
Abstract
Background:
Approximately 55% of individuals return to previous sports levels after anterior cruciate ligament (ACL) reconstruction (ACLR), but the duration of their sporting life post-ACLR and how this differs from uninjured sports participants is unknown.
Purpose:
To trace the 25-year trajectory of sports participation in individuals who have undergone ACLR and compare sporting activity between graft types and between ACLR individuals and uninjured controls.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 62 individuals (44 males; mean age, 27 years) underwent ACLR (31 bone–patellar tendon–bone grafting, 31 semitendinosus/gracilis grafting). Sporting activity was assessed preinjury, at 6 and 25 years after surgery on a 6-point scale based on pivoting demands. A total of 30 uninjured individuals matched for age, sex, and sporting activity were assessed at equivalent time points. Pearson chi-square and Student t tests were used to compare outcomes between graft types and between ACLR individuals and controls.
Results:
In total, 50 (81%) individuals (35 males) with ACLR and 20 (67%) uninjured controls were followed up after 25 years. Overall, 88% of the ACLR group were active in sports, 22% in vigorous pivoting sports. Three ACLR individuals had total knee replacements, 9 ruptured their contralateral ACL, and 8 ruptured their graft. There was no significant difference between graft types in sports level played presurgery (P = .442), 6 years after surgery (P = .511), or 25 years after surgery (P = .100). At 25 years after surgery, ACLR individuals participated in sports at higher levels (P = .005) and over longer periods (P = .032) than controls.
Conclusion:
Interestingly, after ACLR, patients were more engaged in sports than uninjured controls. Although the level of sports activity typically decreased over 25 years, findings highlight the potential for longevity in sports after an ACLR, irrespective of graft type.
Individuals who have sustained an anterior cruciate ligament (ACL) injury often describe returning to sports as a primary reason for choosing ACL reconstruction (ACLR) with postoperative rehabilitation over rehabilitation alone. However, according to 1 systematic review and meta-analysis, only 55% of those who undergo ACLR return to their preinjury level of sports. 1
Evidence of post-ACLR sports participation is clouded by inconsistencies in the definition of sports level between different measures.15,19,22 For example, return-to-sports (RTS) measures have been defined variably as return to either preinjury sports, competitive sports, pivoting sports, or overall sports activity, or according to the Knee injury and Osteoarthritis Outcome Score (KOOS) Sport and Recreation sub-score or the mean Tegner score. 19 In addition, as highlighted by Lindanger et al, 22 some measures do not necessarily capture the extra challenges posed by competitive levels of sports participation, which include higher speeds over greater distances and increased accelerations and decelerations, 29 while others incorporate work and other nonsporting factors into their classification. 32 Regardless, it is a common belief among researchers and clinicians that ACL injury will limit long-term participation in sports, even if the ACL is reconstructed.3,12,22,23,26,31
Numerous studies have assessed sports participation after ACLR, with follow-up times ranging from 1 to 10 years.3,7,13,21,23-25,33 Rates of RTS varied depending on age, elite levels, and measure used. 19 Fewer studies have followed outcomes up to 20 years,11,26,30,31 and of four 25-year follow-up studies,6,10,22,34 only 1 has investigated sports participation specifically. 22 Yet, for the young driven athlete, valid information regarding RTS and the ability to maintain sports participation over the very long term is crucial.
Considering the lack of clarity of a universal definition of post-ACLR RTS and the paucity of long-term outcome data, further research is needed to help inform patients and the health professionals they engage. This prospective study aimed first to trace the trajectory of sports participation in individuals who had undergone ACLR from preinjury, at 6 years after surgery, and at 25 years after surgery. The second aim was to compare sporting activity, including the level and duration of sports, between individuals who had undergone patellar tendon and hamstring grafting. The third aim was to compare sporting activity, including the level and duration of sports, in individuals who had undergone ACLR to a control group of noninjured participants matched prospectively over the same time frame. This study hypothesized that (1) sports participation would decline with time after ACLR, (2) sports participation would be similar between the 2 graft types, and (3) the ACLR and control groups would compare similarly at baseline, but the control group would report higher sporting levels and longevity in sports at the 6- and 25-year follow-ups.
Methods
Study Design
This prospective longitudinal cohort study traces sports involvement from preinjury to 25 years after surgery in 62 individuals who underwent ACLR, in comparison with 30 healthy uninjured individuals over matching time frames. Ethical clearance was granted by The University of Queensland Human Ethics Committee, Australia (2020000921), and all participants provided written informed consent.
Study Population
A total of 62 individuals (44 males; mean age, 27 years; SD, 5.9 years) were recruited from a cohort of 113 patients who were referred to a physical therapy clinic after their ACL injury and underwent ACLR between late 1995 and 1998 (Figure 1). Inclusion criteria for the cohort were unilateral ACL injury, a positive pivot-shift test, a functionally unstable knee, no concomitant ligamentous injuries, and age <40 years. Cohort participants were assessed preoperatively and at 6 years and 25 years after surgery. Individuals with meniscal repairs and with preexisting osteoarthritis (OA) were excluded presurgery. The mean time between ACL injury and surgery was 35 months (SD, 38 months). Of the 62 individuals, 31 underwent bone–patellar tendon–bone (BPTB) grafting and 31 underwent hamstring grafting using semitendinosus/gracilis (STG). In total, 37 individuals had a concurrent meniscectomy and 14 had articular cartilage damage. All participants remained subjectively unstable after a 6-week preoperative physical therapy program, which has been described previously. 18
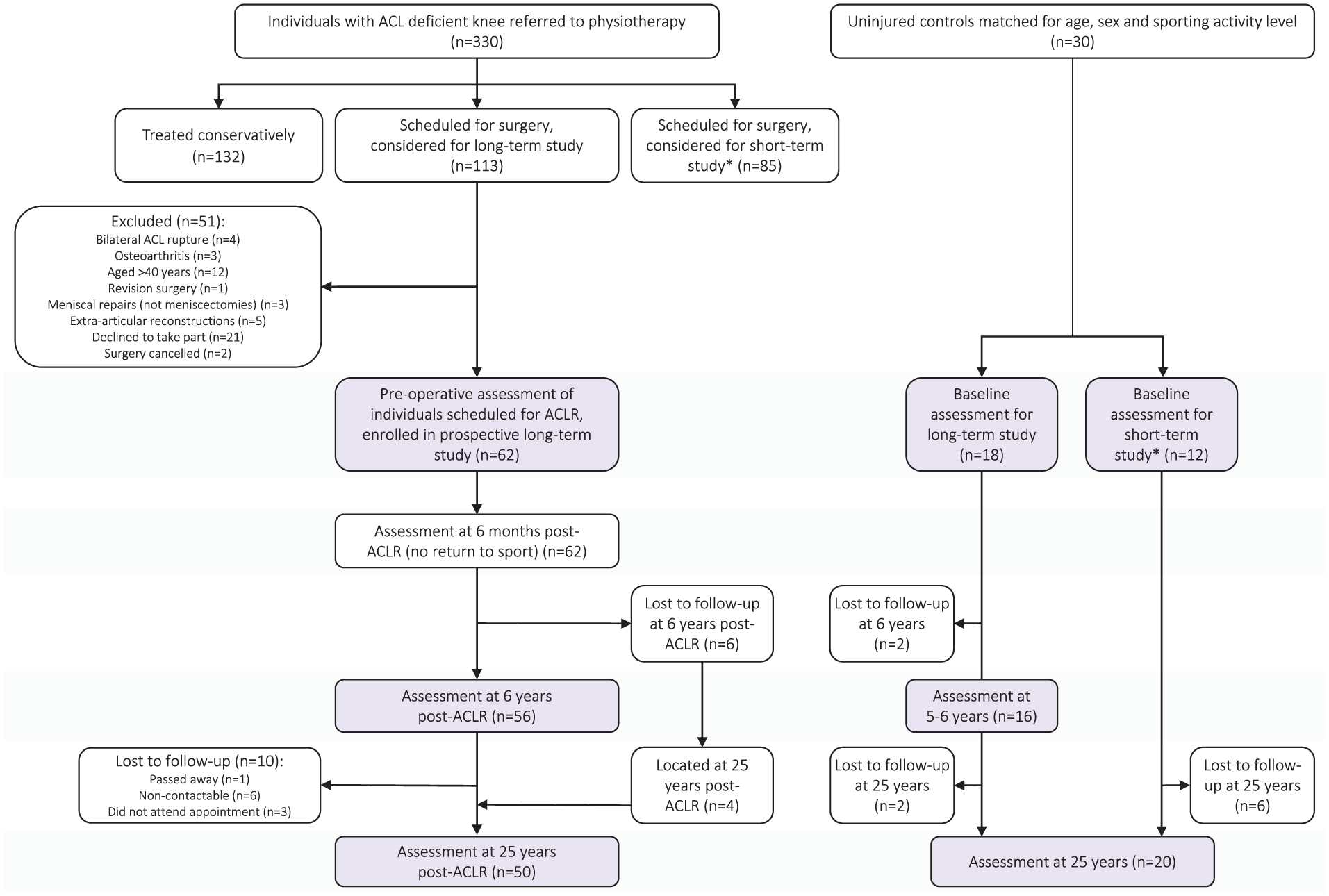
Flowchart showing the recruitment and follow-up time frames of the surgical and uninjured control groups over 25 years. *Control participants recruited to match surgical participants in the short-term study. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
An uninjured group of 30 healthy individuals from a sporting population, matched for age, sex, and sporting activity, at the time of study outset was also recruited (20 males; mean age, 28 years; SD, 8.3 years) (Figure 1). Based on previous studies requiring a significance level of .05 and a power of 0.8, a sample size of 30 was required for each subgroup. 17
Surgery
The ACLR surgery involved either a standard BPTB reconstruction using a mini-arthrotomy with interference screw fixation, or an arthroscopic STG reconstruction using a quadruple-strand graft and interference screw fixation on the femoral and tibial tunnels, as described previously. 17
Physical Therapy
All individuals who underwent ACLR received pre- and postoperative physical therapy as described previously.17-19 This program focused initially on regaining range of movement (especially early extension), activating quadriceps, controlling swelling, and restoring normal gait before progressing through safely graduated stages of restoring neuromuscular control, dynamic stability, strength, balance, agility, plyometric activity, and sports-specific ability. Graft protection was emphasized at each stage. Before returning to sports, individuals were required to complete a comprehensive RTS assessment, including the need to have 90% quadriceps and hamstring strength as assessed at 60 deg/sec on a Cybex II dynamometer, as well as 90% hop indices.
Assessment
Preinjury and 6-year postsurgery sporting levels had previously been recorded for the ACLR group 19 and for controls at comparable time frames. At the 25-year time point, participants were contacted by telephone and invited to attend a long-term follow-up assessment.
Participants completed a RTS questionnaire regarding their highest level of sports reached over the decades after surgery, and how many years they had sustained this level of sports participation. Their current level of sports was also recorded. Sporting activity was measured using a 6-point scale, adapted from the classification of Grindem et al 15 and the Tegner scale 32 to focus on the pivoting demands of individual sports and to capture sports relevant to Australian participants. 20 Sporting levels were classified as follows:
0 = no sport/sporting activity
1 = safe solo nonpivoting sports, including cycling, rowing, walking and gym work
2 = jogging/running, minimal pivoting depending on the surface; triathlons
3 = sports with restricted, less vigorous pivoting, including golf, surfing, surf sports, skiing, tennis, kiteboarding, water skiing, motor cross, boxing, outrigging, campdrafting, and aerobics
4 = vigorous pivoting sports at a recreational level, including touch football, Australian rules football, rugby league, rugby union, Oztag, soccer, cricket, indoor cricket, netball, basketball, squash, hockey, volleyball, rodeo riding, futsal, trail bike riding, dirt bike riding, jiujitsu, karate, or coaching any of the above sports
5 = vigorous pivoting sports at a competitive level
From data collected at baseline, it was possible to assess how sports participation after surgery compared with preinjury sports levels.
Participants in the ACLR and control groups were questioned about any additional injury or surgery at the 6-year and 25-year assessments. Any new relevant operation notes and magnetic resonance imaging (MRI) studies were sourced. All graft and contralateral ACL injuries were confirmed on arthroscopy or MRI, in addition to clinical and KT1000 testing for those seen in person. Participants in the ACLR group were also asked the following 2 questions: (1) comment on whether the cost was worth the benefit of treatment, and (2) do you have any regrets regarding surgery versus no surgery?
Statistical Analysis
Descriptive statistics were calculated for demographic data and outcome measures, and trajectory data were analyzed descriptively. Pearson chi-square tests were used to compare the number of participants at each of the 6 sports levels between the BPTB and STG grafting groups and between the ACLR and control groups. The Student t test was used to test for differences in the duration (in years) of sports participation outcomes between groups. Participants with contralateral ACL ruptures were not excluded from this analysis, as in earlier studies,17,19 because all contralateral ruptures had been reconstructed by this stage. There were no missing data.
Results
Figure 1 summarizes the flow of participants in the ACLR and control groups over the 25-year study. At 6 years after surgery, 56 (90%) of the original 62 ACLR cohort were followed up, with findings reported in a previous study. 17 At 25 years after surgery, 50 (81%) individuals (35 males) were followed up, including 4 who had been lost at the 6-year review. From the 50 individuals who completed follow-up at 25 years, 35 were able to attend the clinic and 15 who had moved out of the district were sent the questionnaire. The participants with ACLR had a mean age of 52.5 years (SD, 6.1 years) and were assessed at a mean of 25 years (SD, 1.4 years; range, 23-27 years) after surgery. A total of 24 individuals (17 males) in the ACLR cohort had undergone BPTB grafting and 26 (18 males) STG grafting.
Twenty (67%) of the 30 participants in the control group were followed up at 25 years (mean, 24 years; SD, 1.8 years; range, 21-25 years) (Figure 1). The mean age of the control participants who completed 25-year follow-up was 52.4 years (SD, 7.8 years).
Subsequent Knee Injury and Surgery
The ACLR group reported numerous knee injuries over the 25-year period. These are summarized in Table 1 and detailed for each participant in Appendix Table A1 (available in the online version of this article). Briefly, over time, 8 individuals ruptured their graft, 9 ruptured their contralateral ACL, 17 individuals sustained 20 further meniscal injuries, 3 with bilateral meniscal injuries. Other injuries included a PCL rupture, a contralateral patellar tendon rupture, and a lateral collateral ligament rupture. Two participants had undergone a high tibial osteotomy, both of whom had medial meniscus injuries at the time of surgery. Three participants had undergone bilateral total knee replacement surgery: 1 had an initial medial meniscus injury, 1 had an initial cartilage injury and subsequent meniscal injury, and 1 had injuries to the medial meniscus, lateral meniscus, and cartilage at the time of reconstruction.
Injuries Sustained Over 25 Years After ACLR a

Individual details can be found in Appendix Table A1 (available online). ACL, anterior cruciate ligament; CL, contralateral; HTO, high tibial osteotomy; PCL, posterior cruciate ligament; PT, patellar tendon; TKA, total knee arthroplasty.
During the same period, one participant from the control group ruptured their ACL, one ruptured their medial collateral ligament and one underwent a meniscectomy. There were no other reported knee injuries or surgeries. The control participant who ruptured their ACL had 12° of knee hyperextension at baseline testing, similar to 12 of the 17 participants with ACLR who ruptured their graft or contralateral ACL.
What Is the Trajectory of Sports Participation Over 25 Years After ACLR?
Before injury, 60 of 62 (97%) individuals participated in sports, with 89% involved in vigorous twisting sports and 8% in sports involving limited twisting activity (Table 2). At 6 years after surgery, 54 of 56 (96%) individuals were still involved in sports, but only 33 (59%) participated in vigorous twisting sports. At 25 years after surgery, 44 (88%) individuals were still involved in sporting activity, with 11 (22%) still partaking in vigorous pivoting sports, and 20 (40%) now participating in safe sports. Figure 2 presents individual trajectory data for the ACLR and control groups. A total of 38 (76%) participants with ACLR reported a decrease in sports participation level over 25 years, 5 (10%) participants reported a lower level at 6 years followed by a higher level at 25 years, and 7 (14%) participants reported the same level across all 3 time points. In comparison, 18 (90%) control participants reported a decrease in sports participation level over 25 years, with 2 (10%) participants reporting stable sports participation level across the 3 time points.
Sports Participation Over 25 Years After ACLR a
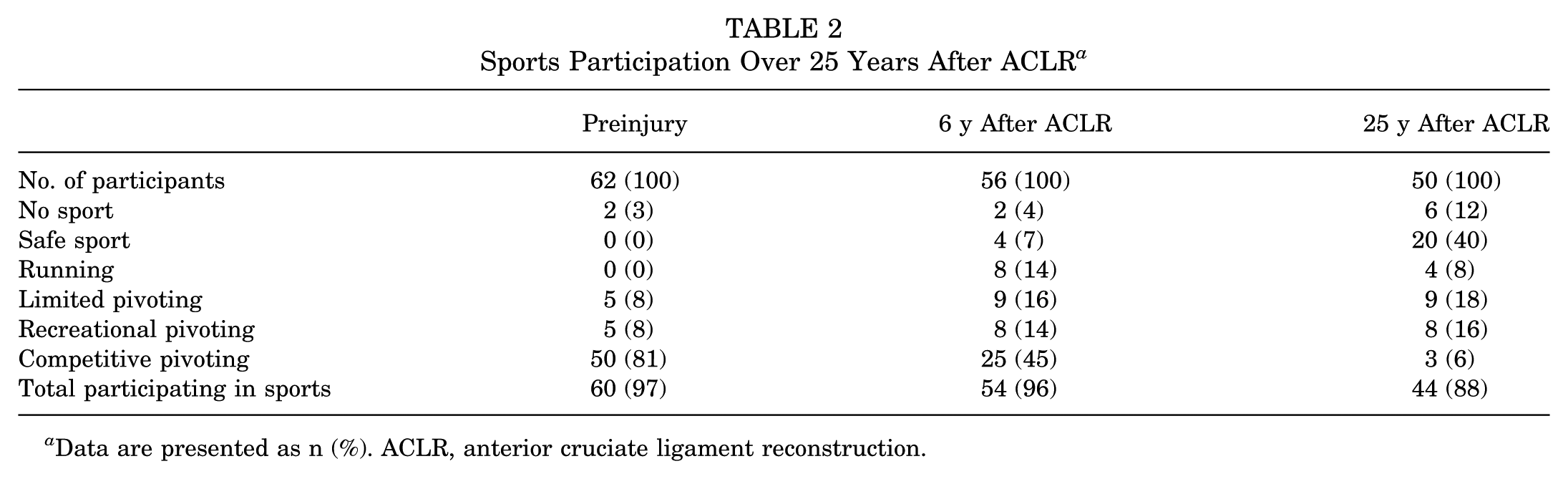
Data are presented as n (%). ACLR, anterior cruciate ligament reconstruction.
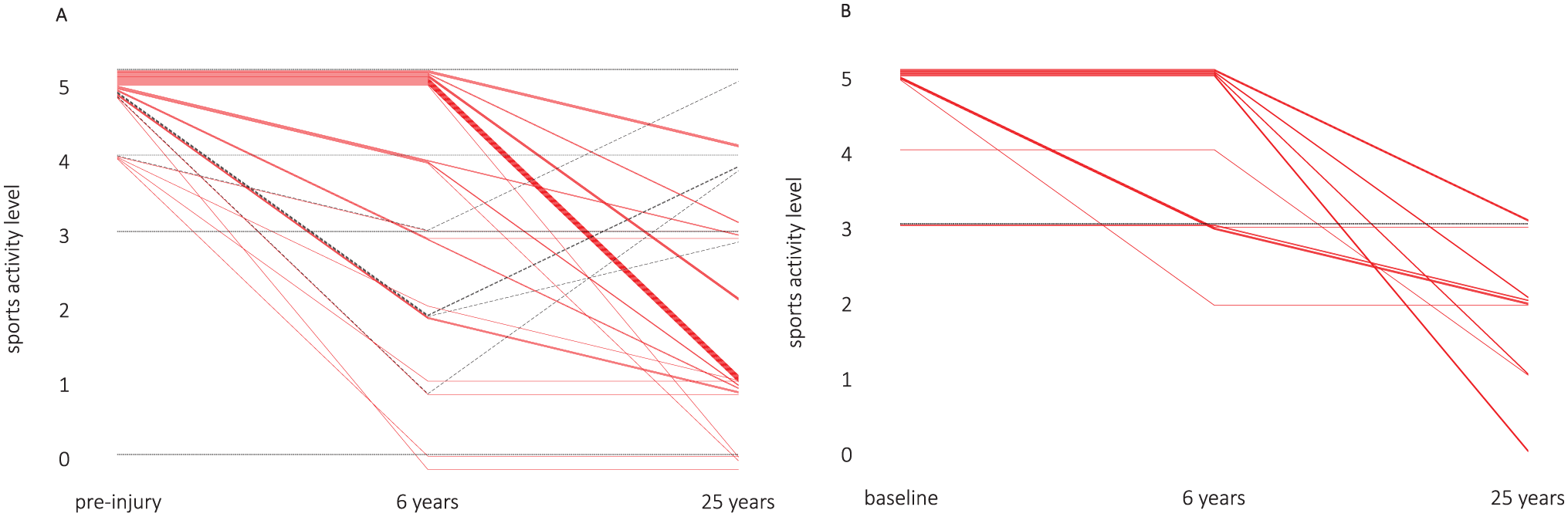
Sports participation trajectories for individuals in the (A) anterior cruciate ligament reconstruction (ACLR) and (B) control groups. Solid red lines indicate participants whose sports participation decreased over 25 years, dashed black lines indicate individuals whose sports participation decreased at 6 years and then increased at 25 years, dotted black lines indicate individuals whose sports participation was stable across all 3 time points.
Does Sports Participation Over 25 Years After ACLR Differ Between Graft Types?
Comparisons between participants who had undergone BPTB grafting (n = 24) and STG grafting (n = 26) revealed no significant differences in percentage participation on the 6-point sports participation scale between the 2 graft types in the level of sports played preinjury (P = .442), in the level of sports played at 6 years after surgery (P = .511), or in the highest level of sports played since surgery (P = .926) (Table 3). There was no significant difference in the mean duration of time spent participating in pivoting sports (P = .154) or in the level of sports played at the 25-year follow-up (P = .100), or in the mean duration of time involved in sports at the highest level (P = .071).
Sports Participation Over 25 Years After ACLR, Comparing Individuals With BPTB Grafts to Those With STG Grafts (N = 50) a
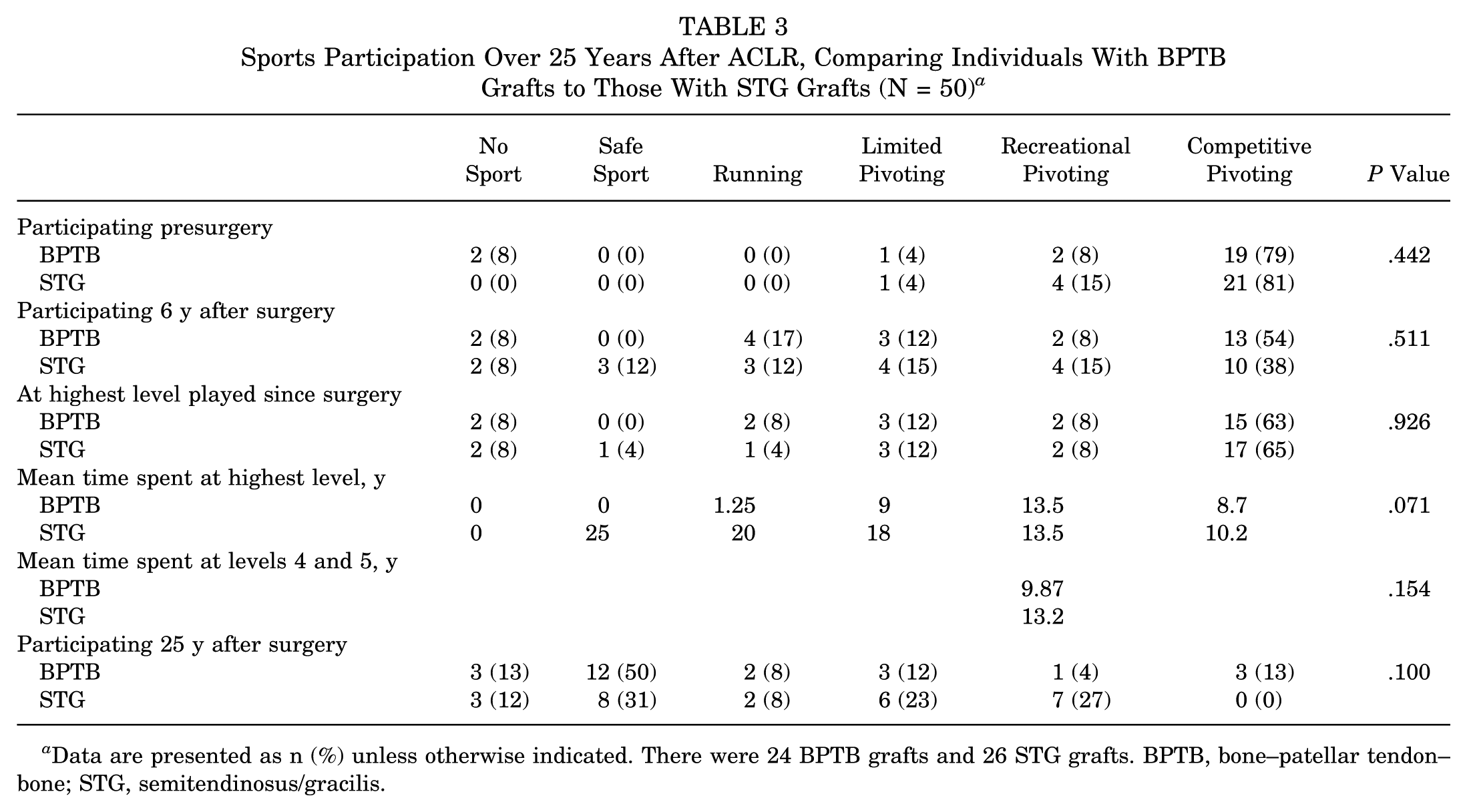
Data are presented as n (%) unless otherwise indicated. There were 24 BPTB grafts and 26 STG grafts. BPTB, bone–patellar tendon–bone; STG, semitendinosus/gracilis.
Does Sports Participation Over 25 Years After ACLR Differ Compared With Uninjured Controls?
There was no significant difference in percentage of participation between the ACLR group and uninjured control group in the level of sports played preinjury or at study onset (P = .121), in the level of sports played at 6 years after surgery/study onset (P = .093), or in the highest sports level played since study onset (P = .417) (Table 4). Similarly, there was no significant difference between the mean time involved in sports at the highest level (P = .690). However, there was a significant difference between groups in the duration of time involved in pivoting sports (P = .032) and in the level of sports played at the 25-year follow-up (P = .005): Participants with ACLR were involved in pivoting sports for significantly longer than uninjured controls, and more participants in the ACLR group engaged in higher levels of sports than controls at 25-years.
Sports Participation Over 25 Years Comparing Individuals After ACLR With Uninjured Controls (N = 70) a
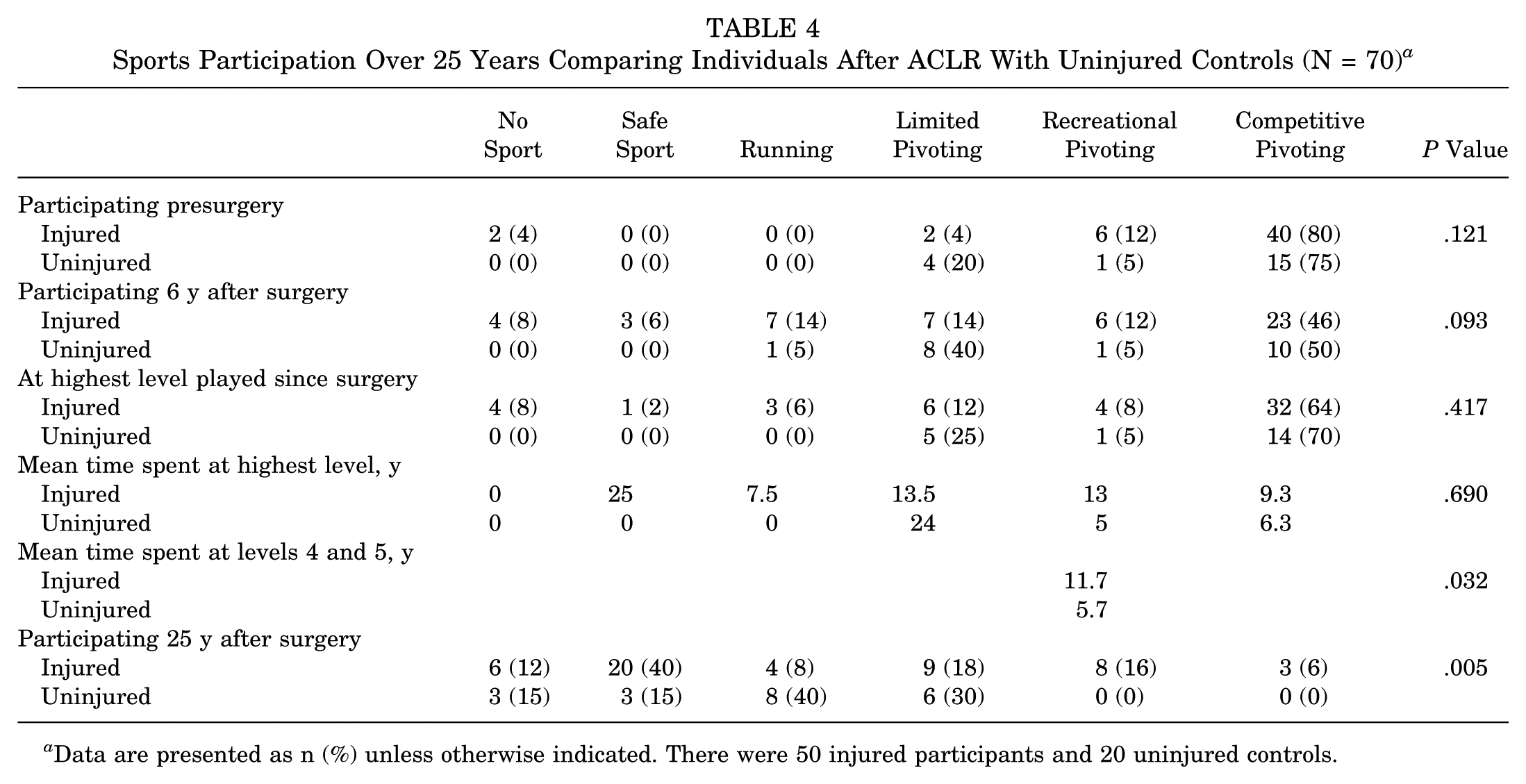
Data are presented as n (%) unless otherwise indicated. There were 50 injured participants and 20 uninjured controls.
Perspectives on Undergoing ACLR Surgery
Despite these sequelae, 49 of the 50 individuals expressed having no regrets about having undergone ACLR and agreed that the costs were worth the benefits. One participant reported regretting surgery, and another reported that he was unsure as to whether the costs were worth the benefit, but he had no regrets about undergoing surgery.
Discussion
This study found that, despite the high incidence of postsurgical injury, the majority of individuals who had undergone ACLR 25 years previously were still involved in sports, sometimes at a high level. The results of this study showed that ACL graft type did not influence sports participation at 6 years or 25 years after surgery. Interestingly, individuals who had undergone ACLR 25 years prior were significantly more active in sports than uninjured controls who were followed over the same time period.
Trajectory of Sports Participation Over 25 Years After ACLR
The level of sports involvement declined over 25 years, with 89% of the ACLR cohort participating in pivoting sports preinjury, 59% at 6 years after surgery, and 22% at 25 years after surgery. Three individuals, all with BPTB grafting, were still competing in pivoting sports at the 25-year follow-up (Table 2), including one individual who represented Australia in the winning team at the Masters Soccer Pan Pacific Games, and another who took part in the Australian National Trail bike riding titles. Overall, at their highest participation level, 72% of participants returned to pivoting sports, with 64% at competition level (Table 4). Furthermore, 58% returned to preinjury sporting levels as assessed on our 6-point scale. Lindanger et al 22 reported that 71% of individuals returned to competitive sports after undergoing ACLR within 24 months of injury, and 53% returned to their preinjury level of sports. The authors did not describe sports participation at 25 years after surgery, but did describe the duration of time spent in sports, reporting that males returned to their primary sports for 10 years and females for 4 years (P < .001). 22 In our current study, the mean duration at the highest level of sports played was 9.7 years. Of the 64% of participants with ACLR who returned to competitive pivoting sports, the mean time competing at this level was 9.3 years. Long-term participation in preinjury sports was also observed; at 25 years after ACLR, 16% of individuals were still playing their preinjury sports and a further 4% were coaching their preinjury sport. Taken together, our findings highlight the potential to return to preinjury sports after ACLR and maintain participation over the long term, including in competitive pivoting sports.
However, it is important to acknowledge that decreases in sports participation over 25 years can be due to a number of reasons. Although 50% of participants in the ACLR group modified their sports because of their knee, other reasons for reducing sports participation included age and lifestyle preferences, family demands, and illness. This is consistent with the work of Lindanger et al, 22 who reported that 48% of their cohort changed their level of sports participation for non–knee-related reasons. Indeed, the present study found that a greater proportion of participants in the control group (90%) reported a reduction in their level of sports participation over 25 years compared with the ACLR group (76%). A follow-up qualitative study in this cohort could explore these factors and their interaction in more depth and identify barriers and facilitators to participating in sports from young adulthood to middle age after ACLR.
Sports Participation Over 25 Years After ACLR Does Not Differ Between Graft Types
As hypothesized, no difference was found in sports participation over 25 years between individuals who had undergone a BPTB graft and those who had an STG graft. Bergeron et al, 5 in their systematic review, also reported no difference in return to baseline sports between the 2 graft types. Interestingly, in this current study, the STG graft group reported a longer duration in their highest level of participation in competitive pivoting sports, compared with the BPTB graft group (mean, 10.2 years vs 8.7 years), but this difference was not significant (P = .071).
Sports Participation Was Higher in Individuals Who Had Undergone ACLR Than in Controls at 25 Years
While this study hypothesized that control participants would reach and sustain higher levels of sports participation than individuals who had undergone ACLR over 25 years, this was not the case. Most surprisingly, there was a significant difference between groups at the 25-year follow-up, with the ACLR group demonstrating a higher percentage of participation in vigorous pivoting sports (22%) than the control group (0%). The time spent playing vigorous pivoting sports was also twice as long for the ACLR group (mean, 11.7 years) than for controls (mean, 5.7 years). This outcome invites both speculation and further research to explore potential reasons that may have influenced this finding. First, it may be that the controls were not well matched with the participants with ACLR regarding sports participation preinjury/baseline data, despite attempts to do so. Second, it is possible that having made a commitment to long-term rehabilitation, the ACLR group was motivated to work hard to pursue their long-term sporting goals. Third, it is possible that the ACLR group was inherently more competitive and determined than their control group counterparts. That is, participants who had undergone ACLR may demonstrate more grit due to innate personality characteristics rather than as a result of their ACL injury. Although this study did not measure grit in this cohort (using the grit scale8,9), it may be useful in future research to determine the effect of grit on very long-term outcomes after ACLR. Two previous studies found that higher baseline grit is associated with better functional outcomes in adolescents who undergo ACLR.4,27
Subsequent Knee Injury, Surgery, and Regrets
One of the determining factors affecting sports performance is considered to be the incidence of reinjury. 2 This study found a high rate of reinjury in the ACLR group, with 20 additional meniscal injuries (Table 1), which affect both sporting outcomes and the development of knee OA, but are seldom reported. 10 Over the 25 years, there were 8 (13%) graft ruptures, the first occurring at 4 years after surgery. Four participants had undergone BPTB grafting, and 4 had STG grafting. One individual chose to undergo revision reconstruction. This rerupture rate is slightly lower than those described at comparable time periods by Salmon et al 31 (21%) and Elveos et al 10 (19%). Nine (15%) participants in the ACLR cohort ruptured their contralateral ACL within 25 years of surgery, consistent with rates described by Salmon et al 31 (12%) and Lindanger et al 22 (19.8%). Interestingly, 2 of the participants who ruptured their contralateral ACL were still currently involved in vigorous pivoting sports 5 years and 10 years after their contralateral ACL injury. Of note is the finding that 4 participants ruptured their ACL graft ≥12 years after surgery, the most recent occurring 20 years after surgery. Three of the contralateral ACL ruptures occurred between 10 and 20 years after surgery. These findings highlight the importance of long-term follow-up to determine and manage ongoing risk of injury and how this influences longevity in sport. Clinicians should also ensure that patients are aware that the risk of graft rupture persists beyond the initial postoperative recovery and RTS phases.
In 1993, Gillquist 14 stated that the only reason to perform an ACLR was “to give the patient enough security to reach the goal of going back to strenuous sports and then ruining the knee.” Overall, our findings dispute this statement. Not only did participants return to and maintain high levels of sports post-ACLR, but they overwhelmingly reported positive perspectives of the ACLR surgery. Despite the high number of injuries and surgeries reported in this study, 49 of the 50 participants, when questioned, responded with a definite “no regrets,” with many explaining that they had enjoyed many years of stability and ability that they believed they would not have had otherwise. Individual comments included “my ACLR gave me back my youth,” ‘I did not think I would ever play sport again,” and “after 25 years, I am training for an Ironman.” Taken together, our findings highlight the potential for those who have undergone ACLR to return to pivoting-based sports activities, despite subsequent knee injuries and surgeries, and maintain sports participation for at least 25 years.
Strengths and Limitations
A major strength of this study is the prospective longitudinal design, following parallel groups of individuals who underwent ACLR and uninjured controls over a 25-year period. All ACLR procedures were performed by 1 surgeon (A.C.K.), and rehabilitation was provided by primarily 1 physical therapist (S.L.K.), offering consistency of care. A further strength is the high rate of follow-up of participants with ACLR (81%), which is higher than that in other long-term studies, which described follow-up rates of 51% 16 and 65% 28 at 25 years after surgery. Our high follow-up rate offsets the relatively small sample size and highlights the importance of building and maintaining relationships in long-term cohort studies. However, we acknowledge the higher loss to follow-up in the control group (33% at 25 years). Notwithstanding the challenges of retaining control participants in a study over 25 years, this did result in a sample size at the 25-year follow-up that was smaller than the sample size indicated necessary by calculations (n = 30). Although the sample size was sufficient to detect significant differences between the ACLR and control groups for level of sports participation at 25 years, and mean time spent at levels 4 and 5, it is plausible that other between-group comparisons may have been underpowered to detect significant differences (eg, level of sports participation at 6 years). A further weakness of this study is that some of the information relied on recall, specifically the questions regarding the highest level of sports played over the 25 years and the duration of participation.
Clinical Implications
For a young athlete who sets out on the ACLR journey, there is little evidence regarding what potential outcomes are possible 25 years later. This study has shown that ACLR using BPTB or STG grafting, followed by intensive rehabilitation, does not appear to be a barrier for continued participation in sports 25 years after surgery. This knowledge may assist the young injured athlete in setting realistic goals for RTS and long-term management to optimize their knee health, participation, and performance.
Conclusion
Although the level of sports participation declined over 25 years after ACLR, nearly one-quarter of participants were still involved in vigorous pivoting sports. As hypothesized, graft type did not influence sports participation over 25 years. Individuals who had undergone ACLR 25 years prior were significantly more involved in sports than uninjured controls, particularly in vigorous pivoting sports. Findings highlight the potential for longevity in sports after an ACLR and may be a useful resource for clinicians working with young athletes who are considering surgical reconstruction.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465251380293 – Supplemental material for Sports Participation 25 Years After Anterior Cruciate Ligament Reconstruction: A Prospective Longitudinal Study Comparing Patients With Patellar Tendon and Hamstring Tendon Grafting to Uninjured Controls
Supplemental material, sj-pdf-1-ajs-10.1177_03635465251380293 for Sports Participation 25 Years After Anterior Cruciate Ligament Reconstruction: A Prospective Longitudinal Study Comparing Patients With Patellar Tendon and Hamstring Tendon Grafting to Uninjured Controls by Susan L Keays, Peter A. Newcombe, Anthony C. Keays, Daniel B. Mellifont and Natalie J. Collins in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank Hashem Mohamed, physiotherapist, for his help with data collection.
Submitted February 22, 2025; accepted August 4, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from The University of Queensland.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.