
Abstract
Background:
Hip arthroscopy has become the mainstay surgical intervention for the treatment of femoroacetabular impingement syndrome (FAIS). However, postoperative outcomes and rates of secondary surgery are mixed in patients with differing levels of preoperative osteoarthritis (OA). Furthermore, there is a paucity of literature comparing patients with and without OA at long-term follow-up.
Purpose:
To compare outcomes and rates of secondary surgery at minimum 10-year follow-up, including revision hip arthroscopy and conversion to total hip arthroplasty (THA), in patients with Tönnis grade 1 undergoing hip arthroscopy for FAIS compared with a propensity-matched control group of patients with Tönnis grade 0.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent primary hip arthroscopy for FAIS between January 2012 and February 2013 were identified. Patients with Tönnis grade 1 were propensity matched in a 1:2 ratio by age, sex, and body mass index (BMI) to patients with Tönnis grade 0. Patient-reported outcomes (PROs) were collected at varying timepoints including preoperatively and 1, 2, 5, and 10 years postoperatively and compared between the 2 cohorts. Rates of minimal clinically important difference (MCID) and Patient Acceptable Symptom State (PASS) achievement at 10 years were evaluated and compared between groups. Rates of secondary surgery including revision hip arthroscopy and conversion to total hip arthroplasty (THA) were evaluated. Gross survivorship between cohorts was evaluated using a Kaplan-Meier gross survivorship curve. A subanalysis was performed comparing patients with Tönnis grade 1 who converted to THA and those who did not.
Results:
A total of 31 patients with Tönnis grade 1 (age, 42.6 ± 9.0 years; BMI, 28.0 ± 6.3) were successfully matched to 62 patients with Tönnis grade 0 (age, 42.1 ± 8.5, P = .805; BMI, 26.1 ± 3.9, P = .117). Both the Tönnis grade 1 and Tönnis grade 0 groups demonstrated significant improvements regarding all PROs at minimum 10 years (P < .05 for all), except for the Hip Outcome Score Activities of Daily Living subscale (HOS-ADL) (P = .066) in the Tönnis grade 1 cohort. No significant difference (P > .05 for all) was noted between cohorts regarding any 10-year PRO. When the authors evaluated comparisons between preoperative and 1-, 2-, 5-, and 10-year PRO measures, significant differences were noted between cohorts regarding 2-year HOS-ADL (P = .021), Hip Outcome Score Sports-Specific subscale (P = .016), and modified Harris Hip Score (P = .026); otherwise, differences did not reach significance. High rates of 10-year MCID and PASS achievement were seen, with no significant differences between groups. Patients with Tönnis grade 1 had significantly higher rates of conversion to THA compared with patients who had Tönnis grade 0 (25.8% vs 4.8%; P = .006). Patients with Tönnis grade 1 had significantly lower gross survivorship compared with those who had Tönnis grade 0 (71.0% vs 85.5%, respectively; P = .04).
Conclusion:
Hip arthroscopy confers comparable postoperative clinical improvements to patients who have FAIS with and without mild OA; however, the benefits among patients with mild OA may be less durable. Patients with Tönnis grade 1 had significantly higher conversion to THA and reduced gross survivorship compared with patients with no evidence of preoperative OA, suggesting that patients with evidence of OA may need to be cautioned on the higher rate of conversion surgery.
Hip arthroscopy has been shown to be an effective treatment option for femoroacetabular impingement syndrome (FAIS), with high rates of patient satisfaction and significant improvements in pain and function postoperatively1,15,26,35,40,47,50,62 as well as high rates of return to sport in athletes.12,13,52 However, not all patients achieve the same outcomes after hip arthroscopy, and preexisting factors, such as degree of preoperative osteoarthritis (OA), may play a role in these variations. 29 Tönnis grade is a common radiographic measure of hip joint degeneration that ranges from 0 to 3.3,7,14,31,46 Although hip arthroscopy is not typically performed in patients with Tönnis grade >1 (indicative of moderate to severe OA), the effect of early-stage OA on outcomes is less clear. 60
Patients with moderate to severe OA (Tönnis grade >1) have consistently been shown to have inferior outcomes after hip arthroscopy compared with those who have no or mild OA.10,18,53,57 Conversely, studies evaluating patients with only mild OA (Tönnis grade 1) have not shown the same extent of reduced clinical outcomes as has been reported in patients with more advanced OA.11,16,17 Importantly, existing investigations into the effect of Tönnis grade 1 OA on hip arthroscopy are limited to short-term and midterm follow-up.10,11,16,17,53,57 Because differences in outcome scores and rates of revision hip arthroscopy and/or conversion to total hip arthroplasty (THA) may not become apparent until long-term follow-up, 8 it is critical to evaluate the long-term outcomes of patients with mild OA undergoing hip arthroscopy compared with those who have no evidence of OA.
Therefore, the purpose of the present study was to compare outcomes and rates of secondary surgery at minimum 10-year follow-up, including revision hip arthroscopy and conversion to THA, in patients with Tönnis grade 1 undergoing hip arthroscopy for FAIS compared with a propensity-matched control group of patients with Tönnis grade 0. We hypothesized that patients with Tönnis grade 1 would experience worse 10-year outcomes and would have a higher rate of secondary surgery.
Methods
Patient Selection
This study received ethical approval from the local institutional review board, and no funding was received for its completion. A retrospective review of a prospectively maintained database from a single institution was conducted, analyzing clinical outcomes of patients who underwent primary hip arthroscopy by the senior author (S.J.N.) between January 1, 2012, and February 27, 2013. All patients included in the study provided their consent to participate in the hip arthroscopy repository. Inclusion criteria were as follows: (1) symptomatic FAIS (ie, hip pain lasting >3 months, positive anterior impingement test during physical examination) and radiographic evidence of cam deformity (90° Dunn radiograph with alpha angle >55°2,23) or pincer deformity (anteroposterior radiograph evaluation with lateral center edge angle >40°, presence of crossover sign, acetabular index <0° 56 ); (2) minimum 10-year follow-up with completion of at least 1 patient-reported outcome (PRO) in the database; and (3) failure of preoperative nonoperative treatment (ie, oral anti-inflammatory medications, physical therapy, activity modification, and/or intra-articular corticosteroid injection).
Exclusion criteria were as follows: (1) Tönnis grade >1 (ie, grades 2 and 3); (2) concomitant hip procedure (eg, microfracture, gluteus medius/minimus repair, psoas lengthening, trochanteric bursectomy); (3) index surgery was a revision hip arthroscopy with our practice; (4) history of developmental hip disorders (eg, slipped capital femoral epiphysis or Legg-Calvé-Perthes disease); and (5) hip dysplasia defined by lateral center edge angle <18°. 19
A total of 298 patients were assessed for eligibility. Of these, 247 were eligible after exclusion criteria. In total, 40 patients had Tönnis grade 1, of whom 31 patients (77.5%) completed at least 1 PRO at an average of 10-year follow-up or reached an endpoint of conversion to THA or revision hip arthroscopy and were included in final analyses. These 31 patients were then propensity matched in a 1:2 ratio by age, sex, and body mass index (BMI) to 62 patients without signs of OA (Tönnis grade 0) (Figure 1).
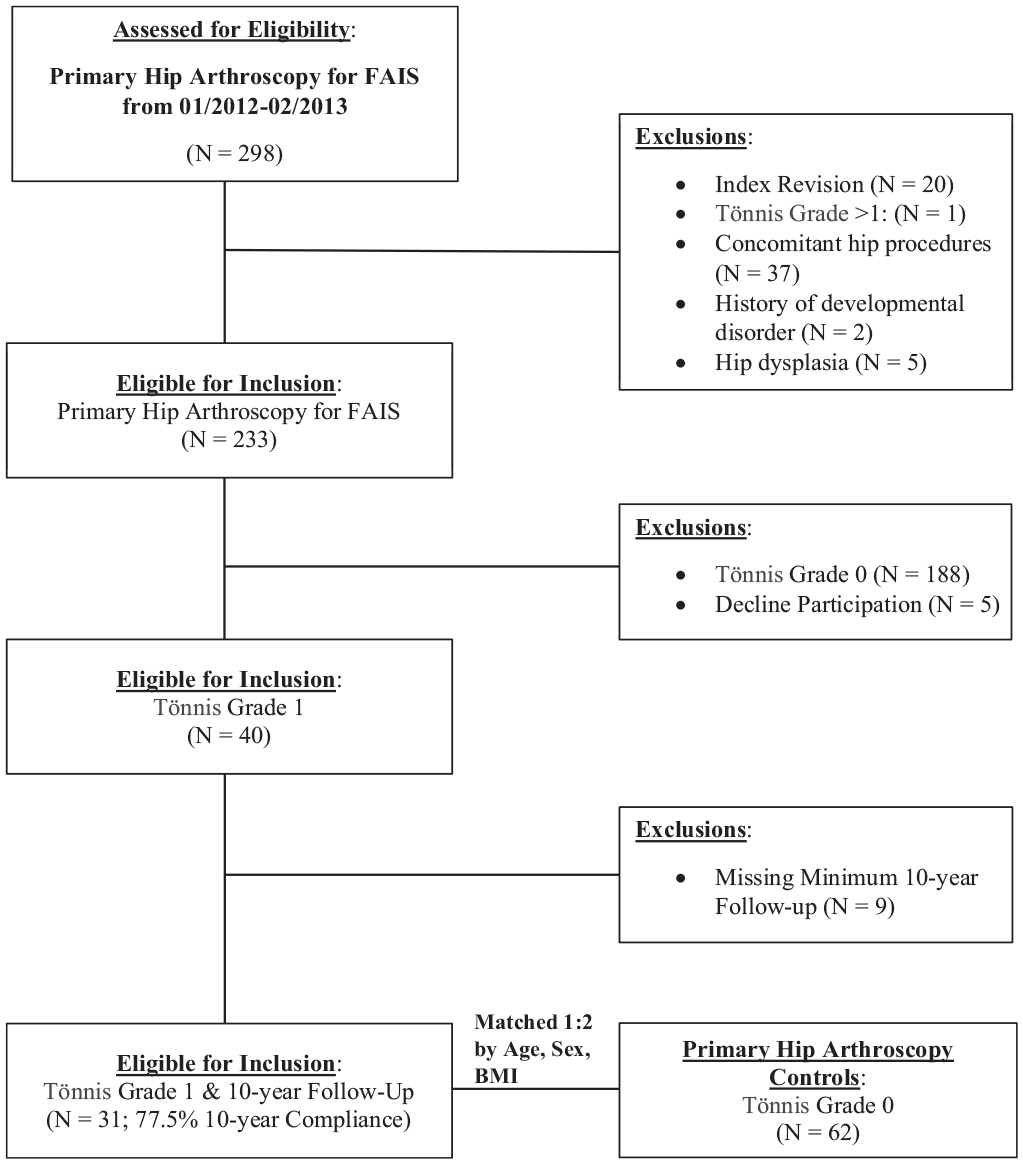
CONSORT (Consolidated Standards of Reporting Trials) diagram of patient selection methods. FAIS, femoroacetabular impingement syndrome.
Preoperative Radiographic Parameters and Evaluation of Hip OA
Patients had a standard hip series of radiographs taken preoperatively and at their initial postoperative clinic visit, including standing anteroposterior view, false-profile view, and Dunn lateral view at 90° of hip flexion. The alpha angle was measured by conventional technique on the Dunn lateral radiograph49,59; the lateral center edge angle 61 and Tönnis angle 17 were measured on the anteroposterior radiograph of the affected hip.
Using a standard series of hip radiographs, including anteroposterior, false-profile, and Dunn lateral views, we used the Tönnis classification system to evaluate for evidence of hip OA as previously described.31,36 Tönnis grade 0 was defined as no evidence of OA, and Tönnis grade 1 was defined as slight narrowing of the joint space, slight lipping of osteophytes, or slight sclerosis of the femoral head or acetabulum (Figure 2).7,31,37 All radiographs were graded by an orthopaedic surgeon who specializes in hip arthroscopy (S.J.N.).
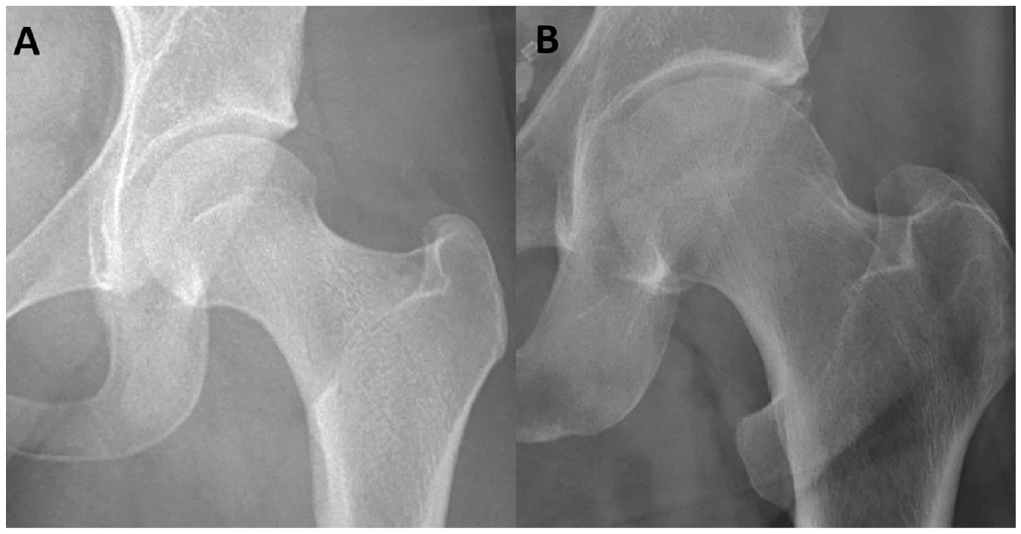
Preoperative anteroposterior radiographs demonstrating left hips with (A) Tönnis grade 0 and (B) Tönnis grade 1 osteoarthritis.
Preoperative Patient Characteristics
The patients’ preoperative baseline characteristics were collected in a secure, prospectively maintained repository. The baseline characteristics recorded included age, sex, and BMI. Additional preoperative characteristics documented included duration of symptoms, smoking status, self reported physical activity status, workers’ compensation status, and psychiatric history. We also collected intraoperative findings, including type of procedure, number of anchors, and presence of acetabular cartilage damage (intraoperative Beck classification)4,5,47 and femoral head cartilage damage (intraoperative International Cartilage Regeneration & Joint Preservation Society [ICRS] classification).2,43,45 Finally, postoperative complications, such as infection, neuropathy, and deep vein thrombosis, were recorded.
Surgical Technique
All surgical procedures were performed by the senior author, using a previously described technique.25,58 In summary, patients received general endotracheal anesthesia, were placed in a modified supine position, and were placed in traction with a well-padded perineal post. The anterolateral and modified midanterior portals were established, and the 2 portals were connected with an arthroscopic scalpel to create the interportal (transverse) portion of the capsulotomy. A cuff of capsular tissue was reserved on the acetabular and femoral sides for later capsular plication or repair. Established techniques were used to address any central femoroacetabular compartment pathology, including pincer morphology and labral tear repair. In cases where labral repair was needed, a distal accessory anterolateral portal was established.25,58 Once central compartment work was complete, traction was released.
Next, the surgeon performed a T-type capsulotomy by extending the interportal capsulotomy inferiorly to the longitudinal limb, providing access to the peripheral compartment. Once in the peripheral compartment, the surgeon achieved direct visualization of the cam deformity, and if a cam deformity was present, osteochondroplasty was performed until appropriate cam resection and adequate femoral head-neck offset were achieved. A dynamic examination of the surgical leg was then carried out to confirm resolution of the cam impingement. Capsular plication and closure were performed using ultra–high molecular weight polyethylene sutures, starting at the base of the vertical portion, followed by the interportal segment. Standard postoperative care and rehabilitation were performed according to the institutional protocol that has been described previously. 41
Evaluation of Patient-Reported Outcomes
PROs were collected preoperatively and at several postoperative time points including 1, 2, 5, and 10 years postoperatively. Patients completed the surveys either during clinic visits, through telephone interviews, or via encrypted email using secure electronic data collection platforms (OBERD, PatientIQ). The following PROs were collected: Hip Outcome Score Activities of Daily Living subscale (HOS-ADL), Hip Outcome Score Sports-Specific subscale (HOS-SS), modified Harris Hip Score (mHHS), 12-item International Hip Outcome Tool (iHOT-12; beginning at 2 years postoperatively), and visual analog scale (VAS) for pain and satisfaction.
Achievement rates of clinically significant outcomes including minimal clinically important difference (MCID)27,55 and Patient Acceptable Symptom State (PASS) 30 were assessed. Using the distribution method, 48 we established cohort-specific MCID thresholds from the senior author’s large 10-year cohort registry (n = 94 patients), and patients’ individual MCID values were compared against this value to evaluate achievement. The following MCID thresholds were calculated and used: HOS-ADL, 10.4; HOS-SS, 14.6; mHHS, 8.8; VAS Pain, 14.6 (Appendix Table A1, available in the online version of this article). Cohort-specific PASS thresholds were also calculated from the large 10-year cohort, using receiver operating characteristic curve analysis with the Youden index to calculate threshold scores.24,42,51 PASS thresholds used were as follows: HOS-ADL, 85.3; HOS-SS, 60.2; mHHS, 76.0; VAS Pain, 27.5; iHOT-12, 71.4 (Appendix Table A1).
Survivorship
Patients who underwent revision hip arthroscopy or THA were also included; however, their PRO data were excluded from any analyses performed after the date of their subsequent operation. At the time of most recent follow-up, all patients were assessed for whether they had undergone a revision hip arthroscopy procedure or conversion to THA. If so, patients were asked at what postoperative timepoint they underwent the secondary procedure. Survivorship, defined as undergoing a secondary surgery including revision hip arthroscopy or conversion to THA, was calculated for both the Tönnis grade 1 and Tönnis grade 0 cohorts, and a Kaplan-Meier survivorship curve was used to compare gross survivorship between the 2 cohorts.
Data Analysis
Propensity matching was used to match patients with Tönnis grade 1 to controls on a 1:2 basis by age, sex, and BMI. Descriptive analyses were reported for preoperative patient characteristics, intraoperative and radiographic findings, and PROs. Continuous variables are reported as means and standard deviations for parametric variables, and categorical variables are presented as counts and percentages. The Shapiro-Wilk test was performed to assess for normality of PROs. Because outcomes were normally distributed, paired-samples t tests were performed to evaluate for significant preoperative to 10-year improvements, whereas independent t tests were used to assess for significant differences between groups. Pearson chi-square analysis was performed to analyze differences in groups regarding categorical variables.
A subanalysis was performed to evaluate the comparisons of preoperative patient characteristics, radiographic findings, and intraoperative findings between patients with and without conversion to THA in the Tönnis grade 1 cohort. Comparisons were limited by sample size between groups but were performed using independent-sample t tests for continuous variables and the Fisher exact test for categorical variables.
For all data analyses, statistical significance was determined by α < .05. Statistical analyses were completed using SPSS Version 28.0 (IBM), and propensity matching was completed with R 4.1.0 (R Core Team).
Results
Patient Characteristics
A total of 31 patients with Tönnis grade 1 (age, 42.6 ± 9.0 years; BMI, 28.0 ± 6.3) were successfully matched to 62 patients with Tönnis grade 0 (age, 42.1 ± 8.5 years, P = .805; BMI, 26.1 ± 3.9, P = .117) at a mean follow-up of 10.3 ± 0.3 years. Preoperative patient characteristics are summarized in Table 1.
Preoperative Patient Characteristics a
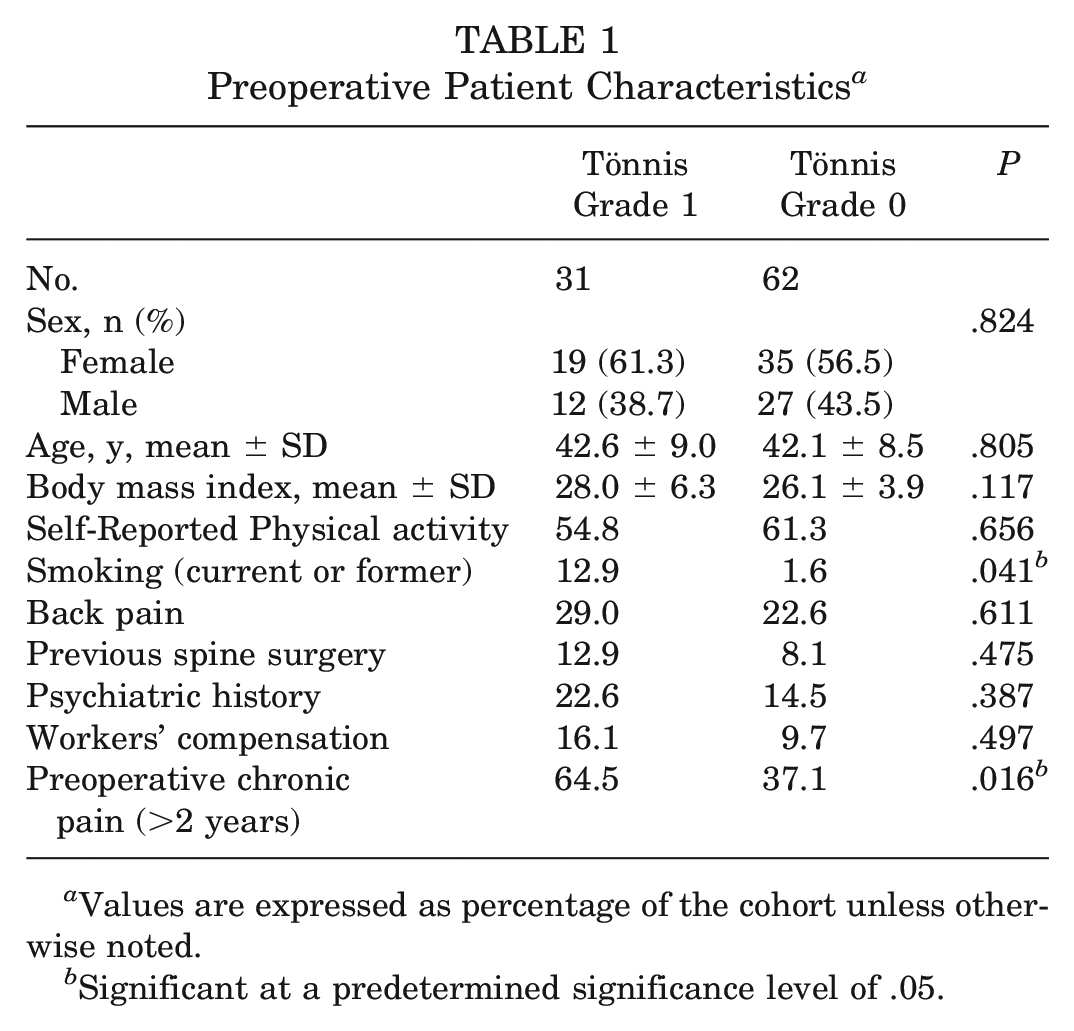
Values are expressed as percentage of the cohort unless otherwise noted.
Significant at a predetermined significance level of .05.
Of note, patients with Tönnis grade 1 had a higher rate of smoking (P = .041) and preoperative chronic pain >2 years (P = .016). Although we found no significant differences in preoperative radiographic measures between groups, patients with Tönnis grade 1 had significantly higher postoperative alpha angles (P = .011) (Table 2). Intraoperatively, patients with Tönnis grade 1 had significantly higher acetabular (P = .002) and femoral head (P = .006) ICRS grades compared with the Tönnis grade 0 cohort (Table 3).
Pre- and Postoperative Radiographic Measurements a
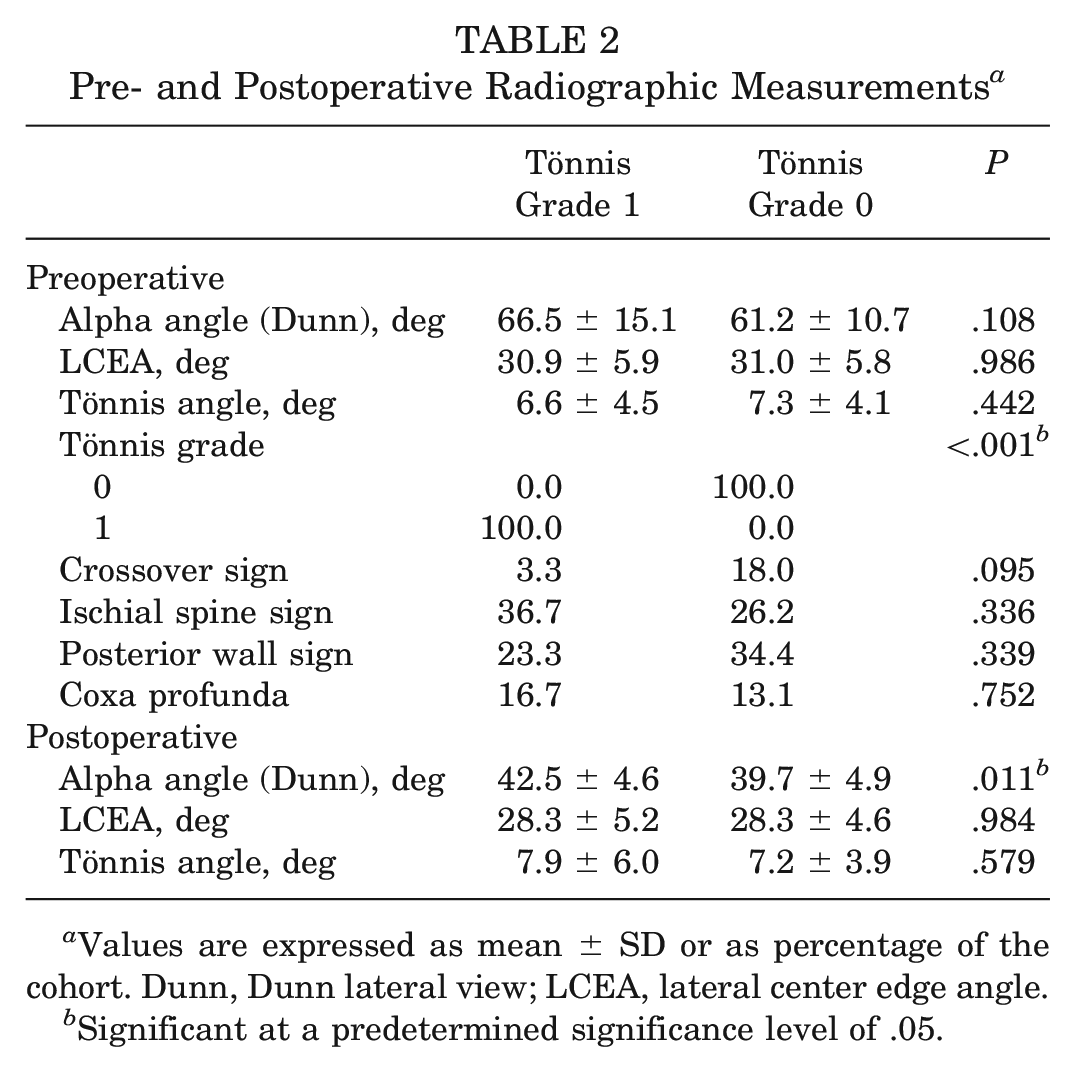
Values are expressed as mean ± SD or as percentage of the cohort. Dunn, Dunn lateral view; LCEA, lateral center edge angle.
Significant at a predetermined significance level of .05.
Intraoperative Findings and Procedures a
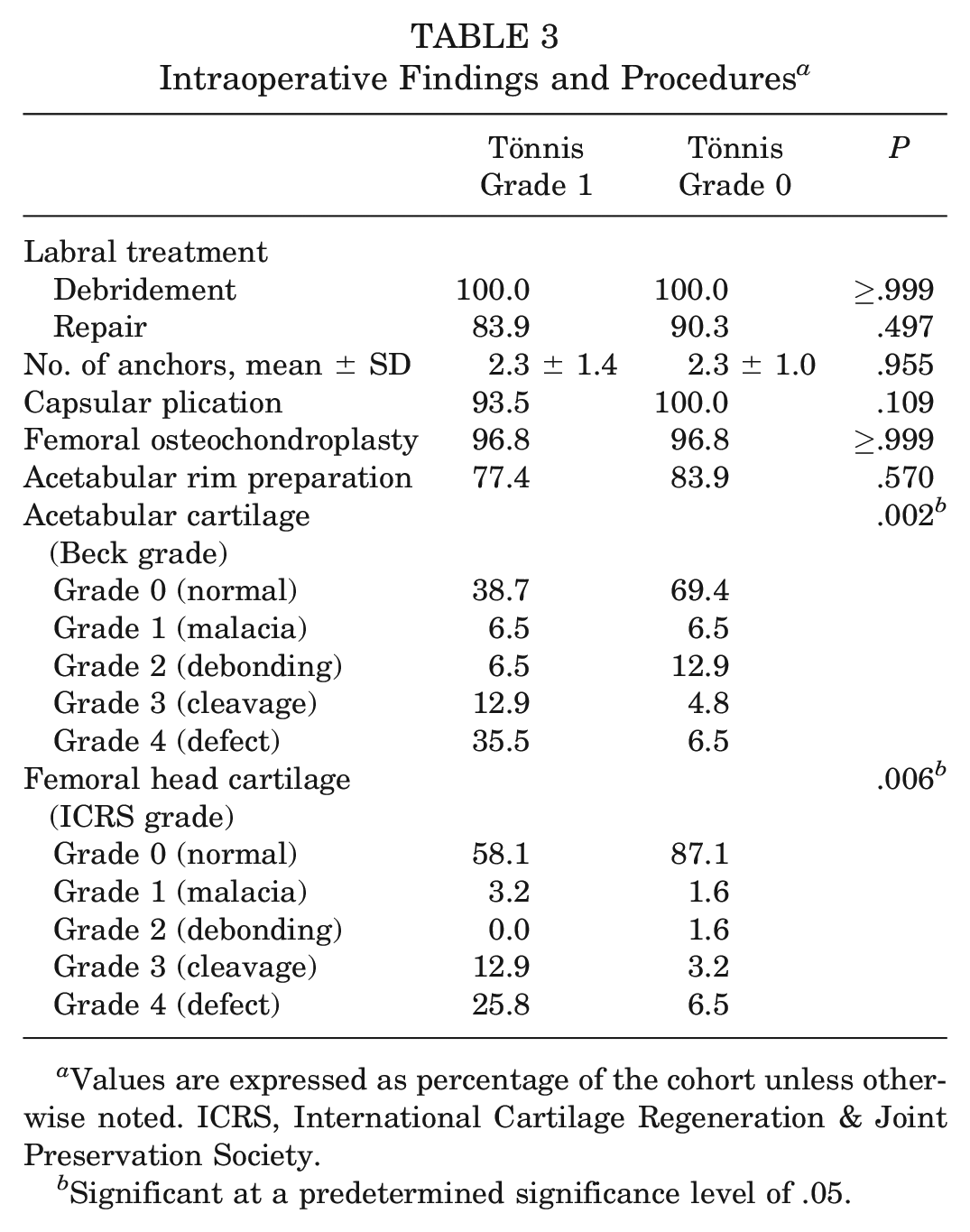
Values are expressed as percentage of the cohort unless otherwise noted. ICRS, International Cartilage Regeneration & Joint Preservation Society.
Significant at a predetermined significance level of .05.
Patient-Reported Outcomes
Both Tönnis grade 1 and Tönnis grade 0 cohorts demonstrated significant improvements preoperatively to 10 years postoperatively (P < .05 for all) regarding all PROs, except for HOS-ADL (P = .066) in the Tönnis grade 1 cohort (Table 4). No significant difference was demonstrated between cohorts regarding magnitude of preoperative to 10-year change (delta) between groups for any PRO measure (Table 4). When evaluating comparisons between preoperative, 1-, 2-, 5-, and 10-year PRO measures, we noted significant differences between cohorts regarding 2-year HOS-ADL (P = .021), HOS-SS (P = .016), and mHHS (P = .026); otherwise, differences did not reach significance (Table 5).
Comparison Between Preoperative and 10-Year Postoperative Patient-Reported Outcomes Within and Between Patients With Tönnis Grade 1 vs Grade 0 Osteoarthritis a
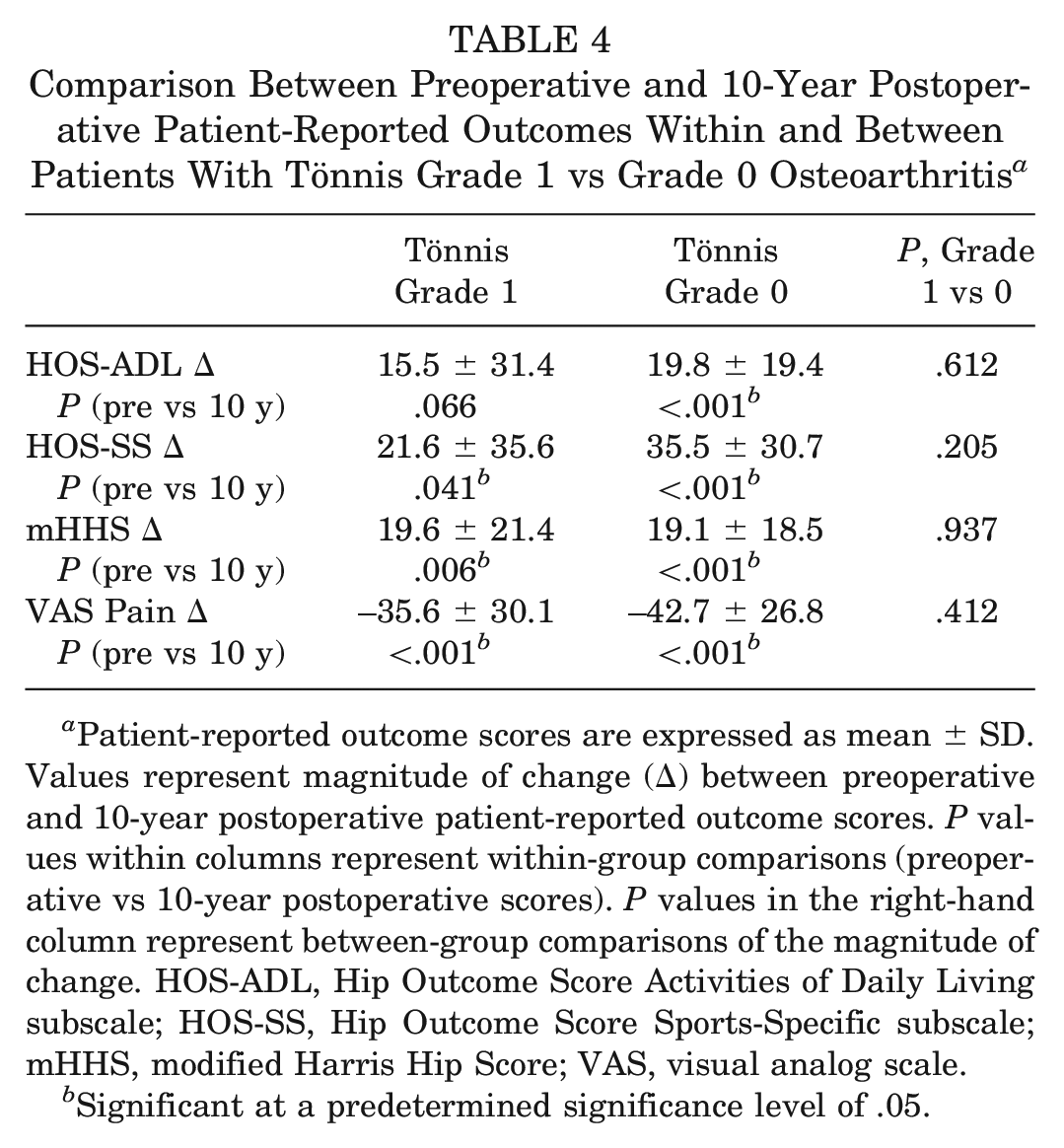
Patient-reported outcome scores are expressed as mean ± SD. Values represent magnitude of change (Δ) between preoperative and 10-year postoperative patient-reported outcome scores. P values within columns represent within-group comparisons (preoperative vs 10-year postoperative scores). P values in the right-hand column represent between-group comparisons of the magnitude of change. HOS-ADL, Hip Outcome Score Activities of Daily Living subscale; HOS-SS, Hip Outcome Score Sports-Specific subscale; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Significant at a predetermined significance level of .05.
Comparison of Patient-Reported Outcomes Between Patients With Tönnis Grade 1 vs Grade 0 Osteoarthritis at Preoperative and 1-, 2-, 5-, and 10-Year Postoperative Timepoints a
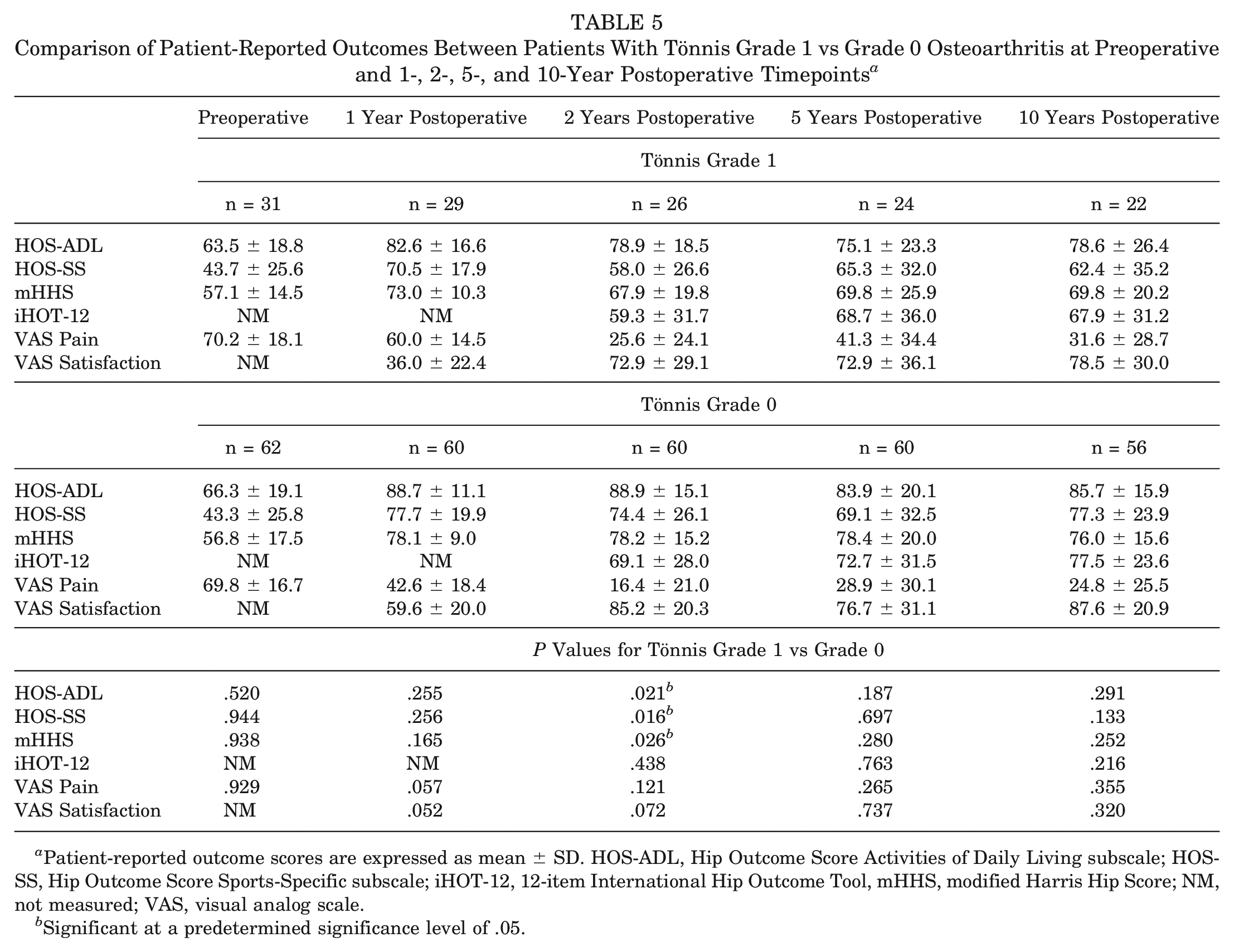
Patient-reported outcome scores are expressed as mean ± SD. HOS-ADL, Hip Outcome Score Activities of Daily Living subscale; HOS-SS, Hip Outcome Score Sports-Specific subscale; iHOT-12, 12-item International Hip Outcome Tool, mHHS, modified Harris Hip Score; NM, not measured; VAS, visual analog scale.
Significant at a predetermined significance level of .05.
Clinically Significant Outcomes
Rates of 10-year MCID and PASS achievement were evaluated against the unique large cohort MCID and PASS thresholds (Appendix Table A1, available online). For all PROs at 10 years, the majority of patients in both the Tönnis grade 1 and grade 0 cohorts reached the MCID threshold, with no significant difference between the 2 groups (Figure 3A). Additionally, high rates of PASS achievement for all PROs were demonstrated by both cohorts, with no significant differences noted between groups (Figure 3B).
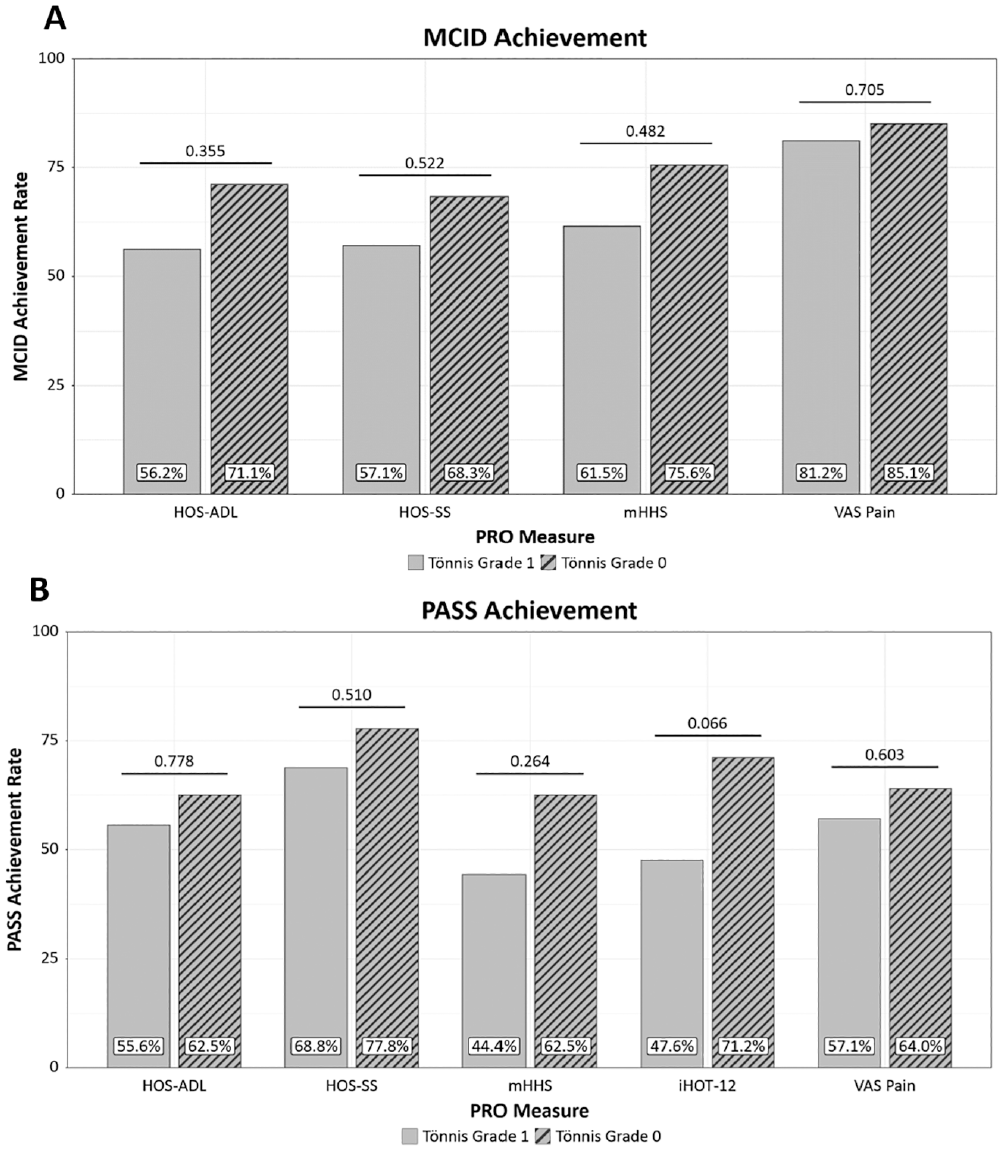
Ten-year achievement rates between patients with Tönnis grade 1 and grade 2 for (A) minimal clinically important difference (MCID) and (B) Patient Acceptable Symptom State (PASS). HOS-ADL, Hip Outcome Score Activities of Daily Living subscale; HOS-SS, Hip Outcome Score Sports-Specific subscale; iHOT-12, 12-item International Hip Outcome Tool, mHHS, modified Harris Hip Score, VAS, visual analog scale.
Survivorship and Secondary Surgery
Postoperative complications rates were similar between cohorts (P = .165) (Table 6). No patient in the Tönnis grade 1 cohort experienced postoperative complications, whereas 1 and 3 patients experienced postoperative infection and neuropathy in the Tönnis grade 0 group, respectively. Similar rates of overall secondary surgery (P = .105) and revision hip arthroscopy (P = .418) were seen between the patients with Tönnis grade 1 and grade 0. However, patients with Tönnis grade 1 underwent significantly higher conversion to THA compared with Tönnis grade 0 (25.8% vs 4.8%%; P = .006). Conversion to THA occurred at a mean duration of 40.4 ± 30.6 months for patients with Tönnis grade 1 compared with 85.0 ± 25.0 months for patients with Tönnis grade 0 (P = .06). Gross survivorship at 10 years was also significantly lower in the Tönnis grade 1 cohort (71.0%) compared with the Tönnis grade 0 cohort (85.5%; P = .04) on Kaplan-Meier analysis (Figure 4).
Postoperative Complications and Reoperations a
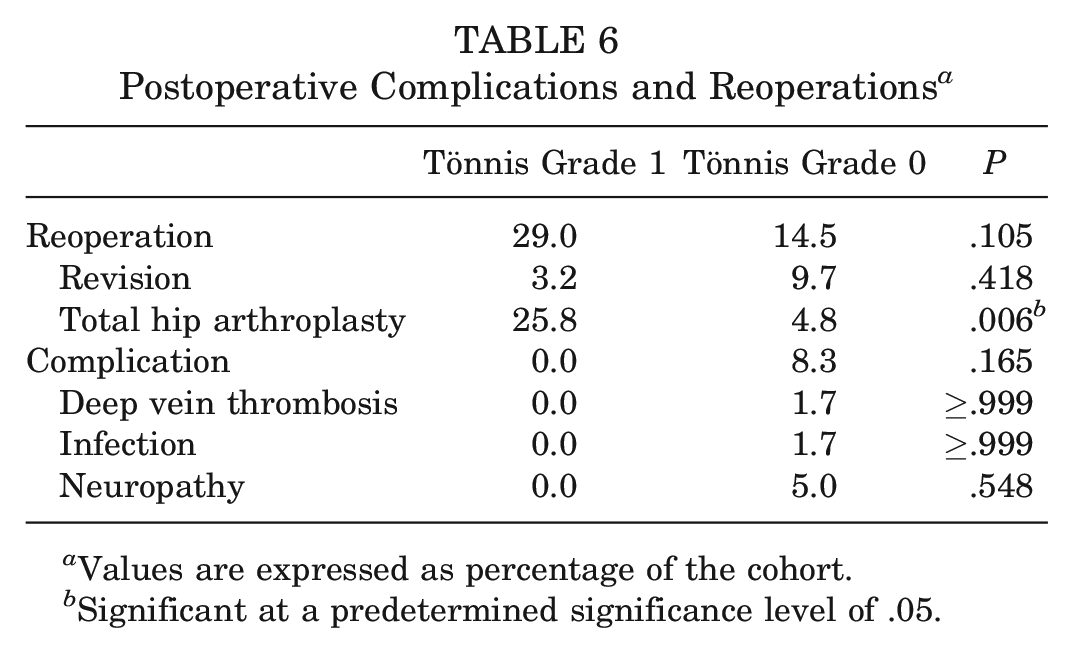
Values are expressed as percentage of the cohort.
Significant at a predetermined significance level of .05.
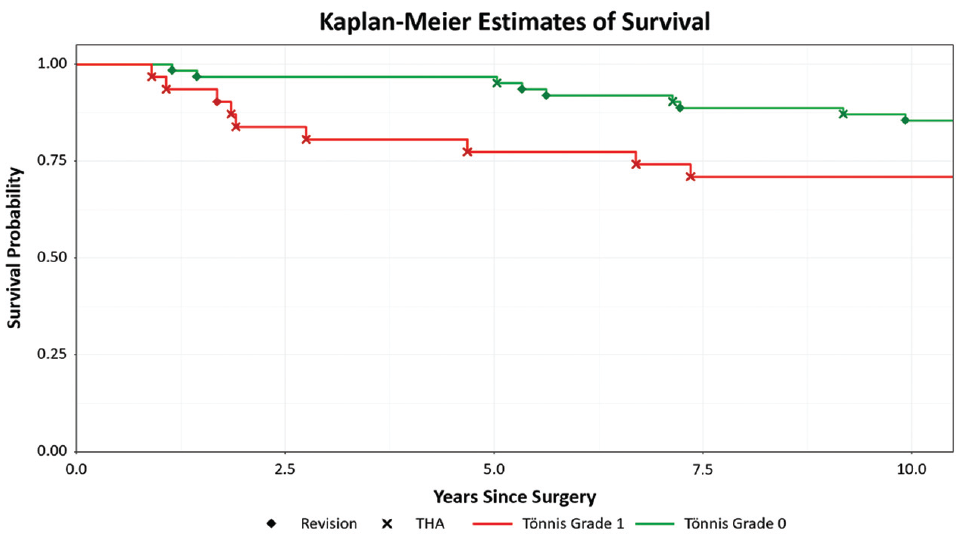
Kaplan-Meier gross 10-year survival curve for patients with Tönnis grade 1 (lower line) and Tönnis grade 0 (upper line). THA, total hip arthroplasty.
Of the patients with Tönnis grade 0 requiring revision (n = 6), 2 patients underwent revision due to heterotopic ossification, 2 patients underwent revision due to recurrent or persistent cam deformity, and 2 patients underwent revision for prolonged pain and lysis of adhesions. One patient in the Tönnis grade 1 cohort underwent revision for lysis of adhesions.
Tönnis Grade 1: THA Conversion Versus No Conversion Subanalysis
A subanalysis was performed for patients with Tönnis grade 1 to compare preoperative patient characteristics, radiographic measurements, and intraoperative findings between those who subsequently had conversion to THA and those who did not (Table 7). The patient who underwent revision was excluded in analyses. Comparisons were limited by sample size. Of note, significant differences were found between groups regarding any grade of femoral head cartilage damage (P = .009) with significant differences between groups regarding rate of grade 0 changes (P = .003).
Subanalysis of Patients With Tönnis Grade 1 Who Underwent Conversion to Total Hip Arthroplasty (THA) vs No Conversion a
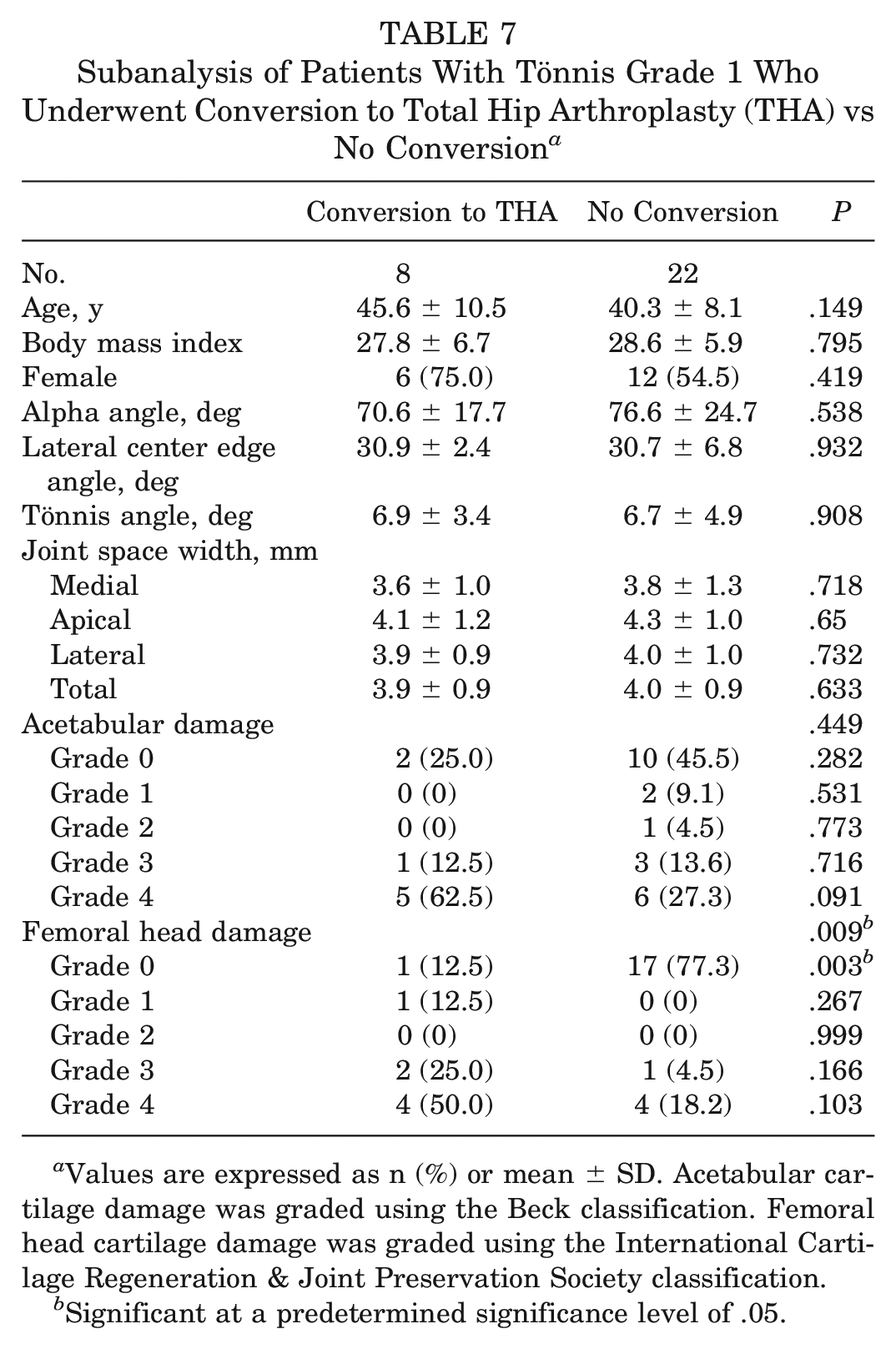
Values are expressed as n (%) or mean ± SD. Acetabular cartilage damage was graded using the Beck classification. Femoral head cartilage damage was graded using the International Cartilage Regeneration & Joint Preservation Society classification.
Significant at a predetermined significance level of .05.
Discussion
The most important findings from the current study are that patients with Tönnis grade 0 or 1 demonstrated significant improvement postoperatively and durable PROs at 10-year follow-up. Patients in both cohorts demonstrated no difference in PROs in any measure at 10 years and had similar magnitudes of change and rates of MCID and PASS achievement. Additionally, both cohorts demonstrated similar rates of revision hip arthroscopy. However, patients with Tönnis grade 1 had reduced survivorship with higher rates (25.8%) of conversion to THA (at a mean time to conversion of 40.4 ± 30.6 months) compared with patients with Tönnis grade 0.
Patients with and without evidence of OA had comparable subjective functional outcomes at 10-year follow-up, indicating that mild OA may not be a contraindication for hip arthroscopy for FAIS. Although previous literature demonstrated favorable postoperative functional outcomes and symptoms in patients with Tönnis grade 1 hips,10,11,16-18,53,57 the long-term outcomes of patients with OA had yet to be determined. Two studies by the same group examined 2-year follow-up outcomes among matched-pair cohorts comparing Tönnis grade 0 and 1 cohorts, as well as comparing Tönnis grade 0, 1, and 2 cohorts, respectively, and revealed no significant differences in PROs between the groups preoperatively or postoperatively.10,11 The same author group later published a matched-pair analysis comparing Tönnis grade 0 and 1 cohorts at 5-year follow-up and found no significant differences in PROs at any time point. 17 In contrast, Sivasundaram et al 57 reported that patients with Tönnis grade 1 had lower postoperative HOS-ADL and HOS-SS scores and lower achievement of PASS for HOS-SS or any outcome compared with the Tönnis grade 0 cohort at 5-year follow-up. Results of the current study demonstrate durable PROs at 10 years alongside high rates of MCID and PASS achievement regardless of Tönnis grade 0 or 1. Although both cohorts demonstrated similar long-term PRO scores and achievement rates of MCID and PASS, the results should be interpreted in the context of the small patient numbers in each cohort and limited analysis due to limited power. Future studies should expand on comparison analysis between patients with Tönnis grade 0 or 1 with larger patient populations.
Although PROs and achievement of clinically significant outcomes were comparable between groups, evidence of mild OA in the Tönnis grade 1 group was associated with worse overall survivorship and high rates of THA conversion compared with the Tönnis grade 0 cohort. The rates of conversion to THA in this study are comparable with current literature for both patients with Tönnis grade 0, ranging from 0% to 10%, and those with Tönnis grade 1, ranging from 10% to 44%.10,11,16,17,53,57 Also similar to the current study, several studies have reported higher rates of conversion to THA in patients with evidence of OA. In a systematic review performed by Domb et al 18 including 2051 hips, of which 1195 hips had arthritis, significant differences were noted in rate of conversion to THA between Tönnis grade 0 (0%), Tönnis grade 1 (16.3%), and Tönnis grade 2 (17.5%). Similarly, investigations at 2-year and 5-year follow-up with matched-pair analysis between different Tönnis grade classifications demonstrated that patients with Tönnis grade ≥1 demonstrated worse overall survivorship and higher rates of THA conversion.10,11,57 Sivasundaram et al 57 reported that failure in the Tönnis grade 1 cohort demonstrated a bimodal distribution, with 53.3% of the failures occurring in the first 26 months and 46.7% of failures occurring after 45 months. Therefore, although patients with Tönnis grade 1 may maintain subjective improvement and comparable functional outcomes to patients with Tönnis grade 0 when not undergoing conversion to THA, both patients and providers should be aware that their risk of THA conversion remains higher than those without evidence of OA.
Although patients with Tönnis grade 1 demonstrated higher overall conversion to THA compared with patients with Tönnis grade 0, the results of the subanalysis between patients with and without conversion to THA in the Tönnis grade 1 cohort merit further discussion. Although the sample size was limited, the conversion cohort had significantly higher grades of femoral head cartilage damage, and their acetabular cartilage grade was higher as well although this did not reach significance (likely due to sample size). Although Tönnis grade is a useful metric, providers should be cautioned that it is a radiographic classification. Accordingly, there may be discrepancies in cartilage injury between patients with Tönnis grade 1 on radiographs that may not be captured by the Tönnis grading system. Therefore, the increased rate of THA conversion seen in the Tönnis grade 1 cohort is likely driven by the underlying patient-specific factors, such as higher degrees of cartilage damage, and should be further elucidated in future studies. It should be noted that during the time of eligibility included in this study, approximately 16% of patients undergoing primary hip arthroscopy had evidence of Tönnis grade 1 changes. The senior author’s indications have matured with the field of hip arthroscopy over the last ≥10 years. Currently, in simultaneous consideration of several important patient factors such as chronologic age, preoperative pain, BMI, duration of preoperative symptoms, and preoperative activity level, the author anecdotally has decreased the overall rate of performing primary hip arthroscopy on patients with evidence of Tönnis grade 1 OA. This further highlights the importance of considering hip arthroscopy on a case-by-case basis between patients and providers.
This study has numerous strengths. First, although long-term studies on hip arthroscopy for FAIS currently exist in the literature, many report on cases in which contemporary hip arthroscopy techniques were not used, and older techniques such as open techniques, 22 the majority of labral treatment was debridement,6,20,22,38,64 and no capsular management were performed.9,44,63,64 To our knowledge, this is the first 10-year investigation that uses contemporary approaches (ie, labral repair, capsular closure, femoral osteochondroplasty) specifically comparing patients with Tönnis grade 0 versus grade 1. Second, this study used a propensity match of age, sex, and BMI to minimize confounding variables when comparing results between groups. Third, a wide variety of PROs were included at preoperative and 10-year timepoints, allowing for the capture of a wide range of patients’ subjective outcomes, as well as to allow for future researchers to look for consistencies in values across studies. Fourth, the study evaluated clinically significant outcomes, including MCID and PASS, allowing us to assess both statistically relevant differences and clinical significance. Fifth, PROs were captured at multiple timepoints, allowing for the capture of not only the preoperative and 10-year timepoint but the trendline up to 10 years as well.
The results of this study must be interpreted through the context of its limitations. First, the present cohort of patients provides data from a single, fellowship-trained sports medicine surgeon with advanced training in hip arthroscopy, thus limiting the study’s generalizability to patients treated by surgeons with differing levels of training and experience. Second, the study is a retrospective cohort study and causation is difficult to determine. Third, although the follow-up rate (77.5%) is high compared with other 10-year outcome studies, selection bias still may be introduced due to the inclusion of only patients who could be contacted. Fourth, although the patient cohorts were successfully propensity matched, differences between groups must be addressed. Patients in the Tönnis grade 1 cohorts demonstrated higher rates of smoking and preoperative chronic pain compared with the Tönnis grade 0 cohort—both of these preoperative patient characteristics have demonstrated implications at varying short- and midterm follow-up.28,32-34,39 Postoperative alpha angles was significantly higher in the Tönnis grade 1 group; however, this finding may be clinically irrelevant, as the differences were small (42° vs 39°) and both values were well under the 50° threshold associated with cam impingement.21,54 Fifth, given the small sample sizes included in both cohorts, analyses comparing PROs and rates of MCID and PASS achievement between groups were likely underpowered to capture differences between groups, which may introduce type II error bias. Sixth, statistical comparisons were limited between patients with Tönnis grade 1 with and without conversion to THA, and conclusions between the groups should be made in caution.
Conclusion
Hip arthroscopy confers comparable postoperative clinical improvements to patients with FAIS with and without mild OA; however, the benefits among patients with mild OA may be less durable. Patients with Tönnis grade 1 had significantly higher conversion to THA and reduced gross survivorship compared with patients with no evidence of preoperative OA, suggesting that patients with evidence of OA may need to be cautioned on the higher rate of conversion surgery.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465231210958 – Supplemental material for Functional Outcome Scores and Conversion to Total Hip Arthroplasty After Hip Arthroscopy for Femoroacetabular Impingement Syndrome in Patients With Tönnis Grade 1 Versus Grade 0 Arthritis: A Propensity-Matched Study at Minimum 10-Year Follow-up
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231210958 for Functional Outcome Scores and Conversion to Total Hip Arthroplasty After Hip Arthroscopy for Femoroacetabular Impingement Syndrome in Patients With Tönnis Grade 1 Versus Grade 0 Arthritis: A Propensity-Matched Study at Minimum 10-Year Follow-up by Thomas W. Fenn, Daniel J. Kaplan, Christopher M. Brusalis, Reagan S. Chapman, Jordan H. Larson and Shane J. Nho in The American Journal of Sports Medicine
Footnotes
Submitted April 3, 2023; accepted September 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.M.B. has received support for education from Smith + Nephew. S.J.N. has received research support from Allosource, Arthrex, Athletico, DJ Orthopedics, Linvatec, Miomed, and Smith + Nephew; consulting fees and royalties from Ossur, Springer, and Stryker; and support for education from Elite Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.