challenges for supplementation programs. This study aimed to better understand these challenges in the context of Vietnam using the HBM to guide the study of factors influencing these 2 key stages of supplementation practice. Results from the study supported the model in explaining women’s behavior around preconception supplementation. They suggested that the first stage, initiation, may be directly influenced by a woman’s beliefs about the severity of nutrient deficiencies and her personal susceptibility to developing these deficiencies. The second stage, adherence/maintenance, may be influenced by the woman’s perceptions of the health benefits of, and barriers to, regular supplement use. By identifying the primary influences on each stage, the complex problem of supplementation may be broken down into resolvable components, at which point action can be taken to address key barriers and reinforce facilitating factors.
Footnotes
Authors’ Note
Meredith Nechitilo participated in developing the research questions, conducting data collection in the field, performing the analysis, and drafting and revising manuscript. Phuong Hong Nguyen is a coinvestigator of the study and contributed to writing proposal, developing the research questions and study design, overseeing data collection, and providing inputs for drafting and revising manuscript. Amy Webb-Girard, Ines Gonzalez-Casanova, and Ann DiGirolamo provided inputs/comments for the analysis and edited and revised the manuscript. Reynaldo Martorell is a coinvestigator of the study and provided inputs/comments for the manuscript. Usha Ramakrishnan is the principal investigator of the study and contributed to writing proposal, developing the research questions and study design, overseeing the study, and providing comments/inputs for manuscript. All authors contributed to the development, review, and approval of the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by the Mathile Institute for the Advancement of Human Nutrition, the Micronutrient Initiative, and the Rollins School of Public Health Global Field Experience fund.