
Abstract
Background:
Sex disparities in return-to-sport (RTS) outcomes after anterior cruciate ligament reconstruction (ACLR) remain poorly reported. Female athletes may demonstrate higher rates of anterior cruciate ligament (ACL) injuries than male athletes yet exhibit lower RTS rates.
Purpose:
To compare postoperative RTS outcomes between male and female patients after primary ACLR.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic search of the PubMed, MEDLINE, Embase, Scopus, and Web of Science databases was conducted from database inception through September 2025, following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Studies directly comparing RTS outcomes between males and females after primary ACLR with ≥12 months of follow-up were included. Data were synthesized using an exploratory random-effects meta-analysis. Odds ratios with 95% confidence intervals were calculated for dichotomous outcomes, and mean differences for continuous variables.
Results:
In total, 25 studies including 7183 athletes (2892 females, 4291 males) met the inclusion criteria. Female athletes demonstrated significantly lower odds of RTS at 12 months (OR, 0.76; 95% CI, 0.62-0.92; P = .005) and up to and including 24 months (OR, 0.72; 95% CI, 0.61-0.85; P < .001). No significant sex-based differences were observed for RTS to competition or return to preinjury levels.
Conclusion:
Female athletes are significantly less likely to RTS after ACLR during the critical midterm recovery period. These findings highlight the need for sex-specific rehabilitation and psychological support strategies to optimize RTS outcomes in female athletes.
Anterior cruciate ligament (ACL) injuries represent one of the most common and significant knee injuries in sport, with significant implications for athletic careers and long-term knee health. The incidence of ACL injury has risen over the last decades, particularly in the younger population and athletes, with pediatric ACL reconstructions (ACLRs) increasing by >40% in Norway between 2005 and 2021.8,40 As female participation in sport continues to increase, the sex disparity with ACL injuries is becoming highly established, with female athletes 2 to 8 times more likely to experience an ACL tear than male athletes. 10 This elevated risk reflects a complex interplay of anatomic, biomechanical, neuromuscular, and hormonal factors that predispose female athletes to injury. 44
Recognizing this, a recent Delphi study by the British Orthopaedic Association, involving patients, carers, and health care professionals, established a consensus-driven set of research priorities specifically addressing female ACL injuries. 10 Through a structured, multiround process, the study identified key areas of uncertainty relating to sex-specific differences in diagnosis, treatment pathways, injury prevention, rehabilitation, and the influence of psychological and environmental factors such as sports infrastructure and nutrition. Addressing these priorities is essential to advancing evidence-based, female-focused approaches to ACL injury management and improving long-term outcomes for females participating in sport.
Return to sport (RTS) after ACLR represents an important checkpoint of successful recovery. 22 Despite advances in surgical techniques and rehabilitation protocols, overall RTS rates remain suboptimal, with estimates suggesting that only 55% to 65% of athletes return to their preinjury level of sport.2,33 Moreover, female athletes may be less likely to RTS after ACLR compared with male athletes, and those who do return often do not return to their preinjury level but return at a lower level of competition or intensity. 33
While previous systematic reviews have evaluated sex-based differences with specific graft types,24,26,37,43 the purpose of this study was to compare postoperative RTS outcomes between male and female athletes after ACLR. Accordingly, we aimed to provide the most comprehensive synthesis of the available evidence to date on sex-based disparities in RTS, including the critical midterm recovery period. We hypothesized that female athletes would be less likely to RTS than male athletes after ACLR, particularly during midterm follow-up.
Methods
This systematic review and meta-analysis was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.47,53 The protocol was prospectively registered in PROSPERO (International Prospective Register of Systematic Reviews). There was no patient or public involvement in this review, and ethical approval was not required.
Search Strategy
A comprehensive literature search was conducted from database inception to September 27, 2025, across the PubMed, Ovid MEDLINE, Web of Science Core Collection, Scopus, and Ovid Embase databases. No publication or language filters were applied during the search. The full search strategy can be found in Supplementary Table 1 (available in the online version of this article).
Study Selection and Inclusion Criteria
Studies were imported into COVIDENCE for duplicate removal and screening. Two reviewers (D.A.E., S.S.G.) independently screened titles and abstracts, with disagreements resolved by a third reviewer (C.M.G.). Reference lists of included studies were also searched manually. Studies were eligible if they (1) directly compared RTS outcomes between males and females, (2) involved primary ACLRs, (3) were primary research studies, and (4) reported outcomes at ≥12 months of follow-up. Exclusion criteria were technical notes, reviews, commentaries, or editorials; studies not available in the English language or with inaccessible full texts; revision ACLRs; or studies that did not report RTS rates stratified by sex. Full inclusion and exclusion criteria are summarized in Supplementary Table 2 (available online). Data were extracted independently by 2 reviewers (D.A.E., S.S.G.) using a standardized pro forma including study characteristics and outcome data. Discrepancies between reviewers were resolved by consensus if necessary.
Outcome Measures
The primary outcomes were RTS rates and time to RTS, assessed at the latest follow-up (≥12 months). Subgroup analysis was conducted based on the type of RTS: (1) RTS at the preinjury level, (2) RTS to competition, and (3) RTS not otherwise classified or generic. Weighted means were calculated and were pooled by sample sizes.
Risk of Bias
Risk of bias was assessed with the ROBINS-I tool for nonrandomized studies. 63 Publication bias was assessed via funnel plots.
Exploratory Meta-analysis
The primary outcomes, RTS rates and time to RTS, were analyzed at multiple time points. For RTS rates, pooled estimates were calculated separately at 12 months, 24 months, up to and including 24 months (using whichever time point was available), and at the longest reported follow-up. Subgroup analyses were also performed. Time to RTS was analyzed as a continuous outcome. RTS rates were synthesized as odds ratios with 95% confidence intervals using the Mantel-Haenszel method. Time to RTS was summarized as mean differences. All analyses were conducted in RStudio (Version 2024.09.1+394) using the meta package. A random-effects model was applied throughout, with between-study variance (τ2) estimated via restricted maximum likelihood. For binary outcomes, a continuity correction of 0.5 was applied only when zero events occurred in one study arm. Studies with zero events in both arms were excluded in accordance with PRISMA recommendations. Given the inherent heterogeneity in study populations, outcome definitions, level of evidence, and methodological granularity, this meta-analysis should be considered exploratory and hypothesis generating rather than definitive. Between-study heterogeneity was assessed using the Cochran Q test, quantified using the I2 statistic, and expressed as τ2. For each pooled effect, the corresponding overall test (Z or t, depending on model) and P value were reported. Funnel plots were generated to assess small-study effects. Statistical significance was set at a P value <.05.
Results
Search Results
The database search identified 3792 studies, of which 301 underwent full-text review, resulting in 25 studies included in our synthesis ‖ (Figure 1, Table 1).
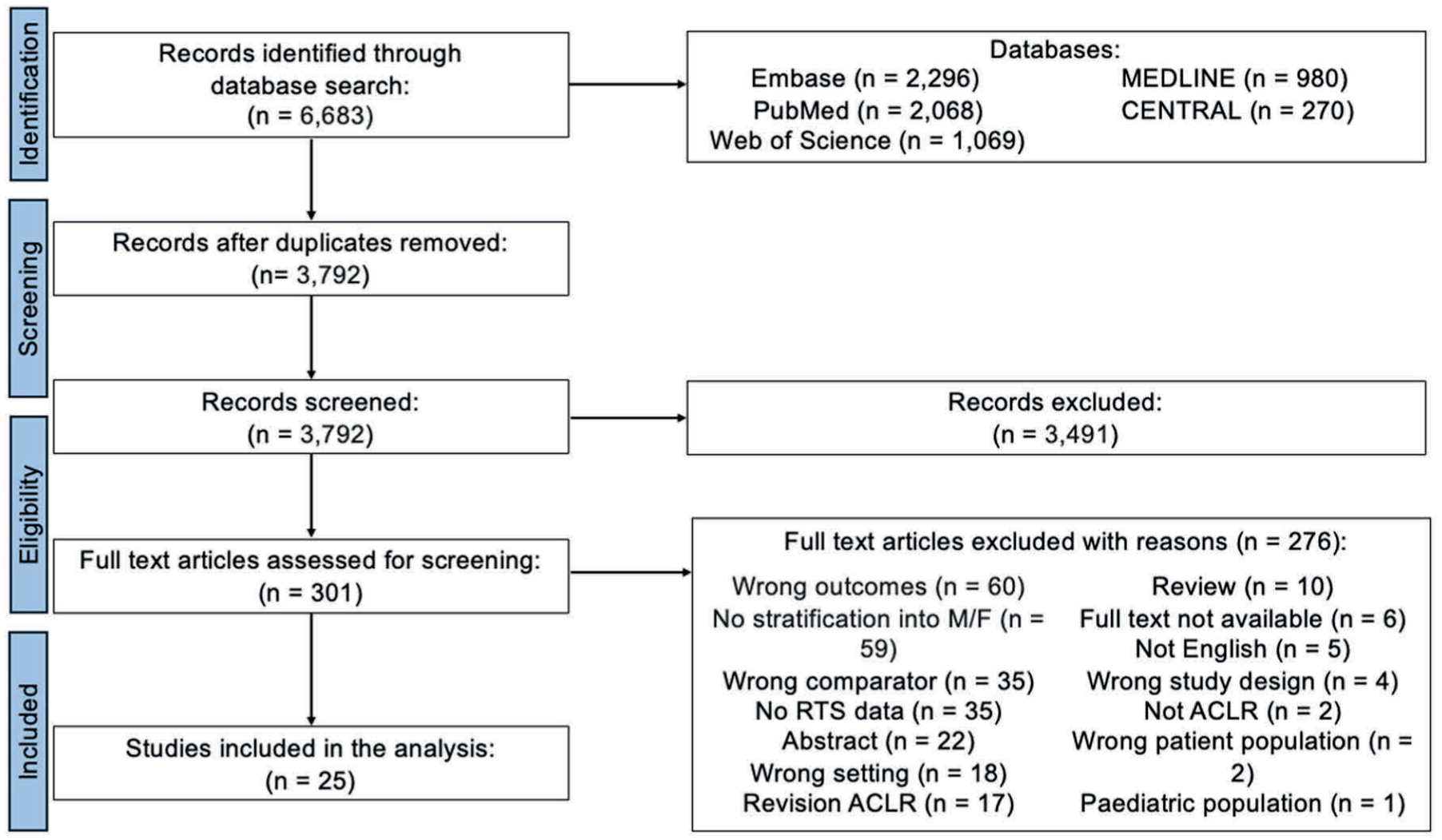
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram illustrating the study selection process for the systematic review. A total of 6683 records were identified across 5 databases (Scopus Embase, PubMed, MEDLINE, and Web of Science). After removing 2891 duplicates, 3792 studies were screened by title and abstract, of which 3491 were excluded. The remaining 301 full-text articles were assessed for eligibility, and 276 were excluded with reasons. In total, 25 studies met the inclusion criteria and were included in the qualitative and quantitative synthesis.
Study Characteristics a
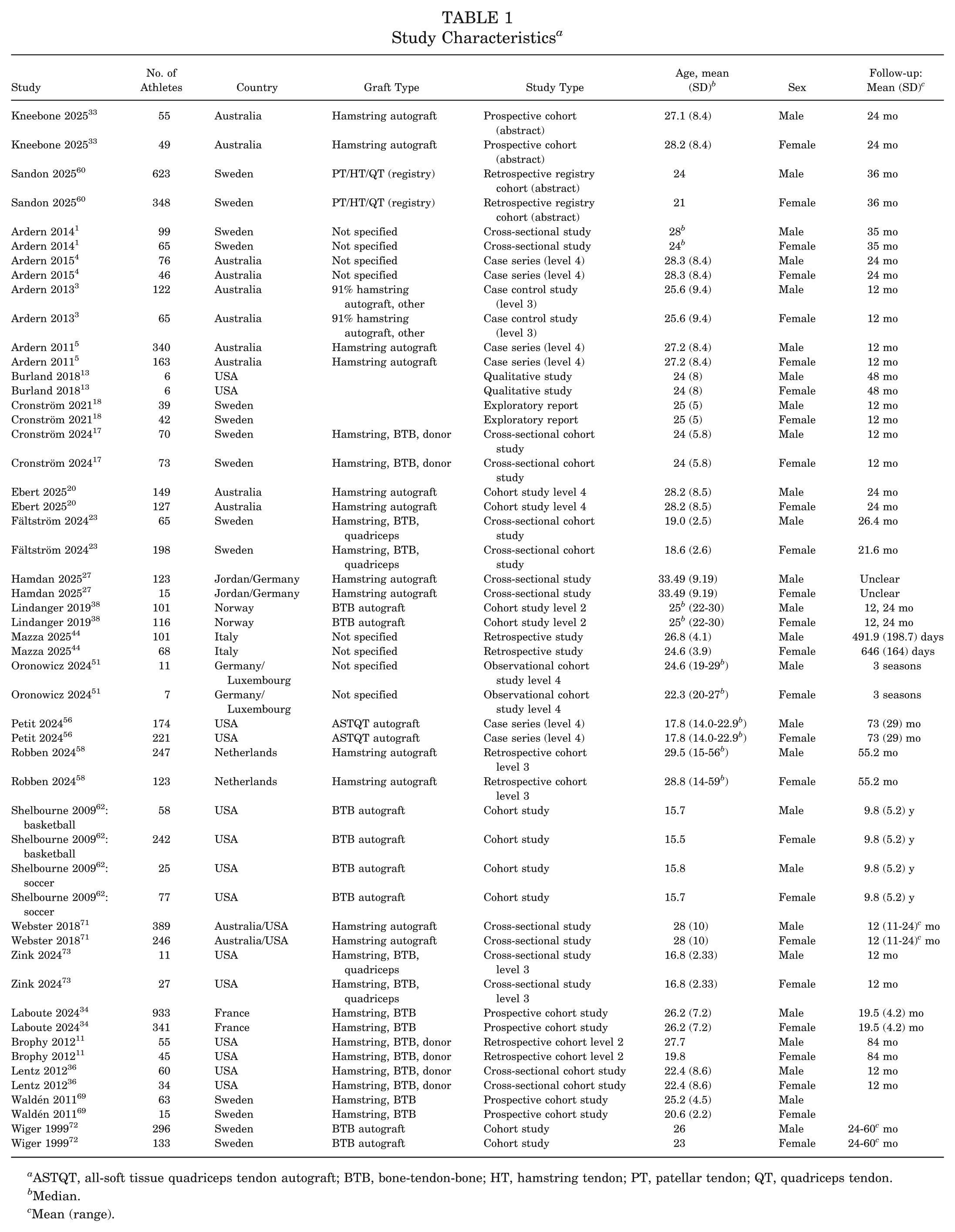
ASTQT, all-soft tissue quadriceps tendon autograft; BTB, bone-tendon-bone; HT, hamstring tendon; PT, patellar tendon; QT, quadriceps tendon.
Median.
Mean (range).
Risk of Bias and Quality Assessment
Of the studies and abstracts assessed, 13 were judged to be at low risk of bias in their selection of participants, 11 were judged as moderate, and 1 was judged as serious (Supplementary Table 3, available online). Sixteen studies were judged to be at moderate risk of bias in their measurement of outcomes, 1 was judged as low risk, and 8 were judged as serious. All studies were found to be at serious risk of bias due to confounding. Twenty-four studies were found to have a serious risk of bias overall, and 1 was found to be at moderate risk.
Characteristics of the Included Studies
The included studies predominantly originated from Europe (52%), followed by the Asia-Pacific region (24%) and North America (24%). The weighted mean age was 25.86 years for males and 23.12 years for females, with an overall age range of 14 to 59 years. The mean postoperative follow-up duration was similar between sexes, averaging 35.69 months for males and 35.70 months for females. Study designs consisted of 48% cohort studies (prospective, retrospective, observational, or registry based), 28% cross-sectional analyses, 12% case series, 4% case-control studies, 4% qualitative studies, and 4% exploratory reports. Graft selection varied across studies, with 36% using mixed graft types (hamstring, patellar, quadriceps, or allograft), 24% using hamstring autografts, 12% using patellar autografts, and 28% not specifying or reporting other graft types.
Systematic Review
The mean RTS time for males was 20.08 months (range, 5.1-55.2 months), and 20.45 months (range, 5.1-55.2 months) for females. Fifteen studies (60%) defined RTS as returning at any level or did not specify criteria. Seven studies (28%) defined RTS as return to preinjury level, and 3 studies (12%) defined RTS as return to competition. Specific definitions can be found in Table 2. The weighted mean RTS rates were 54.80% (range, 13.2%-100%) and 54.31% (range, 12.8%-93%) for males and females, respectively. At 12 months, study-level RTS rates ranged from 13.2% to 87.0% in males and 22.0% to 79.0% in females; at 24 months, RTS rates ranged from 35.0% to 88.0% in males and 40.0% to 82.8% in females (where reported). By RTS definition, studies defining RTS as any level/unspecified reported RTS ranges of 37.0% to 100.0% in males and 26.0% to 82.8% in females; studies defining RTS as return to pre-injury level reported ranges of 13.2% to 87.2% in males and 12.8% to 51.0% in females; and studies defining RTS as return to competition reported ranges of 26.0% to 87.0% in males and 16.7% to 93.0% in females (at latest reported follow-up).
Outcomes a
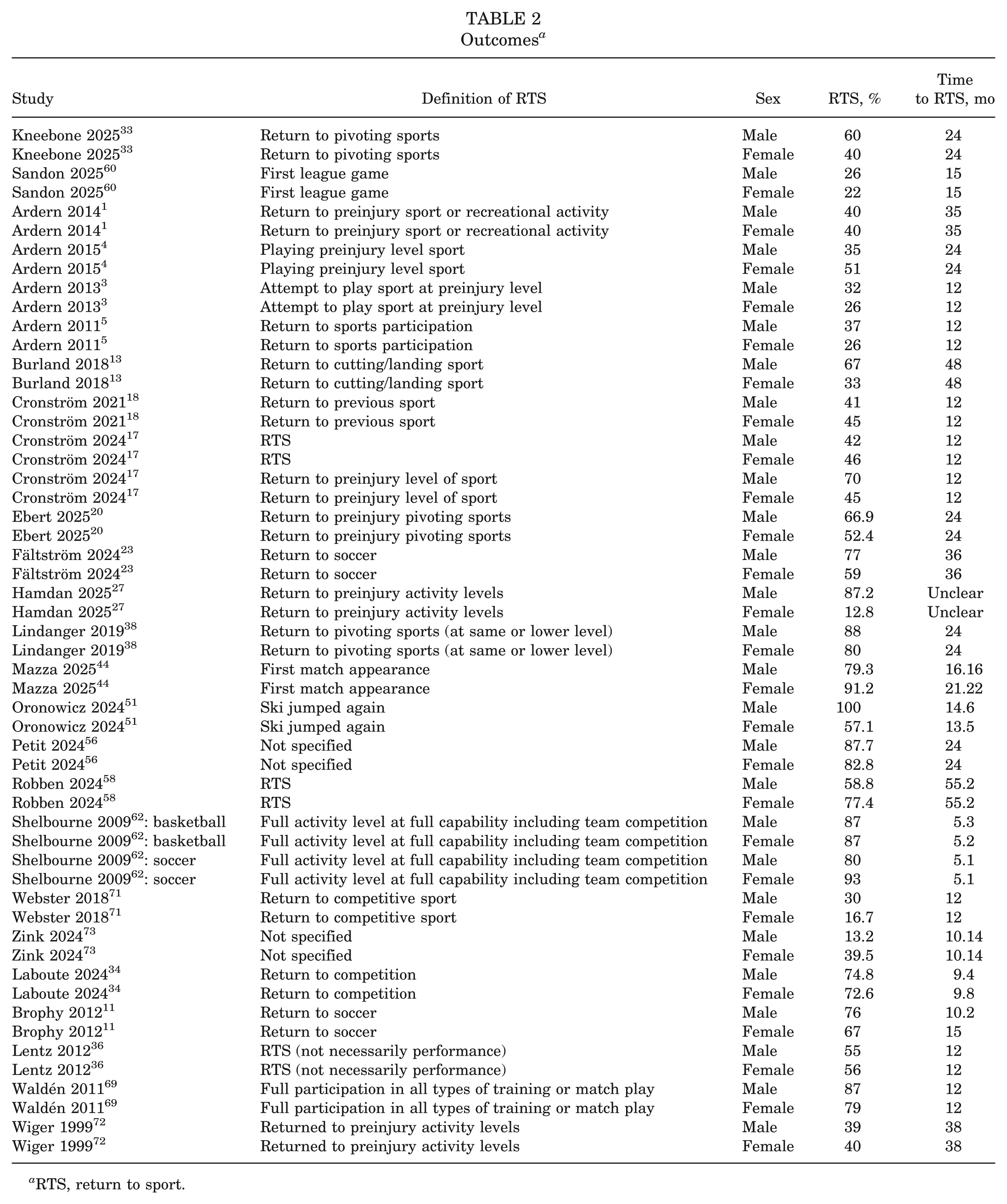
RTS, return to sport.
Meta-analysis: RTS
At 12 months, 8 studies (2238 athletes; 840 female, 1398 male) reported RTS outcomes. The pooled random-effects odds ratio was 0.76 (95% CI, 0.62-0.92; I2 = 4.8%; τ2 < 0.01; P = .005), indicating a significantly lower RTS rate in females (Figure 2).
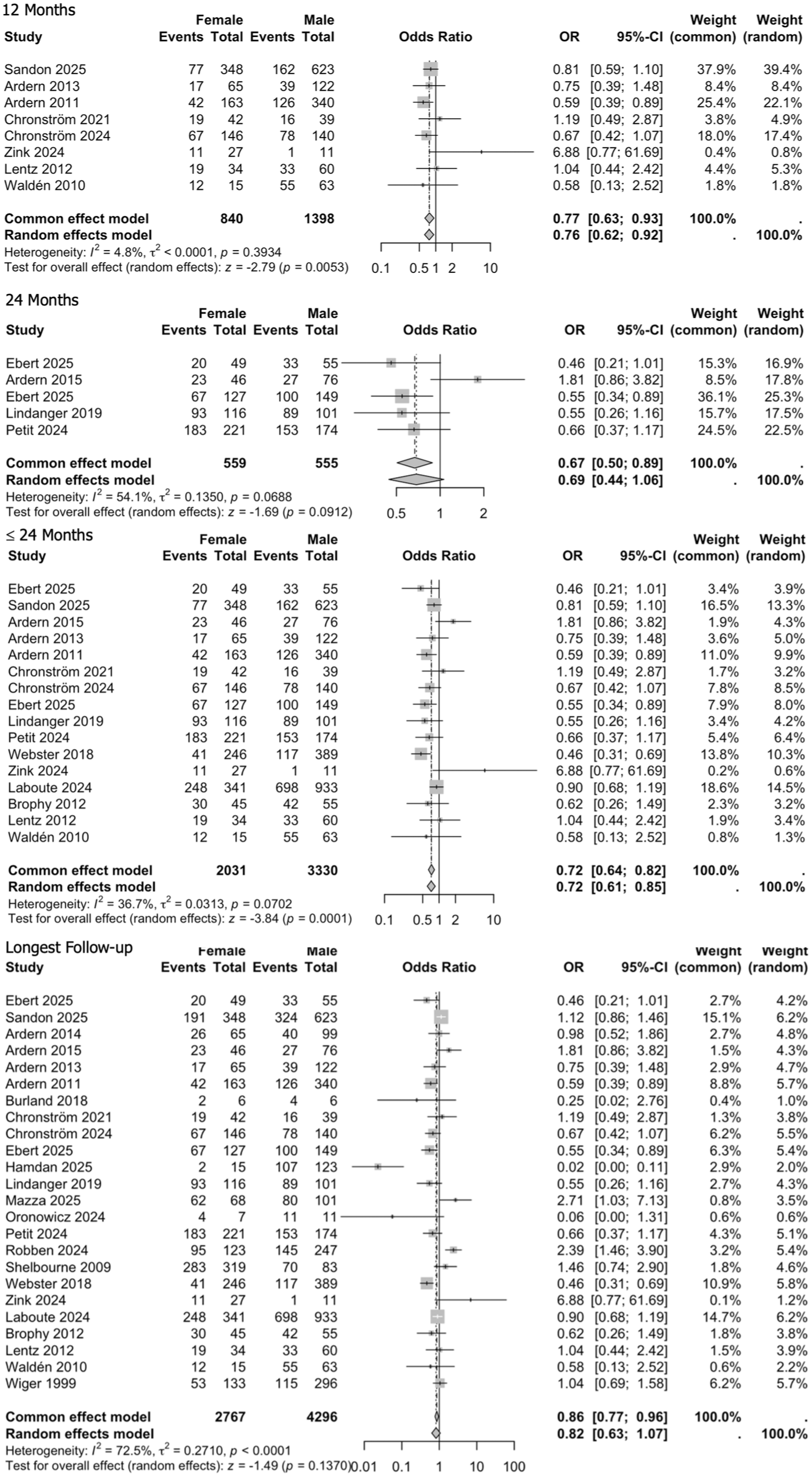
Forest plots comparing return to sport (RTS) between female and male athletes after anterior cruciate ligament reconstruction at different follow-up time points. Events represent the number of athletes who returned to sport; totals represent the number assessed at that time point. Study-specific effect sizes are presented as odds ratios with 95% confidence intervals. Squares indicate individual study estimates (size proportional to study weight), and diamonds indicate pooled estimates (common-effect and random-effects models shown). The vertical reference line denotes no difference between groups (OR, 1). Odds ratios <1 indicate lower odds of RTS in females compared with males. Between-study heterogeneity is reported using I2 and τ2.
At 24 months, 5 studies (1114 athletes; 559 female, 555 male) were available. The pooled odds ratio was 0.69 (95% CI, 0.44-1.06; I2 = 54.1%; τ2 = 0.14; P = .091), again showing no statistically significant sex difference (Figure 2).
At ≤24 months, 16 studies (5361 athletes; 2031 female, 3330 male) contributed data. The pooled random-effects odds ratio was 0.72 (95% CI, 0.61-0.85; I2 = 36.7%; τ2 = 0.03; P < .001), demonstrating a significantly lower likelihood of RTS in females compared with males (Figure 2).
At the longest follow-up, 24 studies (7063 athletes; 2767 female, 4296 male) were included. The pooled odds ratio was 0.82 (95% CI, 0.63-1.07; I2 = 72.5%; τ2 = 0.27; P = .137), suggesting no significant sex-based difference at longer-term follow-up (Figure 2).
Subgroup Analysis
RTS to Preinjury Levels
No significant sex-based differences in return to preinjury-level RTS were found at 12 months, up to 24 months, or at the longest follow-up. Analysis at 24 months was not performed due to insufficient data (Supplementary Figures 1–4, available online).
RTS to Competition
No significant sex-based differences in RTS to competition were found up to 24 months or at the longest follow-up. Analyses at 12 and 24 months were not performed due to insufficient data. (Supplementary Figures 1–4, available online)
RTS Not Otherwise Classified or Generic
At 12 months, there was no significant sex difference in RTS (Supplementary Figure 1, available online). At 24 months, 3 studies (716 athletes; 386 females, 330 males) showed lower RTS rates in females (OR, 0.57; 95% CI, 0.39-0.85; P = .006) (Supplementary Figure 2, available online). Up to 24 months, 9 studies (1715 athletes; 758 females, 957 males) also showed reduced RTS in females (OR, 0.70; 95% CI, 0.56-0.88; P = .002) (Supplementary Figure 3, available online). At the longest follow-up, no significant difference was observed (Supplementary Figure 4, available online).
Time to RTS
Seven studies (2972 athletes; 1155 female, 1817 male) reported time to RTS. The pooled random-effects mean difference was 0.48 months (95% CI, −0.19 to 1.14; I2 = 68.2%; τ2 = 0.43; P = .161), showing no statistically significant differences (Figure 3).
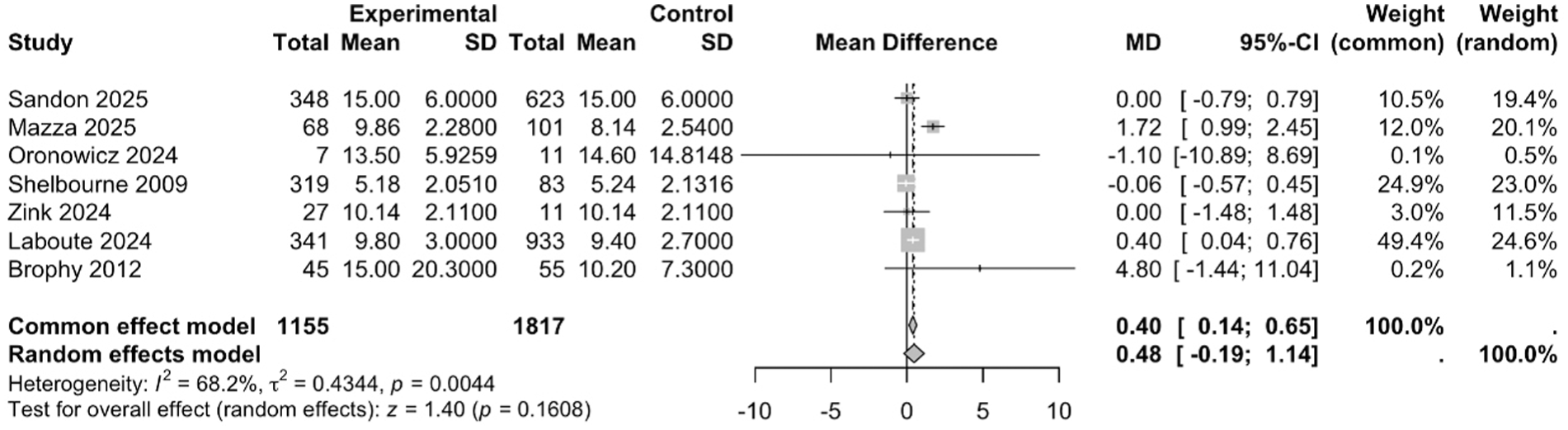
Forest plot comparing time to return to sport (RTS) between female and male athletes after anterior cruciate ligament reconstruction. Continuous outcomes are presented as mean difference (MD) with 95% confidence interval, where the experimental group corresponds to females and the control group corresponds to males (as displayed). Positive mean differences indicate longer time to RTS in females; negative mean differences indicate shorter time to RTS in females. Squares represent individual study estimates (size proportional to study weight), and diamonds represent pooled estimates (common-effect and random-effects models shown). Between-study heterogeneity is reported using I2 and τ2.
Discussion
This systematic review and exploratory meta-analysis represents the most comprehensive examination to date of sex disparities in RTS outcomes after ACLR. Data from 25 studies and >7100 athletes demonstrated sex disparities in RTS after ACLR. Sex-based differences in RTS were evident at 12 months and up to 24 months postoperatively, with females demonstrating approximately 28% lower odds of returning to sport within the first 2 years after ACLR. These findings suggest that early and midterm RTS rates are lower among female athletes, whereas long-term outcomes appear comparable between sexes. Our findings align with previous literature indicating that female athletes have lower RTS rates after ACLR,42,70 and offer novel insights by demonstrating that the lower RTS rates are most evident during midterm recovery, rather than early or long-term follow-up. This pattern suggests that female-specific support may be most critical during this phase. The absence of sex differences in retear risk and time to RTS further supports the likelihood that the lower RTS rates in females are driven predominantly by modifiable psychological, neuromuscular, rehabilitation, and environmental factors alongside inherent biological differences. 67
Biological and anatomic factors may contribute to the sex-based disparities and to both injury risk and reduced confidence in knee stability. 21 Females typically have a narrower and smaller femoral notch in comparison to males, 14 which can impinge on the lateral aspect of the ACL, increasing strain and tear risk. Moreover, A-shaped femoral notches, a physiological variant, are narrower in all width dimensions, 66 which may correlate with higher ACL injury rates. The female ACL also has a 20% to 30% smaller cross-sectional area than the male ACL, 39 alongside tibial morphological differences,14,15,30 and offers reduced resistance to tensile loading particularly in cutting or pivoting movements found in sporting activities. Genetic factors further contribute, with Magnusson et al, 41 in their population-based longitudinal cohort study in which they examined the incidence of ACL injuries in 88,414 Swedish twins, concluding that genetic factors contribute to approximately 69% of ACL ruptures, 41 likely mediated by inherited traits such as ligament laxity and notch geometry.32,61 Additional anatomic characteristics, including a wider pelvis and increased Q-angle, promote dynamic knee valgus and altered load distribution,35,46 increasing medial compressive and lateral tensile forces across the joint. 31 Collectively, these structural and biological differences may help explain the higher incidence of ACL injuries in females. However, as these characteristics are relatively constant over time and were not directly evaluated in relation to time to RTS within the included studies, their specific contribution to the observed midterm RTS differences remains uncertain. Further biomechanical and prospective research is required to clarify whether and how these factors influence postoperative recovery trajectories and RTS outcomes.
Neuromuscular differences may also influence postoperative function, affecting RTS rates. Females tend to demonstrate a greater degree of valgus collapse and less trunk control when landing,25,35 increasing strain on the ACL. Additionally, females exhibit more quadriceps-dominant movement patterns, relying on quadriceps muscles more than hamstring muscles, which increases anterior tibial translation during deceleration. 6 This is compounded by weaker hamstring co-contraction and reduced hamstring activation, despite the hamstrings serving as a key secondary stabilizer that counters anterior tibial translation.6,7 Consequently, females use quadriceps rather than hamstrings for knee stabilization, reducing dynamic joint stability and prolonging the time required to generate maximal hamstring torque.29,42 Females also demonstrate slower neuromuscular activation, with delayed engagement of stabilizing musculature. The latency between foot contact and hamstring activation ranges from 50 to 180 milliseconds, whereas ACL disruption can occur within 40 to 105 milliseconds, 65 meaning the ACL may fail before protective muscular reflexes can be activated. Moreover, females appear to have a higher risk of graft failure when undergoing hamstring autograft ACLR compared with bone-tendon-bone (BTB) autograft ACLR.12,55,59,64 When hamstring autografts are used, grafts >8 mm in diameter are associated with lower failure rates. 57 Additionally, augmenting either hamstring or BTB autografts with a lateral extra-articular tenodesis reduces the risk of retear by approximately 2.8-fold in elite athletes. 9 These graft-related considerations should be accounted for to optimize ACLR outcomes. Taken together, these anatomic, neuromuscular, and graft-related factors are likely to influence postoperative knee stability in females, potentially affecting RTS patterns. However, as this review did not identify consistent sex differences in graft retear rates or time to RTS, these factors alone are unlikely to fully account for the observed midterm disparity. Prospective studies specifically evaluating recovery trajectories and functional progression are needed to clarify their temporal relevance.
One of the key contributors for lower RTS rates in females is psychological readiness. Kneebone et al 33 demonstrated statistically significant differences in ACL Return to Sport after Injury scores between males and females at 24 months post ACLR. 33 This has been replicated across multiple studies in which males consistently demonstrated higher psychological readiness and higher RTS rates.23,49 This indicates that psychological readiness plays an important role in RTS rates and should be managed appropriately when an athlete is returning to play. Female athletes also report greater fear of reinjury and higher levels of posttraumatic stress after ACL injury, both of which negatively influence willingness and confidence to RTS.38,52 These findings highlight substantial psychological barriers faced by female athletes after ACLR and underscore the need for tailored psychological and behavioral support to optimize RTS outcomes. Nevertheless, psychological variables were not uniformly measured across the included studies, and therefore their direct contribution to the pooled midterm RTS differences cannot be definitively established from the current data.
Hormonal fluctuations across the menstrual cycle have been shown to influence ACL injury risk. Estrogen increases ligament laxity by reducing collagen production and cross-linking, with the risk of ACL tears being highest in the late follicular and ovulatory phases of the menstrual cycle. 16 This hormone-related laxity may destabilize the knee and alter landing, cutting, and pivoting mechanics, particularly relevant in sports with high rotational demand. Moreover, oral contraceptives have been suggested to reduce ACL injuries by up to 63%, likely because combined estrogen-progesterone formulations attenuate cyclical estrogen fluctuations, thereby reducing the ovulatory peak in ligament laxity and lowering susceptibility to injury.19,28 Overall, hormonal influences appear to interact with underlying biomechanical and neuromuscular factors to increase injury susceptibility in females, and may also affect postoperative knee stability, confidence, and ultimately RTS readiness. However, given the paucity of high-level data, and the absence of systematic tracking of hormonal variables within the included RTS studies, their role in explaining the observed midterm RTS disparities remains uncertain. Further prospective research is required to clarify these potential associations.
External factors also play a substantial role in the RTS rates, with Mears et al, 45 in their international study of 1129 players, showing that 91% of athletes believed the type or condition of a playing surface could increase injury risk. 45 The “gendered sporting environment” has become increasingly evident as women's sports expand, with female athletes frequently training and competing on lower-quality pitches and facilities, often due to reduced funding.50,54 Notably, elite female athletes are often provided artificial grass pitches, where ACL injuries are 50% more likely than on natural grass. 48 Given that the majority of ACL injuries in female athletes occur in noncontact situations, the equipment that supports optimal biomechanics is important. Footwear is a key modifiable factor, with differences in foot size and morphology between males and females altering load distribution, yet most football boots are designed around male loading profiles. 50 When female athletes wear boots tailored to male foot shape and force patterns, this can lead to discomfort, suboptimal force transfer, and increased injury risk. 50 Rotational traction is influenced by stud size and configuration, and studs are more likely to catch or lock during pivoting on artificial grass surfaces, where ACL injuries occur more frequently. 68 Despite sex-specific differences in optimal traction profiles, stud and boot designs largely mirror male biomechanical requirements. 50 Equipment-related mismatches may influence postoperative confidence and movement quality, potentially affecting RTS readiness. However, as these variables were not consistently measured in the included studies, their specific contribution to the observed RTS patterns remains uncertain.
An additional consideration is potential response bias within the primary studies. Many relied on retrospective questionnaires or voluntary follow-up, which may underrepresent individuals who did not RTS, particularly females with poorer functional recovery, thereby attenuating observed sex-based differences. This limitation aligns with the risk-of-bias assessment, in which many studies were judged to be at moderate to serious risk due to outcome measurement and confounding. Consequently, the true magnitude and trajectory of sex-based RTS differences may be either under- or overestimated. Future research should prioritize prospective longitudinal designs with standardized RTS definitions and high follow-up completeness to more accurately characterize sex-specific recovery trajectories.
Moreover, the included studies reported outcomes according to biological sex and did not distinguish sex from gender. As gender-related sociocultural factors may also influence RTS outcomes, future research should explicitly differentiate these constructs and evaluate how gender identity and context shape postoperative recovery trajectories.
Limitations
This review has several limitations. The included studies were heterogeneous in population characteristics, surgical techniques, graft types, injury mechanisms, sporting disciplines, and definitions of RTS, which may limit direct comparability between studies. Definitions of RTS varied widely, encompassing return to any activity, return to preinjury level, or return to competitive play, introducing potential inconsistency in outcome classification. Given the paucity of literature stratifying results by sex, there is a limited sample for pooled analysis, potentially limiting the statistical power to detect subtle sex-based differences. Most studies were observational in design and therefore subject to selection bias, confounding, and incomplete adjustment for relevant factors such as rehabilitation intensity, psychological readiness, and access to postoperative care. The predominance of level 2 to 5 evidence further constrains interpretation of pooled effect estimates, and statistical significance should therefore be viewed in the context of observational, heterogeneous data. Reporting of graft selection, surgical approach, and rehabilitation protocols was inconsistent and often incomplete. Although random-effects modeling was applied to account for between-study variability, residual heterogeneity remains likely, particularly as our meta-analysis did not stratify by key covariates such as graft type, body mass index, or age, which may have confounded the results. Accordingly, findings should be interpreted with caution and understood as reflecting observed associations rather than causal effects. Despite these limitations, this exploratory meta-analysis provides the most comprehensive synthesis to date examining sex-based disparities in RTS after ACLR.
Conclusion
Female athletes are significantly less likely to RTS after ACLR in the midterm postoperative period, although long-term return rates appear comparable between sexes. Future research should prioritize prospective studies that stratify outcomes by sex, apply standardized definitions of RTS, and assess the impact of targeted rehabilitation and psychological support strategies to promote equitable recovery and optimize RTS outcomes for all athletes.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261448489 – Supplemental material for Are There Sex Disparities in Return to Sport After Anterior Cruciate Ligament Reconstruction? A Systematic Review and Exploratory Meta-analysis
Supplemental material, sj-docx-1-ajs-10.1177_03635465261448489 for Are There Sex Disparities in Return to Sport After Anterior Cruciate Ligament Reconstruction? A Systematic Review and Exploratory Meta-analysis by Darby Amelia Elliott, Saran Singh Gill and Chinmay Madhukar Gupte in The American Journal of Sports Medicine
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.