
Abstract
Background:
The Major League Baseball (MLB) draft is a common route for players to enter professional baseball in the United States. Players taken in earlier rounds are typically higher-performing players. When looking at pitchers specifically, higher performance at the amateur level may be associated with an increased frequency of adaptive change in the throwing elbow.
Purpose:
To determine whether pitchers taken in earlier rounds of the MLB draft have a greater frequency or extent of pathological change in the elbow, as measured by dynamic stress ultrasound.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Dynamic stress ultrasounds (SUSs) were performed over 18 years on the dominant and nondominant arms of 651 professional pitchers. The 383 drafted players were grouped according to the round in which they were drafted (rounds 1-5, 6-10, 11-20, 21+). Groups were compared with respect to “relative” ulnar collateral ligament (UCL) thickness (dominant-nondominant), relative ulnohumeral joint laxity (joint space distance under stress minus joint space at rest), and the presence of pathology (calcifications, tears, hypoechoic foci, osteophytes). In addition, a subgroup analysis was done to compare the progression of SUS findings over 3 years in players for which data were available.
Results:
Draft round groups did not differ by age, number of previous spring training, or handedness. Comparing baseline measurements, there was no significant relationship between draft round and relative UCL thickness (P = .932), relative laxity (P = .996), or presence of pathology detectable on SUS (P = .642). However, increased relative UCL thickness was significantly associated with the presence of pathology on SUS (odds ratio, 1.45; 95% CI, 1.26-1.69; P < .001). Longitudinally, there was no significant relationship between draft round and 3-year progression of relative laxity, relative UCL thickness, or clinical progression of pathology.
Conclusion:
Higher-performing pitchers are drafted earlier in the MLB draft. This may be attributable to peak pitch velocity, in-game performance, visibility gained during player showcases, or any number of other sport-specific variables. However, despite this, there was no significant relationship between draft round and adaptive changes to the elbow or specific properties of the UCL on stress ultrasound.
Ulnar collateral ligament (UCL) elbow injuries are common in overhead-throwing athletes, particularly baseball players. During the throwing motion, the elbow experiences a substantial amount of valgus stress, which can cause damage to the soft tissue stabilizers.2,9,10,19,33 For players with persistent pain and loss of performance after nonoperative management, UCL reconstruction is a highly reliable treatment option. Major League Baseball (MLB) pitchers have an 80% to 97% rate of return to play within 12 months postoperatively; however, only 67% to 87% return to the same level of play.32,34 Despite increased rates of return to play after reconstruction, identifying risk factors and preventing injury is exceedingly crucial to these professional athletes’ careers.7,8,16,27
Dynamic stress ultrasound (SUS) is a reliable tool for evaluating the structure of the UCL and determining injury.6,10,11,13,15,28,31 The UCL of the dominant arm in pitchers is thicker and has increased laxity compared with the contralateral elbow on SUS.2,10,19,29 Although SUS has been used to evaluate the risk of increased pitch count and pitch volume on the change in UCL morphology, to our knowledge, no study has investigated SUS findings of the UCL in professional baseball players with respect to their draft position in the MLB draft.
This study aimed to compare SUS findings between pitchers drafted in the early rounds versus later rounds in the MLB draft and to assess for significant differences that may predispose either type of player to future injury. The hypothesis was that players drafted earlier would have a thicker UCL with a higher incidence of pathological changes in the UCL. We also hypothesized that players drafted in earlier rounds would have significantly greater progression of UCL thickness over 3 years.
Methods
Inclusion/Exclusion Criteria
Our institutional review board approved this study (Thomas Jefferson University No. iRISID-2022-1198) before we analyzed any collected data. SUS was performed on professional baseball pitchers from a single team over 18 years (2002-2020). In total, 1154 SUSs were performed on 651 unique asymptomatic pitchers. Baseline measurements were taken using players’ first available SUS, with remaining nonbaseline evaluations not considered for this primary analysis to be consistent across all patients (n = 503). The exclusion criteria were as follows: (1) incomplete measurements (n = 3); (2) missing and unobtainable descriptive data (n = 2); and (3) players who were not drafted (n = 263). Those who were not drafted were excluded, as there are reasons for draft ineligibility despite performance ability that could not be controlled for; thus, including nondrafted players would skew the comparison of performance levels that draft grouping takes into account. After appropriate exclusion, 383 professional pitchers and their respective initial SUSs were included in the final analysis (Figure 1).
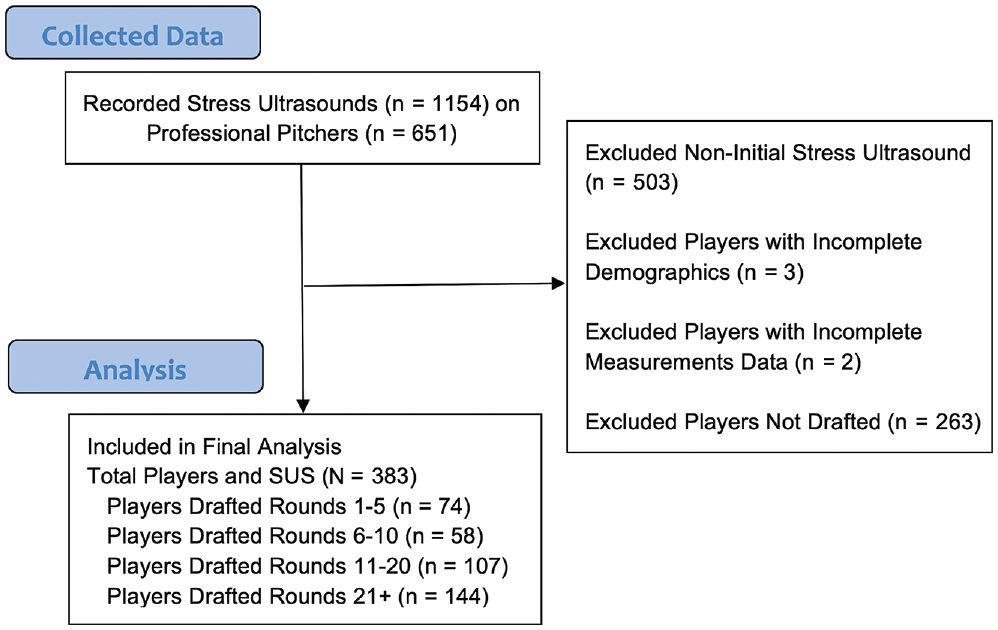
Flowchart of stress ultrasound (SUS) and player screening for initial SUS analysis.
In addition to comparing initial measurements, a 3-year progression on SUS was also analyzed when available (Figure 2). If a player had multiple sets of SUSs separated by 3 years (ie, 2012-2015 and 2013-2016), the earliest set of available measurements was used for analysis.
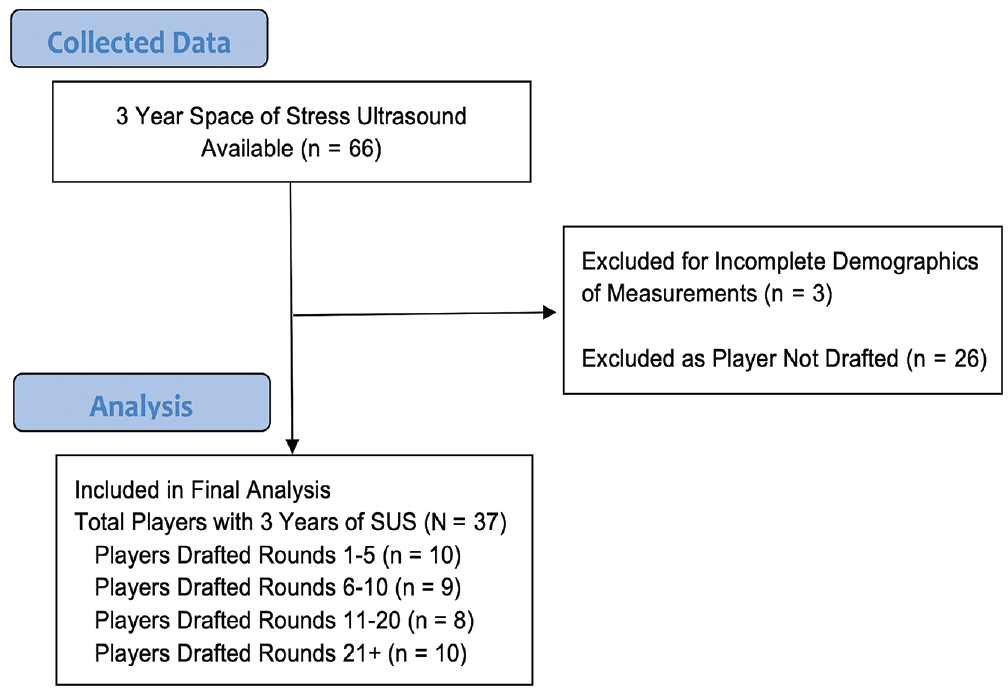
Flowchart of stress ultrasound (SUS) and player screening for 3-year progression SUS analysis.
Imaging Technique
Player evaluation involving SUS of both arms was performed at preseason training sessions over 18 years. SUSs were performed after the same standard sonography technique described by Ciccotti et al. 11 All participants were imaged by a single, experienced musculoskeletal radiologist who was a codeveloper of the current measuring technique utilizing a multifrequency 13-MHx linear-array transducer (SonoSite MicroMaxx or M-Turbo; SonoSite) and standard acoustic coupling gel. Players’ right elbows were placed at 30° in a standardized instrumented device (Telos), with the precise angle measured with a digital goniometer and the longitudinal axes of the forearm and upper arm. Thirty degrees was selected because (1) the UCL has been demonstrated to be the primary restraint against valgus stress at this angle of elbow flexion, and (2) the standardized stress device can consistently apply appropriate stress at lower degrees of elbow flexion. In this position, the thickness of the anterior band of the UCL at the middle portion was measured. Moreover, the ulnohumeral joint space at the anterior band was measured at rest and with a 150 N stress applied (Figure 3). Images were evaluated for calcification, tears, hypoechoic foci, and osteophytes at the same time. After measurements on the right arm, the same process was repeated, and measurements of the left elbow were performed. The order in which limbs were examined was not randomized by arm dominance, to assure consistency and avoid errors in record keeping across the thousands of examinations performed throughout the collection period. Measurements were taken once by the sonologist utilizing the SUS screen electronic calipers with a precision of 0.1 mm. During SUS measurements, player descriptive data—including age and hand dominance—was recorded with the individual's measurements.
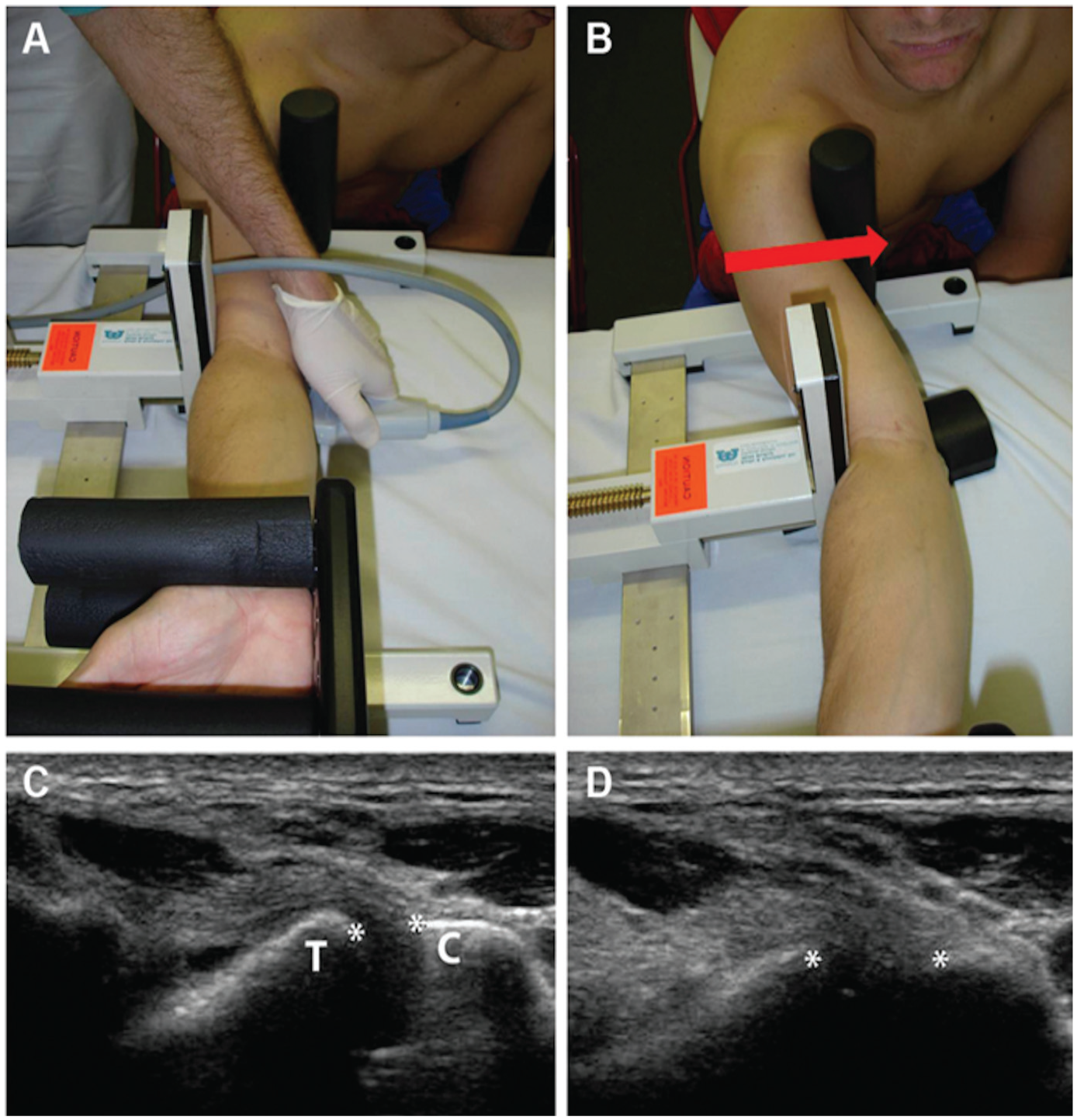
Clinical and ultrasound images at rest and with valgus stress in the pitching arm of an asymptomatic professional baseball pitcher. (A) Stress ultrasound of the elbow in the Telos device. (B) Valgus stress is being applied to the elbow by the Telos device. (C) At rest, the ulnohumeral joint (asterisks) measures 4.2 mm. (D) With valgus stress applied by the Telos device, the ulnohumeral joint (asterisks) widens to 7.9 mm. C, coronoid process; T, trochlea. (Reprinted with permission by SAGE Publications. Ciccotti MG, Atanda A, Nazarian LN, Dodson CC, Holmes L, Cohen SB. Stress sonography of the ulnar collateral ligament of the elbow in professional baseball pitchers: a 10-year study. Am J Sports Med. 2014;42(3):544-551. 11 )
Player Grouping
An internet search of identified pitchers was performed to collect player characteristics, including the round in which players were drafted. All descriptive data for MLB players were collected using publicly available information (https://baseball-almanac.com/). 4 Players were grouped according to the rounds in which they were drafted (draft rounds 1-5, 6-10, 11-20, 21+). Grouping was done similar to draft comparison in a study by Conforti et al, 12 which was done to contrast different levels of performance, with greater pitching ability and potentially greater strain on the UCL in players drafted earlier.
Calculated Measurements
Side-to-side differences in ultrasound measurements were calculated to analyze the effect of pitching on the dominant (throwing) arm. In each player, nondominant arm measurements were subtracted from those taken in the dominant (throwing) arm. We use the term relative to describe these calculated side-to-side differences. The primary outcomes of interest were relative UCL thickness and relative ulnohumeral joint space laxity (ie, joint space distance at rest subtracted from joint space distance under stress). For relative UCL thickness, a positive result indicates that the dominant arm UCL was thicker than the nondominant arm UCL. For relative joint space laxity, a positive result suggests greater laxity in the dominant arm than the nondominant arm. Relative UCL thickness was used for analysis in this study instead of absolute measurements. This was done as relative measurements allow for comparison between groups while accounting for variations between groups in baseline measurements.
The 3-year progression of ultrasound measurements was also performed to assess the cumulative changes in the UCL of professional baseball pitchers. As with the comparison of initial SUS measurements, progressive changes in relative UCL thickness and relative laxity were calculated such that a positive value indicates that the dominant arm UCL saw a relative increase in thickness/laxity during the study period compared with the nondominant arm.
Statistical Analysis
The Mann-Whitney U test or the t test was used to compare continuous data, and the chi-square test or the Fisher exact test was used to compare categorical data. The side-to-side difference was found by subtracting the nondominant side measurements from the dominant side measurements. A logistic regression using the presence of any pathologies as the dependent outcome was also created to assess its relationship with other variables. P < .05 was considered significant. All statistical analyses were done using R Studio Version 3.6.3.
Results
Initial Ultrasound Measurements
Descriptive data for the 383 included professional baseball pitchers who were drafted into a professional affiliation are reported in Table 1. Players were grouped according to their draft round. There were no differences in age at the time of the SUS (P = .850), number of previous spring training (P = .063), or handedness (P = .177).
Descriptive Data of Players Included in the Overall Analysis, Grouping by Draft Rounds a
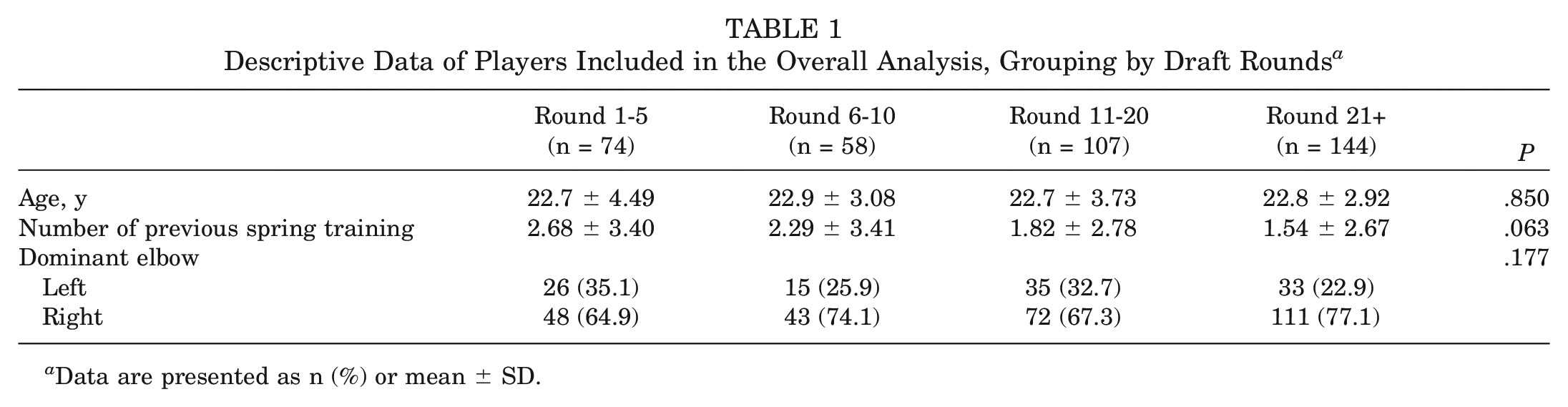
Data are presented as n (%) or mean ± SD.
No significant relationship was observed between the draft round and the relative UCL thickness (P = .932) or relative laxity (P = .996). No significant relationship was found between the draft round and the presence of pathology detectable on SUS (P = .642). Looking at specific pathologies, no difference was detected in the rate of detectable calcifications (P = .531), tears (P≥ .999), hypoechoic foci (P = .198), or osteophytes (P = .750). However, in cases where calcifications were present, there was a significant difference in the size of calcifications between groups (P = .013) (Table 2).
Side-to-Side Comparison of Dominant and Nondominant Arm Initial Ultrasound Measurements a
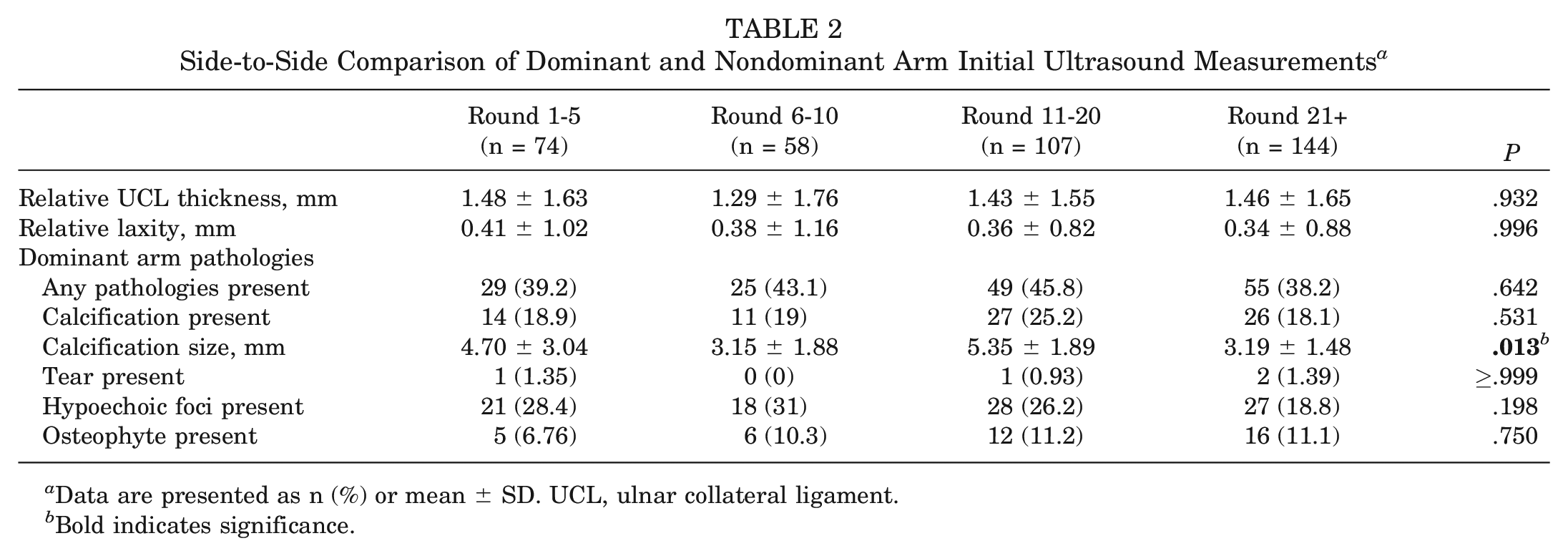
Data are presented as n (%) or mean ± SD. UCL, ulnar collateral ligament.
Bold indicates significance.
A logistic regression utilizing the presence of pathology as the dependent outcome was performed to control for age, handedness, relative UCL thickness, and relative laxity. Increased relative UCL thickness was found to be significantly associated with the presence of any pathology on SUS (odds ratio, 1.45; 95% CI, 1.26-1.69; P < .001).
3-Year Progression
Analysis of the 37 players available for the 3-year follow-up is reported in Table 3.
Descriptive Data for Players Included in the 3-Year Analysis, Grouping by Draft Rounds a
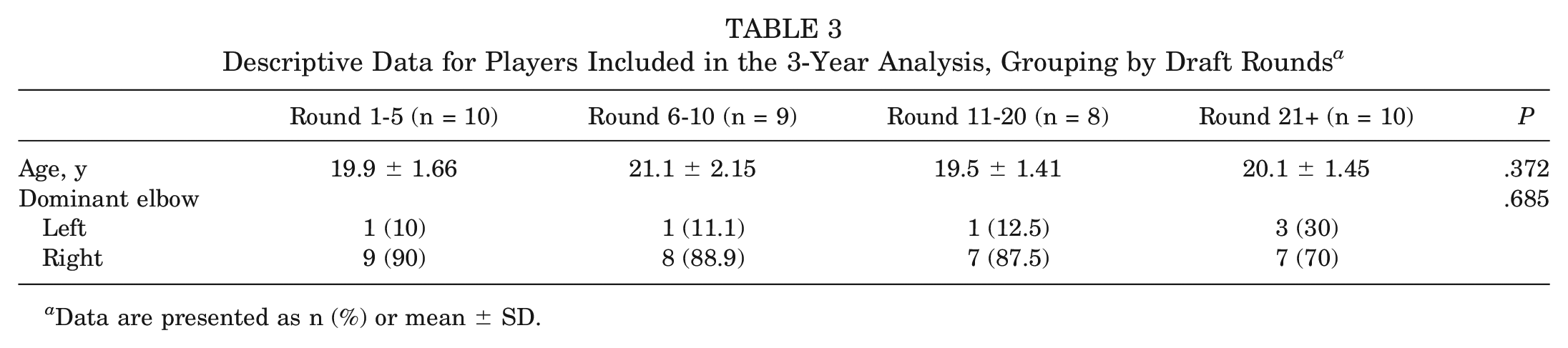
Data are presented as n (%) or mean ± SD.
No significant relationship was observed between the draft round and the progression of relative laxity or relative UCL thickness.
The progression of pathology observed on SUS was also analyzed (Table 4). No significant difference was found in the clinical progression (never present, developed, resolved, present at both times) of calcifications (P = .202), tears (P = .216), hypoechoic foci (P = .083), or osteophytes (P = .619). Moreover, when calcifications were present at both time points, they did not undergo a significant change in size (P = .823).
Comparison of Dominant and Nondominant Arm Stress Ultrasound Measurements Over 3 Years a
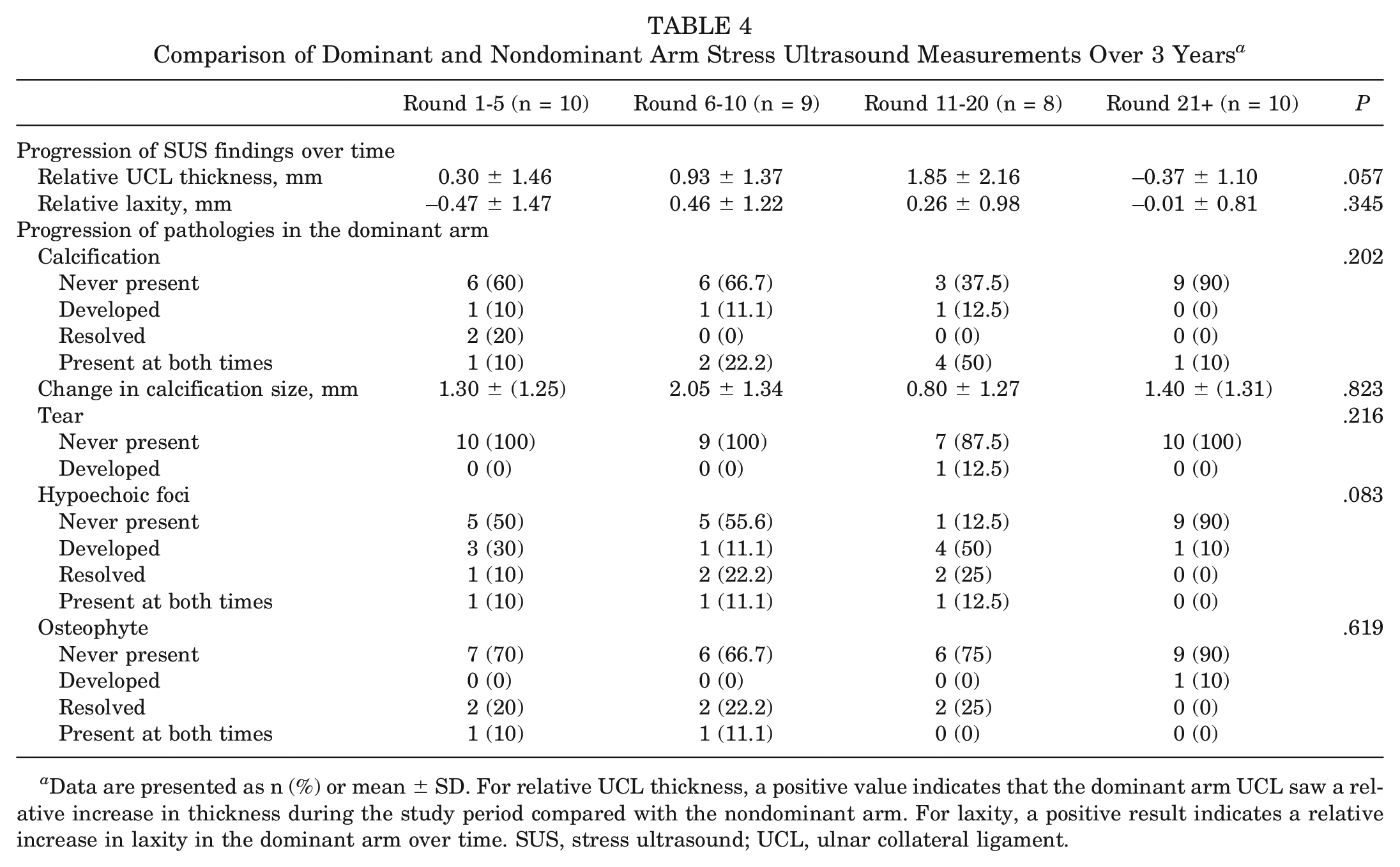
Data are presented as n (%) or mean ± SD. For relative UCL thickness, a positive value indicates that the dominant arm UCL saw a relative increase in thickness during the study period compared with the nondominant arm. For laxity, a positive result indicates a relative increase in laxity in the dominant arm over time. SUS, stress ultrasound; UCL, ulnar collateral ligament.
Discussion
The primary finding of this study was that no significant relationship was found between MLB draft round and UCL thickness or ulnohumeral joint laxity as determined by SUS. Similarly, the 3-year progression of SUS findings did not significantly differ by draft round. This rejects the hypothesis that higher-performing players taken earlier in the draft would have higher rates of elbow pathology on SUS.
The MLB draft is one of the primary routes for players to become professional baseball players in the United States. Higher-performing players are typically drafted in earlier rounds. Previous studies have demonstrated that those drafted in earlier rounds are more likely to play in the major leagues for ≥3 years. 22 In theory, there are fundamental differences between these higher-performing pitchers. They may, for example, pitch at higher velocities, which, in theory, means these players impart greater strain on their UCL during training and competitive appearances. 12 Over time, adaptive changes may occur in response to the repetitive forces that baseball pitching exerts on the elbow. Although it is possible that there may be no relationship between the elbow's adaptive response to stress and performance, it is also possible that examination of the UCLs may reveal differences in players’ physiological ability to adapt to stresses, which has allowed them to achieve their respective level of performance and do so for longer.
UCL Thickness
Previous studies have examined the side-to-side difference in UCL thickness in throwing athletes to assess adaptive changes. One study of 102 youth pitchers reported a mean relative UCL thickness of 0.29 mm (0.31 mm in the 12- to 14-year-old group and 0.24 mm in the 15- to 18-year group), although the authors did not test for the significance of these values. In their study, authors also found a significantly thicker UCL in patients who threw >67 pitches per appearance, >5 innings per appearance, and had >5.5 years of experience pitching than players who did not (P < .001 in all cases). 2 Another study of 127 professional pitchers supported this finding, reporting that UCL thickness correlated with years of pitching experience but found no correlation between UCL thickness and age. 3 In the present study, professional pitchers (mean age, 22.8 years) had a mean relative UCL thickness of 1.43 mm, with no significant difference between players of different groups, suggesting that the round players were drafted did not affect the extent of adaptive change. Furthermore, although the number of previous spring training that players participated in was similar between groups (P = .063), the design of this study did not allow for further analysis of confounding factors such as pitch count or innings per appearance made.
Further examination was done to compare the adaptive changes of these players over a standardized 3-year span. Previous studies by Keller et al 23 and Khalil et al 24 reported significant increases in UCL thickness after just 1 season. However, the clinical significance of these findings is debatable. For example, 1 study 24 found that after an offseason, the significant increase in UCL thickness that occurred over the single season returned to the baseline and was not significantly different from the UCL thickness of the previous preseason. In the present study, although the mean relative thickness in our cohort increased by a mean of 0.61 mm during the 3-year follow-up, measurements did not differ by draft round.
There needs to be more literature exploring the details surrounding ligament hypertrophy and whether it truly represents advantageous changes to the soft tissue of the elbow. Previous studies of the anterior cruciate ligament have found increases in the ligament cross-sectional area in the legs of athletes who were more likely to exert significant mechanical load through 1 knee than the other— figure skaters landing on the same leg repetitively and springboard divers diving from the same leg relatively—compared with contralateral nonloaded legs.5,17 Even though more studies are necessary to identify whether the increased thickness of ligaments may prevent or promote injury, it is reasonable to suggest that adaptive changes to the soft tissue structures offer some benefit to cope with mechanical stress and provide stability to the respective joint. Studies of the UCL have found that increased thickness significantly correlates with decreased relative joint spacing, supporting this concept. 35
Joint Laxity
Regarding joint laxity, a previous study showed that in both preadolescent and collegiate pitchers, after 60 pitches, a significant increase in medial elbow joint space gapping was observed. 25 Similarly, Ciccotti et al 11 reported a significantly increased laxity in the dominant arm of pitchers compared with the nondominant arm, finding a weak positive correlation between UCL thickness and joint space width under stress. In the present study, no significant difference was found between draft round groups despite higher relative laxity in the dominant arms compared with the nondominant arms, indicated by positive values for these measurements. This indicates there is no association between players’ drafted grouping and the relative laxity of the ulnohumeral joint.
To better understand the adaptive changes of the elbow, changes in laxity can be evaluated over time. Across 1 playing season, Khalil et al 24 found no significant changes in joint laxity. In the present study, we expanded on this finding by looking at the progression of relative joint laxity over 3 years. Although there was a mean increase of 0.04 mm across the entire cohort, there was no difference in the progression of relative laxity by players drafted in different rounds. Notably, a previous cross-sectional study by Rijke et al 30 demonstrated that a joint laxity of ≥0.5 mm is necessary to detect the presence of tears in the UCL when 150 N of valgus stress is applied. This would indicate that the mean increase of 0.04 mm in laxity observed in players over 3 years is likely clinically insignificant. 18 In addition, the changes in relative laxity that were detected all fall below the SUS-documented gapping that was observed in previous cadaveric studies after complete transection of just the anterior or the anterior and posterior oblique ligaments of the UCL (1-2 mm vs 4-10 mm, respectively).14,26
Pathologies
In addition to the SUS-measured differences in UCL thickness and joint laxity, previous studies have examined differences in the presence or development of hypoechoic foci or calcifications in the throwing arms of athletes. In examining 26 professional pitchers, Nazarian et al 28 observed an increased prevalence of hypoechoic foci and calcifications in the anterior band of the throwing arm with SUS. This was consistent with a larger study of 368 professional pitchers by Ciccotti et al, 11 which similarly found that hypoechoic foci and calcifications were more observed in the dominant arm on SUS. In the present study, there was no difference in the presence of pathology on initial SUS. However, when present, there was a significant difference between drafted groups in terms of the size of calcifications. Additional regression revealed a positive correlation between any pathology in the dominant arm and UCL thickness. Looking at the initial and the final SUS ≥2 years apart, Ciccotti et al 11 found no difference in the rate at which hypoechoic foci or calcifications presented in the dominant arm. This is consistent with the findings of the present study. The appreciation of intraligamentous calcification and hypoechoic regions within the UCL on SUS may indicate chronic or repetitive stress on the soft tissues of the elbow from the repetitive throwing motion.20,21 Although not specifically predisposing a player to ligament injury, UCL changes may indicate an adaptive response of such structures in response to stress. This was suggested in a previous study, 1 which found posteromedial olecranon osteophytes in professional baseball players undergoing UCL surgery. The authors of that study also found that those players with posteromedial osteophytes had the highest rates of reoperation compared with players who did not. 1 Further investigation is necessary to determine whether posteromedial spurring can predict complete or clinically significant partial ligament tears.
Limitations
This study has limitations that should be considered when examining the results. First, although players in this study were compared depending on the round in which they were drafted, there are other nonperformance-related factors that also play a role in a player's selection. This could not be accounted for and, as such, introduces a potential source of error. Second, previous studies have documented the correlation between UCL adaptations over a season and a player's body mass index, the number of bullpen sessions an athlete performs a week, and the percentage of off-speed pitches thrown that could not be collected because of the retrospective design of this study. 2 Third, the injury data for players >18 years in which these data were collected were unavailable, as such correlations could not be done between the SUS measurements or the progression of these measurements and injuries of the UCL that these athletes sustained or necessary surgeries they underwent. A future study that includes additional descriptive and injury data would allow for a further understanding of adaptive UCL changes in professional pitchers and the progression of these adaptations in the context of injuries. Last, only 9.7% (37/383) of pitchers included in the primary analysis were also included in the secondary analysis of the 3-year progression data. This reflects that in professional baseball, many players in major and minor league teams may move teams, be released, or retire from year to year. As a result, only a small pool of players is available for multiyear assessments such as the one performed here. Therefore, the power of this secondary analysis may be low, and its outcomes should be viewed cautiously.
Conclusion
Higher-performing pitchers are drafted earlier in the MLB draft. This may be attributable to peak pitch velocity, in-game performance, visibility gained during player showcases, or other sport-specific variables. However, despite this, there was no significant relationship between draft round and adaptive changes to the elbow or specific properties of the UCL on SUS.
Footnotes
Submitted April 26, 2023; accepted September 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.B.S. has received research support from Major League Baseball and DJO. R.A.J. has received support for education from Smith & Nephew, Liberty Surgical Inc, and MedInc of Texas, and travel expenses from Arthrex Inc. S.B.C. has received research support from Arthrex Inc and Major League Baseball; consulting fees from CONMED Linvatec, Zimmer, GlaxoSmithKline, Ipsen Biopharmaceuticals Inc, Merck Sharp & Dohme Corporation, and Bayer HealthCare Pharmaceuticals Inc; nonconsulting compensation from Heksinn Therapeutics and Exelixis; and royalties from Zimmer and Slack Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.