
Abstract
Background:
Arthroscopic treatment of femoroacetabular impingement (FAI) and symptomatic labral tears confers short- to midterm benefits, yet further long-term evidence is needed. Moreover, despite the physiological and biomechanical significance of the chondrolabral junction (CLJ), the clinical implications of damage to this transition zone remain understudied.
Purpose:
To (1) report minimum 8-year survivorship and patient-reported outcome measures after hip arthroscopy for FAI and (2) characterize associations between outcomes and patient characteristics (age, body mass index, sex), pathological parameters (Tönnis angle, alpha angle, type of FAI, CLJ breakdown), and procedures performed (labral management, FAI treatment, microfracture).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective cohort study included patients who underwent primary hip arthroscopy for symptomatic labral tears secondary to FAI by a single surgeon between 2002 and 2013. All patients were ≥18 years of age with minimum 8-year follow-up and available preoperative radiographs. The primary outcome was conversion to total hip arthroplasty (THA), and secondary outcomes included revision arthroscopy, patient-reported outcome measures, and patient satisfaction. CLJ breakdown was assessed using the Beck classification. Kaplan-Meier estimates and weighted Cox regression were used to estimate 10-year survivorship (no conversion to THA) and identify risk factors associated with THA conversion.
Results:
In this study of 174 hips (50.6% female; mean age, 37.8 ± 11.2 years) with mean follow-up of 11.1 ± 2.5 years, the 10-year survivorship rate was 81.6% (95% CI, 75.9%-87.7%). Conversion to THA occurred at a mean 4.7 ± 3.8 years postoperatively. Unadjusted analyses revealed several variables significantly associated with THA conversion, including older age; higher body mass index; higher Tönnis grade; labral debridement; and advanced breakdown of the CLJ, labrum, or articular cartilage. Survivorship at 10 years was inferior in patients exhibiting severe (43.6%; 95% CI, 31.9%-59.7%) versus mild (97.9%; 95% CI, 95.1%-100%) breakdown of the CLJ (P < .001). Multivariable analysis identified worsening CLJ breakdown (weighted hazard ratio per 1-unit increase, 6.41; 95% CI, 3.11-13.24), older age (1.09; 95% CI, 1.04-1.14), and higher Tönnis grade (4.59; 95% CI, 2.13-9.90) as independent negative prognosticators (P < .001 for all).
Conclusion:
Although most patients achieved favorable minimum 8-year outcomes, several pre- and intraoperative factors were associated with THA conversion; of these, worse CLJ breakdown, higher Tönnis grade, and older age were the strongest predictors.
Keywords
The acetabular labrum, crucial for hip stability and joint lubrication,16,17,37 is often torn due to femoroacetabular impingement (FAI), a condition characterized by abnormal contact forces between the femoral head (cam) and/or acetabulum (pincer).3,20 If the left untreated, osseous deformities and labral pathologies impede hip biomechanics and synovial fluid dynamics, causing further labral injury; cartilage layer consolidation; and attendant hip symptoms such as groin pain, stiffness, and reduced range of motion (ROM). 44 Nonoperative management remains the first-line treatment and includes activity modification, anti-inflammatory medication, and physical therapy. 47 If these nonoperative modalities fail to relieve symptoms, hip arthroscopy may be considered to treat labral tears, decompress osseous impingement, and address other intra-articular pathologies.
Accumulating evidence has highlighted the potential of hip arthroscopy to improve both symptoms and function in the short- and midterm. However, given the relatively recent increase in the use of hip arthroscopy over the past 2 decades, data regarding long-term survivorship and patient-reported outcome measures (PROMs) are only beginning to emerge.21,31,60 Previous investigations reported overall rates of survivorship (ie, no conversion to total hip arthroplasty [THA]) of 57% to 92% at 10 years and identified older age and more advanced evidence of radiographic (eg, higher Tönnis grade) and/or arthroscopic (eg, higher Outerbridge grade) osteoarthritis as risk factors for failure.6,15,28 Other reported predictors for failure include female sex, extent of labral damage, acetabular chondral lesions requiring microfracture, and joint space narrowing, but additional evidence is needed to inform preoperative risk stratification.8,33,35,59 Notably, although the prognostic value of damage to the articular cartilage and labrum has been explored independently, the clinical implications of injury to the transition zone (ie, chondrolabral junction [CLJ]) between these distinct regions remain unknown.
Although evidence elucidating the biomechanical and physiologic properties of the CLJ continues to increase, the relationship between CLJ breakdown and clinical outcomes after hip arthroscopy for labral pathologies and/or FAI has yet to be explored in available long-term analyses.7,42,45,48 Thus, the purpose of this study was to (1) report minimum 8-year survivorship and PROMs after hip arthroscopy for symptomatic labral tears secondary to FAI and (2) characterize associations between outcomes and patient demographic characteristics (age, body mass index [BMI], sex), pathological parameters (Tönnis angle, alpha angle, type of FAI, CLJ breakdown), and procedures performed (labral management, FAI treatment, microfracture). We hypothesized that CLJ breakdown, older age, osteoarthritis (Tönnis grade >1 or Outerbridge grade >2), and joint space narrowing would predict conversion to THA.
Methods
Patient Sample, Preoperative Assessment, and Study Design
This was a retrospective cohort study of patients undergoing hip arthroscopy by a single surgeon (S.D.M.) between March 2002 and June 2013. This period was chosen to maximize sample size while ensuring minimum 8-year follow-up. During the study period, all patients underwent a stepwise, preoperative assessment that involved hip and pelvic radiographs (including anteroposterior pelvic and Dunn lateral views) and a comprehensive physical examination with labral/FAI provocation testing at the initial office visit. 22 Patients exhibiting positive findings (ie, pain and/or limited ROM in flexion, adduction, and internal rotation or flexion, abduction, and external rotation) underwent further workup with magnetic resonance imaging (MRI; with or without arthrography), diagnostic intra-articular anesthetic/corticosteroid injections, and a minimum 3-month trial of nonoperative management incorporating formal physical therapy. 36 Individuals with persistent hip pain and confirmed labral tears were offered hip arthroscopy. 47
All included patients were ≥18 years of age, underwent hip arthroscopy for the treatment of symptomatic labral tears, completed study surveys ≥8 years after surgery, and were verified to have available preoperative radiographs. Of note, although some included patients did not meet the discrete radiographic criteria for FAI (alpha angle, lateral center-edge angle), all included patients demonstrated impingement symptoms on physical examination (positive flexion, abduction, and external rotation; positive flexion, adduction, and internal rotation; decreased ROM; described above) and therefore met clinical criteria for FAI.22,30 Finally, patients were excluded if they demonstrated radiographic evidence of hip dysplasia (lateral center-edge angle <20°) or had undergone previous ipsilateral hip surgery. 4 Institutional review board approval was obtained (No. 2011P000053). All patients provided informed consent.
Data Collection and Outcomes
Patients were invited to participate in this study if they underwent hip arthroscopy by the senior surgeon (S.D.M.) after March 2002. Participation entailed the completion of telephone or online survey questionnaires regarding subsequent hip surgeries, PROMs, and patient satisfaction. The primary outcome was conversion to THA, ascertained from both patient surveys and independent confirmation using electronic health records. Secondary outcomes included the International Hip Outcome Tool, modified Harris Hip Score, Hip Outcome Score–Activities of Daily Living, Hip Outcome Score–Sports Subscale, Non-Arthritic Hip Score, patient satisfaction surveys, and rates of revision arthroscopy. For comparisons, patients were stratified into cohorts based on conversion to THA during the study period. Baseline characteristics were manually extracted from electronic health records and included age, BMI, sex, race, ethnicity, and laterality. Preoperative radiographs were analyzed to determine Tönnis classification; Tönnis angle; lateral center-edge angle; alpha angle; mean joint space (defined as the mean of the medial, central, and lateral points); and cam, pincer, or mixed FAI morphology. 30 Informed by guidelines from Mannava et al, 30 we defined a cam deformity as an alpha angle >55° and a pincer lesion as a center-edge angle ≥40°. Intraoperative findings were obtained from operative notes and included the extent of cartilage degeneration (Outerbridge classification, presence of chondral flap), 41 labral tear size (using clockface nomenclature), 5 Beck classification of labral damage, 3 Beck classification of transition zone cartilage injury (ie, CLJ breakdown) (Table 1), 32 and procedures performed.
Beck Classification of Transition Zone Cartilage Injury (ie, Chondrolabral Junction Breakdown) Modified From Mayer et al 32
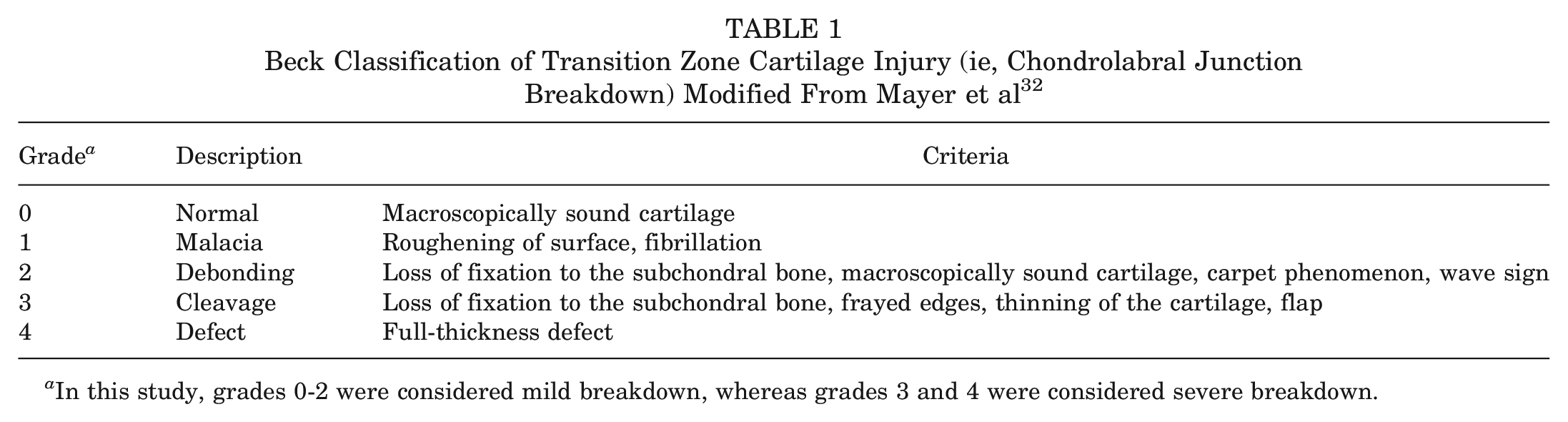
In this study, grades 0-2 were considered mild breakdown, whereas grades 3 and 4 were considered severe breakdown.
Abbreviated Surgical Technique
All surgeries were performed by a single surgeon, as described in previous technical notes.1,11,34,40,52,53 In brief, after intubation and sedation with general anesthesia, patients were positioned supine on a hip distraction table (Smith & Nephew) with a gel-padded perineal post. Anterolateral, anterior, midanterior, and Dienst (placed one-third the distance between the anterior superior iliac spine and the anterolateral portal) portals were established using the puncture capsulotomy technique.1,11 Given the minimally invasive nature of this technique, subsequent closure was not required. For a minority of patients (<10%) exhibiting unusually pronounced cam lesions and/or constrained anatomic features, portals were partially extended and subsequently closed. Electrocautery and intermittent traction were used sparingly to maintain safe intra-articular temperatures and reduce the risk of neurovascular injury, respectively.34,52 As indicated, acetabular recession and acetabuloplasty were performed to address pincer lesions without violating the CLJ.40,53 Labral repair was performed if there existed adequate, healthy labral tissue for suture fixation or if the tear was complex with extension into the CLJ, whereas labral debridement was carried out if the labral tear was hypoplastic, degenerative, or isolated to a single plane involving <50% of the labrum.27,35 Although at the time of publishing the senior surgeon performs primarily labral repair with capsular autograft augmentation, this procedure was not performed during the study period of March 2002 through June 2013.9,39,40 After complete release of traction, dynamic examination and visualization from the peripheral compartment were used to evaluate the labral seal and test for impingement. As necessary, cam lesions were resected with the hip flexed to approximately 45°, with additional flexion applied as indicated to address large, posterosuperior deformities. Heterotopic ossification prophylaxis (eg, indomethacin) was not used routinely in any of the patients.
Postoperative Rehabilitation
Per the senior surgeon’s standard of care, patients were prescribed a uniform 5-phase, patient-guided postoperative protocol, which involved deep vein thrombosis prophylaxis with daily low-dose aspirin (81 mg) for 3 weeks. Patients were permitted immediate weightbearing as tolerated on postoperative day zero, using a flat-footed, stiff-legged gait with crutches. At 6 weeks, patients gradually decreased reliance on crutches and started using a stationary bicycle with minimal resistance and an elevated seat. After 10 weeks, patients were allowed to begin low-resistance elliptical training and light swimming, emphasizing ROM rather than strengthening. At 4 months, mild twisting activities and short-arc leg presses and hamstring curls were permitted. Finally, full-impact loading activities were resumed as tolerated at 6 months, and approval for high-pivoting exercises was given at 9 to 12 months. 36
Statistical Analysis
Categorical variables were analyzed using chi-square or Fisher exact test, as appropriate, and post hoc analyses were conducted using the Holm-Bonferroni method to adjust for multiple comparisons. Continuous variables collected at a single time point (eg, age or BMI) were compared using unpaired t test or 1-way analysis of variance. Kaplan-Meier estimator was used to calculate and graphically illustrate the cumulative risk of converting to THA, stratified by severe (Beck classification of transition zone cartilage injury ≥3) versus mild (classification ≤2) breakdown of the CLJ. Comparisons between groups were performed using the log-rank test.
Cox proportional hazards models were implemented to estimate the adjusted hazard ratio (HR) of CLJ breakdown, controlling for relevant covariates. To assess the fundamental proportional hazards assumption, we tested the correlation of scaled Schoenfeld residuals with rank-ordered time. 46 Such testing revealed violation of this assumption; thus, we used the Schemper weighted model, with robust covariance estimates and truncation of weights at their 95th percentile.13,29,51P values were calculated using Wald test. Model variables were selected based on previous literature and unadjusted analyses.12,27,35,38 To ease interpretability and increase statistical power, we analyzed covariates as continuous variables, if applicable. 2 HRs therefore represent the change in the hazard rate (or risk) of conversion to THA per 1-unit increase in the continuous variable, holding all other covariates constant.
An a priori power analysis was performed leveraging previous literature and clinical expertise.27,33,59 Assuming THA conversion rates of 25% and 5% for the severe and mild CLJ breakdown groups, respectively, an enrollment ratio of 3 to 1 for severe to mild CLJ breakdown, and an alpha of .05, we determined that a total of 141 patients (35 severe breakdown; 106 mild breakdown) were required to achieve 80% power.
Sensitivity and exploratory analyses were performed to evaluate the robustness of our results. First, the primary weighted Cox regression model was repeated using clinically informed dichotomization of covariates to assess potential nonlinear relationships between grading systems and survivorship. Second, separate weighted Cox regression models were implemented to explore associations between conversion to THA and labral tear size or mean joint space width, controlling for age, Tönnis grade, and labral management technique. Third, the latter model was repeated absent Tönnis grade, as mean joint space width and Tönnis grade share inherent similarities. Statistical analysis was performed using R Version 4.2.1 (R Foundation for Statistical Computing), and P < .05 was considered significant.
Results
Participants
Of the 211 patients screened for this study, 174 met inclusion criteria (Figure 1). This sample included 88 women (50.6%) and 86 men with a mean ± SD age of 37.8 ± 11.2 years and BMI of 26.3 ± 4.5. Most patients were White (96.0%) or not Hispanic (97.1%). Regarding preoperative radiographic evidence of osteoarthritis, 78.2% of patients had Tönnis grade ≤1, and 21.8% had Tönnis grade ≥2. Intraoperatively, 30% of patients exhibited severe breakdown of the CLJ (Beck classification ≥3), whereas the remaining 70% displayed mild breakdown (Figure 2). Furthermore, 76% of patients underwent acetabuloplasty, femoroplasty, or both, and similar proportions of patients received labral repair (47.7%) versus debridement (52.3%). Additional pre- and intraoperative patient characteristics are summarized in Tables 2 and 3.
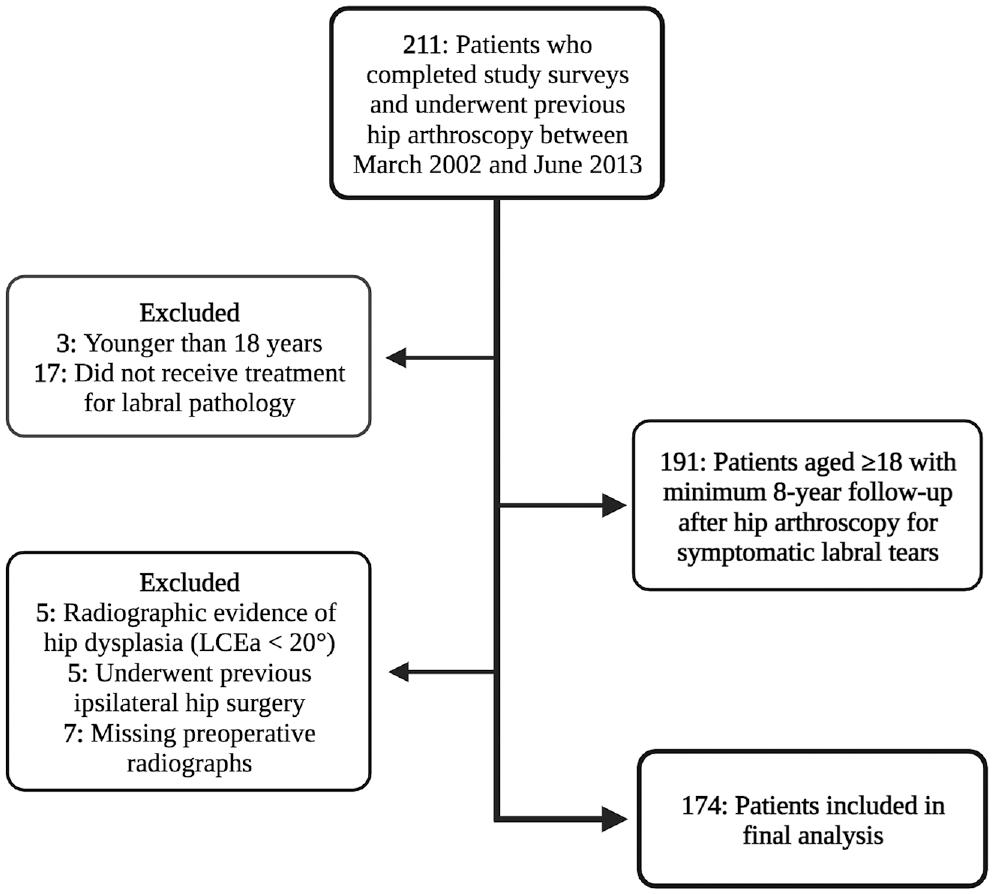
Flowchart detailing the patient selection process. LCEa, lateral center-edge angle.
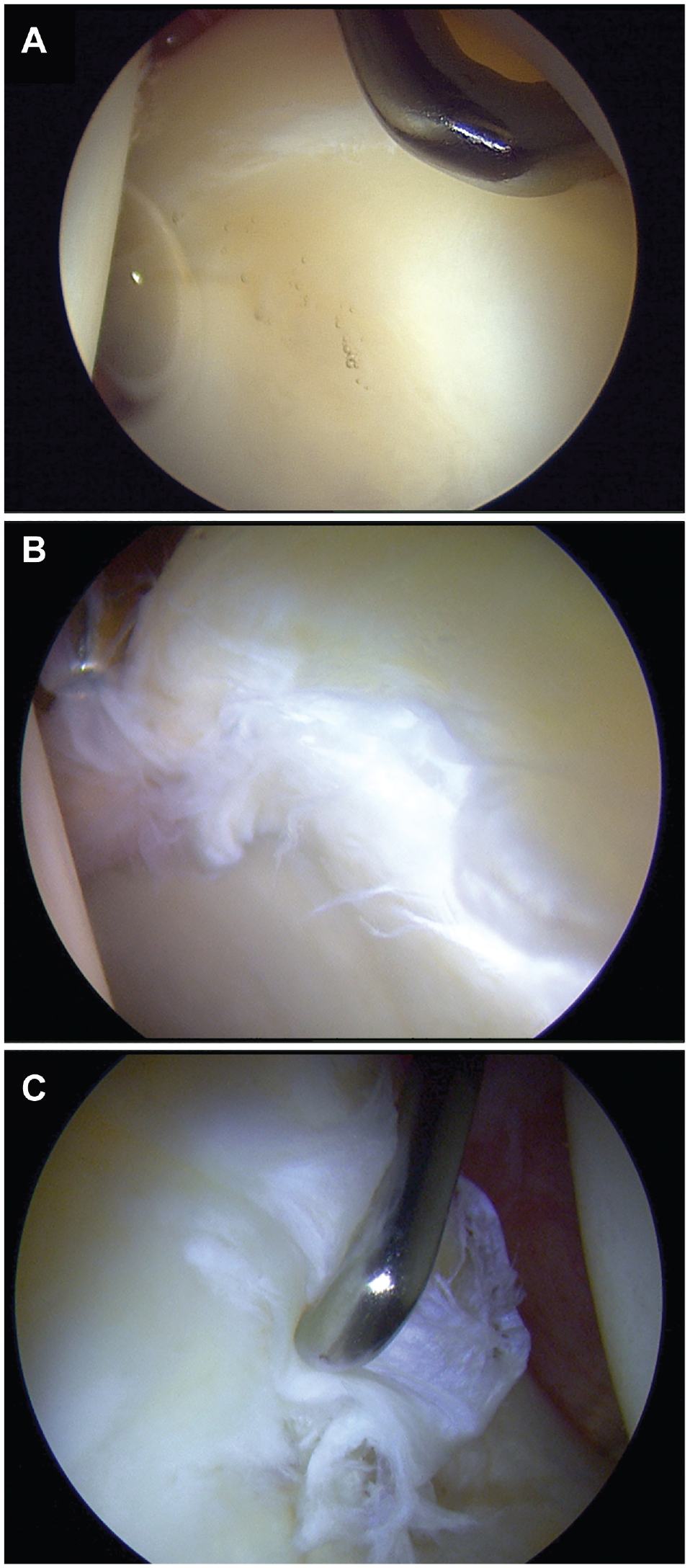
Arthroscopic visualization of different levels of chondrolabral junction breakdown (A, Beck classification = 0; B, Beck classification = 2; C, Beck classification = 4). Severity of chondrolabral junction breakdown was assessed using the Beck classification of transition zone cartilage injury. In the present study, grades 0-2 were considered mild breakdown, whereas grades 3 and 4 were considered severe breakdown.
Baseline Patient Demographic Characteristics and Radiographic Findings a
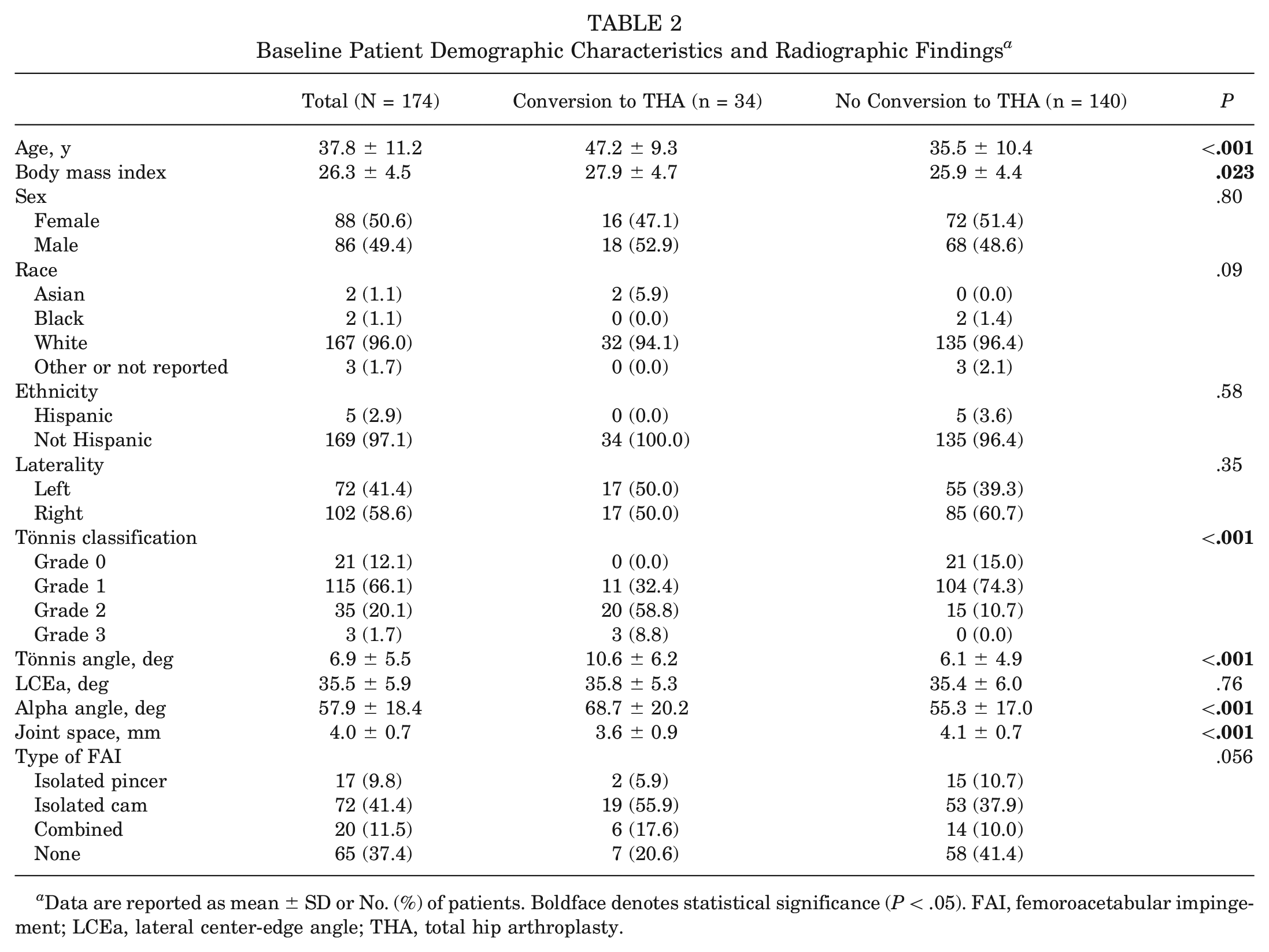
Data are reported as mean ± SD or No. (%) of patients. Boldface denotes statistical significance (P < .05). FAI, femoroacetabular impingement; LCEa, lateral center-edge angle; THA, total hip arthroplasty.
Intraoperative Findings and Procedures Performed a
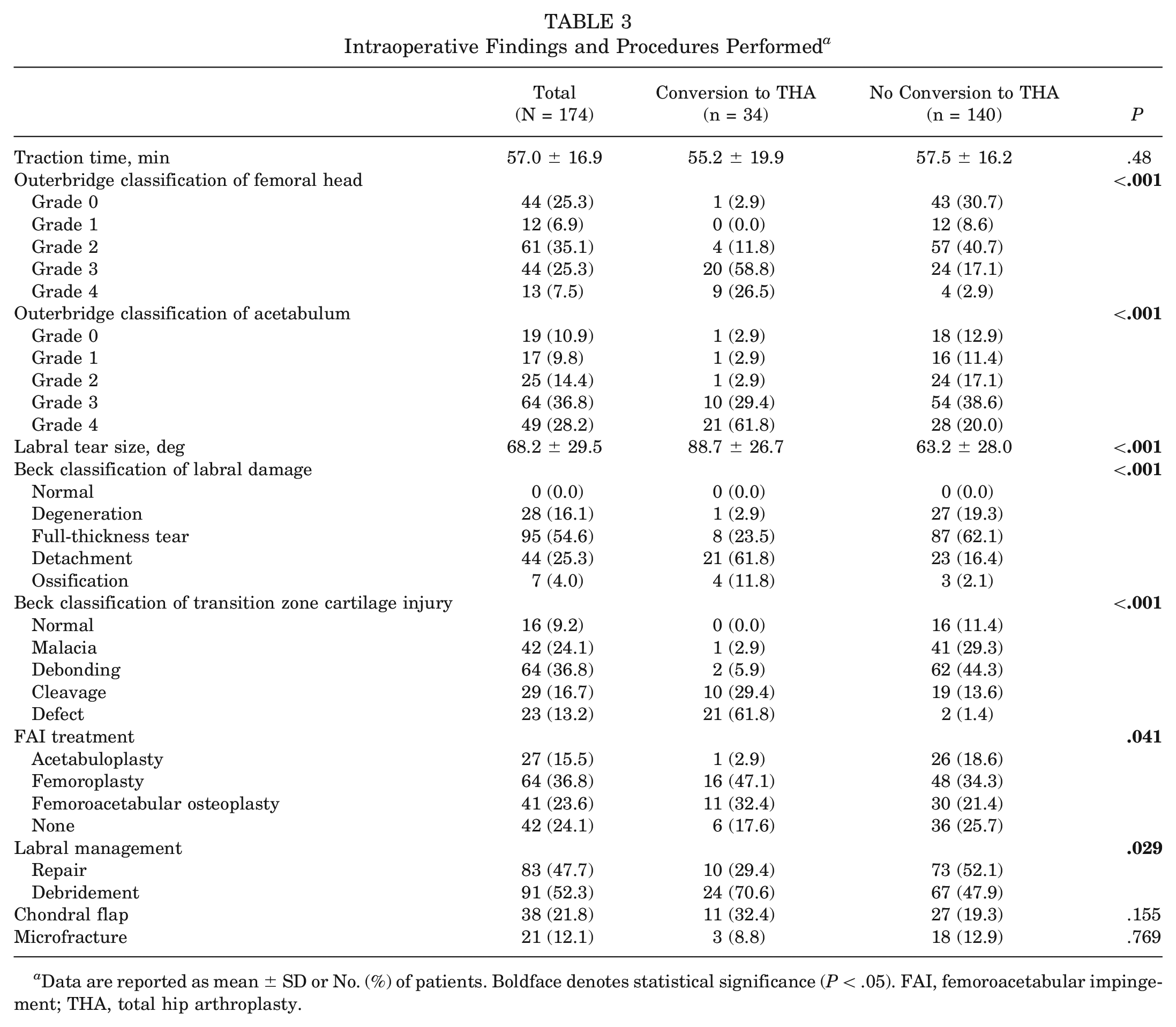
Data are reported as mean ± SD or No. (%) of patients. Boldface denotes statistical significance (P < .05). FAI, femoroacetabular impingement; THA, total hip arthroplasty.
Conversion to Total Hip Arthroplasty
The mean follow-up was 11.1 ± 2.5 years. Ultimately, 34 (19.5%) patients converted to THA at a mean of 4.7 ± 3.8 years after primary hip arthroscopy, whereas 2 patients (1.1%) underwent subsequent hip arthroscopy; neither of these patients converted to THA. In unadjusted analyses, the following preoperative factors were associated with conversion to THA: older age (P < .001), higher BMI (P = .023), worse Tönnis grade (P < .001), larger Tönnis and alpha angles (P < .001 for both), and smaller mean radiographic joint space (P < .001) (Table 2). Additionally, several intraoperative variables were associated with conversion to THA, including breakdown of the CLJ (P < .001), worse cartilage damage on the femoral head or acetabulum (P < .001 for both), larger or more severe labral tearing (P < .001 for both), and labral debridement (P = .029) (Table 3). Of note, although FAI treatment showed significance in the overall Fisher exact test, this association did not remain significant after adjustment for multiple comparisons using the Holm method (P > .1 for all) (Table 3).
Kaplan-Meier analysis was implemented to estimate survivorship (ie, no conversion to THA at minimum 8-year follow-up) over the study period, accounting for variable follow-up times. The overall rate of survivorship at 10 years was 81.6% (95% CI, 75.9%-87.7%). Survivorship at 10 years was strikingly inferior in patients exhibiting severe (43.6%; 95% CI, 31.9%-59.7%) versus mild (97.9%; 95% CI, 95.1%-100%) breakdown of the CLJ (P < .001) (Figure 3).
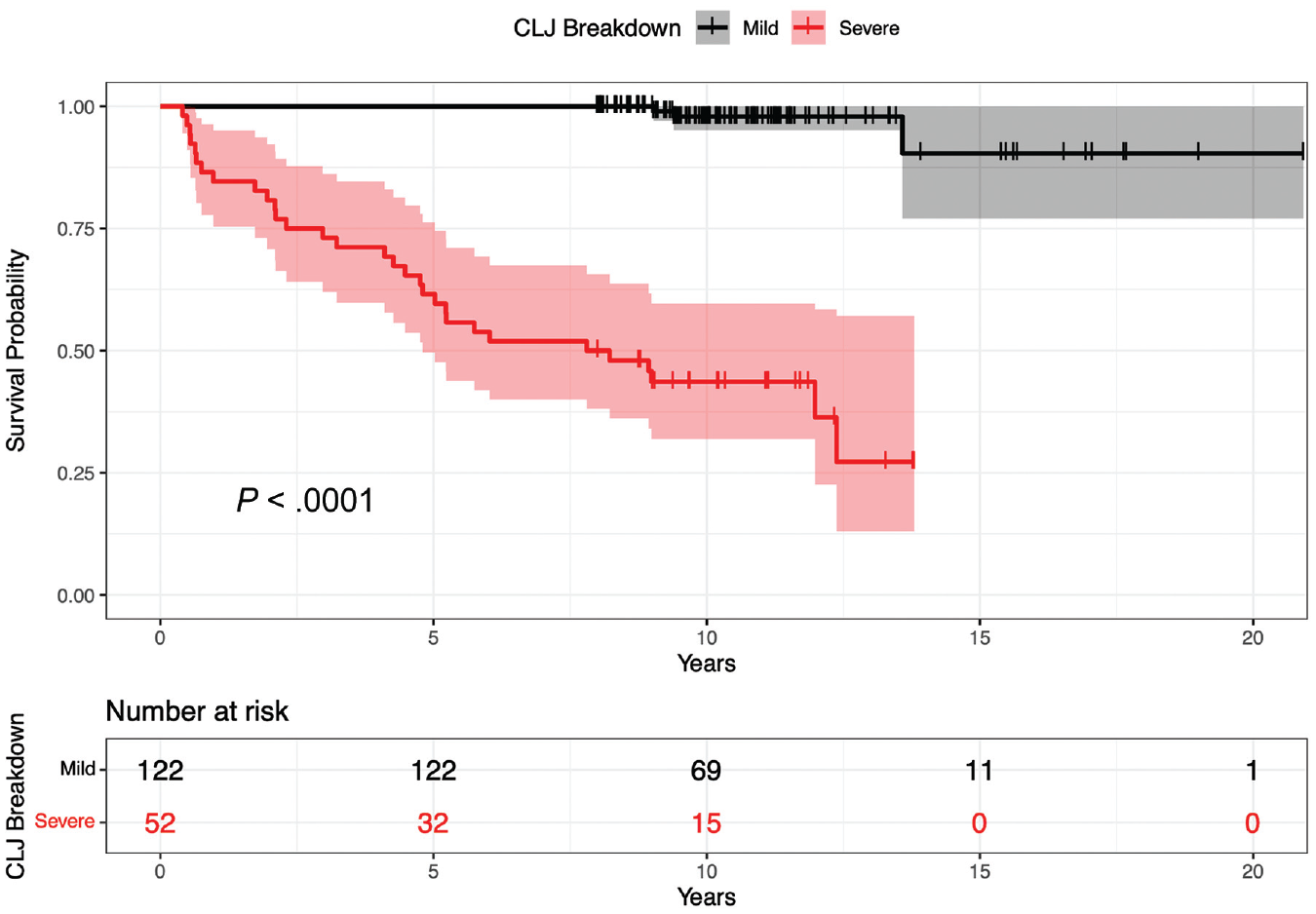
Unadjusted survival (Kaplan-Meier) curves and risk table for patients exhibiting severe versus mild breakdown of the chondrolabral junction (CLJ). Severity of CLJ breakdown was assessed using the Beck classification of transition zone cartilage injury. Grades 3 and 4, severe; grades 0-2, mild.
Weighted Cox regression was performed to identify independent risk factors for conversion to THA, adjusting for relevant covariates and variable follow-up. Significant predictors of failure were worse CLJ breakdown (weighted HR, per 1-unit increase, 6.41; 95% CI, 3.11-13.24; P < .001), older age (weighted HR, per 1-year increase, 1.09; 95% CI, 1.04-1.14; P < .001), and higher Tönnis grade (weighted HR, per 1-unit increase, 4.59; 95% CI, 2.13-9.90; P < .001). Labral management technique, degree of labral damage, and Outerbridge grade were not independent predictors of survivorship (Table 4).
Weighted Cox Regression Adjusting for Patient Characteristics and Variable Follow-up a
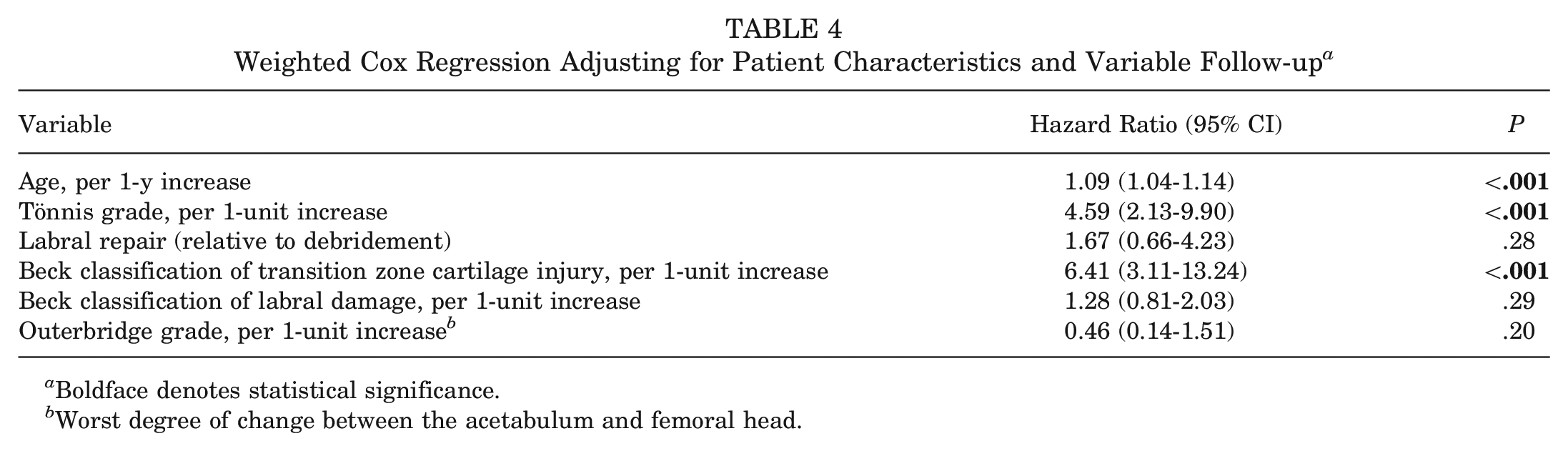
Boldface denotes statistical significance.
Worst degree of change between the acetabulum and femoral head.
Sensitivity and Exploratory Analyses
Similar results were found in the sensitivity analysis including dichotomized covariates, except that severe CLJ breakdown was associated with a higher weighted HR of 15.2 (95% CI, 4.27-53.91; P < .001) and worse labral damage was identified as a significant predictor of failure (weighted HR, 2.40; 95% CI, 1.10-5.21; P = .027) (Appendix Table A1, available in the online version of this article). Furthermore, exploratory analyses revealed larger labral tears and greater joint space narrowing as independent predictors of failure; however, the HR for joint space width was statistically significant only in the model not controlling for Tönnis grade (Appendix Table A2, available online). Last, given the strong relationship between CLJ breakdown and conversion to THA, exploratory analyses were performed to evaluate associations between preoperative characteristics and CLJ breakdown. Severe CLJ breakdown was significantly associated with older age, higher BMI, larger Tönnis and alpha angles, diminished joint space, cam or combined impingement, and higher Tönnis grade (Table 5).
Associations Between Intraoperative Chondrolabral Junction Breakdown and Preoperative Patient Characteristics a
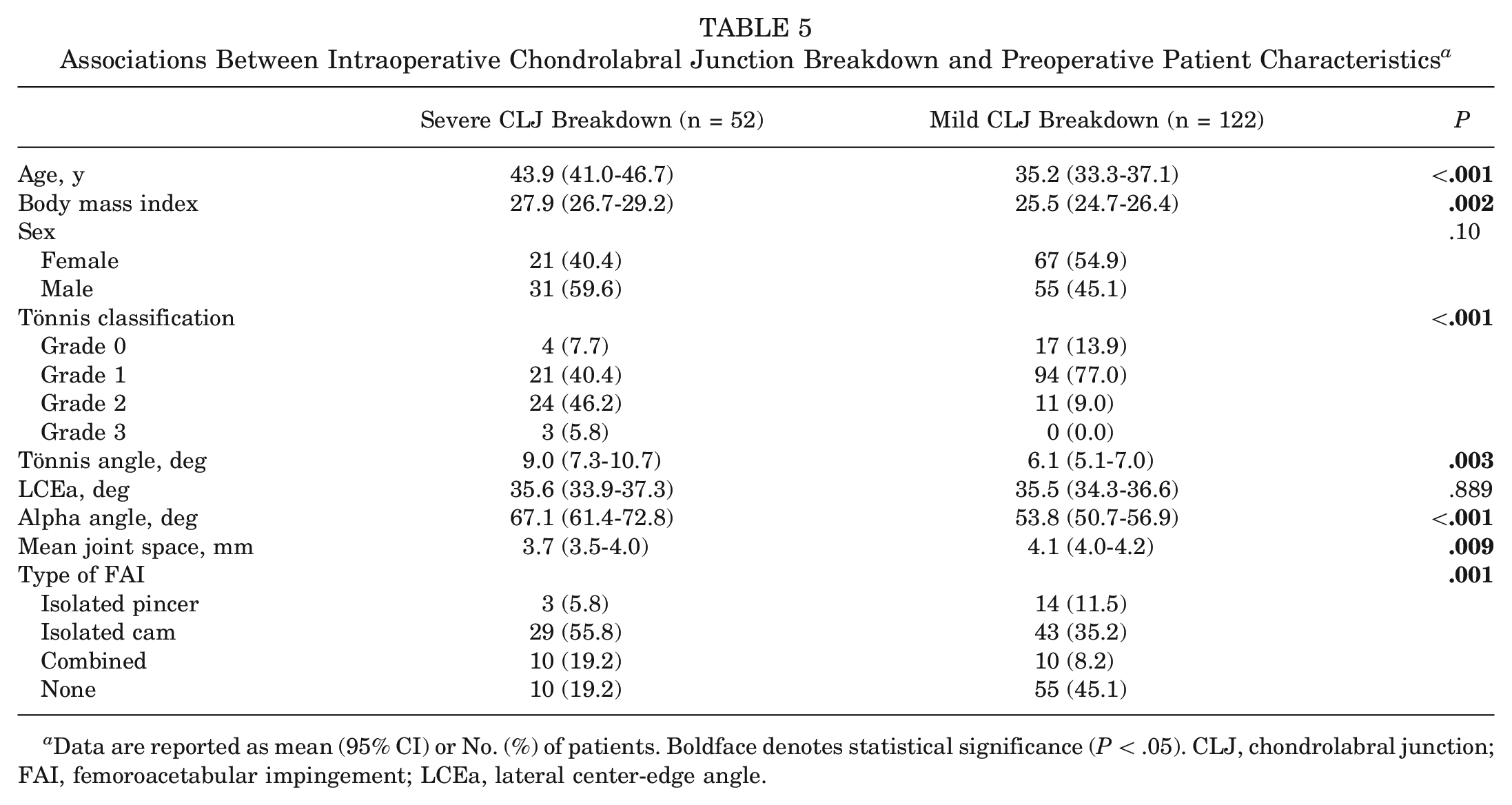
Data are reported as mean (95% CI) or No. (%) of patients. Boldface denotes statistical significance (P < .05). CLJ, chondrolabral junction; FAI, femoroacetabular impingement; LCEa, lateral center-edge angle.
PROMs and Satisfaction
PROMs at final follow-up were similar between patients who exhibited severe versus mild CLJ breakdown and are summarized in Table 6. Regarding patient satisfaction, 148 (87%) of 170 patients responded “yes” to the following question: “Are you satisfied with the treatment you received?” Additionally, 137 (82%) of 168 patients responded “yes” to the following question: “If given the choice in the future, would you choose the same treatment?” These responses did not differ on the basis of intraoperative CLJ breakdown (Table 6).
Patient-Reported Outcome Measures and Satisfaction at Final Follow-up a
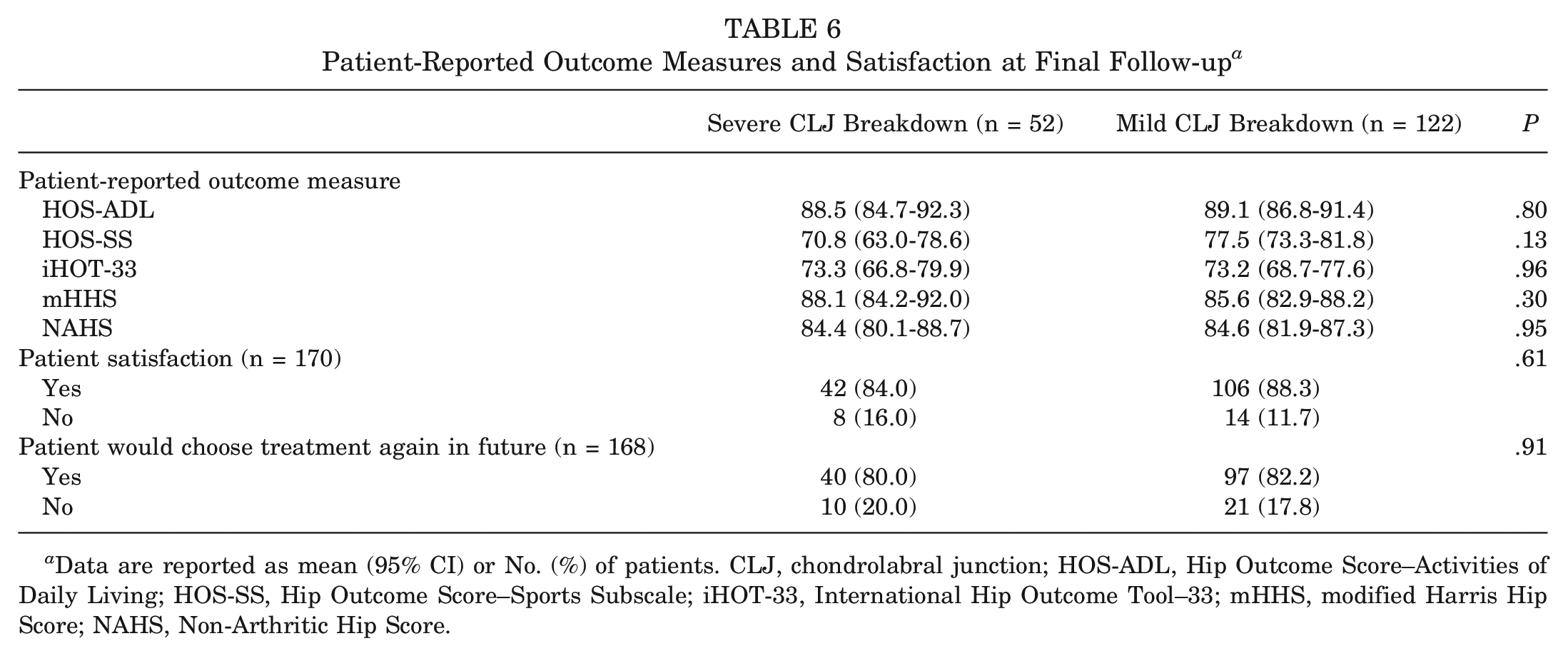
Data are reported as mean (95% CI) or No. (%) of patients. CLJ, chondrolabral junction; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-33, International Hip Outcome Tool–33; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score.
Discussion
As the incidence of hip arthroscopy rapidly increases, insights into the patient-specific characteristics that predict durable long-term outcomes are critical both to support surgeons in preoperative risk stratification and to promote shared decision-making. 60 The present study analyzed a large cohort of patients with minimum 8-year and mean 11-year follow-up to identify pre- and intraoperative factors associated with conversion to THA. After adjusting for relevant confounders and variable follow-up, we identified older age, worse Tönnis grade, and more severe CLJ breakdown as independent predictors of progression to THA, with CLJ breakdown being the strongest indicator. Indeed, using Kaplan-Meier analysis, we estimated the 10-year survivorship for patients with severe versus mild CLJ breakdown to be 43.6% versus 97.9%, respectively. Altogether, our findings both align with previous literature and reveal CLJ breakdown as a novel predictor of long-term outcomes after hip arthroscopy.
Halting the progression of CLJ breakdown may be crucial for achieving durable outcomes because this region acts as a seamless transition zone between the fibrocartilaginous labrum and hyaline articular cartilage. Specifically, the CLJ possesses distinct histological features that facilitate smooth force transmission and structural continuity under high shear stresses. Recent translational research indicates that the CLJ is primarily composed of crimped, type I collagen, which “unbuckles” during tensile loading and reverts to its original crimped architecture upon unloading. This extension-recovery property allows the labrum to maintain its elasticity without undergoing permanent deformation. 48 Relatedly, cadaveric studies have revealed that disrupting the CLJ compromises the labrum’s sealing capacity, elevating the risk for progression to osteoarthritis.7,14,16,45
Despite these critical functions, a histologic study using an ovine model has suggested the CLJ possesses limited regenerative potential, with only partial healing via fibrovascular scarring observed 12 weeks after arthroscopic labral repair. 42 It has been speculated that incomplete reconstitution of this region via fibrovascular scar likely results from the reduced blood supply to the labrum and CLJ, which is abundant in the fetal hip but severely diminished in the adult hip.26,56 Consistent with these preclinical investigations, our study found lower survivorship among patients with advanced CLJ breakdown observed intraoperatively, substantiating this transition zone’s limited healing capacity and underscoring the importance of intervening before severe damage occurs. A recent finite-element modeling study suggested that such prevention may be achieved by preemptively addressing osseous deformities. Specifically, physiologically realistic simulations suggested that cam lesions exert elevated shear stress and strain forces on the CLJ, predisposing breakdown at this interface. 55 However, given the relatively high prevalence of asymptomatic FAI, it may be challenging to discern whether cam deformities will remain asymptomatic or cause irreversible chondrolabral injury that compromises the clinical benefit of hip arthroscopy. 19
Emerging MRI techniques capable of noninvasively detecting and monitoring intra-articular damage may prove critical in preventing irreparable breakdown of the CLJ. In the present study, CLJ breakdown was observed arthroscopically, as imaging modalities available during the study period prevented the preoperative assessment of CLJ breakdown. However, innovative imaging technologies (eg, 3.0-T delayed gadolinium-enhanced MRI of cartilage; T1ρ, T2, and T2* mapping) may enhance grading of the CLJ preoperatively and enable surgeons to better prognosticate long-term outcomes.25,49 Until these modalities become routinely accessible for clinical use, orthopaedic surgeons may leverage associations between CLJ breakdown and observable preoperative factors (eg, radiographic parameters, age, BMI) established in the present study.
To our knowledge, no previous studies have correlated clinical outcomes with the degree of CLJ breakdown observed intraoperatively, but several have investigated the safety and efficacy of “CLJ-preserving” surgical techniques. In a retrospective cohort study involving 1010 hips, Webb et al 58 found that preserving the CLJ was associated with a reduction in the proportion of revision surgery due to capsulolabral adhesions (46% vs 17%). Additional case series have associated acetabuloplasty without labral detachment with significant improvements in postoperative PROMs, although these studies lacked comparison groups.10,18,53 Notably, the methods of CLJ preservation varied between surgeons, but these studies collectively suggested (1) growing interest in preserving the CLJ and (2) positive, albeit preliminary, outcomes associated with such preservation.
In addition to elucidating CLJ breakdown as a novel predictor of conversion to THA, the current investigation complements existing literature by corroborating older age and higher Tönnis grade as risk factors—trends that have emerged across varied patient samples and surgical indications. In the context of FAI, most investigations have linked older age with lower survivorship at long-term follow-up.6,8,35,59 Although these studies collectively solidify older age as a risk factor for eventual conversion to THA, they do not imply that hip arthroscopy should be reserved for younger patients. Martin et al 31 recently conducted a randomized controlled trial demonstrating favorable hip arthroscopy outcomes in patients >40 years old, suggesting that older age is not a contraindication for arthroscopic acetabular labral repair in this population. Instead, age should be carefully considered alongside other pertinent patient characteristics during the shared decision-making process.
Regarding Tönnis classification, our findings validate previous studies correlating higher grades with inferior outcomes at all follow-up time points.6,8,12,38,59 Also using preoperative radiographs, Philippon et al 43 and Ruzbarsky et al 50 reported an association between diminished joint space and higher rates of conversion to THA. The present study similarly identified this association but only in the sensitivity analysis not including Tönnis grade. Although both metrics separately predicted THA conversion, our analyses indicated that they do not each contribute independent explanatory power, likely owing to their inherent similarities. Thus, the choice between these preoperative assessment tools may depend on surgeon preference, patient characteristics, and the specific method used to quantify joint space width (ie, minimum vs mean measurement).
Limitations
The conclusions of this study should be interpreted in the context of certain limitations. First, consistent with the dynamic landscape of hip arthroscopy, the senior surgeon’s operative technique has evolved since the study period. For example, although >50% of patients in the present study underwent labral debridement, at the time of publishing the senior surgeon no longer routinely performs this procedure, instead primarily performing labral repair with capsular autograft augmentation.9,39,40 Considering the rapid advancements in hip preservation, we conjecture that this limitation would apply to any long-term investigation. Second, given the time frame of the present study, our analysis may have included patients who would not be indicated for hip preservation surgery using current evidence-based practices, such as patients with Tönnis grade ≥2. Again, this limitation is intrinsic to the study design, and excluding these patients would both inflate survival estimates and preclude substantiation of established risk factors (eg, Tönnis grade ≥2 or severe joint space narrowing).12,38,43,50 Third, due to the relatively recent practice of routine PROM collection, preoperative PROMs were not available, preventing the analysis of postoperative score changes or clinically meaningful improvements and representing an important consideration for future investigations. However, the primary outcome of this study was conversion to THA; the lack of preoperative PROMs did not diminish our ability to establish associations between patient-specific characteristics and rates of conversion. Furthermore, we reported 5 validated PROMs at final follow-up, as well as patient satisfaction and whether patients would choose the treatment again in the future. We believe that these metrics serve as valuable proxies for clinically meaningful improvements such as Substantial Clinical Benefit and Patient Acceptable Symptom State, which are, fundamentally, measures of patient satisfaction.23,24 Fourth, commensurate with all retrospective studies, our findings are not sufficient to establish causation between CLJ breakdown identified at the time of hip arthroscopy and inferior minimum 8-year outcomes, as other unmeasured factors may have mediated this association. 57 For example, patients who exhibited more severe CLJ breakdown intraoperatively may have possessed underlying genetic architectures predisposing them to a more rapid progression of CLJ breakdown and chondral degredation. 54 Similarly, patients with severe CLJ breakdown may have presented with a later stage of osteoarthritis, which inherently predicts inferior long-term survivorship. To address this, multivariable regression analyses and several sensitivity analyses were implemented to adjust for clinically relevant preoperative (age, Tönnis grade) and intraoperative (Outerbridge grade, Beck labral damage) factors. Future prospective clinical studies—in addition to cadaveric and in vivo biomechanical analyses—are needed to further clarify both the anatomic role of the CLJ and the relationship between its breakdown and outcomes after hip arthroscopy.
Conclusion
Although most patients achieved favorable minimum 8-year outcomes, several pre- and intraoperative factors were associated with THA conversion; of these, worse CLJ breakdown, higher Tönnis grade, and older age were the strongest predictors.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465241234258 – Supplemental material for Association Between Chondrolabral Junction Breakdown and Conversion to Total Hip Arthroplasty After Hip Arthroscopy for Symptomatic Labral Tears: Minimum 8-Year Follow-up
Supplemental material, sj-pdf-1-ajs-10.1177_03635465241234258 for Association Between Chondrolabral Junction Breakdown and Conversion to Total Hip Arthroplasty After Hip Arthroscopy for Symptomatic Labral Tears: Minimum 8-Year Follow-up by Michael C. Dean, Nathan J. Cherian, Zachary L. LaPorte, Christopher T. Eberlin, Charles Wang, Kaveh A. Torabian, Kieran S. Dowley, Michael P. Kucharik, Paul F. Abraham, Mark R. Nazal and Scott D. Martin in The American Journal of Sports Medicine
Footnotes
Acknowledgements
Special thanks for the continued support of the Conine Family Fund for Joint Preservation and Mark Cote, DPT, MS, from Mass General Brigham for assistance with statistical analyses.
Submitted June 30, 2023; accepted December 20, 2023.
Presented at the annual meeting of the AOSSM, Washington, DC, July 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Conine Family Fund for Joint Preservation. C.W. has received support for education from Smith & Nephew and hospitality payments from Exactech. S.D.M. has received support for education from Kairos Surgical and a gift from Allergan. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.