
Abstract
Background:
The nature and severity of 3 categories of maternal stressors (nutritional, infectious, and psychosocial) that may impact maternal health and early infant growth are not often considered together.
Objectives:
To describe quantitative methodologies; assess construct validity of questionnaires; report variability in sociodemographic, obstetric, nutritional, infectious, and psychosocial characteristics; and compare characteristics between pregnancy and lactation and between study cohorts of Mam-Mayan mother–infant dyads.
Methods:
Grounded in participatory action research and a socioecological framework, this observational study enrolled a longitudinal cohort of 155 women, followed during pregnancy (6-9 months), early (0-6 weeks), and later (4-6 months) postpartum, and 2 cross-sectional cohorts (60 early and 56 later postpartum). Household and social factors; obstetric history; nutritional, infectious, and psychosocial stressors; and infant characteristics were explored.
Results:
Diet diversity (3.4 ± 1.3) and adult food security (38%) were low. Urinary and gastrointestinal infections were rare (<5%), whereas experience of local idioms of distress was frequent (20%-50%). Participants reported low maternal autonomy (81%), high paternal support (70%), small social support networks (2.7 ± 1.3 individuals), and high trust in family (88%) and community-based institutions (61%-65%) but low trust in government services (6%). Domestic violence was commonly reported (22%). Infant stunting was common (36% early postpartum and 43% later postpartum) despite frequent antenatal care visits (7.5 ± 3.8). Participant engagement with the research team did not influence study outcomes based on comparisons between longitudinal and cross-sectional cohorts.
Conclusions:
The variability in sociodemographic, nutritional, and psychosocial variables, will allow exploration of factors that promote resilience or increase vulnerability of the mother–infant dyad.
Keywords
Background
Within the context of health of mother–infant dyads in impoverished developing country populations, maternal nutritional status, diet diversity, 1,2 and child nutritional status 3,4 have received the most attention. However, there is evidence that a much wider range of maternal factors is involved. Maternal hookworm infection, 5 urinary tract infection, 6 and periodontal disease 7 have each been associated with intrauterine growth retardation and low birth weight (LBW). In addition, rural place of residence, low socioeconomic status, and marginalized ethnicity 1,8 ; poor social support 9 ; poor maternal autonomy and self-efficacy 10 ; and maternal experience of violence 11 have been associated with stunting. Finally, maternal anxiety and depression have been associated with impaired infant growth in both developed and developing countries. 12,13 In indigenous cultures, these conditions are described through local idioms of distress 14,15 and remain largely unexplored in their impact on maternal–child health.
Despite the diversity of factors known to influence the health of the mother–infant dyad, there remains a large gap in our understanding and in our ability to implement effective measures to promote health. 4 Recent calls for greater consideration of social, cultural, and other context-specific factors in global health 16,17 require researchers to bridge disciplines and think beyond conventional frameworks. In response to such a request, we propose a socioecological conceptual framework (Figure 1) that recognizes 3 broad categories of stressors (nutritional, infectious, and psychosocial) that may cumulatively affect the mother and ultimately impact her infant. The nature and severity of these stressors, and how a mother experiences them, are in turn directly influenced by social (social capital, gender relations, and cultural norms) 9 -11 and sociodemographic (living conditions and food security) 1,8 factors, which may either promote resilience or increase vulnerability.
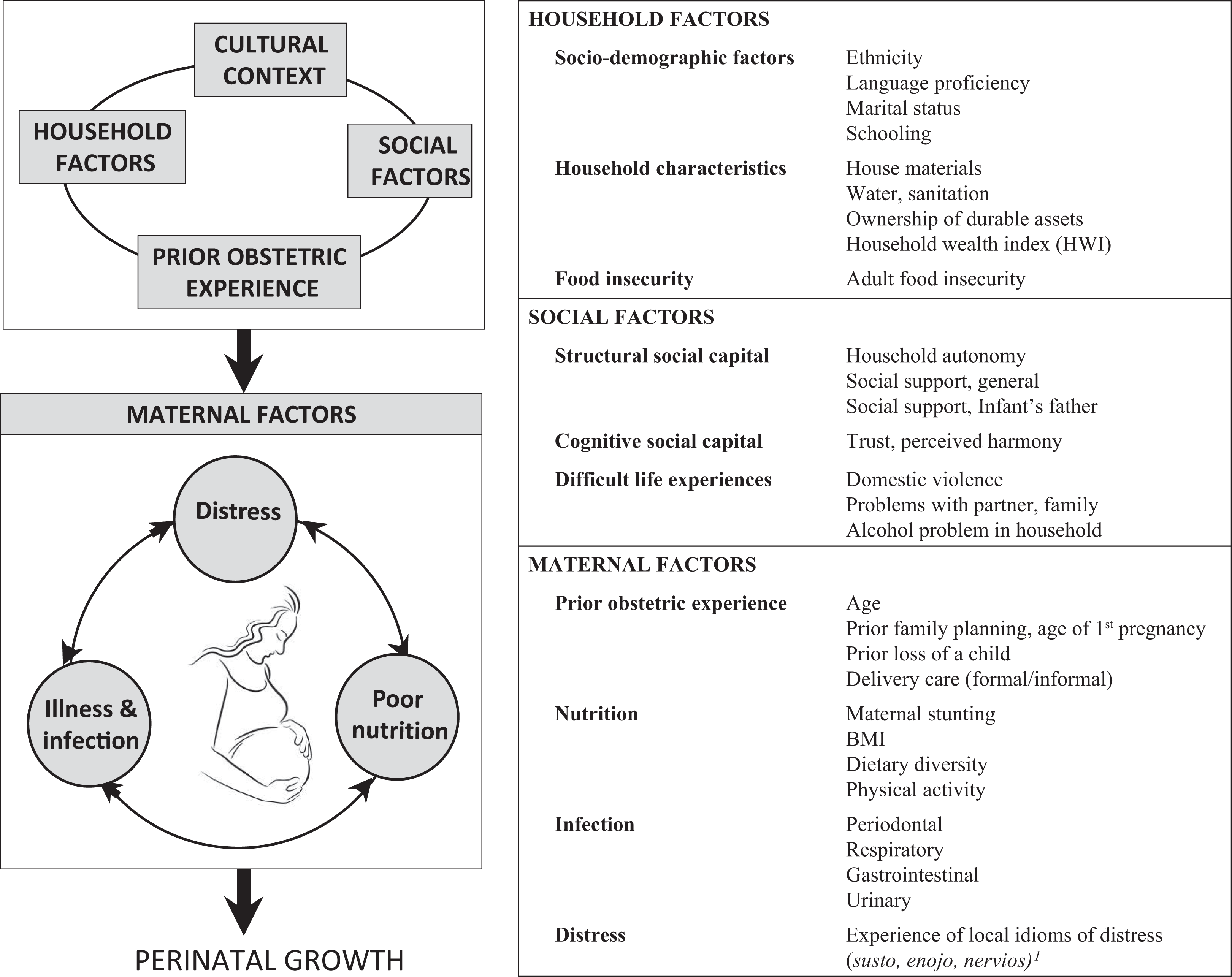
Conceptual socioecological framework that distinguishes 3 broad categories of stressors affecting the mother (nutrition, infection, and psychosocial distress) that may cumulatively impact the health of the maternal–infant dyad. Susto, enojo, and nervios are local idioms of distress. Susto is believed to result from a frightening or startling experience, which manifests as an array of symptoms and pathologies. Enojo is a form of anger that leads to headaches, stomach pains, weakness or fatigue, and chronic illness. Nervios is an illness due to experiencing strong emotions, particularly anxiety, grief, and sorrow.
Using a participatory action research (PAR) approach, 18 we conducted a mixed methods study in indigenous Mam women in the Western Highlands of Guatemala to assess the diversity of household, social, and individual-level factors related to maternal nutrition, infection, and psychosocial distress that may influence the health of the mother–infant dyad from the sixth month of pregnancy to 6 months postpartum (PP). Although Guatemala has the highest percentage of stunting in Latin America and among the 10 worst worldwide, 8,19 stunting rates reach over 80% of children younger than 5 years in some Western Highland indigenous communities, 19 where prior work by our group has shown that up to 38% of infants are already stunted at birth, 20 implying that maternal influences during pregnancy require further attention.
As the first in a series, this article presents the quantitative methodologies, including an assessment of internal consistency and construct validity of questionnaires, and the descriptive results emerging from the quantitative component of the study. Secondary objectives include (1) identifying which nutritional, infection/illness, and psychosocial measures had sufficient variability to warrant further exploration, (2) determining whether ongoing engagement with the longitudinal cohort affected measures through comparison with paired cross-sectional cohorts, and (3) comparing these measures across pregnancy, early and later PP. The qualitative components of the larger mixed methods study and the analyses that make attributions of causality with regard to fetal and early infant growth will form the basis of subsequent publications.
Methods
Study Setting
The Mam constitute the fourth largest Mayan population in Guatemala 21 and live in the Western Highland departments of Huehuetenango, San Marcos, and Quetzaltenango. 22 The study was conducted in 8 rural Mam communities located at 2500 to 2900 m elevation and within ∼15 km of San Juan Ostuncalco (∼30-minute drive on mix of dirt and paved road) and ∼25 km of the city of Quetzaltenango (∼60-minute drive on paved road). Community populations of 1000 to 4000 have been characterized by dispersed houses and high rates of poverty (68% extreme poverty and 19% poverty). 23,24 Communities were engaged in subsistence agriculture with similar socioeconomic and infrastructural conditions. All were involved in the nationwide rural health Programa de Extensión de Cobertura. Full-time community health workers (CHWs), a nurse who visited the community health post every 7 to 14 days, and traditional midwives (comadronas) provided maternal health care.
Participatory Action Research
Participatory action research was adopted in an effort to ensure that the research was culturally sensitive, relevant, and respectful of local values. 18 An initial needs assessment allowed community women to identify their most pressing concerns regarding maternal and child health, which guided the study’s lines of inquiry. In addition, 21 Mam women, including the research coordinator, 2 traditional midwives, and 12 CHWs, participated in all aspects of the study: design, pretesting and semantic validation of study instruments, participant recruitment, administration of questionnaires, collection of biological samples, house visits and follow-up, and ongoing knowledge exchange.
Study Design
This integrated mixed methods research involved 1 longitudinal cohort, as well as 2 cross-sectional cohorts that were included to determine whether ongoing involvement with the longitudinal cohort altered outcomes. The longitudinal cohort was recruited during pregnancy and seen 3 times: 6 to 9 months of pregnancy (June 2012 to January 2013), 0 to 6 weeks PP (early PP; July 2012 to May 2013), and 4 to 6 months PP (later PP; November 2012 to October 2013; Figure 2). One of the 2 cross-sectional cohorts of mother–infant dyads was recruited early PP (June 2012 to March 2013), and the second was recruited later PP (June 2012 to September 2012). Data collection included both quantitative and qualitative methodologies. The present article describes the quantitative aspects of the research, and a description of the qualitative components will be presented separately.
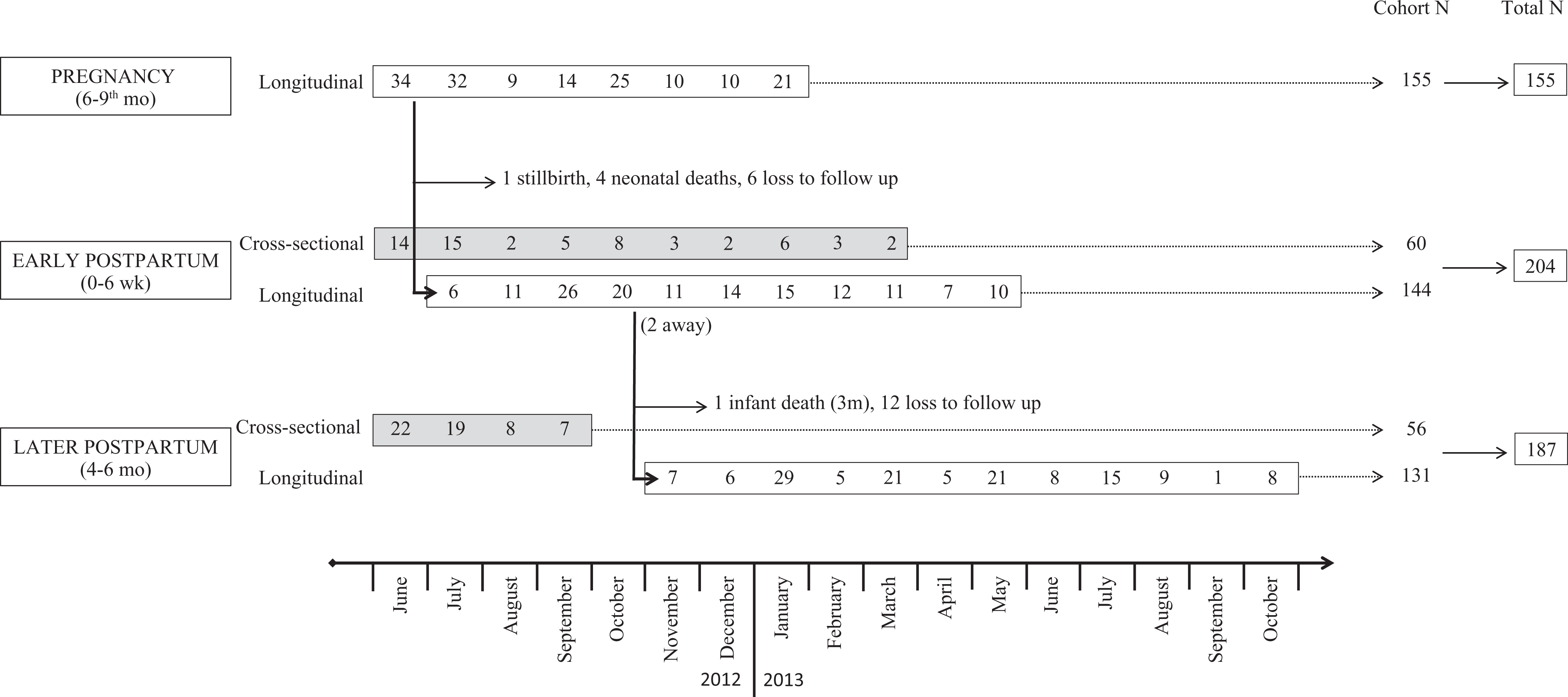
Temporal pattern of participant recruitment into the longitudinal (white) and cross-sectional (gray) cohorts, loss to follow-up, chronology of pregnancy, early and later postpartum visits, and cohort and total sample sizes.
Inclusion and Exclusion Criteria
For the longitudinal cohort, inclusion criteria were (1) consenting women from the study communities and (2) pregnancy confirmed by measurement of suprapubic fundal height ≥5 cm above the umbilicus, suggesting a gestational age ≥6 months. 25 There were no exclusion criteria, however, the participation of 6 was discontinued following notification that their infant had died. For the cross-sectional cohorts, the inclusion criteria were (1) consenting women from the study communities and (2) infants aged either 0 to 6 weeks (early PP cross-sectional cohort) or 4 to 6 months (later PP cross-sectional cohort) based on infant date of birth. The only exclusion criterion for the cross-sectional cohorts was a nonsingleton birth.
Recruitment and Ethics
Women were recruited with the assistance of the 20 community staff (CHWs and comadronas) from June 2012 to March 2013 (Figure 2) in an effort to include all women until the predetermined samples sizes were achieved. Recruitment methods included home visits, loudspeaker announcements, and word-of-mouth invitations to attend meetings at the community health post where the study was explained, questions were answered, and women were invited to provide fully informed written consent (thumbprint if unable to sign) if they wished to participate. Women who had delivered within the previous 40 days were observing a period of cuarentena; therefore, all procedures were carried out during a home visit.
The institutional review boards of both McGill University and the Center for Studies of Sensory Impairment, Aging and Metabolism in Guatemala, approved the study, and permission was obtained from community leaders and the local authorities of the Ministry of Health. Participants were referred to the public health system whenever medically indicated. Laboratory results were communicated to participants directly, and treatment was provided free of charge for any diagnosed infection.
Sample Size and Loss to Follow-Up
Power estimations for the longitudinal cohort determined that 118 participants would be necessary to detect an effect size of 0.15 for infant length-for-age (HAZ) z score, assuming inclusion of 10 independent variables within a multiple regression analysis with α = 0.05 and β = 0.2. 26 Assuming 12% loss to follow-up, we enrolled 155 participants (Figure 2), 59 in their second and 96 in their third trimester. One mother lost her infant in pregnancy (stillbirth), 4 in the neonatal period prior to the early PP visit, and 1 at 3 months PP. In addition, 18 women (11.6%) were lost to follow-up due to participant decision or relocation. Loss to follow-up was higher in the community (32%) where families more often migrated to the coast for work compared with the other communities (10%; P = .001) where migration was less frequent. The final sample sizes for the longitudinal cohort were 155 during pregnancy, 144 early PP, and 131 later PP.
Power estimations for each cross-sectional cohort determined that 46 participants would be necessary to detect a difference in infant HAZ z score of 0.5 units between the cross-sectional and the longitudinal cohorts, with α = 0.05 and β = 0.2. 26 Assuming 12% loss to follow-up, we enrolled 60 and 56 mother–infant dyads in the early and later PP cohorts, respectively.
The combined sample sizes per perinatal stage were therefore 155 women in pregnancy (all longitudinal), 204 early PP (144 longitudinal and 60 cross-sectional), and 187 later PP (131 longitudinal and 56 cross-sectional; Figure 2). Later comparison with an independent census made available to us after completion of the study revealed that of all infants born in study communities during the 10-month recruitment period, 49% had been enrolled.
Qualitative Methodologies
This component of our mixed methods research will be explored in a separate publication. Briefly, local narratives and beliefs relating to health and illness, dietary practices, and local sources of maternal stress versus resilience were explored using focus groups, key informant interviews, as well as PhotoVoice methodologies developed for use in marginalized populations. 27 PhotoVoice derives ethnographic data from participant narratives based on photographs that they take of their lives, daily activities, and beliefs and provides insights that might not emerge during traditional interviews or focus group discussions. 27
Quantitative Methodologies
At each sampling period, community staff administered a structured questionnaire in Spanish or Mam about household and social factors, obstetric and medical history, and current symptoms (20-45 minutes); staff nutritionists measured anthropometry of mothers and infants (15 minutes) and conducted a previous-day dietary recall (15 minutes); and a physician reviewed all questionnaire information, inquired about particularly sensitive information such as safety and exposure to violence within the home environment, and performed a physical examination (<30 minutes). Breast milk was collected from lactating women, and the women were given instructions for collecting stool, urine, and saliva samples (<15 minutes) that were subsequently delivered by staff to a laboratory in Quetzaltenango. A follow-up home visit was performed by community staff, nutritionists, and the physician to administer a food security questionnaire (5 minutes), a previous-day physical activity recall (15 minutes), a second previous-day dietary recall (15 minutes), and to pick up any remaining samples and deliver laboratory results and any warranted treatment (<5 minutes).
Household factors
Sociodemographic factors
Women were asked about language proficiency (Mam, Spanish), marital status (married, informal union, single, separated, or widowed), occupation, schooling (none, primary, or ≥secondary), and religion (evangelical or Roman Catholic). As no universal definition exists to define indigenous ethnicity due to its complex sociopolitical nature, 28 women were categorized as being Mam if they wore indigenous clothing and/or if they spoke Mam (99% concordance). Women were asked whether their family owned land, and if so, whether they planted maize, potato, fava or black beans, greens, and/or fruits.
House construction materials were defined by floor type (cement, ceramic tiles, or dirt), wall material (wood, cement block, adobe [earthen brick], or lamina [corrugated sheet metal]), water source (household faucet, public faucet, well, river or stream, other), and sanitation facilities (toilet, pit latrine, or neither). Women were also asked whether their family had electricity or owned any of the following durable assets: radio, television, mobile phone, sewing machine, oven, refrigerator, bicycle, car, or truck.
Measuring household income is difficult in a region such as the study area where sources of income vary daily, weekly, and seasonally, most families engage in home production and informal work, and women have little knowledge about the income of other family members. 23 Therefore, a Household Wealth Index (HWI) was constructed as a proxy for long-term wealth, according to Demographic Health Survey methods. 29 Thirteen items (dirt floor, ceramic/cement floor, adobe/lamina walls, cement block walls, electricity, and ownership of a radio, television, mobile phone, sewing machine, oven, refrigerator, bicycle, and car/truck) underwent principal components analysis (PCA). The HWI was calculated as the sum of the relative weightings of each asset and housing construction material. It was used as a continuous variable, and each household was also categorized as being in the lowest (lowest 40%), middle (middle 40%), or highest (top 20%) asset category.
Adult food insecurity
A 9-item household Adult Food Insecurity Score was adapted from the 14-item experience-based Food Security Questionnaire used by the Panama Ministry of Health. 30 The 5 items pertaining to children were excluded given that 40% of the study participants were primiparous. This questionnaire was chosen over the Latino American and Caribbean Food Security Scale based on pilot testing results that revealed poor local understanding of the subtle differences between its questions. The questionnaire asked questions about lacking money to purchase food, decreasing amount of food or frequency of meals because of lack of money, experiencing hunger, and effects of agricultural production and the environment on food production. Individual items were scored on a 4-point Likert scale (never, sometimes, almost always, and always). The cumulative Adult Food Insecurity Score ranging from 0 to 27 was categorized into food secure (0) versus mildly (1-9), moderately (10-18), and severely (19-27) food insecure.
Social factors
Structural social capital, which pertains to participation and connectedness, was assessed through the measurement of maternal autonomy, social support (general and specific to the study infant’s father), and group membership. 31 With regard to social support, 3 dimensions were assessed: emotional support (enabling people to “feel” things), instrumental support (enabling people to “do things”), and informational support (enabling people to “know” things). 31 Cognitive social capital, which pertains to reciprocity, trust, and norms, was assessed through the measurement of social trust and perception of harmony. 31
Maternal autonomy
A Maternal Autonomy Score was calculated using a 5-item questionnaire that assessed women’s involvement in household decision making about food and medicine purchases, health visits for herself or infant, and household finances. 32 For each item, 2 points were assigned if the respondent made the decision on her own and 1 if decision making was shared. The cumulative score ranging from 0 to 10 was used both as a continuous variable and as a categorical variable based on no (0), low (1-5), and moderate/high levels (6-10) of autonomy.
Social support and group membership
A Paternal Support Score was calculated using a 5-item questionnaire, 33 which inquired about support received from the baby’s father (providing financial support, spending time with her, helping her make difficult decisions, providing affection, and showing interest in caring for the newborn). Each item rated paternal support on a 3-point Likert scale from 0 to 2 (never, sometimes, and always). The resulting cumulative score ranging from 0 to 10 was used both as a continuous variable and as a categorical variable of no (<1), low (1-5), moderate (6-8), and high (9-10) levels of paternal support.
A Social Support Score was calculated using an 8-item questionnaire adapted from the Social Provisions Scale 34 and the Social Network Questionnaire. 35 Items inquired about how many people overall could the respondent count on to deliver emotional, instrumental, and informational support when needed (to provide a listening ear, help make difficult decisions, give useful advice about pregnancy and newborn care, look after family safety, ensure that mother and child received medical care, provide enough money to buy basic necessities, and help with child care). The score (the sum of the total number of people for each item divided by the number of items) was used as a continuous variable and to define categories of social support as lowest (for scores <1), average (1-2), and highest (>2). The number of individuals in network was obtained by summing the number of different individuals identified throughout the 8 items and was used as a continuous variable.
Group membership was defined as active membership in a cooperative or union, community association, women’s association, religious group, health organization, or political group. A binary variable was created for active group membership that differentiated women who did versus did not participate in any group.
Social harmony and trust
Social harmony was scored according to whether women felt that most people got along well in their community (yes, no, or more or less). A binary variable was created that differentiated “yes” from other responses.
Trust was evaluated using a 13-item questionnaire adapted from Pennock’s Wellbeing Survey 36 that inquired about a participant’s level of trust (never, sometimes, and always) in various institutions, which were later grouped according to initial PCA loading into family, neighborhood (neighbors and church), public services (community health center, hospital, police, and school), government institutions (government and mayor), nongovernment institutions (nongovernmental organization [NGO] and women’s group), and media (television and newspapers).
Experience of difficult life events
An adapted Life Experience Survey 37 inquired about experience of various stressful life events (yes/no), including experience during pregnancy or PP of various potentially stressful life events (loss, difficulties with partner or other family members, and household alcohol abuse). In addition, an open-ended discussion in a space that ensured confidentiality and safety was used to explore particularly sensitive topics such as experience of domestic violence including verbal, physical, or sexual. Any indication of a stressful life event was used to build dichotomous variables reflecting exposure to each life event.
Maternal factors
Obstetric experience
Maternal age was determined based on the mother’s date of birth or self-reported age when the date was unknown (n = 7). Age at delivery was categorized as <20 years, 20 to 34 years, and ≥35 years, reflecting the greater obstetric risks associated with either extreme of age. 38 Parity, defined as the number of live births, was categorized as 1, 2 to 4, and ≥5, reflecting the greater obstetric risks associated with primiparity and grand multiparity. 38 Loss of a previous child under 5 years was recorded and classified as stillbirth, death within the first 28 days PP, or ≥28 days PP. Mean birth spacing interval during the woman’s reproductive years was classified as <3 or ≥3 years. 38 Prenatal and delivery services were identified as either informal (if delivered by a comadrona) or formal (in public or private facility). Frequency of antenatal care (ANC) was categorized as never, 1 to 3, or ≥4 times. 39 Women were also asked whether they had taken prenatal vitamins, iron, or folic acid supplements.
Maternal nutrition
Maternal height was measured in duplicate to the nearest 0.5 cm using a wall stadiometer, shoeless and with the gaze in the Frankfort plane. Heights <145 cm were classified as stunted. 1 Weight was measured in duplicate to the nearest 100 g using a digital scale (SECA 803, Hamburg, Germany). Body mass index (BMI) was calculated in PP women as weight (kg) divided by height squared (m2) and classified as underweight (BMI < 18.5 kg/m2), normal (BMI = 18.5-24.9 kg/m2), overweight (BMI = 25.0-29.9 kg/m2), or obese (BMI ≥ 30.0 kg/m2). 40
A maternal Dietary Diversity Score was derived from a single previous-day dietary recall at each sampling period. All foods and beverages reported, with a minimum portion size of 15 g, were classified into the following 10 food groups: starchy staples, legumes (beans/peas), nuts/seeds, dairy, flesh foods, eggs, vitamin A-rich dark green leafy vegetables, other vitamin A-rich vegetables/fruits, other vegetables, and other fruits. 41 The score was calculated as the sum of all food groups consumed, and a dichotomous variable of probable micronutrient adequacy (yes/no) was created based on a cutoff score of ≥5 food groups. 41
Physical activity was assessed through a previous-day activity recall inquiring about type of activity, frequency, intensity (0-5), and duration. 42 Physical activities were grouped by indoor domestic chores (cooking, cleaning, and weaving/sewing), outdoor domestic chores (washing clothes, tending to animals, running errands, and performing heavy manual labor such as agricultural work), nondomestic work activities (store keeping), social activities (church attendance, visiting friends/family, and health visits), exercise (walking), sedentary (rest, watching television, and eating), and childcare. Means (hours/day) for each activity were calculated. Because Mam women commonly practice cuarentena, a recovery period of ∼40 days PP when a mother is expected to dedicate herself to breastfeeding and taking care of her newborn, 43 early PP estimates were only calculated for those women ≤40 days PP. Activities that involved leaving the community were noted. A subjective Physical Activity Intensity Score was calculated from all activities except sedentary activities and childcare as the sum of individual activity scores, each calculated as duration multiplied by participant-perceived intensity. Women were also asked about their utilization of a temascal, a sauna typically used in the Highlands for bathing, relaxation, and healing purposes and strongly tied to PP care within local cultural practices. 44
Maternal illness and infection
Women were asked about their experience within the last week (yes/no) of symptoms suggestive of infection (fever, headache, cough, flu-like symptoms, skin changes, vomiting, abdominal pain, diarrhea, dysuria, and vaginal discharge) and of specific nutrient deficiencies. 25 Periodontal disease was diagnosed through detection of dental cavities (caries) or inflammation of the gum (gingivitis). Reported symptoms of upper (cough, nasal congestion, and sore throat) or lower (productive cough and difficulty breathing) respiratory tracts were complemented by examination of the sinuses, oral cavity and cervical lymph nodes, and lung auscultation (decreased breath sounds, rales, and crepitus). Reported gastrointestinal symptoms were evaluated by physical examination for abdominal distension or tenderness, hepatosplenomegaly, and quality of bowel sounds. Skin lesions typical of scabies (small papulovesicular lesions), cellulitis (warmth, erythema, and swelling), and abscesses were recorded. Clinical findings associated with specific nutrient deficits were assessed, including nail spooning and nail/conjunctival pallor (iron-deficiency anemia) and goiter (iodine deficiency).
Urine samples were collected from women at all sampling periods, except later PP for asymptomatic, longitudinal women. An experienced laboratory technician analyzed the samples using dipstick analysis and urine microscopy to yield pyuria, defined as >5 neutrophils per high-power field (HPF) of unspun urine. 45 A culture was performed if infection was suspected on initial testing (positive leukocyte esterase and nitrites by dipstick, pyuria). 45 In pregnant women, asymptomatic bacteriuria ≥105 colony-forming units/mL was considered pathological, whereas only symptomatic bacteriuria was considered pathological in nonpregnant women. 45
Stool samples were analyzed for leukocytes, nematodes, and protozoa using a direct smear by an experienced laboratory technician trained in parasitology. The direct smear methodology was validated for detection of nematodes via Kato-Katz on 30 specimens, with a finding of 100% concordance (data not shown). Both pathogenic (Giardia spp, Entamoeba histolytica, and Entamoeba dispar) and nonpathogenic (Blastocystis hominis, Entamoeba coli, Endolimax nana, and Iodamoeba butschlii) protozoa were recorded, with the latter being used as a measure of exposure to potentially contaminated food and water sources. Of note, B. hominis is generally considered nonpathogenic, but there is growing evidence that it may be an emerging pathogen. 46 Fecal leukocyte counts >10/HPF were considered indicative of an inflammatory process. 47
Saliva samples were collected from mothers at each perinatal stage to assess diurnal cortisol as an indicator of stress. Breast milk samples were also collected at both early and later PP sampling periods to measure cortisol and to detect subclinical mastitis. Details regarding collection and analyses will be reported separately.
Local idioms of distress
The lack of culturally appropriate mental health assessment tools is a barrier to screening and evaluating of emotional distress in diverse populations. Women were asked about current experience of local idioms of distress that have been described previously in this population and that were mentioned during the pilot study. 15,48,49 Susto is believed to result from a frightening or startling experience, ranging from an accidental fall or physical trauma to witnessing an accident or human suffering, which, sometimes only after a significant time lapse, affects the normal equilibrium of the human body and manifests as a diverse array of symptoms and pathologies. 48 Enojo is described as an anger that upsets the body’s equilibrium and leads to headaches, stomach pains, weakness or fatigue, and chronic illness. 48 Nervios is an illness due to experiencing strong emotions, particularly anxiety, grief, and sorrow (pena). 48
Infant factors
Infant characteristics
Infant age and sex were recorded. For women in the longitudinal cohort that recalled the date of their last menstrual period (LMP; n = 82; 56%), gestational age was calculated, in weeks, as the difference between the LMP and birth, and infants were classified as premature if born <37 weeks. 50 Mother-reported infant birth weight was classified as LBW if <2.5 kg. 51
Infant anthropometry and feeding practices
Recumbent supine length (cm) was measured thrice according to standardized procedures using an infantometer (SECA 210) and recorded to the nearest 0.5 cm, and the final value was the mean. Weight (kg) was measured to the nearest 100 g using a digital infant scale (SECA 354). Head circumference (cm) was measured thrice using a head circumference baby band (SECA 212). Length-for-age, weight-for-age (WAZ), height-for-weight, and head-circumference-for-age (HCZ) z scores were calculated as indicators of infant nutritional status using WHO Anthro software (3.1). 52 Stunting, underweight, wasting, and microcephaly were defined as z scores <−2.0 standard deviation (SD) below the respective WHO reference median. Scores <−3.0 SD were considered severe.
Infant feeding practices were classified as exclusive breastfeeding (breast milk and certain medications), predominant breastfeeding (breast milk plus certain liquids and medications), and mixed feeding (breast milk and any solid or semisolid foods) based on the reported feeding practices since birth. 53 Timing of initiation of breastfeeding was also determined.
Infant mortality and morbidity
Neonatal mortality was calculated as the number of deaths of longitudinal infants during the first 28 days PP, divided by the number of live births for which the birth outcome was known (n = 149), multiplied by 1000.
Mothers were asked whether their infant had experienced any of the local idioms of distress during the last week or at any time since birth. According to local beliefs, susto in newborns is usually transferred from the mother during pregnancy or via breastfeeding and manifests as poor appetite, discoloration, irritability, and fatigue. 14,48 Mollera caída presents as a sunken fontanel and is attributed to sudden movement or cold air, especially if the infant’s head is uncovered. 14,48 Empujo is an illness of newborns that manifests as straining, irritability, and distended stomach. Mal de ojo in vulnerable infants is most often related to a loss of the body’s normal hot–cold equilibrium due to experiencing a “hot” condition, such as a penetrating gaze or contact with pregnant or menstruating women, drunken individuals, or persons who have been out in the sun, and it results in fever, crying, irritability, poor sleep and appetite, stomach pains, diarrhea, and cold extremities. 14,48 These local idioms of distress are considered general indicators of poor infant health.
Mothers were asked whether their infant had experienced (yes/no) symptoms of infection or compromised feeding, including fever, cough, flu-like illness, vomiting, diarrhea, stomach discomfort, or gas within the last week. A physical examination conducted by a physician assessed for any congenital abnormalities or complications of delivery and diagnosed infection and poor feeding. 25 Dehydration was assessed (skin turgor and sunken fontanelle). Cough and reported symptoms of upper (nasal congestion) or lower (difficulty breathing) respiratory tracts were complemented by observation (use of accessory muscles of breathing), examination of the sinuses, oral cavity and cervical lymph nodes, and lung auscultation. Report of gastrointestinal symptoms was followed by evaluation for abdominal distension or tenderness and quality of bowel sounds. Among skin infections, lesions typical of scabies, cellulitis, and diaper dermatitis (erythema of genital area) were recorded. The umbilical area was assessed for adequate healing and for any signs of infection (erythema, swelling, and drainage).
Stool samples collected later PP were analyzed for leukocytes, nematodes, and protozoa using a direct smear by an experienced laboratory technician. Protozoa were recorded as described previously.
Statistical Analyses
All statistical analyses were carried out using IBM SPSS Statistics Program version 22.0 (SPSS Inc/IBM Chicago, Illinois). Descriptive statistics (mean ± SD, percentages ± 95% binomial confidence interval) were computed, and coefficients of variation (CVs) were computed for continuous variables.
Internal consistency of questionnaire items was assessed using Cronbach α test for adult food insecurity, maternal autonomy, paternal support, and social support and classified as excellent (α ≥ 0.9), good (0.9 > α ≥ 0.8), acceptable (0.8 > α ≥ 0.7), questionable (0.7 > α ≥ 0.6), or poor (0.6 > α ≥ 0.5). 54 If α ≥ 0.8, PCA was then used to assess whether questionnaire items measured multiple dimensions (construct validity) and whether the items could be grouped into dimension-specific variables.
Longitudinal and cross-sectional cohorts were compared using χ2 or Fisher exact tests for categorical variables, Student’s t tests or analysis of variance (ANOVA) for normally distributed continuous variables, and Wilcoxon Mann-Whitney U test or Kruskal-Wallis test for nonnormally distributed continuous variables. Within the longitudinal cohort, comparisons across sampling periods were done by repeated-measures ANOVA or related samples Friedman 2-way ANOVA by ranks for continuous variables and related samples Cochran Q test for categorical variables. The level of significance was set at P < .05. In order to assess which factors had sufficient variability to warrant future exploration of their associations with the health of the mother–infant dyad, we considered that continuous variables with a CV > 15% are likely to have sufficient variability to be informative in future analyses.
Results and Discussion
Household Factors
Sociodemographic factors
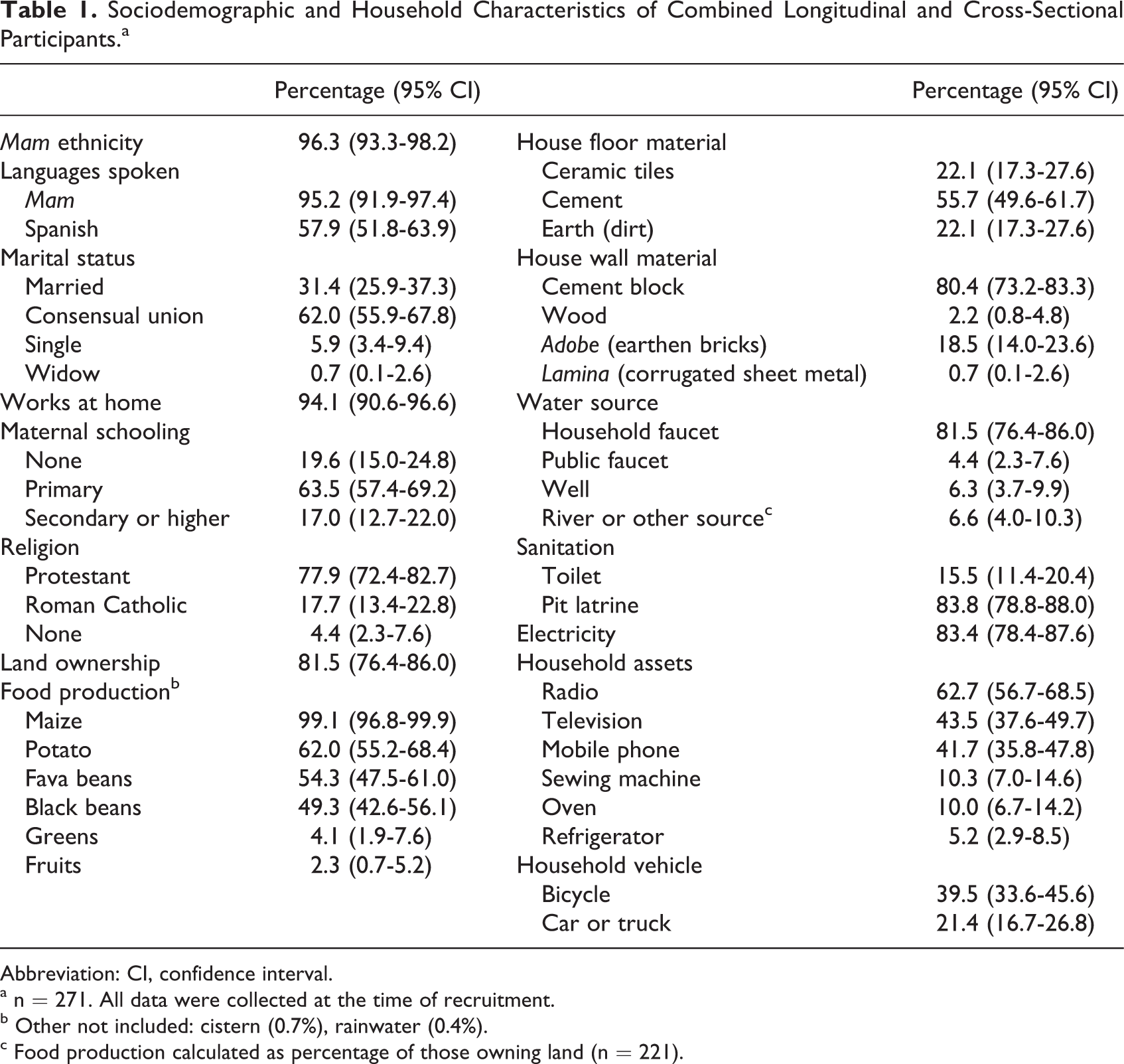
Based on study inclusion criteria, all participants lived in rural communities and the majority (96%) was Mam indigenous (Table 1). Most women (94%) self-identified as housewives, and only 7 reported employment outside the home (Table 1). Fewer (6%) participants were single compared to women of reproductive age nationally (31%), and only one-third of women in a relationship were married compared to two-thirds nationally. 19 Marital status is highly relevant to gender relations, and without legal protection in the case of separation, consensual unions in rural Latin America are typified by lower bargaining power of women and as advantageous to men. 55 Although the percentage of study participants who had never attended school was similar to the national percentage, both at ∼20% (Table 1), the percentage of secondary schooling among study participants (17%) was half the national level (34%). 19
Sociodemographic and Household Characteristics of Combined Longitudinal and Cross-Sectional Participants.a
Abbreviation: CI, confidence interval.
a n = 271. All data were collected at the time of recruitment.
b Other not included: cistern (0.7%), rainwater (0.4%).
c Food production calculated as percentage of those owning land (n = 221).
Almost all women (99%) lived in households that practiced subsistence agriculture and cultivated maize, and the majority also cultivated potatoes and legumes (black and broad beans; Table 1), as is characteristic in this area of Guatemala. 22,23 The first principal component of the HWI explained 29% of variance. All women in the highest HWI category (top 20%) lived in houses made of blocks with cement or ceramic floors, whereas 47% of those in the lowest HWI category (lowest 40%) lived in adobe houses and 54% had dirt floors. Although electricity was available to 73% of the poorest households (compared to 96% in the highest HWI category), few of the poorer households had radios (39%), televisions (13%), stoves (3%), refrigerators (2%), or cars or trucks (4%), compared to the households in the highest asset category (96%, 29%, 95%, 18%, and 61%, respectively). Compared to other rural populations, in Guatemala, access to piped water, sanitation, electricity, housing material, and ownership of a motor vehicle was overall better, and conversely, ownership of other household assets (radio, television, mobile phone, and refrigerator) was lower. 19
Adult food insecurity
Internal consistency between items in the Adult Food Insecurity Questionnaire was good both during pregnancy and early PP (Cronbach α = 0.85) and later PP (α = 0.89), consistent with prior use of this questionnaire in Panama (Krause RJ (PhD), personal communication, 2012). The first, second, and third principal components measured reduced food access, experience of hunger, and environmental causes, respectively. The 2 former components are common dimensions assessed in food security questionnaires. 56 However, that environmental causes emerged as a latent component—a finding highly relevant to subsistence farming contexts, where difficulty in growing food due to inclement weather and lack of primary resources such as seeds and land both have a significant impact on a household’s economy and access to food—is novel and worthy of particular attention, as most food security questionnaires do not assess this dimension. 57,58 Considerable variability in the Adult Food Insecurity Score existed between households (CV > 100%). Approximately two-thirds (62%) experienced some degree of food insecurity in the previous month (Table 2), which closely paralleled findings from the National Maternal-Infant Health Survey 2008 to 2009 pertaining to the Western Highlands 57 where 64% of all households had experienced adult food insecurity, compared to 57% nationally, with most affected households being poor, rural, and indigenous. 57 However, our rates of severe adult food insecurity were lower (<5%) compared to 18% reported for this area of Guatemala, 57 perhaps because of differences in the questionnaires utilized. Previous findings in this area of Guatemala 57 suggested that severity of household food security increases with inclusion of child food security questions, a dimension we were not able to measure given the high rate of primiparity in our study population.
Adult Food Insecurity and Social Factors by Sampling Period.a,b,c
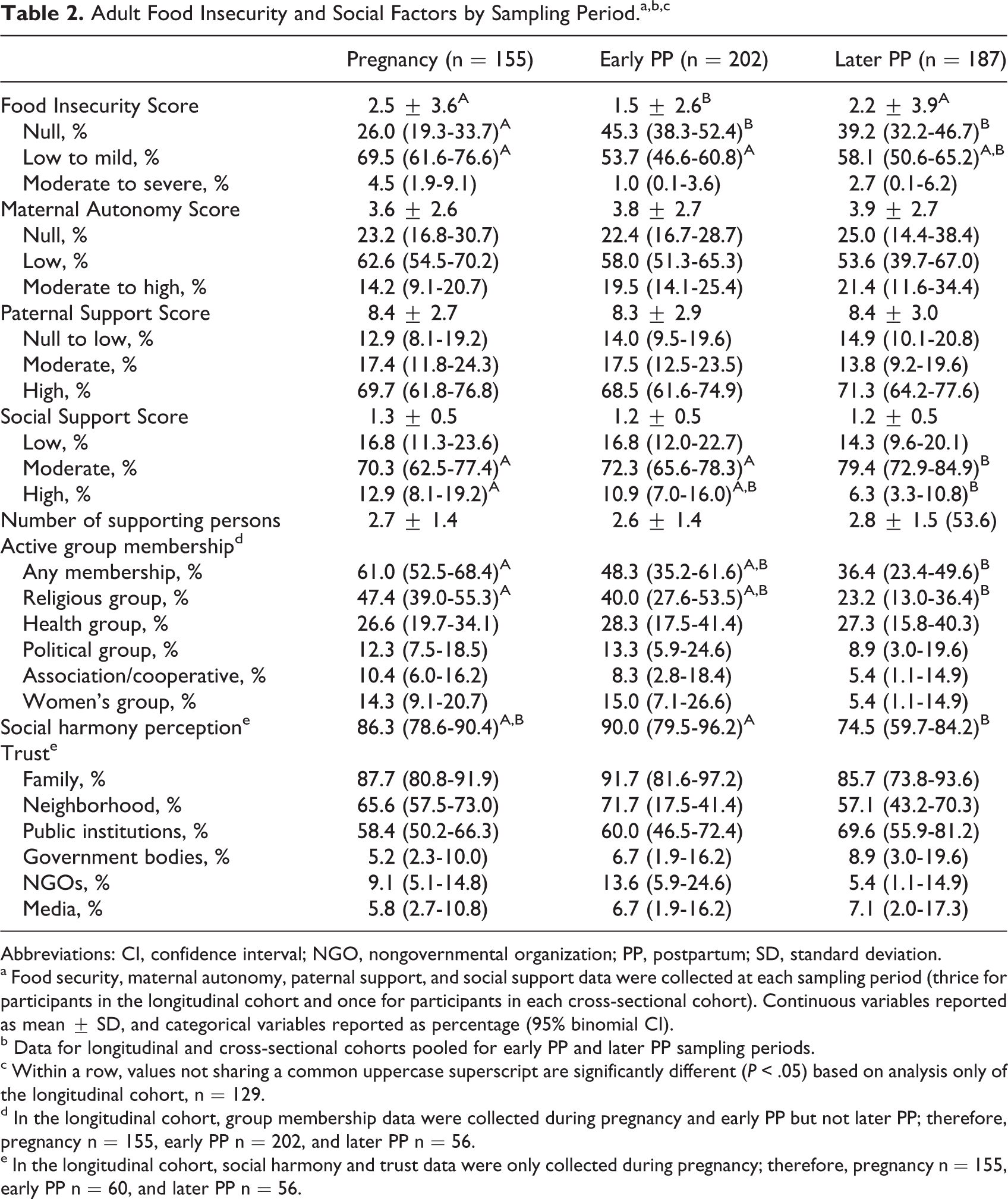
Abbreviations: CI, confidence interval; NGO, nongovernmental organization; PP, postpartum; SD, standard deviation.
a Food security, maternal autonomy, paternal support, and social support data were collected at each sampling period (thrice for participants in the longitudinal cohort and once for participants in each cross-sectional cohort). Continuous variables reported as mean ± SD, and categorical variables reported as percentage (95% binomial CI).
b Data for longitudinal and cross-sectional cohorts pooled for early PP and later PP sampling periods.
c Within a row, values not sharing a common uppercase superscript are significantly different (P < .05) based on analysis only of the longitudinal cohort, n = 129.
d In the longitudinal cohort, group membership data were collected during pregnancy and early PP but not later PP; therefore, pregnancy n = 155, early PP n = 202, and later PP n = 56.
e In the longitudinal cohort, social harmony and trust data were only collected during pregnancy; therefore, pregnancy n = 155, early PP n = 60, and later PP n = 56.
Social Factors
Social capital
Maternal autonomy
Internal consistency between items in the Maternal Autonomy Score was excellent (Cronbach α > 0.90), and there was considerable variability among households (CV > 65%). Most women reported no (24%) or low (58%) autonomy, whereas only 19% reported moderate to high autonomy (Table 2). Women reported the lowest autonomy in the management of household money and the highest autonomy in decisions relating to food purchases. These findings are consistent with prior research in Guatemala, including indigenous populations where 38% of women of reproductive age have no say in household decision making, 73% need their partner’s authorization to visit a doctor, and 69% to make any household expenditures. 19 Greater female involvement in decision making has been associated in indigenous areas of Guatemala with higher maternal schooling and earnings, Spanish proficiency, and women’s ability to make strategic life choices 59,60 and nationally with reduced frequency of domestic violence. 19
Social support and group membership
Internal consistency between items of the Paternal Support Score was excellent (Cronbach α = 0.93 in pregnancy and early PP and 0.96 later PP). The score had moderate variability (CV > 30%). Most women (70%) reported high levels of support from the infant’s father, but 14% reported no or low paternal support (Table 2). Among the types of paternal support, emotional support (affection) was the most commonly reported (84%), whereas helping to care for the infant was the least commonly reported (76%). These findings are consistent with prior reports in Guatemala, 19,55,59 where men are typically highly involved in household decision making including decisions related to maternal and child health.
Internal consistency between items of the Social Support Score was good (Cronbach α = 0.84 in pregnancy, 0.91 early PP, and 0.85 later PP). The resulting score had moderate variability (CV > 35%). Most women (74%) reported moderate levels of social support, whereas 16% reported low levels (Table 2). Emotional and informational forms of support (both 96%) and support at home to have time to rest (84%) or to secure the family’s safety (89%) were the most common. Women relied on a small social network (2.7 individuals; Table 2) that most often included the mother and partner/spouse, followed by father, father-in-law, children, stepsiblings, and health care providers. It has been suggested that the small size of such networks may increase women’s vulnerability to potential shocks such as illness or death of a main support person, especially in areas, such as our study area, that face extreme poverty and have little access to social safety nets. 61
Active group membership was reported by 48% of women, most commonly in religious (36%) and health (28%) groups (Table 2). These likely are an important source of knowledge exchange and social support for women.
Social harmony and trust
Because internal consistency of the Trust Questionnaire was poor to questionable (Cronbach α = 0.50-0.67), no composite Trust Score was developed. Instead, we present responses to individual questions. Early PP, more women (90%) reported social harmony in their communities compared to later PP (75%). Most (88%) women reported a high level of trust in their families but only 65% in their neighborhoods, 61% in public institutions, 9% in NGOs, and 6% in government services or the media (Table 2). That few women trusted institutions outside their community likely reflects local norms and beliefs, as well as experience with racism and discrimination. 62 Low levels of trust in turn likely translate into reluctance in seeking help, 63,64 further increasing the vulnerability of the population.
Experience of difficult life events
Domestic violence, household alcohol abuse, and problems with the newborn’s father were the most commonly reported difficult life events, affecting 22%, 32%, and 18% of longitudinal women, respectively. These values were comparable to national statistics of intimate partner violence within the last 12 months among indigenous women (20%) and in the overall population (23%). 19 Although our study did not explore contributing factors, national statistics 19 suggest that regardless of location of residence or ethnicity, domestic violence is most likely to occur when the perpetrator is drunk (30%) or jealous (25%) or when the victim disobeys him (16%), complains (16%) or refuses to engage in sexual activity (14%), and most often results in depression and sadness (78%), fear (67%), headache and body pains (63%), anxiety (51%), and loss of interest in living (51%). All could have consequences for maternal and child health. 65
Maternal Factors
Obstetric experience
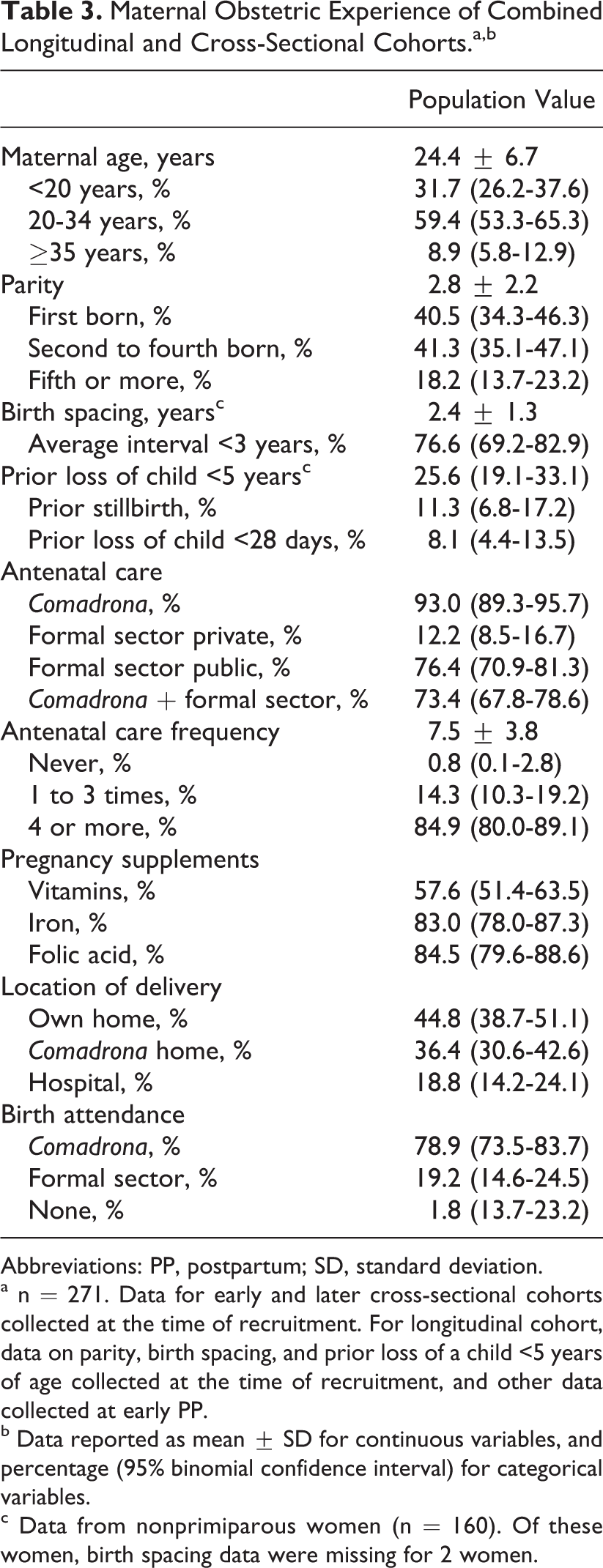
The majority of pregnancies were high risk based on maternal age (<20 and ≥35 years), parity (primiparous and grand multiparous), and/or birth spacing interval (<3 years; Table 3). Mean age at delivery for primiparous women was 19.5 years. Among the 4 women ≥40 years, parity ranged from 8 to 11; nationally, mean parity for women ≥40 years was 5.2. 19 Prior neonatal and child mortality among nonprimiparous participants was 8% and 26%, respectively, and both were higher than the 2% and 5%, respectively, reported nationally for the previous 10 years (2% and 6%, respectively, for indigenous women). 19
Maternal Obstetric Experience of Combined Longitudinal and Cross-Sectional Cohorts.a,b
Abbreviations: PP, postpartum; SD, standard deviation.
a n = 271. Data for early and later cross-sectional cohorts collected at the time of recruitment. For longitudinal cohort, data on parity, birth spacing, and prior loss of a child <5 years of age collected at the time of recruitment, and other data collected at early PP.
b Data reported as mean ± SD for continuous variables, and percentage (95% binomial confidence interval) for categorical variables.
c Data from nonprimiparous women (n = 160). Of these women, birth spacing data were missing for 2 women.
Regarding ANC, women attended a mean of 7.5 ANC visits, only 15% attended less than the WHO-recommended 4 visits, and some women were seen up to 20 times (Table 3). Most women (93%) consulted comadronas, compared to only 31% of indigenous women nationwide. 19 On the other hand, a similar percentage of study participants received ANC from the formal sector (78%) compared with indigenous women overall in Guatemala (74%). Of these, 86% used public services, most often the community health post. Most deliveries occurred either in the woman’s home or in the comadrona’s home, and 79% were attended by a comadrona. Only one-fifth (19%) of the women delivered in a hospital compared with 51.2% nationally and 36.0% for indigenous women in Guatemala. 19 The lower percentage of hospital deliveries may be due to the poor access to formal obstetric health services, high social cohesion, trust within communities and in local cultural norms and traditional Mam practices, and/or low trust in government services by participants. Indeed, previous ethnographic studies have cited various sociocultural factors that explain low utilization of formal health services by indigenous women in Guatemala, 66 including lack of confidence in biomedical treatments, perception of poor quality of care, discriminating or condescending treatment by medical personnel, inability of medical staff to speak indigenous languages, embarrassment over being examined, and greater confidence in comadronas. Moreover, relations between formal and traditional providers are often tense due to social, ethnic, and cultural differences and a strong history of devaluation of indigenous knowledge and practices. 67
Nutrition
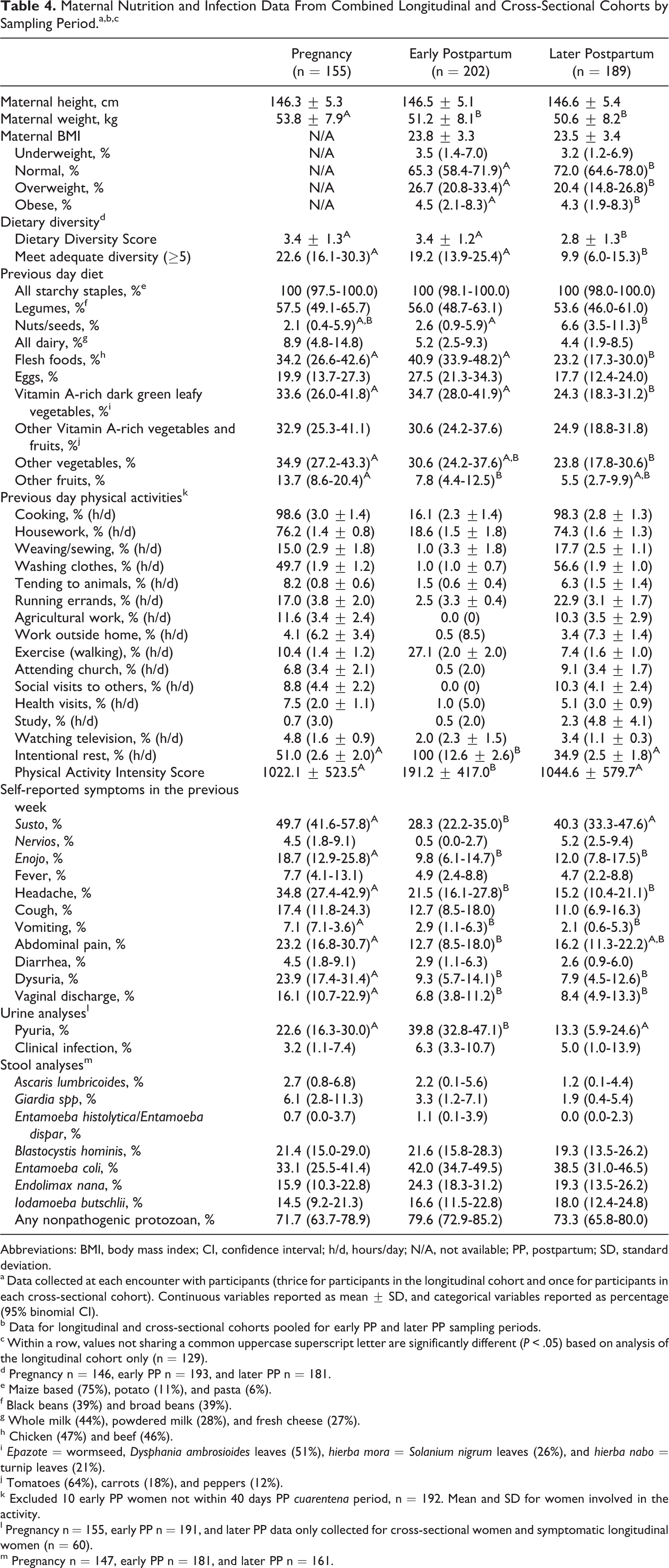
Mean maternal height was 146.5 ± 5.2 cm (132.0-162.0 cm; CV: 4%; Table 4), and 33% of women were stunted as compared to 31% overall in Guatemala and 48% in indigenous populations. 19 Based on early and later PP measurements, less than 4% of mothers were underweight, two-thirds had a normal BMI, and one-fourth was overweight (20%) or obese (4%). These findings contrast with national statistics 19 where only 2% of women of reproductive age are underweight, 35% are overweight, and 15% are obese. No difference in BMI was detected between early and later PP visits, consistent with findings in urban Quetzaltenango where maternal BMI did not change between early PP and 2 years PP. 68
Maternal Nutrition and Infection Data From Combined Longitudinal and Cross-Sectional Cohorts by Sampling Period.a,b, c
Abbreviations: BMI, body mass index; CI, confidence interval; h/d, hours/day; N/A, not available; PP, postpartum; SD, standard deviation.
a Data collected at each encounter with participants (thrice for participants in the longitudinal cohort and once for participants in each cross-sectional cohort). Continuous variables reported as mean ± SD, and categorical variables reported as percentage (95% binomial CI).
b Data for longitudinal and cross-sectional cohorts pooled for early PP and later PP sampling periods.
c Within a row, values not sharing a common uppercase superscript letter are significantly different (P < .05) based on analysis of the longitudinal cohort only (n = 129).
d Pregnancy n = 146, early PP n = 193, and later PP n = 181.
e Maize based (75%), potato (11%), and pasta (6%).
f Black beans (39%) and broad beans (39%).
g Whole milk (44%), powdered milk (28%), and fresh cheese (27%).
h Chicken (47%) and beef (46%).
i Epazote = wormseed, Dysphania ambrosioides leaves (51%), hierba mora = Solanium nigrum leaves (26%), and hierba nabo = turnip leaves (21%).
j Tomatoes (64%), carrots (18%), and peppers (12%).
k Excluded 10 early PP women not within 40 days PP cuarentena period, n = 192. Mean and SD for women involved in the activity.
l Pregnancy n = 155, early PP n = 191, and later PP data only collected for cross-sectional women and symptomatic longitudinal women (n = 60).
m Pregnancy n = 147, early PP n = 181, and later PP n = 161.
Dietary Diversity Scores were 3.4, 3.4, and 2.8 in pregnancy, early PP, and later PP, respectively (Table 4). All women consumed starchy staples (mostly maize), and over half consumed legumes (most commonly black and broad beans) the previous day (Table 4). One-third consumed flesh foods (mostly chicken or beef), dark green leafy vegetables (such as epazote, hierba mora, and hierba nabo), other vegetables (such as onions and güisquil), and vitamin A-rich vegetables and fruits (mostly tomatoes and carrots). One-fifth consumed eggs. Consumption of other fruits, dairy, and nuts/seeds was particularly low. Consumption of flesh foods, vegetables, and fruits was higher during pregnancy and early PP compared to later PP (P < .05), whereas consumption of nuts/seeds was lower (P = .039). These findings are consistent with prior dietary diversity research in Guatemala. 69 Women appeared to make an effort to increase the diversity of their diets during pregnancy and early PP. However, given that only one-fifth of pregnant and early PP women and one-tenth of later PP women consumed foods from at least 5 food groups on the previous day (Table 4), close to 80% of women did not meet adequate diet diversity and therefore were at risk of inadequate micronutrient intake. 41
With regard to physical activity, other than childcare, the most common activities reported during pregnancy and later PP were domestic chores, social activities, and resting (Table 4). Early PP, during the cuarentena, the most common activities were rest and childcare. Pregnant and later PP women were more likely to leave the community than early PP women (11% vs 2%), most commonly to run errands or sell produce in nearby San Juan Ostuncalco, and to have a higher Physical Activity Intensity Score (P < .001). In addition, most women in all sampling periods reported routinely using the temascal, which also provided time for rest.
Illness and infection
Maternal experience of biomedical symptoms within the previous week was greatest for headache, cough, abdominal pain, dysuria, and vaginal discharge, most of which were more frequent during pregnancy than PP (P < .05; Table 4). Most women had periodontal disease in the forms of caries (78%) and/or gingivitis (66%). In addition, premature loss of permanent teeth, a useful composite marker of adverse social and economic conditions, malnutrition, and lack of health care services, 70 affected nearly two-thirds (59%) of women, with 22% missing ≥5 teeth. Epigastric tenderness and signs of anemia were uncommon (8% and 5%, respectively), and hypertension, pneumonia, and clinical mastitis were present in <1%.
Laboratory-diagnosed urinary or gastrointestinal infection was rare (Table 4). Despite a high prevalence (∼75%) of nonpathogenic protozoans, a potential indicator of an unsanitary environment, women exhibited a very low prevalence of helminth (Ascaris lumbricoides) or other parasitic infection (Giardia spp, E. histolytica/E. dispar) compared to school-aged children in a nearby, similar altitude rural area (Palajunoj Valley) where prevalence were A. lumbricoides 18%, E. histolytica/E. dispar 16%, Giardia lamblia 11%, Hymenolepis nana 5%, and B. hominis 3%. 71 Others have similarly found significant differences in infection prevalence between neighboring rural communities through spatial clustering analyses. 72 However, the low prevalence of helminth infection in study women could be due to the particular ecology of our study area including altitude, soil type, precipitation, or temperature, all of which are known to influence transmission dynamics, 73 or the lower sensitivity of direct smears compared with Kato-Katz for detecting nematode eggs. 74
Local idioms of distress
Both susto and enojo were more commonly reported during pregnancy and later PP compared with early PP (P < .05; Table 4). Few (<5%) women reported experiencing nervios. This study will allow inquiry as to the impact of maternal experience of local idioms of distress on the maternal–infant dyad, which may be best complemented by our qualitative data.
Infant Factors
Infant characteristics
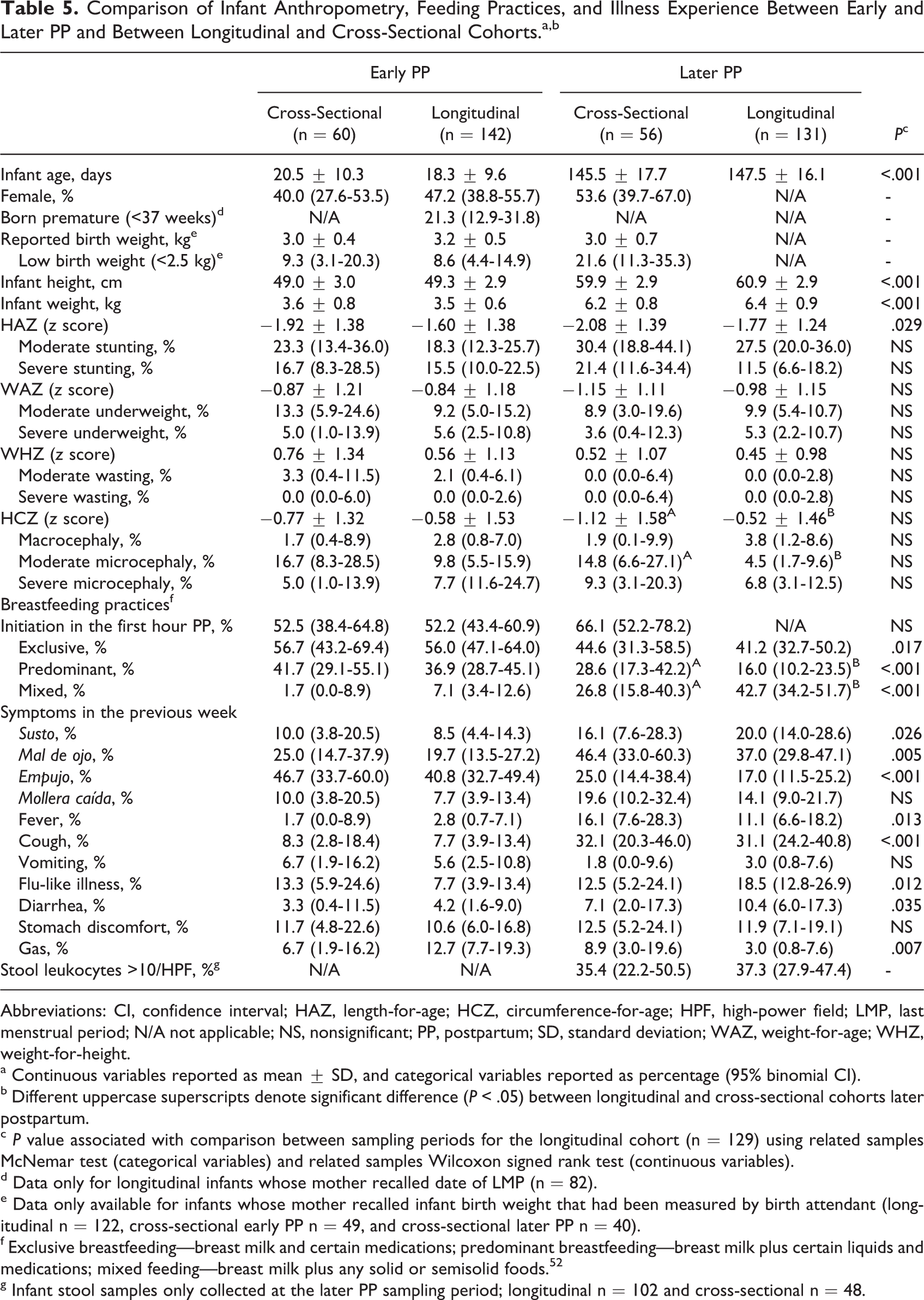
Mean infant ages were 19 days (early PP) and 147 days (later PP), and 47% of infants were female (Table 5). Among the 82 longitudinal infants for whom we knew maternal LMP, one-fifth was premature, with mean gestational age of 34.5 weeks. This contrasted with the national rate of 8%, 9% in Latin America and 11% worldwide, and with Malawi, which has the highest rate in the world at 18% 50 and begs for skepticism in the accuracy of the self-reported LMP. According to mother’s recall of infant birth weight, 9% of all early PP infants had LBW, compared to an overall rate of LBW in Guatemala of 11% and in rural populations of 12%. 19 These findings contrast with observations that in developing countries, the ratio of intrauterine growth retardation to prematurity favors the former. 75
Comparison of Infant Anthropometry, Feeding Practices, and Illness Experience Between Early and Later PP and Between Longitudinal and Cross-Sectional Cohorts.a, b
Abbreviations: CI, confidence interval; HAZ, length-for-age; HCZ, circumference-for-age; HPF, high-power field; LMP, last menstrual period; N/A not applicable; NS, nonsignificant; PP, postpartum; SD, standard deviation; WAZ, weight-for-age; WHZ, weight-for-height.
a Continuous variables reported as mean ± SD, and categorical variables reported as percentage (95% binomial CI).
b Different uppercase superscripts denote significant difference (P < .05) between longitudinal and cross-sectional cohorts later postpartum.
c P value associated with comparison between sampling periods for the longitudinal cohort (n = 129) using related samples McNemar test (categorical variables) and related samples Wilcoxon signed rank test (continuous variables).
d Data only for longitudinal infants whose mother recalled date of LMP (n = 82).
e Data only available for infants whose mother recalled infant birth weight that had been measured by birth attendant (longitudinal n = 122, cross-sectional early PP n = 49, and cross-sectional later PP n = 40).
f Exclusive breastfeeding—breast milk and certain medications; predominant breastfeeding—breast milk plus certain liquids and medications; mixed feeding—breast milk plus any solid or semisolid foods. 52
g Infant stool samples only collected at the later PP sampling period; longitudinal n = 102 and cross-sectional n = 48.
Nutrition
With regard to infant anthropometry, CVs for all scores exceeded 70%, indicating considerable variation in our study population (Table 5). Over one-third (36%) of infants was already stunted early PP. No national data are available for comparison, but studies in urban Quetzaltenango 20 and rural Chimaltenango 76 revealed lower early PP stunting rates, at 25% and 16%, respectively. In our study, infant HAZ further declined between early and later PP visits (P = .029) to reach stunting of 43% at the later visit, compared to 56% in rural Chimaltenango 76 and 24% in Guatemalan infants 3 to 5 months old. 19
The percentage of underweight and wasted infants was 16% and 3% during early PP and 14% and 0% during later PP, respectively (Table 5), compared to national rates of 5 and 1%, respectively, in 3- to 5-month-old infants. 19 Microcephaly affected 19% of infants during early PP and 15% during later PP. This was unexpected given the paucity of prior national or international data on microcephaly and the results of a cohort study in rural Chimaltenango 76 in which low infant HCZ was not encountered.
With regard to infant feeding practices, just over half (55%) of the study infants initiated breastfeeding within the first hour PP (Table 5), which, according to prior work by our group, 77 was associated with delivery at the comadrona’s home, mother-perceived sufficient breast milk, later exclusive breastfeeding, and higher WAZ. Within the first week PP, 26% had received ritual fluids or agüitas (19% prior to initiation of breastfeeding), most frequently as warm water (for perceived insufficient milk), and infusions of anise or orange leaves (for stomach discomfort) and chamomile (for irritability and crying). Rates of exclusive versus mixed feeding were 56% and 5% during early PP and 42% and 8% during later PP, respectively, with exclusive breastfeeding rates being comparable to those overall in Guatemala (56% at 0-3 months and 43% at 3-5 months). 19 Of mixed-fed infants, 10% had initiated mixed feeding at 2 months, 25% at 3 months, and 65% at 4 months.
Mortality and morbidity
The neonatal mortality rate was high within our study population, at 27 per 1000 live births, compared to 18 overall in Guatemala and 21 within its indigenous population 19 and 9 in Latin America and the Caribbean. 78
The majority of mothers reported that their infant was affected by at least 1 local idiom of distress. At the early PP visit, the most common infant ailments were, by decreasing frequency, empujo, mal de ojo, gas, and stomach discomfort, and at the later PP visit, mal de ojo, cough, empujo, and mollera caída (Table 5). The concurrent influences of local cultural practices and western influences were evident in our observations. Highlighting the poor local uptake of western concepts, women reported local idioms of distress more frequently than they did symptoms representing a biomedical understanding of health and illness. This is consistent with prior findings among rural Mam mothers 79 that explanation of illness is most often based on local concepts of health and illness, namely an imbalance of the body’s equilibrium due to climate, behavior, or emotional states.
Infant physical examinations were for the most part normal. Most common findings (all <10%) included umbilical erythema, perineal rash, and upper respiratory infection, for which most treatments were sought from traditional healers and consisted of herbal preparations. Less than 1% had a congenital abnormality (suspected Hirschsprung disease), cellulitis, or pneumonia. Stool samples were returned for 80% of later PP infants, and one-third had fecal leukocytosis, indicative of intestinal inflammation and most likely due to bacterial infection and/or environmental enteropathy, which is common in developing countries and can develop as early as 2 to 12 weeks after birth due to chronic exposure to fecal contamination. 80
Comparison of Longitudinal and Cross-Sectional Arms of the Study
A methodological challenge of longitudinal studies, and especially of those that actively incorporate PAR, is that the presence of the research team may affect study outcomes either directly (through, for example, treatment of medical conditions) or indirectly (for example, through behaviour change in response to exposure to new information and people). 18 The main reason to include both longitudinal and cross-sectional cohorts in our study design was to confirm that ongoing engagement with study participants through frequent follow-up with women had no impact on the measured variables. Analyses revealed only 4 differences between paired longitudinal and cross-sectional cohorts. First, longitudinal women were significantly more likely to have reported experiencing difficult life events than their cross-sectional counterparts (P < .05), most likely due to new incidents between the early PP and late PP visits, increased trust by participants of the research team, and repeated opportunity to report violence. Second, at the early PP visit, cross-sectional women spent less time resting than did longitudinal women (P = .004). Third, at the later PP visit, cross-sectional women had a lower Dietary Diversity Score (P < .02) and consumed legumes, vitamin A-rich leafy green vegetables, and other vegetables less frequently than did longitudinal women (P < .05), which could potentially be due to temporal differences in when the later PP dietary information was collected from the 2 cohorts. Finally, later PP, moderate microcephaly was more common in the cross-sectional than the longitudinal cohort (P = .027), but analyses revealed no differences between longitudinal and cross-sectional cohorts in linear growth or weight of infants, either early or later PP.
Strengths and Limitations
Our study design has several strengths. Continued engagement with communities, close collaboration with CHWs and comadronas, and delivery of laboratory results and treatments engendered confidence between participants and the research team. Furthermore, we chose only to collect biological samples considered by the women to be noninvasive (urine, stool, breast milk, and saliva). Together, these elements minimized loss to follow-up. Skilled interviewers and privacy during the interviews enabled disclosure of violence. Finally, we have a diverse database covering household characteristics, social context, experience of difficult life events, obstetric history, maternal nutrition, infection and psychosocial distress, and infant nutrition and infection. This will allow for a comprehensive exploration of determinants of the health of the maternal–infant dyad in this setting.
We however acknowledge 6 limitations. First, sampling bias may have occurred as only half of potentially eligible women living in study communities presented for enrollment, as assessed by later review of a census. It is likely that our recruitment methods did not reach all women and that some women could not present themselves on the specific clinic days, but we acknowledge the possibility that nonparticipants might constitute a distinct population (ie, working mothers, women facing particularly harsh living conditions, women not given permission by a partner or parent to participate, and women who did not have confidence in CHWs or comadronas). Second, our loss to follow-up in the longitudinal cohort was higher in 1 community relative to the other 7. Indeed, in this 1 community, fewer families owned land (70% vs 84%, P = .021) and families often traveled to the coast for work, early PP maternal underweight was more common (11% vs 2%, P = .043), women’s social support score was lower (1.0 vs 1.3, P = .003), and more infants were severely stunted both early (31% vs 13%, P = .020) and later (32% vs 11%, P = .015) PP. These distinct characteristics of this community may need to be considered if these variables emerge in subsequent analyses of the data. Third, intestinal infections may have been underreported due to limitations in locally available diagnostic methods. Fourth, compliance among women in the longitudinal cohort in providing fecal samples declined over the 3 visits (94%, 86%, and 80%), perhaps because women were, for the most part, asymptomatic. Fifth, many women did not know the date of their LMP, and birth weight data were dependent on mother’s recall and had been collected using varying methods, limiting our ability to accurately determine gestational age, prematurity, and birth weight. Finally, as demonstrated by differences between our data and Guatemalan data, study findings may not be generalizable to other communities in Guatemala.
Conclusion
The first 1000 days of life has been recognized as “the window of opportunity,” whereby concerted action and investment in maternal and child health can have a life-changing impact on a child’s future and help break the cycle of poverty. Although maternal and child nutrition has received most attention, a wide and multisectoral range of factors—including household and psychosocial—has been associated with early infant growth. Our socioecological conceptual framework intends to bridge this gap. The diversity of quantitative data and the considerable variability detected in such areas as household wealth, maternal autonomy, social support, diet diversity, and infant feeding practices provide a rich database from which we will explore, in subsequent papers, the stressors that may influence the health of the maternal–infant dyad. The qualitative component of the research, also to be described separately, will provide ethnographic insights that will not only guide our interpretation of quantitative data analyses but also reveal relevant information not captured by quantitative data. Finally, the richness of this database will allow us to identify unique coping strategies that promote resilience within this vulnerable population.
Footnotes
Acknowledgments
The authors would like to thank the study participants; involved communities; the local staff for help recruiting participants, collecting data, and optimizing follow-up; Marta Escobar and Alejandra Maldonado for anthropometric and nutritional assessments; Maria García for assistance with project coordination and data entry; Elena Ruiz for dietary data entry; Gloria Hidalgo for use of laboratory facilities and Flory de Canastuj for stool analyses at the Hospital La Democracia; Rosario García for local support and document translation; and the following students for field assistance: Caitlin Crowley, Mariah Kincaid, Lucy Manchester, Eleanor Platt, Olivia Russell, Cindy Stoffel, and Christine Whang. We also acknowledge helpful suggestions from Professor Duncan Pedersen, MD (Douglas Institute Research Centre, Quebec, Canada) regarding local idioms of distress in Mayan women.
Authors’ Note
A. M. Chomat contributed to conception and design, contributed to analysis, drafted the manuscript, gave final approval, participated in obtaining funding and supervision, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. N. W. Solomons, K. G. Koski, and M. E. Scott contributed to conception and design, contributed to analysis and interpretation of data, drafted the manuscript, critically revised the manuscript, participated in obtaining funding and supervision, gave final approval, and agree to be accountable for all aspects of work ensuring integrity and accuracy. H. M. Wren contributed to analysis, design of the study, data collection, interpretation of data, and critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. M. Vossenaar contributed to analysis, participated in the design of study instruments, interpretation of data, and critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was obtained from the SDE-Graduate Women in Science, USA, the Global Health Research Capacity Strengthening Program, Canada, the Programme de Bourses d’Excellence pour Etudiants Etrangers (PBEEE), Quebec, Canada, the McGill University Graduate Travel Award, and the Institute of Parasitology at McGill University Graduate Excellence Fellowship. Research at the Institute of Parasitology is supported by a Regroupement stratégique grant from Fonds de recherche du Québec—Nature et technologies. The funders had no role in the design, analysis, or writing of this article.