
Abstract
Background:
Hip arthroscopic surgery for femoroacetabular impingement syndrome (FAIS) has proven to be an effective surgical intervention, with high rates of return to sport and work as well as favorable outcomes at short- and midterm follow-up. However, limited data exist on outcomes at long-term follow-up.
Purpose:
To evaluate patient-reported outcomes (PROs) at a minimum 10-year follow-up after primary hip arthroscopic surgery including labral repair, femoral osteochondroplasty, acetabular osteochondroplasty, and capsular closure for FAIS.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent primary hip arthroscopic surgery for FAIS between June 2012 and January 2013 were identified. PROs were collected preoperatively and at a minimum of 10 years postoperatively, including the Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Subscale (HOS-SS), modified Harris Hip Score (mHHS), International Hip Outcome Tool–12 (iHOT-12), and visual analog scale (VAS) for pain and satisfaction. Unique minimal clinically important difference (MCID) and patient acceptable symptom state (PASS) thresholds were calculated, and their rates of achievement were analyzed. An alpha level of <.05 was used to determine statistical significance.
Results:
A total of 94 patients (55 female; mean age, 34.3 ± 12.4 years) were analyzed with a mean follow-up of 10.1 ± 0.3 years (range, 10.0-10.7 years). Patients demonstrated significant 10-year improvement across all PRO measures (P < .001). MCID and PASS thresholds were calculated as follows: HOS-ADL (10.4 and 85.3, respectively), HOS-SS (14.6 and 60.2, respectively), mHHS (8.8 and 76.0, respectively), VAS pain (14.6 and 27.5, respectively), and iHOT-12 (PASS: 71.4). The majority of patients achieved the MCID and PASS for each PRO measure: HOS-ADL (73.4% and 70.9%, respectively), HOS-SS (78.5% and 77.2%, respectively), mHHS (81.0% and 70.9%, respectively), VAS pain (88.6% and 70.9%, respectively), and iHOT-12 (PASS: 73.4%). Overall, 9 patients (9.6%) underwent subsequent revision hip arthroscopic surgery at a mean 4.9 ± 3.7 years (range, 1.1-10.1 years) postoperatively, and 6 patients (6.4%) underwent conversion to total hip arthroplasty at a mean 4.1 ± 3.1 years (range, 0.9-9.3 years) postoperatively.
Conclusion:
Patients who underwent primary hip arthroscopic surgery for FAIS utilizing contemporary methods of labral repair, acetabular and/or femoral osteochondroplasty, and capsular closure commonly experienced sustained clinical improvement and reported high levels of satisfaction at a minimum 10-year follow-up with low rates of reoperation.
Since its initial description by Ganz and colleagues 23 in 2003, femoroacetabular impingement syndrome (FAIS) has garnered widespread recognition as a significant source of hip pain and dysfunction. Accordingly, hip arthroscopic procedures have rapidly become popular, 46 with an 85% increase in volume in the United States between 2011 and 2018. 73 In its earliest iterations, hip arthroscopic surgery was performed without significant consideration given to capsular management. Subsequent biomechanical research revealed deleterious effects associated with unrepaired capsulotomy on joint stability as well as improved biomechanical function with capsular repair.1,33 Numerous clinical studies have corroborated the importance of meticulous repair of the hip capsule.9,14,22,24,37,66,69 Additionally, labral repair has been shown to result in superior outcomes compared with labral debridement.35,39,49
Previously published long-term clinical outcomes assessing the efficacy of hip arthroscopic surgery for the treatment of FAIS have necessarily included patients without capsular repair and/or labral repair when such procedures would be indicated in modern practice.17-25 As a result, these investigations do not reflect the long-term findings associated with contemporary techniques for the treatment of FAIS, including surgical correction of pathomorphology, chondrolabral refixation, and capsular management. The current literature supports that hip arthroscopic surgery for FAIS has reliable short- and midterm patient-reported outcomes (PROs) and clinical success,2,15,30,38,43,52,57,70 including in athletes11,12,59 and adolescents,31,42 among other unique populations. However, longer-term data using modern hip arthroscopic techniques for the treatment of FAIS are limited.
The purpose of the present study was to evaluate PROs and rates of revision hip arthroscopic surgery and conversion to total hip arthroplasty (THA) at a minimum 10-year follow-up after primary hip arthroscopic surgery including modern techniques of chondrolabral refixation, femoral osteochondroplasty, acetabular osteochondroplasty, and capsular repair for FAIS. We hypothesized that hip arthroscopic surgery would produce sustained clinical benefits and favorable PROs, with low rates of patients requiring revision hip arthroscopic surgery or conversion to THA.
Methods
Patient Selection
This study was approved by our institutional review board. No funding was received for the completion of this work. We conducted a retrospective review of a prospectively maintained single-institution database to analyze the clinical outcomes of patients who underwent primary hip arthroscopic surgery performed by the senior author (S.J.N.) from June 1, 2012, to January 31, 2013. All patients consented to participate in the hip arthroscopic surgery repository. Inclusion criteria were as follows: (1) clinical (eg, hip pain lasting >3 months, positive anterior impingement test finding) and radiographic (ie, cam deformity: 90° Dunn view with alpha angle >55°4,26; pincer deformity: anteroposterior view with lateral center edge angle [LCEA] >40°, presence of cross-over sign, acetabular index <0° 61 ) evidence of symptomatic FAIS, (2) minimum 10-year follow-up with the completion of at least one PRO measure, and (3) failure of nonoperative treatment (ie, oral anti-inflammatory drugs, physical therapy, activity modification, and/or intra-articular corticosteroid injections).
Exclusion criteria were as follows: (1) index surgery at our practice was revision hip arthroscopic surgery, (2) Tönnis grade >1 osteoarthritis, (3) concomitant hip procedures (eg, gluteus medius/minimus repair, microfracture, psoas lengthening), (4) history of pediatric developmental hip disorders (eg, slipped capital femoral epiphysis or Legg-Calvé-Perthes disease), and (5) hip dysplasia defined as an LCEA <20°. 18
A total of 168 hips were assessed for eligibility. Of these, 133 were eligible after exclusion criteria. Overall, 94 patients (70.7% follow-up rate) completed at least one PRO measure at a minimum of 10-year follow-up or underwent conversion to THA or revision hip arthroscopic surgery and were included in final analyses (Figure 1).
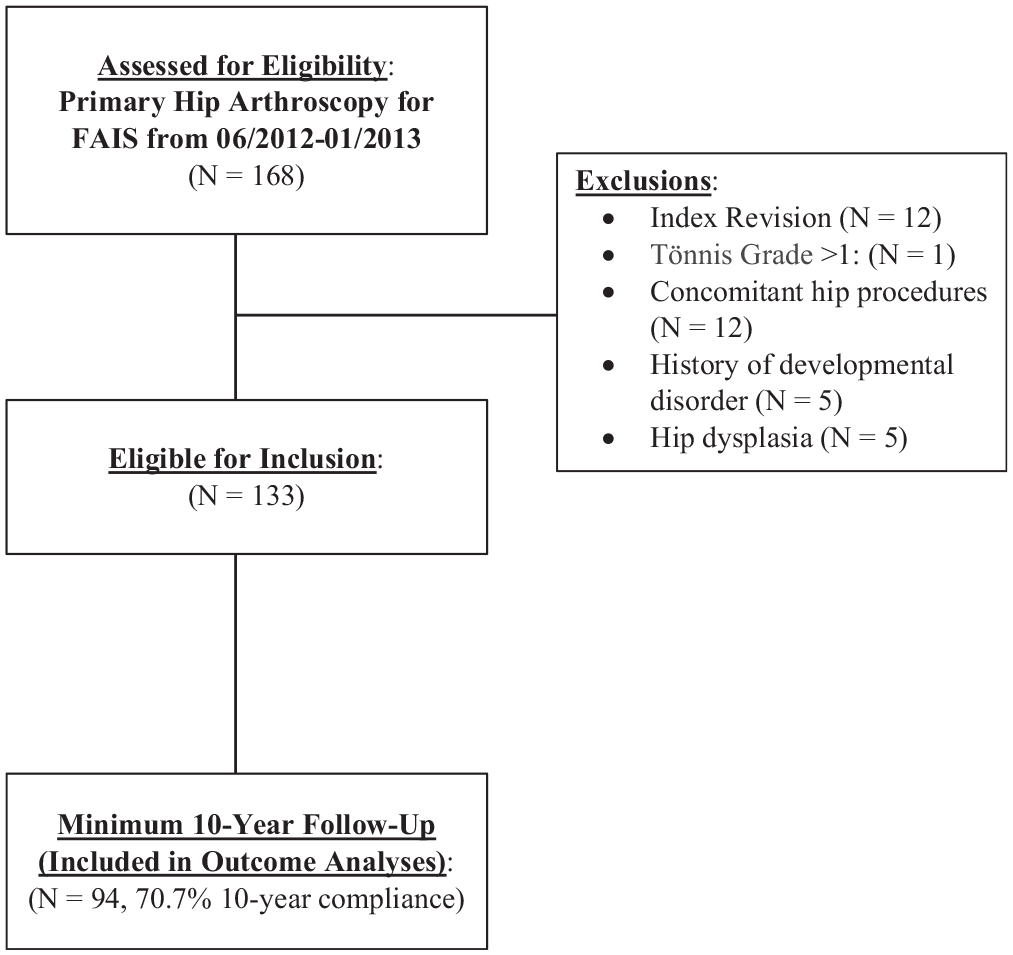
Consolidated Standards of Reporting Trials (CONSORT) diagram of patient selection. FAIS, femoroacetabular impingement syndrome.
Patient Characteristics
Baseline patient information, including age, sex, and body mass index, was collected. Additional preoperative characteristics obtained included duration of symptoms, smoking status, physical activity status, workers’ compensation status, and psychiatric history. Intraoperative findings were also collected including type of procedure, number of anchors, and presence of acetabular cartilage damage (Beck classification)5,6,50 and femoral head cartilage damage (Beck classification).3,47 Lastly, postoperative complications including infections, neuropathy, and deep vein thrombosis were recorded. All information was collected in a secure, prospectively maintained repository.
Radiographic Examination
Patients underwent a standard hip series of radiographs preoperatively and at their initial postoperative clinic visit including standing anteroposterior, false profile, and Dunn lateral (at 90° of hip flexion) views. The alpha angle was measured by a conventional technique in the Dunn lateral view,54,67 and the LCEA13,68 and Tönnis angle 16 were measured in the anteroposterior view of the affected hip.
Surgical Technique
Using a technique that has been described previously, all surgical procedures were performed by the senior author (S.J.N.).29,65 Briefly, patients underwent general anesthesia, were placed in a modified supine position, and were placed in traction with a well-padded perineal post. The anterolateral and modified midanterior portals were then established, and an arthroscopic scalpel was used to connect the 2 portals, creating the interportal (transverse) portion of the capsulotomy site while reserving some tissue on the acetabular and femoral sides for later capsular closure. Any central femoroacetabular compartment abnormality, including pincer morphology and labral tearing, was addressed using well-established techniques.29,65 Where there was acetabular cartilage damage, chondroplasty was performed as necessary. A distal accessory anterolateral portal was established when indicated to facilitate labral repair. After central compartment work was complete, traction was released.
T-type capsulotomy was performed by extending the interportal capsulotomy site inferiorly to the longitudinal limb. Access was then gained to the peripheral compartment, allowing direct visualization of the cam deformity, and, if present, osteochondroplasty was performed until appropriate cam resection and an adequate femoral head-neck offset were achieved. Subsequently, a dynamic examination of the surgical leg was performed to ensure resolution of the cam impingement. Capsular closure was performed with ultra-high molecular weight polyethylene sutures, beginning at the base of the vertical portion and followed by the interportal segment.
Postoperative Rehabilitation
Postoperative care and rehabilitation were performed by employing a previously published 4-phase rehabilitation protocol standard to our institution. 44 Over the course of the first phase (approximately weeks 1-6), rehabilitation was directed toward the goal of gradually increasing walking, with patients transitioning off braces and crutches. During the second phase (approximately weeks 7-12), the goal was to progress gait and address any compensatory gait strategies. During the third phase (approximately weeks 13-16), the focus was to return patients to preinjury activity levels. Finally, during the fourth phase (weeks 16 and beyond), rehabilitation included sport-specific training and a gradual transition to return to sport.
Assessment of PROs
PROs were collected via secure electronic data collection platforms (OBERD or PatientIQ) preoperatively and at several time points postoperatively, including at 1, 2, 5, and 10 years. Patients completed surveys at the clinic, through a telephone interview, or via encrypted email. PROs obtained included scores for the Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Subscale (HOS-SS), modified Harris Hip Score (mHHS), International Hip Outcome Tool–12 (iHOT-12; beginning at 2 years postoperatively), and visual analog scale (VAS) for pain and satisfaction. Patients who underwent revision hip arthroscopic surgery or conversion to THA were also included; however, they were removed from any PRO analyses that were conducted after the date of their subsequent procedure (eg, if a patient underwent revision at 3 years after the index procedure, he or she would be included in 2-year PRO analysis but not in 5- and 10-year analyses).
Evaluation of Clinically Significant Outcomes
Clinically significant outcomes were evaluated, which included the minimal clinically important difference (MCID)32,60 and patient acceptable symptom state (PASS). 34 Incomplete or missing PRO surveys were excluded from analyses of clinically significant outcomes.
Unique MCID thresholds for the HOS-ADL, HOS-SS, mHHS, and VAS pain at a minimum of 10 years were calculated using the distribution method, taking one-half the standard deviation of the difference between preoperative and 10-year postoperative PRO scores. 53 Once the unique MCID threshold was established, the difference in PRO scores from preoperatively to 10 years was calculated and compared with the MCID threshold to determine the rate of achievement. Unique MCID thresholds were calculated as follows: HOS-ADL, 10.4; HOS-SS, 14.6; mHHS, 8.8; and VAS pain, 14.6.
To determine unique PASS thresholds, receiver operating characteristic (ROC) curve analysis with the Youden index (calculated as sensitivity + specificity) was performed for each PRO measure. At the 10-year time point, patients were asked the following yes/no question: “Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?” The answer to this question was coded as a binary outcome (0 = no, 1 = yes) for ROC area under the curve (AUC) analysis. A minimum AUC of 0.7 was required to be considered acceptable discriminative ability.27,45,58 To determine the threshold along the point coordinates of the ROC curve, the Youden index was utilized to maximize the sensitivity and specificity of the score. Once established, each patient’s 10-year PRO scores were compared with the threshold for each PRO measure to determine the rate of achievement. Unique PASS thresholds for the HOS-ADL, HOS-SS, mHHS, iHOT-12, and VAS pain were calculated as follows: 85.3, 60.2, 76.0, 71.4, and 27.5, respectively. All thresholds demonstrated acceptable discriminative ability (AUC >0.7) with high sensitivity and specificity.
Statistical Analysis
Descriptive statistics were reported for patient characteristics, intraoperative findings, radiographic measurements, and PRO scores. Continuous variables are reported as means and standard deviations, while categorical variables are presented as counts and percentages. Outcomes were assessed for normality using the Shapiro-Wilk test. As outcomes were normally distributed, the paired-samples t test was utilized to assess for significant improvements in PROs relative to preoperative values.
An alpha level of < .05 was used to determine statistical significance. To ensure a proper sample size for the primary outcome of interest (10-year improvement in PROs), post hoc power analysis was performed and demonstrated that, with 94 total patients with preoperative and postoperative measurements and a medium (0.5) effect size, the study had 99.7% power. All statistical analyses were conducted using SPSS (Version 28.0; IBM).
Results
Patient Characteristics
A total of 94 patients (55 female and 39 male; mean age, 34.3 ± 12.4 years [range, 15.0-62.0 years]) had a minimum of 10-year follow-up and were included in final analyses. Patients had a mean follow-up of 10.1 ± 0.3 years (range, 10.0-10.7 years). Preoperative patient characteristics are summarized in Table 1. Labral repair was performed in 95.7% of the patients, and 100.0% underwent capsular closure. The mean preoperative LCEA was 30.1°± 6.0° (range, 20.0°-44.2°), and the mean preoperative alpha angle was 64.4°± 12.9° (range, 43.5°-92.1°) (Table 2).
Baseline Patient Characteristics a
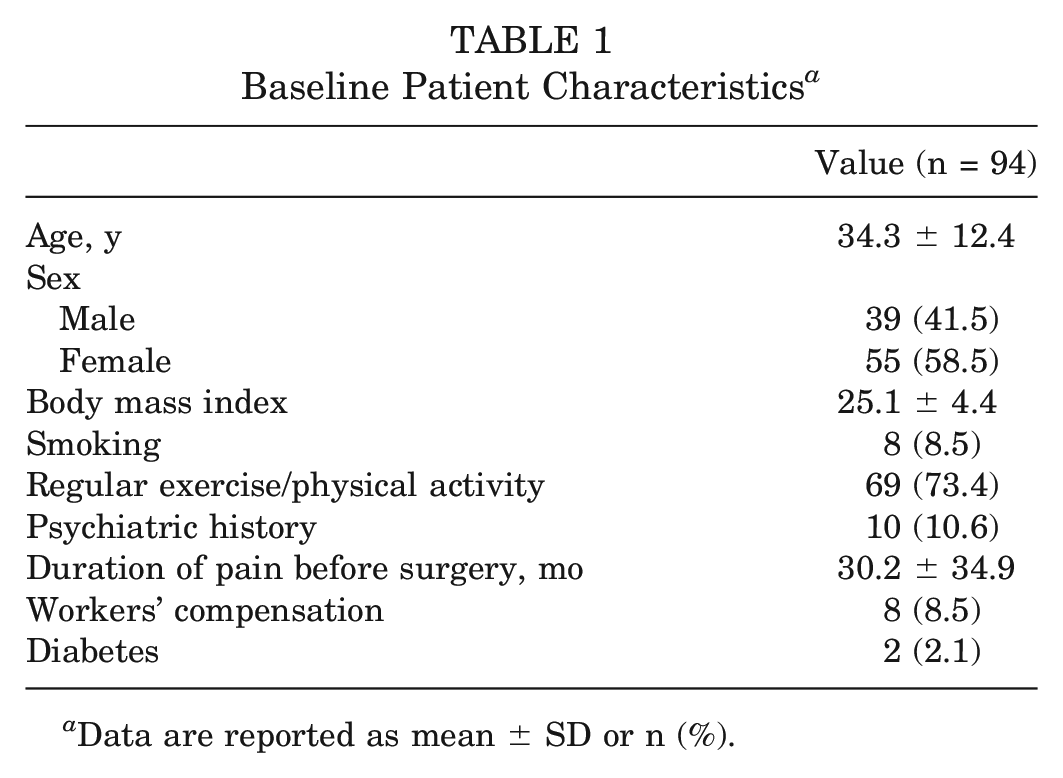
Data are reported as mean ± SD or n (%).
Radiographic and Intraoperative Findings a
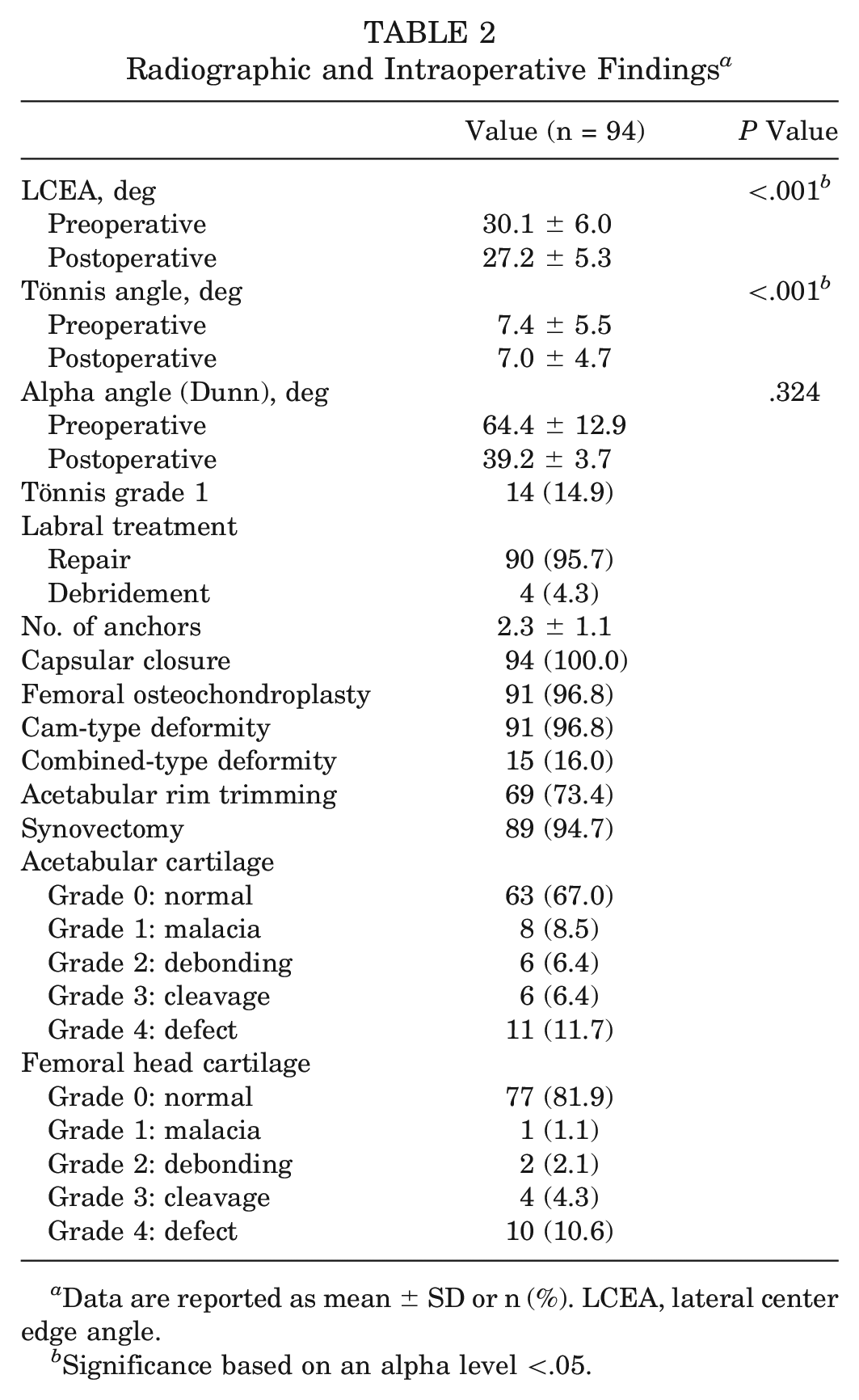
Data are reported as mean ± SD or n (%). LCEA, lateral center edge angle.
Significance based on an alpha level <.05.
10-Year PROs
On average, for those who did not require revision or conversion to THA, patients demonstrated a significant improvement in all PROs from preoperatively to 10 years postoperatively (P < .001) (Table 3). Additionally, favorable outcomes were seen for the iHOT-12 and VAS satisfaction at 10 years.
Patient-Reported Outcomes at Baseline and 10 Years a
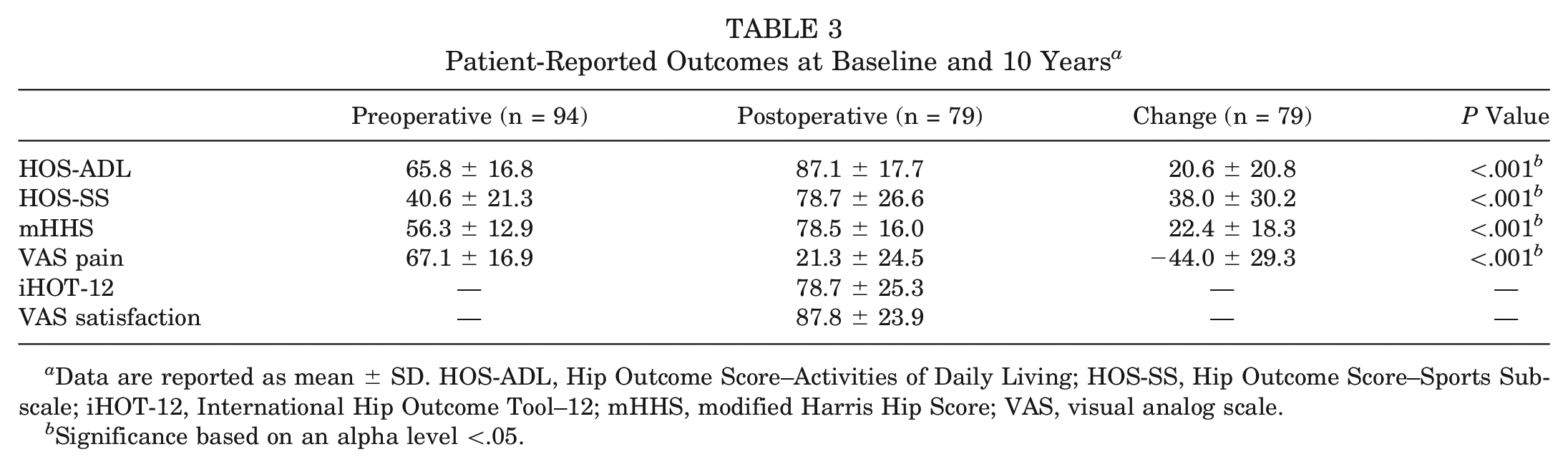
Data are reported as mean ± SD. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Significance based on an alpha level <.05.
Postoperative PRO Trend
Patients improved significantly from preoperatively to 1-year follow-up regarding HOS-ADL, HOS-SS, mHHS, and VAS pain scores (P < .001 for all). Between the 1- and 2-year follow-up time points, VAS pain (P = .005) and satisfaction (P = .019) scores demonstrated significant improvement; otherwise, no significant changes were seen regarding the other PRO measures (P > .05). Between the 2- and 5-year time points, the VAS pain score significantly worsened (P < .001), whereas between the 5- and 10-year time points, the VAS pain score significantly improved (P < .001). Otherwise, no significant changes were noted in the other PRO measures between 2 and 5 years and between 5 and 10 years (Table 4 and Figure 2).
Patient-Reported Outcomes Stratified by Preoperative and Postoperative Time Points a
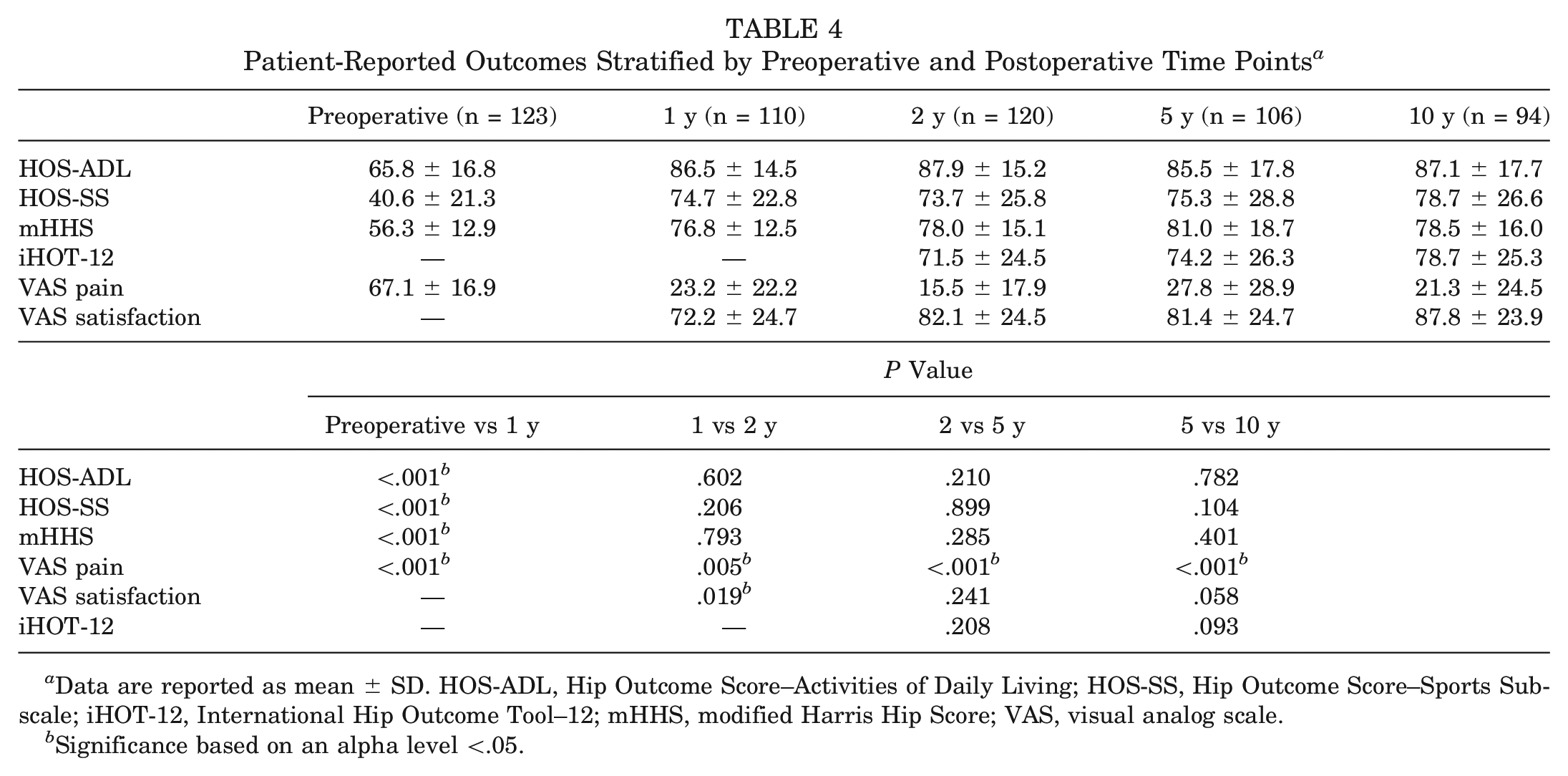
Data are reported as mean ± SD. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Significance based on an alpha level <.05.
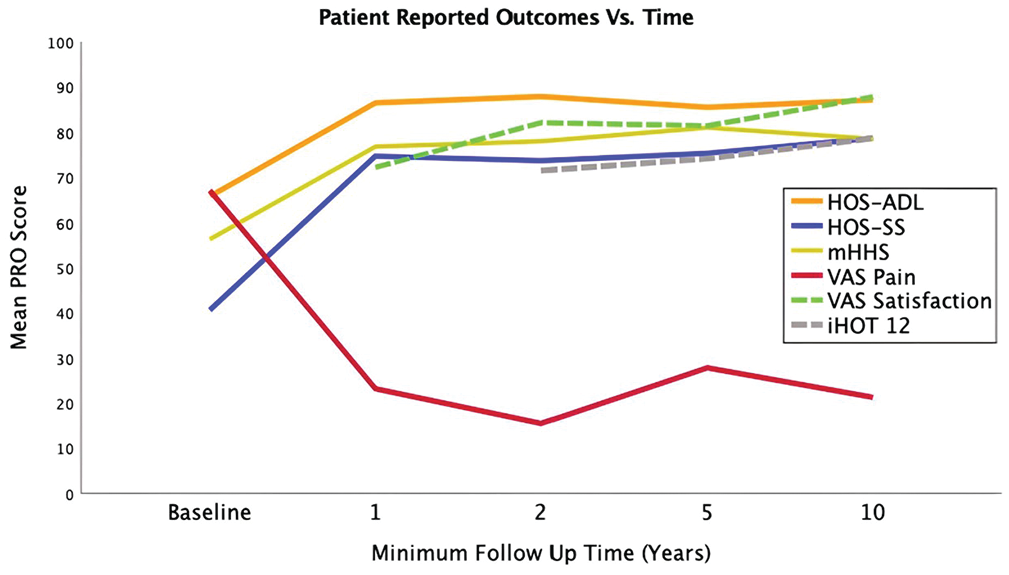
Patient-reported outcome (PRO) comparisons at sequential time points. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Clinically Significant Outcomes
Achievement rates for the MCID and PASS of patients (n = 79) who did not undergo secondary surgery are noted in Table 5. The majority of patients achieved the MCID for all PRO measures. Additionally, the majority of patients achieved the PASS for all PRO measures. Furthermore, a majority of patients achieved positive clinical outcomes, with 91.1% of patients exceeding the MCID for at least one PRO measure, 79.7% achieving the PASS for at least one PRO measure, and 77.2% surpassing both the MCID and PASS for at least one PRO measure.
MCID and PASS Threshold Scores a
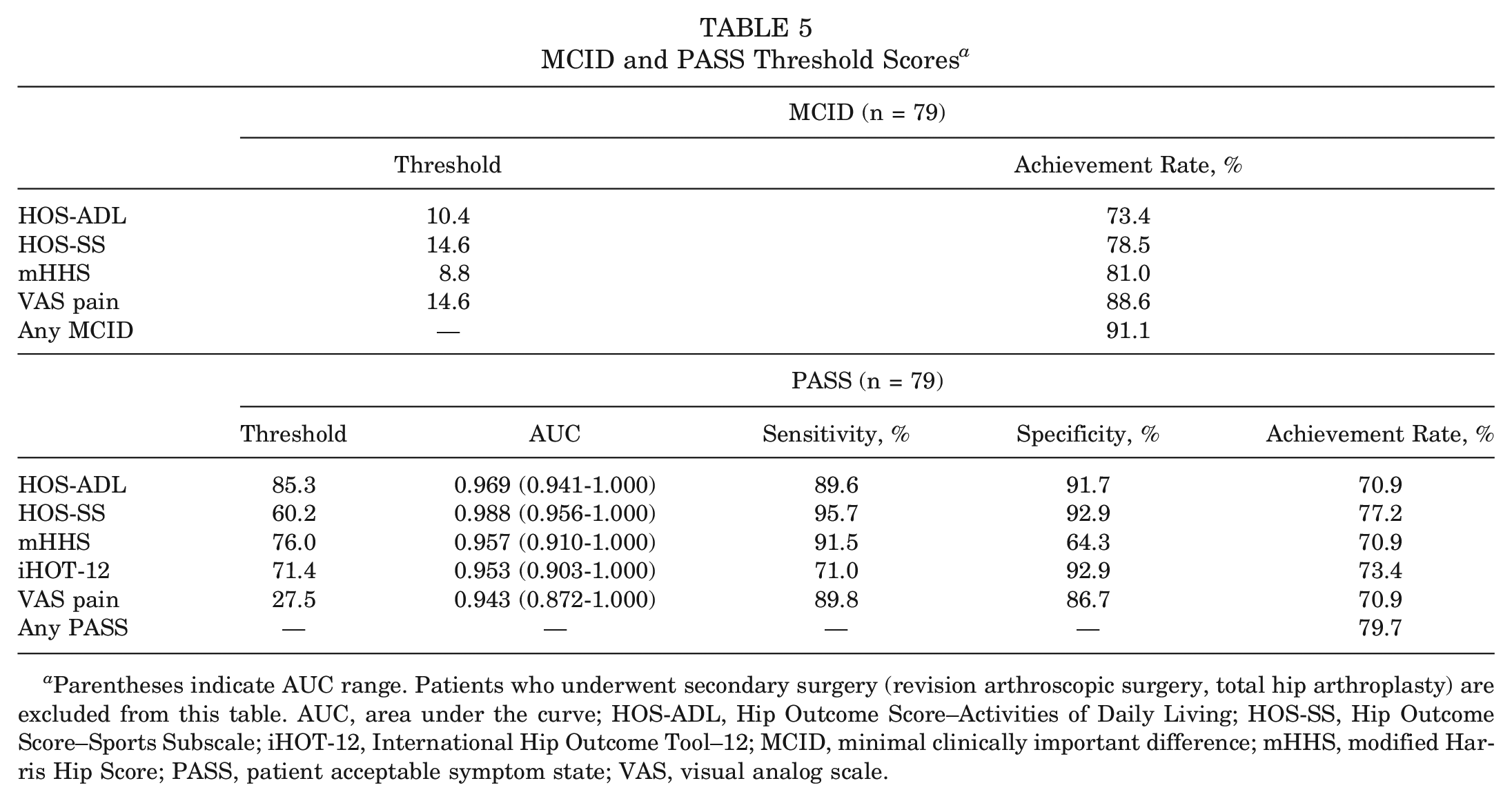
Parentheses indicate AUC range. Patients who underwent secondary surgery (revision arthroscopic surgery, total hip arthroplasty) are excluded from this table. AUC, area under the curve; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, International Hip Outcome Tool–12; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptom state; VAS, visual analog scale.
When including results of patients who underwent either revision surgery or conversion to THA as failures, the rates of achieving the MCID and PASS were as follows: HOS-ADL (61.7% and 60.0%, respectively), HOS-SS (66.0% and 64.9%, respectively), mHHS (68.1% and 60.0%, respectively), VAS pain (74.5% and 60.0%, respectively), and iHOT-12 (PASS: 61.7%). Furthermore, 76.6% of patients achieved the MCID for any PRO measure, and 67.0% of patients achieved the PASS for any PRO measure.
Reoperation and Complication Rates
The gross survival rate, as displayed by the Kaplan-Meier curve, was 84.0% at 10-year follow-up (Figure 3A). There were 9 patients (9.6%) who underwent revision hip arthroscopic surgery at a mean 4.9 ± 3.7 years (range, 1.1-10.1 years) postoperatively. Of the 9 patients undergoing revision, 3 (33.3%) underwent surgery because of prolonged pain, 3 (33.3%) because of adhesions/scar tissue, 2 (22.2%) because of heterotopic ossification, and 1 (11.1%) because of recurrent cam deformity. There were 6 patients (6.4%) who underwent conversion to THA at a mean 4.1 ± 3.1 years (range, 0.9-9.3 years) postoperatively (Figure 3B). Complications included 1 patient (1.1%) experiencing deep vein thrombosis at 1.5 weeks postoperatively and 2 cases (2.1%) of immediate postoperative transient pudendal neuropathy, both of which resolved by 6 months postoperatively. No complications occurred in this cohort beyond 6 months postoperatively.
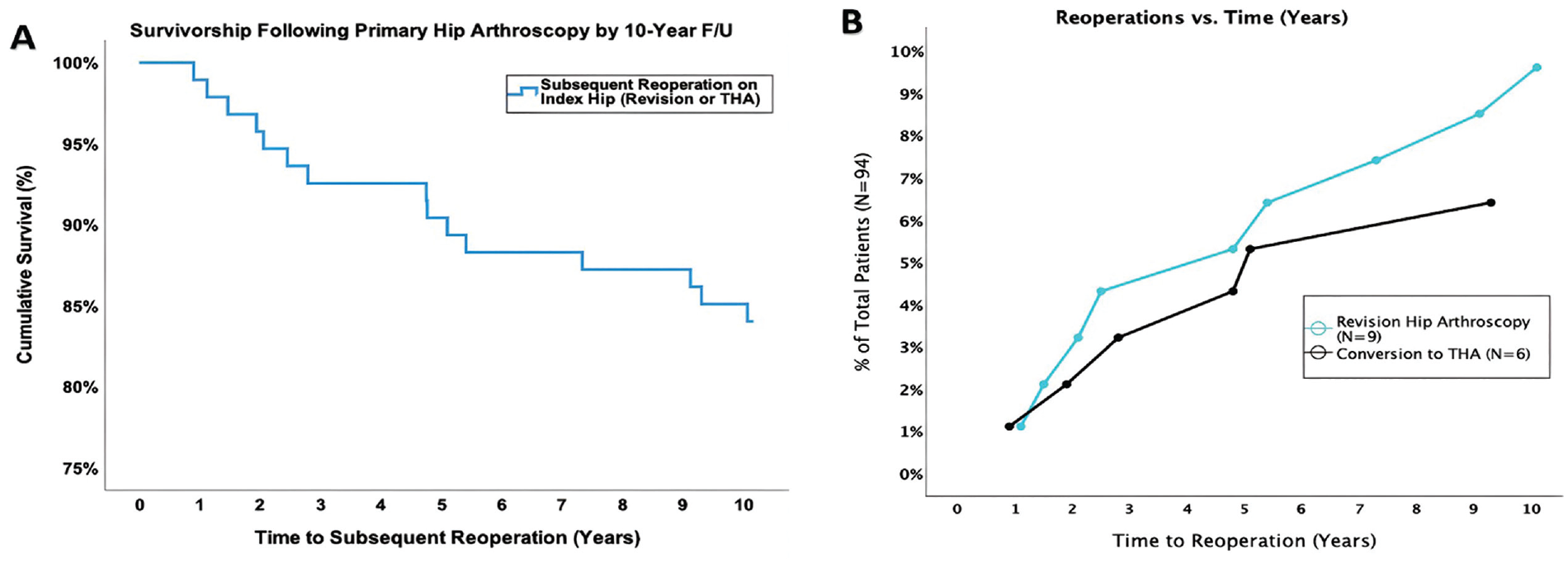
(A) Kaplan-Meier gross survival curve for a minimum 10-year follow-up. (B) Trend of revision hip arthroscopic surgery and conversion to total hip arthroplasty (THA) from baseline to 10-year follow-up.
Discussion
The most important findings from the present investigation are that patients sustained significant improvement in PRO scores at 10-year follow-up, with the majority reaching the MCID and achieving the PASS. There were low rates of patients who underwent revision arthroscopic surgery (9.6%) or conversion to THA (6.4%). These results confirm our hypotheses and support the sustained benefit of the contemporary treatment of appropriately selected patients with FAIS with hip arthroscopic surgery including chondrolabral repair, acetabular and/or femoral osteochondroplasty, and capsular closure. The preeminent strength of this investigation is that it is one of the largest studies of primary hip arthroscopic surgery for FAIS using modern techniques with a long-term follow-up.
Although there are valuable longer-term studies on hip arthroscopic surgery in the literature, many that are currently available report on cases in which contemporary techniques were not employed. For example, previous long-term follow-up studies have described surgical techniques that approach the central compartment only, 8 perform debridement or resection of the labrum as opposed to repair as a major treatment method,7,19,25,40,72 utilize open techniques, 25 and do not include or specify capsular closure/repair.10,49,71,72 Moreover, many of these studies are limited by a low rate (<50%) of follow-up, which may bias results.19,48,71 The 70.7% follow-up rate of the current study is high relative to the current literature, and our study is one of the few to utilize consistent contemporary approaches (chondrolabral repair, acetabular and/or femoral osteochondroplasty, capsular closure) for treatment. As techniques in hip arthroscopic surgery continue to evolve, it is important to evaluate whether such changes translate to improved outcomes. Grammatopoulos et al 25 reported 10-year outcomes including patients who underwent open treatment with surgical hip dislocation, combined open and arthroscopic treatment, arthroscopic labral debridement, and arthroscopic labral repair and did not find, in their case series, clear relationships between the technique and outcomes. However, it is known now that correction of bony morphology is critical, labral debridement is inferior to repair, and capsular closure is paramount to better clinical outcomes.36,51,62
In the present study, patients obtained sustained clinically significant outcomes at a minimum 10 years of follow-up. Specifically, 91.1% of patients exceeded the MCID for at least one PRO measure, 79.7% achieved the PASS for at least one PRO measure, and 77.2% of patients met both the MCID and PASS for at least one PRO measure. These findings are consistent with previous literature on shorter-term outcomes. Levy et al, 41 in 2016, performed a meta-analysis of 81 studies on primary hip arthroscopic surgery and found that >90% of study populations met the MCID for the mHHS, HOS-ADL, and HOS-SS. PASS rates, on the other hand, were lower, with 88% for the mHHS but only 25% and 30% for the HOS-ADL and HOS-SS, respectively. 41 One explanation for why the present study’s PASS rates were >70% for each PRO measure is the consistent use of modern surgical techniques. Other long-term studies with similar surgical approaches are needed to validate the success rates seen in the present study.
Other important findings of this study are the trends in PRO improvement over time. When evaluating the PROs sequentially, it appears that the majority of improvement occurred within the first 2 years. Besides the VAS pain, there were no significant differences found between the 2- and 5-year time points and between the 5- and 10-year time points for any of the other PRO measures. Flores et al 21 also found that patients improved up to 2 years postoperatively, with the majority of improvement occurring in the first 3 months. Nwachukwu et al 56 similarly found that more than half of patients achieved clinically significant outcomes (MCID and substantial clinical benefit) by 6 months postoperatively, although improvement continued to 2 years. Nwachukwu et al, 55 in a separate study, continued to find that the highest proportion of patients achieved clinically significant outcomes at 2 years postoperatively, and even though patients had sustained clinical outcomes at 5 years, the proportion at that time point was fewer than at the 2-year time point. The present study demonstrates that results were sustained even longer to 10 years, but longer-term data will better elucidate the expected total duration of improvement. These data are valuable for patient counseling, as patients may be told to continue to expect improvement until approximately 2 years, but after that time, additional benefit is unlikely. Another notable perspective is that many patients doing well at 2 and 5 years will continue to have durable results at 10 years. One study showed that patients not meeting the MCID or substantial clinical benefit by 1 year postoperatively are at risk of subsequent surgery within 5 years postoperatively. 20 Furthermore, the trend identified in VAS pain scores can likely be attributed to the timeline of patients undergoing revision and conversion to THA; from 2 to 5 years postoperatively, patients who would undergo secondary surgery were still included in PRO analyses, contributing to the higher VAS pain scores seen at the 5-year time point. When these patients undergoing secondary surgery (revision and conversion to THA) were excluded subsequently beyond the 2- to 5-year time frame, the VAS scores therefore improved at 10 years postoperatively.
At a minimum 10-year follow-up, the rate of subsequent ipsilateral arthroscopic surgery was 9.6%, and 6.4% of patients underwent conversion to THA, with a cumulative survival rate for reoperation at 10 years of almost 85%. Because the number of total failures was small in this cohort, it is challenging to accurately understand the reasons for failure in these patients. Previous studies have consistently identified older age, among other factors, such as a greater degree of degeneration in the hip joint, as a risk for failure.2,30,63 Although some data exist suggesting smaller rates of reoperation than in the present study, those other studies have a much shorter follow-up. 28 The mean time to revision hip arthroscopic surgery was nearly 5 years, and the mean time to conversion to THA was just over 4 years, suggesting that at least midterm follow-up is needed to understand meaningful reoperation rates. When evaluating the trend of reoperations over time, it appears that more reoperations for revision hip arthroscopic surgery and conversion to THA occurred around 5 years and later. All patients in this cohort undergoing a reoperation earlier than 5 years seemed to undergo surgery within the first 2 years, suggesting that certain patients may declare failed results for these procedures quickly. Future studies may investigate how to identify early versus late failures and what patient characteristics may distinguish them for preoperative counseling and planning. Additionally, future studies with a further follow-up past 10 years would be useful to understand how long improvements can be sustained and what effect a longer follow-up has on the rates of subsequent surgery. Finally, additional analysis including regression analysis analyzing risk factors for failure and secondary surgery should be performed with larger study populations.
Limitations
This study has several limitations. It is a retrospective case series, and causation is difficult to determine. Although the follow-up rate of 70.7% is high for this long-term time frame and relative to the current literature, it still may introduce an element of bias in the results because of the inclusion of only patients who were able to be contacted. Furthermore, given the relatively low number of patients who underwent revision hip arthroscopic surgery or conversion to THA, it is not yet possible to determine causative differences between patients undergoing revision hip arthroscopic surgery or conversion to THA and those who did not. The study cohort included patients with borderline hip dysplasia (ie, LCEA of 20°-25°); even though these patients have high long-term survivorship,17,64 they may represent a different abnormality than patients without any dysplasia. Finally, the present study reports data from surgical procedures performed by a single fellowship-trained sports medicine surgeon with advanced training and experience in hip arthroscopic surgery practicing at a high-volume, tertiary referral orthopaedic practice. Consequently, the study results may not be generalizable to patients treated by surgeons with different levels of training, experience, and/or hip arthroscopic case volume.
Conclusion
Patients undergoing primary hip arthroscopic surgery for FAIS utilizing contemporary methods of chondrolabral repair, acetabular and/or femoral osteochondroplasty, and capsular closure commonly experienced sustained clinical improvement and reported high levels of satisfaction at a minimum 10-year follow-up with low rates of reoperation.
Footnotes
Submitted May 8, 2023; accepted September 15, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.A. has received support for education from Smith+Nephew. C.M.B. has received support for education from Smith+Nephew and hospitality payments from Exactech. S.J.N. has received research support from AlloSource, Arthrex, Athletico, DJ Orthopedics, Linvatec, MioMed, and Smith+Nephew; consulting fees from Ossur, SI-BONE, Springer, and Stryker; royalties from Ossur, Springer, and Stryker; and support for education from Elite Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.