
Abstract
Background:
Meniscal allograft transplantation (MAT) is an accepted and effective treatment option in the context of unsalvageable menisci, particularly in young and active patients. It has been shown to reduce pain and improve knee function in previously symptomatic patients. However, there is still limited knowledge about the long-term survival rates of allografts, the durability of clinical results, and the influence of patient-specific parameters, such as leg alignment, tibial slope, and preoperative International Cartilage Regeneration & Joint Preservation Society (ICRS) grade.
Purpose:
To determine (1) the long-term clinical success rate after MAT with bony fixation in a large, single-center cohort of consecutive patients, and (2) if patient-specific and procedural variables influence the clinical, anatomic, and subjective outcomes and risk of failure.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Data on 185 consecutive knees undergoing MAT in a single institution were prospectively collected and screened for inclusion in this study. The minimum follow-up time was 2 years. Radiographic variables (ICRS grade and Kellgren-Lawrence grade) were assessed preoperatively and at follow-up. Subjective patient-reported outcome measures (PROMs) (Lysholm score, Knee injury and Osteoarthritis Outcome Score [KOOS] including subscores, International Knee Documentation Committee [IKDC] score, and visual analog scale [VAS] score) were collected preoperatively and at follow-up. Clinical failure was defined as revision surgery due to graft failure or conversion to total knee arthroplasty. Anatomic failure was considered a tear covering >20% of the allograft, any peripheral tear, and unstable peripheral fixation leading to dislocation of the graft. Subjective failure was defined as Lysholm score ≤65. Preoperative tibial slope and leg alignment were assessed. Survival analyses were performed using the Kaplan-Meier estimate. Univariate and multivariate analyses were performed to determine risk factors for clinical and anatomic failure.
Results:
A total of 157 knees met inclusion criteria. After a mean follow-up time of 7 ± 3.5 years, 127 (80.9%) knees were free of clinical, anatomic, and subjective failure. Fourteen (8.9%) knees experienced clinical failure, 26 (16.6%) knees were identified as having experienced anatomic failure, and 13 (8.3%) patients experienced subjective failure with a reported Lysholm score of ≤65 at a mean follow-up of 7 years. Concurrent osteochondral allograft transplantation was identified as a predictor of both clinical (hazard ratio [HR], 4.55; 95% CI, 1.46-14.17; P = .009) and anatomic (HR, 3.05; 95% CI, 1.34-6.92; P = .008) failure. Cartilage damage of ICRS grade 3 or 4 of the index compartment conveyed an increased risk for clinical (HR, 3.41; 95% CI, 1.05-11.01; P = .04) and anatomic (HR, 3.04; 95% CI, 1.31-7.11; P = .01) failure. High-grade cartilage damage preoperatively (HR, 10.67; 95% CI, 1.037-109.768; P = .046), patient age >25 years (HR, 5.44; 95% CI, 0.120-246.070; P = .384), and a body mass index >30 (HR, 2.24; 95% CI, 0.748-6.705; P = .149) were associated with subjective failure. PROMs including KOOS and IKDC were significantly improved at final follow-up compared with preoperative scores across all measurements (P < .005).
Conclusion:
MAT showed good to excellent clinical results at a mean follow-up of 7 years. Low ICRS lesion grade was associated with a higher clinical and anatomic survival rate. Patients with concurrent OCA transplantation are at a higher risk of clinical and anatomic failure, but still report significantly improved PROMs. These results suggest that MAT has a lasting beneficial effect both in isolation and in complex cases with ≥1 concurrent procedures.
Keywords
The menisci are recognized as important anatomic structures in the knee, influencing biomechanical joint stability, load distribution, shock absorption, decrease of contact stress, proprioception, and joint lubrication.5,19,40,41 Because of this vital role in maintaining joint homeostasis, meniscal preservation techniques are the surgeon's first choice in the face of meniscal pathology. In an intact knee, the medial and lateral menisci bear approximately 50% and 70% of the load, respectively. 30 Meniscal tears are frequent and were observed in 4% of individuals <40 years of age and 19% of individuals >40 years of age with asymptomatic, uninjured knees. 14 Among patients reporting knee pain, the incidence of a structurally deficient meniscus has been reported to exceed 70%. 17 While reparative approaches are usually the first line of treatment, tissue-preserving surgery is not always feasible. Consequently, primary or secondary (partial) meniscectomy remains the most frequently performed arthroscopic surgery of the knee joint for symptomatic, irreparable meniscal tears, with 760,000 outpatient procedures performed annually in the United States. 29 A deficient meniscus will alter the biomechanical and biological condition of the knee joint, resulting in increased contact pressure of the knee and initiating a cascade of often painful joint degeneration.9,62 Meniscal allograft transplantation (MAT) is an established treatment for postmeniscectomy syndrome, which is characterized by a symptomatic pain developing after meniscectomy. 15 Substitution of the resected meniscus by an allograft can restore meniscal function and prevent rapid degeneration of the joint by decreasing contact pressure of the articular cartilage surface and alleviating pain. 18
MAT has been used in clinical practice since the late 1980s and is currently a widely accepted treatment option, especially for young and active patients experiencing postmeniscectomy syndrome.16,53 While full restoration of joint biomechanics and contact pressure by an allograft has not yet been obtained, significant improvements were found in biomechanical studies in an in vitro setting.3,31,69 Despite structural limitations, a meta-analysis of 3157 MAT procedures found significantly improved clinical outcomes at medium- and long-term follow-up. 16 Graft survival rates ranging from 60% to 86% after 10 and 15 years have been reported, indicating lasting ingrowth of the graft and stable treatment results.27,51,54,72 However, current evidence of long-term allograft survivorship and function is limited due to small study sizes rarely exceeding 100 patients,25,48,75 unstandardized definitions of clinical and anatomic failure, and heterogeneous study cohorts.75,77 Furthermore, relevant information such as preoperative Kellgren-Lawrence or Tönnis grade, preoperative International Cartilage Regeneration & Joint Preservation Society (ICRS) grade, tibial slope, and leg alignment are often underreported, impeding interpretation of presented data.11,26,37
Previous studies have identified generalized degenerative arthritis as a prognostic factor for poor allograft function and survival, leading to exclusion of these patients in a variety of studies.26,48,55,63,73,79 However, recent evidence suggests that even in knees with severe focal chondral damage, MAT can be an effective treatment, leading to improved clinical scores and decreased pain, especially when combined with cartilage procedures.1,4,22,45,68 However, the potential chondroprotective capability of MAT, and therefore its role as a preventive procedure in the asymptomatic knee, remains controversial.46,64,70,74,77,78 Currently, it is unclear if extended cartilage damage imposes a contraindication for MAT; therefore, patients with high-grade articular damage were not excluded from this study.
The purpose of the present study was to report the clinical results, graft survivorship, and failure rate of a large cohort of MAT procedures performed with bone fixation in a single center over an extended period. The secondary aim was to identify potential radiographic, surgical, and patient-specific risk factors for MAT failure and secondary surgeries, and thereby identify predictors for successful clinical use. We hypothesized that an increased preoperative ICRS grade of the index compartment, an elevated preoperative Kellgren-Lawrence grade, the complexity of cases (previous procedures and concurrent surgery), body mass index (BMI), and patient age could affect graft survival rate, radiographic results, and patient-reported outcome measures (PROMs).
Methods
Study Population and Design
This was a retrospective review of prospectively collected data on all MAT procedures that were performed at a single institution (Mayo Clinic) from 2005 to 2020. Institutional review board approval was obtained before the beginning of the study (IRB No. 15-000601), and all patients provided informed consent. A search of the institutional medical records database was performed to identify all patients who were treated with a MAT procedure. Patients were included if they underwent either medial or lateral MAT surgery and reached a minimum follow-up time of 2 years. Age, elevated preoperative osteoarthritis grade, and concurrent procedures were not limitations for inclusion. Exclusion criteria consisted of (1) soft tissue fixation of the allograft and (2) <2 years of follow-up. Accordingly, 157 of 185 patients were enrolled in this study. Twenty-eight patients were excluded due to loss to follow-up (Figure 1).
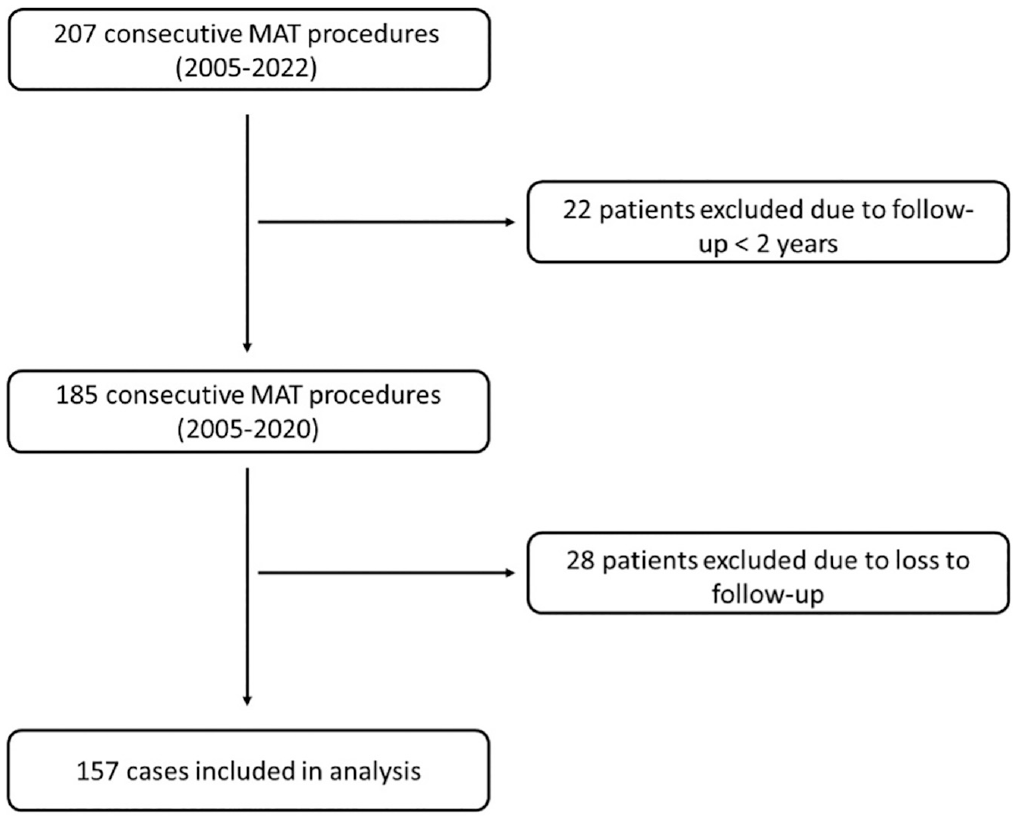
Flowchart displaying patient selection for this study. MAT, meniscal allograft transplantation.
Eligibility criteria for MAT surgery were unicompartmental knee pain and/or discomfort after meniscectomy thought to be caused by loss of meniscal tissue. In cases with axial varus malalignment ≥5° and/or instability of the knee joint, a corrective osteotomy or stabilization procedure was performed at the time of transplantation. Cartilage lesions were addressed concomitantly or before the MAT procedure. In case of concomitant anterior cruciate ligament (ACL) revision surgery, bone grafting was routinely performed before the MAT procedure.
Surgical Technique and Rehabilitation
All MAT procedures were performed at a single institution using fresh-frozen size-matched allografts that were provided by commercial vendors. Size matching was carried out according to the methods introduced by Pollard et al 60 and Van Thiel et al. 76
All patients underwent MAT with bony fixation of the graft. All medial allografts were carried out with the bone plug technique. 80 Lateral allografts were fixated with either the bone plug technique or the dovetail technique. 35 The surgical techniques used in this study for MAT have been described in detail previously by the senior author (A.J.K.).57,80 The sequence of the procedure for patients receiving osteochondral allograft (OCA) alongside MAT involved completing the meniscal transplantation phase first, followed by the OCA phase using a mini-arthrotomy. It is important to note that for patients undergoing MAT simultaneously, the meniscal repair sutures were not tied until after the OCA had been positioned, and these sutures were tied with the knee fully extended. In cases where concomitant high tibial osteotomy was performed, the osteotomy phase was conducted as the final step, after the completion of OCA (and after MAT if applicable).
The postoperative rehabilitation protocol started with a restricted range of motion (ROM) of 90° and partial weightbearing in full extension using crutches for 4 weeks. Isometric exercises, cryotherapy, and closed-kinetic chain strengthening were performed. At 4 weeks after operation (OP), weightbearing as tolerated was allowed, full ROM and aerobic exercise were introduced, and the knee immobilizer was discontinued. At week 16, patients were allowed to return to activity as tolerated and a jogging program was initiated. Basic plyometric exercises were introduced with caution to avoid loaded high knee flexion. Attention was shifted to strength, endurance, and proprioception training. Noncontact sports were allowed after 6 months, with a return to high-demand sports after 8 months. There were no substantial differences in rehabilitation protocol between patients treated with a solitary MAT and patients undergoing MAT and concurrent ACL revision or OCA transplantation. Patients undergoing concomitant alignment-correcting osteotomy performed touch weightbearing for 5 weeks in full extension and progressed to full weightbearing within 3 weeks thereafter.
Patient Evaluation
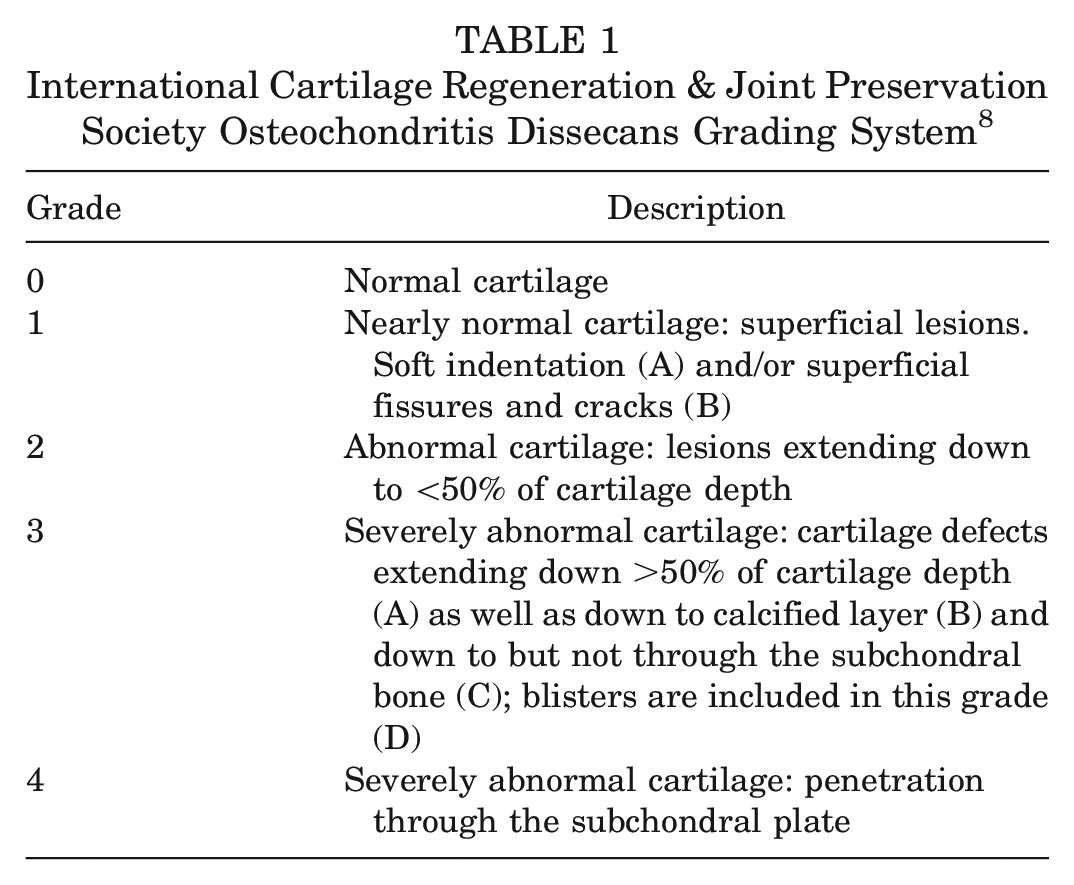
Patient-specific details were manually extracted from medical charts, including radiographic studies, postoperative procedures, and clinical evaluations. Concomitant pathologies were assessed using a combination of clinical, radiographic, and magnetic resonance imaging (MRI) findings; confirmed intraoperatively; and documented in surgical reports. The extent of cartilage lesions was graded preoperatively using the ICRS classification based on MRI (Table 1). 8 Routine preoperative radiographic examination included standing anteroposterior, 45° flexion weightbearing posteroanterior, lateral, Merchant, and standing long-leg anteroposterior views. Kellgren-Lawrence grade was assessed using radiographs taken pre- and postoperatively. Tibial slope was measured on lateral knee radiographs, and mechanical leg axis was measured on preoperative standing long-leg films. All radiographic measurements were carried out by a fellowship-trained orthopaedic surgeon (M.H.). In case of concomitant alignment correction, immediate postoperative radiographs were used for determination of tibial slope and leg axis. The allograft was assessed using postoperative MRI and/or follow-up arthroscopy. Second-look procedures were solely preformed for clinical indications such as persistent pain and limited ROM. PROMs were recorded preoperatively and at the final follow-up. Patients were contacted by telephone and email by 3 authors (M.H., K.P., A.W.). Patients were considered lost to follow-up when no adequate contact information was available or if no response could be acquired after 3 attempts of contact via telephone, followed by 3 emails sent out over 3 weeks. Pre- and postoperative International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, a 0- to 10-point visual analog scale (VAS) for pain, and Knee injury and Osteoarthritis Outcome Score (KOOS) including subscores were recorded. 81 The Lysholm score was recorded at the final follow-up. 13 All procedures performed during the follow-up period were documented.
International Cartilage Regeneration & Joint Preservation Society Osteochondritis Dissecans Grading System 8
Definition of Failure
Anatomic failure was defined as a tear involving >20% of the allograft, any peripheral tear, and unstable peripheral fixation leading to dislocation of the graft confirmed by MRI or second-look arthroscopy. MRI grading was based on the criteria of Stoller 71 and was evaluated by a fellowship-trained orthopaedic surgeon (M.H.) who did not perform the surgeries. Clinical failure was considered as revision surgery due to graft failure (including meniscectomy of >50% of graft and revision MAT), axis-correcting osteotomies due to clinical symptoms, conversion to total knee arthroplasty, and unicondylar knee arthroplasty. Subjective failure was defined as Lysholm score ≤65 at the final follow-up. This threshold was chosen as it has been established as the threshold postoperative score that best reflects satisfied patients by previous studies.26,49
Statistical Analysis
Descriptive statistics including mean, standard deviation, and range were used to characterize results with continuous values, while percentages were used for proportions. Patient and surgery details were compared between groups using Wilcoxon rank-sum tests for continuous variables (age, BMI, lesion size, and number of implants) and Fisher exact tests for categorical variables (sex, laterality, surgery type, condyle location, lesion stability, and implant material). Kaplan-Meier survival curves were constructed for the entire study population and subgroups to compare failure rates. Survival proportions at 2, 5, 7, and 10 years and a mean survival time were calculated. A univariate Cox proportional hazards model was used to analyze the risk of failure based on patient-specific and radiographic parameters. Within each group, other risk factors for failure were assessed using odds ratios and Fisher exact tests for dichotomous variables along with nominal logistic fit models for continuous or ordinal variables. Significant variables were used to construct a multivariate Cox proportional hazards model for the effect of these variables on failure rate. The PROMs were compared using Wilcoxon rank-sum tests; analyses were performed between pre- and postoperative scores for each measure within each group, and for the baseline and final scores between groups.
Results
A total of 157 patients (93 men and 64 women), with a mean follow-up of 7 ± 3.5 years, were included (Table 2). The cohort's mean age at index surgery was 24.9 ± 8.6 years. Patients had a mean of 1.7 ± 1.1 previous surgeries before MAT and a mean period of 2.7 ± 3.1 years from the first meniscal surgery to MAT. Among them, 82 (52%) patients had medial MAT, while 75 (48%) patients underwent lateral MAT. At index surgery, 10.8% had normal cartilage (ICRS grade 0), while varying degrees of cartilage damage were observed in the remaining cases. Isolated MAT was performed on 29% of patients, while 71% underwent concurrent procedures, most commonly ACL reconstruction (39%), OCA (20%), and contralateral meniscal repair (14%) (Table 3).
Descriptive and Clinical Patient Characteristics of 157 Patients a
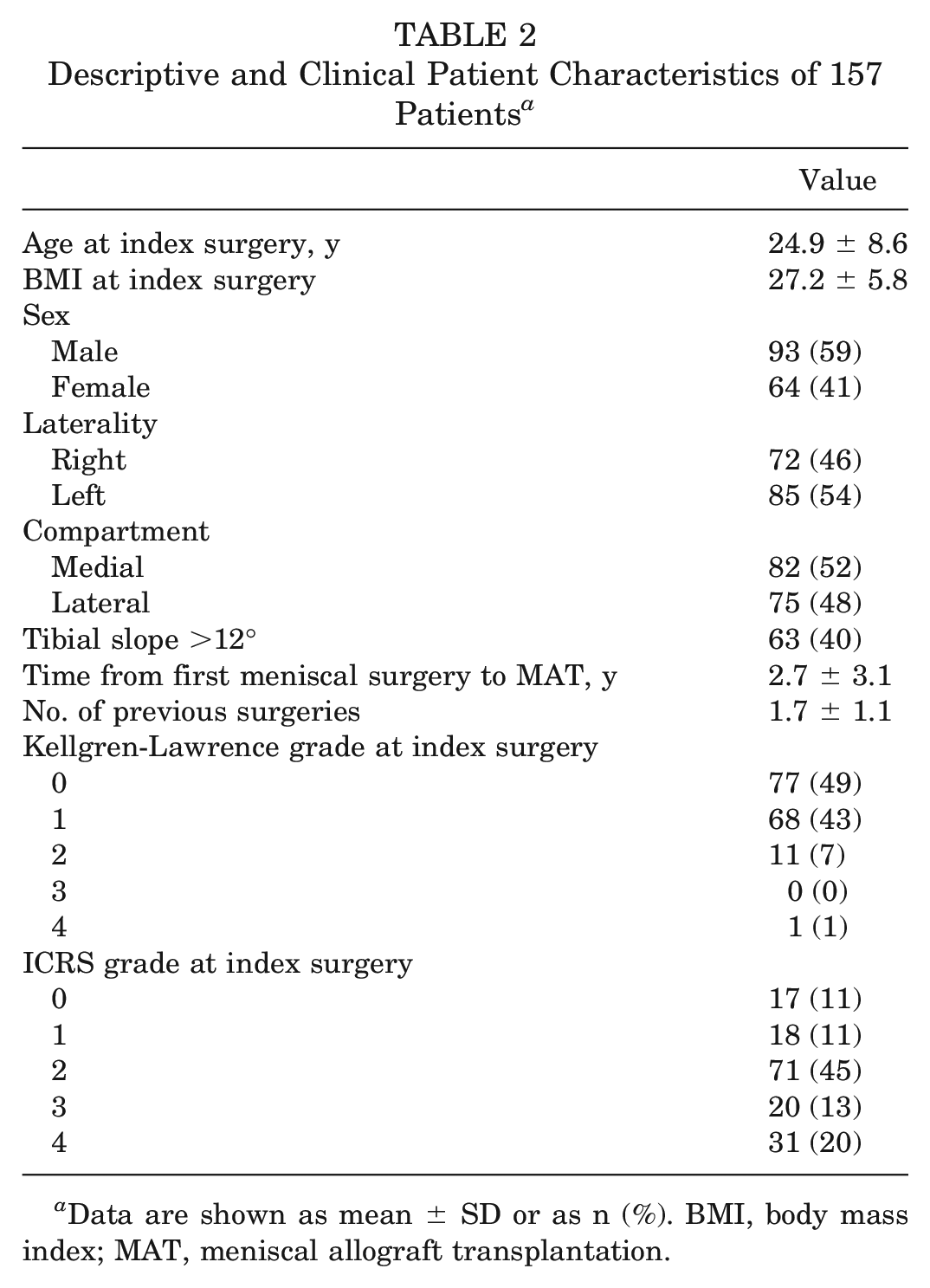
Data are shown as mean ± SD or as n (%). BMI, body mass index; MAT, meniscal allograft transplantation.
Concurrent Procedure Performed at the Time of Meniscal Allograft Transplantation in the Same Knee a
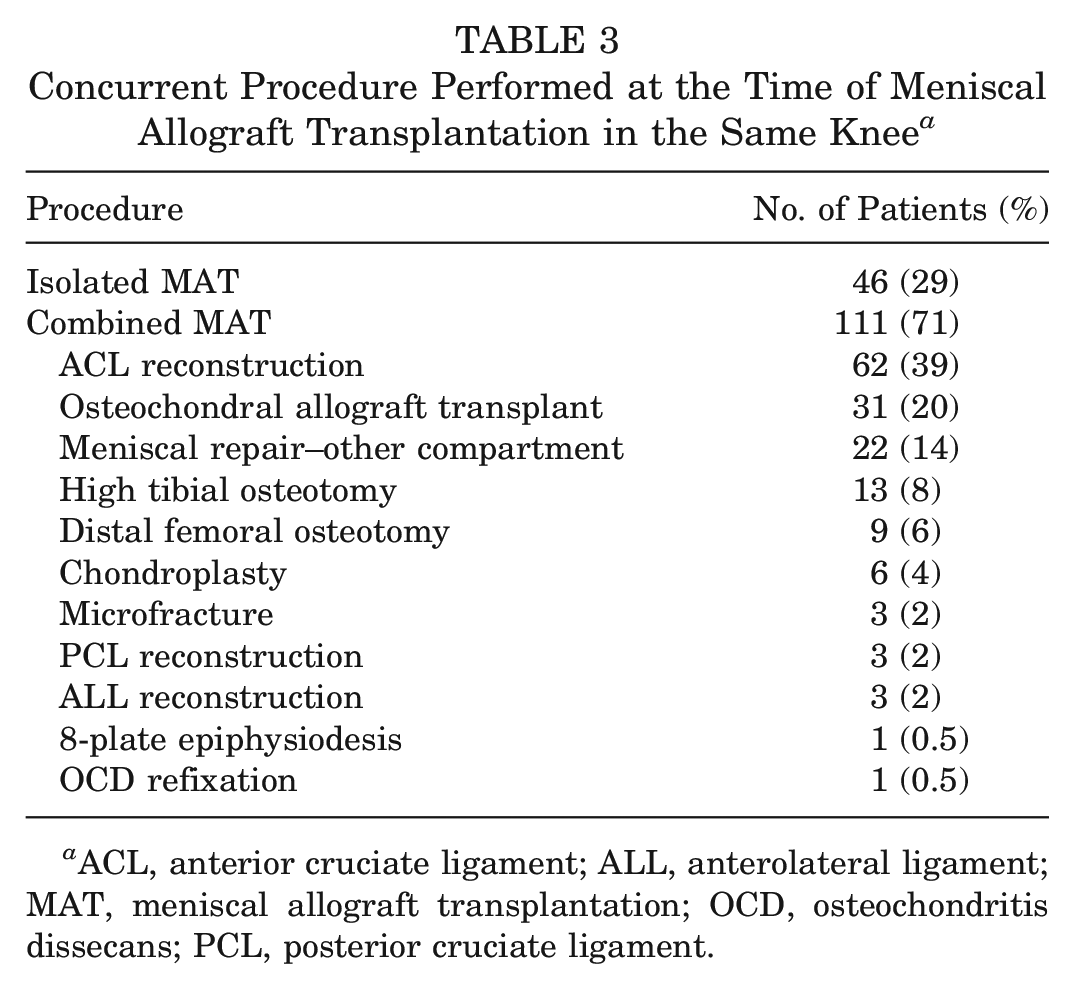
ACL, anterior cruciate ligament; ALL, anterolateral ligament; MAT, meniscal allograft transplantation; OCD, osteochondritis dissecans; PCL, posterior cruciate ligament.
Patients underwent 1.7 ± 1.1 surgeries of the same knee before the index surgery, and 2.7 ± 3.1 years passed from the first meniscal procedure until MAT. A total of 45 surgeries were performed after MAT, with diagnostic arthroscopy (n = 25) being the most frequent procedure (Table 4).
Surgeries Before and After MAT a
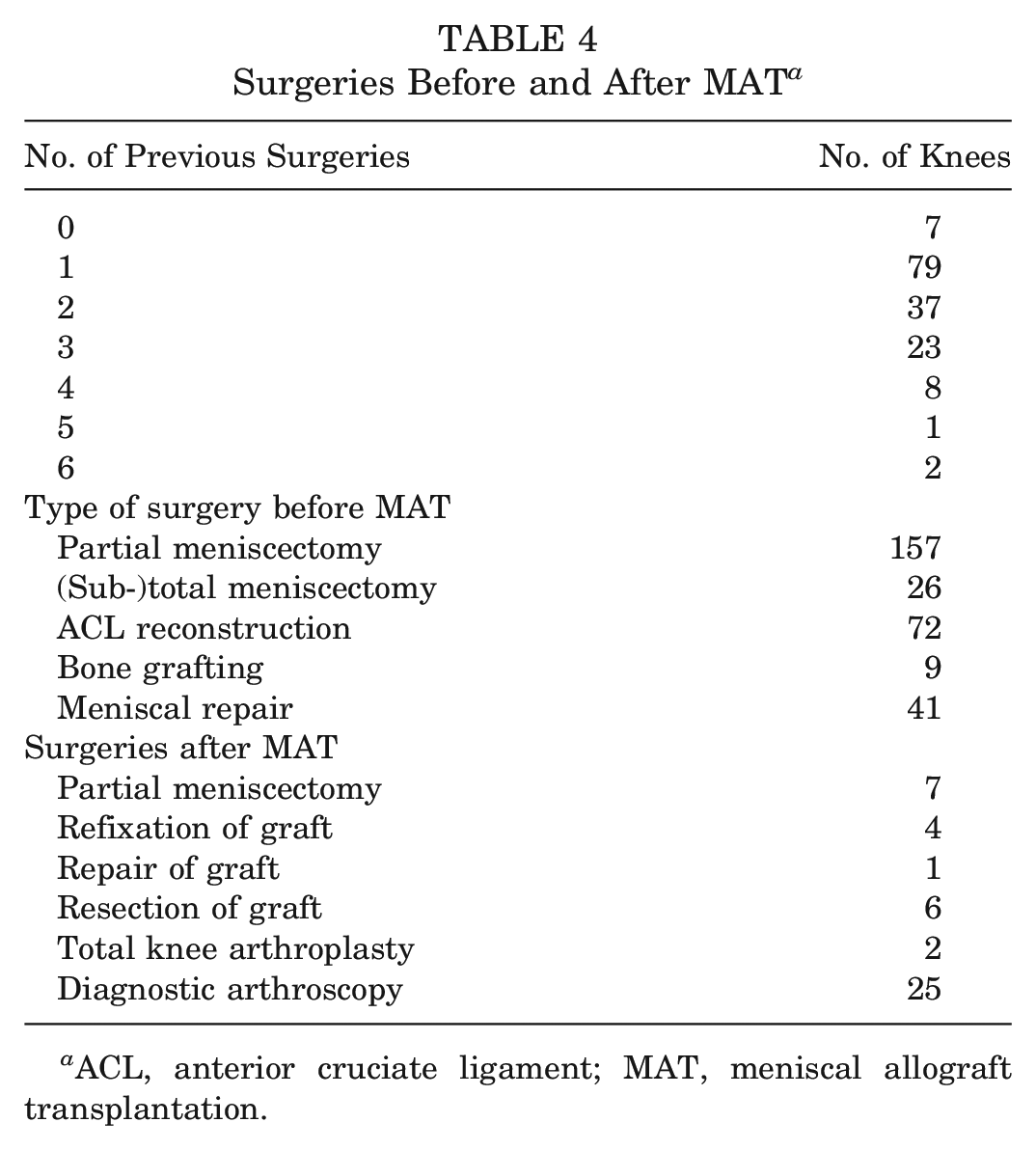
ACL, anterior cruciate ligament; MAT, meniscal allograft transplantation.
Clinical Failure
Clinical failure occurred in 14 (8.9%) knees after a mean follow-up of 71.2 ± 44.2 months (range, 24-198 months). Eight (57.1%) medial MAT and (42.9%) 6 lateral MAT failed. Failures were addressed with a meniscectomy of >50% of the graft in 5 cases, a resection of the graft in 6 cases, a conversion to total knee arthroplasty in 2 cases (at patient ages of 28 and 33 years), and an unsuccessful graft refixation in 1 case. Of the failures, 4 grafts were fixed with the dovetail technique and 10 grafts had a bone plug fixation. The 5- and 10-year clinical survival rates of MAT in our series were 96.8% and 93%, respectively.
The mean survival rates of medial and lateral MATs did not differ (Figure 2). The survival probability of patients treated with concurrent OCA was lower than that of patients without a concurrent OCA (P = .01) (Figure 3). In a univariate Cox regression analysis, concurrent OCA conveyed a hazard ratio (HR) for clinical MAT failure of 4.6 (95% CI, 1.5-14.2; P = .009) (Table 5). Low or no preoperative cartilage damage of the index compartment (grade 0 and 1) was associated with a higher survival probability than higher-grade cartilage damage (grades 2-4) according to the ICRS classification (P = .033) (Figure 4). An elevated Kellgren-Lawrence score before MAT increased the risk of clinical failure (HR, 2.01; 95% CI, 1.002-4.038; P = .049) (Figure 5). BMI, age at index surgery, fixation technique, and tibial slope were not significant risk factors for clinical failure (Table 5).
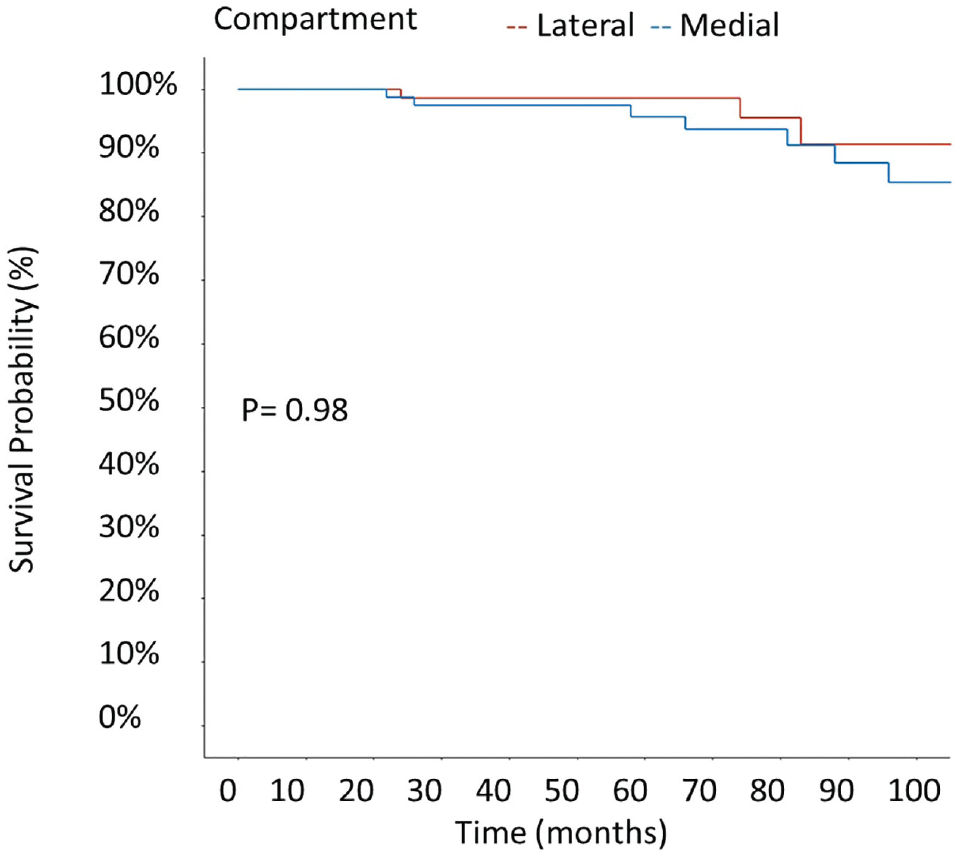
Kaplan-Meier estimates of clinical failure according to compartment (lateral/medial).
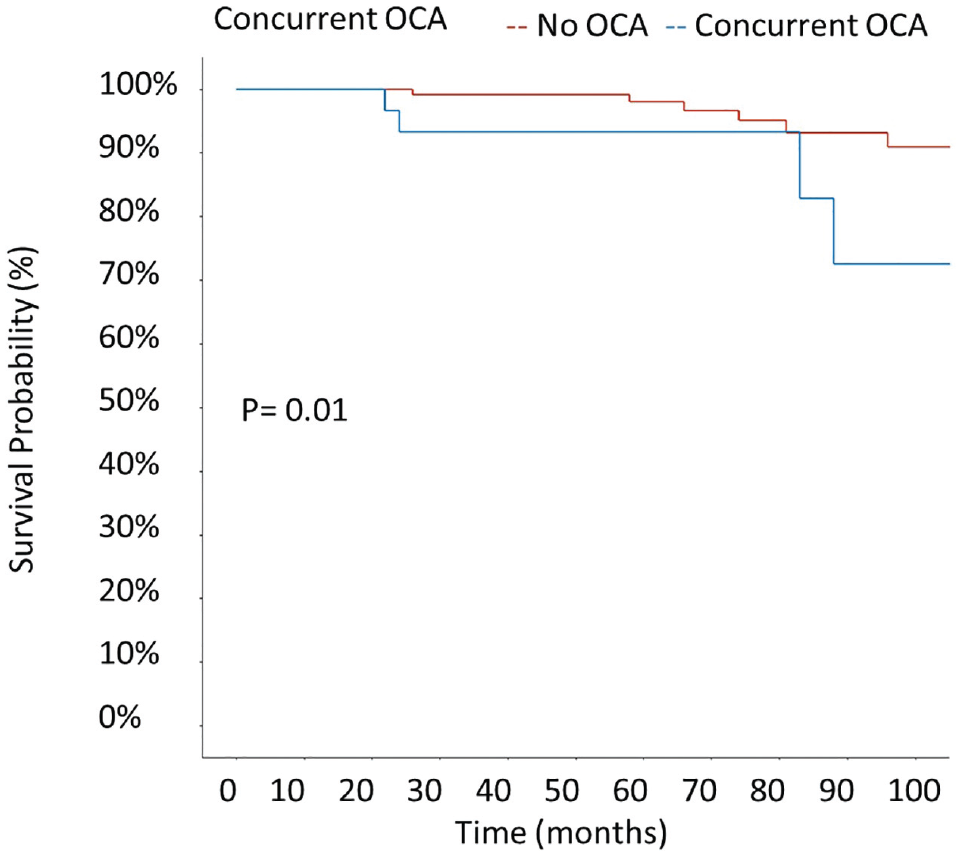
Kaplan-Meier survival curve for clinical failure according to concurrent osteochondral allograft (OCA) transplantation.
Univariate Analysis of the Hazards for Anatomic and Clinical Failure Based on Patient-Specific Variables a
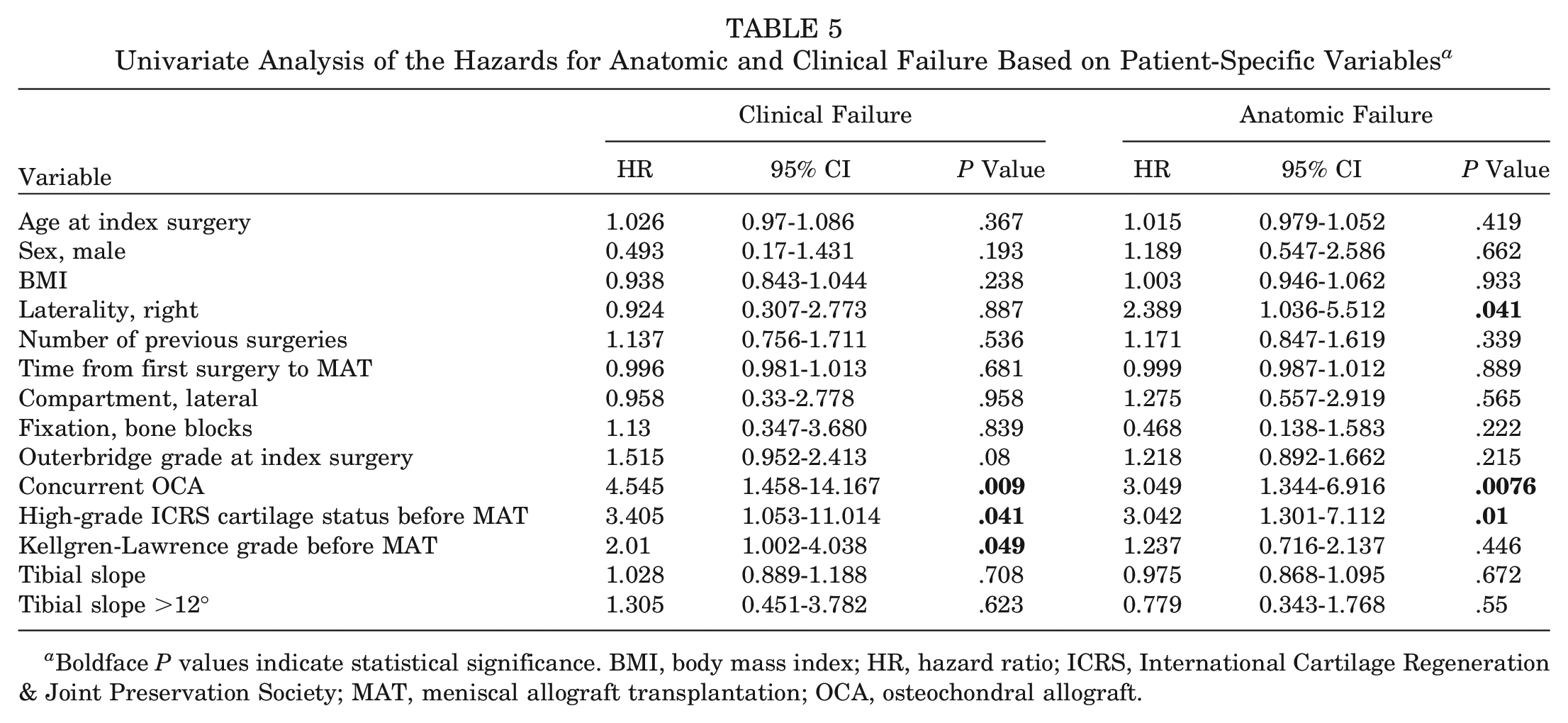
Boldface P values indicate statistical significance. BMI, body mass index; HR, hazard ratio; ICRS, International Cartilage Regeneration & Joint Preservation Society; MAT, meniscal allograft transplantation; OCA, osteochondral allograft.
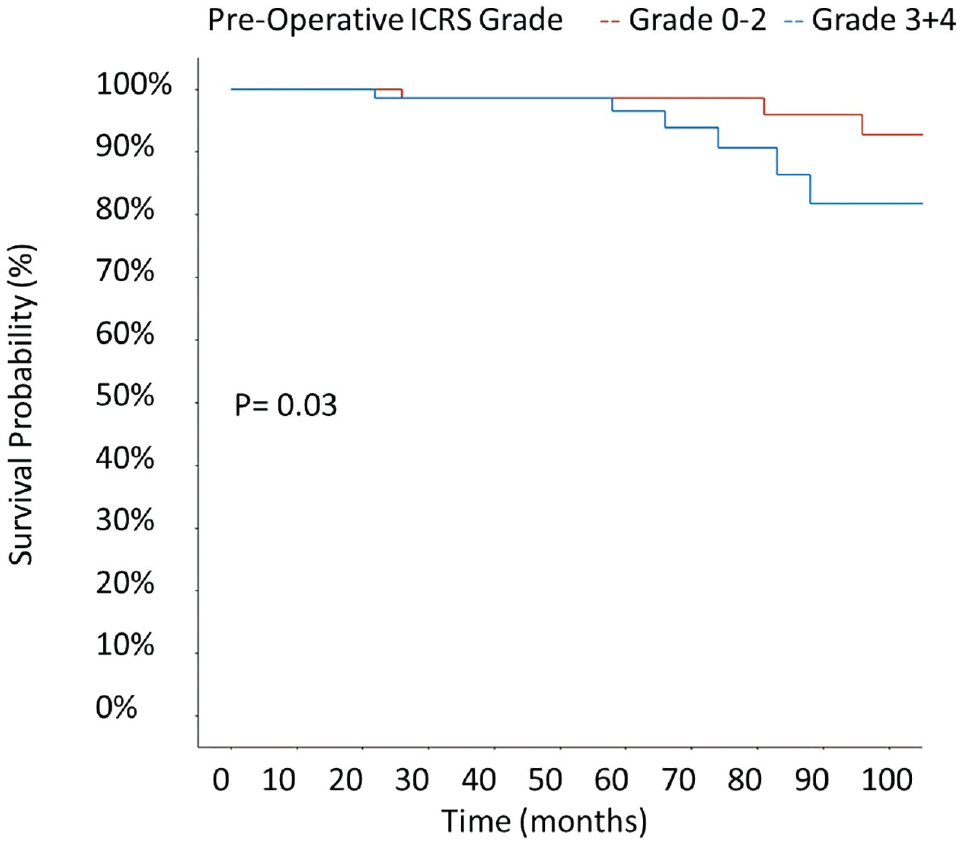
Kaplan-Meier survival curve for clinical failure according to preoperative International Cartilage Regeneration & Joint Preservation Society (ICRS) grade of the index compartment.
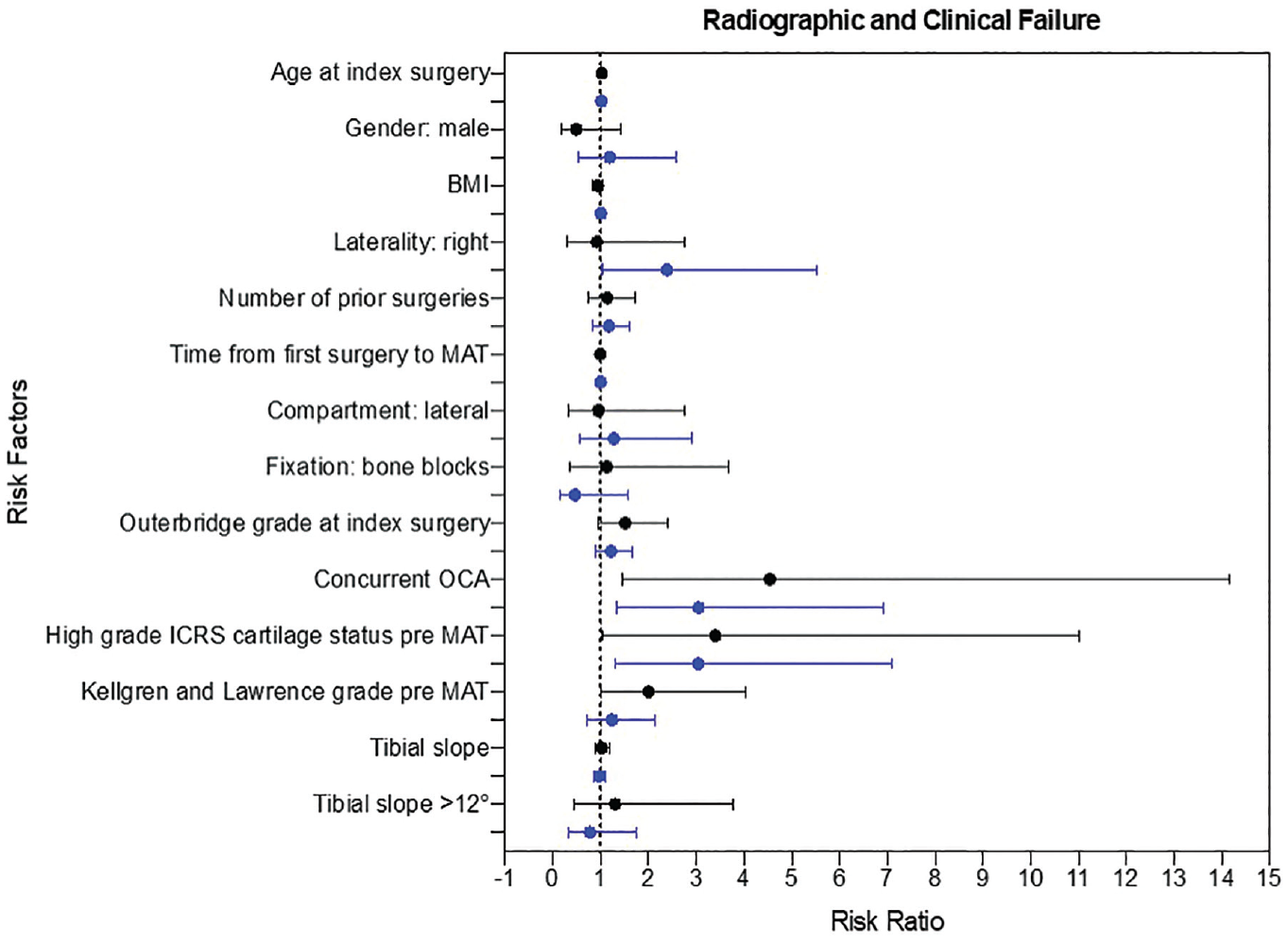
Forest plot of risk factors for failure and conferred risk ratio. Blue lines, anatomic failure; black lines, clinical failure. BMI, body mass index; ICRS, International Cartilage Regeneration & Joint Preservation Society; MAT, meniscal allograft transplantation; OCA, osteochondral allograft.
Anatomic Failure
In all, 26 (16.6%) patients experienced anatomic failure. Of these, 10 patients were also graded as experiencing clinical failure, and 6 patients had a Lysholm score <65. Of the 26 patients who were classified having experienced anatomic failure, 13 underwent a reoperation. Four patients were treated with a partial meniscectomy, 1 graft was refixed, 4 grafts were resected, 1 patient was converted to total knee arthroplasty, and 3 knees were subject to a revision MAT. The survival rate as defined by anatomic failure was 91.7% at 2 years, 88.5% at 5 years, 86.9% at 7 years, and 85.1% at 10 years (Figure 6). Concurrent OCA procedure (HR, 3.049; 95% CI, 1.344-6.916; P = .0076) and higher-grade ICRS (grades 3 and 4) cartilage status pre-MAT (HR, 3.042; 95% CI, 1.301-7.112; P = .01) conveyed an elevated risk for anatomic failure (Table 5). The multivariate Cox proportional hazards model, adjusting for cofounders, reported a significant effect of high-grade cartilage damage preoperatively on anatomic failure rate (HR, 3.211; 95% CI, 1.213-8.472; P = .001) (Table 6).
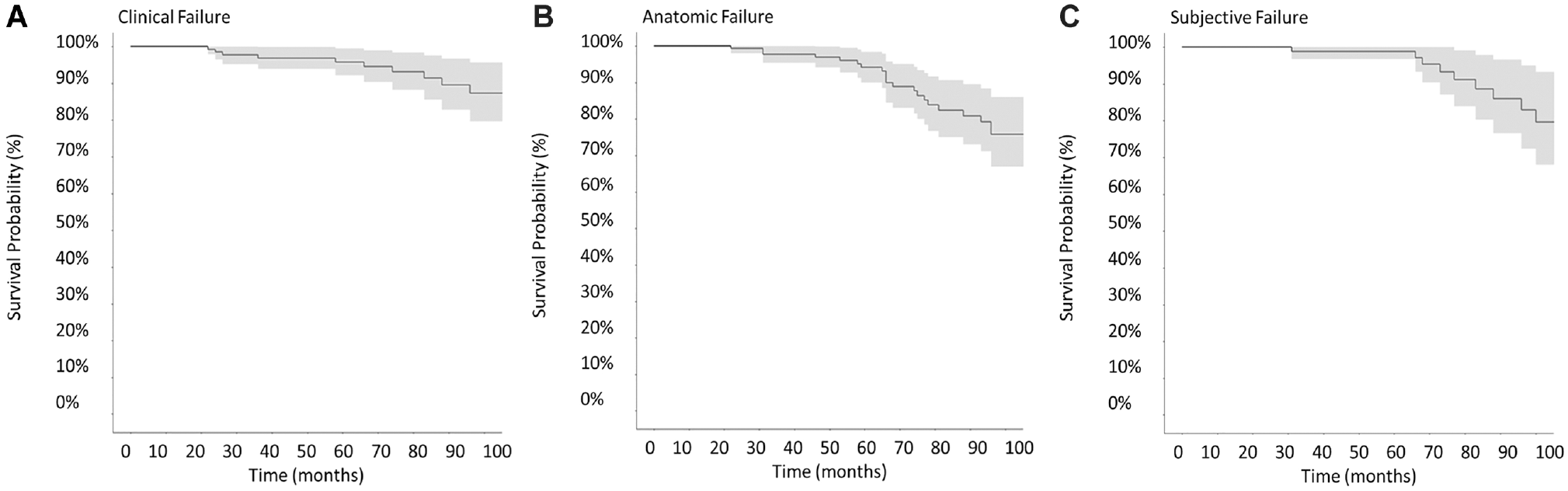
Kaplan-Meier estimate of survival according to different endpoints. (A) Survival time to clinical failure. (B) Survival time to anatomic failure. (C) Survival time to subjective failure.
Cox Proportional Hazards Model Analysis According to ICRS Grade a
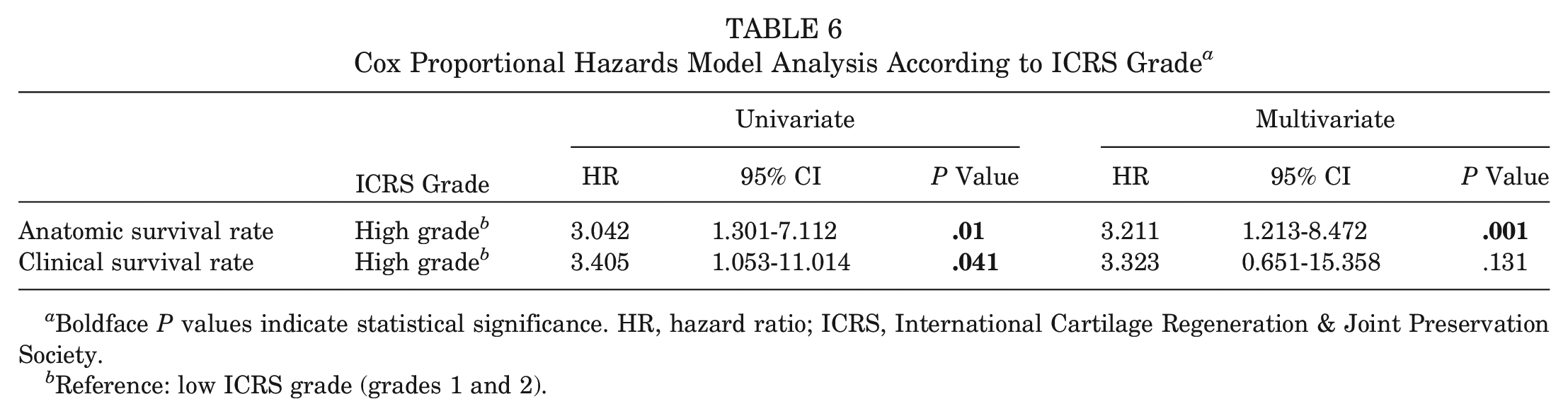
Boldface P values indicate statistical significance. HR, hazard ratio; ICRS, International Cartilage Regeneration & Joint Preservation Society.
Reference: low ICRS grade (grades 1 and 2).
The anatomic survival rate was significantly higher in the group with a low cartilage grade than in the cohort with high ICRS grades (P = .003, log-rank test) (Figure 7).
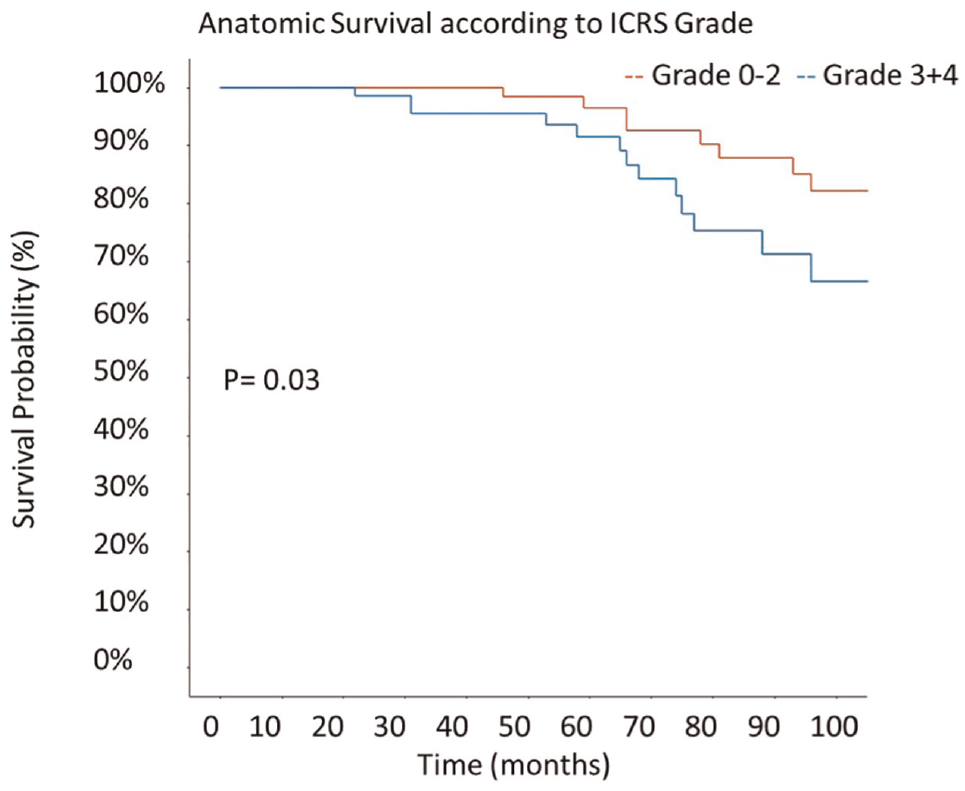
Anatomic survival according to preoperative cartilage status. ICRS, International Cartilage Regeneration & Joint Preservation Society.
PROMs and Subjective Failure
Outcomes were assessed using the IKDC score, KOOS, and Lysholm score (Figure 8). Overall, PROMs improved compared with the preoperative state. The mean differences between scores at the final follow-up were significantly increased when compared with preoperative scores (P < .05). Overall, the mean final IKDC score was 79.6 ± 17.3, and the mean final KOOS values were 89.1 ± 13.2 for pain, 77.2 ± 21.8 for symptoms, 93.4 ± 11.1 for activities of daily living, 72.7 ± 25.3 for sports, and 67 ± 23.2 for quality of life. The VAS score was 1.7 ± 1.8 at the final follow-up.
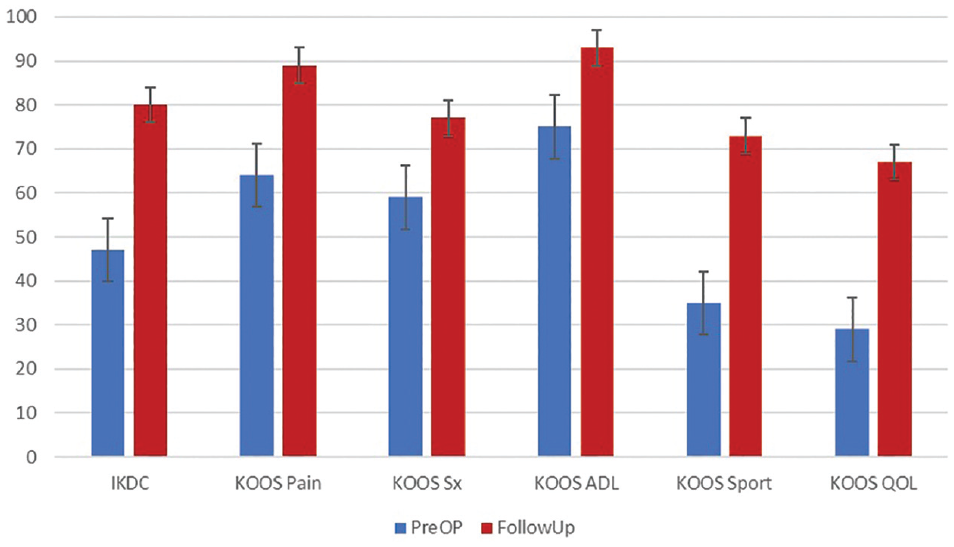
Comparison of International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form and Knee injury and Osteoarthritis Outcome Score (KOOS) results. Error bars indicate standard error. ADL, activities of daily living; QOL, knee-related quality of life; Sports, function in sports and recreation; Sx, symptoms.
Thirteen (8.3%) patients reported a Lysholm score of ≤65 and were considered to have experienced subjective failure of the MAT procedure at the final follow-up. Of these patients, 3 were found to have also experienced clinical failure and 7 experienced anatomic failure. The mean Lysholm score of the subjective failure cohort was 41.5 ± 13.1, while the score of the overall study population was 78.3 ± 20.6. With univariate analysis, high-grade cartilage damage preoperatively (HR, 10.67; 95% CI, 1.037-109.768; P = .046) and patient age >25 years (HR, 5.436; 95% CI, 0.120-246.070; P = .384) were associated with subjective failure. A BMI >30 conveyed a hazard ratio of 2.24 (95% CI, 0.748-6.705; P = .149) for subjective failure.
Discussion
This study reported on a mean 7-year follow-up for 157 patients who underwent MAT with bony fixation. The principal finding of this investigation was that good survival rates, increased patient satisfaction, and clinical scores can be expected after a follow-up of up to 16 years. It was found that better cartilage status was associated with higher clinical and anatomic survival rates, while concurrent OCA transplantation was associated with significantly worse clinical, anatomic, and subjective outcomes.
Survivorship in the current study was high at 91.1%. A systematic review conducted by Novaretti et al 54 in 2019, which included 688 MAT cases from 11 studies, reported an overall survival rate of 73.5% at 10 years after transplantation. This indicates that a significant proportion of patients maintain a functioning transplanted meniscus over the long term.
Furthermore, a study by Elattar et al in 2011 18 examined the survivorship of MAT in a large cohort of 1068 patients. The authors reported, whatever the follow-up period and the scoring system used, patients continuously showed clinical improvement.
It is worth noting that survivorship rates can vary depending on various factors such as patient age, activity level, concomitant knee pathologies, and surgical techniques. A study by Noyes et al in 2004 55 evaluated the survivorship of MAT in young and active patients and found a survival rate of 63% at 10 years, emphasizing the importance of patient selection in achieving favorable outcomes.
While survivorship rates indicate the longevity of the transplanted meniscus, it is important to consider that individual patient outcomes can vary. Factors such as graft extrusion, graft degeneration, and subsequent knee osteoarthritis can influence the functional outcomes and survivorship of MAT.
The presented study population was exclusively treated with MAT with bone fixation (Figure 9 and 10). Multiple biomechanical studies and meta-analyses have shown that soft tissue fixation of the graft is associated with higher contact pressure of the articular cartilage, elevated failure rate, and more frequent reoperations of the graft.2,12,52,56,58 It was found that the risks of failure and reoperation were the lowest in patients receiving transplanted allografts secured using bone plugs. 56 However, consensus is lacking regarding the recommended method of MAT fixation, and the selection of fixation technique stems from individual surgeon preference, leading to limited comparability between studies. Interestingly, a recent large (324 procedures) case series by Grassi et al 26 reported a clinical failure rate of 21.6% in a surgical cohort treated with soft tissue fixated MAT, significantly exceeding the findings of the current study (8.9%). However, their patient cohort was older (mean, 39.5 years), complicating the comparison and interpretation of the results. Lee et al 42 reported on 222 procedures of MAT with bone fixation and found a clinical failure rate of 11%. Similar results were recently presented by Kim et al, 36 with a clinical failure rate of 8%, corresponding with the finding of the present study.
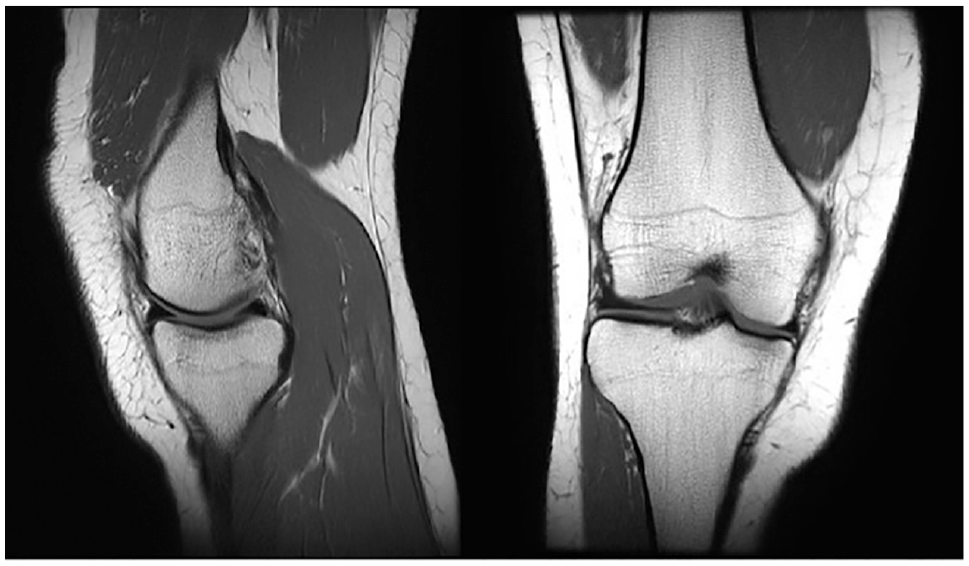
Magnetic resonance imaging scans of a medial meniscal allograft 3 years after transplantation showing anatomic positioning and healing of allograft in (left) sagittal and (right) coronal sections.
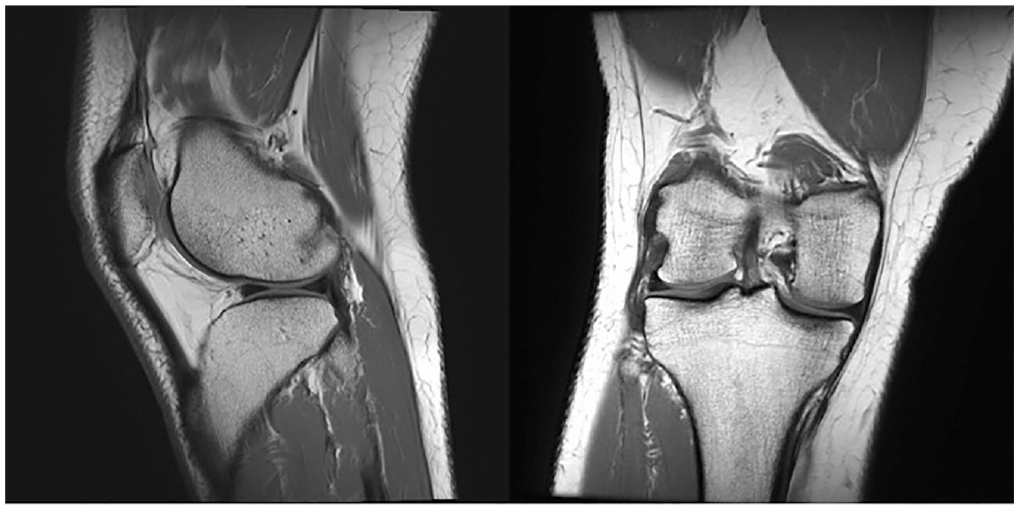
Magnetic resonance imaging scans of a lateral meniscal allograft 3 years after transplantation and concurrent lateral femoral condyle osteochondral allograft transplantation for a 16 × 16-mm full-thickness osteochondral defect. Shown are anatomic positioning and healing of allograft in the (left) sagittal and (right) coronal sections.
The study cohort's mean age of 25 years was notably young, setting it apart from other large MAT case series, which have generally studied older patient cohorts.26,38,48,75,77,83,84 MAT is generally considered an effective reconstructive procedure that can improve symptoms in the affected compartment of the meniscectomized knee and delay progression of articular cartilage degeneration. MAT is indicated in young patients with a meniscal deficiency as they are at high risk of early-onset knee osteoarthritis and are not candidates for arthroplasty. 44 However, ligamentous instability, malalignment, and high-grade articular cartilage loss have been identified to negatively influence MAT outcomes.10,23,34 Accordingly, 111 (71%) procedures in the present study were carried out with ≥1 concurrent surgeries (154 in total), addressing ligamentous instability, malalignment, and cartilage damage. This corresponds with a systematic review by Rosso et al 65 that reported that ≥1 concomitant procedures were performed with MAT in 51% of the cases included in their analysis. This trend addresses the well-documented finding that isolated MAT without correction of accompanying pathologies such as ligament laxity, malalignment, or chondral wear will lead to poorer results.10,24,73 Hence, the number of concurrent surgeries can be used as a global measure of the general condition of the treated knee. Therefore, worse outcomes may be anticipated in patients undergoing concurrent procedures compared with those undergoing isolated MAT. While most studies report primarily on isolated MAT procedures, the present study investigated a unique population ratio with >70% of patients undergoing ≥1 concurrent procedures, which reflects a high case complexity. 43
Articular cartilage damage to the femoral condyles is common in the postmeniscectomy state. 67 This is caused by increased pressure applied to the articular chondral surface, increasing contact loading on chondrocytes. 47 While historically MAT was considered contraindicated in the presence of high-grade focal articular cartilage lesions, studies began to emerge suggesting favorable results when combining MAT with cartilage restorative procedures.6,24,66 In the present study, we report results for 31 patients who underwent OCA transplantation for symptomatic cartilage defects. MAT carried out concurrently with OCA transplantation was associated with elevated failure rates in all categories compared with MAT without OCA transplantation. However, PROMs significantly improved, and the clinical, anatomic, and subjective failure rates at the final follow-up were low. Our findings are consistent with the results of 4 other published investigations that have specifically examined clinical results after combined MAT and OCA.1,23,24,66
Cartilage status of the index compartment has been identified as a prognostic factor for MAT outcome in the present study. These results are supported by previous studies that have reported a correlation between ICRS grade and clinical and anatomic failure rates.7,48,59 However, caution has to be taken when comparing failure rates among different MAT case series because the definitions of clinical and anatomic failure vary and remain controversial. Various criteria are in use as a definition of failure, including graft repair, graft resection, conversion to total knee arthroplasty, clinical outcomes, PROMs, MRI evidence, and second-look arthroscopy. Furthermore, patient-specific parameters vary widely among studies, and objective quantification of outcomes is not always available.36,50,54,56 Therefore, the present study reports clinical, anatomic, and subjective outcomes, avoiding amalgamating patient-reported outcomes with objective clinical diagnostic modalities, such as MRI and second-look procedures. Lee et al 48 reported the effect of ICRS lesion grade on graft survival after medial MAT, assuming a difference in outcomes between medial and lateral MAT. Such an effect was not found in the present study, as results between medial and lateral MAT did not differ. However, the authors found a disparity in outcomes wherein high-grade ICRS lesions were associated with worse anatomic outcomes, while patients still reported fair and improved PROMs. 48 A similar association was present in the current study. Despite a higher anatomic failure rate among patients with high-grade cartilage damage, PROMs remained stable and above the limits of subjective failure (KOOS, 72; IKDC, 70; Lysholm, 69). The minimal clinically important difference (MCID) for the IKDC score is 16.7 at 12 months, which the difference in the high ICRS grade subgroup did not surpass, thus being indicative of a clinically silent change and leading us to question the clinical relevance of a graft tear in some cases. 28 Of note, surgeons need to be aware that even in clinically satisfied patients with good self-reported outcomes, a tear of the graft can be present. Corresponding to the ICRS grade, patients with a Kellgren-Lawrence grade >2 were at increased risk for clinical failure. However, MAT still improved the KOOS and IKDC score in those patients, indicating a beneficial effect of meniscal restoration even in patients with moderate preoperative osteoarthritis. Thus, MAT might have a potential role as a salvage procedure in selected older patients with arthritic changes of the knee, as a recent study found positive effects of meniscal preservation in older patients. 32 The distribution-based MCID in patients after MAT was also determined for the Lysholm score (12.3) and the KOOS Pain (9.9), Symptoms (9.7), Activities of Daily Living (9.5), Sport (13.3), and Quality of Life (14.6) subscores. 49 All thresholds were surpassed in the current study, indicating a relevant clinical effect of MAT on PROMs.
Other patient-specific factors such as age at index surgery, BMI, sex, leg axis, and tibial slope had no significant effect on measured outcomes. Similar results were reported by Frank et al, 21 who reported that PROMs improved similarly after MAT in both patients aged ≥40 and those <40 at the final follow-up with no significant differences in MCID achievement rate, complication rate, reoperation rate, time to reoperation, or failure rate between groups. These results align with the current study in which no significant effect of age on radiographic and clinical failure was detected. Previous studies have suggested that patients with obesity had an increased rate of graft failure. 33 The mean BMI in our study group was 27.2, indicating that our study cohort was overweight according to the definition of the World Health Organization, but not obese, with only 9 patients with a BMI ≥30. 61 This might have influenced the positive results of our study, because increased body weight is known to accelerate the progression of osteoarthritis and increase the risk of degenerative meniscal tears. 20 The tibial slope, known to affect survival of ACL reconstructions, had no significant statistical influence on anatomic, clinical, and subjective survival of MAT. However, a slope of >12° was present in 63 patients at a mean of 14.1°, which might not be enough to have a relevant clinical effect. 82
There are limitations in our study design. First, selection bias might be present as this was a retrospective study. Collection of clinical scores via telephone might be subject to reporting and recall bias. However, previous studies showed that PROMs could be reliably collected through telephone interviews. 39 Second, we separated PROMs from objective clinical outcomes such as MRI findings, radiographs, and second-look arthroscopy. Furthermore, we distinguished between clinical and anatomic failure. We are convinced this precise approach generates a good interpretation basis and avoids overlap of subjective and objective outcomes. However, it might impede comparability to other MAT studies using less precise definitions of failure. Third, we describe a single method of treatment for one patient cohort without comparison with another treatment approach. This is due to evidence that bone fixation of MAT is most likely superior to soft tissue fixation. 56 Fourth, the Lysholm score was only collected at the final follow-up as a commonly used parameter for subjective outcome of MAT.26,48,84 Therefore, it cannot be compared with a preoperative score. However, the KOOS and IKDC score were collected at 2 time points, and a correlation between scores has previously been reported. 13 As a result, validated presentation of PROMs is ensured. In many cases, MAT was carried out concomitantly with additional procedures. In these cases, it is not possible to differentiate between the effect of MAT and the concomitant procedure on outcome measures. Furthermore, after OP MRI was performed according to symptoms, leaving the possibility that anatomic failure occurred without symptoms and could have been missed due to lack of radiographic follow-up. Despite these limitations, our study reports on a large, young population treated with medial and lateral MAT in the context of mostly complex cases. Follow-up with up to 16 years is relatively high compared with previous studies, but the heterogeneity of length of follow-up in our cohort is a significant limitation. Furthermore, this study examines the effect of tibial slope on clinical, anatomic, and subjective outcomes, considering the currently scarce data available on this correlation.
Conclusion
MAT showed good to excellent clinical results at a mean follow-up of 7 years. Low ICRS lesion grade was associated with a higher clinical and anatomic survival rate. Patients with concurrent OCA transplantation are at higher risk of clinical and anatomic failure but still report significantly improved PROMs. These results suggest that MAT has a lasting beneficial effect both in isolation and in complex cases with ≥1 concurrent procedures.
Footnotes
Submitted December 22, 2022; accepted September 15, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.H. was funded by Deutsche Forschungsgemeinschaft (DFG; German Research Foundation) Projektnummer 466023693. The authors acknowledge support from the Foderaro-Quattrone Musculoskeletal-Orthopaedic Surgery Research Innovation Fund. M.J.S. has received royalties, consulting fees, and compensation for services other than consulting from Arthrex Inc; and research support from Stryker. B.A.L. has received royalties, consulting fees, and compensation for services other than consulting from Arthrex Inc; consulting fees from Smith + Nephew; and speaking fees from Linvatec. D.B.F.S. has received consulting fees from Smith + Nephew and research support from JRF. A.J.K. has received research support from Aesculap/B.Braun, Arthrex, Arthritis Foundation, Ceterix, and Histogenics; consulting fees from Arthrex, JRF Ortho, Vericel, and Responsive Arthroscopy; royalties from Arthrex and Responsive Arthroscopy; honoraria from JRF, Vericel, and Musculoskeletal Transplant Foundation; grant from DJO; and personal fees from Ceterix Orthopaedic, Gemini Mountain Medical, and Smith + Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.