
Abstract
Background:
There is scarce literature on clinically significant values after arthroscopic Bankart repair (ABR).
Purpose:
To determine the minimal clinically important difference (MCID) and the patient acceptable symptom state (PASS) thresholds at 1 year for the Rowe and Athletic Shoulder Outcome Scoring System (ASOSS) scores after ABR and to determine the effect of patient characteristics on these metrics after ABR.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective review of patients undergoing ABR from a single institution between January 2017 and January 2020 was performed. Patients with at least 1 episode of instability and a minimum follow-up of 12 months were included. The exclusion criteria were as follows: bony defects of >20% on the anteroinferior portion of the glenoid based on a preoperative computed tomography scan; engaging Hill-Sachs lesions at 90° of abduction and 90° of external rotation based on an arthroscopic examination; previous surgery on the same shoulder; multidirectional instability or concomitant repair of full-thickness rotator cuff tears; superior labral anterior to posterior lesions; posterior labral tears; or humeral avulsion of the glenohumeral ligament lesions. Patient-reported outcome measures were collected both preoperatively and 1-year postoperatively. Delta was defined as the change between preoperative and 1-year postoperative scores. Distribution-based (one-half the standard deviation of the difference between pre- and postoperative outcome scores) and anchored-based approaches (response to a satisfaction question at 1 year) were used to estimate the MCID and the PASS, respectively. The optimal cutoff point, where sensitivity and specificity were maximized, and the percentage of patients achieving those thresholds were also calculated.
Results:
Overall, 190 patients were included. The distribution-based MCID for the Rowe and ASOSS scores were calculated to be 8.2 and 8.7, respectively. The rate of patients who achieved MCID thresholds was 96% for the Rowe and 96% for ASOSS scores. The PASS threshold for the Rowe and ASOSS scores were ≥80 and ≥90, respectively. The rate of patients who achieved PASS scores after ABR were 86% and 83%, respectively. The MCID and PASS values showed great variability based on sex (men: 8.5 and ≥85 for Rowe / 8.9 and ≥90 for ASOSS, respectively, vs women: 6.7 and ≥73 for Rowe / 8.1 and ≥75 for ASOSS), age (≥21: 8.4 and ≥80 / 9.2 and ≥90 vs <21: 7.8 and ≥75 / 7.7 and ≥85), sports participation (sports: 8.8 and ≥85 / 9.5 and ≥90 vs no sports: 8.1 and ≥75 / 8.6 and ≥80), and type of athlete (competitive: 8.4 and ≥85 / 8.9 and ≥87 vs recreational: 7.5 and ≥73 / 8.1 and ≥68).
Conclusion:
This study identified the MCID and PASS thresholds for the Rowe and ASOSS scores at 1 year after ABR. However, these values showed great variability when accounting for different patient characteristics such as sex, age, sports participation, and type of athlete, highlighting the importance of considering individual patient-specific characteristics for optimal treatment decision-making and ensuring treatment success tailored to each patient’s unique needs and expectations.
Keywords
Arthroscopic Bankart repair (ABR) is considered one of the most common procedures to address shoulder instability, and it has been associated with excellent outcomes.1-3 Historically, a successful outcome after surgery involves no recurrent instability and improvement in physician-assessed outcome measurements. In the transition toward a patient-centered health care system, patient-reported outcomes measures (PROMs) have become increasingly important because they directly correlate with patient satisfaction and experience after surgery. Of all the shoulder-specific PROMs, the Rowe and the Athletic Shoulder Outcome Scoring System (ASOSS) are among the most common PROMs used for evaluating patients for shoulder instability. 3 Despite this, these traditional scales are generally measured in a continuous manner, aiming for a statistically significant difference, which makes it difficult to interpret their results in terms of objective clinical significance.
To adequately interpret PROMs for clinical use, the concepts of the minimal clinically important difference (MCID) and the patient acceptable symptom state (PASS) have been described. The MCID represents the smallest change between 2 scores that can be perceived as meaningful by patients, while the PASS is defined as the higher level of recovery beyond which the patients consider themselves well, and can be used to infer a satisfactory outcome.20,27,28,40 Previous studies have defined MCID values for the Rowe score, the Western Ontario Shoulder Instability Index, and the Oxford Shoulder Instability Score after ABR.11,29 Despite this, no studies have attempted to identify MCID values for the ASOSS score or PASS thresholds for the Rowe and ASOSS scores, which are 2 frequently used scores in glenohumeral instability research. 3
The MCID and PASS thresholds have demonstrated marked variation based on patient characteristics, type of intervention, preoperative diagnosis, and method of estimation, which may result in over- or underestimation of failure to improve. 36 However, contemporary literature lacks analyses estimating these thresholds while accounting for the modifying or confounding effect of patient characteristics after ABR.11,29 A better understanding of these metrics may help surgeons use directly targeted evidence-based methods for evaluating patient improvement and guiding clinical decisions.
Therefore, this study aimed to determine the MCID and PASS thresholds at 1 year for the Rowe and ASOSS scores after ABR and to determine the effect of patient characteristics on these metrics after ABR. We hypothesized that our study would successfully identify the MCID and PASS thresholds for the mentioned PROMs and that these values would exhibit great variability based on specific patient characteristics.
Methods
Study Population
A retrospective study was made of consecutive ABR procedures performed between January 2017 and January 2020 at a single academic institution. The study protocol was approved by the local ethics committee of our institution (institutional review board: 00010193), and all patients provided written informed consent to participate in this study. The inclusion criteria were as follows: anterior shoulder instability; at least 1 episode of instability—defined as a dislocation with spontaneous reduction or a complete dislocation requiring a reduction; and a minimum follow-up of 12 months. The exclusion criteria were as follows: bony defects of >20% on the anteroinferior portion of the glenoid based on preoperative computed tomography scan 7 ; engaging Hill-Sachs lesions at 90° of abduction and 90° of external rotation based on an arthroscopic examination 6 ; previous surgery on the same shoulder; multidirectional instability or concomitant repair of full-thickness rotator cuff tears; superior labral anterior to posterior (SLAP) lesions; posterior labral tears; or humeral avulsion of the glenohumeral ligament lesions.
Patient Evaluation
The Rowe score was used as a global outcome measure of the glenohumeral joint status, including range of motion, pain, and apprehension, while the ASOSS was used to measure shoulder-dependent sports ability, including performance during return to sports activity and the ability to compete at the same level.34,35 PROMs were collected both preoperatively and 1-year postoperatively for analysis. Delta was defined as the change between preoperative and 1-year postoperative scores. We classified competitive athletes according to a study by Araújo and Scharhag 4 (regular sports with competitions and practices at least 2 times a week).
Surgical Technique and Rehabilitation Protocol
All ABRs were performed by 3 different surgeons (L.A.R., I.T., M.R.) with the patient in the lateral decubitus position with use of combined general endotracheal and regional anesthesia. Labral repairs were performedas with suture anchors with nonabsorbable sutures using sliding knots. No patients in this series underwent concomitant posterior-inferior capsulolabral repair, rotator interval closure, SLAP repair, or remplissage. Postoperatively, all patients followed a standardized postoperative physical therapy and rehabilitation program. Finally, return to sports was authorized when the patients were pain-free without apprehension, full shoulder range of motion had been achieved, and shoulder strength was similar to that before the injury.
Statistical Analysis
Continuous variables are presented as means ± standard deviations or medians and interquartile range according to distribution, and categorical variables are presented as absolute and relative frequencies. The MCID was then estimated to reflect the minimum PROMs improvement that translates into a patient-perceived change in their health status. The MCID was calculated through distribution-based methods.5,12,31 In line with previous studies in the literature, the MCID was determined using a distribution-based method of one-half the standard deviation of the difference between preoperative and postoperative outcome scores.5,12,19,21 PASS values represented thresholds that indicate optimal patient satisfaction and were estimated using an anchor-based approach, which corresponds to a response to a question at 1 year (“Taking into account all the activity you have during your daily life, your level of pain, and also your activity limitations and participation restrictions, do you consider the current state of your shoulder satisfactory?”). 33 To determine the cutoff points, receiver operating characteristic curve analyses were conducted independently for each PROM in relation to the binary satisfaction variable and the 1-year PROM scores. This was used to determine the thresholds that best discriminated between patients who achieved satisfaction and those who did not. This was accomplished by identifying the threshold value where sensitivity and specificity were maximized.8,17,18 Statistical analyses were performed using Stata Version 17 (Stata Corp). P < .05 was considered statistically significant.
Results
Study Population
A total of 225 patients required arthroscopic stabilization after an instability event during the study period. Of these, 20 patients did not meet the study criteria, and 15 were lost to follow-up. Thus, complete follow-up was available in 190/205 patients (92.6%) (Figure 1). Overall, 88% of patients (n = 167) had a satisfactory response to the anchored question. Further baseline patient characteristics are detailed in Table 1.
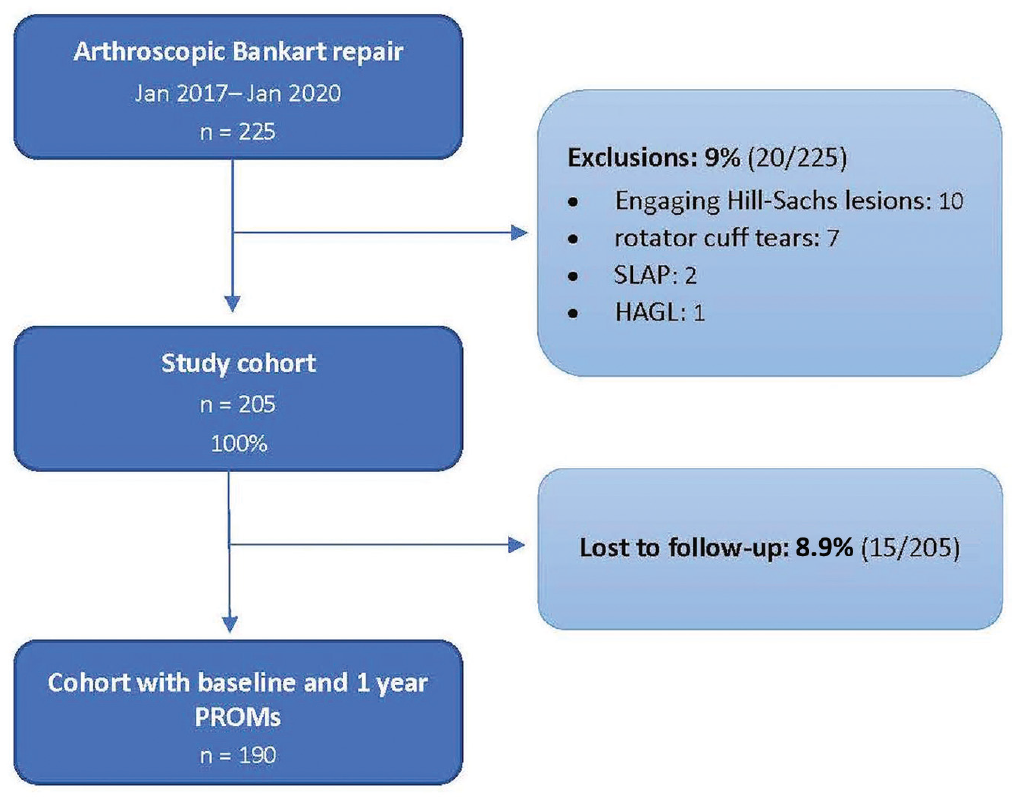
STROBE diagram representing the flow of patients within the study. HAGL, humeral avulsion glenohumeral ligament; SLAP, superior labral anterior to posterior; STROBE, Strengthening the Reporting of Observational studies in Epidemiology.
Baseline Characteristics of the Study Population a
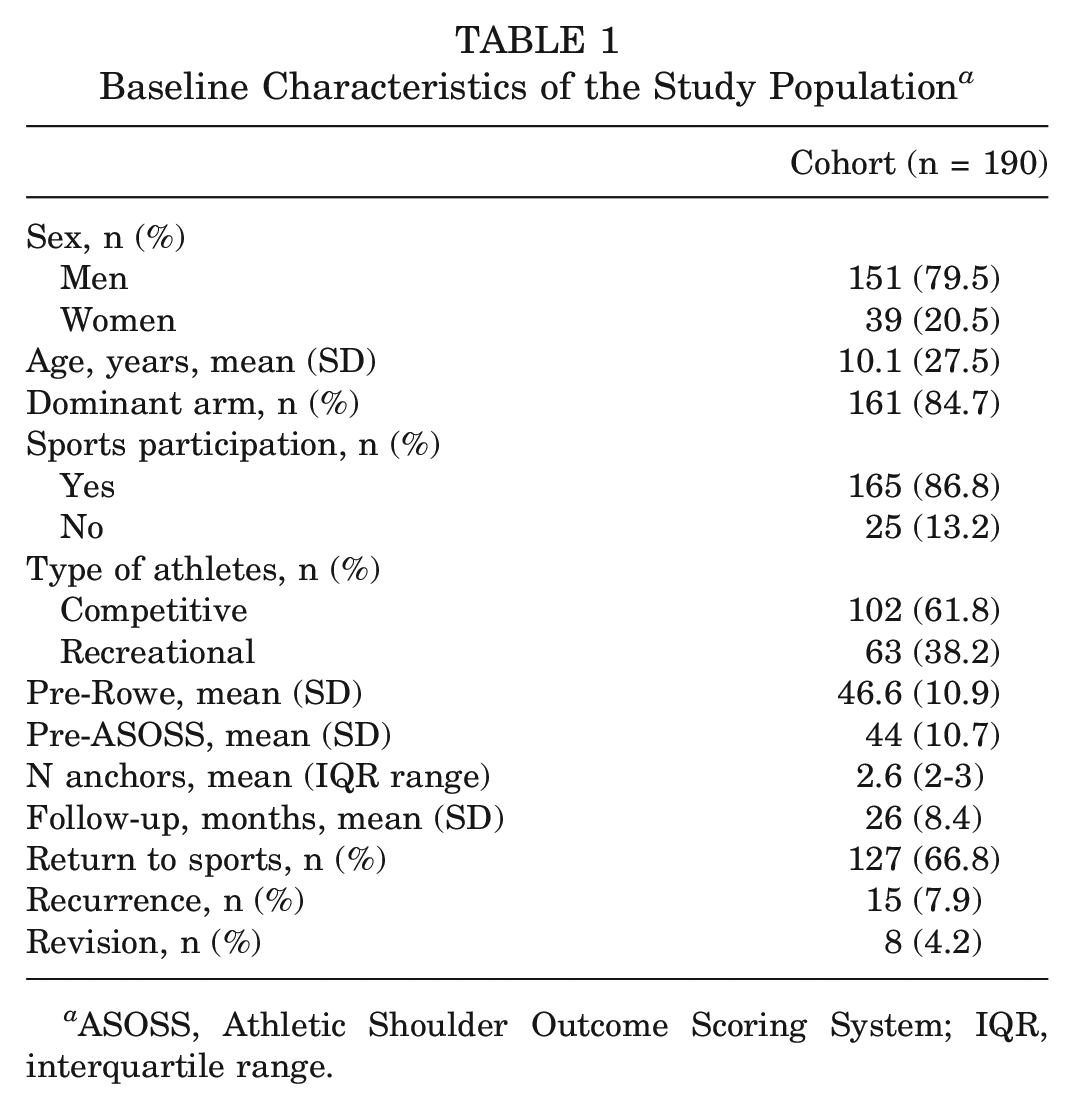
ASOSS, Athletic Shoulder Outcome Scoring System; IQR, interquartile range.
Study Population, Patient-Reported Outcomes, MCID, and PASS Thresholds
Postoperative functional outcomes were significantly improved compared with the baseline (P < .001) (Table 2).
Postoperative Clinical Outcomes After ABR a
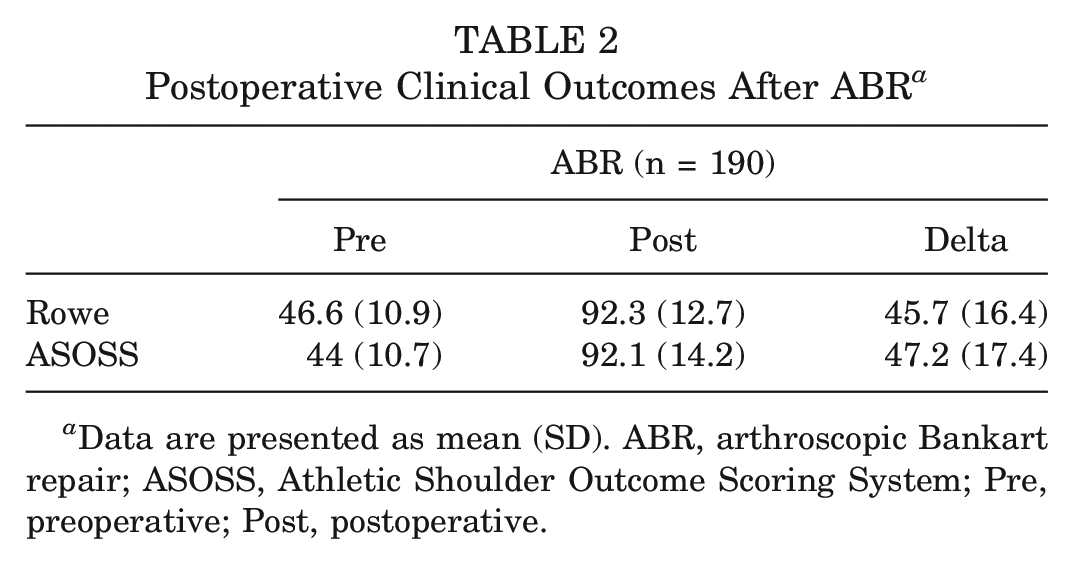
Data are presented as mean (SD). ABR, arthroscopic Bankart repair; ASOSS, Athletic Shoulder Outcome Scoring System; Pre, preoperative; Post, postoperative.
The MCID for the Rowe was 8.2, with 96% of patients achieving this MCID (Table 3). The PASS threshold was ≥80 (area under the curve [AUC], 0.93 [CI, 0.83-0.97]; sensitivity, 95%; specificity, 82%) and was achieved by 86% of the cohort (Figure 2).
Study Population Cutoff Values for the Rowe and ASOSS Scores a
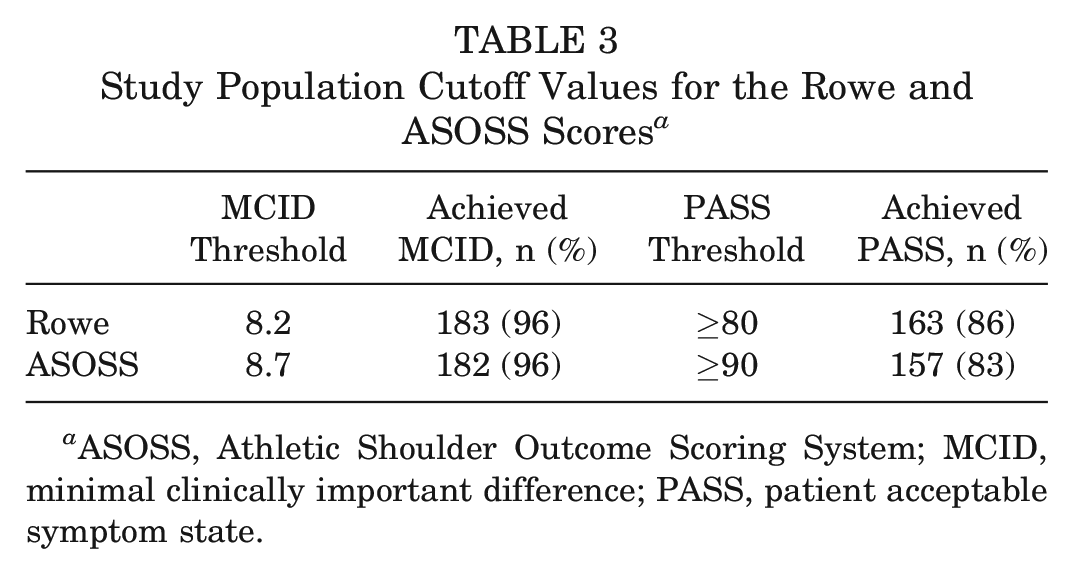
ASOSS, Athletic Shoulder Outcome Scoring System; MCID, minimal clinically important difference; PASS, patient acceptable symptom state.
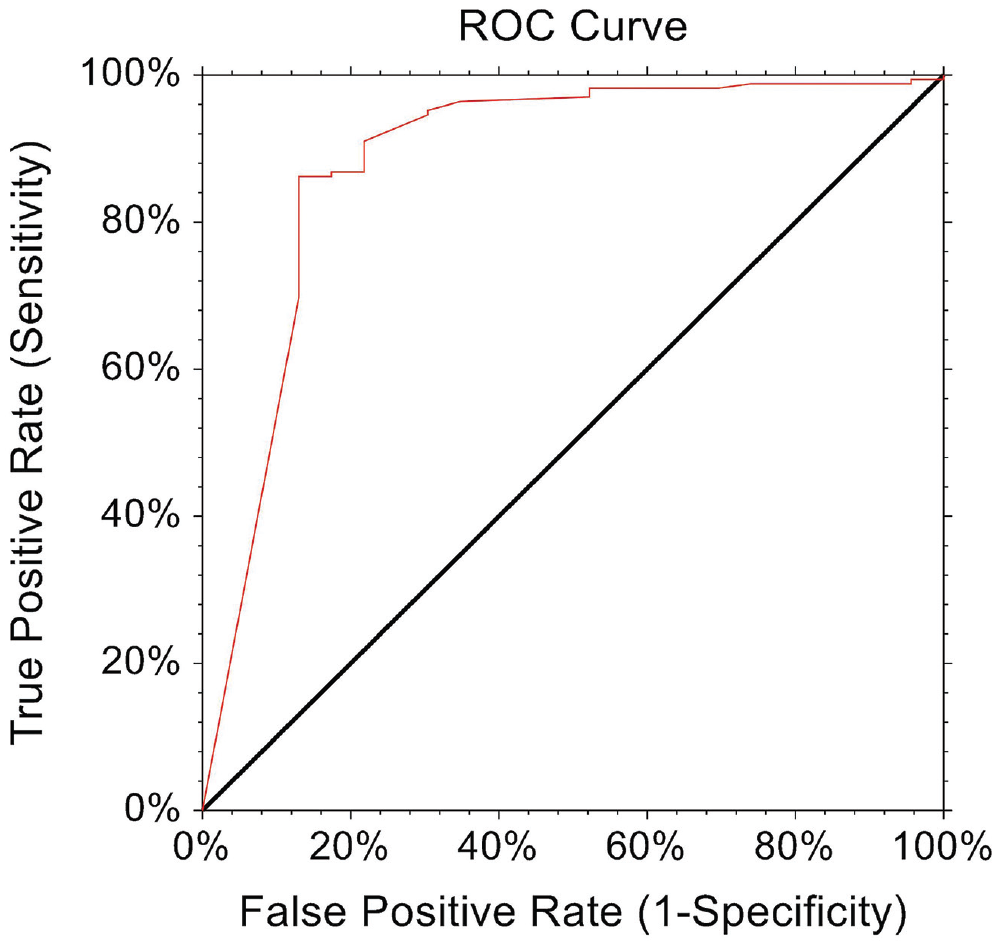
ROC curve analysis for the Rowe score threshold value for 1 year of the PASS. PASS, patient acceptable symptom state; ROC, receiver operating characteristic.
The MCID for the ASOSS was 8.7, with 96% of patients achieving this MCID (Table 3). The PASS threshold was ≥90 (AUC, 0.88 [CI 0.75-0.94]; sensitivity, 86%; specificity, 86%) and was achieved by 83% of the cohort (Figure 3).
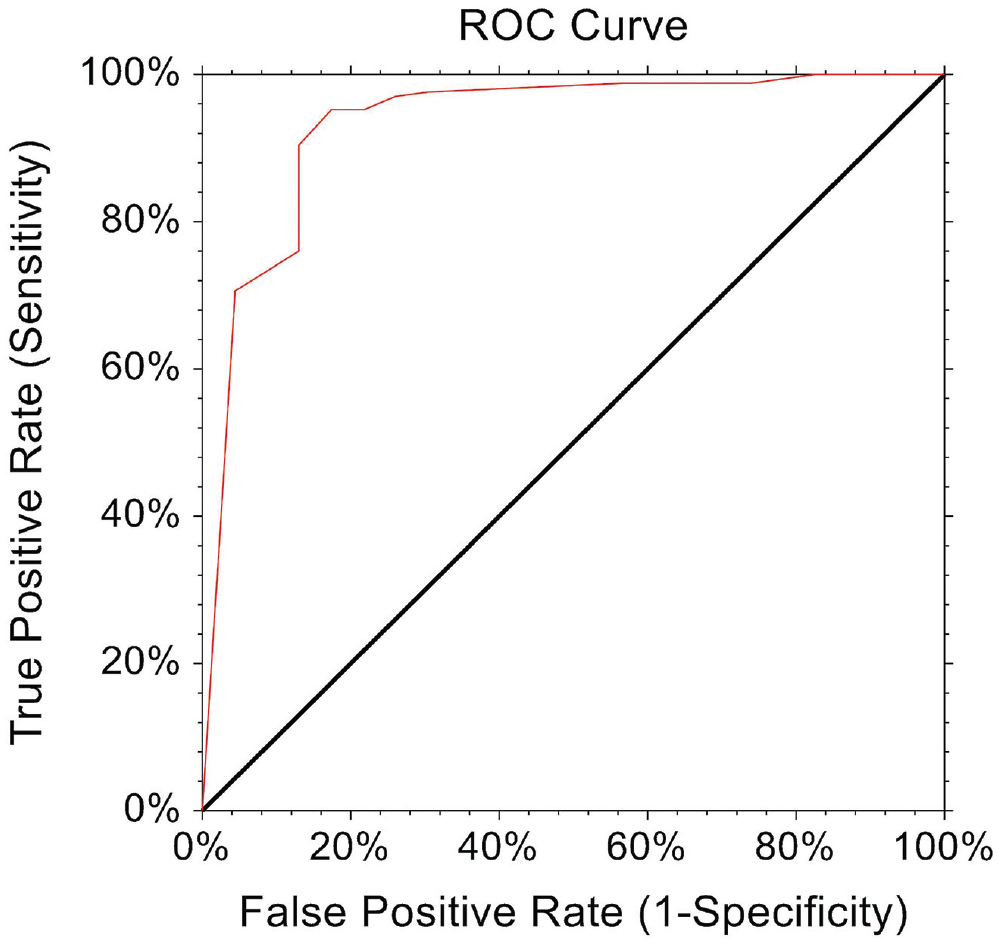
ROC curve analysis for the ASOSS score threshold value for 1 year PASS. ASOSS, Athletic Shoulder Outcome Scoring System; PASS, patient acceptable symptom state; ROC, receiver operating characteristic.
MCID and PASS Thresholds Stratified by Age and Sex
There were differences in the MCID and PASS thresholds when stratified by age, with patients ≥21 years showing slightly higher values. Male patients also demonstrated higher MCID and PASS thresholds compared with female patients. Table 4 presents the MCID and PASS thresholds for each metric stratified according to age and sex.
MCID and PASS Stratified According to Age and Sex a
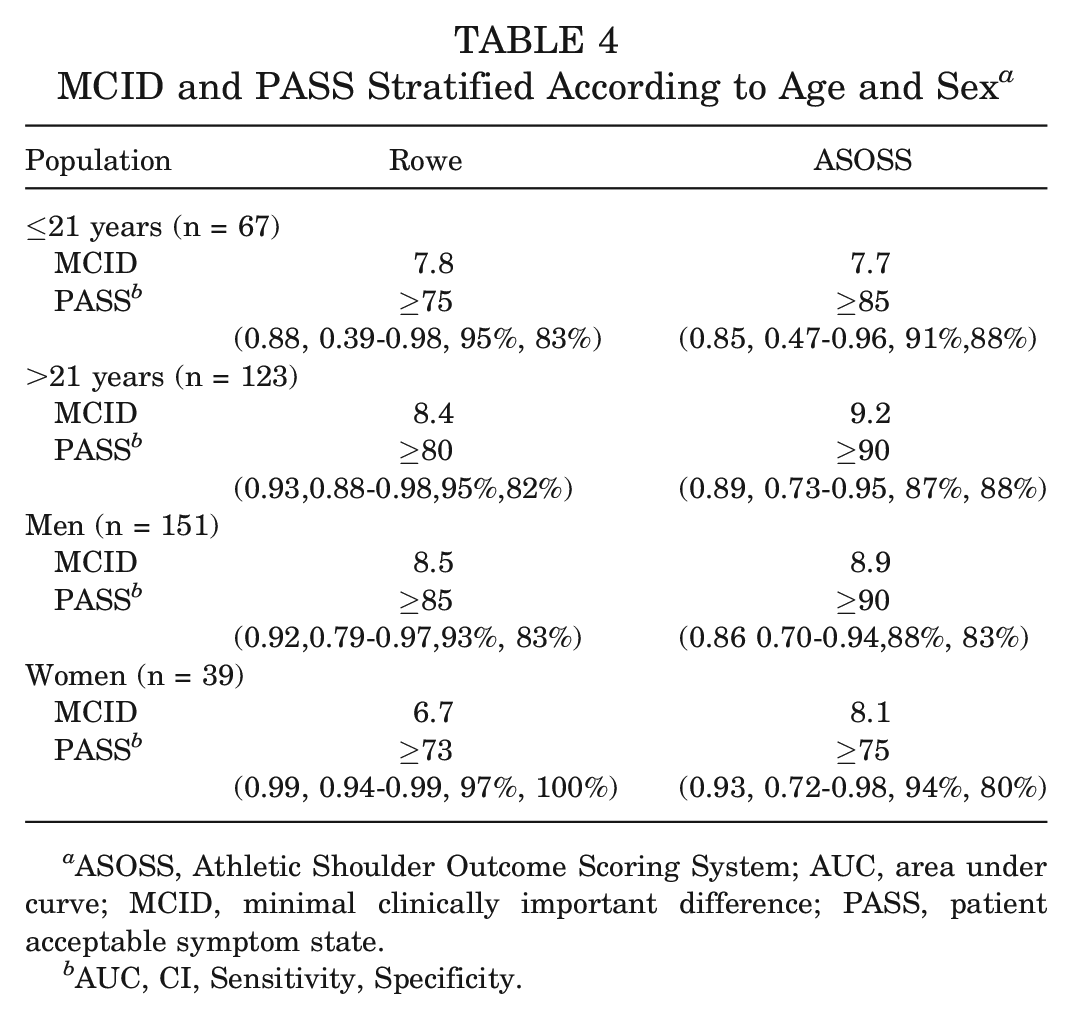
ASOSS, Athletic Shoulder Outcome Scoring System; AUC, area under curve; MCID, minimal clinically important difference; PASS, patient acceptable symptom state.
AUC, CI, Sensitivity, Specificity.
MCID and PASS Thresholds Stratified by Sports Participation and Type of Athlete
Sports participation and competitive athletes have shown higher MCID and PASS thresholds when compared with no sports participation and recreational athletes. Table 5 presents MCID and PASS thresholds for each metric stratified according to sports participation and type of athlete.
MCID and PASS Stratified According to Sports Participation and Type of Athlete a
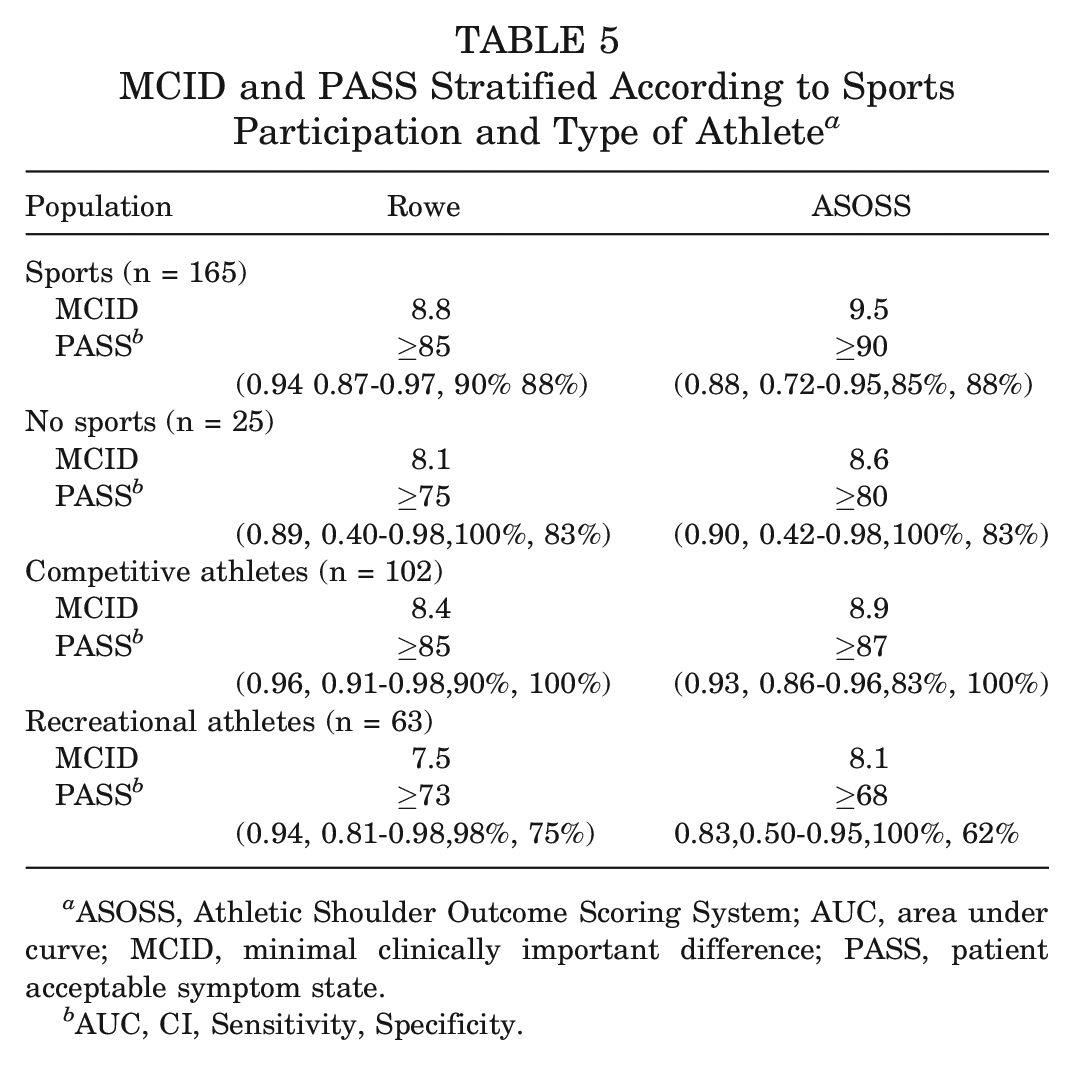
ASOSS, Athletic Shoulder Outcome Scoring System; AUC, area under curve; MCID, minimal clinically important difference; PASS, patient acceptable symptom state.
AUC, CI, Sensitivity, Specificity.
Discussion
The most important finding of the present study was that it identified MCID and PASS thresholds for the Rowe and ASOSS scores 1 year after ABR. However, these values showed great variability when accounting for different patient characteristics. Using these population-based values will enable future studies to accurately evaluate the clinical outcomes after ABR and determine whether patients have achieved clinically satisfactory outcomes. In patients with glenohumeral instability, ABR has been associated with excellent functional outcomes, offering an effective alternative to other shoulder stabilization techniques.10,24 This study reports MCID and PASS thresholds for the Rowe and ASOSS scores in patients undergoing ABR. As many orthopaedic surgeons administer these scores for patient evaluation, these findings may provide context for evaluating the patient perception of success after surgery.
The alignment of PROMs with patient-centered metrics has been an ongoing process for the past few years. Previous work has detailed the MCID and PASS metrics for multiple different PROMs after shoulder arthroplasty, rotator cuff repair, and bicep tenodesis.14,15,25,32,36,37 However, only a few studies have established these metrics after shoulder instability surgery.11,25,36 Foong et al 11 established an MCID threshold of 8.6 for the Oxford Shoulder Instability score, while Park et al 29 determined a 9.7 MCID value for the Rowe score and 151.9 for the Western Ontario Shoulder Instability Index after ABR, using a distribution-based method. Similarly, we found an MCID threshold of 8.2 for the Rowe score, with 96% of patients achieving success. However, to our knowledge, our study is the first to describe the MCID for an ASOSS score of 8.7, with 95% of patients achieving success. This high rate of patients achieving MCID thresholds was expected based on the low MCID threshold and the fact that most of our patients improved significantly in terms of stability, function, motion, and strength compared with the baseline.
With the advent of value-based care, clinicians need to ensure that patients not only “feel better” (MCID concept) but also “feel good” after surgery (PASS concept).13,39 A metric such as the PASS, which targets a final health state acceptable to the patient after treatment rather than a change in score before to after treatment, may be more appropriate for this situation. However, there are no PASS thresholds reported in the current literature after ABR. We specifically found thresholds of ≥80 and ≥90 for the Rowe and ASOSS scores, with 86% and 83% of patients achieving success, respectively. The value of defining PASS thresholds for these scores is that they can facilitate the interpretation of these commonly used PROMs when evaluating the satisfaction of individual patients after ABR. As a result, the focus is kept on patient-centered outcomes rather than statistical significance.
Even though the PASS and MCID values are of great value, 1 reported limitation is that they have shown significant variability among PROM scores.22,23,26 Several factors may explain this variability, including the use of different terminology, multiple methods to calculate MCID, the presence of heterogeneous characteristics, disease severity, baseline PROMs, and time-point analysis of the study population.23,26 For instance, Park et al 29 calculated MCID values for the Rowe score using anchored- and distribution-based methods, finding a 4-point difference with higher values in the former. In another study, Park et al 30 found that factors such as body mass index, number of dislocations, symptom duration, and Hill-Sachs lesions were correlated with the MCID values for the Rowe and ASES scores after arthroscopic stabilization surgery. This highlights the importance of considering baseline patient factors when interpreting MCID values. Therefore, threshold variability poses a clinical dilemma, given that using higher cutoffs to evaluate patient improvement may lead to an increase in the number of patients whose outcomes are designated as “treatment failures.” 9 In contrast, implementing lower thresholds may exaggerate rates of attaining higher levels of functional improvement. 9 Consequently, it is important to exercise extreme caution when applying a previously established threshold for a specific intervention. 23 There has been no attempt to calculate MCID and PASS thresholds after ABR, although existing evidence indicates the influence of many factors on these values. Therefore, it is essential to determine these values after taking into account baseline patient characteristics.
Our stratification of MCID and PASS results according to age, sex, sports participation, and type of athlete revealed some noteworthy findings. Indeed, male sex, age ≥21 years, sports participation, and competitive athletes required higher MCID and PASS thresholds to achieve success compared with female sex, age ≤21 years, no sports participation, and noncompetitive athletes. We hypothesized that this might result from underlying differences in expectations among these different patient populations. For instance, a competitive athlete may expect to return to competitive high-performance level. Therefore, achieving success for this specific patient will require higher functional outcome scores compared with a noncompetitive athlete or a patient who does not play any sports and who may be expecting to return to their nondemanding sport or daily activity levels, which will require lower functional outcome scores. Therefore, to put our findings into context, if we use our general study population thresholds for determining success, we may be overestimating treatment failures for some of those populations who require lower thresholds for success. Therefore, if the MCID and PASS values are different for each population in each situation, it may not be possible at all to define 1 value, and instead a range of values should be used for a measurement instrument. 38 Future studies are encouraged to implement these population-based values in their populations. In the current trend toward a more patient-centered health care system, considering patient characteristics for measuring these metrics could significantly contribute to improving the accuracy of patient assessment.
Limitations
There are several limitations to the present study that should be considered. We only used a distribution-based method of calculating the MCID without implementing an anchor-based comparison.9,19,21 There has not been a standardized approach to patient satisfaction in the literature, as some studies have used dichotomous anchor questions. In contrast, others have used a Likert scale with different ranges of options. 16 Another factor to consider is the time period at which the MCID and the PASS are measured because patient satisfaction and expectations may not remain constant over time after ABR. Last, we only described threshold values for 2 of many PROMs used to evaluate shoulder instability surgery outcomes. 41 The decision to include these scores is because the MCID and the PASS have not been previously described for these scores after Bankart repair and because they are widely used in the literature related to glenohumeral instability.
Conclusion
This study identified the MCID and PASS thresholds for the Rowe and ASOSS scores at 1 year after ABR. However, these values showed great variability when accounting for patient characteristics such as sex, age, sports participation, and type of athlete. The wide variability in MCID and PASS values based on patient characteristics underscores the necessity of caution and the adoption of a patient-centered approach when interpreting outcome measures after ABR, highlighting the importance of considering individual patient-specific characteristics for optimal treatment decision-making and ensuring treatment success tailored to each patient’s unique needs and expectations.
Footnotes
Submitted April 4, 2023; accepted September 6, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.