
Abstract
Background:
Preoperative risk factors contributing to poor outcomes after arthroscopic partial meniscectomy (APM) have not yet been consolidated and codified into an index scoring system used to predict APM success.
Purpose:
To create an index score using available preoperative factors to predict the likelihood of favorable postoperative outcomes after APM.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A consecutive cohort of patients undergoing primary APM were enrolled in this study. Patients completed pre- and postoperative patient-reported outcome measure (PROM) questionnaires that included the Knee injury and Osteoarthritis Outcome Score (KOOS), visual analog scale (VAS) for pain, Veterans RAND 12-Item Health Survey (VR-12 Physical and Mental), and Marx Activity Rating Scale (MARS). Multivariable logistic regression models were performed to evaluate independent predictors of KOOS Pain, Symptoms, and Activities of Daily Living scores and achievement of the minimal clinically important difference (MCID) and substantial clinical benefit (SCB). The authors assigned points to each variable proportional to its odds ratio, rounded to the nearest integer, to generate the index score.
Results:
In total, 468 patients (mean age, 49 years [SD, 10.4 years; range, 19-81 years]) were included in this study. In the univariate analysis, shorter symptom duration, lower Kellgren-Lawrence (KL) grade, lower preoperative KOOS Pain value, and lower VR-12 Physical score were associated with a higher likelihood of clinical improvement at 1 year. In the multivariable model for clinical improvement with MCID, symptom duration (<3 months: OR, 3.00 [95% CI, 1.45-6.19]; 3-6 months: OR, 2.03 [95% CI, 1.10-3.72], compared with >6 months), KL grade (grade 0: OR, 3.54 [95% CI, 1.66-7.54]; grade 1: OR, 3.04 [95% CI, 1.48-6.26]; grade 2: OR, 2.31 [95% CI, 1.02-5.27], compared with grade 3), and preoperative KOOS Pain value (score <45: OR, 3.00 [95% CI, 1.57-5.76]; score of 45-60: OR, 2.80 [95% CI, 1.47-5.35], compared with score >60) were independent significant predictors for clinical improvement. The scoring algorithm demonstrated that a higher total score predicted a higher likelihood of achieving the MCID: 0 = 40%, 1 = 68%, 2 = 80%, 3 = 89%, and 4 = 96%.
Conclusion:
Using this model, the authors developed an index score that, using preoperative factors, can help identify which patients will achieve clinical improvement after APM. Longer symptom duration and higher KL grade were associated with a decreased likelihood of clinical improvement as measured by KOOS Pain at 1 year postoperatively.
Meniscal tears are one of the most common knee conditions managed by orthopaedic surgeons, and arthroscopic partial meniscectomy (APM) has been shown to be the most commonly performed meniscal surgical treatment in the United States. 3 The current recommendations for APM vary based on the cause of the tear. The current American Academy of Orthopaedic Surgery guidelines recommend physical therapy before APM for degenerative tears associated with osteoarthritis (OA).1,14 Several studies have suggested that APM may be especially beneficial as a treatment for meniscal tears in non-osteoarthritic knees.2,9,11
Management of meniscal tears would be enhanced with more data on factors associated with the success of APM. Several preoperative risk factors contribute to poor outcomes after APM, such as symptom duration and radiographic OA at baseline.7,12,13 Some studies suggest that increased duration between symptom onset and surgical intervention and increased radiographic OA at baseline may be associated with worse outcomes.12,13 Additionally, factors such as baseline knee functional score, location of the tear (medial vs lateral), body mass index (BMI), preoperative activity level, age, sex, leg malalignment, degenerative versus traumatic cause, anterior cruciate ligament (ACL) laxity, and presence of chondral damage on magnetic resonance imaging (MRI) have been studied and do not demonstrate a straightforward effect on postoperative outcomes.8-12,20,25 In general, there is conflicting evidence on whether these variables influence outcomes.
Preoperative risk factors have not previously been consolidated and codified into an index scoring system used to predict the success of APM. Therefore, the present study was designed to create a screening tool that, when used in clinical practice, can help to identify patients likely to have a successful outcome from APM. Index scores have been used by surgeons to simplify the process of selecting patients for other surgeries, such as arthroscopic versus open shoulder stabilization. 25 Furthermore, index scores have been used to incorporate risk factors for lateral patellar dislocation into a clinically useful tool for initial risk assessment. 6 The purpose of this study was to create an index score using easily available preoperative risk factors such as Kellgren-Lawrence (KL) grade, age, duration of symptoms, BMI, activity level, and preoperative outcome scores to predict the likelihood of favorable postoperative outcomes after APM. It is important to note that because this index score is derived from patients undergoing APM, it will be useful to predict which patients undergoing APM are likely to have a good outcome but will not be able to compare the benefits of undergoing APM versus other nonoperative treatments such as physical therapy alone. This index is intended to help surgeons discuss with patients the likely outcomes after a potential APM.
Methods
Source of Patients and Inclusion and Exclusion Criteria
After approval from the Mass General Brigham Institutional Review Board (IRB No. 2011P002663), we retrospectively reviewed a prospectively enrolled database of a consecutive cohort of patients from a single surgeon (E.G.M.) at a single academic medical center in an outpatient setting from August 2012 through October 2020 who were scheduled to undergo primary APM. These patients had knee pain and meniscal tear and had undergone a minimum of 6 weeks of nonoperative treatment measures, including activity modification, anti-inflammatory medications, physical therapy, and injection, with no improvement. A single surgeon (E.G.M.) performed all cases using the same surgical technique. Inclusion criteria for this study were primary APM with or without chondroplasty (cartilage debridement) and debridement. Patients were indicated for APM if they had meniscal tears in the white-white zone or unstable tears. All patients followed the same postoperative rehabilitation protocol. Each patient provided informed consent before enrollment. We collected and stored all data in a Health Insurance Portability and Accountability Act–compliant global registry database (Surgical Outcomes System [SOS]; Arthrex).
Data Collection
All patients completed preoperative questionnaires that included the Knee injury and Osteoarthritis Outcome Score (KOOS)22-24 questionnaire, visual analog scale (VAS) to measure overall pain level, Veterans RAND 12-Item Health Survey (VR-12 Physical and Mental) 15 to evaluate a patient’s perspective of their overall health, and Marx Activity Rating Scale (MARS). 21 After consent and enrollment, patients were emailed a link to an electronic survey with 1 email reminder and/or telephone call from a research assistant if outcome measures were not completed in a timely manner.
We collected patient characteristics (Table 1) and reviewed medical records to determine the most recent radiograph date before APM. Four research team members (N.L., A.M., C.U., H.M.) independently analyzed the preoperative standing AP radiographs according to the KL score, which determines OA severity on a scale of 0 to 4. 16 The 4 reviewers underwent several training sessions to read radiographs before this process to ensure agreement among readers. All radiographs were graded independently by a minimum of 2 reviewers, (N.L., A.M., C.U., H.M.) and any discrepant readings were evaluated by an orthopaedic surgeon (E.M.) to determine a final score.
Preoperatively Collected Patient Characteristics and Baseline PROMs a
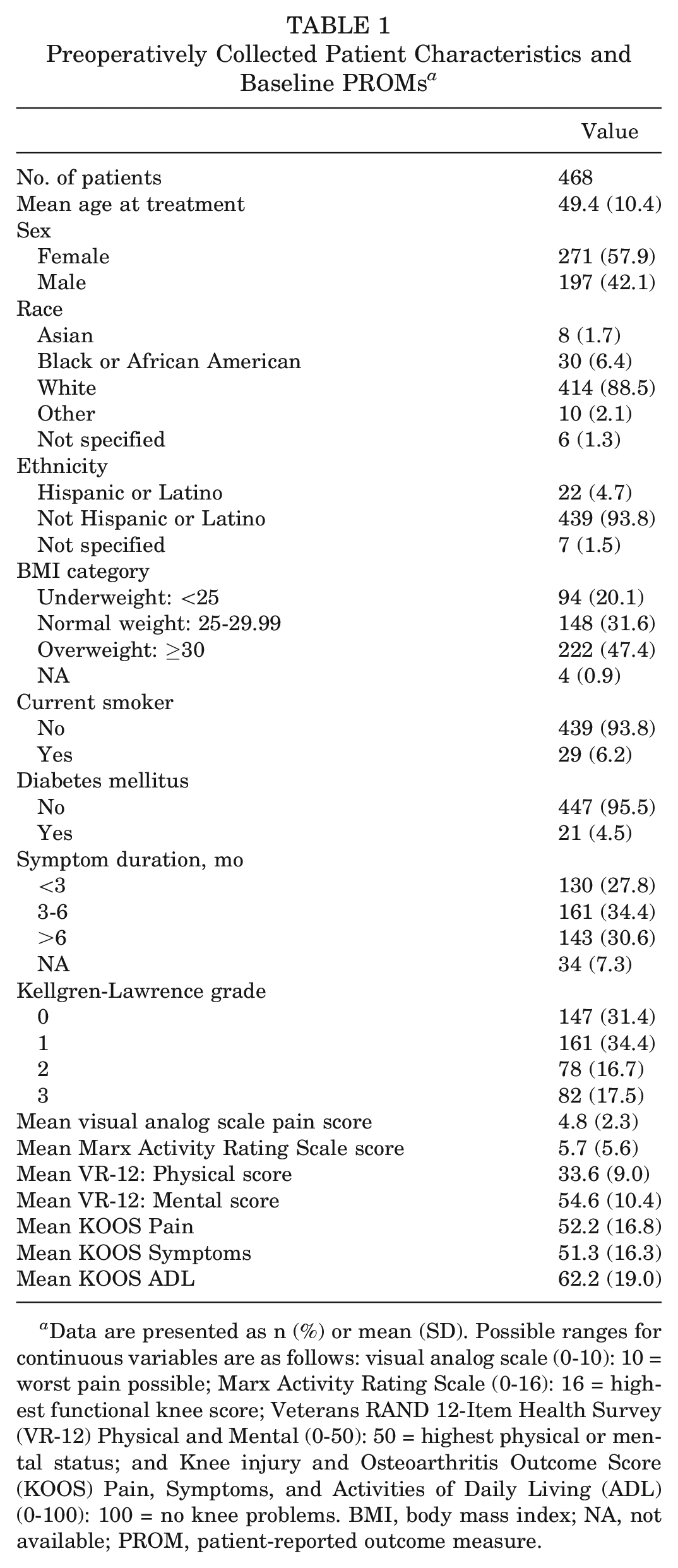
Data are presented as n (%) or mean (SD). Possible ranges for continuous variables are as follows: visual analog scale (0-10): 10 = worst pain possible; Marx Activity Rating Scale (0-16): 16 = highest functional knee score; Veterans RAND 12-Item Health Survey (VR-12) Physical and Mental (0-50): 50 = highest physical or mental status; and Knee injury and Osteoarthritis Outcome Score (KOOS) Pain, Symptoms, and Activities of Daily Living (ADL) (0-100): 100 = no knee problems. BMI, body mass index; NA, not available; PROM, patient-reported outcome measure.
Statistical Analysis
The primary outcome was clinical improvement in KOOS Pain scale at 1 year postoperatively. The secondary outcomes were improvement in KOOS Symptoms and Activities of Daily Living (ADL) subscales. Clinical improvement with a minimal clinically important difference (MCID) was defined as a change ≥10 for all 3 subscales or any improvement with a score of ≥90 at the 1-year follow-up. Clinical improvement with a substantial clinical benefit (SCB) was defined as ≥22 for Pain, ≥7 for Symptoms, and ≥17 for ADL or any improvement with a score of ≥90 at the 1-year follow-up. These cutoffs were chosen as previously established, 4 and any improvement reaching a score of ≥90 was considered to be clinically sufficient. Potential predictors included patient age, sex, BMI, comorbidity and symptom duration, KL grade, and other preoperative patient-reported outcome measures (PROMs) (VAS, VR-12 Physical, VR-12 Mental, and MARS). We first conducted univariate analysis to identify potential risk factors for each of the 3 outcomes (Pain, Symptoms, and ADL scores) and 2 types of improvement (MCID and SCB). We then conducted multivariable logistic regression models to evaluate independent predictors of these outcomes. To generate a risk score, we assigned points to each variable proportional to its odds ratio, rounded to the nearest integer. For ease of clinical application, we also developed abbreviated models with limited factors that are more clinically available (Appendix Figure A1, available in the online version of this article). Two-sided P values of ≤.05 were considered statistically significant. All analyses were conducted using SAS Version 9.4.
Sample Size and Power
For the purpose of identifying potential predictors, the study had 80% power to detect a 13% absolute difference (70% vs 57%) in the proportion of patients achieving clinical improvement between any 2 groups with a 2-sided significance level of .05, when the sample sizes are relatively equal between the 2 groups.
Results
In total, 1916 patients were prospectively enrolled in our database, and initial exclusion criteria included concomitant ligamentous knee injury, revision APM, and hardware removal. This led to our cohort of 697 patients who underwent APM with or without chondroplasty. From there we excluded 132 patients who were missing preoperative or 1-year postoperative data, to result in a cohort of 565 patients. Next, 21 patients were excluded for secondary surgeries and 26 patients were excluded after undergoing concomitant ligamentous procedures. We then reviewed radiographic data for each patient in this cohort. We excluded 7 patients who were <18 years of age and 29 patients due to a lack of radiographs in their records or images that were not able to be evaluated by our reviewers. Lastly, 14 patients were excluded for missing preoperative KOOS values. Figure 1 demonstrates the exclusion criteria for our cohort, resulting in our final cohort of 468 patients.
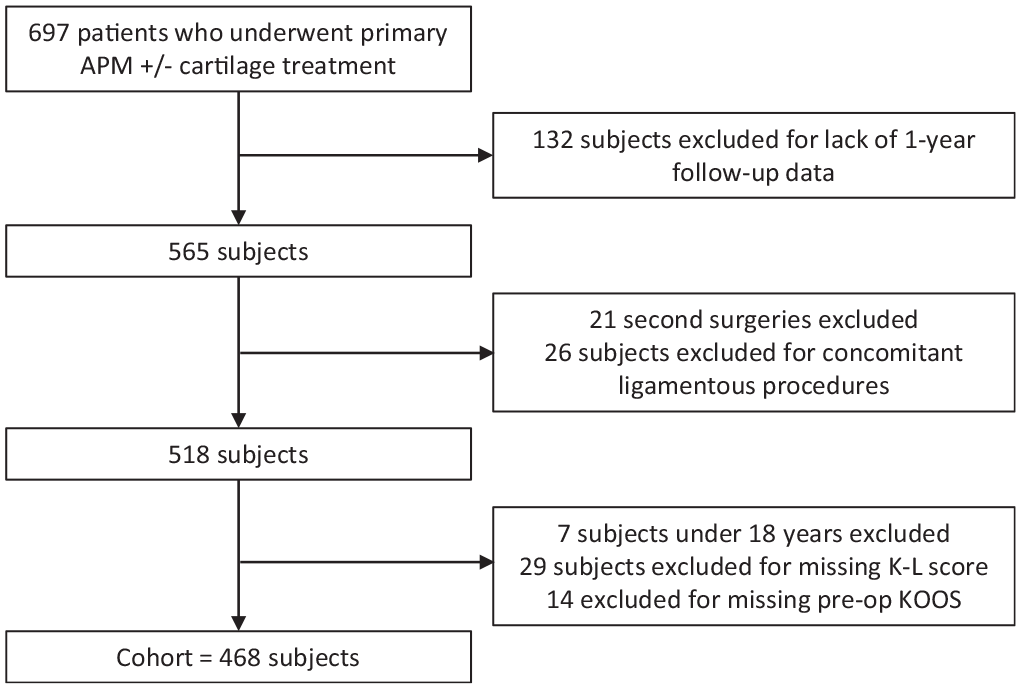
Flowchart. APM, arthroscopic partial meniscectomy; K-L, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score.
Among the 468 included patients who underwent APM between August 2012 and October 2020, the mean age was 49 years (SD, 10.4 years; range, 19-81 years), 42% of patients were male, 89% were White, and 48.3% were either overweight or obese (Table 1).
For the primary outcome, KOOS Pain, 84% of patients achieved clinical improvement with MCID and 69% achieved clinical improvement with SCB at 1 year postoperatively. Lower KL grade, lower preoperative KOOS Pain value, and lower VR-12 Physical score were associated with a higher likelihood of clinical improvement with MCID or SCB at 1 year (Table 2).
Bivariate Analysis of Potential Predictors for KOOS Pain Value a
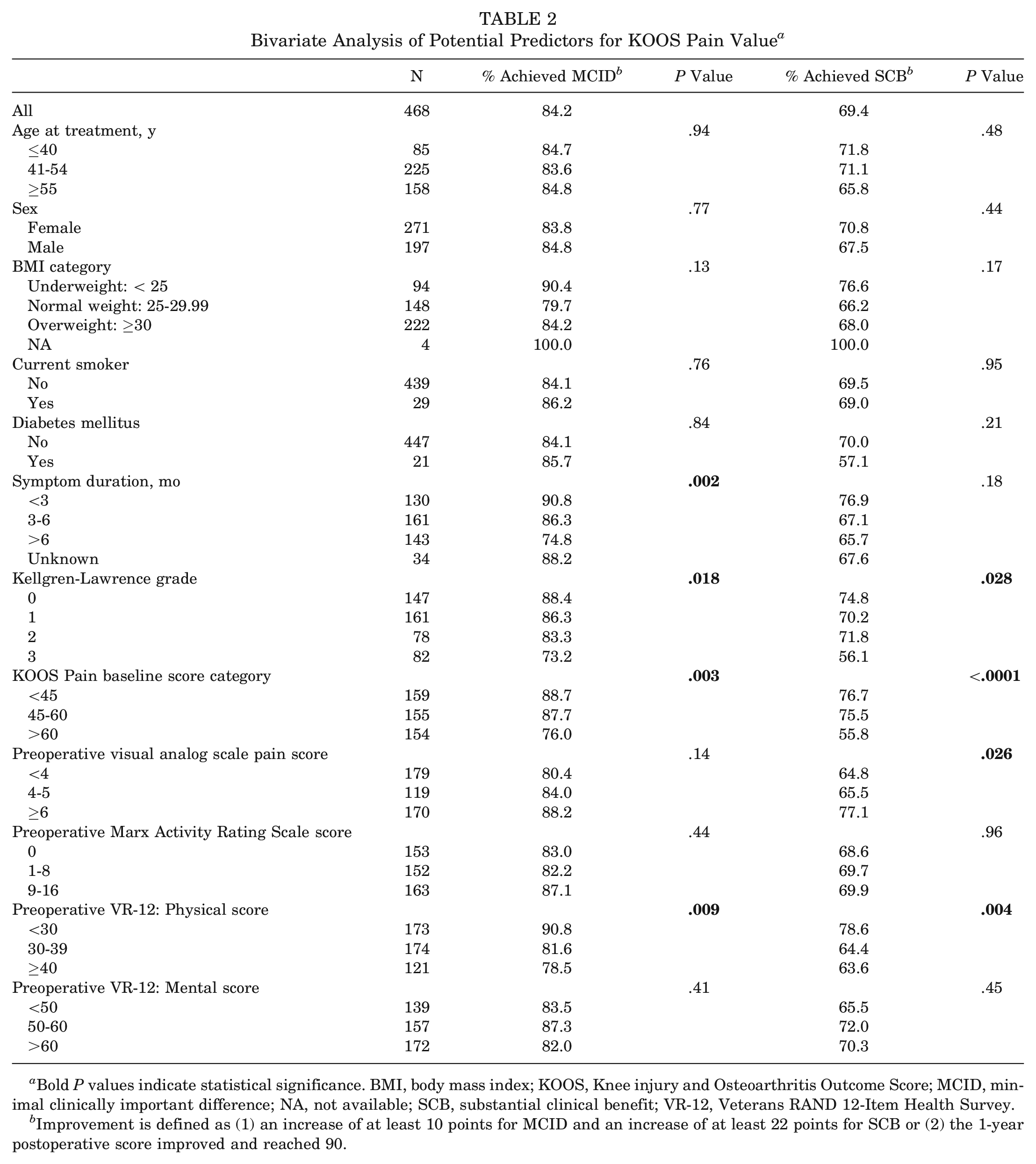
Bold P values indicate statistical significance. BMI, body mass index; KOOS, Knee injury and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; NA, not available; SCB, substantial clinical benefit; VR-12, Veterans RAND 12-Item Health Survey.
Improvement is defined as (1) an increase of at least 10 points for MCID and an increase of at least 22 points for SCB or (2) the 1-year postoperative score improved and reached 90.
In the multivariable model for clinical improvement with MCID, symptom duration (<3 months: OR, 3.00 [95% CI, 1.45-6.19]; 3-6 months: OR, 2.03 [95% CI, 1.10-3.72], compared with >6 months), KL grade (grade 0: OR, 3.54 [95% CI, 1.66-7.54]; grade 1: OR, 3.04 [95% CI, 1.48-6.26]; grade 2: OR, 2.31 [95% CI, 1.02-5.27], compared with grade 3), and preoperative KOOS Pain value (score <45: OR, 3.00 [95% CI, 1.57-5.76]; score of 45-60: OR, 2.80 [95% CI, 1.47-5.35], compared with score >60) were the independent significant predictors for clinical improvement. We generated a scoring algorithm based on the adjusted odds ratios from the model: those with KL grade 0 were assigned 2 points, and those with symptom duration ≤6 months and those with KL grade 1 or 2 were each assigned 1 point. The scoring algorithm performed very well, with a higher total score predicting a higher likelihood of achieving clinical improvement with MCID: 40% among those with score 0, 68% among those with score 1, 80% among those with score 2, 89% among those with score 3, and 96% among those with score 4 (Table 3).
Logistic Regression Model Effects and Scoring Algorithm for Achieving Clinical Improvement in KOOS Pain a
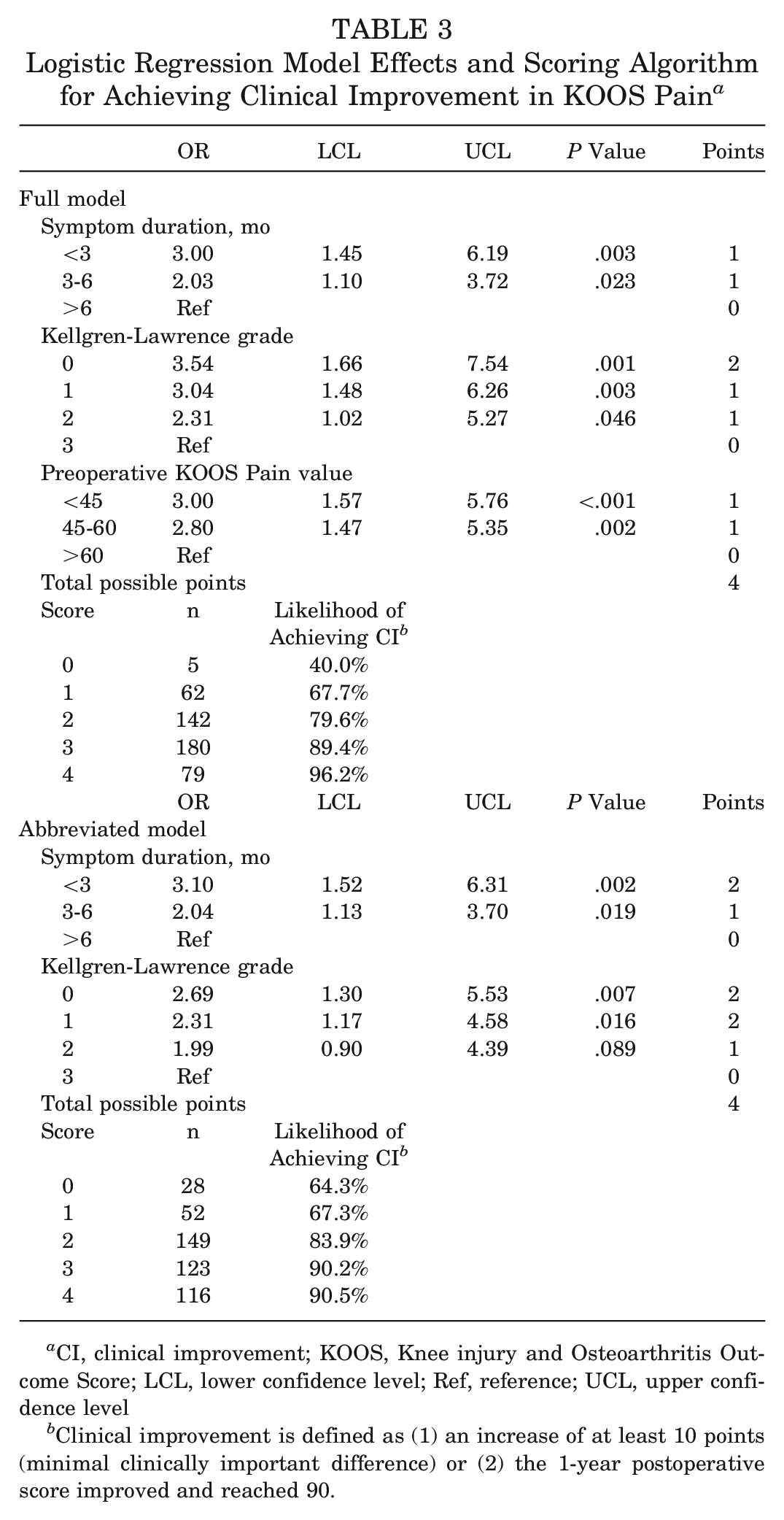
CI, clinical improvement; KOOS, Knee injury and Osteoarthritis Outcome Score; LCL, lower confidence level; Ref, reference; UCL, upper confidence level
Clinical improvement is defined as (1) an increase of at least 10 points (minimal clinically important difference) or (2) the 1-year postoperative score improved and reached 90.
Because the preoperative KOOS Pain value may not be readily available, we also developed an abbreviated model including only symptom duration and KL grade for achieving clinical improvement with MCID. The abbreviated model can be used in a clinical setting to evaluate a patient’s likelihood of achieving the MCID. The corresponding scoring algorithm assigned 2 points to those with KL grade 0 or 1 or symptom duration <6 months and 1 point to those with symptom duration of 3 to 6 months or KL grade 2 (Table 3). As expected, the abbreviated scoring algorithm did not perform as well as the one developed from the full model but was still able to distinguish those with a lower likelihood of achieving clinical improvement from those with a higher likelihood: 64% of those with a score of 0 achieved clinical improvement with MCID compared with 91% of those with a score of 4.
The model and scoring algorithm for achieving clinical improvement with SCB in KOOS Pain was similar, with more points assigned to those with a lower preoperative KOOS Pain value (Appendix Table A2, available online). Those with a higher total score were more likely to achieve clinical improvement (ranging from 38% of those with a total score of 0 to 82% of those with a score ≥4) (Appendix Table A3, available online).
For the secondary outcomes, 77% of patients achieved clinical improvement with MCID and 82% achieved clinical improvement with SCB for KOOS Symptoms (Appendix Table A1, available online). The predictors for these secondary outcomes were similar to those for KOOS Pain: shorter symptom duration, lower KL grade, and lower preoperative KOOS Symptoms value were associated with a higher likelihood of clinical improvement at 1 year (Appendix Table A1, available online). The scoring algorithm for achieving clinical improvement with MCID (Appendix Table A2, available online) also performed well, with a score of 0 corresponding to 50% achieving clinical improvement with MCID and a score of ≥4 corresponding to 91% achieving clinical improvement with MCID (Appendix Table A3). The model, scoring algorithm, and performance for achieving clinical improvement with SCB were similar (Appendix Tables A2 and A3, available online).
For KOOS ADL, 84% of patients achieved clinical improvement with MCID and 77% achieved clinical improvement with SCB (Appendix Table A1, available online). The scoring algorithms included preoperative KOOS ADL value, symptom duration, preoperative MARS score, and BMI (Appendix Table A2, available online) and performed well with a score of 0 corresponding to 47% achieving clinical improvement with MCID and a score of ≥4 corresponding to 99% achieving clinical improvement with MCID (Appendix Table A3, available online). The model, scoring algorithm and performance for achieving clinical improvement with SCB were also similar (Appendix Tables A2 and A3, available online).
The authors created an easy-to-print and easy-to-use APM index clinical scoring form that clinicians can use when discussing the management of symptomatic meniscal tears with patients (Figure 2). Use of the APM index score only requires patients to have had standard knee radiographs for KL grading and a known symptom duration from their meniscal tear (Figure A1).
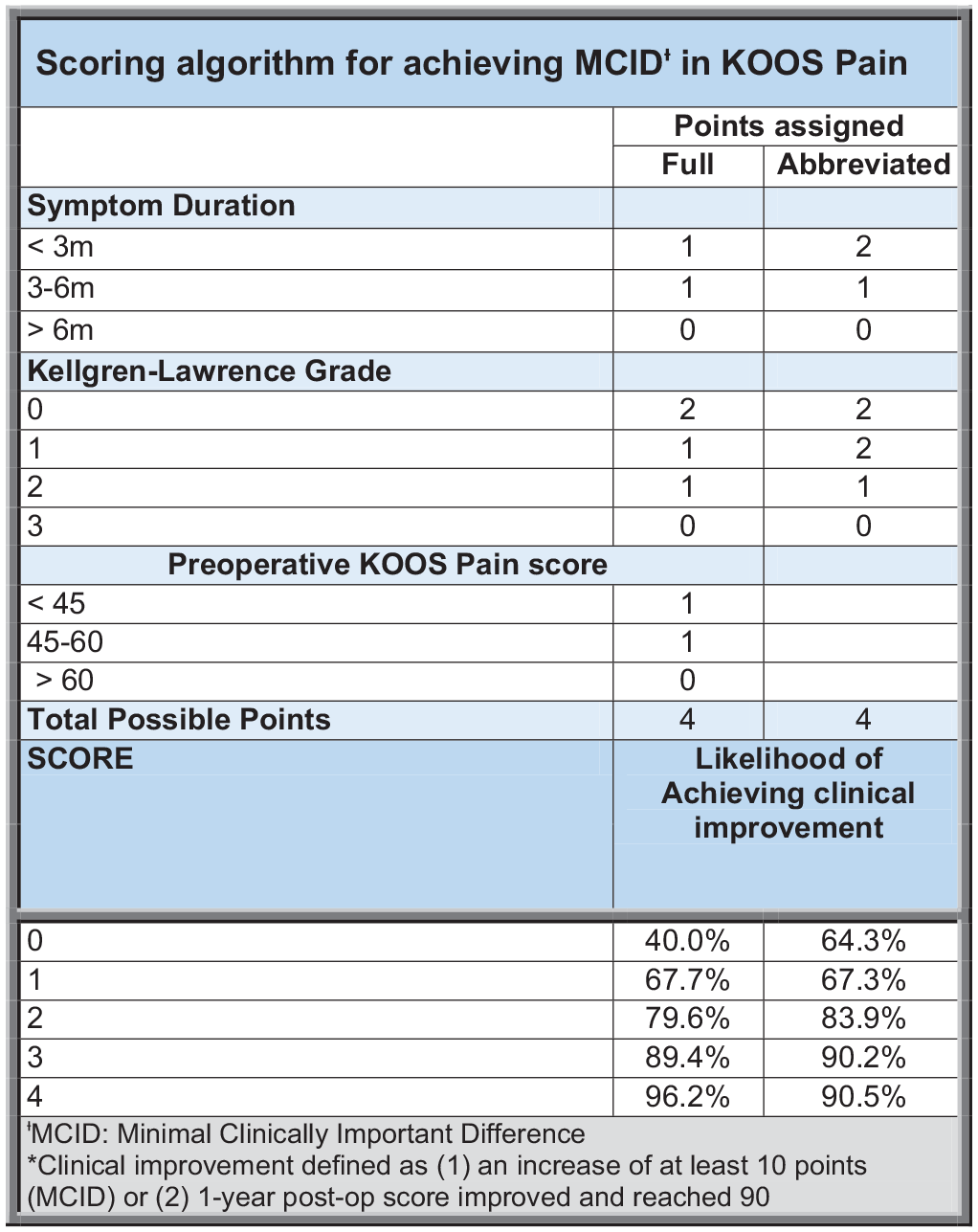
Scoring algorithm for achieving minimal clinically important difference (MCID) in Knee injury and Osteoarthritis Outcome Score (KOOS) Pain.
Discussion
The current study has developed an index score instrument intended for use in a clinical setting to engage in shared decision-making with patients regarding knee arthroscopy for treating symptomatic meniscal tears. We found that, after knee arthroscopy, the majority of patients achieved MCID for KOOS Pain, KOOS Symptoms, and KOOS ADL questionnaires from baseline to 1 year postoperatively. For all KOOS domains, our model found that shorter symptom duration, lower baseline KL grade, and lower pretreatment KOOS Pain value were the strongest predictors of achieving the respective MCIDs at 1 year postoperatively.
Using the data, we created an index score specifically focused on KOOS Pain. The primary scoring algorithm included symptom duration, KL grade, and preoperative KOOS Pain as the predictors for achieving MCID at 1 year postoperatively. Because we intend for the scoring algorithm to be used in a clinical setting, we also created a modified scoring algorithm that does not include the preoperative KOOS value as a predictor, as many physicians may not have access to a KOOS value at the preoperative clinical visit.
The findings from this study support the overall consensus that preoperative factors can help predict how patients do after APM. Our study found that longer symptom duration, higher KL grade, worse KOOS Pain value, and worse VR-12 Physical component score were associated with a decreased likelihood of clinical improvement as measured by KOOS Pain at 1 year postoperatively. These findings support current literature that states that symptom duration and worse baseline OA lead to worse outcomes postoperatively.7,12,13 A recent study demonstrated tear laterality, type, and higher KOOS value are associated with postoperative APM clinical improvement. 8 Another study demonstrated that in patients with degenerative meniscal tears, larger excision, complex tears, and extrusion were risk factors for worse postoperative outcomes, indicating a potential utility of preoperative MRI in predicting postoperative improvement. 17 While the literature includes other factors such as baseline knee function, location of tear (medial vs lateral), BMI, age, sex, leg malalignment, ACL laxity, chondral damage on preoperative MRI, and acuity of tear (degenerative vs traumatic), our study found that symptom duration, KL grade, and preoperative KOOS Pain value were the only independent predictors for achieving MCID or a KOOS Pain value of 90 by 1 year postoperatively.8-12,25
Other publications have shown similar results to the current study regarding the relationship between shorter duration of symptoms and better preoperative functional scores before APM and increased improvement in outcomes. For example, Haviv et al 13 found that patients with a duration of symptoms of <3 months and patients with higher preoperative Lysholm scores experienced more significant improvement in Lysholm score after APM. Lee et al 18 demonstrated that patients with KL grade ≥2 had a significantly increased risk for end-stage arthritis, eventually requiring conversion to total knee replacement (TKR) after partial meniscectomy. Li et al 19 found that patients with KL grade ≥3 were approximately 3 times more likely to be converted to TKR after knee arthroscopy. A more recent study by Aprato et al 5 found that female sex, older age, malalignment, and advanced chondral lesions were significantly associated with subsequent TKR in the 20 years after APM. Furthermore, their study found that age >60 years was a significant predictor for poor KOOS results at the 20-year follow-up. 5 These results generally align with our finding that the extent of OA is associated with KOOS improvement and long-term outcomes after APM.
Similar associations were seen for our secondary outcomes, which included likelihood of clinical improvement at 1 year postoperatively for both KOOS Symptoms and KOOS ADL. The preoperative KOOS subscales (Symptoms or ADL) were independent predictors of their respective outcomes postoperatively. Furthermore, for KOOS ADL, the scoring algorithm included BMI and MARS, which supports the findings in other current literature that these factors influence postoperative outcomes after APM.8,10
The scoring algorithm performed well in all 3 KOOS subscales. Although this study is focused on KOOS Pain, a higher total score predicted a higher likelihood of achieving the MCID for KOOS Symptoms and KOOS ADL as well.
We acknowledge several limitations to our investigation. Although 2 trained reviewers determined the KL score for each radiograph independently, and the senior author (E.G.M.) resolved any discrepancies in scores, there is potential for error due to human measurement in KL grades. The cutoffs used for the score determination in the current study were derived from another study. Furthermore, our data were developed from a single surgeon at a single institution and therefore may not be applicable to all patients in all geographic areas. Because this study was performed with a single cohort, we recommend that the results be validated with another study population. The strengths of this investigation include the large sample size and the consistency in surgical technique and postoperative rehabilitation, as all surgeries were performed by the same orthopaedic surgeon. It provides users with a simple scoring system to inform patients with a symptomatic meniscal tear of their potential for improvement after APM.
Conclusion
This study found that preoperative factors, including shorter symptom duration, lower KL grade, and decreased preoperative pain, are predictors of clinically important improvement after APM. The APM index score is a simple tool to use in real time to inform patients with a symptomatic meniscal tear of their probability for improvement after APM. Further research should be conducted to determine how this scoring algorithm performs in a clinical setting and whether it can be used to inform physician and patient discussions regarding knee arthroscopy and APM to treat symptomatic meniscal tears.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465231210303 – Supplemental material for Preoperative Predictors of Arthroscopic Partial Meniscectomy Outcomes: The APM Index Score
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231210303 for Preoperative Predictors of Arthroscopic Partial Meniscectomy Outcomes: The APM Index Score by Natalie A. Lowenstein, Yuchiao Chang, Hanna Mass, Angela M. Mercurio, Chierika Ukogu, Jeffrey N. Katz and Elizabeth G. Matzkin in The American Journal of Sports Medicine
Footnotes
Presented at the annual meeting of the AOSSM, Washington, DC, July 2023.
Submitted April 28, 2023; accepted September 15, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.N.K. has received honoraria from Pfizer. E.G.M. has received support for education from Peerless Surgical and Kairos Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.