
Abstract
Background:
Serum retinol concentrations are homeostatically controlled and only fall when liver stores of vitamin A are very low. Nevertheless, low concentrations of serum retinol occur in apparently healthy people where there is no evidence of vitamin A deficiency (VAD).
Objective:
To determine the reason for low serum vitamin A concentrations where there is no VAD.
Methods:
We observed that elevated acute-phase protein (APP) concentrations often accompanied low retinol concentrations, and we developed a model of the inflammatory response to categorize 4 groups of participants termed reference (no raised APP), incubation (raised acute APP only), early convalescence (both acute and chronic APP raised), and late convalescence (raised chronic APP only). We identified 7 studies with participants who could be allocated to the 4 groups, and using meta-analysis methods we calculated correction (ie, multiplication) factors 1.13, 1.24, and 1.11 to remove the influence of inflammation from the incubation, early, and late convalescent groups, respectively.
Conclusion:
In nutrition surveys or intervention studies to measure vitamin A status, workers should measure APP and correct retinol concentrations using the multiplication factors where inflammation is found.
Introduction
In 2003, we published an article describing a meta-analysis of studies on serum retinol concentrations in which we showed how to remove the effects of inflammation to improve the use of serum retinol as a biomarker of vitamin A status. 1 In fact our work on vitamin A began some 15 years earlier when we struggled to find explanations for low serum retinol concentrations in places where there was no other evidence of poor vitamin A status. 2
At that time, there was much evidence of poor vitamin A status in the world, particularly in countries of Southeast Asia, 3 Africa, 4 and also in India. 5 However, there were also some strange reports such as that from a regional hospital in Cape Town in South Africa, 6 where the workers reported dramatic effects of vitamin A supplements in children with severe measles in comparison to those who did not receive vitamin A, on all clinical biomarkers (pneumonia, diarrhea, and croup) including a 33% reduction in the time spent in hospital and the number of deaths was more than halved. Surprisingly though, the authors pointed out that VAD in their locality was rare and their search in the late 1990s of more than 160 000 hospital records could find only 3 hospital admissions for vitamin A deficiency (VAD) and none since 1985.
My own interest in vitamin A began while working in Linxian province in the People’s Republic of China. The region had a very high prevalence of esophageal cancer, and workers at the International Agency for Research on Cancer were interested in determining whether supplements of vitamin A, riboflavin, and zinc would reduce the prevalence of a risk factor for esophageal cancer, namely, esophagitis, an inflammation of the wall of the lower esophagus. 7 Baseline measurement of the 3 nutrients showed that there were indeed low serum concentrations of the 3 nutrients, but I puzzled over the interpretation of the retinol results (Table 1). 2 The Chinese results were 25% to 33% lower in both sexes than typical results obtained in Western countries, 8 but there was no clinical evidence of VAD in the community. The people we were studying were poor rural farmers whose diet was predominantly vegetarian and people were outwardly strong and healthy. Jim Olson had reported that in the face of a dietary VAD, plasma retinol concentrations were physiologically controlled and did not fall until liver reserves fell to a very low level. 9 The concentrations of serum β-carotene concentrations in the Chinese farmers were adequate, comparable with UK values (Table 1), and did not suggest a dietary VAD. My colleagues did show that the prevalence of esophagitis was high in the community but there were no reports of VAD. Furthermore, we saw no eye signs to indicate VAD in children in a local school and as far as we could understand there was no mention of, or word for, “night blindness.” Night blindness is a difficulty in seeing in dim light, and where VAD occurs there is usually a local word to describe this condition. However, although there was no clinical evidence of VAD, we accepted that the retinol results suggested vitamin A status was at least suboptimal.
Serum Retinol and β-Carotene Concentrations in Apparently Health Adults in Linxian Province in the People’s Republic of China in Comparison With British Adults.a
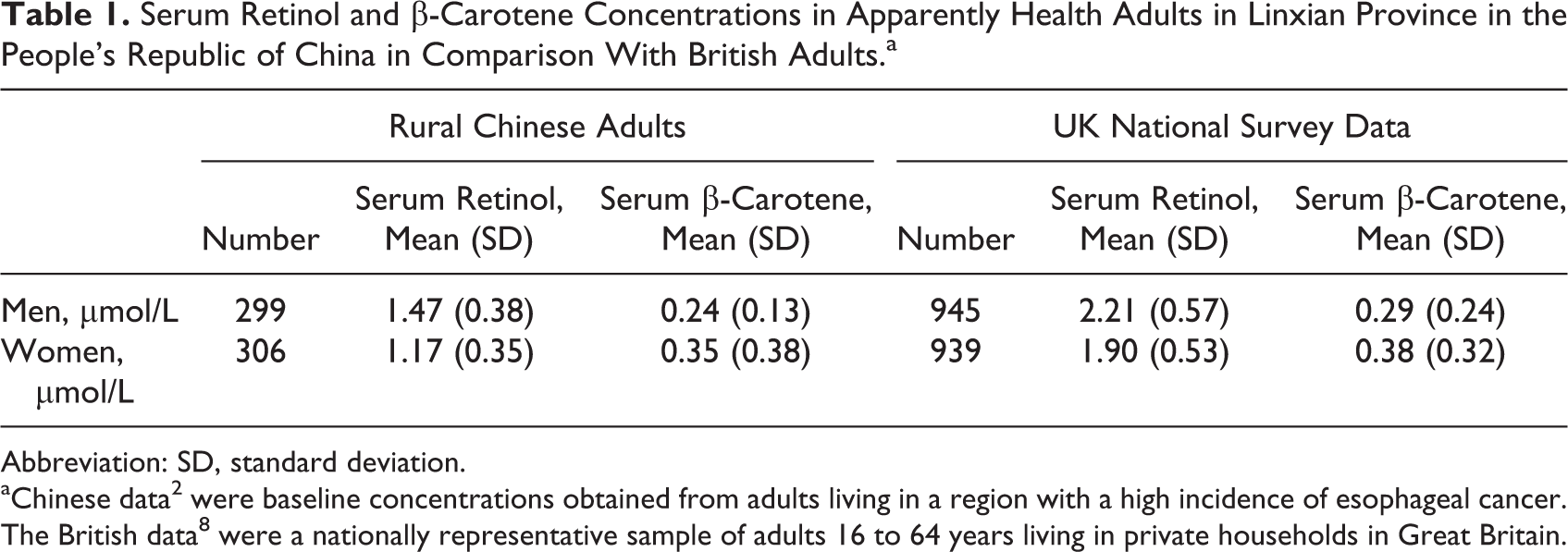
Abbreviation: SD, standard deviation.
Marginal Malnutrition
In the late 1980s, micronutrient biomarkers were of considerable interest to researchers to predict a risk of disease. Poor vitamin A status was believed to predict the risk of various cancers, and workers attached particular importance to low serum β-carotene concentrations. 9,10 A number of prospective community studies had shown that low β-carotene concentrations at baseline were associated with higher risks of lung cancer 5 to 10 years later. 11 A prospective study in healthy middle-aged men in the United Kingdom had also reported low serum albumin was strongly associated with mortality from heart disease, cancer, and deaths from all causes 10 years later. 12 Even when deaths in the first 5 years were excluded, the correlations still persisted. At that time, serum albumin was commonly regarded as a biomarker of protein intake and status, and the workers in that study had no prior hypothesis that albumin was a predictor of mortality. 12 Nevertheless, there was growing awareness that the metabolism of albumin was altered in disease and that serum concentrations fell quickly following infection and trauma, and albumin was regarded by some as a negative acute-phase protein (APP). 13
Subclinical Disease and Serum Retinol Concentration
The APPs are biomarkers of disease and mostly increase following infection and trauma. The first APP we looked at in relation to vitamin A was α1-antichymotrypsin (ACT). Workers examining the merits of 5 different APPs in the recognition of inflammatory conditions reported that while all had similar specificities, ACT was more sensitive than the others, including C-reactive protein (CRP), as ACT had a longer half-life. Both CRP and ACT responded rapidly to infection (within 6 hours). 14 We also chose ACT because workers in The Gambia who were investigating the associations between subclinical disease, gut integrity, and stunting 15 had measured serum ACT concentrations in The Gambian infants over a period of 13 months (Figure 1). 17 The cutoff for an abnormal activity of ACT is a concentration >0.6 g/L, and it is clear from the figure that ACT activity was abnormal in most infants in every month of the year. However, seasonal fluctuations in their data showed that mean serum ACT concentrations only approached normality at a time when mangos were in abundance. Mangos are an important source of dietary vitamin A, and the mango season, which runs approximately from May to June, coincided with the time of least inflammation. The researchers had not measured serum retinol but their data suggested that there might be an inverse relationship between inflammation and vitamin A status, as there was less inflammation when the intake of vitamin A was high. We also found 2 other studies, which confirmed a reciprocal relationship between serum retinol concentrations and inflammation measured using CRP. 18,19 Both studies reported a 30% to 40% fall in serum retinol concentrations in healthy individuals undergoing elective surgery in the immediate postsurgical 48 hours and peak concentrations of CRP coincided with the nadir of serum retinol. Figure 2 shows the typical acute-phase response following the surgery reported in one of these studies. 19 Mean serum retinol concentrations fall rapidly and then return to presurgical levels at 7 days. To produce such changes in serum retinol concentrations using dietary deficiency and repletion, would require many months, 20 and it was clear from this work that serum retinol concentrations were rapidly and strongly influenced by inflammation.
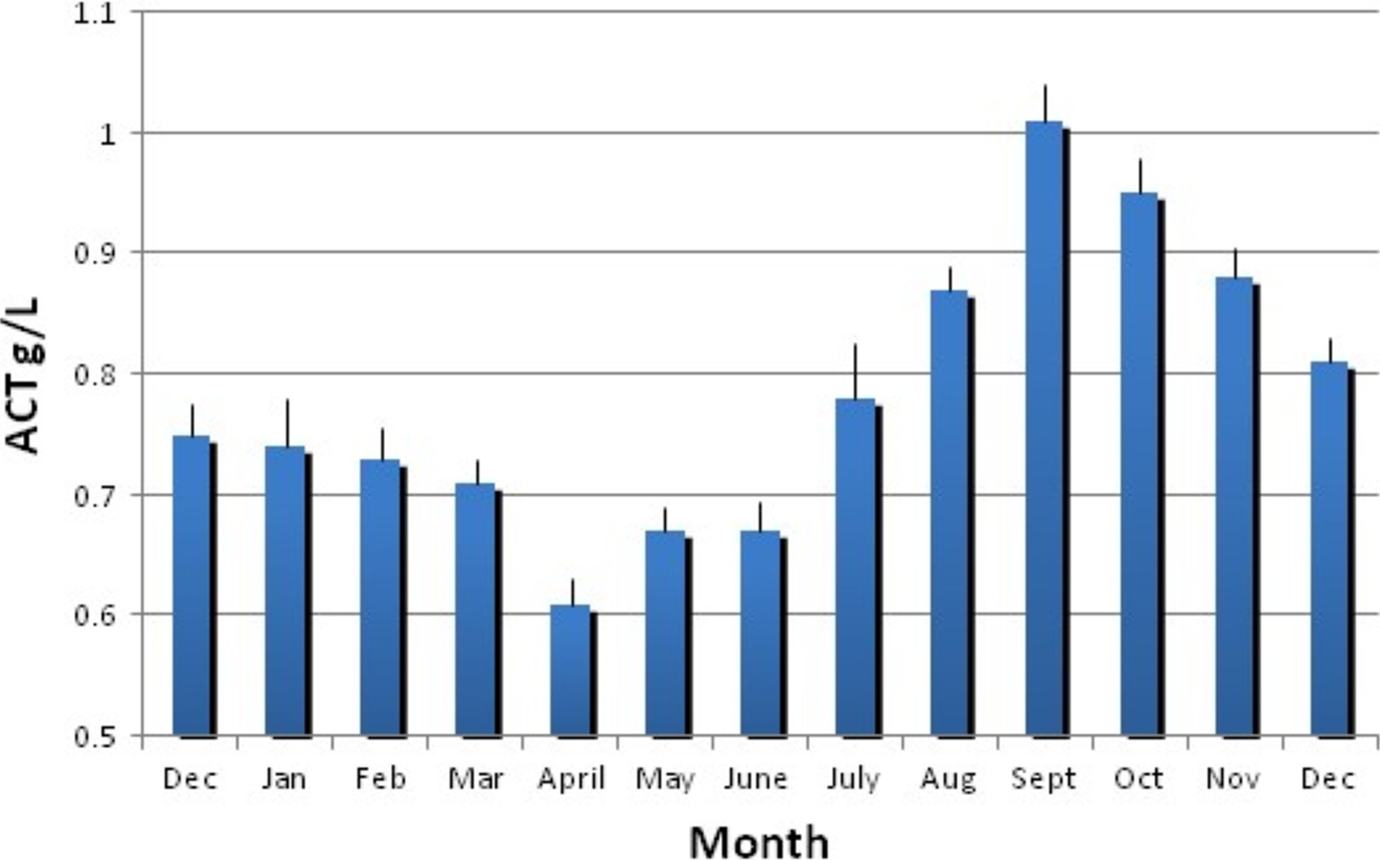
Serum α-1-antichymotrypsin concentrations in Gambian infants. Seasonal changes in α1-antichymotrypsin (ACT) concentrations. Each bar shows the mean (standard error) values for 50 to 60 infants with a mean age of ∼8 months. Infant concentrations of ACT were measured monthly following recruitment at ∼2 months until the study end at 15 months. Adapted from reference 16 with permission.
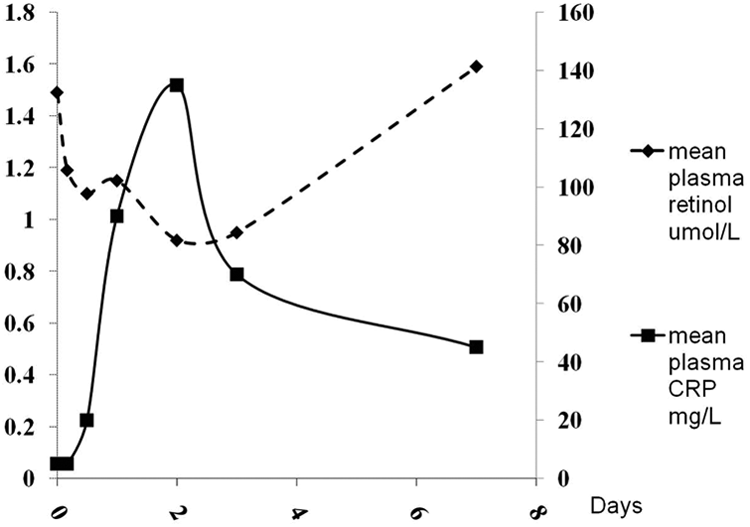
Changes in serum retinol and C-reactive protein (CRP) concentrations following uncomplicated orthopedic surgery. 19 This figure shows fall in plasma retinol concentrations accompanied by a rise in plasma CRP concentrations following surgery in previously healthy and well-fed people. After 48 hours, retinol returns to normal as CRP concentrations fall.
Although the studies of Ramsden et al 18 and Louw and colleagues 19 showed that serum CRP and retinol concentrations changed over similar time spans following surgery, these studies were the responses of previously healthy and well-fed people. In a community where marginal or chronic malnutrition existed, the inflammatory response by retinol to an infection may be different. In particular, malnutrition may make the return to normal following the clinical disease longer than that seen in the postsurgical studies. We decided we also needed a biomarker of chronic or long-term inflammation, and the APP orosomucoid or α1-acid glycoprotein (AGP) appeared to be a suitable candidate. The AGP begins to increase with the onset of infection, 14,21 but the rise is slow and the concentration does not exceed the normal range until 2 to 5 days after the initial trauma and has a relatively long half-life during the convalescent period. 13,22
Model to Categorize Subclinical Inflammation
The model we developed to illustrate the influence of inflammation on serum retinol concentrations is shown in Figure 3. The model mimics the theoretical cycle of events displayed by retinol and the APP following a trauma. It was based on what was known concerning the responses of the acute (CRP or ACT) and chronic (AGP) APP and that of serum retinol to inflammation and trauma and was used to categorize serum samples from apparently healthy individuals into 4 groups. The model also shows a period of clinical sickness; however, the changes in retinol and the APP during clinical sickness were not the focus of these studies, since our main aim was to monitor inflammation in people who would be included in surveys or intervention studies. In such studies, ethical concerns would ensure that sick people would be excluded and their illness treated.
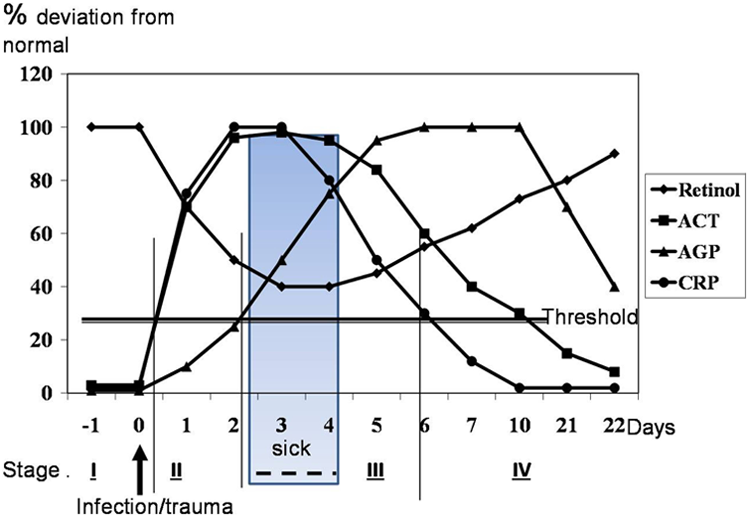
Model of behavior of acute phase proteins and retinol during course of infection. 23 This figure shows the typical behavior of 3 acute phase proteins C-reactive protein (CRP), α1-antichymotrypsin (ACT), and α1-acid glycoprotein (AGP) during a hypothetical infection beginning at day 1. Threshold indicates the cutoff separating normal acute phase protein concentration and inflammation. Roman numerals indicate the groups of participants identified by the acute phase proteins namely reference (I), incubation (II), early (III), and late convalescence (IV), see methods for details. The partly obscured box indicates a period of ∼48 hour (but could be longer) when clinical disease is present where participants would be treated and not recruited for study.
The 4 groups are indicated by Roman numerals in Figure 3. Group 1 was regarded as the reference or healthy group and included participants with no raised APP. Group 2 we called the “incubation group” and included participants where only the acute APP was increased (CRP > 5 mg/L or ACT >6 g/L) and AGP was normal (
The first study where we used the model examined serum retinol concentrations from 2519 preschool children (6-60 months) collected as part of a nutritional survey in North-West Frontier Province, Pakistan. 24 The APPs used to categorize the samples were ACT and AGP, and the results are shown in Table 2. It was very apparent that a very large proportion of the children (46%, n = 1155) displayed covert inflammation. Most of this inflammation (76%) was found in the late convalescent group with most of the remainder in early convalescence. Only 14 participants had inflammation in the incubation group, and these data suggested to us that acute infection was relatively infrequent at the time of the survey or incubation was very short but once infected, children experienced a prolonged period of chronic inflammation, that is, full recovery back to health was slow.
Serum Retinol Concentrations of Preschool Children Sampled From Rural and Urban Areas in the North-West Frontier Province, Pakistan, Categorized by Inflammation Status.a
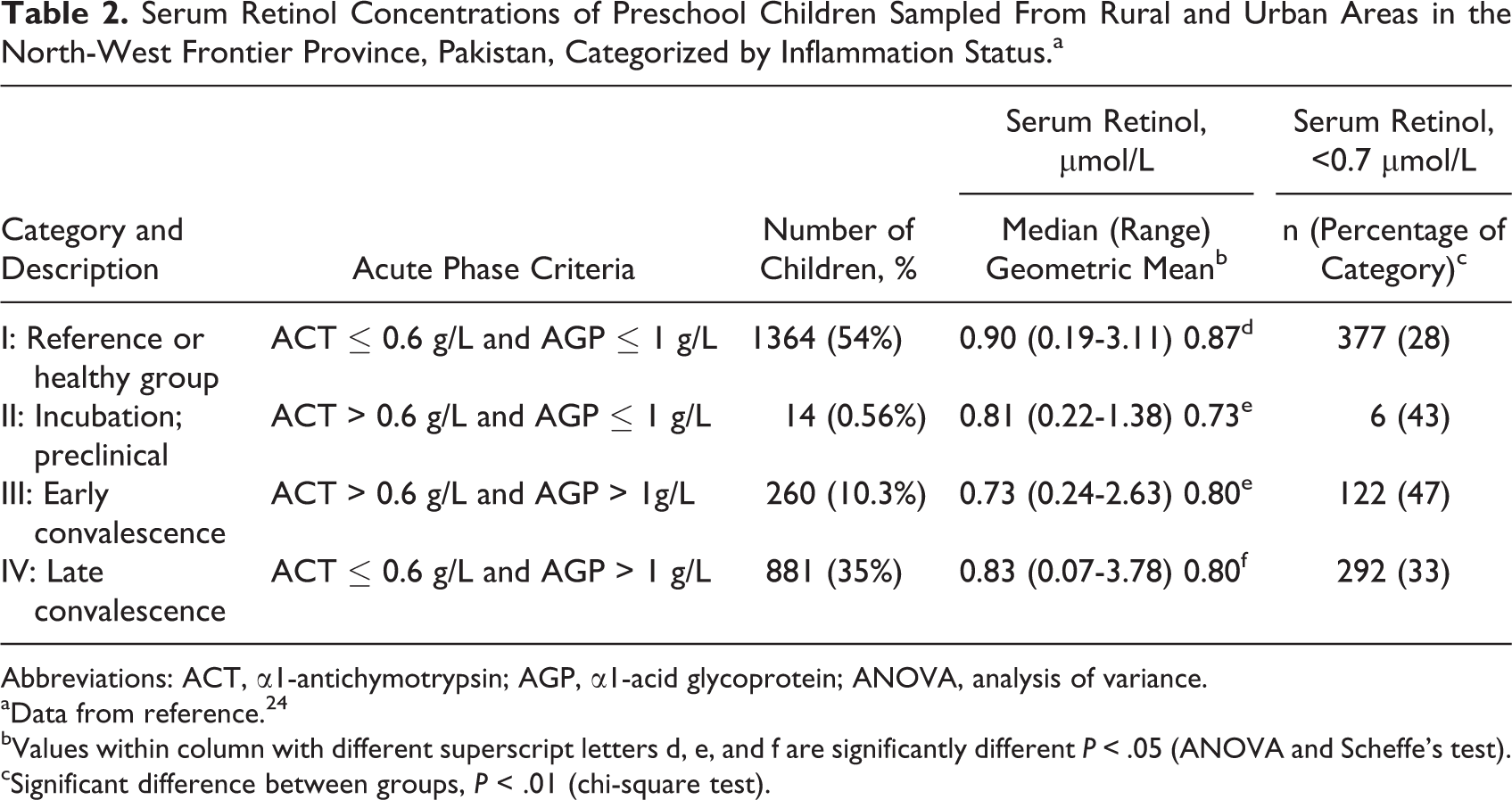
Abbreviations: ACT, α1-antichymotrypsin; AGP, α1-acid glycoprotein; ANOVA, analysis of variance.
aData from reference. 24
bValues within column with different superscript letters d, e, and f are significantly different P < .05 (ANOVA and Scheffe’s test).
cSignificant difference between groups, P < .01 (chi-square test).
In the total survey sample, low retinol concentrations suggested that there were 32% of children (n = 797) at risk of VAD (retinol < 0.7 μmol/L). The proportions of low serum retinol concentrations in the inflammation groups were higher than in the reference group but only significant in the early convalescent group (47%). There were still 28% of children with low retinol values in the reference group and we assumed that the vitamin A status of the reference group will be the closest to the true vitamin A status of the community. The mean retinol concentration of preschool children in developed countries is very close to 1.0 μmol/L, 25 whereas the median or geometric mean retinol concentrations of the Pakistani children in the reference group were 0.9 and 0.87 μmol/L, respectively, suggesting that low retinol values were due to both dietary deficiency and the effects of inflammation.
In this study, the number of children in the reference group was large enough to give a reliable estimate of status. For smaller studies, however, it is desirable to find a way of correcting retinol concentrations to remove the influence of inflammation so that all data can be used to provide the best estimate of status in a community. Although the Pakistani study was very large, a single study alone could not be relied on to do this, and instead we would need to amass information from other studies where retinol and inflammation biomarkers had been measured and analyze these using meta-analysis techniques. We also noted that there was a very strong correlation between serum ACT and AGP concentrations (r = .74, P < .001) in the Pakistani study. 24 Undoubtedly, this was because both were measuring the presence of inflammation but we were anxious to differentiate acute and chronic inflammation as much as possible, and the study of Calvin et al showed that ACT responded over a longer time than CRP, that is, into the chronic inflammation phase. 14 We decided future studies should use CRP and AGP rather than ACT and AGP to differentiate the 2 phases separately as far as possible.
Correction Factors to Remove the Influence of Inflammation From Serum Retinol Concentrations
To calculate correction factors, studies were identified in which acute and chronic APPs were measured together with serum retinol in apparently healthy people. 1 Of the studies identified, all used CRP as the acute APP except the Pakistani study (Table 3). In each study, the 2 APPs were used to define the reference group and the 3 inflammation groups as described in Figure 3.
Studies Identified for a Four-Group Vitamin A Meta-Analysis.a
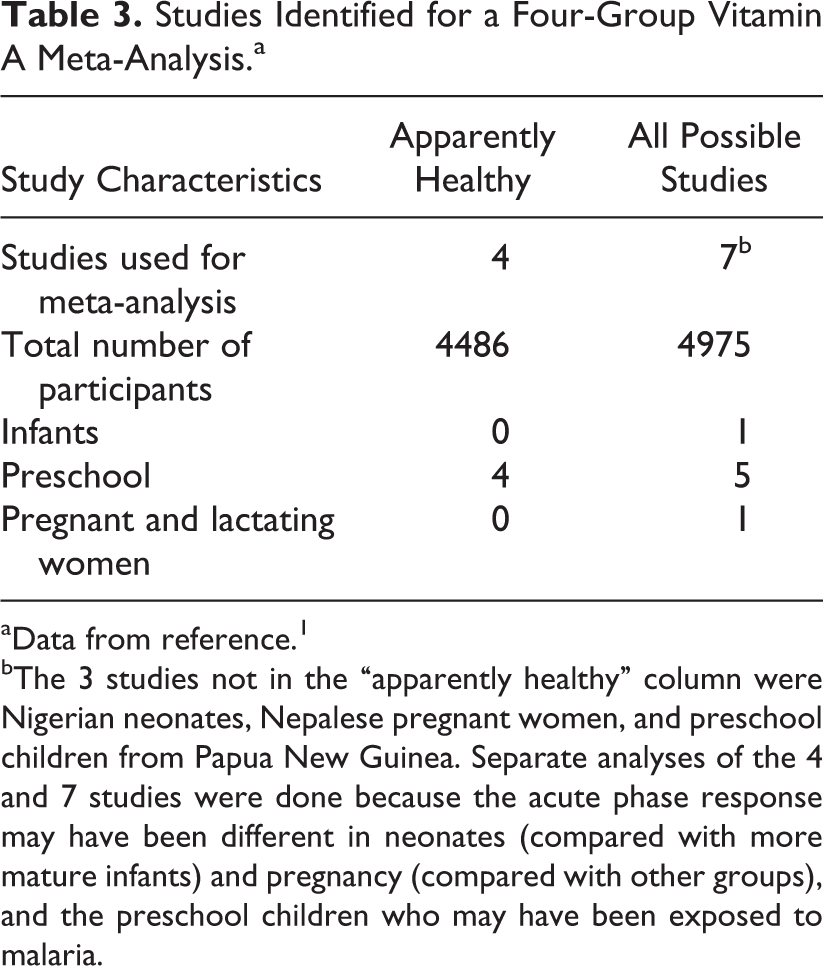
aData from reference. 1
bThe 3 studies not in the “apparently healthy” column were Nigerian neonates, Nepalese pregnant women, and preschool children from Papua New Guinea. Separate analyses of the 4 and 7 studies were done because the acute phase response may have been different in neonates (compared with more mature infants) and pregnancy (compared with other groups), and the preschool children who may have been exposed to malaria.
We identified 15 studies where serum retinol and APPs were measured but when participants were categorized by inflammation, only 7 of the studies had participants in all 4 groups and in 3 of the studies, there was some uncertainty whether the participants were apparently healthy (Table 3). There were also other difficulties to be controlled, for example, very large differences in sample sizes between studies and differences in methods to analyze AGP. We therefore ran the 4 and 7 studies in separate analyses (Table 4) and with and without the Pakistan sample to determine whether and how the different factors influenced the behavior of serum retinol in the different groups.
Summary Results From the Four-Group Meta-Analysis of Serum Retinol Concentrations in Apparently Healthy Participants.a
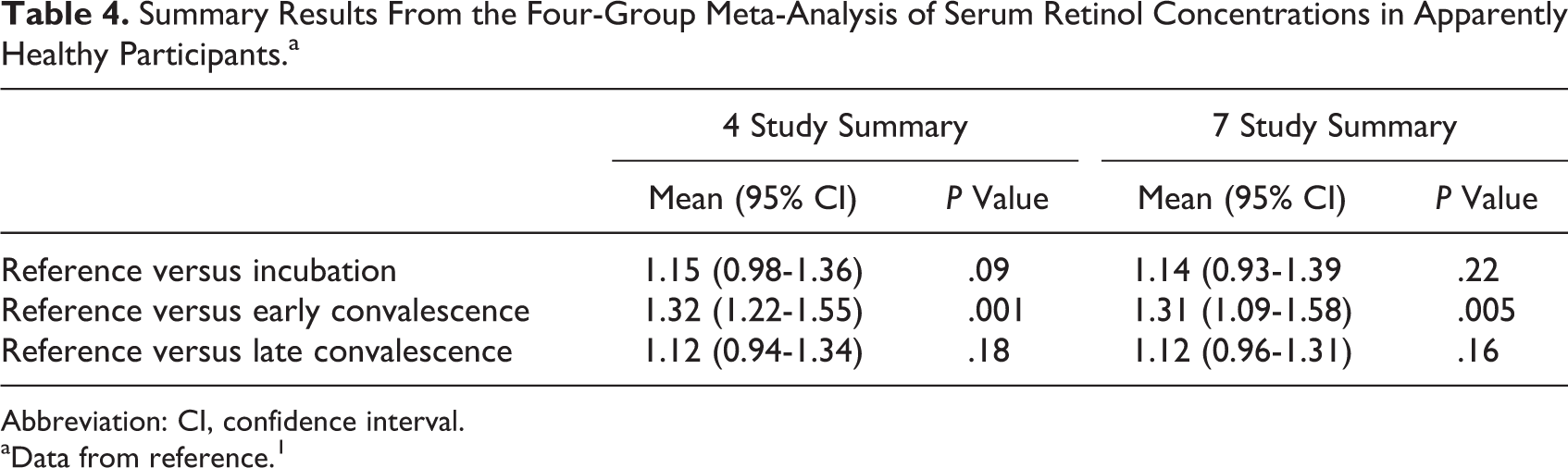
Abbreviation: CI, confidence interval.
aData from reference. 1
In the meta-analysis, plasma retinol concentrations were transformed using logarithms, and analysis of the 4 inflammation groups provided 6 pairs for comparison. Of these, only 3 were useful for the calculation of correction factors, namely, the ratios between the reference group and each of the inflammation groups. Each of the 3 pairs was summarized by study and analyzed as follows: The summary statistic (effect size) was the difference between 2 log means, and the variability between each summary statistic was related to sample sizes. In general, studies with larger numbers of samples have a smaller variability than those with smaller numbers. To combine the summary statistics of all studies, traditional weights were calculated based on the inverse of the within-study variance and therefore a relatively imprecise estimate of the study summary received less weight than a study with a smaller variance.
To estimate the variability of the overall summary statistic and provide study-to-study variation, the random effects model was used for the analyses reported, as it allowed for small differences among studies and enabled the generation of valid standard deviations. The mean ratios obtained from the analyses of the 4 and 7 studies were indistinguishable (Table 4). The ratios provided estimates for the depression in serum retinol for each of the inflammation groups relative to the reference group, and these were converted to multiplication factors 1.13, 1.24, and 1.11 for the incubation, early, and late convalescent groups, respectively. 1 That is, to correct plasma retinol for the effects of inflammation in the incubation, early, and late convalescent groups, all serum retinol values within the respective groups were multiplied by 1.13, 1.24, or 1.11, respectively, and the corrected concentrations added to the reference group samples to calculate the prevalence of VAD in the total sample.
The Need to Correct Serum Retinol Concentration for Inflammation
In sick patients, it is widely accepted that metabolism is disturbed and that inflammation will interfere with measurements of nutritional status. However, inflammation may also be present in apparently healthy people and depress serum retinol concentrations; therefore, it is very important that workers in national surveys should measure one or more APP to ensure that the true level of deficiency can be established in a community. Incorrect data on vitamin A status can only lead to false assumptions on status which might divert attention from the true cause of low retinol concentrations and promote the unnecessary use of supplements where none may be needed.
Removing the effects of inflammation from serum retinol concentrations is also necessary in vitamin A intervention studies. First, it is useful to confirm the presence of VAD by prior correction of serum retinol concentrations to remove the influence of inflammation, which may show the intervention to be unnecessary. Second, as low retinol concentrations will be influenced by the prevalence of inflammation and infection in a community, seasonal variations will potentially have more influence on the study outcome than the intervention. Even if a follow-up assessment is planned at the same time of year as the baseline study, the prevalence of inflammation may not be consistent year to year, resulting in variation in the apparent prevalence of low serum retinol concentrations.
Conclusion
We began by trying to understand why serum retinol concentrations in some developing countries were lower than those in developed countries when there is no evidence of VAD in the community. We observed that serum biomarkers of inflammation were lower at those times of the year when there was a rich dietary source of vitamin A available and that serum retinol concentrations were transiently lower following surgery. Using CRP and AGP, we developed a model of an inflammatory response to categorize the serum retinol concentrations by inflammatory status into 4 groups. The 4 groups comprised a reference group where there was no inflammation and 3 groups where inflammation was detected. Using meta-analysis techniques, we compared serum retinol concentrations between the 4 groups in 7 studies, where retinol and an acute and chronic APP had been measured. The comparisons enabled us to calculate multiplication factors to remove the influence of inflammation from serum retinol concentrations in the 3 groups where raised APPs were detected.
Footnotes
Authors’ Note
Rainer Gross Award Winner 2014: In November 2014, Professor David Thurnham was awarded the Rainer Gross Award (![]() ) by the Hildegard Grunow Foundation. This Award is given to recognize the merits of those who continue the generation and pursuit of innovative ideas and projects in nutrition and health in developing societies. In this issue of the Bulletin, we are pleased to be publishing Professor Thurnham’s article, “Inflammation and vitamin A,” the work outlined in this article was the basis for the Rainer Gross Award.
) by the Hildegard Grunow Foundation. This Award is given to recognize the merits of those who continue the generation and pursuit of innovative ideas and projects in nutrition and health in developing societies. In this issue of the Bulletin, we are pleased to be publishing Professor Thurnham’s article, “Inflammation and vitamin A,” the work outlined in this article was the basis for the Rainer Gross Award.
This article is based on a presentation given by Professor David Thurnham in Las Palmas on November 10, 2014 at the III World Congress on Public Health Nutrition to thank the Hildegard-Grunow Foundation for the Rainer Gross award given to him for contributions to solving burning problems in Third World nutrition.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.