
Abstract
Background:
Arthroscopy is a commonly performed orthopaedic procedure with postoperative infection risk factors including male sex, tobacco use, and preoperative steroid injections. However, studies focusing on risk factors are limited to single joints with limited numbers of patients; therefore, inconsistencies remain.
Purpose:
To review and analyze predictive risk factors for postarthroscopy infections across arthroscopy of the ankle, knee, hip, shoulder, and elbow.
Study Design:
Systematic review and meta-analysis; Level of evidence, 3.
Methods:
The PubMed, Scopus, and Embase databases were searched using terms related to “arthroscopy” and “infection” to determine risk associated with patient-specific factors. Pooled analysis was conducted using R for smoking, diabetes mellitus (DM), body mass index (BMI) between 30 and 40, BMI >40, intraoperative corticosteroid injection (CSI), and preoperative CSI administration at 2-week intervals up to 8 weeks before operation.
Results:
The search included 1384 studies, of which 125 were determined to meet all inclusion criteria. Postarthroscopic infection risk is significantly increased in patients who had intraoperative intra-articular steroid use (OR, 5.97; 95% CI, 2.66-13.39), steroid use within 2 weeks (OR, 3.36; 95% CI, 2.43-4.65) and 2 to 4 weeks before operation (OR, 1.89; 95% CI, 1.48-2.42), DM (OR, 1.49; 95% CI, 1.24-1.79), BMI of 30 to 40 (OR, 1.29; 95% CI, 1.22-1.37), and BMI >40 (OR, 1.76; 95% CI, 1.41-2.19) and patients who smoked tobacco (OR, 1.59; 95% CI, 1.38-1.83).
The overall risk of infection was 0.84%. Across joints, infection rates varied by procedure type. Knee and hip surgeries demonstrated low weighted mean infection rates (0.61% and 0.59%, respectively), as did shoulder procedures (0.47%). Elbow surgeries had the highest mean infection rate (2.3%), and limited data suggested a low rate for ankle procedures (0.27%).
Conclusion:
Significant increases in postoperative infection risk in patients who underwent arthroscopy of the ankle, knee, hip, shoulder, and elbow were noted with intraoperative intra-articular CSI administration or preoperative CSI administration within 4 weeks of surgery, BMI >30, diabetes, and smoking tobacco. Given the prevalence of these risk factors, patient-specific considerations and interventions should be used to mitigate risk and improve patient outcomes.
Arthroscopy is one of the most common orthopaedic procedures for pathologies of the ankle, knee, hip, shoulder, and elbow. The minimally invasive nature of this intervention minimizes damage to surrounding tissue, allowing for faster recovery times. 33 However, it still poses a risk of complications, including but not limited to deep vein thrombosis, hemorrhage, and surgical site infection (SSI). 28
Previous studies have investigated rates of postarthroscopic infection and identified risk factors related to patient characteristics, comorbidities, and social habits. Specifically, male sex, tobacco use, and preoperative intra-articular steroid injections have been identified as predictors of increased SSI risk after arthroscopy.10,26 Other risk factors explored include diabetes mellitus (DM), tobacco use, and medical comorbidities (eg, arthritis, chronic kidney disease, and hypertension).17,27 Previous studies have focused on a single joint or procedure; however, patient numbers in these studies are limited, and a broader analysis of risk factors for postarthroscopic infections across joints is limited.
Given the lack of consensus in case series on the risk factors associated with infection after arthroscopic procedures and lack of data on risk factors of infection across joints, this systematic review and meta-analysis aimed to better define the risk factors related to postarthroscopic infection in the ankle, knee, hip, shoulder, and elbow.
Methods
Literature Search and Study Selection
Between May 15, 2025, and June 29, 2025, 3 reviewers (A.S., S.I. and E.N.B.) performed a literature search in 3 online databases (PubMed, Embase, and Scopus) to identify studies that specifically reported or investigated postsurgical infection in the form of SSI, septic arthritis, or subsequent surgery for infection. Search terms included “arthroscopy” or “endoarthoscopy” and “surgical wound infection” or “post operative infection.” Full search criteria can be found in Appendix A (available online). Covidence (2025) was utilized to identify literature reporting risk factors for postarthroscopic infections. 34 The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed for study selection. 4
Inclusion criteria consisted of case-control, cross-sectional, prospective, and retrospective cohort studies, or randomized controlled trials that reported exposure or intervention factors that contributed to SSIs after joint (knee, shoulder, hip, ankle, or elbow) arthroscopy. Studies were excluded if they were not available in the English language, were published before 1912, used animal models, or consisted of other modalities of surgery within 2 weeks. Case reports, reviews, expert opinions, meta-analyses, or meeting reports were also excluded, as well as studies with insufficient experimental data.
Two independent reviewers screened the full titles, abstracts, and full manuscripts. A senior reviewer (E.N.B.) served as a tiebreaker for all conflicts. The literature search yielded 1384 initial publications. Of the 1384 publications initially identified, 125 were ultimately determined to fit all inclusion criteria and can be found in Appendix B (available online).
Study Quality Assessment
Quality assessment of studies included for review was completed using the Methodological Index for Non-Randomized Studies. 30 Based on these criteria, noncomparative studies can receive a maximum score of 16, while comparative studies can receive a maximum score of 24. Study quality was assessed as follows: for noncomparative studies, a score of 0 to 4 was considered very low quality; 5 to 7, low quality; 8 to 12, fair quality; and ≥13, high quality. For comparative studies, 0 to 6 was considered very low quality; 7 to 10, low quality; 11 to 15, fair quality; 16 to 20, good quality, and ≥21, high quality.
Data Extraction
For all studies, data regarding the author, year of publication, location of research, study design, level of evidence, and size of patient cohort were recorded. Additional data recorded included mean age of the cohort, percent female sex, size of experimental and control groups, joint(s) operated on, all independent and dependent variables noted, and patient outcomes. Independent variables of interest were perioperative corticosteroid injection (CSI), perioperative glycemic control, smoking history, age, and body mass index (BMI). Additional variables we analyzed included adjunct procedures such as magnetic resonance arthropathy (MRA), surgical technique, antibiotic prophylaxis, preoperative soaking of grafts in antibiotics, and use of autografts versus allografts.
Statistical Analysis
Pooled analysis was conducted for risk factors with at least 4 analyzable effects using inverse variance weighting with a fixed-effects model for studies with heterogeneity <50% and a random-effects model for those with heterogeneity >50%. Because of the limited number of papers with fully available population statistics, variance was estimated using 95% confidence intervals. Pooled analysis was conducted for smoking history, DM, BMI between 30 and 40, BMI >40, intraoperative steroid use, and preoperative steroid use at 2-week intervals up to 8 weeks before operation. All data analyses were performed using R (Version 4.5.1). Pooled analyses were calculated using the meta package (Version 8.2-1). 3
Results
This analysis draws from approximately 70 distinct study entries listed in the provided data set. These studies span a range of procedures and anatomic sites. The postoperative infection rates vary by body part and context. These infection rates were stratified by joint as well as risk factor and are summarized in Table 1.
Postarthroscopic Infection Rates by Risk Factor and Joint a
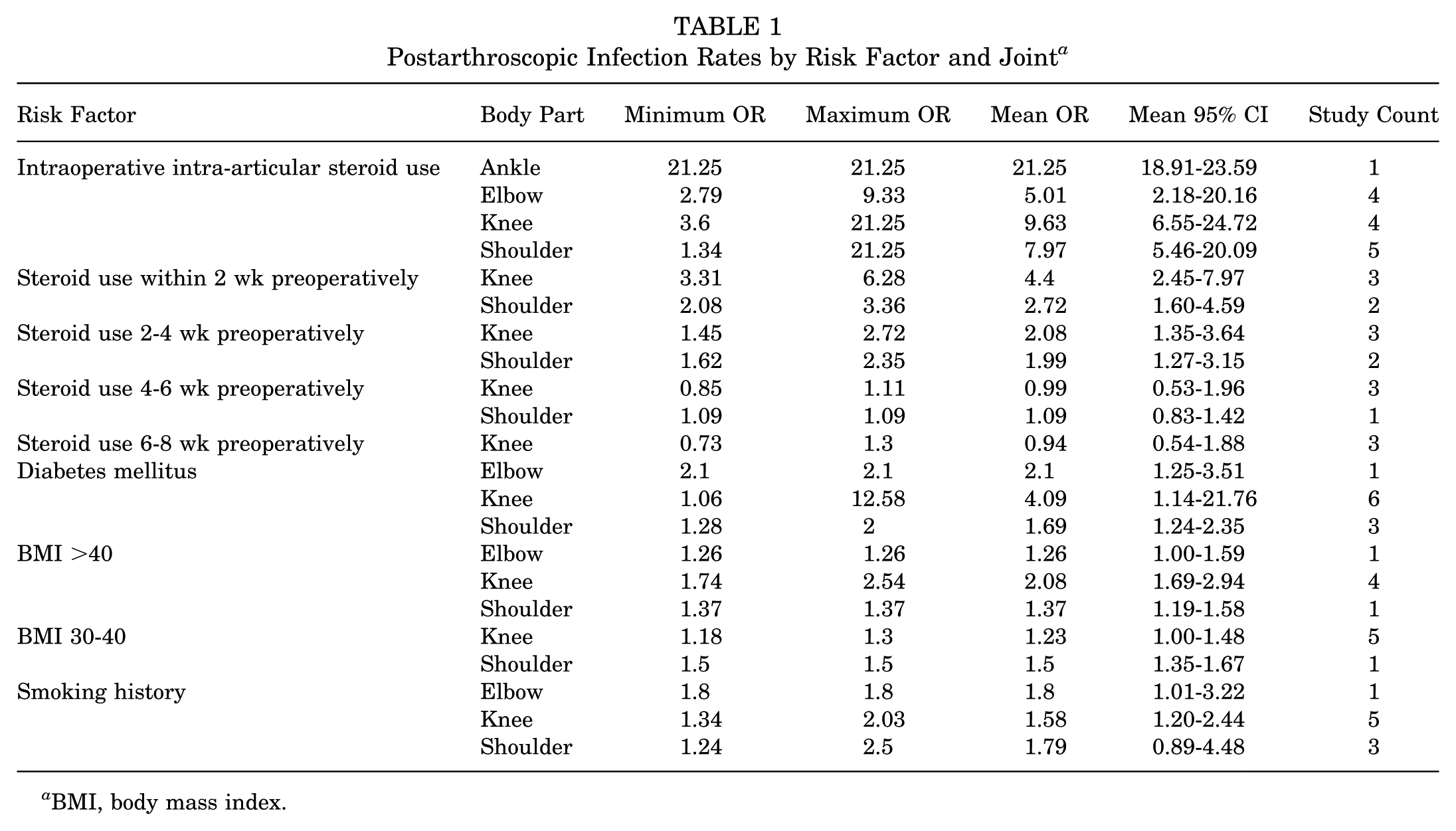
BMI, body mass index.
Knee procedures are the most extensively represented, with infection rates ranging from 0.15% to 2.47%, with most studies clustering around 0.3% to 0.9%. After weighting by participant count, the mean infection rate for knee surgeries was 0.61%. Shoulder procedures showed a broader range, from 0.11% to 3.5%, although most large studies reported rates <1%. The weighted mean infection rate for shoulder surgeries was 0.47%. Hip procedures generally reported low infection rates, between 0.21% and 1.12%. The weighted mean for hip surgeries was 0.59%. Elbow surgeries, although less common, show higher infection rates, ranging from 1.55% to 8.9%. This resulted in a weighted mean of 2.3%. Ankle procedures are represented by limited data, with 1 study reporting a rate of 0.27%. When combining all joints with available infection rates and participant counts, the overall weighted mean infection rate across joint procedures was 0.84%.
Corticosteroid Injections
Intraoperative Steroid Use
Patients receiving intraoperative intra-articular CSI demonstrated a markedly increased risk of postarthroscopic infection. The pooled odds ratio across 5 studies was 5.97 (95% CI, 2.66-13.39), with substantial heterogeneity (I2 = 98.2%; P < .001). Despite the wide variability between studies, all estimates were consistently elevated above unity, indicating a robust positive association (Figure 1A, Table 2).
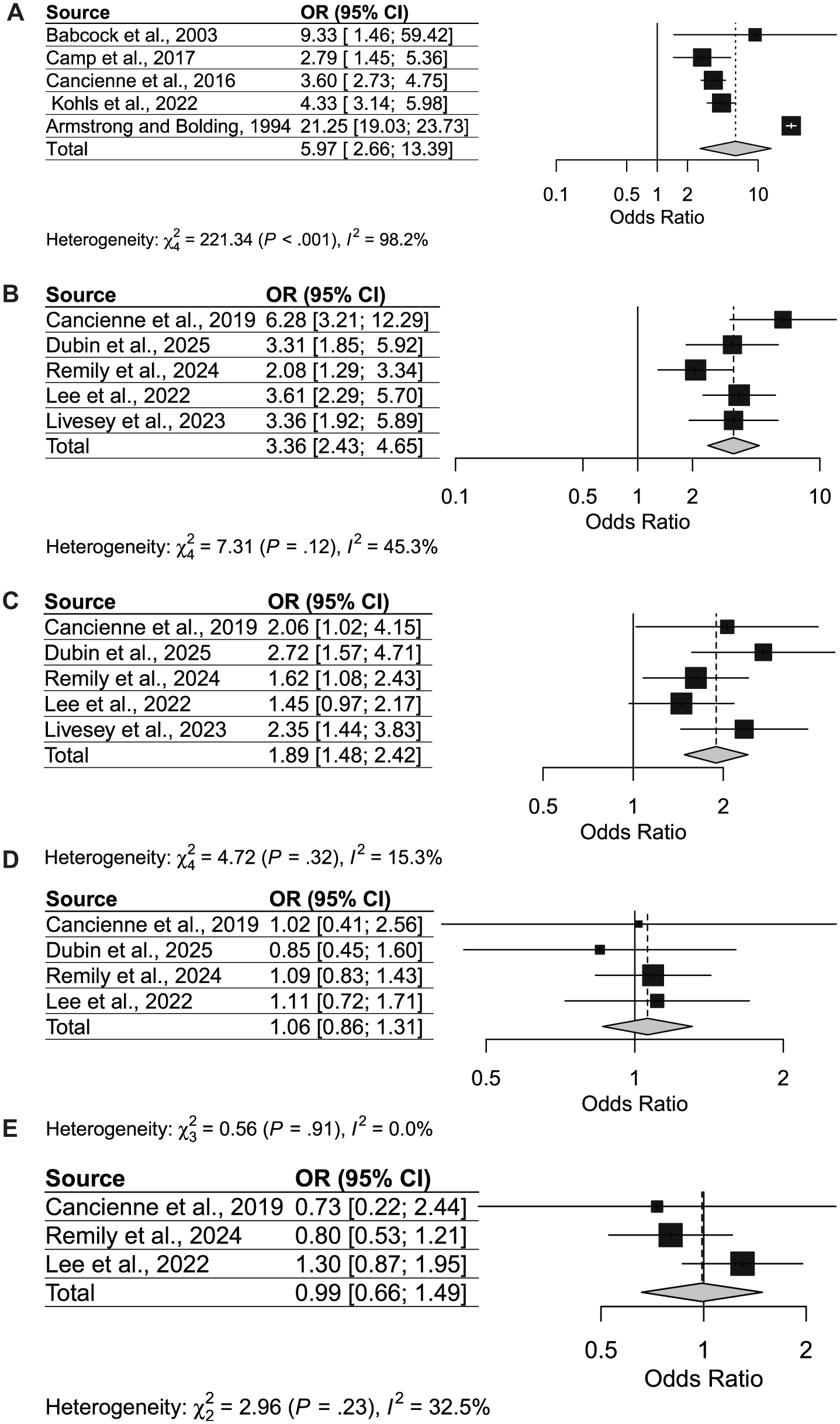
(A) Forest plot of infection risk in patients receiving intraoperative steroids. (B) Forest plot of infection risk in patients receiving steroids 2 weeks before arthroscopy. (C) Forest plot of infection risk in patients receiving steroids between 2 and 4 weeks before arthroscopy. (D) Forest plot of infection risk in patients receiving steroids between 4 and 6 weeks before arthroscopy. (E) Forest plot of infection risk in patients receiving steroids between 6 and 8 weeks before arthroscopy.
Change in Postarthroscopic Infection Rate by Risk Factor a
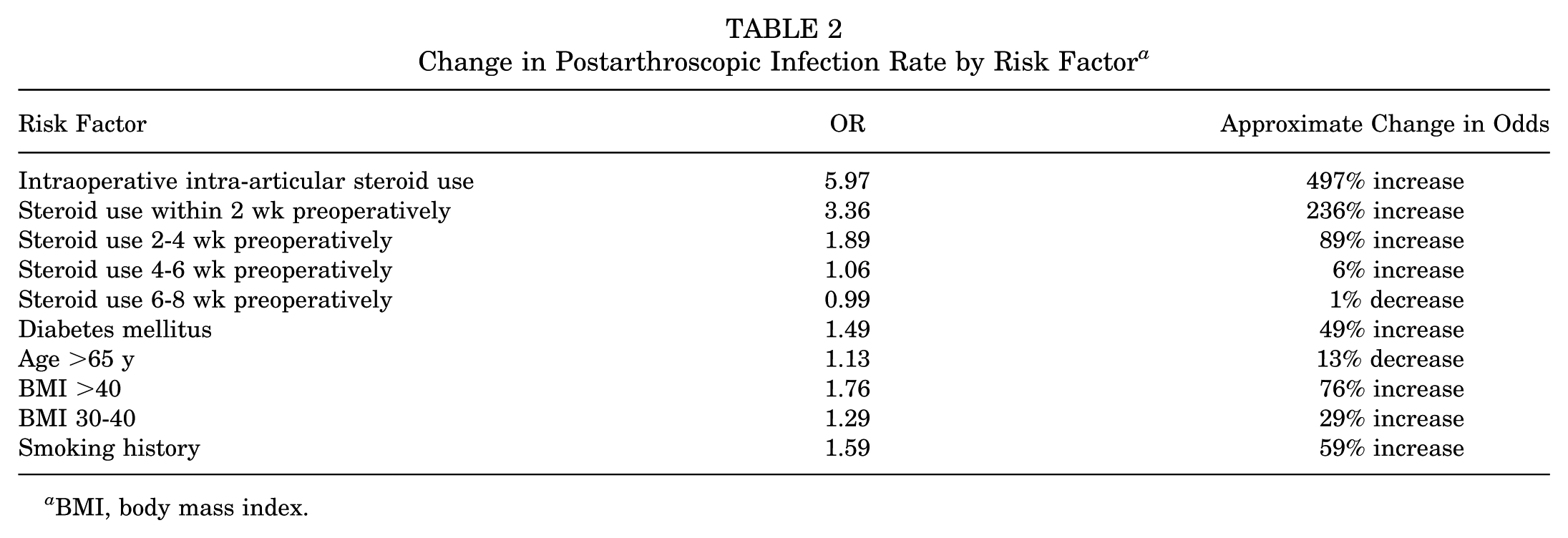
BMI, body mass index.
Steroid Use Within 2 Weeks Preoperatively
Analysis of 5 studies showed that intra-articular CSI use within 2 weeks before arthroscopy was associated with a significantly higher risk of infection (pooled OR, 3.36; 95% CI, 2.43-4.65). Heterogeneity was moderate (I2 = 45.3%; P = .12). All individual study estimates demonstrated increased risk, supporting a consistent effect during this perioperative window (Figure 1B, Table 2).
Steroid Use 2 to 4 Weeks Preoperatively
Intra-articular CSI use 2 to 4 weeks before arthroscopy also conferred an elevated infection risk (pooled OR, 1.89; 95% CI, 1.48-2.42), based on 5 studies. Heterogeneity was low (I2 = 15.3%; P = .32). Most studies demonstrated odds ratios >1, suggesting a diminishing but still significant risk effect as the interval between steroid exposure and surgery lengthens (Figure 1C, Table 2).
Steroid Use 4 to 6 Weeks Preoperatively
When steroids were administered 4 to 6 weeks before arthroscopy, no significant association with infection risk was detected (pooled OR, 1.06; 95% CI, 0.86-1.31). Heterogeneity was negligible (I2 = 0.0%; P = .91). Individual study estimates clustered closely around the null, indicating that infection risk was not meaningfully increased at this interval (Figure 1D, Table 2).
Steroid Use 6 to 8 Weeks Preoperatively
Similarly, steroid administration 6 to 8 weeks before surgery was not associated with higher infection risk (pooled OR, 0.99; 95% CI, 0.66-1.49). Heterogeneity was low (I2 = 32.5%; P = .23). Point estimates varied, but the pooled result was essentially null (Figure 1E, Table 2).
Postoperative and Chronic Steroid Use
One study investigated infection rates after arthroscopic rotator cuff repair, debridement, or subacromial decompression in private payers and Medicare national insurance databases who received CSIs 1 month, 2 months, 3 months, and 4 months postsurgery. 14 The study found that patients who received a CSI within 1 month was the only group that had a significantly higher rate of postoperative infections (private payer: OR, 2.63; P = .014; Medicare: OR, 11.2; P < .0001). Another study found that patients with chronic steroid use did not have significantly higher rates of postoperative superficial (P = .998), deep (P = .999), or organ space (P = .206) SSI or sepsis (P = .415). 9 However, these patients did have a higher rate of mortality within 30 days after arthroscopic rotator cuff repair (OR, 8.15; 95% CI, 1.45-45.86; P = .017).
Diabetes Mellitus
Ten studies assessed diabetes as a risk factor for postarthroscopic infection. All studies defined DM as hemoglobin A1c (HbA1c) >8. Several large database studies reported consistent, statistically significant associations, while a few smaller clinical studies demonstrated wider confidence intervals but maintained the same direction of effect. The pooled analysis demonstrated a significant increase in postoperative infection risk among patients with diabetes (OR, 1.49; 95% CI, 1.24-1.79). Heterogeneity was high (I2 = 78.9%; P < .001), indicating variability across data sets; however, the overall association remained strong (Figure 2, Table 2).
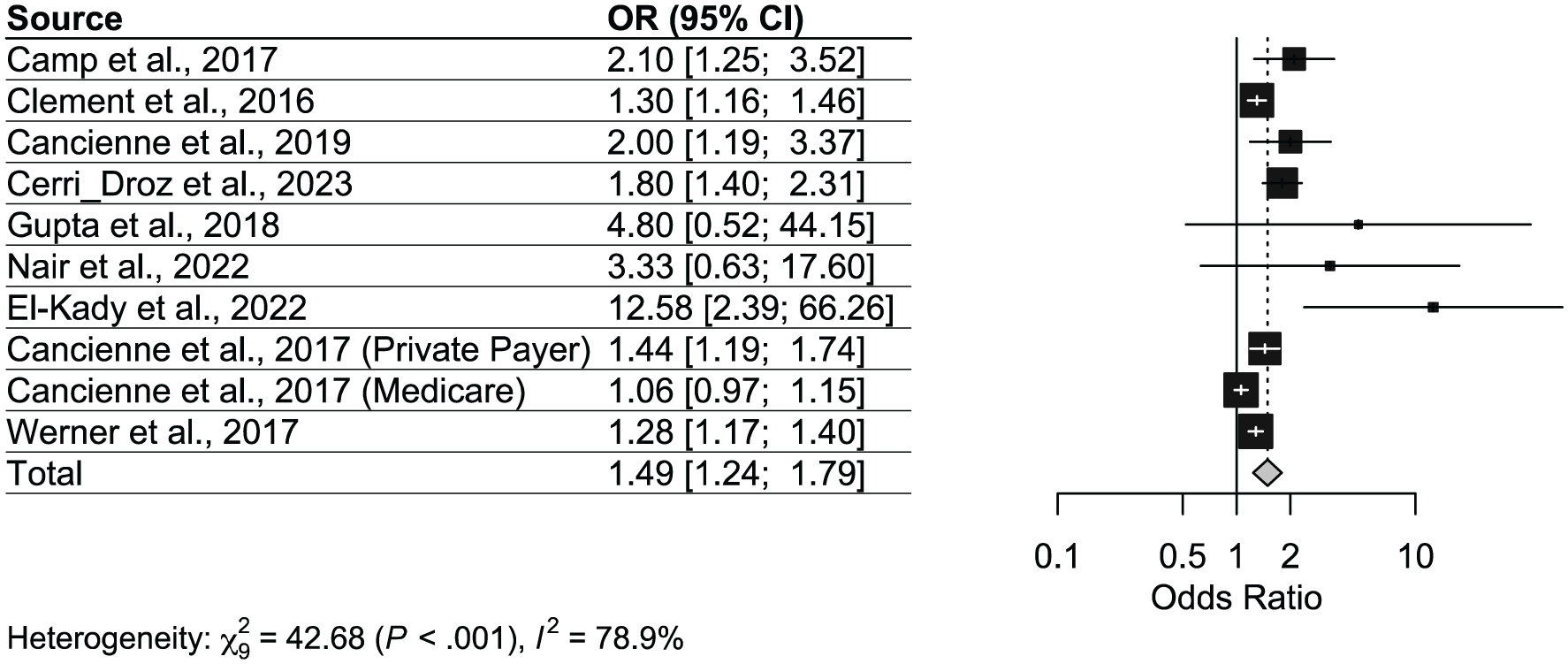
Forest plot for postarthroscopic infection risk odds ratios in patients with diabetes mellitus.
Studies have also investigated insulin dependence and the risk of postarthroscopic infection. One study linked insulin-dependent DM with a significantly increased risk of surgical complications (OR, 2.19; 95% CI, 1.226-1.157), including deep infections (OR, 3.08; 95% CI, 1.753-5.419), return to the operating room (OR, 1.93; 95% CI, 1.28-2.919), and unplanned hospital admission (OR, 1.77; 95% CI, 1.289-2.431). 32 In contrast, a different study found non–insulin-dependent DM as an independent risk factor for sepsis (OR, 2.77; 95% CI, 1.01-7.58; P = .047), while insulin-dependent DM was not (P = .172). 7
Another study associated glucagon-like peptide-1 (GLP-1) agonist (semaglutide) use in patients with type 2 DM with decreased rates of SSI (OR, 2.22; P = .049), venous thromboembolism (OR, 3.10; P < .001), sepsis (OR, 3.87; P < .001), and cardiac events (OR, 3.96; P < .001), as well as decreased rates of urinary tract infection (OR, 3.27), pneumonia (OR, 3.88), acute kidney injury (OR, 3.91), and emergency department visits (OR, 2.51) (P < .001 for all) after arthroscopic rotator cuff repair, compared with patients with diabetes who did not use semaglutides. 27 Patients who used semaglutides also had a lower 2-year retear rate (P < .001).
Tobacco Use
Across 9 included studies, tobacco users were consistently associated with higher odds of postarthroscopic infection. Individual study estimates ranged from odds ratios of 1.24 to 2.50, with several large database studies demonstrating statistically significant effects. Although some smaller studies reported wide confidence intervals crossing the null, the overall direction of effect favored an increased risk among tobacco users (Figure 3, Table 2).
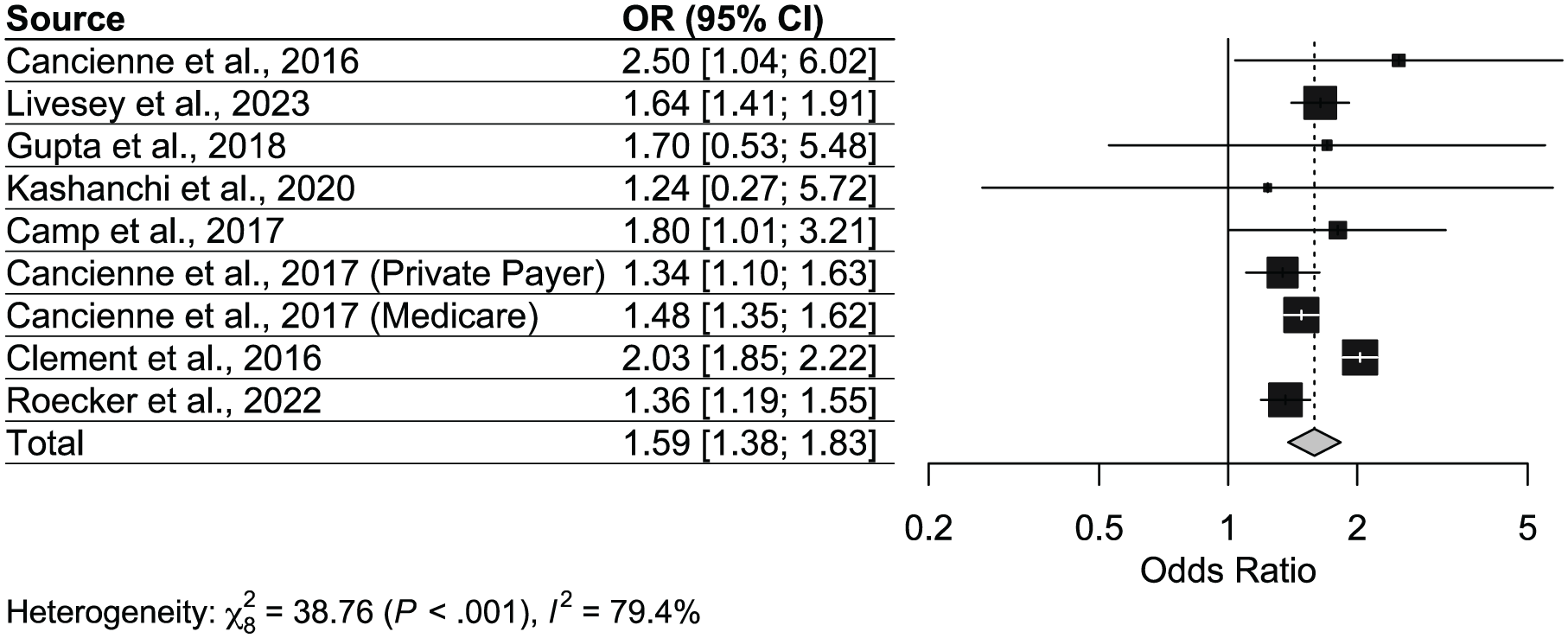
Forest plot for postarthroscopic infection risk odds ratios in patients who use tobacco.
The pooled analysis yielded a statistically significant association between tobacco use and infection risk (OR, 1.59; 95% CI, 1.38-1.83), indicating that tobacco users had approximately 60% higher odds of developing postoperative infection after arthroscopy compared to non–tobacco users. Heterogeneity across studies was substantial (χ2 = 38.76; P < .001; I2 = 79.4%), reflecting variability in study populations and data sources.
Age
Three studies with 4 analyzable effects evaluated whether age >65 years was associated with an increased risk of postarthroscopic infection. One study provided odds ratios with respect to patients <65 years; therefore, the reciprocal was calculated to maintain consistency. The pooled odds ratio was 1.13 (95% CI, 0.67-1.90), indicating no statistically significant association. However, there was substantial heterogeneity (I2 = 97.9%; P < .001) (Figure 4, Table 2).
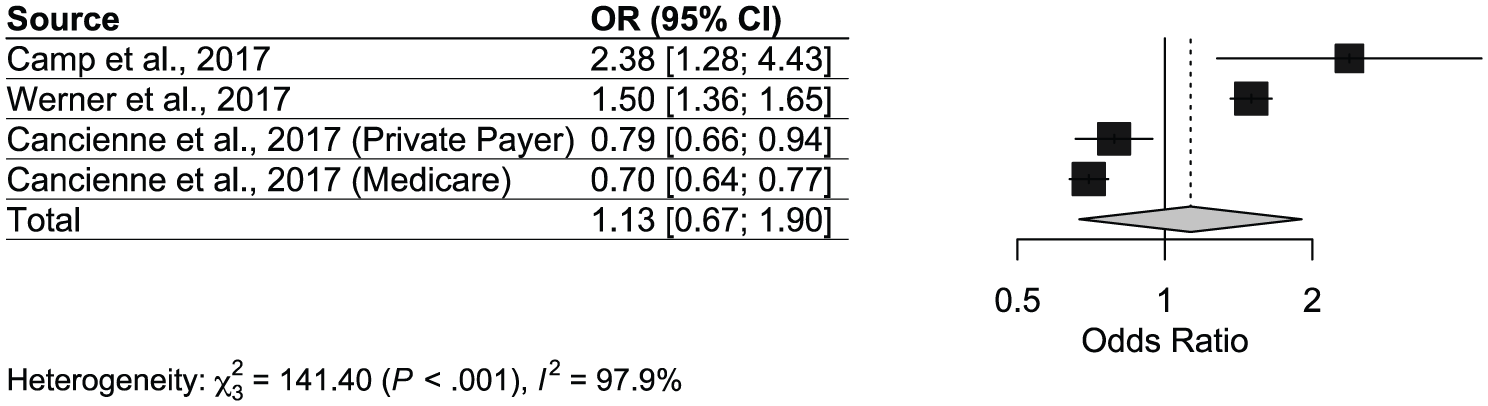
Forest plot for postarthroscopic infection risk odds ratios in patients >65 years of age.
Individual study findings were inconsistent. One large data set study found old age had protective or neutral effects on postoperative infection rates in 2 independent populations (OR, 0.79; 95% CI, 0.66-0.94; and OR, 0.70; 95% CI, 0.64-0.77), 6 while others indicated increased risk (OR, 2.38; 95% CI, 1.28-4.43 5 ; and OR, 1.50; 95% CI, 1.36-1.65 23 ). This variability explains the high heterogeneity and suggests that the relationship between age and infection risk may be influenced by study design, population differences, or confounding factors.
BMI
BMI 30 to 40 (Obese)
Across 6 studies, patients with BMI between 30 and 40 had a modest but statistically significant increased risk of infection compared with nonobese patients. The pooled OR was 1.29 (95% CI, 1.22-1.37). Heterogeneity was moderate (I2 = 58.3%; P = .04). Most individual studies reported effect sizes above unity, with odds ratios ranging from 1.18 to 1.50, indicating a consistent signal that obesity confers additional risk (Figure 5A, Table 2).
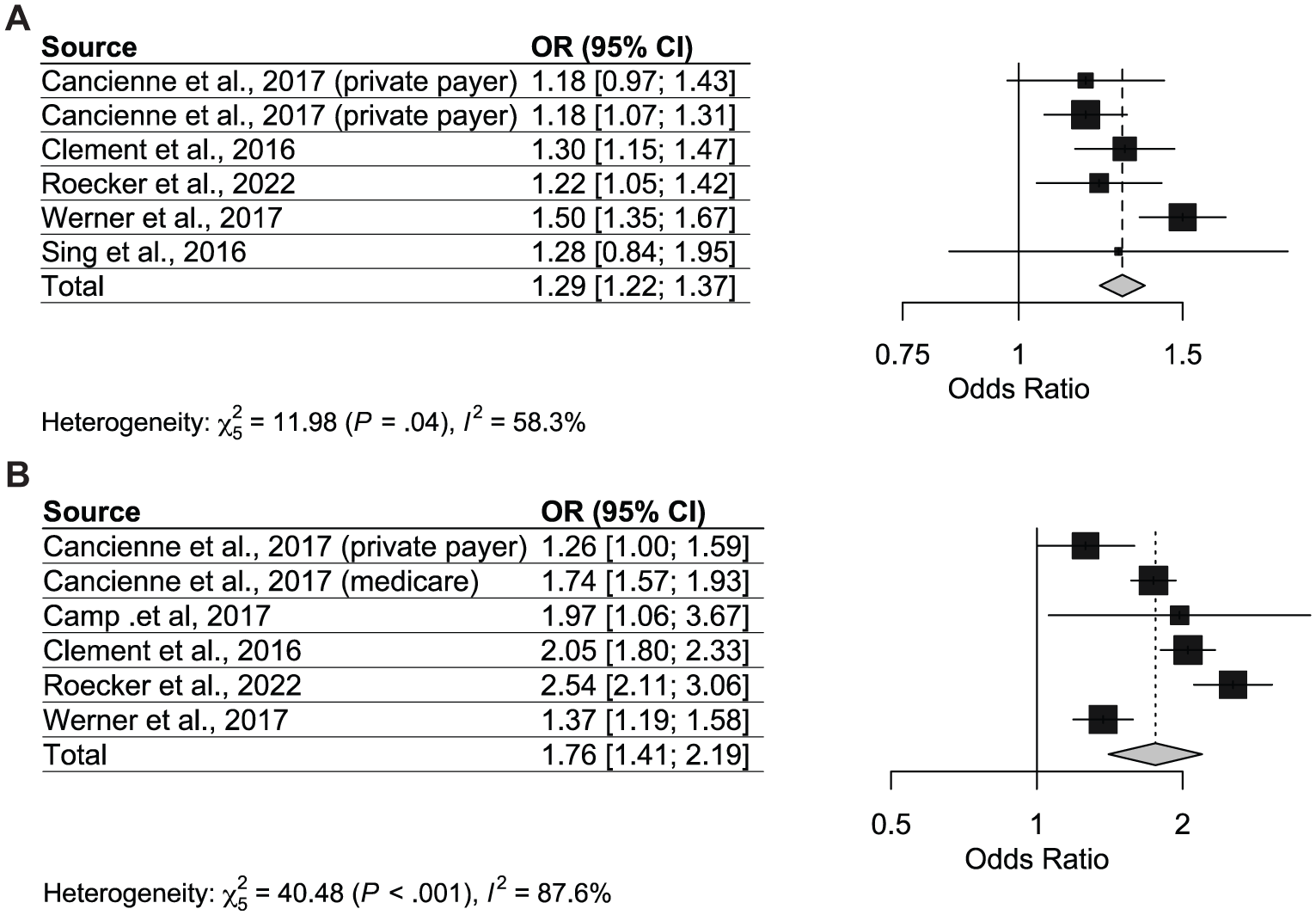
(A) Forest plot for postarthroscopic infection risk odds ratios in patients with BMI between 30 and 40. (B) Forest plot for postarthroscopic infection risk odds ratios in patients with BMI >40.
BMI >40 (Morbidly Obese)
Patients with BMI >40 demonstrated a substantially greater infection risk. The pooled OR across 6 studies was 1.76 (95% CI, 1.41-2.19), with high heterogeneity (I2 = 87.6%; P < .001). Individual study estimates varied from 1.26 to 2.54, but all indicated a positive association. The magnitude of risk was consistently higher than that observed for patients with a BMI of 30 to 40 (Figure 5B, Table 2).
Sex
Across studies, male sex generally increased the risk of postoperative infection, although the magnitude varies by procedure and data set. After anterior cruciate ligament (ACL) reconstruction, men had 58% higher odds of infection within 6 months (OR, 1.58; 95% CI, 1.43-1.75; P < .001). 25 In population data on knee arthroscopy requiring reoperation, adult men were infected nearly twice as often as women and boys nearly 3 times as often as girls (both P < .001). 35 Several shoulder cohorts also suggested higher male risk: 1 case-control study found that male sex strongly was associated with acute infection after rotator cuff repair (OR, 9.52; P = .042), and Cutibacterium acnes was more common in men. 22 Interestingly, however, other large population studies reported no sex difference in overall infection incidence. Taken together, male sex is a consistent risk factor in many arthroscopic procedures, but the effect is not universal; procedure type, organism profile, and co–risk factors likely modify the association.
Other Risk Factors
In addition to aforementioned risk factors, studies also identified chronic conditions like arthritis, chronic kidney disease, dialysis, hypertension, anemia, and alcohol use as significant risk factors for postarthroscopic infection. Sports played also contributed to an elevated risk, with summer sports such as soccer having a higher incidence of postarthroscopic ACL reconstruction risk than winter sports such as skiing (P = .02). 16 One study found that patients with mild, moderate, and severe anemia had a significantly higher rate of all complications, including sepsis-related complications, after shoulder arthroscopy (OR, 4.76; P = .004). 15
Operative factors such as adjunct procedures (eg, MRA), technique used, and preoperative or intraoperative antibiotic prophylaxis were also found to modify infection risk. One study found a significantly increased rate of infection in patients who underwent MRA or CSI within 2 weeks of surgery but found an increased rate of infection only in patients who underwent CSI within 2 to 4 weeks of surgery. 18 Another study found that gentamicin presoaking of hamstring autografts during ACL reconstruction had no significant difference in superficial infection rates but did result in decreased deep intra-articular infection rates (P = .004). 20 A different study found no significant difference in infection risk when performing ACL reconstructions using autografts and allografts (OR, 1.83; 95% CI, 0.16-12.94; P = .765). 13
Discussion
This systematic review and meta-analysis of infection related to arthroscopy demonstrated that patients who used steroids intra-articularly within 4 weeks of arthroscopy, patients with diabetes, those who smoke, and those with a BMI >30 have a significantly increased risk of postarthroscopic infection. Increasing age was not associated with an increased risk of infection. Additionally, male sex was a consistent risk factor in many arthroscopic procedures, but the effect varied, with procedure type, organism profile, and comorbid risk factors likely modifying the association. These findings may be valuable in counseling patients, addressing potentially modifiable risk factors before surgery, and risk stratification for improved postoperative planning.
Regarding steroid injections, we noted a time-dependent risk, with patients receiving injections intraoperatively at the highest risk, with a continued elevated risk up to 4 weeks before arthroscopy. However, beyond 4 weeks, no significant association with infection risk was found. Postoperatively, 1 study found that patients who received a CSI up to 1 month after surgery had higher infection rates, but not those who received a CSI beyond this time. Another study found that patients with chronic steroid use did not have significantly higher rates of postarthroscopic infection but did have a higher rate of mortality within 30 days. These findings are in concordance with official guidelines adopted by the American Academy of Orthopaedic Surgeons. 2 While these guidelines do not explicitly state a minimum duration between intra-articular steroid injection and surgery, other studies recommend a minimum of 2 months to prevent SSI. 10 However, our results indicate a low risk of infection with as little as 1 month between injection and surgery, although other risk factors must be considered as well.
Medical comorbidities may also place a patient at risk. Patients with a BMI between 30 and 40 had a modest increase in risk, with patients with a BMI >40 demonstrating a remarkably increased risk of postoperative infection risk. The correlation between BMI and SSI has been well established in prior literature, possibly due to a variety of factors, such as increased risk of soft tissue injury, postoperative fat liquefication, or changes in collagen structure.19,24 While a prior meta-analysis also found that obesity was a risk factor in the development of SSI after knee arthroscopy, the study did not delineate between a BMI of 30 and 40 and a BMI >40. 17 Our finding that there is a robust difference between these 2 BMI categories supports separate analysis of these groups in the future and risk stratification along these lines.
Similarly, patients with an HbA1c >8 or perioperative evidence of poor glycemic control showed increased postoperative infection rates. This finding is consistent with other review studies that also found that DM is associated with an increased risk of SSIs across multiple types of surgery with glycemic control as an independent risk factor for the development of SSI.1,36 While preoperative glycemic control is crucial in the prevention of SSI, another review study in cardiovascular surgery indicated that tight glycemic control in the perioperative period via the use of continuous insulin infusions was also key in decreasing SSIs. Additionally, 1 study regarding the use of GLP-1 agonists (semaglutide) found a decrease in SSIs, in line with prior reviews. 8 Interestingly, we found mixed results regarding differences in SSIs between insulin-dependent DM and non–insulin-dependent DM, indicating further study is warranted.
Additionally, tobacco use was associated with approximately 60% higher odds of postoperative infection compared to non–tobacco users. Although most studies included cigarette and non-cigarette tobacco use, 3 studies specified inclusion of only cigarette smokers.11,12,18 This finding is in line with other studies that indicate current smoking is associated with SSI in various types of surgery.21,29 Tobacco use represents a modifiable risk factor, and patient counseling before surgery is an opportunity to decrease the risk of SSI. Interestingly, smoking on the same day of surgery is independently associated with an increased risk of SSI in elective surgery. 21 Furthermore, a randomized controlled trial regarding abstinence from smoking found a significant difference in SSIs between patients who continued smoking before surgical incisions and those who abstained from smoking for 4 weeks. 31 While this has not been studied in arthroscopy, it represents an area for further research and potential counseling.
One study analyzed data from 4801 patients in the ACL registry of the FIFA Medical Centre of Excellence Regensburg who had undergone surgical ACL repairs over a 5-year period. This study was the first to report that soccer players had a significantly higher infection rate than skiers (P = .02). 16 Additional studies between sport-specific differences in infection rate such as gear used, time of year the sport is played, and practice conditions can help identify factors that may contribute to this discrepancy and help establish risk factors that we can then work to mitigate.
One study also discussed elevated rates of infection in patients with anemia, while another found that preoperative MRA increased infection rates in a more limited way than CSI. One study noted a decrease in deep intra-articular infection rates with gentamicin presoaking of hamstring autografts during ACL reconstruction, while another found no significant difference with the use of allografts and autografts for the same procedure. Each of these studies highlights a unique risk factor that can be corrected, for example, by ensuring anemia management preoperatively, soaking grafts in antibiotics, and substituting autografts for allografts when needed. More studies are required to further substantiate these findings and offer actionable ways to improve postarthroscopic infection risk.
While several prior systematic reviews have examined infection risk after arthroscopy of individual joints, to our knowledge, this is the first comprehensive review to assess infection risk factors across multiple large joints—ankle, knee, hip, shoulder, and elbow—using consistent criteria. This broader scope allows for a more generalized understanding of risk factors that apply across joint types, offering greater utility for perioperative planning. Our study also incorporates more recent data and offers a more detailed breakdown of risk associated with timing of steroid injections, BMI thresholds, and glycemic control.
These findings underscore the importance of preoperative risk stratification and patient optimization. Identifying high-risk patients, such as those with poorly controlled diabetes, recent CSIs, morbid obesity, or who smoke, can inform management strategies. These may include enhanced preoperative counseling, consideration of prophylactic antibiotics, extended postoperative monitoring, and targeted follow-up protocols to reduce infection risk and improve outcomes.
Limitations
This study must be considered in the context of its limitations. Many of the included studies were retrospective in design, and heterogeneity among study methodologies limited the ability to synthesize data quantitatively. In addition, exclusion of non–English-language studies may have introduced selection bias and contributed to an overrepresentation of North American and European populations. Furthermore, this study was limited by the amount of available data for SSIs of specific joint types and risk factors that were too small for further analysis. The overall quality of our findings is inherently linked to the quality of the studies included.
Conclusion
Significant increases in postoperative infection risk in patients who underwent arthroscopy of the ankle, knee, hip, shoulder, and elbow were noted with intraoperative intra-articular CSI administration or preoperative CSI administration within 4 weeks of surgery, BMI >30, diabetes, and smoking tobacco. Given the prevalence of these risk factors, patient-specific considerations and interventions should be used to mitigate risk and improve patient outcomes.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465261429468 – Supplemental material for Risk Factors for Infection After Ankle, Knee, Hip, Shoulder, or Elbow Arthroscopy: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-ajs-10.1177_03635465261429468 for Risk Factors for Infection After Ankle, Knee, Hip, Shoulder, or Elbow Arthroscopy: A Systematic Review and Meta-analysis by Anouska Saraf, Sage Iwamoto, Sakshi Krishna, Vincent G. Young and Eric N. Bowman in The American Journal of Sports Medicine
Supplemental Material
sj-pdf-2-ajs-10.1177_03635465261429468 – Supplemental material for Risk Factors for Infection After Ankle, Knee, Hip, Shoulder, or Elbow Arthroscopy: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-2-ajs-10.1177_03635465261429468 for Risk Factors for Infection After Ankle, Knee, Hip, Shoulder, or Elbow Arthroscopy: A Systematic Review and Meta-analysis by Anouska Saraf, Sage Iwamoto, Sakshi Krishna, Vincent G. Young and Eric N. Bowman in The American Journal of Sports Medicine
Footnotes
Submitted November 6, 2025; accepted January 29, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.