
Abstract
Background:
Vitamin A (VA) deficiency (VAD) is still a concern in many parts of the world, and multiple intervention strategies are being implemented to reduce the prevalence of VAD and associated morbidity and mortality. Because some individuals within a population may be exposed to multiple VA interventions, concerns have been raised about the possible risk of hypervitaminosis A.
Objectives:
A consultative meeting was held in Vienna, Austria, in March 2014 to (1) review current knowledge concerning the safety and effectiveness of large-scale programs to control VAD, (2) develop a related research agenda, and (3) review current available methods to assess VA status and risk of hypervitaminosis A.
Methods:
Multiple countries were represented and shared their experiences using a variety of assessment methods, including retinol isotope dilution (RID) techniques. Discussion included next steps to refine assessment methodology, investigate RID limitations under different conditions, and review programmatic approaches to ensure VA adequacy and avoid excessive intakes.
Results:
Fortification programs have resulted in adequate VA status in Guatemala, Zambia, and parts of Cameroon. Dietary patterns in several countries revealed that some people may consume excessive preformed VA from fortified foods.
Conclusion:
Additional studies are needed to compare biomarkers of tissue damage to RID methods during hypervitaminosis A and to determine what other biomarkers can be used to assess excessive preformed VA intake.
Introduction
Vitamin A (VA) deficiency (VAD) affects 190 million children less than 6 years of age worldwide, occurring most frequently in sub-Saharan Africa and South and Southeast Asia. 1 While VAD is a public health problem, high-dose VA supplementation has proven effective in reducing morbidity, mortality, and blindness in young children. 2 In such settings, the World Health Organization recommends high-potency VA supplementation every 4 to 6 months for children 6 to 59 months of age. 1 Other intervention strategies are also available to reduce the risk of VAD. Fortification of common foods with VA, such as cooking oil, table sugar, bouillon cubes, cereal flour, or dairy products, 3,4 can be a cost-effective intervention for reducing VAD where there is a suitable food vehicle, and the national food industry is sufficiently developed to implement this technology. Additional approaches to control VAD include agricultural interventions and dietary modification strategies to increase the production, availability, accessibility, and consumption of VA-rich foods as well as continuous supplementation with low-dose VA in products such as micronutrient powders and small-quantity lipid-based nutrient supplements.
As countries begin to deploy multiple interventions to reduce VAD, often managed by independent entities in both public and private sectors, the risk of excessive VA intake must also be considered. Thus, it is important to determine whether these programs do in fact place some individuals at risk of hypervitaminosis A; and, if so, how the programs could be modified to reduce this possibility while still providing the benefit of VA to those at risk of deficiency. Assessing the impact of combined VA supplementation and food fortification is difficult because of the limited responsiveness of serum retinol concentrations to interventions that increase VA intake. 5,6 Among the currently used VA biomarkers (Table 1), 7,8 more sensitive biomarkers of VA status are needed to evaluate the effectiveness and safety of VA interventions across the full spectrum of VA status from deficiency through hypervitaminosis A.
Current Cutoffs Used for Vitamin A Deficiency or Hypervitaminosis A Status for Common Biomarkers of Status.
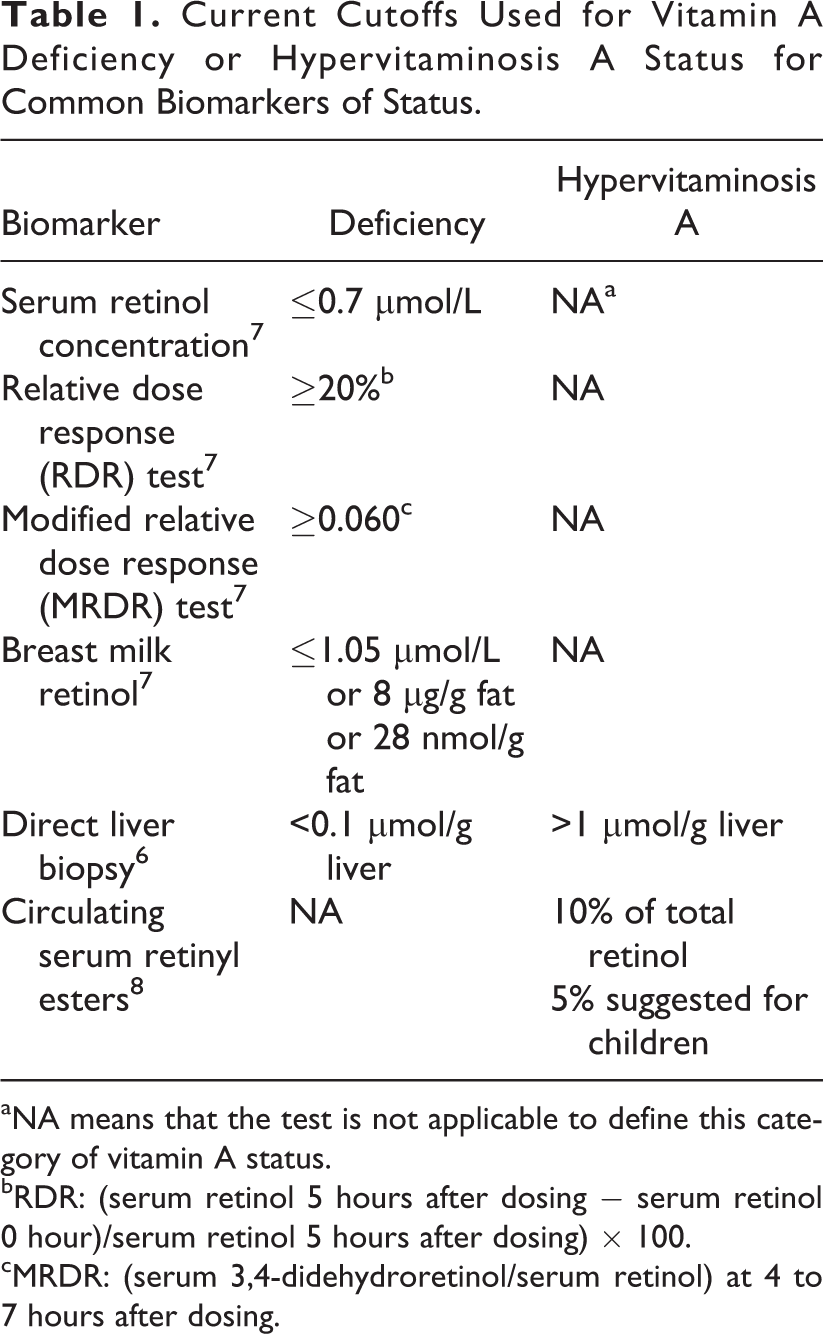
aNA means that the test is not applicable to define this category of vitamin A status.
bRDR: (serum retinol 5 hours after dosing − serum retinol 0 hour)/serum retinol 5 hours after dosing) × 100.
cMRDR: (serum 3,4-didehydroretinol/serum retinol) at 4 to 7 hours after dosing.
The retinol isotope dilution (RID) method is one of the few methods available to monitor the VA status of populations, including young children, across the full range of statuses. 6,9 However, there are still some methodological issues that need to be addressed to ensure the validity of the method in settings with high rates of infection and inflammation, concurrent micronutrient deficiencies, or very high hepatic VA content.
This series of 3 papers report on a technical meeting co-organized by the International Atomic Energy Agency and The Bill & Melinda Gates Foundation with the objectives to review current knowledge of the safety and effectiveness of large-scale interventions intended to prevent VAD and to develop a research agenda for assessing, monitoring, and preventing health risks of excessive VA intake in populations. Areas of discussion covered biomarkers of VA excess, the strengths and limitations of the RID methods for assessing VA excess in field settings, and how best to monitor and evaluate VA intervention programs.
Hypervitaminosis A
Although there is concern that exposure to multiple VA intervention programs may result in VA intakes 10 above current recommended intakes (Table 2), clinically detectable signs of VA toxicity are rare. Acute toxicity has been reported in arctic areas among individuals consuming polar bear liver, which is very high in VA; and case reports of chronic toxicity have been published for individuals consuming ≥30 000 μg/d (105 μmol/d) for several months. 11 -13 Clinical symptoms include increased cerebro-spinal fluid pressure, brain swelling, bulging fontanelle in infants, double vision, headache, skin exfoliation, bone pain, hemorrhages, liver enlargement and fibrosis, and ultimately death. 11,12 Chronic VA intakes >1500 μg/d (5.2 μmol/d) have been associated with an increased risk of hip fracture in 2 studies, 14,15 but the opposite effect was noted in 2 other studies, which found a positive association between dietary VA and bone mineral density in premenopausal women. 16,17
Recommendations for Vitamin A Intake (µg RAE or RE/d) by Age or Population Group by the Institute of Medicine and the Food and Agricultural Organization. The Tolerable Upper Intake Level is Based on Preformed Retinol Alone.
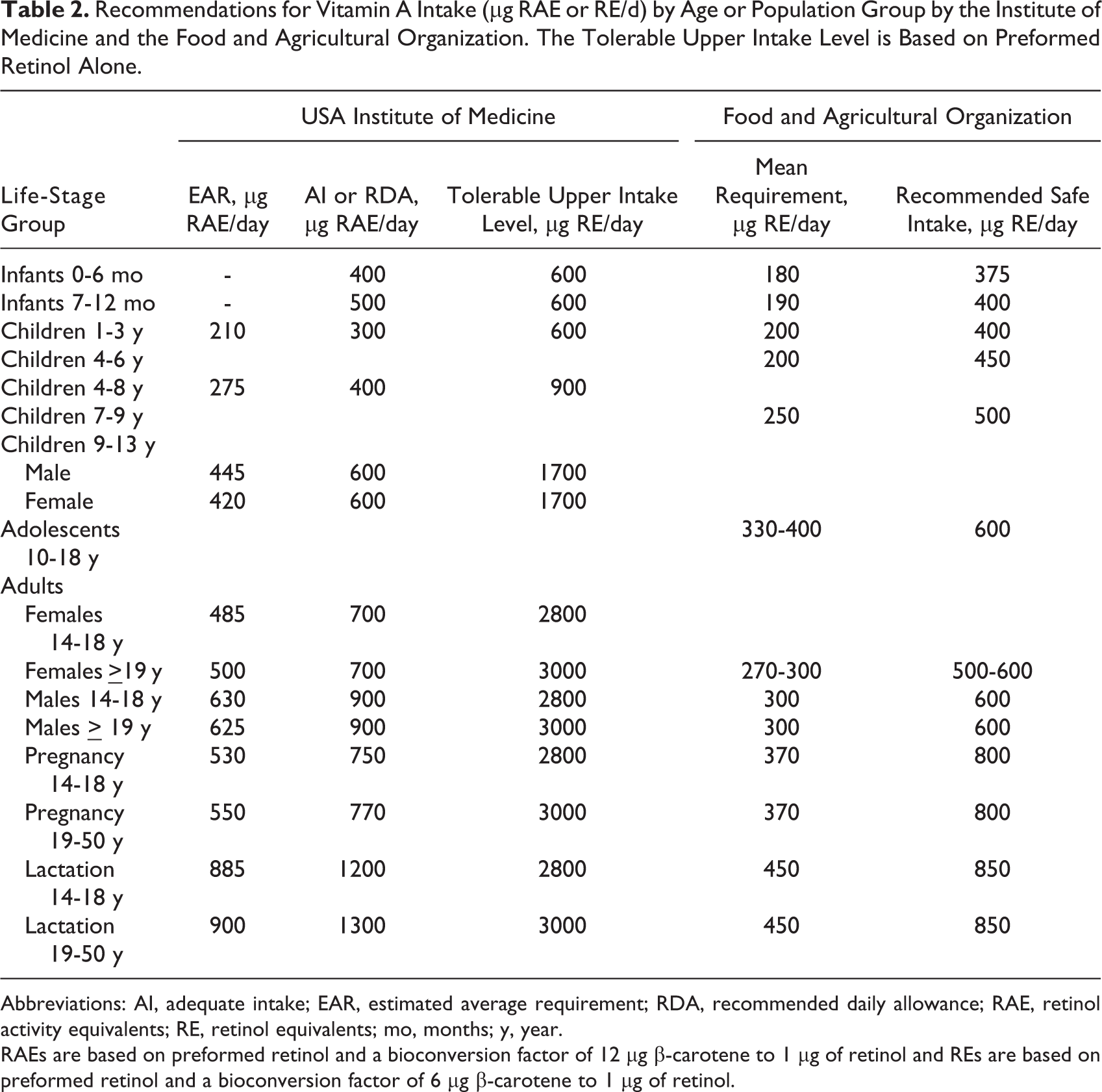
Abbreviations: AI, adequate intake; EAR, estimated average requirement; RDA, recommended daily allowance; RAE, retinol activity equivalents; RE, retinol equivalents; mo, months; y, year.
RAEs are based on preformed retinol and a bioconversion factor of 12 μg β-carotene to 1 μg of retinol and REs are based on preformed retinol and a bioconversion factor of 6 μg β-carotene to 1 μg of retinol.
In North America, the acceptable tolerable upper intake levels (ULs) for VA intake are extrapolated from the “lowest-observed-adverse-effect levels” (LOAELs) of intake, which are based on a small number of case reports of VA toxicity. 13 The ULs are set at the “no-observed-adverse effect levels” (NOAEL) of VA intake that are derived from the LOAELs based on “uncertainty factors.” For infants and young children, the LOAEL is 6000 µg/d, and it was obtained by averaging the lowest level of VA intake in 4 case reports of hypervitaminosis A. An uncertainty factor of 10 was used to set the UL at 600 µg/d. The UL of 600 µg/d applies to infants and children up to 3 years of age (Table 2). Because of the scarcity of data on which to base ULs for VA intake, an approach called “key events analysis” has been used to identify early biomarkers of excessive VA status. This analysis involves determining the major biological steps that occur physiologically in an effort to maintain homeostasis to define the VA dose exposure that leads to excessive systemic levels and subsequently to increased adverse event risk. 18 Potential biomarkers that need further investigation at the population level to indicate excessive status include elevated serum concentrations of retinyl esters (described further in paper 3 of this series), retinoic acid and its polar metabolites, the retinol to retinol-binding protein (RBP) ratio, liver transaminases, and serum markers of hepatic fibrosis and bone demineralization. However, liver function tests may be less useful in populations with underlying liver abnormalities related to infectious hepatitis, chronic malaria, and exposure to environmental toxins, such as aflatoxin. Breast milk retinol concentration reflects maternal dietary VA intake and may be useful as a marker of excessive intake in populations exposed to multiple VA interventions. Expression of VA-responsive genes, adipose tissue biopsies, and liver VA concentration obtained from biopsy or autopsy specimens may also be useful for assessment of excessive VA status.
Stable Isotope Dilution Methodology for Assessing Impact and Safety of VA Interventions
The RID technique provides a quantitative estimate of total body VA pool size and liver VA concentration. This is based on the assumptions that 80% to 90% of the total body VA is stored in the liver of well-nourished individuals, and the weight of the liver has a fixed relationship with body weight at different ages. 19 The technique is responsive to supplementation with VA and has been used successfully in apparently healthy populations in low-income countries to assess the efficacy of VA interventions and to estimate VA requirements. 3,4,20 -26 Recently, compartmental modeling of human VA kinetic data has been used to develop a shorter stable isotope dilution method for easier application in field settings and for predicting the efficacy and safety of VA interventions. 27 These models can be useful for assessing both the potential efficacy of interventions for increasing VA status and the potential risk of toxicity in populations exposed to multiple VA interventions.
Although the RID technique is clearly useful for assessing the impact of VA interventions in populations with low to adequate VA status, more work is needed to determine whether the technique provides an accurate estimate of total body stores of VA when status is excessive. There is concern that the stable isotope tracer may not fully mix with VA that is stored in liver stellate cells or in other extrahepatic storage pools with slow turnover rates when VA stores are very high. This phenomenon will underestimate true total body stores because the tracer is not equally distributed among VA-containing pools. Also, intestinal malabsorption, infection, inflammation, and iron deficiency may affect the accuracy of RID techniques. 28 -32 In these cases, total body store calculations will overestimate actual stores because the serum to liver ratio of the tracer to tracee may be lowered during these situations. For example, studies in children indicate that intestinal absorption of VA is reduced, and urinary retinol losses are increased during febrile infections, 28 -30 which affects the individual estimates of dose absorbed. Kinetic studies in rats suggest that hepatic mobilization of retinol is reduced in inflammation and iron deficiency and that the serum isotopic ratio of labeled to nonlabeled VA may be reduced compared with the ratio in liver. 31,32 These conditions could affect the accuracy of estimates of total body VA stores. Populations in low-income countries often have high rates of infection, inflammation, and other nutrient deficiencies. 33,34 Thus, more work is needed to better understand how to apply RID techniques in this context.
Country Reports of Large-Scale VA Intervention Programs
Using dietary data to assess the risk of excessive VA intake
The potential risk of excessive dietary VA intake in populations exposed to large-scale fortification programs has been investigated in Guatemala and Cameroon. In the 1960s, hypovitaminosis A was common in Central America; and in 1981, Arroyave et al reported that 83% of families were consuming <50% of recommended VA intakes. 35 In response to these observations, a national fortification program was temporarily initiated in Guatemala and subsequently relaunched in 1988. In 2011, the Ministry of Health in Guatemala completed a survey in women (15-49 years old) and children (6-59 months of age), which included assessments of serum retinol, RBP, and the amount of fortificant in sugar. When the concentration of VA in the sugar is combined with national sugar consumption and fortification coverage data, mean VA intake from fortified sugar can be estimated. No children had serum retinol concentrations <0.7 μmol/L, and only 5% of women had values <1.05 μmol/L. Furthermore, in a subset of women and children, the modified relative dose–response test, which is an indirect qualitative measure of liver stores, was normal. Only 1 child tested above the cutoff for deficiency, defined as a 3,4-didehydroretinol to retinol ratio > 0.060 (Table 1; unpublished observations). These results indicate that in the presence of the sugar fortification program, VAD is no longer a public health problem in Guatemala.
Currently, 5 mg VA/kg sugar is the mandated minimum level of fortification in Guatemala, and 15 mg/kg is the target level. In household surveys of sugar fortification levels, 80% to 93% of households had sugar VA concentrations above the mandated minimum level of fortification. Based on household-level dietary intake data, it was estimated that with a VA concentration of 9 mg/kg sugar, almost all children would consume more than the estimated average requirement, and most children’s consumption would be in the safe range of intakes. However, because of concern that some children may be consuming more than the UL, Guatemala is planning to lower the target fortification level to 7 mg/kg sugar; although to date, this has not occurred. Moreover, the government now recommends that VA supplementation should be used only for younger children, and no other foods should be fortified in Guatemala.
Cameroon has a history of clinical VAD, 36,37 so periodic high potency VA supplementation was started in 2002. Mandatory oil fortification was initiated in 2011 as an additional strategy to alleviate VAD. To determine appropriate fortification levels, nationally representative dietary data were used to predict the prevalence of inadequate or excessive intakes, based on the current amounts of VA intake and consumption of the fortified food. Using this type of dietary intake information, it is possible to simulate the effects of fortifying multiple vehicles and using different levels of fortification. A range of fortification levels are used globally. For example, Cameroon fortifies at a level of 12 mg VA/kg oil, 38 compared with 6 mg/kg for Nigeria, 39 10 mg/kg for Ghana, 40 24 mg/kg for Bolivia, 41 and 30 mg/kg for Uganda. 42 At the current level of fortification, it is unlikely that Cameroonian women or children would exceed the UL. However, under simulated scenarios with increased levels of VA in oil or fortification of additional food vehicles, some children in Cameroon would be at risk of consuming more than the UL (600 µg retinol equivalents/d). These simulation models are useful for comparing impacts of fortification in different geographic regions. For example, in Cameroon, the North region appears to have the most room to improve VA intakes, whereas, Yaoundé and Douala, the major metropolitan areas in the southern region, have a greater risk of excessive VA intakes if the proposed level of fortification is actually delivered.
Excessive intakes of VA have also been reported in other countries where multiple foods are fortified with VA. In Uganda, for example, where several VA-fortified foods are available on the market, another dietary simulation study found that 70% of the children residing in the capital city of Kampala would have VA intakes above the UL if multiple food vehicles were fortified at the levels examined. 43 Likewise, in the United States and Canada, 5% to 21% of children from different age-groups are consuming more than the UL with fortified foods. 44,45
Uses of RID Studies to Estimate Requirements and Evaluate Intervention Programs
Population surveys in China have revealed a low prevalence of serum retinol concentrations <0.7 μmol/L among children, ranging from 6% in urban areas to 15% in rural areas. 46 The RID studies were conducted to determine the dietary reference intake for VA in Chinese adults, based on the level of VA intake needed to maintain an estimated liver concentration of 20 μg/g liver (0.07 μmol/g liver). 13 A total of 116 Chinese adults (35-55 years old) consumed a low VA diet supplemented with 0, 200, 400, or 600 μg VA/d. Total body VA content was measured at the beginning and end of the dietary period using 1 mg deuterated retinyl acetate. Serum retinol concentrations did not respond to the intervention. According to the paired RID data, males needed 560 μg and females needed 480 μg retinol activity equivalents (RAE) to maintain the desired liver VA concentrations (unpublished observations).
In Mexico, a national micronutrient status assessment survey in 1999 found that 26% to 50% of children had low serum retinol concentrations, depending on the region of the country. In addition, the mean modified relative dose–response test result in schoolchildren was a 3,4-didehydroretinol to retinol ratio of 0.09, with a range of 0.06 to 0.13, indicating inadequacy. In Mexico, high-dose VA supplementation is targeted to children <4 years old twice per year. A study with children from low socioeconomic status was completed to assess the effect of VA-fortified milk delivered in a school breakfast program. 3 The randomized trial was conducted in 3- to 6-year-old children (n = 27) with initial serum retinol concentrations of 0.35 to 1.05 μmol/L and normal C-reactive protein concentrations indicating lack of inflammation. The children received 250 mL/day of milk that contained 196 μg RAE/d (49% of the recommended daily allowance) for a period of 90 days. After the intervention, estimated liver VA concentrations increased significantly from 0.34 to 0.47 μmol/g liver in the fortified-milk group compared with 0.25 to 0.28 μmol/g liver in the control group, and serum retinol concentrations were higher in the fortified-milk group than the control. A total of 12.4 mg retinol was accrued in the liver, indicating that 70% of the additional VA in the fortified milk was stored. 3
Stable Isotope Methods to Evaluate Pro-VA Carotenoid Activity
Food matrices affect the bioequivalence of pro-VA carotenoids, and studies have reported a wide range of bioconversion factors. 47 Furthermore, it appears that some people can be categorized as either low responders to β-carotene supplementation, in which case serum β-carotene concentrations do not substantially increase, 48 or low converters of pro-VA carotenoids to retinol. 49 These phenotypes may be the result of common genetic polymorphisms, 50,51 which are estimated to occur in 24% and 42% for the 2 most common allele variants. 51 Among other methods, stable isotope techniques have been used to evaluate pro-VA bioavailability. Isotope studies have evaluated β-carotene in oil 48,49,52,53 and demonstrated postabsorptive bioconversion of β-carotene to VA. 49,53,54 Isotopic methods have also been used to demonstrate bioconversion by changes in body stores of VA 21 and uptake of VA from intrinsically labeled, hydroponically grown plants such as spinach, carrots, 55 spirulina, 54 golden rice, 56,57 and orange biofortified maize. 58 Pro-VA biofortification is the process of producing staple foods with enhanced pro-VA carotenoid concentrations either through traditional breeding or genetic engineering. 59 Biofortification of staple crops with pro-VA carotenoids would have less risk of excessive VA intakes than fortification with preformed retinyl palmitate. 60 Recently, physiological amounts of labeled β-carotene were administered to evaluate interindividual variation in β-carotene absorption. 61 Thus, stable isotope methods have moved beyond just evaluation of total body stores of VA.
Program Issues
The final session of the meeting focused on current intervention strategies for controlling VAD and possible approaches for monitoring the risk of excessive VA intake. The first 2 presentations in this session described the efforts of the Global Alliance for VA (GAVA) to develop a framework for program decision making regarding when to transition from high-dose VA supplementation programs to other strategies for ensuring adequate and safe levels of VA intake and is discussed further in article 2 of this series. In particular, the GAVA framework suggests that a preliminary situational analysis be completed to review nationally representative information on dietary intake of VA, markers of population VA status, and coverage of VAD control programs. Because periodic high-dose VA supplementation affects the population distribution of serum retinol concentration for just a limited time period (∼4-8 weeks) following supplementation, GAVA has suggested that this indicator can be used to determine the underlying VA status of the population and need for continued supplementation. In other words, if the distribution of serum retinol concentration assessed at least 8 weeks after a round of high-dose VA supplementation indicates that VAD is no longer a public health problem, periodic VA supplementation should be reevaluated. Global Alliance for VA is currently assessing the feasibility of implementing this program decision-making algorithm in several countries as described in paper 2 of this series. If feasible, these recommendations should be supported with measures of total body stores using RID methods in subgroups.
Public health programs in low-income countries have focused almost exclusively on the control of VAD, and guidelines are not yet available for monitoring possible effects of excessive intakes. As discussed earlier, assessment of excessive intakes remains problematic because of uncertainties surrounding the assessment methods and possible confounding effects of infection and other factors, lack of reference data and/or logistical complexity, and the high cost of implementation in a nationally representative sample of the population. Thus, additional research is needed to evaluate existing biomarkers of excessive intake and/or develop new ones as discussed in paper 3 of this series.
Because the risk of excessive VA intake may be greatest in the presence of concurrent large-scale food fortification and VA supplementation programs, it is important to ensure that the level of fortification is appropriate for the amounts of food vehicle consumed by different subgroups of the population, especially for women of reproductive age and children, and that the actual amounts of fortification fall within the targeted range. The former requires assessment of dietary intake among representative subgroups of the population at risk of inadequate and excessive intakes, and the latter requires periodic sampling and analysis of fortified foods. Examples were presented on the use of dietary data for simulating the impact of fortification programs on total VA intake in Cameroon and periodic sampling of sugar to monitor VA concentration in Guatemala.
Other approaches to deliver VA and avoid the risk of excessive intake were considered. Research indicates that bioconversion of pro-VA carotenoids to VA is regulated by VA status and thus would mitigate hypervitaminosis A risk. 10,59 Thus, delivering additional VA in the form of pro-VA carotenoids in industrially fortified or biofortified foods was also considered. The group that considered industrial fortification with β-carotene concluded that this may be technically and biologically feasible, but the cost of β-carotene is currently greater than the cost of an equivalent amount of VA provided as retinyl palmitate, so the feasibility of this approach is likely to be limited by economic considerations. β-Carotene premix for fortified foods would be even more prohibitive if the fortificant would need to be encapsulated to avoid coloring the food vehicle or introducing other undesirable sensory properties.
Biofortification refers to the process of increasing the nutrient content of foods by means of modified agronomic practices, conventional breeding of high-nutrient varieties, or genetic engineering. 59 Current biofortification programs for VA rely on selective breeding of sweet potato, maize, and cassava for varieties with high β-carotene content or genetic engineering in the case of rice. Criteria were described for determining which crops would be most appropriate in particular countries. Results of efficacy and effectiveness trials indicate that consumption of high-β-carotene orange-fleshed sweet potato increases VA intake and biomarkers of VA status. 62,63 Efficacy trials of biofortified orange maize demonstrate improved VA liver stores, 60 and studies of cassava also suggest positive results on biomarkers of VA status (unpublished observations).
Conclusions and Future Directions
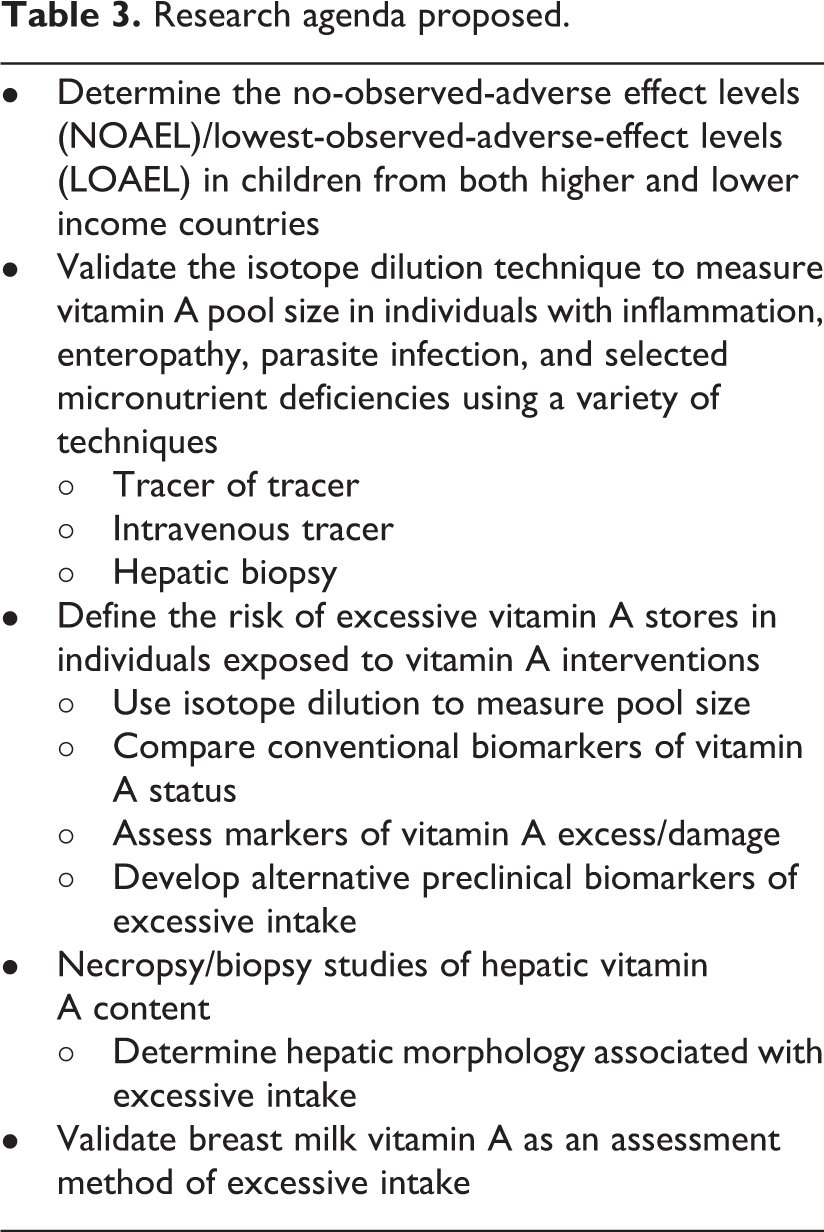
Vitamin A deficiency remains a public health problem in many low-income countries, and large-scale intervention programs are needed to avert mortality and morbidity attributable to VAD. At the same time, it is essential to ensure that intervention programs do not place individuals at risk of excessive VA intake. The RID methods are powerful tools for assessing total body VA content, but additional studies should be performed with concurrent comparisons of tissue damage associated with severe hypervitaminosis A to determine other biomarkers that can be used to assess the risk of excessive intake (Table 3). Measurements to consider include the serum retinol to RBP ratio to determine RBP saturation levels, serum and breast milk retinyl ester and carotenoid concentrations, polar retinoid metabolites in serum and urine, liver enzymes or fibrogenesis markers in the serum, and retinoic acid responsive proteins (eg, retinoic acid receptor-β and cellular retinoic acid binding protein 2). In addition, studies that involve proteomics, expression of VA-responsive genes, or tissue biopsies may shed light on future less invasive methods. Furthermore, it may be possible to examine the amount of tracer absorbed and retained (eg, tracer of the tracer, intravenous, and oral comparisons) to better determine the amount of VA tracer dose absorbed and the effects of inflammation and body composition on RID measurements.
Research agenda proposed.
Another future direction for fortification would be to evaluate β-carotene as a biologically feasible fortificant. β-Carotene fortification is currently not economically feasible. Nonetheless, it could be a safer fortificant, even at higher doses, for a wide range of population risk groups due to regulated bioconversion. Although increased cancer incidence occurred after high-dose β-carotene supplementation in smokers and asbestos workers, 64 lower amounts of dietary β-carotene intake beyond VA requirements are thought to be benign, although they may cause a yellowish or orange pigmentation of the skin, noticeable in the hand palms and foot soles. 8,65 Studies are needed to compare the biological efficacy of β-carotene versus preformed retinyl ester fortification. Although technical feasibility needs to be considered, laboratory studies have shown β-carotene to be stable under controlled conditions, but repeated processing can reduce the antioxidant properties of β-carotene. Incorporating β-carotene into grain products has resulted in losses ranging from 4% to 34%, 66 although a specifically patented version of β-carotene has been incorporated into cereal products (eg, in either a water-insoluble beadlet or particle form) without major changes in color, aroma, or flavor and with minimal risks of oxidation. Technological challenges and economic feasibility need to be considered for β-carotene fortification to be more viable when compared with retinyl palmitate. 67
Research Recommendations
To evaluate the safety of large-scale VA intervention programs, several lines of future research were recommended. First, more information should be obtained to determine the NOAEL/LOAEL in children from both higher and lower income countries. Second, the RID test should be validated in individuals with inflammation, enteropathy, parasite infection, and selected micronutrient deficiencies using a variety of comparison techniques, such as applying a tracer of the VA tracer using an intravenous tracer or measuring VA concentration in hepatic biopsy. Third, the risk of excessive VA intake should be assessed in individuals exposed to VA interventions using the RID test to measure VA pool size, conventional biomarkers of VA status, markers of VA excess/damage, and necropsy/biopsy studies of hepatic VA content and associated hepatic morphology. Finally, breast milk retinol concentrations should be evaluated as a method to assess exposure to excessive VA intake.
Footnotes
Authors’ Note
This is paper one in a series of meeting reports from an International Atomic Energy Agency Technical Meeting (TM-48778) held in Vienna, Austria; March 24-25, 2014; entitled “Assessing Vitamin A Safety in Large-Scale Nutrition Intervention Programmes: Setting the Research Agenda”. Sherry A. Tanumihardjo acted as guest editor for this series.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.