
Abstract
Background:
Few previous studies have investigated how different injury mechanisms leading to sport-related concussion (SRC) in soccer may affect outcomes.
Purpose:
To describe injury mechanisms and evaluate injury mechanisms as predictors of symptom severity, return to play (RTP) initiation, and unrestricted RTP (URTP) in a cohort of collegiate soccer players.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
The Concussion Assessment, Research and Education (CARE) Consortium database was used. The mechanism of injury was categorized into head-to-ball, head-to-head, head-to-body, and head-to-ground/equipment. Baseline/acute injury characteristics—including Sports Concussion Assessment Tool–3 total symptom severity (TSS), loss of consciousness (LOC), and altered mental status (AMS); descriptive data; and recovery (RTP and URTP)—were compared. Multivariable regression and Weibull models were used to assess the predictive value of the mechanism of injury on TSS and RTP/URTP, respectively.
Results:
Among 391 soccer SRCs, 32.7% were attributed to a head-to-ball mechanism, 27.9% to a head-to-body mechanism, 21.7% to a head-to-head mechanism, and 17.6% to a head-to-ground/equipment mechanism. Event type was significantly associated with injury mechanism [χ2(3) = 63; P < .001), such that more head-to-ball concussions occurred in practice sessions (n = 92 [51.1%] vs n = 36 [17.1%]) and more head-to-head (n = 65 [30.8%] vs n = 20 [11.1]) and head-to-body (n = 76 [36%] vs n = 33 [18.3%]) concussions occurred in competition. The primary position was significantly associated with injury mechanism [χ2(3) = 24; P < .004], with goalkeepers having no SRCs from the head-to-head mechanism (n = 0 [0%]) and forward players having the least head-to-body mechanism (n = 15 [19.2%]). LOC was also associated with injury mechanism (P = .034), with LOC being most prevalent in head-to-ground/equipment. Finally, AMS was most prevalent in head-to-ball (n = 54 [34.2%]) and head-to-body (n = 48 [30.4%]) mechanisms [χ2(3) = 9; P = .029]. In our multivariable models, the mechanism was not a predictor of TSS or RTP; however, it was associated with URTP (P = .044), with head-to-equipment/ground injuries resulting in the shortest mean number of days (14 ± 9.1 days) to URTP and the head-to-ball mechanism the longest (18.6 ± 21.6 days).
Conclusion:
The mechanism of injury differed by event type and primary position, and LOC and AMS were different across mechanisms. Even though the mechanism of injury was not a significant predictor of acute symptom burden or time until RTP initiation, those with head-to-equipment/ground injuries spent the shortest time until URTP, and those with head-to-ball injuries had the longest time until URTP.
Sport-related concussion (SRC) is an ever-growing public health concern and has been studied extensively in recent decades. Soccer remains among the most popular in the United States among the various youth and collegiate sports.24,37,43 Across the country, it is estimated that 3.9 million children and adolescents participate in soccer every year, with youth participation growing by approximately 90% in the past decade 39 and a 17% increase in collegiate soccer participation over a similar time frame. 37 With a steady increase in soccer participation at both the youth and the collegiate levels and a relatively high SRC incidence relative to other sports,7,28 more studies investigating risk factors and preventive strategies are warranted in the setting of SRC in soccer. 38
Soccer is unique in that aerial challenges, during which players lobby for ball possession using their heads, are an integral component of play. Consequently, the sport presents a wide range of possible mechanisms of injury that may lead to SRC. 38 To identify risk factors for SRC, studies have investigated different mechanisms leading to SRC across a wide range of sports,1,4,13,17 including soccer. 26 In 2021, using data from the Concussion Assessment, Research and Education (CARE) Consortium, Kaminski et al 26 performed a retrospective review of 262 concussed soccer players and found that 67% of SRCs resulted from collisions (ie, collisions with teammate/opponent or tackled by opponent) and unintentional contact (ie, contact with the ball) compared with aerial challenges. Moreover, defenders were more likely than midfielders to sustain concussions during aerial challenges (eg, headers [intentional aerial challenges to obtain possession of the ball] with and without physical contact) than collisions. 26 Bretzin et al 4 found that male high school soccer players most often sustain SRCs from contact with another player, while female players do so more often from nonplayer contact. Similar findings were seen among collegiate athletes, such that male players were 2.29 times more likely to have a concussion involving a collision with another player compared with female counterparts. 29 Finally, several studies have reported that female soccer players experience SRC more frequently from a head-to-ball impact than their male counterparts.3,6,11,12
Although previous studies have presented the frequency and proportion of SRC mechanisms in soccer, few have addressed how the mechanism may affect recovery after injury. One study 46 evaluated injury mechanisms and recovery in various sports and found no differences in recovery among collegiate soccer players based on mechanism. Chandran et al 9 found that mechanism was predictive of time to symptom resolution, with nonplayer-to-player contact having higher odds of greater symptom duration compared with a player-to-player injury mechanism. Given the heterogeneous findings regarding how SRC mechanisms influence outcomes in sports and the limited data focusing exclusively on soccer, we examined this topic in a large cohort of collegiate soccer players from a multi-institutional study. Our objectives were to evaluate the mechanism of injury as a predictor of postinjury symptom severity, days to initiation of return to play (RTP) protocol, and days to unrestricted RTP (URTP).
Methods
Participants
As part of the CARE Consortium, 30 universities took part in a multisite prospective cohort study investigating the natural history (ie, presentation, diagnosis, and recovery) of SRC. 5 The present study included CARE baseline and postconcussion data collected between 2014 and 2020. Before data collection, the local institutional review board and the Human Research Protection Office of each institution approved the study protocol. All participants provided written informed consent. For our study, only soccer-related concussions were included. Only athletes’ first reported SRC during the study period was included—that is, repeat concussions of the same athlete were excluded.
Measures/Procedures
Based on previous literature that investigated the mechanism of injury leading to SRCs across various sports,3,4,6,12,26,46 contact mechanism was defined as what a player collided with at the time of injury and categorized into 4 domains based on free text data entry: head-to-ball, head-to-head, head-to-body, and head-to-ground/equipment. An independent study personnel collected all information regarding the mechanisms and were present at each practice and competition at the time of the injury. Self-reported information collected at baseline were as follows: sex, player position, concussion history, diagnosis of attention deficit hyperactivity disorder (ADHD), preinjury history of migraine headaches, and/or psychiatric disorders. Athletes who were suspected of sustaining an SRC were immediately removed from play and evaluated/diagnosed by the local health care team at the participating site based on current concussion consensus guidelines. 5 The providing health care team reported acute injury characteristics—that is, event type, altered mental status (AMS), and loss of consciousness (LOC). Event type (game/practice), AMS (yes/no), and LOC (yes/no) were recorded as a binary variable.31,33,40 Durations of AMS and LOC for those who experienced AMC/LOC were recorded. 34 AMS refers to any period of alterations in cognition, consciousness, or awareness, often accompanied by symptoms such as confusion and retrograde/anterograde amnesia,2,41 and LOC refers to a temporary and abrupt disruption of responsiveness after injury.16,27,41 All postinjury Sports Concussion Assessment Tool–3 (SCAT3) total symptom severity (TSS) scores were recorded within 48 hours of injury. Total SCAT3 TSS scores were calculated using a 22-item self-reported measure recording symptom severity on a 7-point Likert scale 30 (range, 0-132) at the time the RTP protocol began and again when the athlete was cleared for URTP. Finally, recovery outcomes included days to initiation of RTP protocol (reintroduction of gradual physical activity) and URTP.
Statistical Analysis
Descriptive and postinjury data were examined using descriptive statistics—counts/percentages for categorical variables and means/standard deviations or medians/interquartile ranges for continuous variables. Pearson chi-square tests—or Fisher exact tests when appropriate—were conducted to examine associations between categorical variables and injury mechanisms. SCAT3 TSS, days to initiation of RTP, and days to URTP followed a nonparametric distribution; therefore, Kruskal-Wallis tests were used to examine potential differences across injury mechanisms.
Multivariable negative binomial regression was used to examine the association (evaluated as ratios) between the injury mechanism and the SCAT3 TSS (adjusting for covariate effects) because the SCAT3 TSS was observed to be notably overdispersed. Covariates in this model were determined based on previous studies that investigated mechanisms in soccer6,26,46 and included sex (women [reference variable], men), history of concussions (none [reference variable], ≥1), history of psychiatric disorders (no [reference variable], yes), history of migraine headache (no [reference variable], yes), history of ADHD (no [reference variable], yes), event type (competition [reference variable], practice), primary position (defensive back [reference variable], forward [attack], goalkeeper, midfielder), LOC (no [reference variable], yes), and AMS (no [reference variable], yes). The SCAT3 TSS assessment time point was added as a covariate but was removed, as it did not reach statistical significance.
Univariate and multivariable survival analytic techniques were used to examine the effect of the injury mechanism on SRC recovery. Separate Kaplan-Meier curves (with medians and interquartile ranges) were constructed to examine recovery trajectories for each of the 2 SRC recovery endpoints—initiation of RTP protocol and URTP. In addition, log-rank tests were used to evaluate differences in the median time to the endpoints across injury mechanisms. To examine the effect of injury mechanism on recovery—that is, time to initiation of RTP protocol and URTP—2 separate accelerated failure time models with Weibull distributions were constructed. 8 The Weibull distribution was selected because this probability distribution possesses monotonic qualities. Covariates included in the negative binomial regression were also included in these 2 models, along with postinjury SCAT3 TSS. Effect estimates, with corresponding 95% CIs, excluding 1, were deemed statistically significant at the .05 level. Data management and all analyses were conducted using the R Foundation for Statistical Programming Version 4.2.1.
Results
Sample Description
During the study period, 5485 SRCs across all sports were reported. Records were excluded if they were not the athlete's first reported concussion during the study period, were attributed to SRCs outside of soccer, or had missing data. Figure 1 shows a detailed CONSORT (Consolidated Standards of Reporting Trials) participant flow diagram.
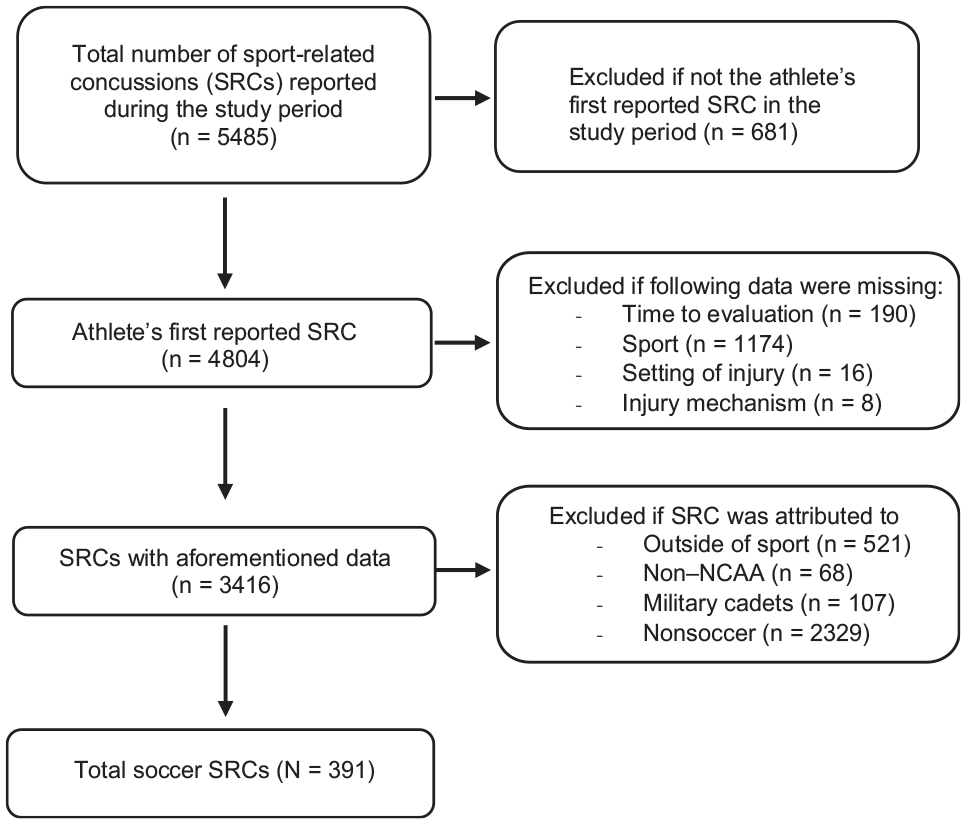
CONSORT (Consolidated Standards of Reporting Trials) diagram of participant flow. NCAA, National Collegiate Athletic Association.
Among a total of 391 soccer SRCs included, 56.8% were women, and 32.7% were attributed to a head-to-ball mechanism, 27.9% to a head-to-body mechanism, 21.7% to a head-to-head mechanism, and 17.6% to a head-to-ground/equipment mechanism. Concussion history, history of psychiatric disorder, history of preinjury migraine headaches, and history of ADHD (P > .05) did not significantly differ based on SRC mechanisms. Baseline SCAT3 TSS varied significantly across injury mechanisms [χ2(3) = 11; P = .013) (Table 1).
Comparisons of Baseline and Injury Characteristics by Injury Mechanism a
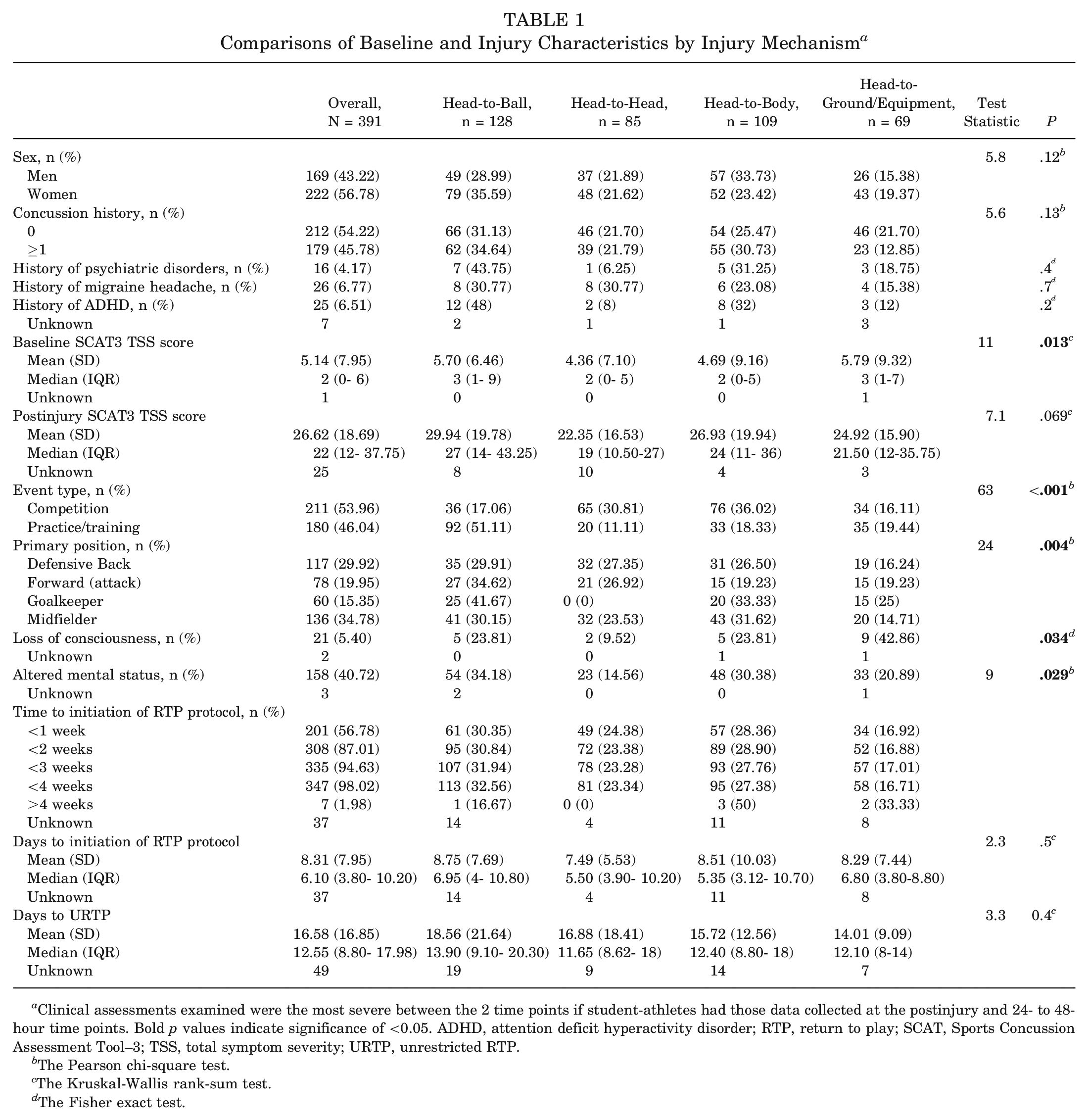
Clinical assessments examined were the most severe between the 2 time points if student-athletes had those data collected at the postinjury and 24- to 48-hour time points. Bold p values indicate significance of <0.05. ADHD, attention deficit hyperactivity disorder; RTP, return to play; SCAT, Sports Concussion Assessment Tool–3; TSS, total symptom severity; URTP, unrestricted RTP.
The Pearson chi-square test.
The Kruskal-Wallis rank-sum test.
The Fisher exact test.
Postinjury Characteristics
The median immediate postinjury SCAT3 TSS was 22 (12-37.75) and was comparable across injury mechanisms (P = .069) (Table 1). Event type was significantly associated with injury mechanism [χ2(3) = 63; P < .001], such that more head-to-ball injuries were seen in practice versus competition (n = 92 [51.11%] vs n = 36 [17.06%]), whereas more head-to-head (n = 65 [30.81%] vs n = 20 [11.11%]) and head-to-body (n = 76 [36.02%] vs n = 33 [18.33%]) injuries occurred in competition (Table 1). Sex was not significantly associated with the mechanism of injury (P = .12). Primary position was associated considerably with the mechanism of injury [χ2(3) = 24; P < .004], such that goalkeepers had no SRCs from a head-to-head mechanism (n = 0 [0%]) and forward players had the least from a head-to-body mechanism (n = 15 [19.23%]) compared with other player positions; both positions had the highest prevalence of SRCs from the head-to-ball mechanism. LOC was also significantly associated with mechanism (P = .034), most prevalently in the head-to-ground/equipment mechanism (n = 9 [42.86%]). Finally, AMS was significantly different across mechanisms (P = .029), such that AMS was most prevalent in head-to-ball (n = 54 [34.18%]) and head-to-body (n = 48 [30.38%]) mechanisms. Of athletes who endorsed AMS (n = 158), the mean (standard deviation) symptom duration in days was 6.79 (6.23), and the median (IQR range) symptom duration in days was 5 (3-8 days). Of athletes who endorsed LOC (n = 18), the mean (standard deviation) of LOC duration in seconds was 16.61 (17.76 sec), and the median (IQR range) of LOC duration in seconds was 10 (5-20 sec).
In the multivariable negative binomial regression model, the injury mechanism was not observed to be a predictor of TSS (P = .3) (Table 2). Sex was a predictor of TSS, and men had a lower TSS than women (ratio, 0.81 [95% CI, 0.69-0.96]; P = .013). In addition, the presence of AMS was shown to be a significant predictor of higher TSS (ratio, 1.20 [95% CI, 1.01-1.41]; P = .036) relative to injuries without AMS.
Multivariable Negative Binomial Regression Modeling Predictors of Postinjury SCAT3 TSS a
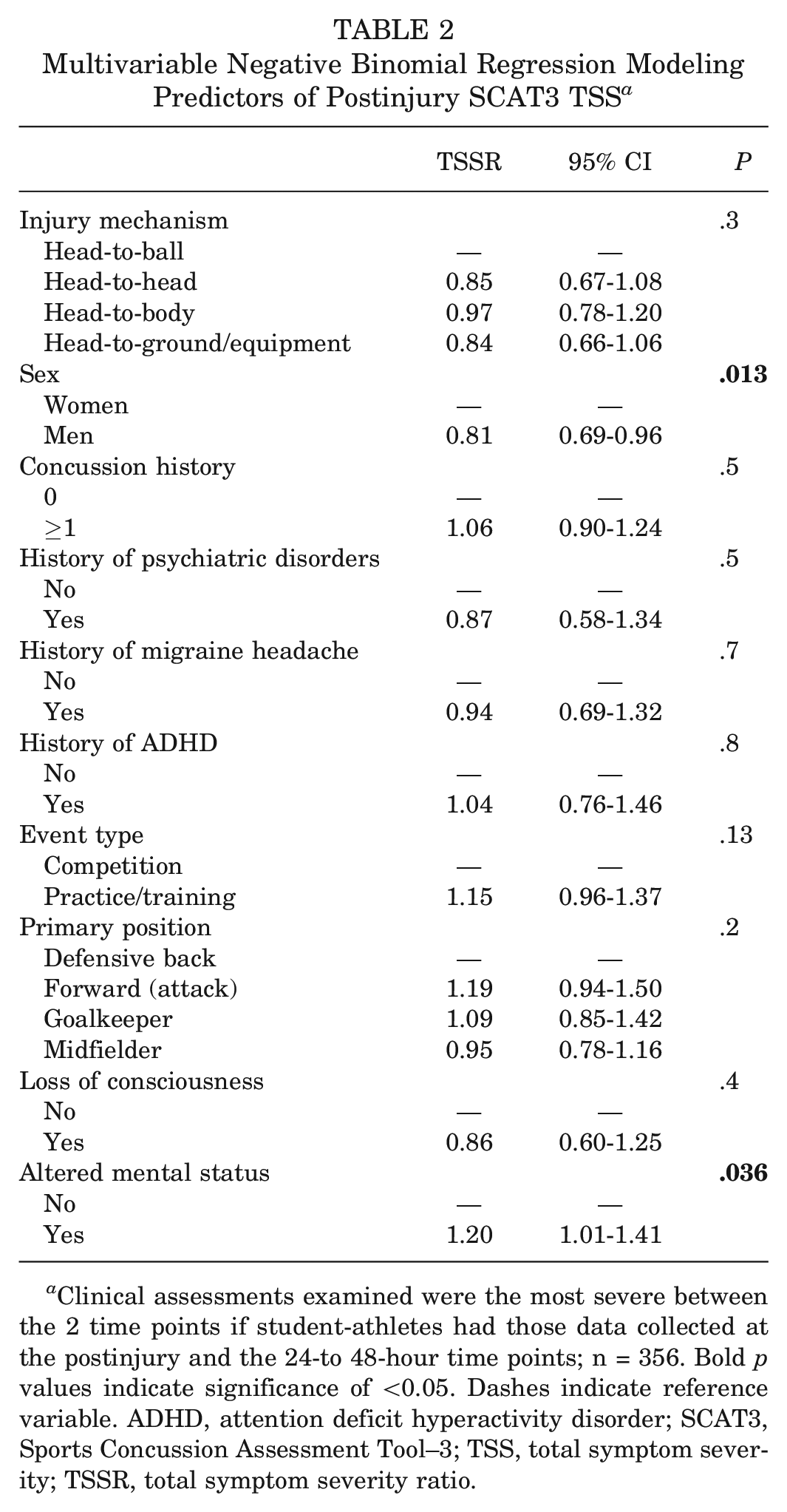
Clinical assessments examined were the most severe between the 2 time points if student-athletes had those data collected at the postinjury and the 24-to 48-hour time points; n = 356. Bold p values indicate significance of <0.05. Dashes indicate reference variable. ADHD, attention deficit hyperactivity disorder; SCAT3, Sports Concussion Assessment Tool–3; TSS, total symptom severity; TSSR, total symptom severity ratio.
Recovery
Kruskal-Wallis rank sum tests showed that days to initiation of RTP protocol [χ2(3) = 2.3; P > .05] and days to URTP [χ2(3) = 3.3; P > .05] were comparable across injury mechanisms (Table 1). Kaplan-Meier estimates for days to initiation of RTP and URTP across mechanisms are shown in Figure 2. Parameter estimates with corresponding 95% CIs from the final Weibull Accelerated Failure Time models for the time to initiation of RTP protocol and the time to URTP are shown in Tables 3 and 4. The injury mechanism was not associated with the time spent recovering to initiate the RTP protocol (P = .2) (Table 3). Significant covariates were as follows: history of ADHD (P = .016), event type (P = .030), LOC (P = .012), AMS (P = .006), and TSS (P < .001). The injury mechanism was associated with the time spent recovering until URTP (P = .044) (Table 4). The estimated time to being cleared for URTP was 26% lower for SRCs attributed to head-to-ground/equipment contact (parameter estimates, −0.30 [95% CI −0.57 to −0.04). Event type (P = .003) and postinjury SCAT3 TSS (P = .004) were the only 2 significant covariates.
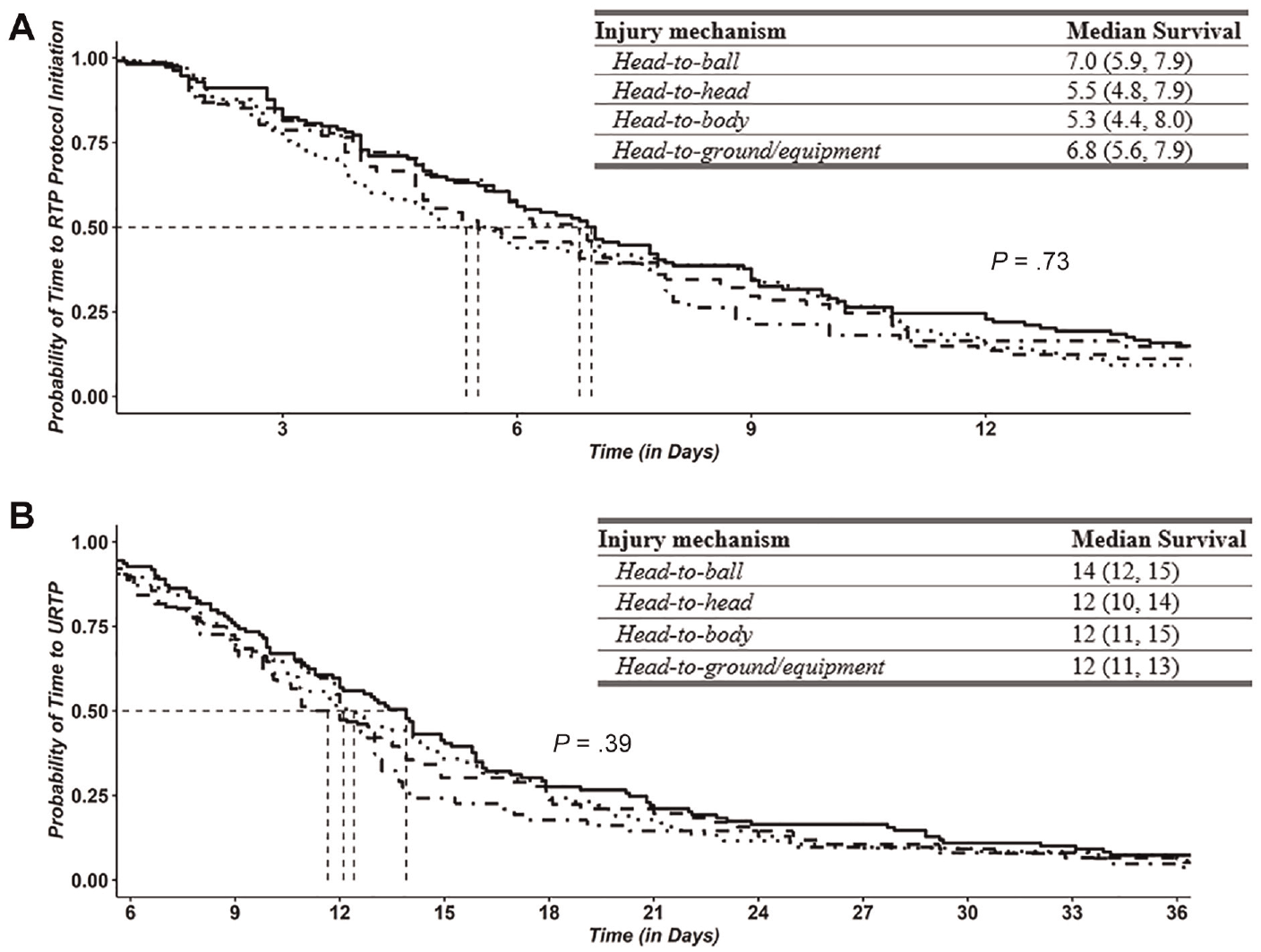
Kaplan-Meier estimates (median, 95% CIs) for (A) the time (days) to initiation of the RTP protocol, and (B) the time (days) to URTP time across injury mechanisms (head-to-ball, head-to-head, head-to-body, and head-to-ground/equipment). Log-rank tests assessed statistical differences in days to events for the 2 aforementioned sport-related concussion recovery endpoints. The solid line shows head-to-ball, the dashed line shows head-to-head, the dotted line shows head-to-body, and the dashed and dotted line shows head-to-ground/equipment. RTP, return to play; URTP, unrestricted return to play.
Parameter Estimates for Relative Changes in Time Spent Injured From the Final Survival Model of Time Spent Injured to the RTP Protocol Initiation Using a Weibull Distribution for Survival Times a
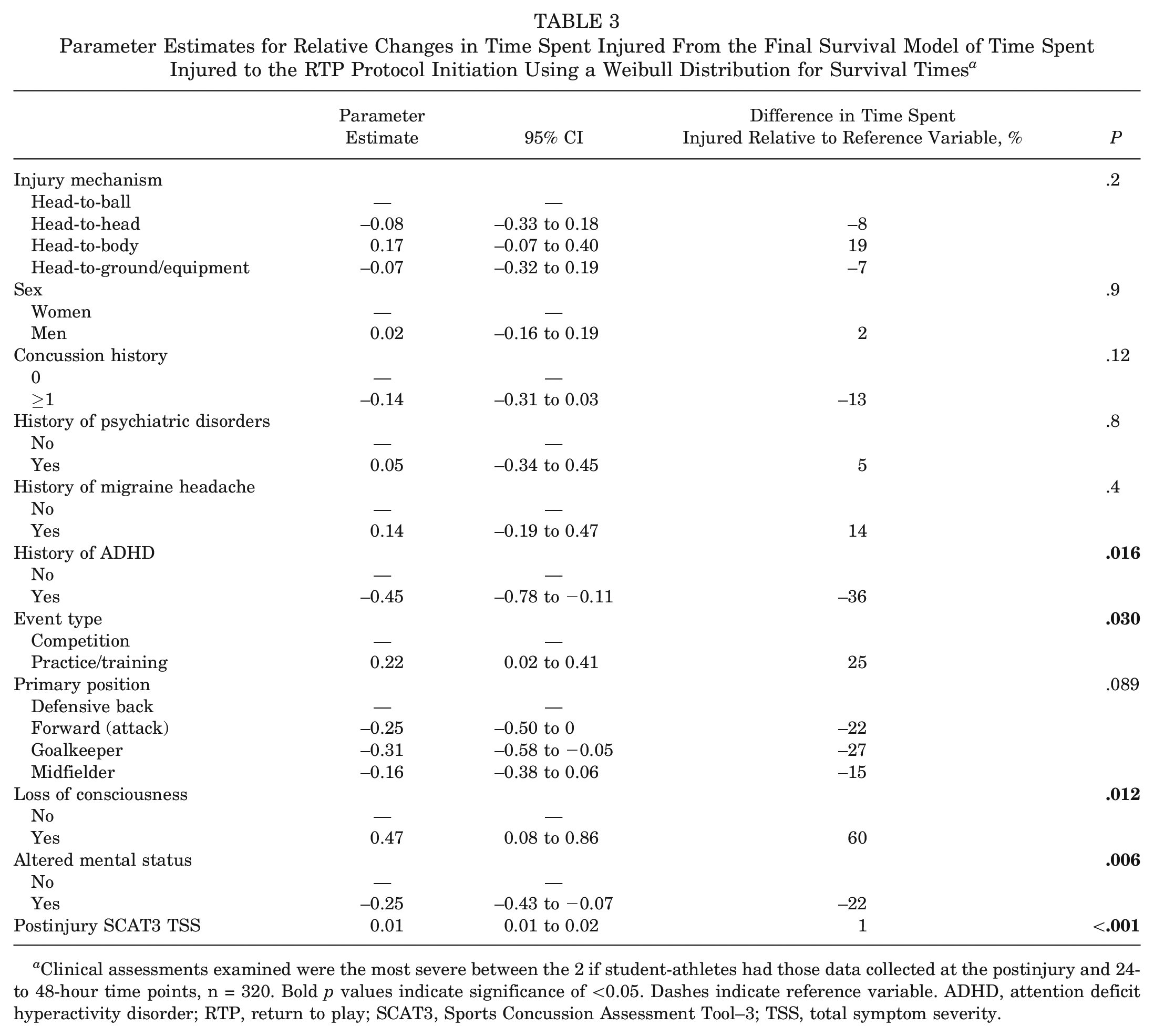
Clinical assessments examined were the most severe between the 2 if student-athletes had those data collected at the postinjury and 24- to 48-hour time points, n = 320. Bold p values indicate significance of <0.05. Dashes indicate reference variable. ADHD, attention deficit hyperactivity disorder; RTP, return to play; SCAT3, Sports Concussion Assessment Tool–3; TSS, total symptom severity.
Parameter Estimates for Relative Changes in Time Spent Injured From the Final Survival Model of Time Spent Injured to URTP Using a Weibull Distribution for Survival Times a
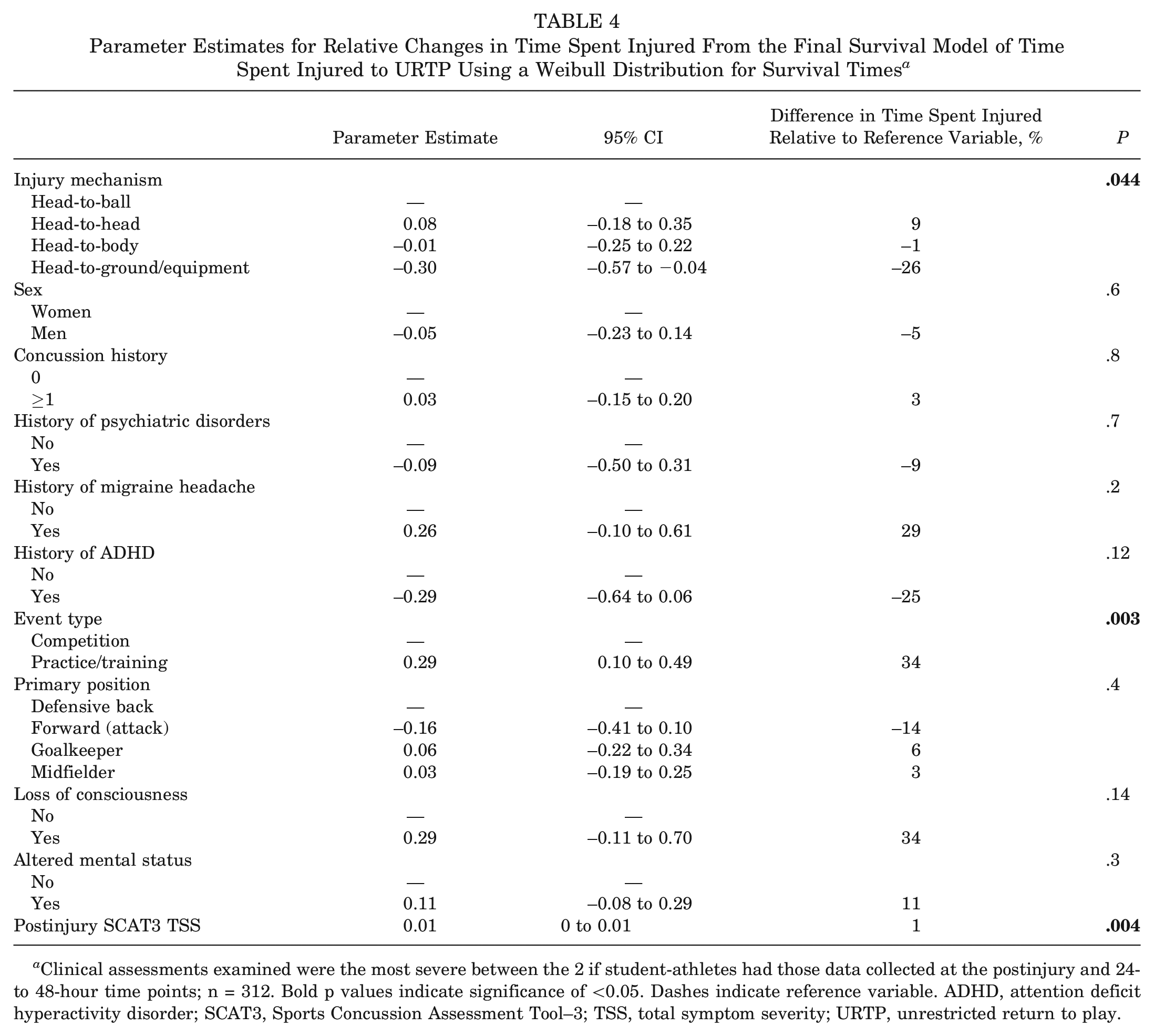
Clinical assessments examined were the most severe between the 2 if student-athletes had those data collected at the postinjury and 24- to 48-hour time points; n = 312. Bold p values indicate significance of <0.05. Dashes indicate reference variable. ADHD, attention deficit hyperactivity disorder; SCAT3, Sports Concussion Assessment Tool–3; TSS, total symptom severity; URTP, unrestricted return to play.
Discussion
The present study evaluated initial SRC presentation and recovery based on injury mechanisms in a large cohort of male and female soccer players. Our analyses showed more head-to-ball injuries in practice, while more head-to-head and head-to-body injuries occurred in competition. There were no differences in mechanisms based on sex. Goalkeepers had no SRCs from a head-to-head mechanism, and forward players had the least head-to-body SRCs, but both positions had the most SRCs from a head-to-ball mechanism relative to other positions. LOC was most prevalent in head-to-ground/equipment mechanisms, and AMS was most common in head-to-ball and head-to-body mechanisms. The mechanism did not predict acute symptom burden or days to initiation of RTP. Finally, the mechanism was a significant predictor of URTP, such that those with head-to-equipment/ground injuries had the shortest time to URTP and athletes with the head-to-ball mechanism had the longest time to URTP. To our knowledge, our study is the first to investigate exclusively in collegiate soccer how different SRC mechanisms may contribute to varying RTP and URTP after injury.
The mechanism of injury varied based on practice versus competition, such that more head-to-ball injuries were seen in practice, while more head-to-head and head-to-body injuries occurred in competition. Competition may incite more aggressive play with higher intensity,20,45 leading to more collisions among players within and between teams, as head-to-body typically results from head colliding with another player's elbow or knee during contact. More head-to-head mechanisms may also mean that more aerial challenges are attempted during practice. However, it is important to note that the exposure metric (eg, per athlete exposure, per practice/game session by minute) was not calculated; therefore, our results do not directly compare the likelihood of these injuries between game versus practice. Regarding sex, previous studies have noted differences in injury mechanisms,4,26 such that female players were more likely than their male counterparts to sustain SRC from nonplayer contact (eg, head-to-ball) versus player contact (eg, head-to-body). However, we did not find any differences in mechanism based on sex, although sex was noted to be a significant predictor of acute symptom burden. Sex was not a significant predictor of outcomes in both initiation to RTP and URTP.
Regarding mechanism and player positions, our results indicate that goalkeepers had no SRCs from a head-to-head mechanism and forward players had the least from a head-to-body mechanism, but both positions had the most SRCs from a head-to-ball mechanism. Kaminski et al 26 found that collegiate soccer SRCs resulting from collision mechanisms were less likely in forwards and goalkeepers compared with midfielders and defenders. Although our categorization of mechanisms differed from efforts of Kaminski et al (collisions vs unintentional contact vs aerial challenges), the overarching findings seem consistent and suggest that forwards and goalkeepers are less prone to SRC from contact with other players. Goalkeepers and forwards, positions that typically spend less time moving across the field when compared with midfielders and defenders, may expose themselves less to physical contact with other players moving at high speeds on the soccer field. Forwards specifically focus on goal scoring, whereas midfielders and defenders often challenge opposing players to obtain possession of the ball. Goalkeepers can certainly collide with other players, but they rarely need to use their heads during play and can use their hands to gain possession of the ball, thereby protecting their heads from injury.
The present study represents a novel effort to characterize AMS and LOC as a function of mechanisms of injury in soccer. Chandran et al, 10 in a retrospective cohort of 9542 high school athletes with SRCs across 20 different sports, found that a higher percentage of person-to-person contacts showed confusion/disorientation (34.4% vs 38.7%; P < .001) and difficulty concentrating (54.1% vs 57%; P = .009), comparable with AMS, compared with non–person to person contact. However, no differences were noted for LOC between these mechanisms, although sample heterogeneity may have influenced this finding. Our study found that LOC was most prevalent in head-to-ground/equipment mechanisms. Ground/equipment represents stationary entities in the soccer field, including the ground, goalpost, and bleachers, all of which, we hypothesize, may present hard, unforgiving surfaces when compared with the ball or the human body. In addition, compared with head-to-ball or player-to-player mechanisms, where a player could have been more aware of the incoming contact (eg, seeing the incoming tackle, intentional aerial challenges), head-to-ground/equipment could have constituted injuries that were unforeseen to the player. LOC has been previously explored as a potential indicator of worse injury severity in the acute setting of SRC, yet findings remain equivocal.18,35,36 A meta-analysis of 31 studies 18 revealed that athletes who experienced LOC had worse neuropsychological functioning at 10 days of SRC compared with those who did not experience LOC, but other studies36,42 did not find an association between LOC and acute postconcussion symptoms. Fewer studies42,47 have investigated LOC as a predictor of recovery and have found no significant associations. Chandran et al, 9 focusing exclusively on SRCs among high school players, found that the mechanism of injury was not associated with acute symptoms after SRC. Using a collegiate athlete cohort, we broach the idea that while mechanisms of injury can determine injury characteristics (ie, LOC and AMS), they may not greatly affect overall total symptomology acutely after injury.
Regarding outcomes, the mechanism of injury was predictive of days to URTP, such that the head-to-ground had the shortest recovery while the head-to-ball had the longest, which presents interesting and somewhat unexpected findings. First, the head-to-equipment/ground mechanism was shown to have the shortest time to URTP—the same mechanism that was earlier shown to have the highest prevalence of LOC. Second, the mechanism was not predictive of TSS in our earlier regression. Given the well-established relationship between acute symptom burden and recovery after concussion,21-23,25,44 this is an interesting finding. One potential explanation may be attributed to the heterogeneity of the ground/equipment category, which encompasses a wide range of entities from ground to bleachers and presents a large range of injury mechanisms. Previous retrospective cohort studies examining concussions in soccer did not find differences in the time to symptom resolution based on both contact mechanism (ground/equipment vs head vs player nonhead [any other body part besides the head] as well as head vs body)17,46 and player mechanism (player action during the time of injury; offensive ball carrying vs challenging ball/loose ball vs header). 46 However, another study 9 focusing specifically on high school soccer players, found that mechanism was associated with time to symptom resolution, with nonplayer-to-player contact having higher odds of a greater symptom duration compared with player-to-player contact. Our findings suggest that contact mechanism may be a significant predictor of URTP, depending on how the mechanism is defined operationally.
Notable differences exist in the categorization of mechanisms among the previously mentioned studies. Future efforts could incorporate advanced technology such as videography techniques and head impact accelerometry, which may provide valuable insight into the acute injury mechanisms and their relation to outcomes through a more consistent data collection.14,15,19,46 Furthermore, additional characterization of the specific dynamics, critical measures, and kinematics of the head impact that led to a concussion (eg, force, area of contact, location of the head, and acceleration) may help elucidate nuanced similarities and differences between each mechanism of injury (eg, head-to-ball vs head-to-head). Understanding injury mechanisms and their association with outcomes is an important topic in the SRC literature, as it may help inform clinical practice and provide guidance on education, policy changes, and preventive strategies for athletes, coaches, and sports organizations.
This study has some limitations. First, we were limited in our categorization of the injury mechanism because of the retrospective nature of our analyses. In addition, even though there are many ways to categorize mechanisms, previous literature that investigated injury mechanisms across various sports was referenced when designing the methods for this study.3,4,6,12,26,46 For instance, for the head-to-ball mechanism, the way data were collected did not differentiate between headers/aerial challenges, which are intentional and unintentional hit to the head by a ball. For head-to-head, it is unclear which concussions were from aerial duels versus head-to-head resulting from other contact. In addition, we understand that the head-to-ground/equipment mechanism may represent a heterogeneous group, combining those who collided with the ground with those who collided with other objects (eg, goalpost, bleachers). In addition, while only 1 mechanism was assigned per athlete, multiple mechanisms may have been experienced at the time of injury and some mechanisms may have been missed by the independent study personnel (eg, during the contest for the ball in the air [head-to-ball], head-to-body control may have also occurred). Finally, the head-to-ball mechanism may not only occur during intentional heading but also may encompass mechanisms involving unintentional contact of the athlete's head to a ball. Second, given that this is a multicenter study, we acknowledge that subtle variability in clinical care, protocols for RTP initiation, and clearance for URTP between institutions may be present. However, the variability increases the external validity of our findings. Third, the timing of the year during which the SRC occurred for each athlete was not specified, and we recognize that the pace and urgency of management may vary based on the timing of injury during a season. Fourth, our analyses did not include the following variables: time to reporting and early/late exercise after SRC. 32 All our athletes had their TSS scores recorded within 48 hours of injury. Although early/late exercise during the recovery phase 32 is an interesting variable, this was beyond the scope of our study. For instance, a player with the head-to-ground/equipment mechanism may have also collided with another player before hitting the ground. However, these limitations may be inevitable until videography techniques are incorporated into the study design.14,15,19 Previous lifetime history of concussion was not included for every athlete in our multivariable models, and this may have influenced acute presentation and recovery. Finally, as previously discussed, this study represents an original effort to explore the influence of various SRC mechanisms on recovery patterns as a function of RTP in a large cohort of collegiate soccer players. An important aspect to note is that, because of the novelty of some of our findings, certain results may not be immediately interpretable in both the biomechanical and the clinical contexts. Nevertheless, we believe that these results provide a valuable platform for future research efforts, which may help give more relevance and context to the findings in this study.
Conclusion
A multicenter, prospective cohort study examining concussions in soccer showed several noteworthy trends. Although more head-to-ball injuries were seen in practice, more head-to-head and head-to-body injuries occurred in competition. Goalkeepers had the least number of SRCs from the head-to-head mechanism, and forwards had the least number of SRCs from the head-to-body mechanism. LOC was most prevalent in head-to-ground/equipment mechanisms, and AMS was most common in head-to-ball and head-to-body mechanisms. The mechanism of injury did not significantly predict acute symptom burden; however, the head-to-ground mechanism had a shorter recovery to URTP, while the head-to-ball mechanism had the longest. The present study represents a novel effort to explore the influence of SRC mechanisms on recovery in a large cohort of collegiate soccer players and provides a valuable platform for future efforts. Understanding the mechanisms of SRCs and their associations with symptoms and recovery can benefit health care professionals, coaches, and athletes in the assessment, management, and prevention of concussions in soccer, ultimately improving the safety and well-being of players.
Authors
Jacob Jo, BA (Department of Neurological Surgery, Vanderbilt Sports Concussion Center, Vanderbilt University Medical Center, Nashville, Tennessee, USA; Department of Neurological Surgery, Vanderbilt University Medical Center, Nashville, Tennessee, USA; Vanderbilt University School of Medicine, Nashville, Tennessee, USA); Adrian J. Boltz, MSH (Michigan Concussion Center, University of Michigan, Ann Arbor, Michigan, USA); Kristen L. Williams, MS, LAT, ATC (Department of Neurological Surgery, Vanderbilt Sports Concussion Center, Vanderbilt University Medical Center, Nashville, Tennessee, USA; Department of Neurological Surgery, Vanderbilt University Medical Center, Nashville, Tennessee, USA); Paul F. Pasquina, MD (Department of Physical Medicine and Rehabilitation at the Uniformed Services University of the Health Sciences in Bethesda, Maryland, USA); Thomas W. McAllister, MD (Department of Psychiatry, Indiana University School of Medicine, Indianapolis, Indiana, USA); Michael A. McCrea, PhD, ABPP (Department of Neurosurgery, Medical College of Wisconsin, Milwaukee, Wisconsin, USA; Department of Neurology, Medical College of Wisconsin, Milwaukee, Wisconsin, USA); Steven P. Broglio, PhD, ATC (Michigan Concussion Center, University of Michigan, Ann Arbor, Michigan, USA); Scott L. Zuckerman, MD, MPH (Department of Neurological Surgery, Vanderbilt Sports Concussion Center, Vanderbilt University Medical Center, Nashville, Tennessee, USA; Department of Neurological Surgery, Vanderbilt University Medical Center, Nashville, Tennessee, USA); Douglas P. Terry, PhD (Department of Neurological Surgery, Vanderbilt University Medical Center, Nashville, Tennessee, USA; Department of Neurological Surgery, Vanderbilt University Medical Center, Nashville, Tennessee, USA; Vanderbilt University Medical Center, Nashville, Tennessee, USA); and CARE Consortium Investigators, listed alphabetically by last name: Kristy Arbogast, PhD (University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania, USA); Holly J. Benjamin, MD (University of Chicago, Chicago, Illinois, USA); Alison Brooks, MD (University of Wisconsin–Madison, Madison, Wisconsin, USA); Kenneth L. Cameron, PhD (United States Military Academy, West Point, New York, USA); Sara P.D. Chrisman, MD (University of Washington, Seattle, Washington, USA); James R. Clugston, MD (University of Florida, Gainesville, Florida, USA); Micky Collins, PhD (University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA); John DiFiori, MD (Hospital for Special Surgery, New York, New York, USA); James T. Eckner, MD, MS (University of Michigan, Michigan, USA); Carlos Estevez, DPT (United States Coast Guard Academy, New London, Connecticut, USA); Luis A. Feigenbaum, PT, DPT, ATC, LAT (University of Miami, Coral Gables, Florida, USA); Joshua T. Goldman, MD (University of California, Los Angeles, Los Angeles, California, USA); April Hoy, MS (Azusa Pacific University, Azusa, California, USA); Thomas W. Kaminski, PhD (University of Delaware, Newark, Delaware, USA); Louise A. Kelly, PhD (California Lutheran University, Thousand Oaks, California, USA); Anthony P. Kontos, PhD (University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA); Dianne Langford, PhD (Temple University, Philadelphia, Pennsylvania, USA); Laura J. Lintner, DO (Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA); Christina L. Master, MD (University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania, USA); Jane McDevitt, PhD (Temple University, Philadelphia, Pennsylvania, USA); Gerald McGinty, PT (United States Air Force Academy, El Paso, Colorado, USA); Chris Miles, MD (Wake Forest University, Winston-Salem, North Carolina, USA); Justus Ortega, PhD (California State Polytechnic University, Pomona, California, USA); Nicholas Port, PhD (Indiana University, Bloomington, Indiana, USA); Steve Rowson, PhD (Virginia Tech, Blacksburg, Virginia, USA); Julianne Schmidt, PhD, ATC (University of Georgia, Athens, Georgia, USA); Adam Susmarski, DO (United States Naval Academy, Annapolis, Maryland, USA); and Steven Svoboda, MD (MedStar Health, Columbia, Maryland, USA).
Footnotes
Acknowledgements
The authors thank Jody Harland, Janetta Matesan, and Michael Menser (Indiana University School of Medicine); Ashley Rettmann and Nicole L’Heureux (University of Michigan); Melissa McEachern (Medical College of Wisconsin); Michael Jarrett, Vibeke Brinck, and Bianca Byrne (Quesgen); Melissa Baker, Christy Collins, Will Felix, and Bethany Morath, (Datalys Center for Sports Injury Research and Prevention); and the research and medical staff at each of the CARE participation sites. The authors are grateful for the participation of the student-athletes, without whom this research would not be possible.
Submitted August 25, 2023; accepted February 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This project was supported, in part, by the Grand Alliance Sport-Related Concussion Assessment, Research, and Education (CARE) Consortium, funded, in part by the National Collegiate Athletic Association (NCAA) and the DoD. The U.S. Army Medical Research Acquisition Activity is the awarding and administering acquisition office. This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs through the Psychological Health and Traumatic Brain Injury Program under award No. W81XWH-14-2-0151. A.J.B. has been part of projects that have received funding from the DoD, the National Operating Committee on Standards from Athletic Equipment, the National Athletic Trainer's Association (NATA) Research and Education Foundation, and the NCAA. P.F.P. is an employee of the DoD and has previously received other DoD-related grants. T.W.M. has received research support from the NCAA, the US DoD, and the National Institutes of Health (NIH). He also reports textbook royalties from American Psychiatric Press Publishing Inc and serves on the Concussion Committee Scientific Advisory Board for the Australian Football League. M.A.M. has received research funding from the NIH, the Centers for Disease Control and Prevention (CDC), the DoD, the NCAA, the National Football League (NFL), and Abbott Laboratories. S.P.B. has received research funding from the NIH, the CDC, the DoD-USA Medical Research Acquisition Activity, the NCAA, the NATA Research and Education Foundation, the NFL/Under Armour/GE, Simbex, and ElmindA. He has consulted for US Soccer, US Cycling, the University of Calgary SHRed Concussions external advisory board, and medicolegal litigation. S.L.Z. is a member of the NFL Head, Neck, and Spine Committee. D.P.T. serves as a scientific advisor for HitIQ. He previously consulted for REACT Neuro Inc. He has a consulting practice in forensic neuropsychology, including expert testimony, involving individuals who have sustained mild traumatic brain injury (including former athletes). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.