
Abstract
Background:
Blood flow restriction training (BFR-t) data are heterogeneous. It is unclear whether rehabilitation with BFR-t after an anterior cruciate ligament (ACL) injury is more effective in improving muscle strength and muscle size than standard rehabilitation.
Purpose:
To review outcomes after an ACL injury and subsequent reconstruction in studies comparing rehabilitation with and without BFR-t.
Study Design:
Systematic review. Level of evidence, 3.
Methods:
A search of English-language human clinical studies published in the past 20 years (2002-2022) was carried out in 5 health sciences databases, involving participants aged 18-65 undergoing rehabilitation for an ACL injury. Outcomes associated with muscle strength, muscle size, and knee-specific patient-reported outcome measures (PROMs) were extracted from studies meeting inclusion criteria and compared.
Results:
The literature search identified 279 studies, of which 5 met the selection criteria. Two studies suggested that BFR-t rehabilitation after an ACL injury improved knee or thigh muscle strength and muscle size compared with rehabilitation consisting of comparable and higher load resistance training, with two studies suggesting the opposite. The single study measuring PROMs showed improvement compared to traditional rehabilitation, with no difference in muscle strength or size.
Conclusion:
BFR-t after an ACL injury seems to benefit muscle strength, muscle size, and PROM scores compared with standard rehabilitation alone. However, only 1 large study included all these outcomes, which has yet to be replicated in other settings. Further studies utilizing similar methods with a common set of outcome measures are required to confirm the effects of BFR-t on ACL rehabilitation.
The anterior cruciate ligament (ACL) in the knee joint prevents excessive anterior tibial movements and is the most commonly injured knee ligament, 16 with an estimated incidence of 30 to 78 per 100,000 people each year 15 and an estimated cost of $17.7 billion in the United States per annum. 31 It is frequently atraumatically injured during sporting activities after a sudden change of direction, such as cutting or landing, that involve decelerating and/or rotational movements.3,4 Female patients are 2 to 8 times more likely to injure their ACL than male patients.3,17 ACL reconstruction (ACLR) using a hamstring tendon graft is a standard procedure for ACL injuries, 34 with rates of ACLR in the United Kingdom increasing 12-fold over the past 20 years. 1 After ACLR, 61% to 89% of athletes return to sport in 8 to 18 months. 15
Recovery after surgery can be difficult, especially when regaining the size and function of the quadriceps muscle. This problem is caused by several connected variables: muscle atrophy and inhibition, pain and swelling management, neuromuscular control and proprioception, joint effusion, and range of motion limitations.21,39,40 Regardless of the treatment approach, an ACL injury has a lengthy recovery period, results in decreased physical activity and sports participation, 12 and is associated with joint cartilage degradation 14 and an increased risk of developing knee osteoarthritis.13,30
After an ACL injury and subsequent surgery, recovering quadriceps function is a complex journey that requires a rehabilitation strategy to target neuromuscular control, range of motion restrictions, and muscle atrophy.21,22 In standard rehabilitation, physical therapists seek to maximize outcomes to return to preinjury function by strategically implementing modalities such as electrical stimulation, neuromuscular electrical stimulation, eccentric strengthening, and closed kinetic chain exercises. These strategies aim to preserve and improve quadriceps and hamstring strength to optimize knee function and reduce pain. 15 As an ACL injury adversely affects quadriceps strength, resistance training is recommended to stimulate muscle hypertrophy and increase muscle strength. 25 Resistance training guidelines suggest a load of 60% to 70% of 1-repetition maximum (1RM) 2 ; however, patients with ACL injuries might not be able to tolerate such loads because of pain, swelling, inflammation, and their overall perceived knee function. 33 A new development is blood flow restriction training (BFR-t), which combines low-load exercises and blood flow occlusion to achieve a similar muscle hypertrophic stimulus to that achieved with high-load exercises. 9 Initial evidence suggests that BFR-t improves strength in both the quadriceps and the hamstring muscles after ACLR. 44
BFR-t uses a tourniquet cuff to partially restrict arterial flow and prevent venous return from active muscles. 26 This causes hypoxia and metabolic stress, 29 triggering the mammalian target of rapamycin and mitogen-activated protein kinase signaling pathways.10,26,45 The mammalian target of rapamycin pathway is a key regulator of anabolic and catabolic signal transduction in skeletal muscles and thus muscle mass accretion and wasting. There is no current consensus regarding the benefits of BFR-t in rehabilitation. Several studies on lower limb rehabilitation have reported increases in muscle size and muscle strength after the application of BFR-t24,26,36 following ACLR, with others reporting similar or no significant changes when comparing standard training with BFR-t. 23 BFR-t is considered low risk,29,35 with minor side effects including dizziness, numbness, delayed-onset muscle soreness, itching, and discomfort in the application area. 41 However, rare serious complications, including deep vein thrombosis, stroke, nerve damage, and rhabdomyolysis, have been reported.19,39
BFR-t data are heterogeneous, and it is unclear whether ACL rehabilitation with BFR-t is more effective in improving muscle strength and muscle size than standard rehabilitation. It is, therefore, essential to determine if BFR-t in patients with ACL injuries is beneficial and, if so, create a standardized rehabilitation protocol including application time and measurement methodology. This systematic review aimed to examine the effectiveness of rehabilitation with BFR-t versus similar rehabilitation practice without BFR-t in patients undergoing ACLR. The outcomes assessed were (1) knee extensor and/or flexor muscle strength, (2) muscle size utilizing magnetic resonance imaging (MRI) or ultrasonography, and (3) knee-specific patient-reported outcome measure (PROM) scores.
Methods
Study Protocol and Search Strategy
The study protocol was registered on PROSPERO and is reported in line with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines 38 and the Cochrane Handbook for Systematic Reviews of Interventions. 18 The PICO (Population, Intervention, Comparison, and Outcome) framework (Table 1) was used to outline the research question and shape the search strategy. 18
PICO Framework a
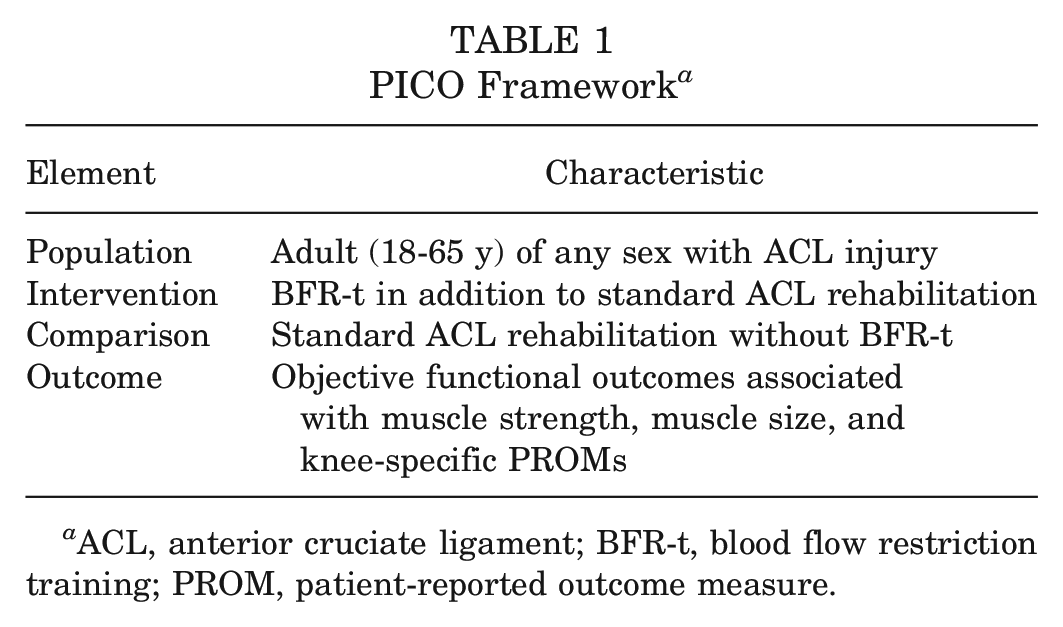
ACL, anterior cruciate ligament; BFR-t, blood flow restriction training; PROM, patient-reported outcome measure.
The following keywords, with their appropriateness checked by a scoping search, were used:
anterior cruciate ligament injuries, anterior cruciate ligament, anterior cruciate ligament reconstruction, ACL, ACLR
BFR, blood flow restriction
A search was carried out in MEDLINE, Embase, SPORTDiscus, and CINAHL. The physical therapy database PEDro as well as the trial registers Cochrane Central Register of Controlled Trials, ClinicalTrials.gov, and International Clinical Trials Registry Platform were also searched.
The search strategy included subject headings and keywords relating to ACL injuries, ACLR, and BFR-t. Truncation, relevant synonyms, and proximity searching were used to broaden the search. The full search strategy is provided in the Appendix (available in the online version of this article). Results were limited to between 2002 and the date of the search (July 6, 2022). No other search limits or filters were used. In addition, 51 articles were retrieved from the reference lists of previous systematic reviews identified by the initial search. The records were de-duplicated in EndNote (Clarivate) before screening.
Study Selection
Duplicates and non–English language studies were removed. Title screening, followed by abstract screening, was undertaken to exclude studies not meeting inclusion criteria (performed by V.C.).
Inclusion criteria were as follows:
published studies in the English language
participants aged 18 to 65 years
primary unilateral ACL injury (complete or partial) undergoing rehabilitation
details of BFR-t (timing during rehabilitation, BFR-t tool used, pressure applied, occlusion and nonocclusion exercise prescription)
rehabilitation details (duration, frequency, volume, intensity, type)
muscle adaptation outcomes reported
○ knee extensor and flexor muscle strength (isometric, concentric, eccentric)
○ muscle volume
○ anatomic cross-sectional area (CSA)
knee-specific PROMs
randomized controlled trial (RCT) or case-control study design
Exclusion criteria were as follows:
in vitro studies and animal or cadaveric studies
participants aged <18 and >65 years
presence of a confounding injury, such as spinal cord injury, polytrauma, systemic inflammatory condition, or joint infection
Data Extraction
Overall, 2 reviewers (V.C. and T.V.) independently extracted data from the selected studies using a standardized and pre-piloted extraction form in Excel (Microsoft), including the following:
(1) first author, year, study design, title, study objective
(2) participant characteristics (sex, age), number of participants, ACL injury type
(3) rehabilitation details including BFR-t timing, BFR-t tool used, pressure applied, BFR-t exercise prescription, nonocclusion exercise prescription
(4) follow-up time points, muscle groups assessed, muscle strength measurement methods and outcomes, muscle size measurement methods and outcomes, PROMs used and outcomes
The collected data were processed and analyzed and are summarized in the Appendix (available online).
Data Synthesis and Statistical Analysis
Collected data were processed and compared to identify similarities and discrepancies among the studies. Again, the same 2 reviewers checked the data extracted from each study before they were entered into Review Manager (Version 5.4; Cochrane) and Rayyan 37 (https://www.rayyan.ai/). The primary outcome variables were knee extensor and flexor muscle strength, muscle size, and PROMs. Intervention outcomes were summarized using established measurements of knee muscle function and/or size and knee-specific PROMs. The results were summarized with a qualitative narrative synthesis (by V.C.), structured by type of intervention, outcome, and content.
Risk-of-Bias and Quality Assessments
One reviewer (V.C.) assessed the methodological quality and risk of bias of the selected studies using the RCT checklist by Critical Appraisal Skills Programme 7 and the Cochrane risk-of-bias 2 tool. 43 The following domains were considered: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, and incomplete outcome data (attrition). A high attrition bias was defined as a loss of participants >20%. A risk-of-bias summary using the Cochrane risk-of-bias 2 tool was reported using a traffic light icon plot representing a low (green), unclear (yellow), or high (red) risk.
Patient and Public Involvement
This article was written in response to a discussion among English clinical practitioners working in the clinical field of ACL rehabilitation concerned about efficacy evidence, the incorporation of current research, and acceptable protocol replication, which took place in early 2021. There were 2 practitioners (J.S. and O.O.S.) who facilitated the creation and refinement of study questions. A third practitioner (S.K.) reviewed the results and this paper.
Results
The total number of identified studies was 279 from 5 databases (n = 163), 3 registers (n = 65), and the reference lists of previous systematic reviews (n = 51) (Figure 1), reduced to 91 after 184 duplicates and 4 studies in a non-English language were removed. After title screening, 54 more studies were excluded.
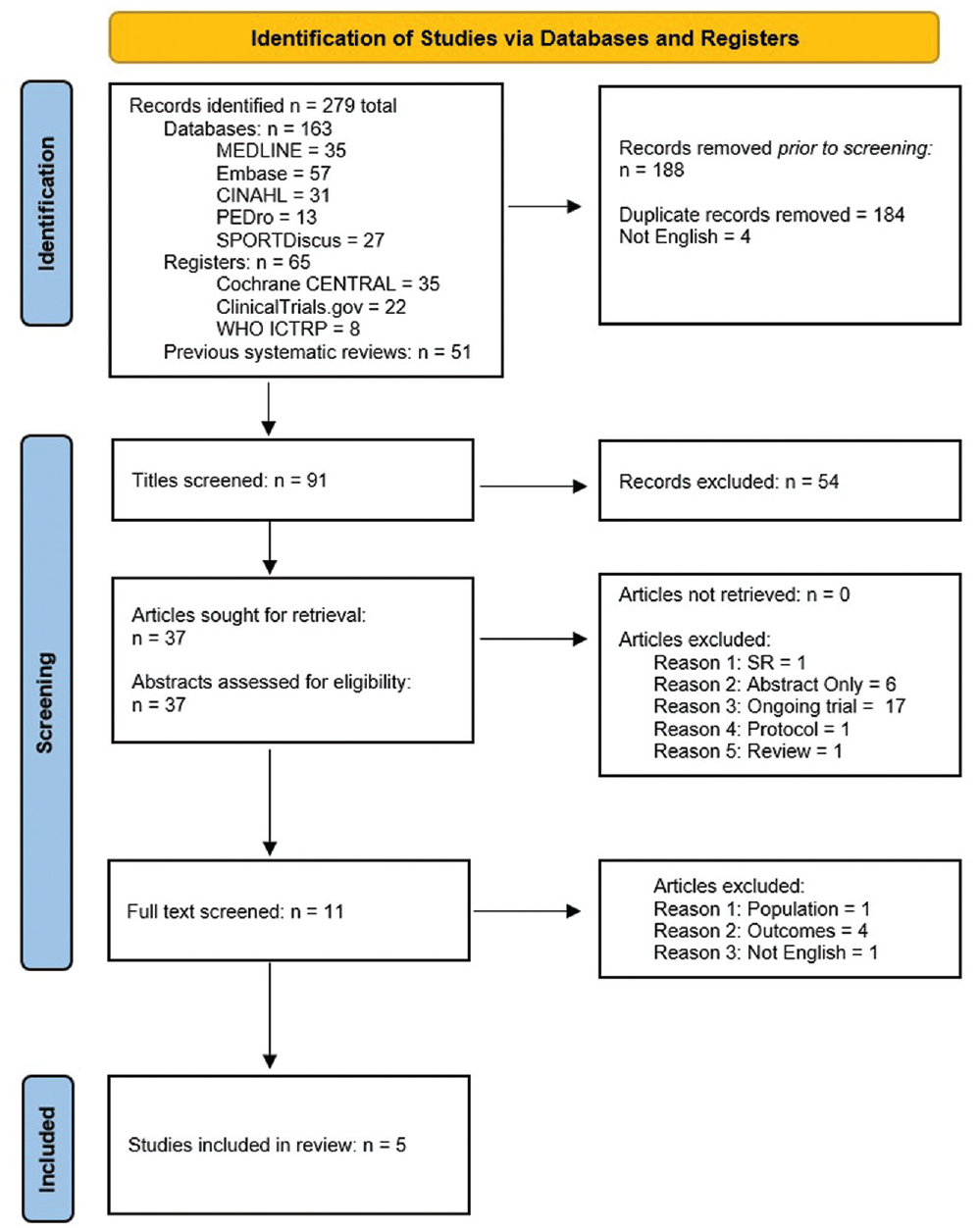
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart showing the selection process of studies. 38 SR, systematic review.
All 37 remaining studies were retrieved, with abstracts screened for eligibility according to the inclusion/exclusion criteria: a further 26 studies were excluded. Full-text screening of 11 articles was performed: 5 were deemed to meet the inclusion criteria and were included.
Study and Participant Characteristics
The 5 included studies compared an intervention (BFR-t) group and a non–BFR-t group, with a total of 130 participants, 71 male and 59 female, and a median or mean age of 24 to 38 years. Overall, 78 participants (60.0%) underwent BFR-t, and 16 (12.3%) underwent sham BFR-t. The remaining 36 participants were in the non-BFR-t group. In addition, 4 studies involved participants who underwent ACLR with a hamstring tendon graft, and 1 study involved participants before ACLR. 24 Further, 3 studies were RCTs,21,23,36 and 2 studies were quasi-RCTs.24,47
Interventions and Outcomes
The included studies aimed to investigate the effects of BFR-t in patients with ACL injuries at different time points before (prehabilitation) or after (rehabilitation) surgery (Figure 2). A total of 2 studies used BFR-t before ACLR as prehabilitation only,24,47 with Žargi et al 47 applying a cuff during surgery. In 3 studies, BFR-t was used in the rehabilitation period after surgery only, occurring at 2, 8, and 16 weeks after ACLR.21,23,36
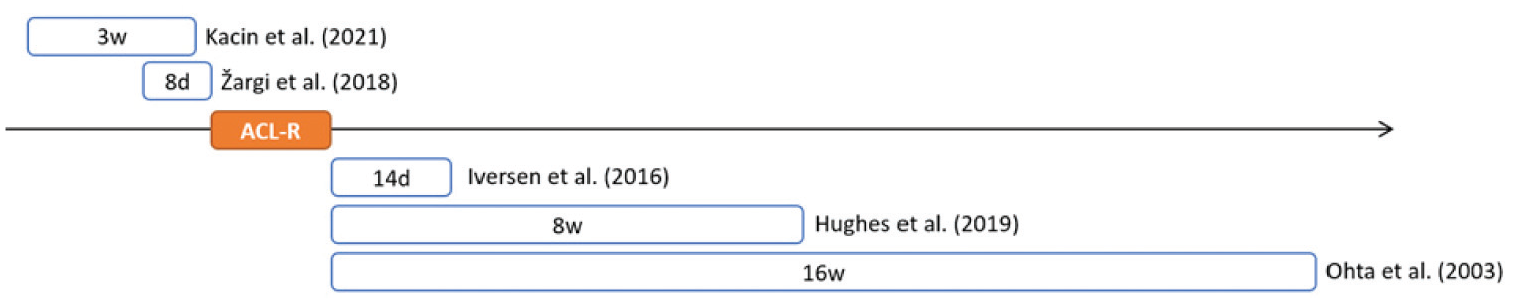
Intervention timing for each study. ACL-R, anterior cruciate ligament reconstruction (day of surgery).
There were 3 studies21,24,36 that assessed knee extensor muscle strength by measuring concentric isokinetic strength: 2 studies used 2 different angular velocities (60 and 120 deg/s 24 and 60 and 180 deg/s 36 ), and 1 study evaluated 3 angular velocities (60, 150, and 300 deg/s). 21 Additionally, 4 studies assessed knee extensor muscle size: 3 studies used MRI,23,24,36 and 1 study used ultrasound. 21 Only 1 study evaluated knee-specific PROMs, including the International Knee Documentation Committee subjective knee form, Knee injury and Osteoarthritis Outcome Score, Lysholm knee scoring scale, Tegner activity scale, and Lower Extremity Functional Scale. 21
The studies involved different BFR-t techniques (Table 2). Hughes et al 21 used an automatic personalized tourniquet system, Kacin et al 24 used a wide double-chamber pneumatic cuff with asymmetric pressure, Ohta et al 36 used an air tourniquet, and Iversen et al 23 and Žargi et al 47 used a 14 cm–wide contoured pneumatic occlusion cuff.
Methods and Interventions Used a
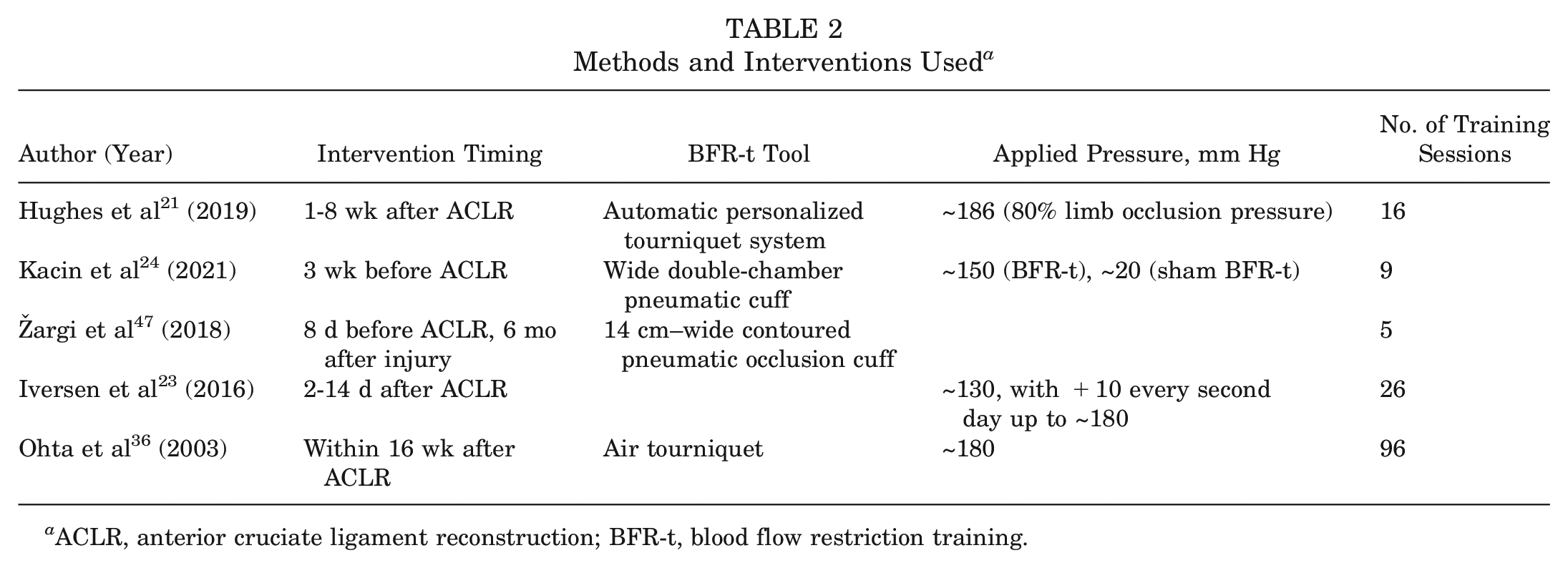
ACLR, anterior cruciate ligament reconstruction; BFR-t, blood flow restriction training.
The pressure applied differed between the studies. There were 2 studies that applied a pressure of 150 mm Hg to the BFR-t group and 20 mm Hg to the sham BFR-t group.24,47 One study increased the pressure up to 180 mm Hg from a starting point of 130 mm Hg. 23 Hughes et al 21 applied an occlusion pressure to the injured group of up to 186 mm Hg, about 80% of limb occlusion pressure. The remaining study applied a pressure of about 180 mm Hg. 36
Overall, 3 studies21,24,47 included tests and training interventions in laboratory settings. In the remaining studies,23,36 participants completed training with a BFR-t cuff independently at home after instruction (Appendix [Data Extraction], available online). Each study used different exercise programs: 4 studies prescribed the same exercises for both the intervention and the non–BFR-t groups.23,24,36,47 One study prescribed the same exercises for both the intervention and the non–BFR-t groups; however, the intervention group used a load of 30% of predicted 1RM, and the non–BFR-t group used a load of 70% of predicted 1RM. 21 The Appendix (available online) shows the detailed methods used to measure outcomes.
Quality of Studies
All 5 studies had a risk of bias (Figure 3). Three studies21,23,47 were at a high risk of performance bias, while 1 study was unclear. 36 The risk of selection bias was high in 2 studies36,47 and unclear in a third study. 23 No risk of detection or attrition bias was detected in any study. No study blinded both participants and assessors.
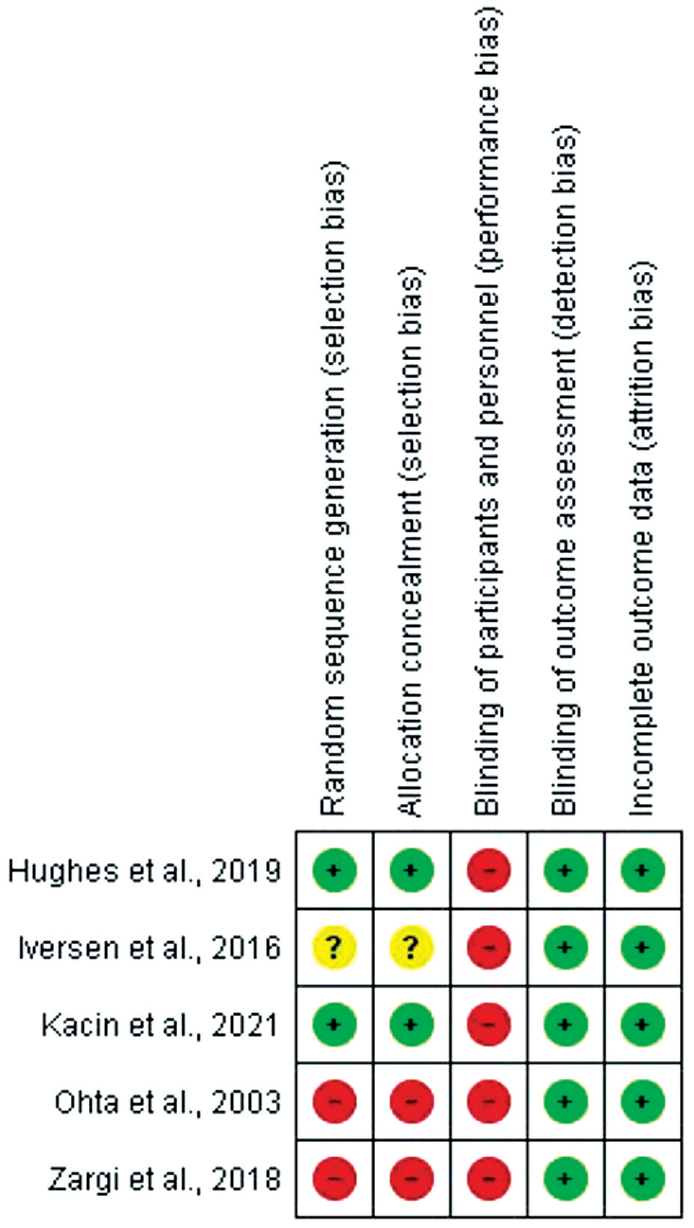
Risk-of-bias summary for the included studies, reported using a traffic light icon plot. Green, yellow, and red colors represent a low, unclear, and high risk of bias, respectively.
Findings
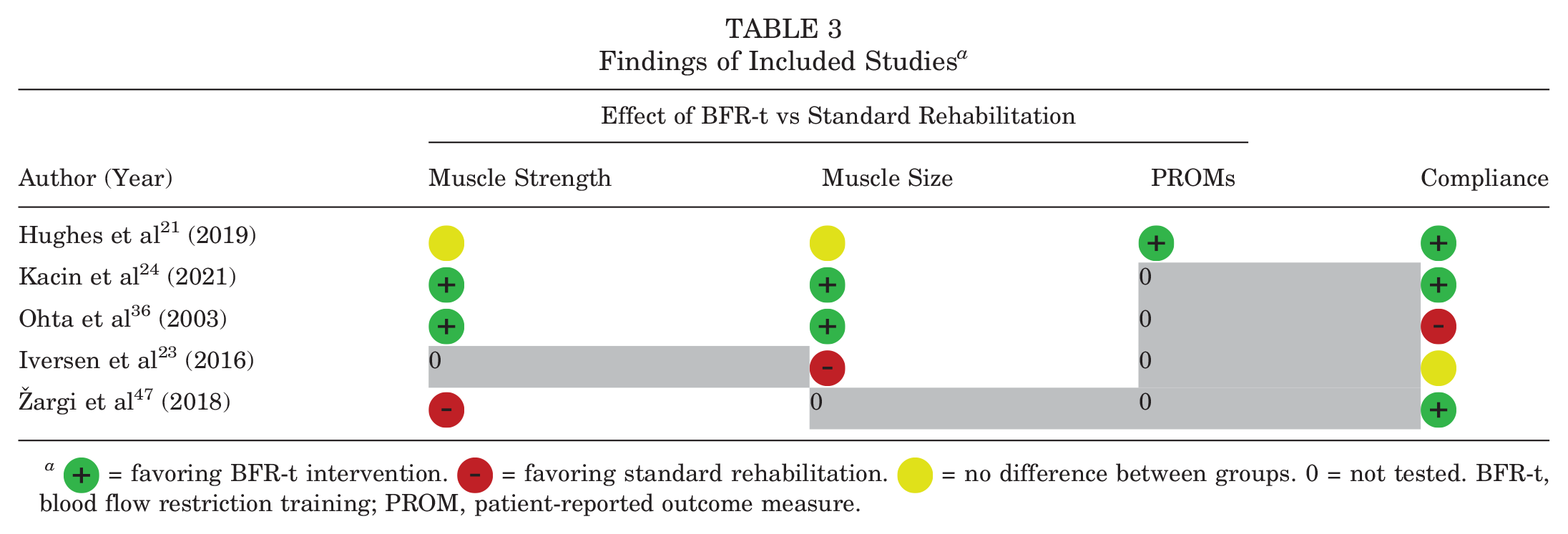
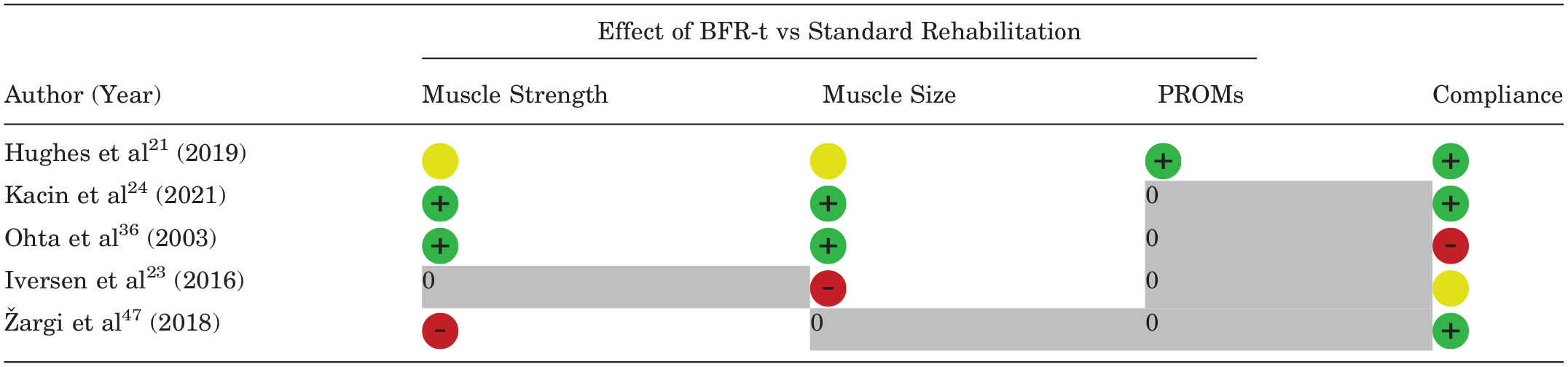
Overall, 4 studies investigated knee extensor and flexor muscle strength and/or muscle size changes after BFR-t. Only 1 study 21 also examined PROMs. There were 2 studies that reported a greater increase in muscle strength and muscle size in the BFR-t group compared with the non–BFR-t group (Table 3).24,36
Findings of Included Studies a
 = favoring BFR-t intervention.
= favoring BFR-t intervention.  = favoring standard rehabilitation.
= favoring standard rehabilitation.  = no difference between groups. 0 = not tested. BFR-t, blood flow restriction training; PROM, patient-reported outcome measure.
= no difference between groups. 0 = not tested. BFR-t, blood flow restriction training; PROM, patient-reported outcome measure.
Knee extensor and flexor muscle strength were assessed by unilateral 10RM leg presses and concentric isokinetic and isometric dynamometry. All 4 studies used validated imaging techniques to measure muscle size, 32 with 3 studies using MRI23,24,36 and 1 study using ultrasonography. 21 However, Hughes et al 21 did not report ultrasound operator training, which, given the dependence of ultrasound results on operator skill, may increase the probability of type II error.
Kacin et al 24 reported a greater increase in concentric isokinetic knee extension peak torque (at 60 and 120 deg/s) and quadriceps CSA for the BFR-t group compared with the sham BFR-t group. Changes in knee flexor muscle strength and hamstring muscle size were comparable between the 2 groups. Ohta et al 36 found that participants in the BFR-t group had greater increases in knee extensor muscle strength (both concentric isokinetic and isometric) and CSA than participants who underwent standard nonocclusion rehabilitation.
Hughes et al 21 did not observe any significant difference in 10RM strength gains between the BFR-t and non–BFR-t groups after 8 weeks of training. The BFR-t group showed similar muscle strength and muscle size improvements to the heavy-load resistance training group after ACLR and rehabilitation. BFR-t attenuated concentric isokinetic strength losses from before surgery to after training (8 weeks after surgery) more than heavy-load resistance training for knee extensors and flexors at a range of angular velocities. However, they reported a reduction in knee extension peak torque at 60 deg/s in both groups, and knee extension peak torque was lower than pre–ACLR values in both groups. They also reported a similar increase in knee extensor muscle size in both groups. The improvement in PROM scores was greater in the BFR-t group and was associated with better physical function.
Iversen et al 23 reported a loss of quadriceps CSA (~13%) in both the BFR-t and the non–BFR-t groups at 14 days after ACLR, with no significant difference between groups. Žargi et al 47 observed a similar reduction in knee extension torque during a maximum voluntary isometric contraction in both the BFR-t and the sham BFR-t groups from before surgery to 12 weeks after ACLR.
Because of the heterogeneous assessment methods, a meta-analysis based on these results could not be conducted, and reporting guidelines for a narrative synthesis were followed. 6
Discussion
This systematic review included 5 studies that examined the effects of BFR-t on knee extensor and flexor muscle strength and muscle size as well as perceived knee function after ACL injuries (and reconstruction). The results of these studies support the reasonable conclusion that BFR-t has an unclear effect on muscle strength and muscle size. Specifically, it is unclear if BFR-t increases or decreases knee extensor and flexor muscle strength and muscle size in comparison with standard nonocclusion rehabilitation for patients with ACL injuries. However, BFR-t may improve knee-specific physical function and PROM scores. 21
Likely because of the heterogeneity of the methods and interventions used, current evidence is insufficient to determine whether BFR-t significantly affects these outcome measures. Furthermore, it is unclear which BFR-t protocol will be most beneficial for patients undergoing ACLR. When examining knee extensor and flexor muscle strength, 2 studies found greater strength gains with BFR-t compared with nonocclusion training,24,36 and 1 study 21 found no difference in strength gains between the intervention and nonintervention groups. Also, 1 study 47 showed that BFR-t did not attenuate strength losses more than standard prehabilitation. Overall, 50% of studies that measured muscle size observed a difference between groups and reported a greater increase in muscle size for participants who underwent BFR-t compared with those who underwent standard rehabilitation. Despite detecting a change in muscle size, the other half of the studies did not observe any significant difference between groups. One study detected a decrease in CSA in both groups after 14 days from ACLR 23 ; these findings suggest that BFR-t did not attenuate the loss in CSA more than non–BFR-t rehabilitation. The only study 21 that assessed PROMs reported a greater improvement on all PROMs for the BFR-t group compared with the non–BFR-t group.
Previous Findings
Hughes et al 19 conducted a systematic review of 20 RCTs from 2000 to 2016 comparing low-load and high-load lower limb training with and without BFR-t. Their findings indicate that combining BFR-t and low-load training in rehabilitation settings can produce a greater muscle strength response than low-load training alone. The current review, however, did not find the same result; instead, it demonstrated uncertainty about the efficacy of BFR-t on muscle strength and muscle size in patients with an ACL injury. Multiple factors could explain these inconsistencies, including the initial injury (Hughes et al 19 only included 3 studies involving participants with ACL injuries) and age (Hughes et al 19 reviewed 13 studies with elderly participants).
Effect of BFR-t on Muscle Strength and Muscle Size
Kacin et al 24 observed greater increases in knee extensor and flexor muscle strength and CSA when using low-load BFR-t compared with standard nonocclusion training. However, they only compared the magnitude of the changes between the BFR-t and sham BFR-t groups, without assessing whether these changes were significant. Their intervention occurred 3 weeks before ACLR. Although it is not possible to state that BFR-t had a significant effect, the difference recorded between groups suggests that the short application time of BFR-t induced positive physiological adaptations, demonstrating that it can be a useful prehabilitation tool.
Ohta et al 36 also observed a greater increase in knee extensor muscle strength and CSA. However, the knee flexor CSA results showed attenuation in atrophy in both the BFR-t and the non–BFR-t groups, with no significant difference between the 2 groups.
Ohta et al 36 showed a mismatch between their presented results and their interpretation of them. The authors’ interpretation suggests a significant increase in knee muscle strength in the BFR-t group; however, concentric isokinetic and isometric knee extensor/flexor outcomes (interlimb ratios) did not show a significant increase but a smaller reduction from before surgery to after ACLR in the BFR-t group. The authors only independently compared the interlimb ratios (asymmetry) between the groups before and after ACLR but did not assess the group and time interaction to determine if a significant reduction existed over time and whether the magnitude of this reduction differed between the groups. Additionally, an interpretation of their knee flexor muscle strength outcomes should be carefully considered. Hamstring tendon graft harvesting likely led to semitendinosus muscle atrophy, with some individual variability in recovering from that process, which makes an interpretation of their results challenging.
Regarding muscle size, the authors reported a statistically significant increase in knee extensor CSA in the BFR-t group at 16 weeks after ACLR. However, the data are presented as 2 parameters and ratios, which cannot be compared directly: CSA of the injured leg versus CSA of the healthy leg before surgery and CSA of the injured leg before versus after surgery. The authors reported that knee extensor CSA had an 8% increase in the non–BFR-t group and only 1% increase in the BFR-t group after 16 weeks of rehabilitation, with no significant between-group difference. Overall, this study seems to have several methodological limitations; therefore, its results should be interpreted cautiously.
“Dose” of Interventions and Timing of Assessments
Žargi et al 47 and Iversen et al 23 observed reduced muscle strength and muscle size, respectively. In Žargi et al's study, the BFR-t protocol was applied for 5 sessions in the 8 days before ACLR, showing that the reduction in knee extension torque during a maximum voluntary isometric contraction from before surgery to 12 weeks after ACLR was similar between groups. Therefore, when applied before ACLR, BFR-t did not attenuate strength losses more than a standard prehabilitation program. However, in this study, no muscle function assessment was performed immediately after the BFR-t intervention. Therefore, the immediate effects of the preconditioning intervention are unknown. Also, the low number of training sessions and the intervention timing were likely not enough to see significant results, as the current literature suggests that the minimal duration of the intervention to observe a significant difference is 6 to 12 weeks and 12 to 24 weeks for muscle strength and muscle size gains, respectively. 40 Kacin et al 24 also applied BFR-t before ACLR. However, their intervention lasted 3 weeks, with measurements performed before and after the intervention but not after ACLR. The authors reported increased knee extensor and flexor muscle strength after BFR-t compared with sham BFR-t.
Iversen et al 23 reported that the application of intermittent BFR-t between 2 and 14 days after ACLR did not significantly prevent quadriceps atrophy more than standard training. Again, the choice of intervention timing could have affected the outcomes because of postoperative pain, swelling, stiffness, and limited range of motion, 15 restricting the participant's ability to exercise, especially as it was a nonsupervised home-based exercise program.
Hughes et al 21 is the only study in this review that assessed knee extensor and flexor muscle strength and muscle size as well as knee-specific PROMs. According to their findings, muscle strength and muscle size increased similarly in both the BFR-t and the non–BFR-t groups after ACLR and rehabilitation, in line with previous literature that showed that an 8-week BFR-t protocol based on an external load of 30% of 1RM resulted in a similar increase in 10RM strength compared with high-load resistance training.5,27 In contrast with Kacin et al, 24 who used open kinetic chain exercises, Hughes et al 21 used closed kinetic chain exercises and reported a reduction in knee extension concentric peak torque at 60 deg/s in both groups. Previous literature reported that open kinetic chain exercises improve knee extension peak torque at 60 deg/s 24 ; therefore, a BFR-t protocol after ACLR involving both methods could be more beneficial to regaining muscle strength. However, when comparing these 2 studies, some consideration is needed: during the first few weeks after reconstructive surgery, patients experience knee pain, swelling, and inflammation and must be careful to prevent graft ruptures. Kacin et al 24 conducted the intervention before surgery, while Hughes et al 21 conducted the intervention after surgery. Therefore, differences in the knee condition before and after surgery should be considered when comparing study outcomes. Knee flexion peak torque results are consistent with Ohta et al. 36 The different effect of BFR-t on flexor muscles is likely because of the use of a hamstring tendon graft for ACLR rather than the training tool itself. Namely, harvesting a hamstring tendon for ACLR could result in a significant secondary injury to the medial hamstring muscle, thus negatively affecting the outcomes of the flexor muscles. 46
Muscle size data concur with a meta-analysis by Lixandrão et al, 28 which reported equal improvements in muscle mass in both the low-load BFR-t and the high-load resistance training groups of healthy participants. In both groups, these increases were observed in weeks 5 to 8, which is in line with previous studies in which the muscle size increase was estimated at 6% to 8% in 5 to 12 training weeks.10,11
Despite Hughes et al’s 21 providing an accurate description of the methods used for muscle size measurements, it is unclear who the ultrasound assessor was. Ultrasonography is recognized as a valid, reliable, and repeatable technique for the assessment of CSA. 42 However, it is impossible to determine if the sonographers of this study received adequate training. The other studies used MRI, a gold standard imaging modality utilized to examine muscle CSA and volume. 32 MRI is considered a valid and reliable modality 8 ; the fact that Hughes et al 21 is the only study that did not use MRI makes the results less comparable.
Interestingly, Hughes et al 21 also observed that knee pain was reduced more in the BFR-t group compared with the non–BFR-t group, leading to greater physical function improvement. This could be caused by a lighter load (30% of 1RM) applied to the BFR-t group and by the hypoalgesic effect that involves mechanisms such as conditioned pain modulation, the recruitment of fast-twitch fibers, opioid and endocannabinoid systems, and increased heart rate and blood pressure. 20 These mechanisms, however, are not yet understood.
Strengths and Limitations
This review, answering a question that has not been addressed in the current literature, has many strengths. A comprehensive and extensive study search was performed in multiple databases, registers, and previous systematic reviews, identifying a homogeneous population. A comparison of studies that reported conflicting results raised more questions about BFR-t and its efficacy in ACL rehabilitation and paves the way for future research. However, there are also some limitations. A comparison between results could not be accurately performed because of the variability of the assessment methods, intervention timing, and training plans. Despite efforts to assess the risk of bias in all studies, the findings may have been misleading because of type I or II errors; a power analysis for clinical studies was not performed, and PROM scores could not be compared, as only 1 study assessed them. In 2 studies, the rate of training compliance may have been negatively affected. All these considerations could have contributed to a type II error.
Unfortunately, this review did not find any relevant studies that included patients in their late teens, which is a high-risk population for ACL injuries. This is an unmet need and should be prioritized in future research studies.
Future Perspective
Based on the findings of the included studies, it is reasonable to conclude that the effect of BFR-t on muscle strength and muscle size is uncertain, and it is unclear whether BFR-t increases or decreases knee extensor and flexor muscle strength and muscle size more than standard nonocclusion rehabilitation for those with an ACL injury. BFR-t may improve knee-specific PROM scores and physical function. However, given the abovementioned limitations, these findings should be interpreted cautiously.
Multiple potential confounding factors affect the efficacy of BFR-t, including the population, condition, assessment method, intervention timing, and exercise protocol. The high variability of assessment methods and protocols in this review demonstrates the importance of standard methodology and protocols when employing BFR-t in rehabilitation clinical practice and research. Therefore, future RCTs should consider target population characteristics, intervention timing and outcomes, intervention content, outcome measures, and supervision of compliance.
Conclusion
There is growing interest in using BFR-t in ACL rehabilitation in clinical settings. This review has shed light on the potential effects of BFR-t on muscle strength, muscle size, and knee-specific PROM scores in patients with ACL injuries. However, it demonstrated that because of the heterogeneity of the methods and interventions used, current evidence is insufficient to determine whether BFR-t substantially affects these outcome measures. The range of outcome measures used by Hughes et al 21 appears to be the most comprehensive. It is also unclear which BFR-t protocol is the most beneficial for patients undergoing ACLR. Furthermore, none of these studies has been replicated in large populations. Future studies should be conducted to develop a better understanding of the most beneficial rehabilitation program using similar outcome measures. Finally, to avoid unmeasured bias, larger sham-controlled studies will provide more definitive answers about the efficacy of these methods.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465241232002 – Supplemental material for Comparison of Blood Flow Restriction Interventions to Standard Rehabilitation After an Anterior Cruciate Ligament Injury
Supplemental material, sj-docx-1-ajs-10.1177_03635465241232002 for Comparison of Blood Flow Restriction Interventions to Standard Rehabilitation After an Anterior Cruciate Ligament Injury by Valentina Colombo, Tamara Valenčič, Kat Steiner, Jakob Škarabot, Jonathan Folland, Oliver O’Sullivan and Stefan Kluzek in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank the following people for their contribution to patient and public involvement (PPI), protocol development, and discussion regarding the clinical effectiveness of these methods: Dr Rebecca Gould, Mr Fionn MacPartlin, and Mr Alan Hazlett.
Submitted May 28, 2023; accepted December 12, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at https://education.sportsmed.org/Public/Catalog/Home.aspx?CourseSearch=1&Criteria=9&Option=25. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.