
Abstract
Background:
Despite the well-established role of lateral extra-articular procedures (LEAPs) in reducing failure rates after anterior cruciate ligament (ACL) reconstruction (ACLR) in the adult population, similar in-depth research for the adolescent and pediatric population remains lacking.
Purpose:
To examine the effect of the LEAP augmentation on the rerupture rate after ACLR in patients aged <18 years.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a retrospective analysis of prospectively collected data from October 2012 to June 2020, involving adolescents <18 years old undergoing primary ACLR with a minimum follow-up of 2 years. Two groups, matched for age, sex, Tegner activity scale, and presence of meniscal injury, were established: ACLR alone and ACLR+LEAP augmentation. The primary outcome measure was the rate of rerupture after ACLR. The secondary outcome measures were the rate of non–graft rupture related reoperation after ACLR; rate of return to sport (RTS) rate, timing, and level compared with preinjury status; and functional scores including the International Knee Documentation Committee (IKDC) score, Knee injury and Osteoarthritis Outcome Score (KOOS) (Pain, Symptoms, Activities of Daily Living, Sport and Recreation, and Quality of Life), Tegner activity scale score, ACL Return to Sport after Injury (ACL-RSI) score, and Lysholm score.
Results:
After accounting for follow-up losses, we analyzed 132 patients who underwent ACLR alone and 121 patients who underwent ACLR+LEAP from the initial 147 per group. The mean age of the patients in both groups was 16.1 years (SD, 1.1 and 1.0 years, respectively), with similar patient and injury characteristics across both groups (P > .05). Both groups also showed comparable preoperative functional scores. A significantly lower preoperative ACL-RSI score was observed in the ACLR-alone group compared with the ACLR+LEAP group (P = .0044). Graft rupture was significantly less common in the ACLR+LEAP group (2.5%) than in the ACLR-alone group (13.6%) (P = .002). The attributable risk reduction for ACLR+LEAP was 11.1%, and the calculated number needed to treat was 9. Kaplan-Meier analysis showed significantly better rerupture-free survival at 5 years for the ACLR+LEAP group (P = .001). Cox regression confirmed a 6-fold increased rerupture risk in the ACLR-alone group (P = .004). At the final follow-up, despite similar IKDC, KOOS, Lysholm, and ACL-RSI values across both groups, the ACLR+LEAP group had a significantly higher Tegner score (7.2 vs 6.3; P = .0042). No significant differences were observed in RTS rates or sport level compared with preinjury states between the groups.
Conclusion:
ACLR+LEAP augmentation significantly reduced rerupture risk and facilitated higher postoperative activity levels in adolescents.
Registration:
NCT02511158 (ClinicalTrials.gov identifier).
Keywords
Anterior cruciate ligament (ACL) ruptures are an increasingly diagnosed injury in the adolescent population, with a steady rise in the rate of ACL reconstructions (ACLRs), increasing from 17.6 in 1990 to 50.9 in 2009 per 100,000 persons aged 3 to 20 years.1,8 This is likely because of the increased engagement of adolescents in competitive sport activity.1,8 These injuries can result in significant morbidity, affecting the sporting career of young athletes, and may lead to early onset of osteoarthritis.3,22,36
One particularity of this age group is the increased susceptibility to graft rerupture.6,11,42 Recent systematic analysis identified age, specifically <20 years, as a significant risk factor of graft failure.6,11,42 Further key predictors of failure identified across these studies in the general population include smaller graft diameter, absence of the lateral extra-articular procedure (LEAP) in adult studies, greater posterior tibial slope, high-grade knee laxity, the use of allograft instead of autograft, and an early return to high-level sport activities.6,11,42 When it comes to physis consideration, a recent systematic review revealed that although the physeal-sparing ACLR technique offered better knee laxity restoration compared with complete transphyseal and partial transphyseal methods, all 3 approaches resulted in similar clinical outcomes, specifically in terms of rerupture rates, growth disturbances, and axial deviations. 29
Despite the well-established role of LEAP in reducing failure rates after ACLR in the adult population,15,38 a similar depth of research for the pediatric population remains lacking. The current literature primarily comprises descriptive studies and a systematic review of descriptive studies, ‖ with only a handful of comparative studies available.12,20,25,31 These comparative studies often have limitations because of their design, 20 sample size,25,31 lack of matched comparison groups,20,25 and absence of randomization.20,25,31 This gap in substantial evidence was underscored in a recent cross-sectional survey by Madhan et al, 24 who examined the practices of 87 surgeons in the Pediatric Research in Sports Medicine Society. 24 This study revealed that only 56% of surgeons sometimes performed LEAP with primary ACLR and 79% with revision ACLR, with the predominant deterrent being a perceived lack of sufficient evidence to support these practices. 24
The primary aim of this study was to evaluate the rate of rerupture after ACLR in adolescent patients when treated with or without LEAP. The secondary aim of this study was to compare the rates of non–graft rupture related reoperation and functional outcomes of these 2 strategies, considering several patient-reported outcome measures and return to sport (RTS).
We hypothesized that the addition of LEAP would significantly decrease the failure rate after ACLR.
Methods
Study Design and Setting
This was a retrospective analysis of prospectively collected data between October 2012 and June 2020 at a specialized sport surgery referral center. It forms part of the French prospective ACLR cohort study (ClinicalTrials.gov identifier: NCT02511158).
Inclusion Criteria
Inclusion criteria included patients <18 years of age who underwent primary ACLR and who had ≥2 years of follow-up. Exclusion criteria were revision surgery, multiligamentous knee injury, and refusal to participate in the study.
To minimize selection bias, a matching technique was used to establish 2 comparable groups. These groups were differentiated based on whether a LEAP was performed during the ACLR. The variable criteria used for matching included age, sex, Tegner activity scale (TAS), and the presence of a meniscal injury.
Outcome Measures
The primary outcome measure was rerupture after ACLR. The secondary outcome measures were the rate of non–graft rupture related reoperation (including arthrolysis, cyclops, and meniscal injury), the RTS metrics (rate, timing, and level as compared with preinjury status), and functional scores including the International Knee Documentation Committee (IKDC) score, 16 Knee injury and Osteoarthritis Outcome Score (KOOS) (Pain, Symptoms, Activities of Daily Living, Sport and Recreation, and Quality of Life),28,33 TAS score, 39 ACL Return to Sport after Injury (ACL-RSI) score,2,40 and Lysholm score. 23
A subgroup analysis was also undertaken to compare the outcome measures when only the quadrupled hamstring grafts were taken into account.
Collected Data
All data were collected prospectively using an internet-based software (Websurvey) that was accessed by both surgeons and patients. The collected data comprised patient characteristics including age at the time of surgery, body mass index, sex, and side, as well as circumstances of the accident (public road accident, domestic accident, or sport accident), presence of chondral lesion, meniscal lesion, physical examination finding, time between accident and surgery, and level of sport activity (competition, occasional active leisure, regular leisure, professional, or sedentary). Other preoperative measures included preoperative IKDC subjective score; KOOS score for Symptoms and stiffness; 33 Lysholm score; TAS score; and ACL-RSI score.
Surgical Intervention
Six senior orthopaedic surgeons specializing in sport surgery (including N.L., A.G., A.M., A.H.) operated on patients in this study, using different ACLR techniques depending on the surgeon's preference. Every surgeon in the study has both types of techniques—ACLR with or without LEAP—in their surgical armamentarium. The decision to opt for one technique over the other was multifactorial. Factors taken into consideration included the type and level of the patient's sport activity, patient demand, recurvatum, valgus knee alignment, chronicity of the lesion, presence of suturable meniscal lesion, and the severity of the preoperative rotational instability observed. Patients with an open physis were treated with the physeal-sparing quadrupled hamstring technique21,32 and partial transphyseal iliotibial band–based modified Macintosh procedures (combined extra- and intra-articular reconstruction). 9 Patients with a closed physis were treated with quadrupled hamstring grafts (doubled gracilis and doubled semitendinosus or quadrupled semitendinosus), bone–patellar tendon–bone procedures, or iliotibial band–based modified Macintosh procedures. 9
LEAPs included lateral extra-articular tenodesis (LET), 43 anterolateral ligament (ALL) reconstruction using double-bundled gracilis, 34 and combined extra- and intra-articular reconstruction using the modified Macintosh procedure. 9
Exclusively, autografts were used for all surgical interventions in this study.
Postoperative Protocol
All patients adhered to a standard postoperative rehabilitation protocol, which required the use of a hinged brace in full passive extension for several days, after which they commenced a rehabilitation program. The brace remained in use until patients demonstrated effective quadriceps control and mastery of the screw home mechanism, without a strict time frame imposed. Crutches were used until the patient was able to walk without a limp. Full weightbearing was permitted throughout this process.
Ethical and Legal Considerations
The study was approved by the research ethics committee of the center. Patient consent was obtained from the patients when they completed the online survey.
Study Population
Of the 549 consecutive patients operated on during the study time frame, 55 refused to participate in the cohort, leaving 494 eligible participants. These participants were divided into 2 groups: ACLR without LEAP (235 patients) and ACLR+LEAP (259 patients). Application of the propensity score matching technique yielded 147 patients in each arm. After loss to follow-up was accounted for, the final groups analyzed included 132 patients in the ACLR-alone group and 121 patients in the ACLR+LEAP group (Figure 1).
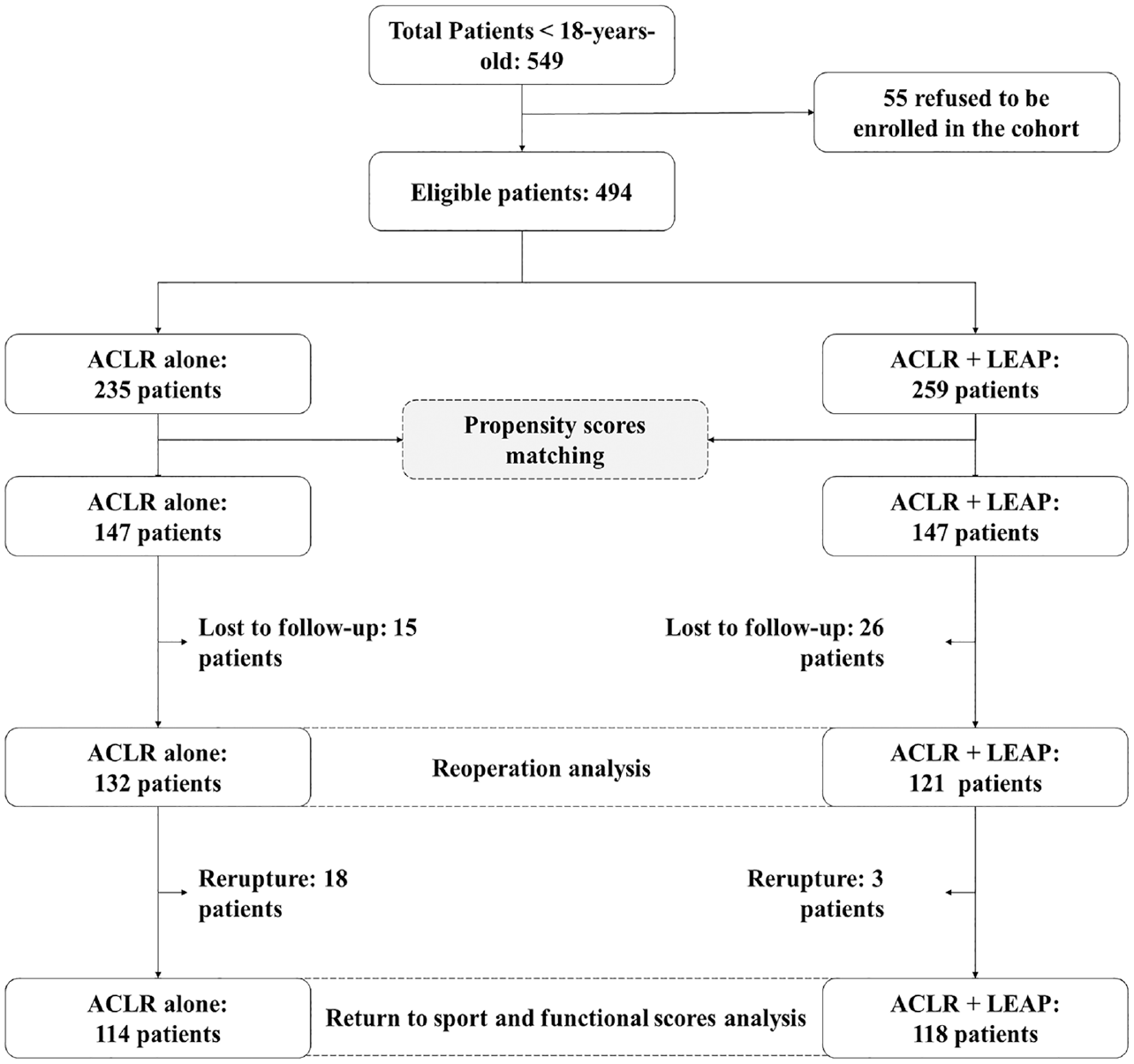
Flowchart for inclusion and analysis. ACLR, anterior cruciate ligament reconstruction; LEAP, lateral extra-articular procedure.
Statistical Analysis
Based on previous studies,12,25,31 the proportion of reruptures in the ACLR-alone group was estimated to be 0.149 and the proportion of reruptures in the ACLR+LEAP group was calculated to be 0.041. It was subsequently determined that 115 participants in each group were required to achieve a statistical power of at least 80% and a significance level of .05.
The study population was matched using a propensity score to minimize selection bias in the 2 groups of reconstruction techniques. Participants were matched in a 1:1 ratio, and matching was performed using a logit scale with a caliper width of 0.2. The matched variables included age, sex, TAS score, and the presence of a meniscal injury.
Qualitative variables, described by their frequency and percentage, were compared using the Pearson chi-square test or Fisher exact test, depending on group sizes. Quantitative data were described using means and standard deviations and were compared using appropriate statistical tests, either the Student t test or Mann-Whitney U test.
Kaplan-Meier curves were generated to assess the survival probability of rerupture at 5 years after surgery between the 2 groups and were compared using the log-rank test using time in months as the time scale. Additionally, a Cox regression model was used to estimate the risk of rerupture based on the type of surgery performed, expressed as a hazard ratio (HR). Two additional metrics were calculated to further clarify the comparative effectiveness of the treatments: the number needed to treat (NNT) and the absolute risk reduction (ARR).
A P value of <.05 was considered statistically significant. All statistical analyses were performed using R software (Version 4.2; R Foundation for Statistical Computing).
Results
Patient Characteristics
Both groups had a mean age of 16.1 years (range, 12.9-17.9 years) (P > .05). The median delay from accident to surgery was 3.7 months (range, 0.3-122.6 months) for the ACLR-alone group and 3.5 months (range Min-Max, 0.0-81.0 months) for the ACLR+LEAP group (P > .05). The mean follow-up period was 4.4 years (SD, 1.6 years) for the ACLR+LEAP group and 5.3 years (SD, 2.2 years) for the ACLR-alone group (P > .05). There was no significant difference between ACLR-alone and ACLR+LEAP groups in terms of body mass index, sex, knee involved, sport type, sport level, accident circumstances, associated chondral and meniscal lesions, and preoperative functional scores (P > .05). However, there was a statistically significant difference in the ACL-RSI score, which was 34.0 (SD, 29.7) for the ACLR-alone group and 43.5 (SD, 28.5) for the ACLR+LEAP group (P = .0044) (Table 1).
Preoperative Characteristics of Patients in Both Study Groups a
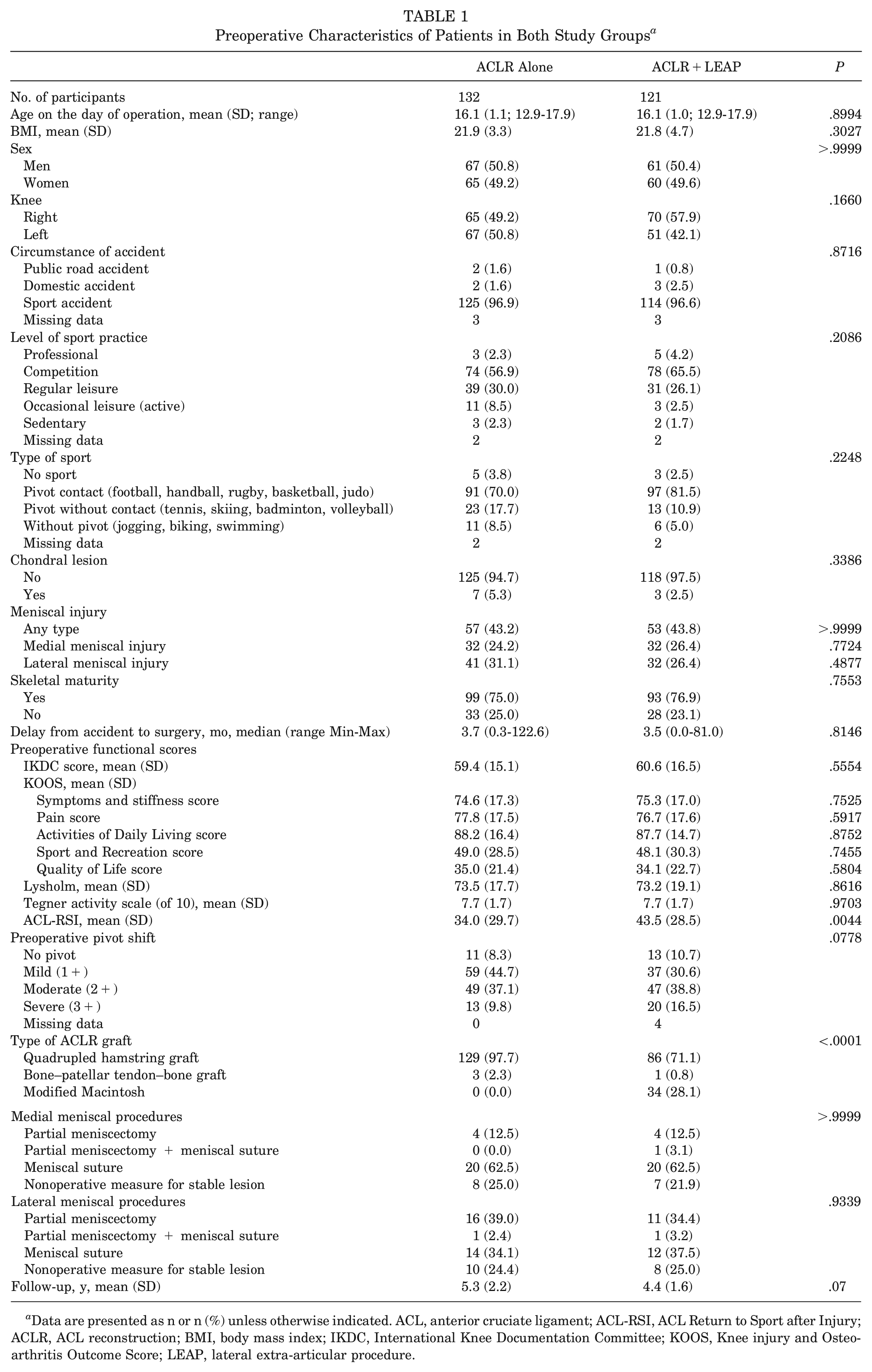
Data are presented as n or n (%) unless otherwise indicated. ACL, anterior cruciate ligament; ACL-RSI, ACL Return to Sport after Injury; ACLR, ACL reconstruction; BMI, body mass index; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; LEAP, lateral extra-articular procedure.
In terms of intra-articular graft usage, the quadrupled hamstring was predominant, used in 129 (97.7%) of the ACLR-alone procedures and 86 (71.1%) of the ACLR+LEAP procedures. The bone–patellar tendon–bone graft was rarely used, with only 3 (2.3%) in the ACLR-alone procedures and 1 (0.8%) in the ACLR+LEAP procedures. In addition, the iliotibial band–based modified Macintosh procedure was used in 34 (28.1%) of the ACLR+LEAP procedures.
LEAP was done using doubled gracilis ALL reconstruction in 18 patients (14.9%), LET in 69 patients (57.0%), and as part of the combined extra- and intra-articular reconstruction using the modified Macintosh procedure in 34 patients (28.1%).
Comparison of Reoperation Rates After ACLR
Graft rupture was significantly less common in the ACLR+LEAP group (2.5%) than in the ACLR-alone group (13.6%) (P = .002). All reruptures observed in both groups involved quadrupled hamstring grafts. Within the ACLR+LEAP group, all 3 instances of graft rerupture occurred with the use of the LEAP tenodesis technique. Furthermore, the mean time to rerupture was slightly longer in the ACLR+LEAP group (mean, 24.5 months; SD, 2.3 months) than in the ACLR-alone group (mean, 18.6 months; SD, 11.9 months), although this difference was not statistically significant (P = .185). The ARR for ACLR+LEAP was 11.1% with an NNT of 9 (Table 2).
Graft Rupture and Reoperation Rates in ACLR-Alone and ACLR+LEAP Groups a
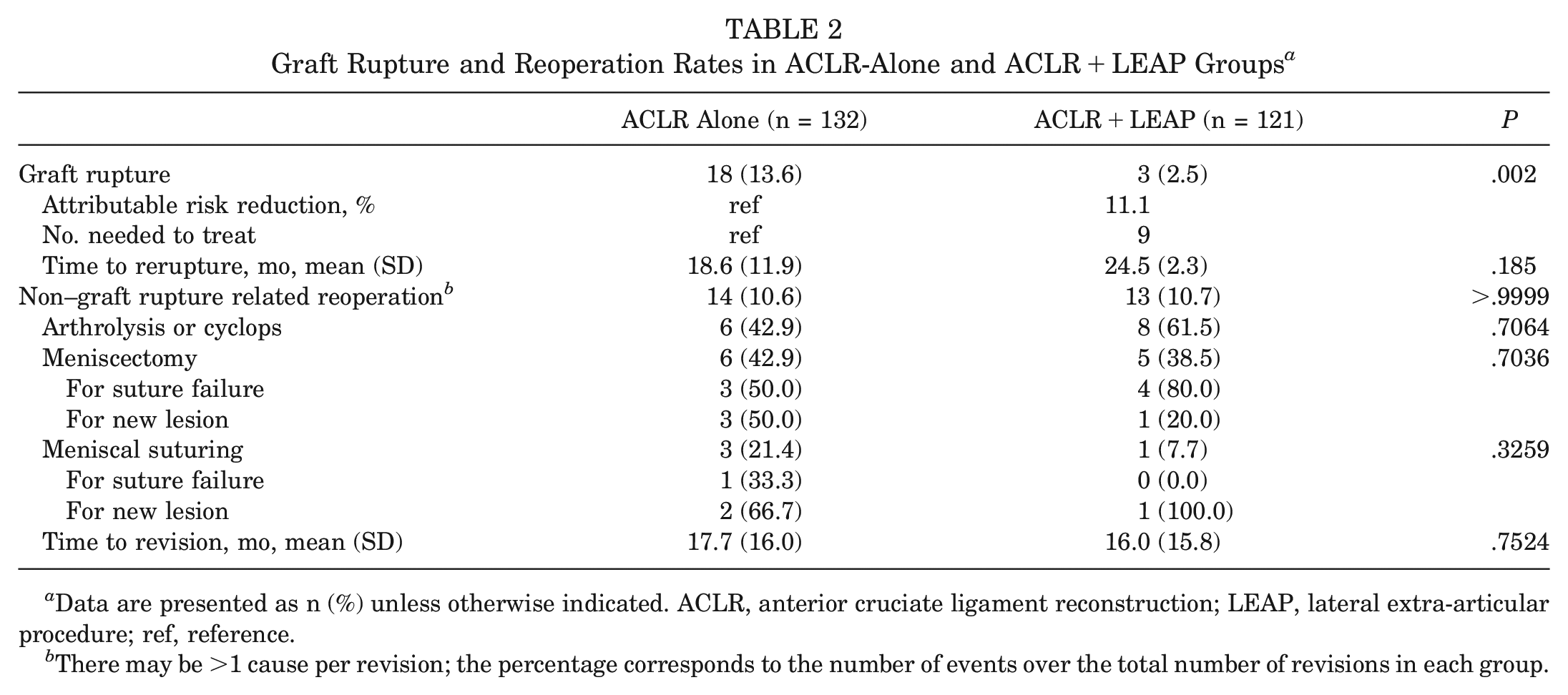
Data are presented as n (%) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; LEAP, lateral extra-articular procedure; ref, reference.
There may be >1 cause per revision; the percentage corresponds to the number of events over the total number of revisions in each group.
Non–graft rupture related reoperations occurred in 10.6% of the ACLR-alone group and 10.7% of the ACLR+LEAP group, a difference that was not statistically significant (P > .05). The mean time to surgical revision was 17.7 months (SD, 16.0 months) for the ACLR-alone group and 16.0 months (SD, 15.8 months) for the ACLR+LEAP group, again with no significant difference (P > .05). Specific causes for surgical revisions—arthrolysis or cyclops, meniscectomy, and meniscal suturing—showed no significant differences between the groups (P > .05)
Kaplan-Meier Survival Curve
The Kaplan-Meier survival curves indicated a statistically significant divergence in rerupture rates between the 2 groups (P = .001; log-rank test), favoring the ACLR+LEAP group (Figure 2). Specifically, the rerupture-free survival rate for the ACLR-alone group at 5 years was 86.4%, compared with 97.5% for the ACLR+LEAP group.
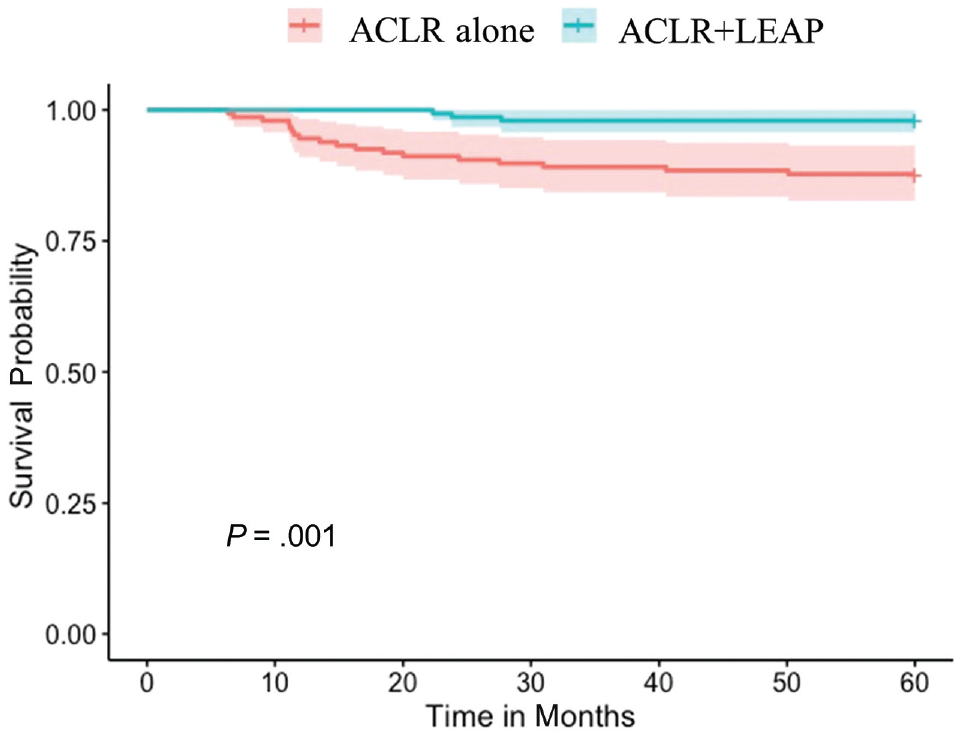
Kaplan-Meier survival curve at 5 years of follow-up. ACLR, anterior cruciate ligament reconstruction; LEAP, lateral extra-articular procedure.
Cox Proportional Hazards Model Regression Analysis
The risk of rerupture was >6 times higher for the ACLR-alone group (HR, 6.08; 95% CI, 1.79-20.7; P = .004) than for the ACLR+LEAP group, which served as the reference group (Table 3).
Cox Model to Estimate the Risk of Rerupture Based on the Type of Procedure Performed a
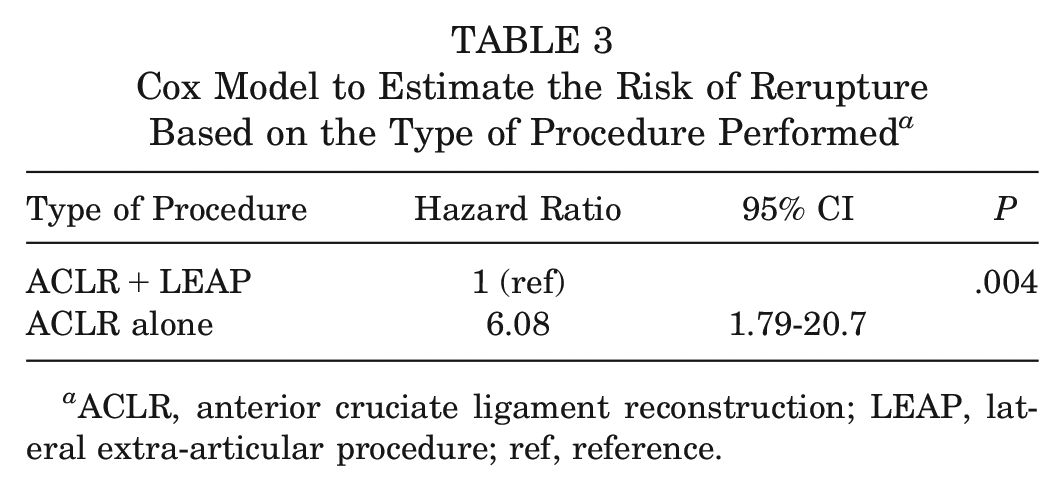
ACLR, anterior cruciate ligament reconstruction; LEAP, lateral extra-articular procedure; ref, reference.
Comparison of Postoperative RTS and Functional Scores
At the final follow-up, both the ACLR-alone and the ACLR+LEAP groups showed comparable scores in various clinical outcome measures, including IKDC score, KOOS, Lysholm score, and ACL-RSI score, with no statistically significant differences. However, an interesting divergence was noted in the TAS score. Despite starting from an identical preoperative baseline of 7.7, the ACLR+LEAP group outperformed the ACLR-alone group, posting a TAS of 7.2 versus 6.3 (P = .0042) (Table 4).
Clinical Scores and Return to Sport at Final Follow-up a
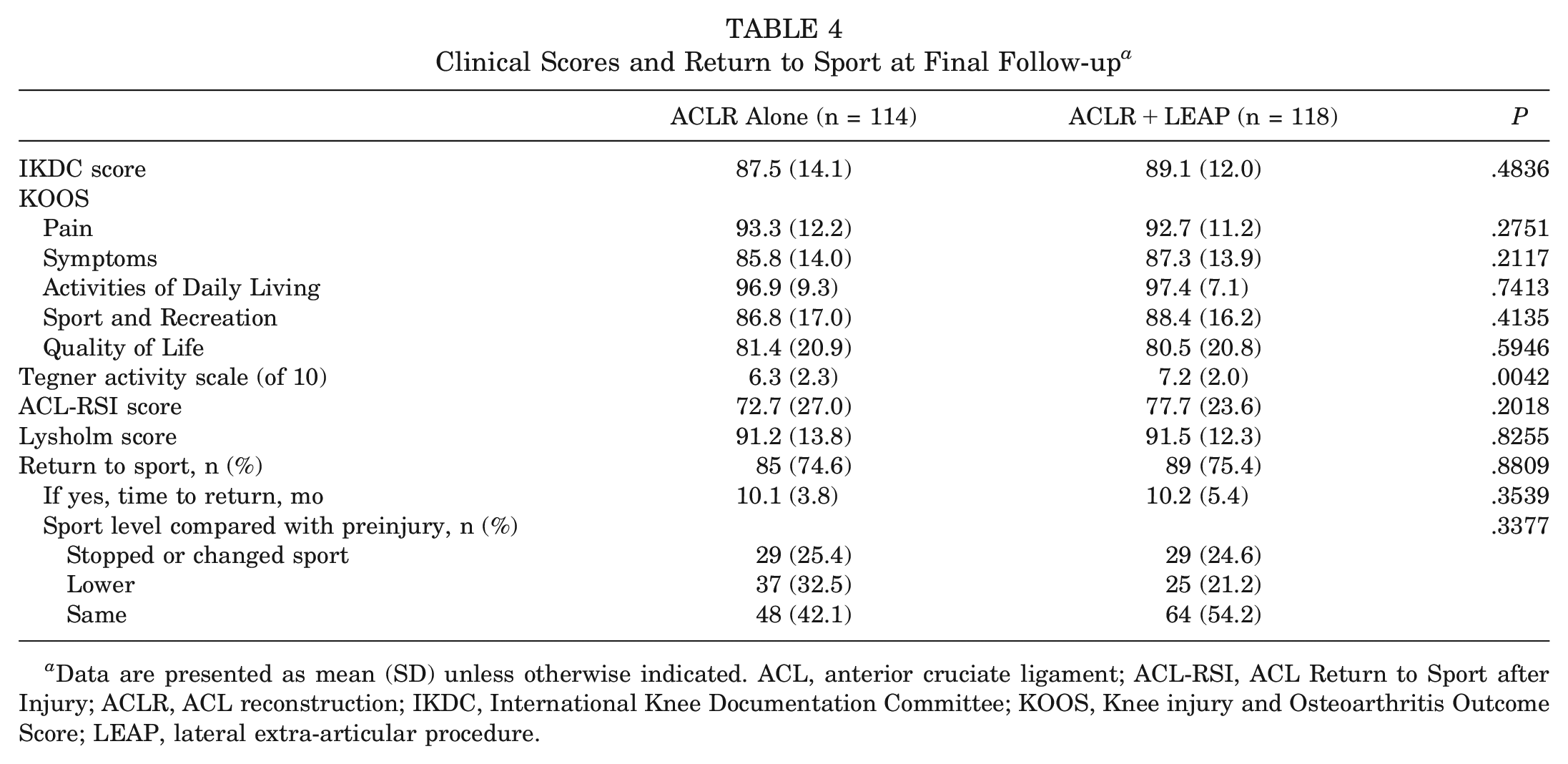
Data are presented as mean (SD) unless otherwise indicated. ACL, anterior cruciate ligament; ACL-RSI, ACL Return to Sport after Injury; ACLR, ACL reconstruction; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; LEAP, lateral extra-articular procedure.
The rate of RTS was similar between both groups, with 74.6% in the ACLR-alone group and 75.4% in the ACLR+LEAP group. A return to similar preinjury level was achieved in 64 (54.2%) for the ACLR+LEAP group compared with 48 (42.1%) for the ACLR-alone group (P = .3377).
Subgroup Analysis of Quadrupled Hamstring ACLR
The subgroup analysis focusing on quadrupled hamstring grafts mirrored the overall findings, maintaining a similar trend in patient characteristics and outcomes between the ACLR-alone and ACLR+LEAP groups. The ACLR+LEAP group exhibited a significant decrease in graft rupture rates, with 3.5% compared with 14.0% for the ACLR-alone group. This difference translates to a 10.5% ARR and an NNT of 9.5 to prevent 1 graft rupture (P = .01). Furthermore, individuals in the ACLR-alone cohort were found to have a >4-fold increased hazard of graft rupture relative to those in the ACLR+LEAP group (HR, 4.34; P = .017) (Appendix, available in the online version of this article).
Discussion
The main finding of this study was that ACLR+LEAP was associated with a lower risk of rerupture in the pediatric and adolescent populations.
Primary Outcome Measures
Our findings are in line with those of previous studies that investigated ACLR+LEAP in adults and have reported rerupture rates ranging from 0% to 5.3%.21,32,43 There are only a few studies, mostly from 2022, that have reported on the rate of rerupture in the pediatric population comparing ACLR procedures with and without LEAP (Table 5).
Summary of Studies Comparing ACLR Versus ACLR+LEAP in the Pediatric Population a
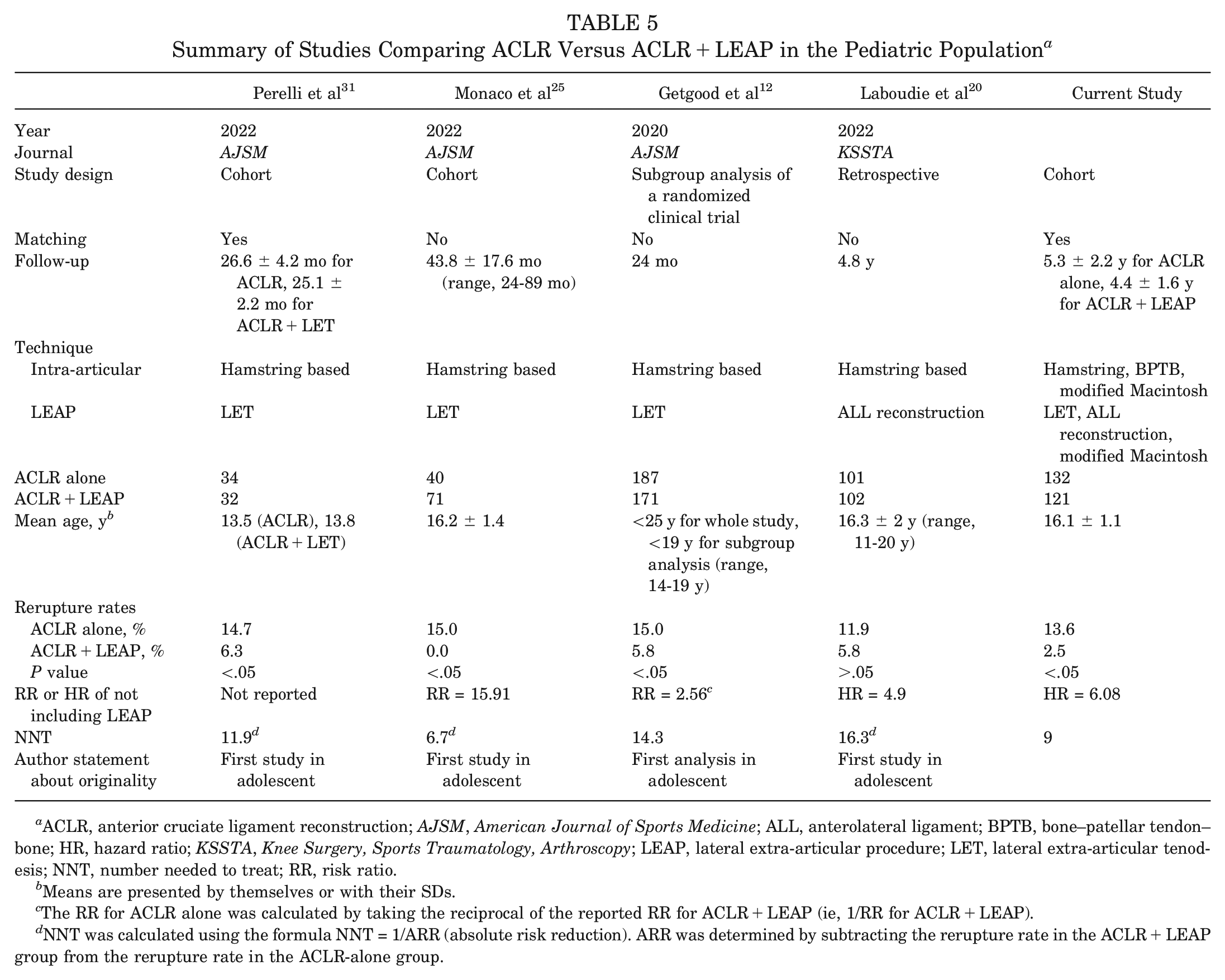
ACLR, anterior cruciate ligament reconstruction; AJSM, American Journal of Sports Medicine; ALL, anterolateral ligament; BPTB, bone–patellar tendon–bone; HR, hazard ratio; KSSTA, Knee Surgery, Sports Traumatology, Arthroscopy; LEAP, lateral extra-articular procedure; LET, lateral extra-articular tenodesis; NNT, number needed to treat; RR, risk ratio.
Means are presented by themselves or with their SDs.
The RR for ACLR alone was calculated by taking the reciprocal of the reported RR for ACLR+LEAP (ie, 1/RR for ACLR+LEAP).
NNT was calculated using the formula NNT = 1/ARR (absolute risk reduction). ARR was determined by subtracting the rerupture rate in the ACLR+LEAP group from the rerupture rate in the ACLR-alone group.
For instance, the matched cohort study of Perelli et al 31 included 34 patients who underwent isolated ACLR and 32 who had combined ACLR+LET. The age range for both groups was 12 to 16 years. They found a higher failure rate in the isolated ACLR group (14.7%) than in the combined ACLR+LET group (6.3%) (P = .021). Although their study provided valuable insights, it was constrained by its relatively small sample size. This limitation has been addressed in our relatively larger-scale cohort. In another nonmatched study, Monaco et al 25 (mean age, 16.2 ± 1.4 years) showed that all graft ruptures occurred in the isolated ACLR group (15.0%; 6/40) at 2 years of follow-up. They revealed that failure to add LET was associated with a 15.91-fold increased risk of graft rupture. This study was limited by the lack of a matching technique and its limited sample size. Laboudie et al 20 reported similar trends without reaching statistical significance in their nonmatched retrospective study. They also reported that the absence of ALL reconstruction was independently associated with an increased rate of reoperations (HR, 4.9; P = .01). Getgood et al 12 studied the hamstring-based ACLR+LET technique in patients <25 years of age. Their subgroup analysis for patients <19 years of age found that ACLR+LET (171 patients) had a 35% lower clinical failure rate (28.7% vs 44.4%; risk ratio, 0.65; 95% CI, 0.49-0.86) and a 61% lower graft rupture rate (5.8% vs 15.0%; risk ratio, 0.39; 95% CI, 0.20-0.78) compared with ACLR alone (187 patients). However, it is important to note that these findings were based on a subgroup analysis that may have been less robust because of the potential biases inherent in such analyses. Our matched analysis on patients <18 years old builds on these findings, by offering age-specific insights on the effect of LEAP addition to ACLR.
As previously stated, the risk of rerupture after ACLR is particularly high in the pediatric population and may reach up to 15% to 25.5%.6,11,41,42 In this sense, our findings are particularly important as they add to the growing evidence supporting the use of LEAP in the pediatric population. Furthermore, our results were derived from integrating multiple types of LEAPs, including ALL reconstruction, LET, and the modified Macintosh technique, as well as employing a range of intra-articular graft techniques, demonstrating that the advantage of LEAP is uniform and consistent across various techniques. In contrast, existing studies have primarily reported the use of hamstring-based grafts coupled with either LET or ALL reconstruction.12,20,25,31 Nevertheless, the calculated NNT to prevent 1 rerupture was found to be 9 in our study, offering a promising improvement compared with the NNT of 14.3 reported by Getgood et al. 12 Thus, we believe the LEAP procedure could potentially be a game-changer in reducing rerupture rates among young athletes.
Secondary Outcome Measures
Another relevant finding in our study is the divergence in the postoperative TAS scores between the 2 groups, for which the TAS was initially controlled. Specifically, the ACLR+LEAP group regained their preoperative activity level with a mean score of 7.2 (SD, 2.0), compared with 6.3 (SD, 2.3) for the ACLR-alone group. The literature presents contradictory findings on this issue. Monaco et al 25 found superior TAS scores in the ACLR+LET group, although their data also showed significantly higher preoperative scores in this group. In contrast, Laboudie et al 20 did not find any significant difference in the postoperative TAS scores between the groups. Similar controversies regarding this matter are found in studies involving adult populations.4,17,37
No significant differences were found in other patient-reported outcome measures between the groups, which aligns with the findings from other studies in the literature.4,17,20,25,31,37 Regarding non–graft rupture related reoperations, our study reported a total rate of 10.6%, with no significant difference between the 2 groups. A similar rate of 10.8% was reported by Monaco et al. 25
Although LEAP has not been shown to be associated with long-term osteoarthritis,7,10,44 these findings are yet to be confirmed and validated in the pediatric population. Furthermore, the risk of these procedures in patients with open physes has not been well explored.19,30
Limitations of this study include the lack of randomization, loss to follow-up, limited sample size, and its monocentricity. We tried to mitigate selection bias by using a matching technique; however, residual confounding due to unmeasured variables that were not included in propensity score matching might still introduce bias. Another limitation of this study is the use of the IKDC score instead of the Pediatric IKDC score. However, a study by Oak et al 27 that investigated the correlation between the IKDC and Pediatric IKDC scores found that the IKDC score can be used and is reliable for the pediatric population. One limitation of our study was the omission of the severity of preoperative rotational instability (pivot-shift grading) from our matching criteria. This could be significant given its potential association with graft rupture risks. However, this variable was not statistically different between groups.
The diverse range of ACLR techniques and LEAP techniques incorporated in our study presents both a potential weakness and a potential strength. On one hand, this variability could introduce confounding factors; on the other, it reinforces the notion that the benefits of LEAP are consistent across different techniques. Whether using anatomic or nonanatomic methods or tenodesis versus ALL reconstruction, the overall advantages of LEAP appear to be technique independent.
Conclusion
Our study supports the growing body of evidence advocating the use of LEAPs in conjunction with ACLR in the pediatric population, particularly to reduce the risk of graft rerupture with an NNT of 9 for ACLR+LEAP and an HR of 6.08 for ACLR. In addition, we observed that the ACLR+LEAP group returned to their preoperative TAS score more frequently than did the ACLR-alone group.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465231223703 – Supplemental material for Impact of Lateral Extra-Articular Procedure Augmentation on Rerupture Risk and Tegner Activity Scale Outcomes in Adolescent Anterior Cruciate Ligament: A Matched Comparative Study With a Minimum 2-Year Follow-up
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231223703 for Impact of Lateral Extra-Articular Procedure Augmentation on Rerupture Risk and Tegner Activity Scale Outcomes in Adolescent Anterior Cruciate Ligament: A Matched Comparative Study With a Minimum 2-Year Follow-up by Mohamad K. Moussa, Nicolas Lefèvre, Eugénie Valentin, Adam Coughlan, Aymen Zgolli, Antoine Gerometta, Alain Meyer and Alexandre Hardy in The American Journal of Sports Medicine
Footnotes
Submitted July 21, 2023; accepted November 15, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. has received consulting fees from Websurvey Society. A.H. has received consulting fees from Arthrex and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.