
Abstract
Background:
A few studies have documented the long-term results of chondrocyte-based procedures for the treatment of patellofemoral cartilage lesions, but specific results are lacking after matrix-assisted autologous chondrocyte transplantation (MACT) for patellar and trochlear lesions.
Purpose:
To document the clinical results of MACT for the treatment of patellar and trochlear chondral defects at long-term follow-up.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 44 patients were prospectively evaluated after MACT for patellofemoral lesions. There were 24 patients affected by patellar lesions, 16 by trochlear lesions, and 4 with both patellar and trochlear defects. Clinical outcomes were analyzed using the International Knee Documentation Committee (IKDC) subjective form, EuroQol visual analog scale, and Tegner score for sport activity level before surgery and at follow-up time points of 5, 10, and a minimum of 15 years (mean final follow-up, 17.6 ± 1.6 years). A Kaplan-Meier survival analysis was performed to examine the survival to failure. Failure was defined as the need for a second surgery because of the persistence of symptoms related to the primary defect.
Results:
An overall significant improvement was documented from baseline to the last follow-up. The IKDC subjective score improved in the trochlear group from 41.0 ± 13.3 at baseline to 83.9 ± 21.6 at 5 years (P < .005), remaining stable up to the final follow-up (81.3 ± 20.5). In the patellar group, the IKDC subjective score improved from 36.1 ± 14.4 at baseline to 72.3 ± 17.5 at 5 years (P < .005), remaining stable up to the final follow-up (62.0 ± 20.3). Patients with trochlear lesions presented higher IKDC subjective scores compared with those with patellar lesions at 5 (P = .029), 10 (P = .023), and ≥15 years (P = .006) of follow-up. Similar trends were documented for the Tegner score, while no differences were documented for the EuroQol visual analog scale score between patellar and trochlear lesions. There were 4 failures (9.1%) during the follow-up period. The Kaplan-Meier survival analysis did not show statistically significant differences between trochlear and patellar lesions.
Conclusion:
This hyaluronic acid–based MACT technique offered positive and durable clinical outcomes with a low failure rate at long-term follow-up in patients affected by patellofemoral cartilage lesions. However, trochlear and patellar lesions demonstrated a notable difference in terms of clinical findings and sport activity level, with significantly higher results for patients with trochlear lesions but less satisfactory outcomes for patients with patellar lesions.
Articular cartilage lesions of the patellofemoral joint remain a challenging problem for orthopaedic surgeons because of the limited cartilage healing potential and the difficulty in restoring its biomechanical features.18,30 This articular location represents a complex anatomic region that sustains significant shear and compression forces, which are often exacerbated by issues such as patellar malalignment, further complicating the treatment and healing of chondral lesions. 27 Consequently, even if the correction of concurrent abnormalities enhances the likelihood of a more favorable outcome, patients affected by chondral lesions of the patellofemoral joint frequently obtain poorer outcomes compared with those with defects of the femoral condyles.3,7
Regenerative techniques, such as matrix-assisted autologous chondrocyte transplantation (MACT), have been demonstrated over the years to be an effective therapeutic strategy to restore the articular surface. 13 This technique overcomes the drawbacks of first-generation autologous chondrocyte implantation, such as periosteal harvest morbidity, hypertrophy, and the need for reintervention. 20 The positive outcomes documented for chondrocyte-based techniques at short-term and midterm follow-up might be explained by their ability to produce hyaline-like cartilage that is mechanically and functionally stable.26,32 Still, an evaluation of these treatment methods at long-term follow-up is paramount, as patients undergoing surgery are often young and require a recovery and return to an active lifestyle over time. The durability of these results has been recently confirmed up to 15 years of follow-up, with studies focusing especially on condylar lesions.3,5 On the other hand, only a few articles have documented the long-term results of chondrocyte-based procedures for the treatment of patellofemoral lesions, and specific results are lacking after MACT for patellar and trochlear lesions.2,4,9,24,28
The primary aim of this prospective study was to document the clinical results of MACT for the treatment of patellar and trochlear chondral defects at long-term follow-up. The secondary aim was to investigate the difference in clinical outcomes between trochlear lesions and patellar lesions at long-term follow-up. The hypothesis was that MACT would provide long-lasting results with a low failure rate, with better outcomes for trochlear lesions compared with patellar lesions.
Methods
Study Design and Eligibility Criteria
This was a long-term evaluation of a previously published prospective study. 11 The evaluation at long-term follow-up was approved by the hospital ethics committee of Istituto Ortopedico Rizzoli (No. 0001748). A total of 53 consecutive patients with full-thickness cartilage defects of the patellofemoral joint were treated with MACT from 2000 to 2006 at a highly specialized referral center for orthopaedic abnormalities (Figure 1). Participation was voluntary, and informed consent was obtained from each patient. Patients underwent surgical treatment for symptomatic focal chondral lesions involving the patellofemoral joint (trochlea or patella) of grade III or IV according to the International Cartilage Regeneration & Joint Preservation Society classification system. Exclusion criteria were untreated patellofemoral malalignment (>10° patellar tilt on axial radiographs and >20-mm tibial tuberosity–trochlear groove distance), untreated lower limb malalignment (>5° on full-length standing anteroposterior radiographs), diffuse osteoarthritis, untreated knee instability, and other general medical comorbidities (rheumatoid arthritis, diabetes, etc). Patients with patellofemoral or tibiofemoral malalignment or knee instability who underwent a combined surgical procedure of realignment or ligament reconstruction were included.
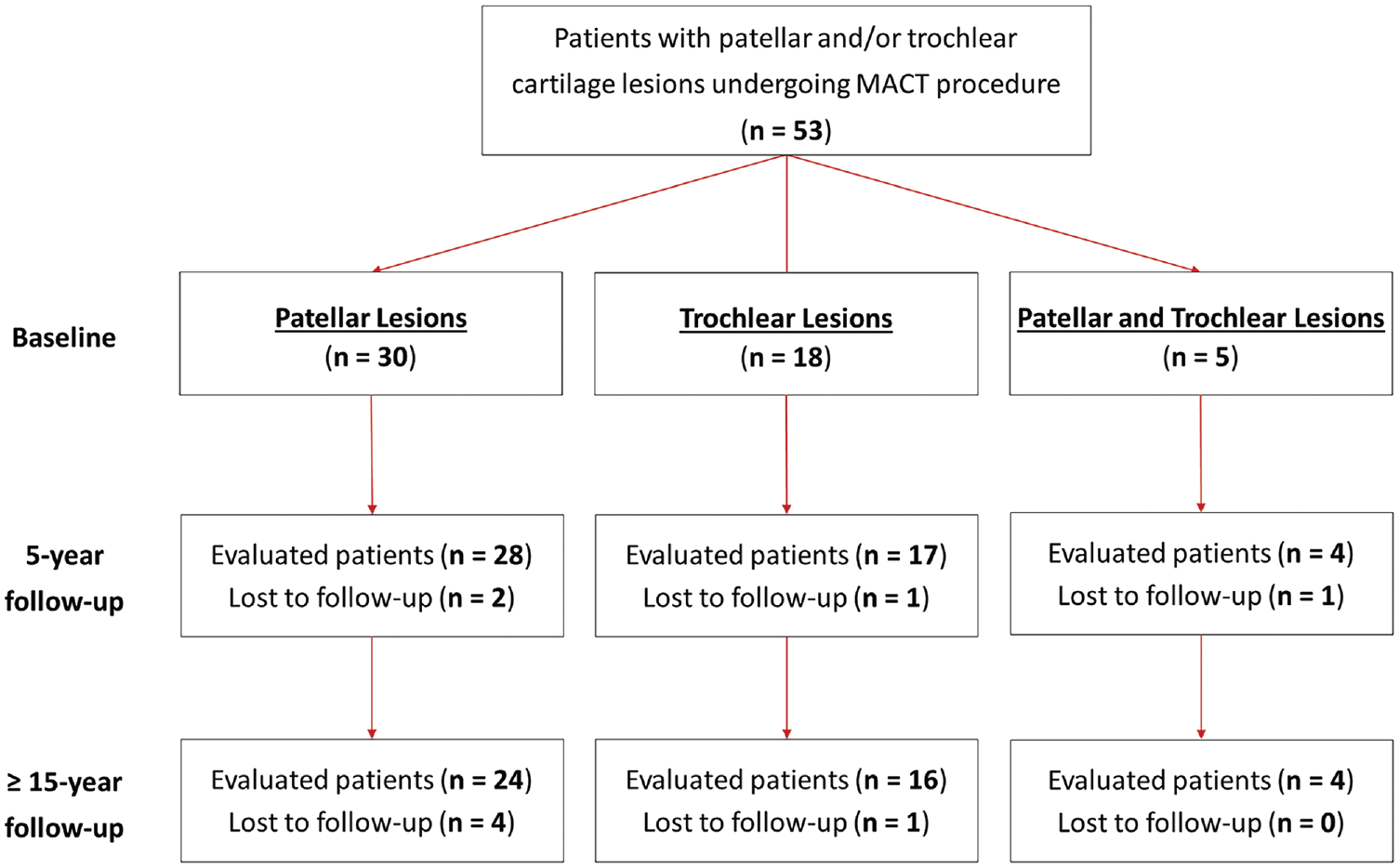
A Strengthening the Reporting of Observational studies in Epidemiology (STROBE) flowchart of patient selection. MACT, matrix-assisted autologous chondrocyte transplantation.
There were 44 patients prospectively evaluated at a minimum of 15 years of follow-up, with 4 patients lost before 5-year follow-up and another 5 patients lost to the last follow-up (total dropout rate of 17% at the final follow-up). The mean final follow-up was 17.6 ± 1.6 years (range, 15-21 years). Overall, 24 patients were affected by patellar lesions, 16 were affected by trochlear lesions, and 4 had both patellar and trochlear defects (Figure 1). A comparative analysis was performed between the 24 patients affected by isolated patellar defects (patellar group) and the 16 patients affected by isolated trochlear defects (trochlear group). The baseline characteristics of the 2 groups are reported in detail in Table 1. The 2 groups were homogeneous for all baseline characteristics, except for sex (trochlear lesions were less common in women; P = .002) and the number of realignment procedures (patellar lesions were more commonly associated with previous or combined realignment procedures; P = .001). Previous surgery for 22 patients included 8 with meniscectomy, 6 with anterior cruciate ligament reconstruction, 5 with debridement, 3 with a realignment procedure, 3 with microfracture, 3 with synovial plica removal, 2 with lateral release, 1 with Hoffa fat pad removal, 1 with loose body removal, 1 with osteochondral transplantation, and 1 with osteochondral fragment fixation. Additionally, 23 patients underwent at least one combined procedure, including 13 with lateral release, 7 with meniscectomy, 5 with a realignment procedure, 2 with anterior cruciate ligament reconstruction, 1 with trochleoplasty, 1 with tibial tuberosity osteotomy, and 1 with patellar tendon scarification.
Baseline Characteristics of Patients a
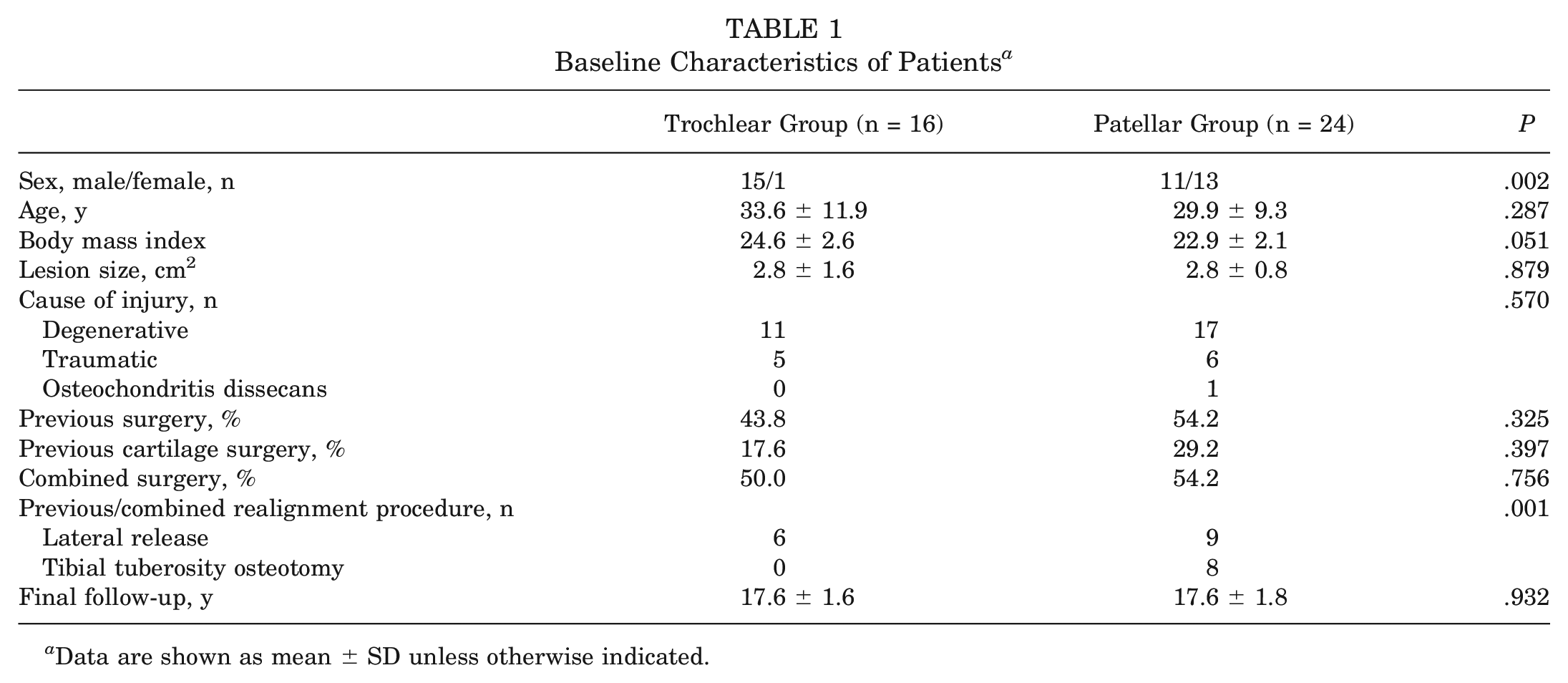
Data are shown as mean ± SD unless otherwise indicated.
Surgical Technique and Clinical Evaluation
As previously described, the surgical technique consisted of 2 steps. 11 Briefly, the first step included biopsy of 150 to 200 mg of healthy cartilage from a nonweightbearing articular area for chondrocyte culture and seeding onto a hyaluronic acid–based scaffold (Hyaff-11; Fidia Advanced Biopolymers Laboratories). Then, resulting bioengineered tissue (Hyalograft C; Fidia Advanced Biopolymers Laboratories) was implanted in a second step according to the arthroscopic technique described by Marcacci et al 25 (for trochlear lesions) or a miniarthrotomic approach (for patellar lesions). 21
All patients were clinically evaluated before surgery and at follow-up visits at 5, 10, and a minimum of 15 years after treatment. Patients completed clinical questionnaires, with doctors available for any questions. If patients were unable to attend an in-person visit at the requested follow-up time point, a physician conducted a telephone interview to collect questionnaire data. Clinical outcomes were examined using the International Knee Documentation Committee (IKDC) subjective form, the Tegner score for sport activity level, and the EuroQol visual analog scale (EQ-VAS) for general health status. Moreover, a comparative analysis between patients treated for isolated patellar lesions and patients treated for isolated trochlear lesions was performed to assess the influence of the lesion site on clinical outcomes.
Treatment was deemed to have failed if the patient needed new surgery because of symptoms related to the primary defect. For patients with failure, the worst clinical evaluation findings between baseline and the last available assessment were considered for the subsequent follow-up. A survival analysis was performed to examine the survival to failure up to the last follow-up.
Statistical Analysis
All continuous data were expressed in terms of the mean and standard deviation, and categorical data were expressed as the frequency and percentage. The Shapiro-Wilk test was performed to assess the normality of continuous variables. The Levene test was used to assess the homoscedasticity of the data. A repeated-measures general linear model with the Šidák test for multiple comparisons was performed to assess the differences at different follow-up time points. Analysis of variance was performed to assess the between-group differences of continuous, normally distributed, and homoscedastic data; the Mann-Whitney nonparametric test was used otherwise. Analysis of variance, followed by the post hoc Šidák test for pairwise comparisons, was performed to assess the among-group differences of continuous, normally distributed, and homoscedastic data; the Kruskal-Wallis nonparametric test, followed by the post hoc Mann-Whitney test with Bonferroni correction for multiple comparisons, was used otherwise. The Spearman rank correlation coefficient was used to assess correlations between numerical scores and continuous data, and the Kendall tau-b correlation coefficient was used to assess correlations between ordinal data. The Fisher exact test was performed to assess the relationship between dichotomous variables. The Pearson chi-square test was performed to investigate relationships between categorical variables. For all tests, P < .05 was considered significant. A Kaplan-Meier survival analysis with the log-rank test was performed to examine the survival to failure. All statistical analyses were performed using SPSS (Version 19.0; IBM).
Results
No complications related to the implant or severe adverse events were observed during the follow-up period. Both patients with trochlear lesions and patients with patellar lesions showed similar clinical trends during follow-up evaluations, with a significant improvement from baseline to all follow-up time points. The comparative analysis between the 2 groups showed overall better results in patients with trochlear lesions at all follow-up time points (Figures 2 and 3).
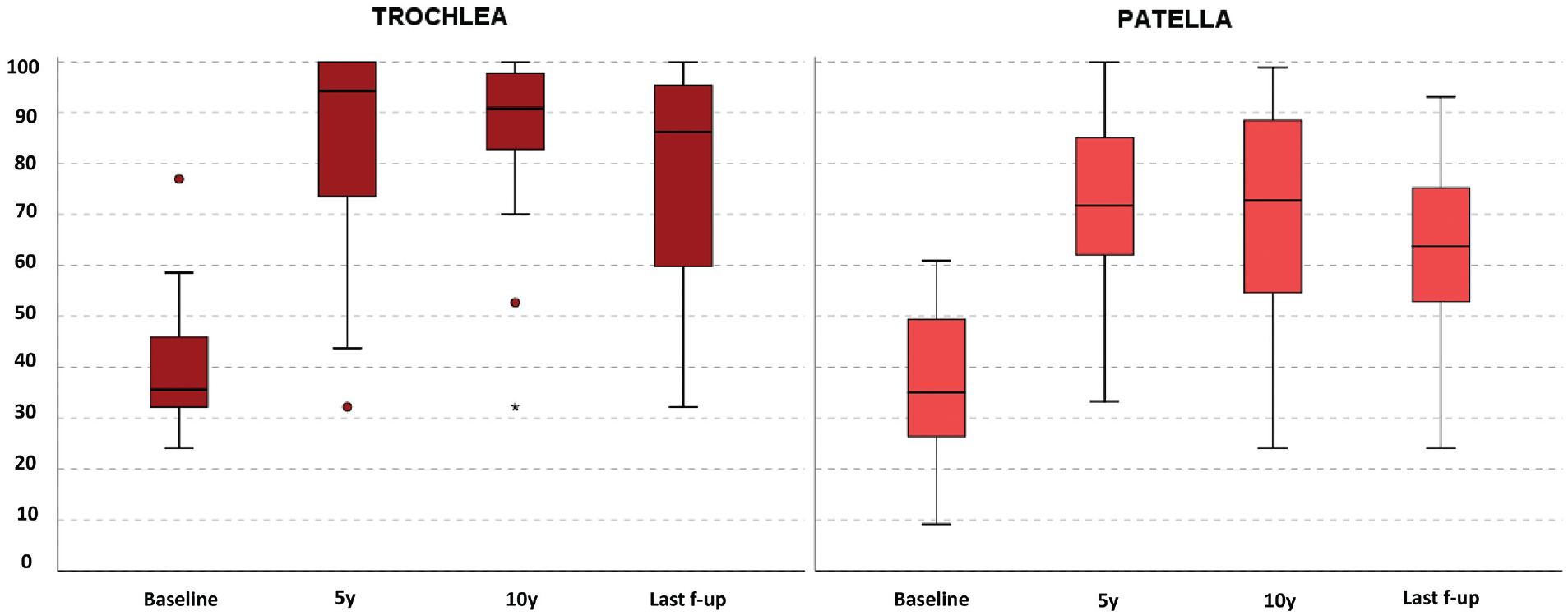
The International Knee Documentation Committee subjective score at baseline and at 5, 10, and ≥15 years of follow-up (f-up) in both treatment groups. The box and whisker plots show medians and interquartile ranges.
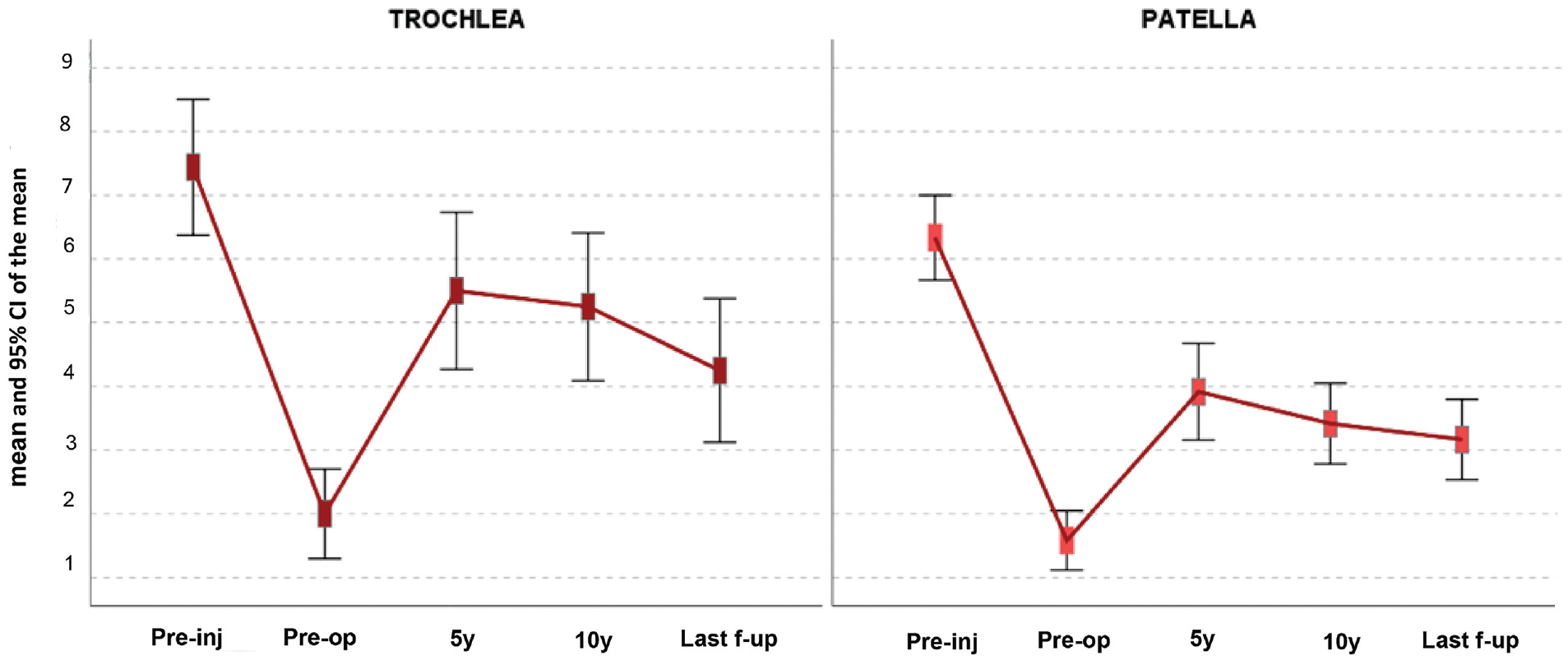
The Tegner score before the injury (Pre-inj), preoperatively (Pre-op), and at 5, 10, and ≥15 years of follow-up (f-up) in both treatment groups.
The IKDC subjective score (Figure 2) improved in the trochlear group from 41.0 ± 13.3 at baseline to 81.3 ± 20.5 at the final follow-up (P < .005). No significant changes were found from 5 (83.9 ± 21.6) and 10 (85.1 ± 18.9) years compared with the last follow-up. In the patellar group, the IKDC subjective score improved from 36.1 ± 14.4 at baseline to 62.0 ± 20.3 at the final follow-up (P < .005). No significant changes were found from 5 (72.3 ± 17.5) and 10 (68.8 ± 22.8) years compared with the last follow-up. The trochlear group showed a higher IKDC subjective score at 5 (P = .029), 10 (P = .023), and ≥15 years (P = .006) compared with the patellar group, while no significant differences were found in terms of improvement from baseline to all follow-up time points between the 2 groups.
The Tegner score (Figure 3) for the trochlear group increased from 2.0 ± 1.3 preoperatively to 4.3 ± 2.1 at the final follow-up (P = .008). No significant changes were found from 5 (5.5 ± 2.3) and 10 (5.3 ± 2.2) years compared with the last follow-up. In the patellar group, the Tegner score increased from 1.6 ± 1.1 preoperatively to 3.0 ± 1.6 at the final follow-up (P < .0005). No significant changes were found from 5 (3.9 ± 1.8) and 10 (3.4 ± 1.5) years compared with the last follow-up. The trochlear group showed a higher Tegner score at 5 (P = .014) and 10 (P = .003) years and better improvement from preoperatively to 10 years compared with the patellar group (3.3 ± 2.2 vs 1.8 ± 1.7, respectively; P = .036). At all follow-up time points, the Tegner score remained lower compared with the preinjury score in both groups (7.4 ± 2.0 and 6.3 ± 1.6, respectively).
The EQ-VAS score increased in the trochlear group from 65.0 ± 18.9 at baseline to 86.3 ± 12.8 at the last follow-up (P = .012) and in the patellar group from 56.0 ± 18.5 at baseline to 78.8 ± 13.5 at the last follow-up (P = .001), without statistically significant differences between the 2 groups in terms of improvements and absolute values. The small number of patients affected by both trochlear and patellar lesions did not allow us to perform a statistical analysis for this group, although their data were comparable with those of the patellar group, with a mean IKDC subjective score of 64.7 ± 16.9 at the last follow-up. Further analysis was performed to determine the parameters that influenced the clinical outcomes at long-term follow-up. In the patellar group, male patients reported higher IKDC subjective scores compared with female patients at baseline (44.6 ± 11.3 vs 28.9 ± 12.9, respectively; P = .005) and at the final follow-up (74.1 ± 11.8 vs 51.8 ± 20.7, respectively; P = .008). Other parameters did not influence the clinical outcomes in both treatment groups. Overall, 4 failures (9.1%) were recorded in the study cohort during the follow-up period: 1 patient with a trochlear lesion was treated with implant removal at 6 years, and 3 patients with patellar lesions were treated with total knee arthroplasty at 5 years, implant removal at 7 years, and implantation with a new scaffold at 7 years, respectively. The Kaplan-Meier survival analysis did not show statistically significant differences between the trochlear and patellar groups (Figure 4), with a mean survival rate at the last follow-up of 90.9% (95% CI, 74.3%-100.0%).
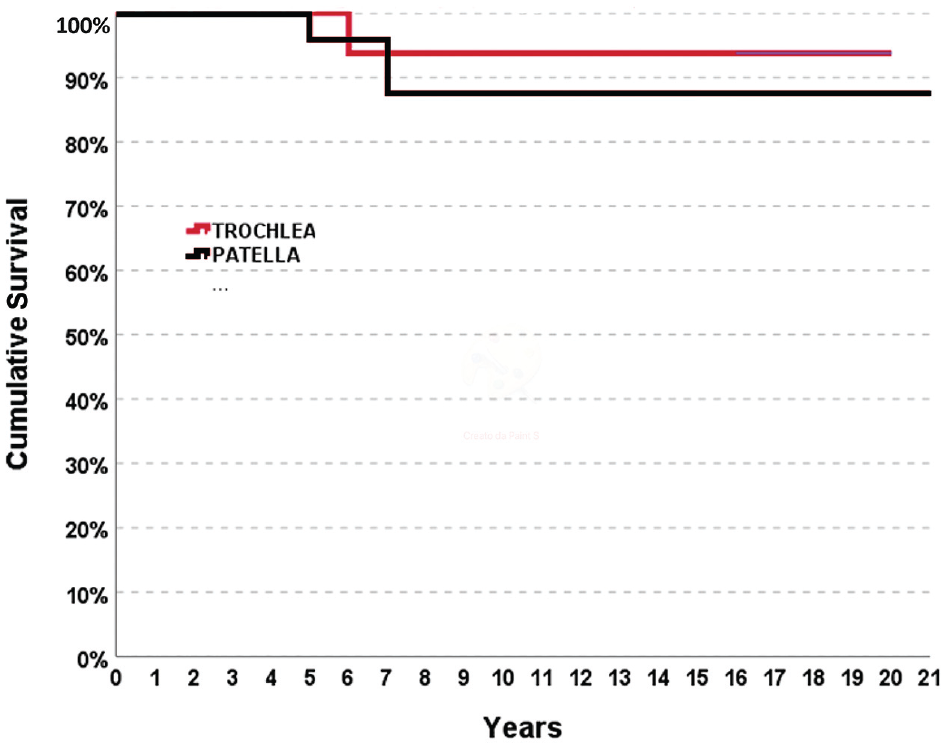
The Kaplan-Meier survival curve for patients treated with matrix-assisted autologous chondrocyte transplantation for patellar and trochlear lesions.
Discussion
The main finding of this study is that the hyaluronic acid–based MACT technique provided satisfactory and stable clinical results with a low failure rate at long-term follow-up in patients affected by patellofemoral cartilage lesions. The comparative analysis between trochlear and patellar defects demonstrated a marked difference at all follow-up time points, with significantly poorer results in patients with patellar lesions in terms of clinical outcomes and sport activity level.
This long-term study confirmed the results previously reported at shorter follow-up, with better clinical outcomes in patients with trochlear lesions treated with MACT compared with those with patellar lesions, indicating that the trochlea and patella should not be considered a single pathological entity in clinical practice.11,16,22 These findings are likely caused by different characteristics in terms of several aspects between the patella and trochlea. The 2 areas present different cartilage tissue in terms of thickness, composition, permeability, and compressive properties. 14 This results in different cartilage features of the 2 sites, with different mechanical characteristics and thus different responses to cartilage regenerative treatment. 23 Accordingly, the same scaffold used for both locations might fulfill the requirements of one site better than the other. For example, if the thickness of a scaffold is adequate for the trochlea, it may be insufficient to entirely restore thicker patellar cartilage. In this light, the thickness of patellar cartilage may determine the fragility of this chondral area as well as the higher difficulty in regenerating it through scaffold implantation, which might explain the lower clinical outcomes observed in this study and in previous studies.11,17,22
The trochlea and patella also differ in terms of biomechanics as well as associated anatomic risk factors for patellofemoral instability. 18 A recent case-control study evaluated the influence of anatomic risk factors in patients with isolated focal patellofemoral cartilage lesions. 1 The authors found that trochlear lesions were more frequent in men, presented at an older age, and had fewer associated anatomic risk factors, while patellar lesions, conversely, were more frequent in women, presented at a younger age, and were more closely associated with anatomic risk factors such as a shallower trochlea or patellar abnormalities (small patellar width). These findings are in line with those of the current study, which also found a higher number of associated patellofemoral procedures in the patellar group compared with the trochlear group. Nevertheless, the higher number of associated patellofemoral procedures, including lateral release, trochleoplasty, and realignment procedures, seemed to not significantly affect the clinical results, as previously reported in the literature, 34 and thus, it does not justify the significant differences observed between the 2 cartilage sites. Similarly, the different surgical approaches for the 2 areas, arthroscopic for trochlear lesions and open for patellar lesions, only affect short-term results, as previously documented in a study comparing arthroscopic and open MACT techniques, while no differences were detected at longer follow-up, regardless of the surgical approach. 21 The significantly higher number of female patients in the patellar group could be another important factor in determining different clinical outcomes between the 2 anatomic regions, although, more than biological differences, this seems to be rather explained by the more common unfavorable conditions in women related to the cause of injury, lesion site, and activity level. 12
Regardless of the different results obtained with trochlear and patellar lesions, both sites presented significant improvements on all evaluations up to the last follow-up. The long-term follow-up represents the greatest strength of this study, which analyzed patients with patellofemoral cartilage lesions treated with MACT at a minimum 15 years of follow-up. A long-term evaluation is particularly important for these patients because they are often young at the time of surgery and need to recover and maintain an active lifestyle over many years. A recent systematic review identified 10 studies evaluating cartilage restoration procedures to treat patellar chondral defects, documenting a maximum follow-up of 91 months. 33 Another study reported clinical results after MACT for patellofemoral chondral lesions up to 10 years of follow-up, reporting durable benefits and a low surgical failure rate (3.1%). 22 In the current study, a longer mean follow-up of 17.6 years allowed us to document a slight, albeit not significant, worsening in terms of clinical outcomes and sport activity level from 10 years to the last evaluation, even though the clinical status remained higher compared with that at the time of surgery. A progressive worsening over time has already been documented after long-term follow-up for other cartilage procedures, probably because of the reduced function of patients in relation to advancing age or to the natural evolution of the disease, and the less satisfactory results over time should be emphasized in particular for patellar lesions.6,10,19 Moreover, the clinical worsening could be caused by a possible deterioration in the tissue quality of regenerated cartilage, which has been reported by other authors based on magnetic resonance imaging (MRI). 8 Rosa et al 29 documented a significant decrease in the MOCART (magnetic resonance observation of cartilage repair tissue) score from short-term to long-term follow-up in 10 patients with knee chondral lesions treated with first-generation autologous chondrocyte implantation. Ebert et al 8 observed a significant deterioration in the parameters of tissue structure and subchondral lamina after a minimum of 10 years in patients with patellofemoral or tibiofemoral cartilage defects treated with matrix-induced autologous chondrocyte implantation, although the authors did not document a significant association between MRI findings and the clinical outcomes.
In this long-term study, despite the slight clinical worsening observed at the last evaluation, clinical scores at >15 years of follow-up remained higher compared with those at baseline, thus supporting the efficacy and durable results of MACT for the treatment of both trochlear and patellar cartilage lesions. Stable results in terms of joint status were confirmed by the low failure rate. Moreover, all the documented failures occurred earlier (from 5 to 7 years), while no failures were documented later. Previous studies have reported that MACT can offer good and long-lasting results at long-term follow-up for condylar cartilage lesions.3,15 Gille et al 15 demonstrated good clinical outcomes in a series of 15 knees treated with collagen-based MACT at a mean of 16 years of follow-up. Andriolo et al 3 performed a long-term evaluation of MACT in 113 patients with knee cartilage defects, reporting stable clinical results at up to 15 years of follow-up and a failure rate of 15%. However, condylar lesions have been shown to behave differently than patellofemoral lesions. In the current study focusing on patellofemoral cartilage lesions, MACT resulted in a low rate of failure at long-term follow-up for both the patella and the trochlea, with only 4 patients (9.1%) requiring a new surgical procedure because of symptoms related to the primary defect (reoperation or major revision). This failure rate is slightly higher compared with that in a recent systematic review investigating results after MACT, reporting a 5% failure rate for the patellofemoral joint. 31 However, the shorter follow-up of the assessed studies could explain the higher failure rate obtained in the current study at longer follow-up, which still documents overall good outcomes.
This study presents some limitations. First, it is a case series without a control group to prove the real efficacy of this MACT technique compared with other cartilage treatment strategies and with the natural course of cartilage lesions in terms of clinical results over time. Moreover, the small sample size precluded the possibility of detecting a correlation between final outcomes and prognostic factors, and the lack of imaging with radiography and MRI did not permit us to draw conclusions about the effect of MACT on regenerating the articular surface and preventing or delaying osteoarthritic degeneration. Other limitations of the present study were the lack of an objective evaluation because of the impossibility of all patients attending all follow-up visits. A few patients were dropouts compared with both the previous midterm study and the original series of patients treated. Nevertheless, considering the very long follow-up period (mean of almost 18 years, with some patients exceeding 20 years since treatment), the overall 17% dropout rate can be deemed acceptable. Finally, the comparative analysis between the trochlear and patellar groups could be affected by intergroup differences in terms of sex and associated surgical procedures, with a high number of female patients and associated procedures in the patellar group. Despite these limitations, this study provided useful information on the long-term efficacy of this MACT technique for the treatment of both patellar and trochlear cartilage lesions, demonstrating durable results and a low failure rate for patellofemoral areas as well as documenting lower clinical outcomes with patellar cartilage lesions compared with trochlear cartilage lesions.
Conclusion
This hyaluronic acid–based MACT technique offered positive and durable clinical outcomes with a low failure rate at long-term follow-up in patients affected by patellofemoral cartilage lesions. However, trochlear and patellar lesions demonstrated a notable difference in terms of clinical findings and sport activity level, with significantly better results for patients with trochlear lesions but less satisfactory outcomes for patients with patellar lesions. These 2 patellofemoral sites should not be considered as a single pathological entity in the research setting and in clinical practice, and both physicians and patients should have proper expectations considering that patellar lesions may lead to less satisfactory results after MACT.
Footnotes
Acknowledgements
The authors acknowledge Elettra Pignotti for statistical analysis.
Submitted October 11, 2023; accepted April 3, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.Z. has received personal fees and grants from Fidia Farmaceutici and CartiHeal. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.