
Abstract
Background:
The role of arthroscopic Latarjet as a revision surgery after failed arthroscopic Bankart repair has yet to be established.
Purpose:
To compare clinical outcomes, recurrences, and complication rates of arthroscopic Latarjet as a revision procedure after failed arthroscopic Bankart repair versus arthroscopic Latarjet as a primary procedure.
Design:
Cohort study; Level of evidence, 3.
Methods:
This is a retrospective study of prospectively collected data of patients who were diagnosed with anterior shoulder instability and underwent arthroscopic Latarjet stabilization between 2009 and 2018. Patients were separated into 2 groups depending on whether Latarjet was performed after a previous instability surgery (revision) or as a primary surgery (primary). Rowe score, Western Ontario Shoulder Instability Index (WOSI), Constant-Murley Shoulder Outcome (CMSO) score, and Single Assessment Numeric Evaluation (SANE) were assessed pre- and postoperatively with a minimum 24 months of follow-up. In addition, pre- and postoperative levels of sports activity, dislocations, subluxations, and complications were assessed.
Results:
A total of 97 patients (n = 62 revision; n = 35 primary), with a mean age of 31.0 ± 8.8 and 29.4 ± 7.6 years old in the revision and primary Latajet group, respectively, met the inclusion criteria. The mean follow-up in the revision group was 32 months (24-53) and 35.5 months (27.7-42.2) in the primary Latarjet group. No significant differences between groups were observed in Rowe score (revision = 91.4, primary = 94.1; P = .223), CMSO score (revision = 90.7, primary = 94; P = .105), and SANE (revision = 85.8, primary = 87.3; P = .683) postoperatively. However, the postoperative difference in the WOSI score between the revision and primary Latarjet groups was nearly significant (510 ± 334 vs 403 ± 343, respectively; P = .05). Four (6.4%) postoperative dislocations were reported in the revision and 1 (2.8%) in the primary Latarjet group (P = .14). Patients in the revision group had a lower return to the previous level of sports participation (P = .008) and decreased external rotation with the arm by the side compared with the primary Latarjet group (P = .000).
Conclusion:
Arthroscopic Latarjet as a revision surgery is a reasonable surgical option in failed Bankart repair cases. The decision to perform arthroscopic Latarjet stabilization as a revision surgery should not be influenced by the potential risk of future complications as it provides comparable clinical outcomes to the primary Latarjet procedure with a low postoperative recurrence rate. However, a decreased level of postoperative sports participation and external rotation with the arm by the side can be expected.
Arthroscopic Bankart repair remains the most frequently performed therapeutic option for recurrent anterior shoulder instability; however, higher recurrence rates have been reported in young patients who participate in collision sports or sustain a critical bony defect. 2 This finding has led to increasing focus on alternative therapeutic options such as the Latarjet procedure.3,4 The Latarjet procedure as primary surgery has even better results than arthroscopic Bankart repair when it comes to postoperative instability (3% vs 28.4%).1,11,13,17 Despite these satisfactory results, there has been controversy about performing the open Latarjet procedure as a primary surgery. The main argument is that unlike arthroscopic Bankart repair, Latarjet is a nonanatomic procedure. Second, the Latarjet procedure has mainly been performed as an open surgery. Third, Latarjet has been associated with a higher postoperative complication rate, comprising up to 30%. 28 Furthermore, the risk of secondary arthropathy over the long term also has been highly debated. 25 In addition, the failed Latarjet technique can be challenging to treat, and revision surgeries of this procedure have shown even poorer outcomes than primary cases. 6 Finally, the Latarjet procedure as a revision surgery has demonstrated satisfactory outcomes,5,26 and many surgeons feel like “burning bridges” when performing the Latarjet procedure as primary surgery. The aforementioned is enough argument to support the idea of saving the Latarjet procedure for revision cases. However, several recent publications have reported inferior outcomes of the open Latarjet after failed labral repair compared with primary Latarjet surgery, suggesting that the revision Latarjet may be better suited as primary surgery for anterior shoulder instability.10,22,30,31 Conversely, others have failed to find a significant difference between primary and revision Latarjet repair. 22
The open Latarjet procedure has been widely successful over the decades, but arthroscopic Latarjet repair as a revision surgery has also been on the rise. 3 However, outcomes of the arthroscopic Latarjet procedure after failed arthroscopic Bankart repair are still a matter of debate and merit further investigation. To our knowledge, there are no studies comparing results of arthroscopic Latarjet repair as a revision surgery versus outcome of the arthroscopic Latarjet procedure performed as primary surgery.
The purpose of the current study was to compare the postoperative clinical outcomes, return to athletic activity, and complication rates between the arthroscopic Latarjet as a primary surgery versus a revision procedure after failed arthroscopic Bankart repair. Our hypothesis was that there would not be differences between the 2 described procedures.
Methods
Study Design and Patient Selection
A retrospective and comparative cohort study of prospectively collected data was performed. Local ethics committee approval was obtained before undertaking the study (IIS-FJD EC study code EO 44-11). Sixty-two patients who underwent an arthroscopic Latarjet procedure for recurrent anterior glenohumeral instability after failed arthroscopic Bankart repair in a third-level hospital between 2010 and 2018 were included as a therapeutic group (revision group). Patients were matched for age, sex, and handedness (dominant/nondominant) with 35 patients who had primary Latarjet repair (primary group), the included patients were matched and were selected from a larger group. All cases were operated on by the same senior surgeon (E.C.) with the patient in the beach-chair position following the technique described by Lafosse et al, 16 which uses a specific instrument set and screws (De Puy Mitek). The capsulolabral tissue was dissected to allow better visualization while preparing the glenoid bone and then later transferred and reattached on the glenoid rim. Clinical and radiological data were prospectively analyzed with a mean 38-month follow-up.
The inclusion criteria for this study were as follows: patients who (1) were aged ≥18 years with or without hyperlaxity, (2) underwent arthroscopic stabilization between 2009 and 2018 for recurrent anterior glenohumeral instability, and (3) had a minimum of 2-year follow-up.
Exclusion criteria were previous Latarjet surgery, open Latarjet revision procedure, posterior or multidirectional instability, superior labrum lesion, significant glenohumeral osteoarthritis (ie, grades 3 and 4) according to the Ogawa classification, 18 avulsion fractures of the greater tuberosity, rotator cuff tears, pathologic involvement of the long head of the biceps requiring tenotomy/tenodesis, and patient noncompliance.
Of 146 patients who underwent the arthroscopic Latarjet procedure between January 2009 and December 2018 at our institution, 65 were patients with failed Bankart repair who underwent arthroscopic Latarjet stabilization as a revision procedure. Three patients were excluded from the final analysis because 2 had a history of multidirectional instability and 1 patient was lost to follow-up. The remaining patients were matched with 37 patients who underwent arthroscopic Latarjet as primary surgery. However, 2 were excluded because of incomplete clinical and radiologic follow-up as they moved to another city. Thus, the final analysis included 62 patients in the revision Latarjet group and 35 in the primary Latarjet group. Figure 1 presents the flowchart of the study.
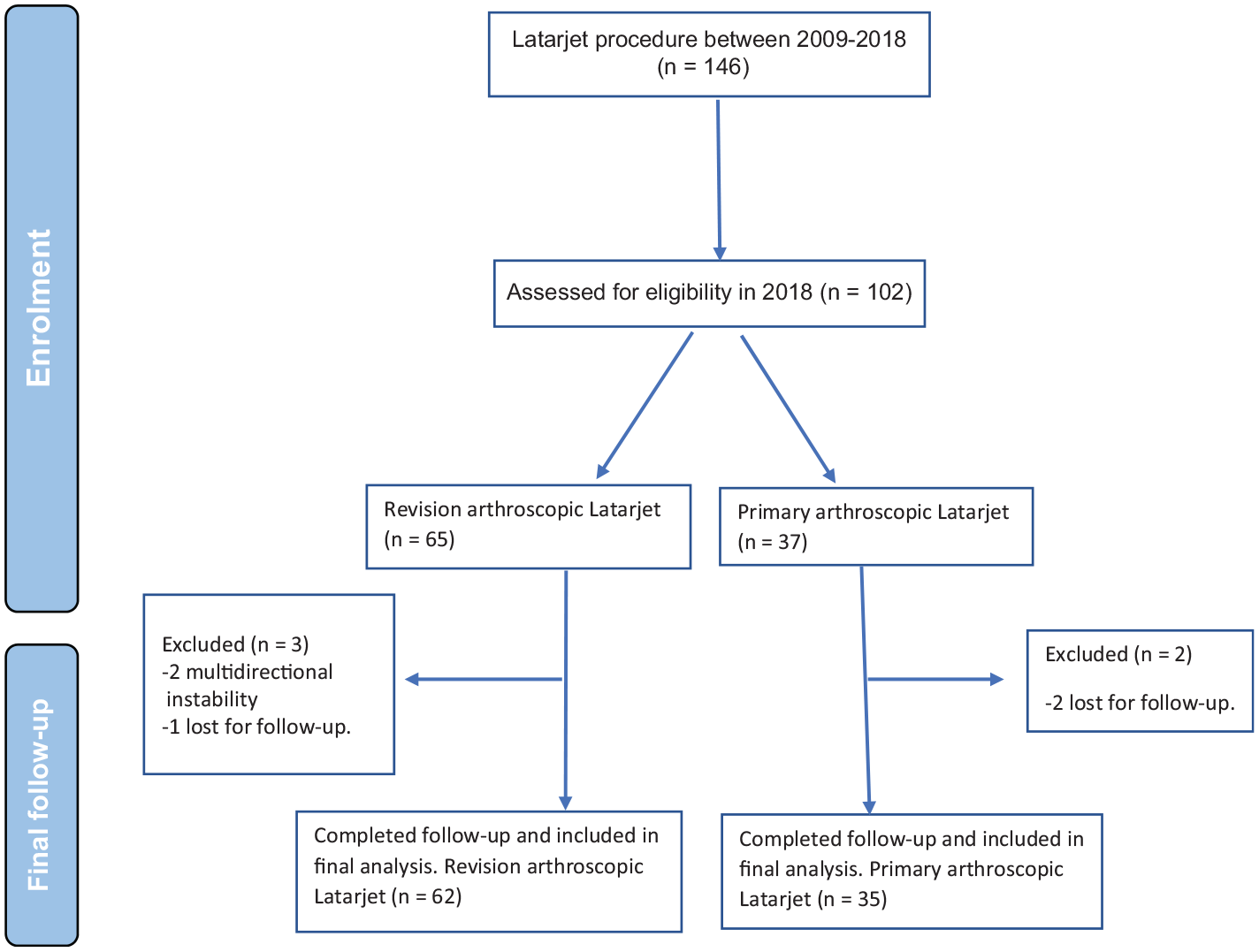
Flowchart outlining the steps from enrollment to final follow-up.
The indication for a primary arthroscopic Latarjet procedure was defined by the presence of a lesion on the anterior aspect of the glenoid rim >15% of the maximal anteroposterior diameter, the presence of an off-track Hill-Sachs lesion, and participation in contact or collision sports. Revision arthroscopic Latarjet was performed after a failed arthroscopic Bankart repair in patients who met the same indications for a primary arthroscopic Latarjet (ie, critical glenoid bone loss, off-track Hill-Sachs lesion, and participation in contact or collision sports). 5
Clinical and Radiologic Assessments
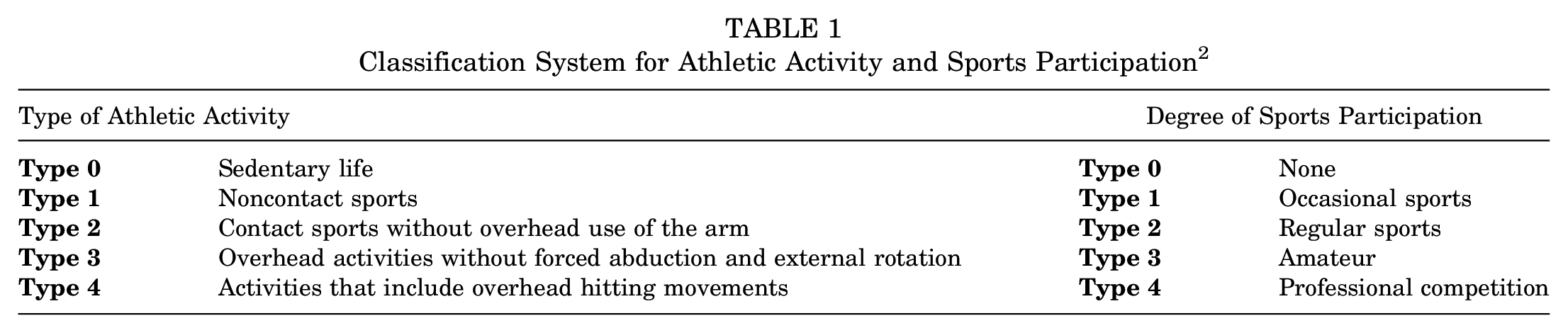
Medical records of all eligible patients were reviewed by 2 independent reviewers in a blinded fashion and independent from the surgeon performing the intervention. The following data were collected: patient demographics, number of episodes of dislocation before and after surgery, time lapse between the first dislocation and surgery, arm dominance, occupation, shoulder hyperlaxity, type and level of athletic activity, and sports participation. Type of athletic activity and degree of sports participation were classified according to Calvo et al, 2 as represented in Table 1.
Classification System for Athletic Activity and Sports Participation 2
Clinical outcomes at a mean of 38 months postoperatively included validated outcome objective assessment using the Rowe and the Constant-Murley Shoulder Outcome (CMSO)7,24 scores as well as subjective patient-reported outcome measures (PROMs) following the Spanish validated version of the Western Ontario Shoulder Instability Index (WOSI) 33 and the Single Assessment Numeric Evaluation (SANE). 15 The WOSI score was used as it is disease specific, is widely used, and has the best rating of psychometric properties. A difference of at least 9.7 and 151.9 in the score has been demonstrated to be clinically relevant using Rowe and WOSI scores, respectively.14,19 On the basis of these data and accepting an α risk of 0.05 and a β risk of 0.2 in a 2-sided test, we determined that ≥17 participants were necessary in each group to detect a statistically significant difference of ≥9.7 points on the Rowe score and 151.9 points on the WOSI score.
Those cases with postoperative subluxation or dislocation were considered recurrence. Range of motion, including external rotation with the elbow at the side and the arm in 90° of abduction in the sitting position, was also measured using a goniometer pre- and postoperatively in all patients.
Pre- and postoperative radiologic assessments were standardized for all included patients. True anteroposterior, Y, and axillary views of the glenohumeral joint as well as a computed tomography (CT) scan were taken in all cases to quantify bone defects and to assess the grade of osteoarthritis. A shoulder and elbow fellow (C.C.), previously trained by a senior musculoskeletal radiologist, carried out all bone defect measurements on a CT scan (Siemens Somatom Definition Flash 128 slice CT Dual Energy; Siemens Healthcare) by using a DICOM (PACS) system and Syngo via imaging software (Siemens Healthcare). Glenoid bony Bankart and humeral head Hill-Sachs index were measured to quantify bone defects, as described previously.8,9 To do so, 2-dimensional sagittal images lateral to the level of the coracoid base were selected. Measurements included native glenoid diameter (D) and anterior glenoid defect (d) using the best-fit circle technique superimposed on the glenoid. Finally, the glenoid track (GT) was calculated (GT = 0.83 × D – d). Humeral measurements were performed on a 2-dimensional axial plane image at the level of the widest portion of the medial part of the Hill-Sachs lesion. Measurements to obtain the Hill-Sachs index included the bony bridge and the Hill-Sachs lesion. The Hill-Sachs index was calculated as the distance between the medial edge of the Hill-Sachs lesion and the insertion of the articular fibers of the rotator cuff. Bone defects were assessed on the imaging studies, while soft tissue abnormalities, such as capsulolabral pathology or biceps tendon involvement, were documented from the preoperative records.
Sagittal CT scan images were assessed at baseline and 6 and 12 months postoperatively to evaluate degree of graft union and osteolysis. Nonuninon was defined as the absence of the bony bridge between the coracoid graft and the glenoid. Osteolysis was evaluated by measuring the distance between each screw and the superior and inferior borders of the graft. A reduction of 1 mm in this distance was considered osteolysis.
The severity of glenohumeral osteoarthritis was graded using CT scans and according to Ogawa et al 18 (Table 2).
Ogawa et al 18 Classification System Describing Osteoarthritic Changes of the Glenohumeral Joint

Surgical Technique
All cases were operated on by the same senior surgeon with the patient in the beach-chair position under traction and according to the technique described by Lafosse et al 16 using a specific instrument set and screws (De Puy Mitek). Postoperatively, all patients underwent a similar postoperative protocol and wore a simple sling for 3 weeks. Afterward, range of motion exercises were prescribed as tolerated, and physical therapy was scheduled 6 weeks after surgery until mobility and strength were regained. Return to sports was allowed once the patient was pain free during a full shoulder range of motion and the strength was similar to that of preinjury level.
Statistical Analyses
Comparisons between groups were made using the chi-square test or Fisher exact test for nominal qualitative variables, the Wilcoxon rank-sum test for ordinal qualitative variables and quantitative variables with a nonnormal distribution, and the Student t test for quantitative variables with a normal distribution. Comparisons between pre- and postsurgery were made using the McNemar test for nominal qualitative variables, the Wilcoxon signed-rank test for ordinal qualitative variables and quantitative variables with a nonnormal distribution, and the paired samples Student t test for quantitative variables with a normal distribution. Normality of quantitative variables was tested by the Shapiro-Wilk test. A subgroup analysis was performed using the Fisher exact, Mann-Whitney, and Wilcoxon signed-rank tests due to smaller sample size. The Benjamini-Hochberg correction method was applied for postoperative clinical outcomes and sports participation to decrease the false discovery rate. We did not use Bonferroni correction because it is a very conservative method and thus increases the probability of type II error. All comparisons were made with a significance level of 5%. Statistical analyses were performed using R-3.6.0 (R Core Team).
Results
The revision group consisted of 62 patients, including 50 men (80.6%) and 12 women (19.3%) with a mean age of 31.0 ± 8.8 years (range, 18-45 years), who underwent arthroscopic Latarjet revision surgery after failed arthroscopic Bankart repair. At the time of revision surgery, 46 patients (74%) had undergone 1 previous stabilization, 12 (19.3%) had undergone 2, and 4 (6.4%) patients had undergone ≥3. Before the Latarjet procedure, 47 patients (75.8%) had sustained redislocations after a traumatic event, and the remaining patients had persistent pain and subjective instability that had an important influence on their activities of daily living.
The primary repair group consisted of 35 patients, including 32 men (91.4%) and 3 women (8.6%), who underwent primary arthroscopic Latarjet procedure. The mean age at the first glenohumeral dislocation was 21.6 years (range, 16-29 years) and 20.7 years (range, 18-27 years) in the revision and primary groups, respectively.
Both cohorts were comparable regarding baseline data except for the number of preoperative dislocations and the presence of an off-track Hill-Sachs lesion, which were significantly higher in the primary group. Table 3 summarizes the baseline data of the 2 therapeutic groups.
Comparison of Baseline Demographics, Patient Characteristics, and Preoperative Patient-Reported Outcome Measures Between the Revision Arthroscopic Latarjet Group and Primary Arthroscopic Latarjet a
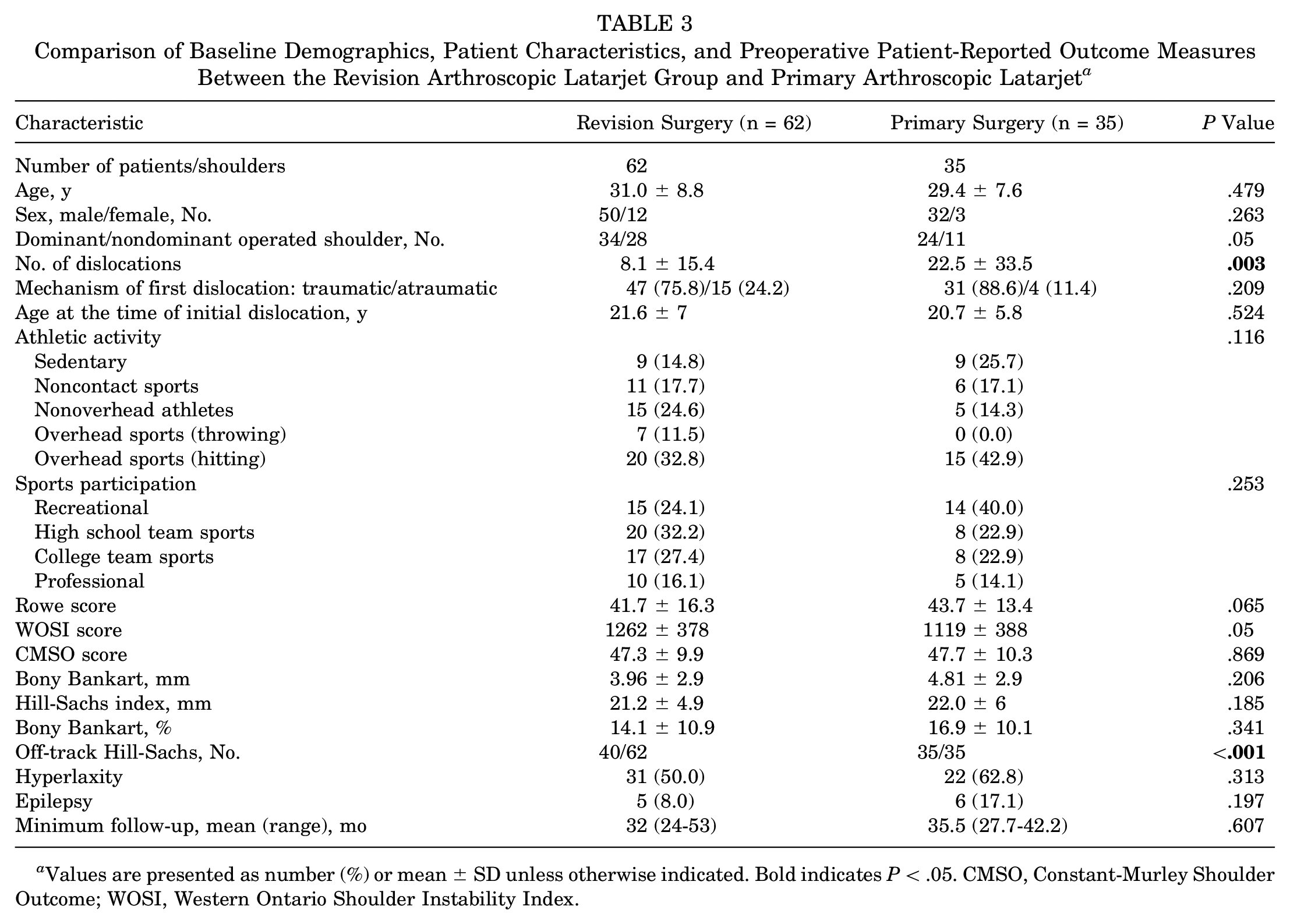
Values are presented as number (%) or mean ± SD unless otherwise indicated. Bold indicates P < .05. CMSO, Constant-Murley Shoulder Outcome; WOSI, Western Ontario Shoulder Instability Index.
Both groups of patients showed significant improvements in subjective outcome scores at final follow-up. Comparative pre- and postoperative PROMs are represented in Figures 2 and 3.
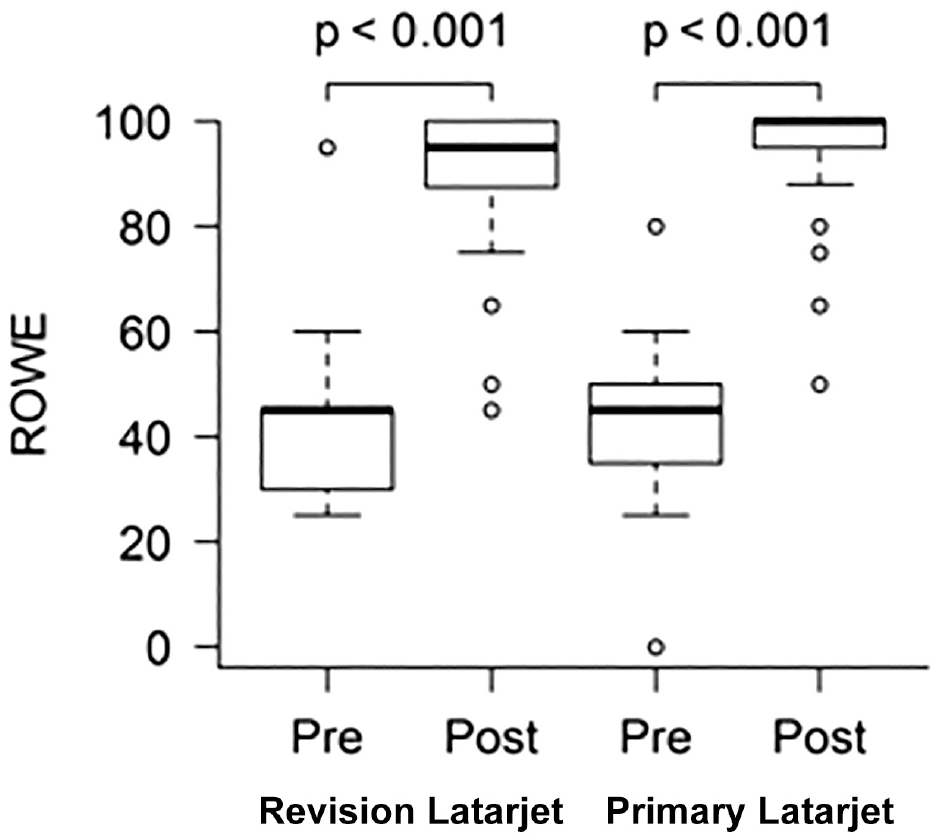
The mean pre- and postoperative outcomes in the Rowe score.
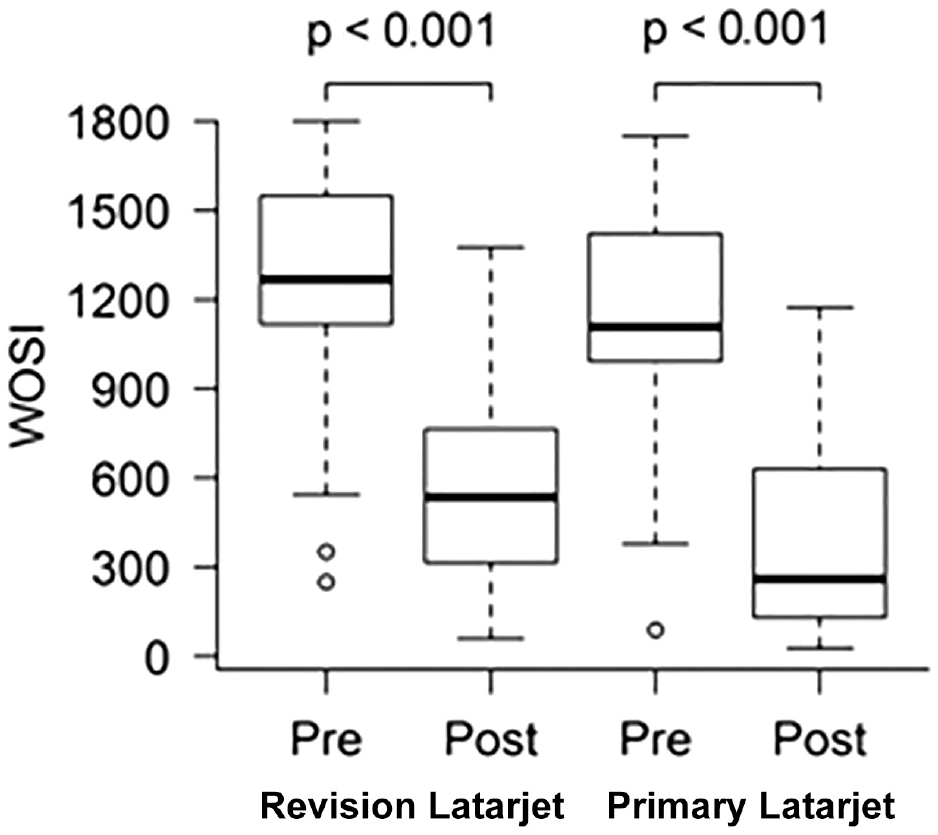
Comparative pre- and postoperative outcomes using the Western Ontario Shoulder Instability Index.
After a minimum follow-up of 32 and 35.5 months in the revision and primary group, 55 (88.7%) and 31 (88.6%) shoulders were subjectively graded as good to excellent using SANE (P ≥ .999).
The mean range of external rotation in 0° of abduction was 46.9° (range, 35-90°) and 69.8° (range, 45-90°) in the revision and primary Latarjet gtroup, respectively. External rotation in 90° of abduction averaged 81.1° (range, 60-90°), and the mean abduction was set at 83.2° (range, 73°-90°). The mean forward flexion increased from 155° (90° to 180°) preoperatively to 173° (155° to 180°) and 160° (90° to 180°) preoperatively to 180° (173° to 180°) in the revision and the primary surgery groups, respectively. Postoperative objective and subjective patient-reported outcomes and shoulder range of motion in both groups are shown in Table 4.
Postoperative Functional Outcomes, Shoulder Range of Motion, Activity Level, and Sports Participation a
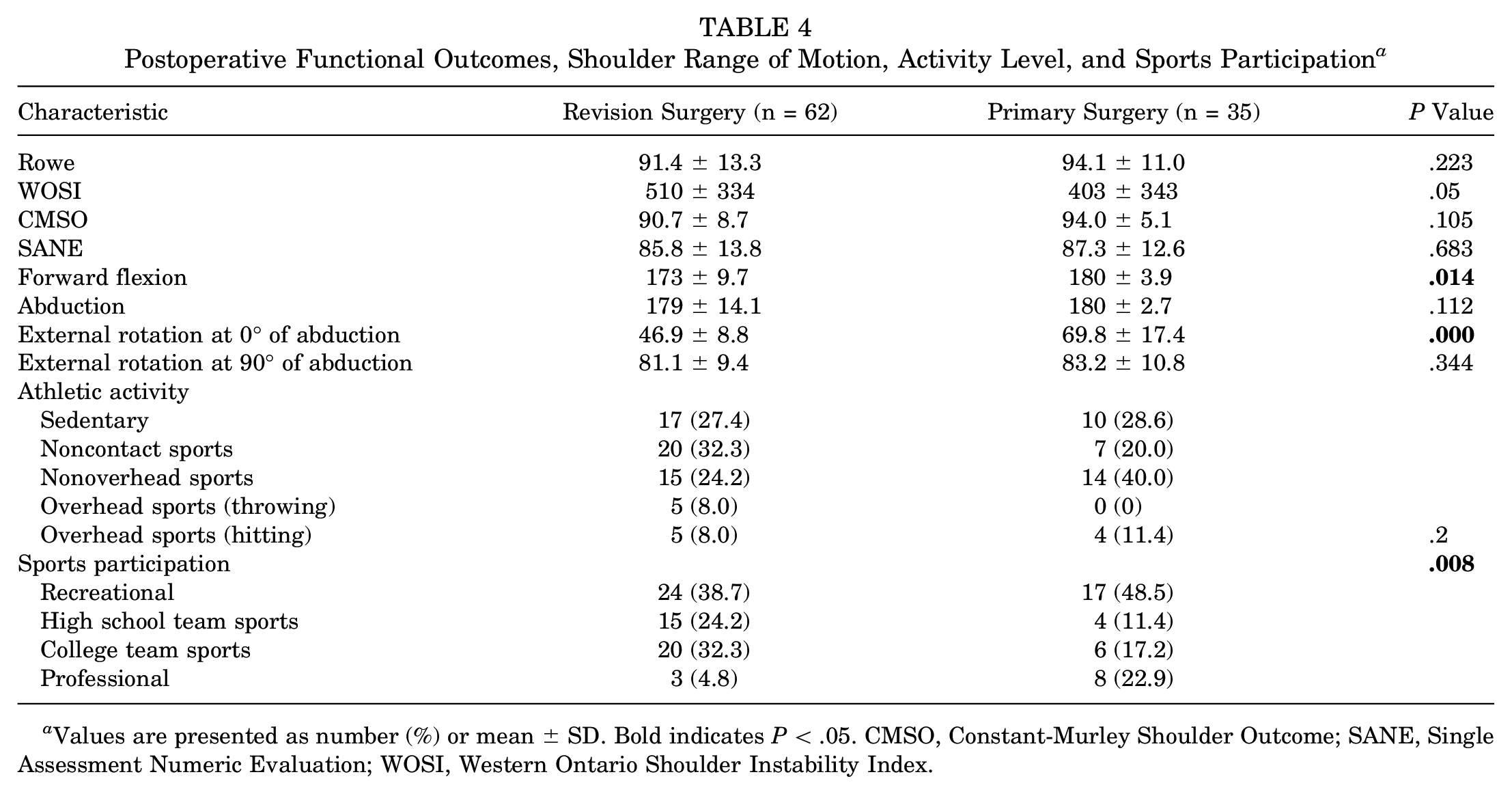
Values are presented as number (%) or mean ± SD. Bold indicates P < .05. CMSO, Constant-Murley Shoulder Outcome; SANE, Single Assessment Numeric Evaluation; WOSI, Western Ontario Shoulder Instability Index.
When the 2 groups were compared, there were no statistically significant differences in any of the assessed postoperative functional scores or in the postoperative range of motion, except for the forward flexion and external rotation with the arm at the side, which were higher in the group of patients who underwent the Latarjet as a primary procedure. No statistically significant differences between groups were observed regarding the postoperative athletic activity level (Figure 4). However, a decreased level of sports participation was observed in the revision group (Figure 5).
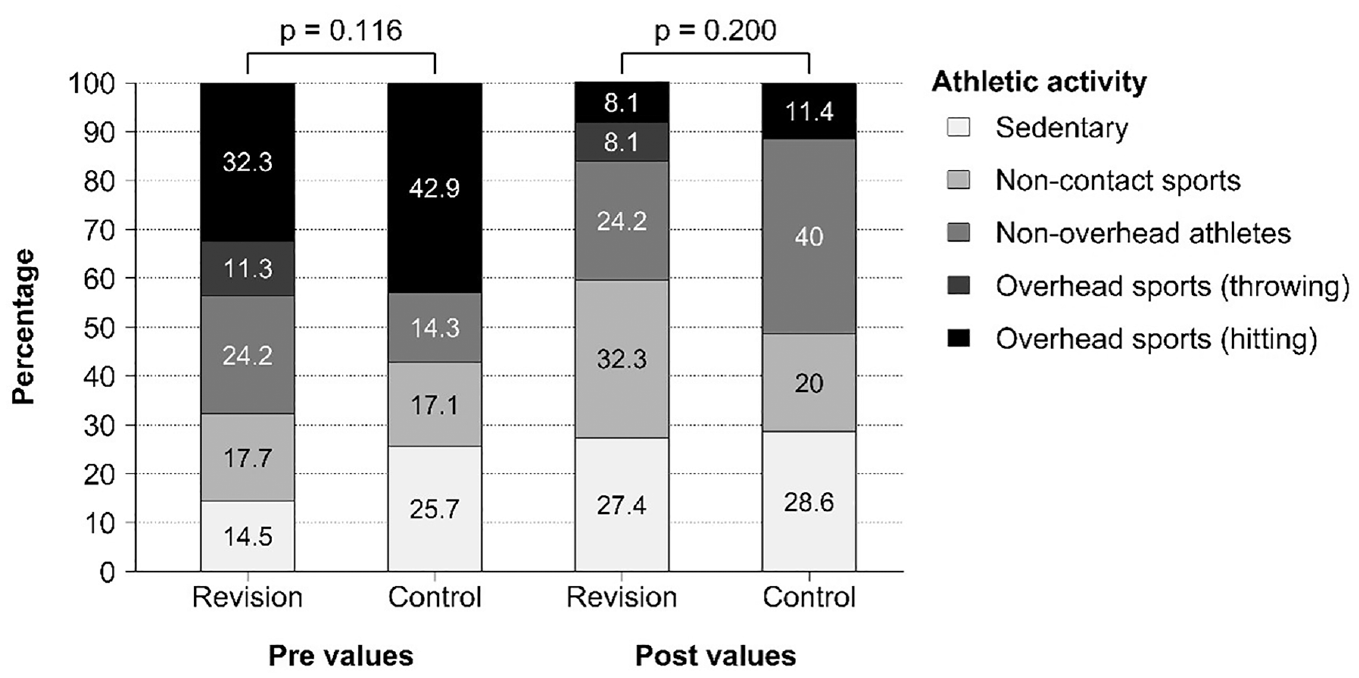
Comparative pre- and postoperative athletic activity levels between the study groups.
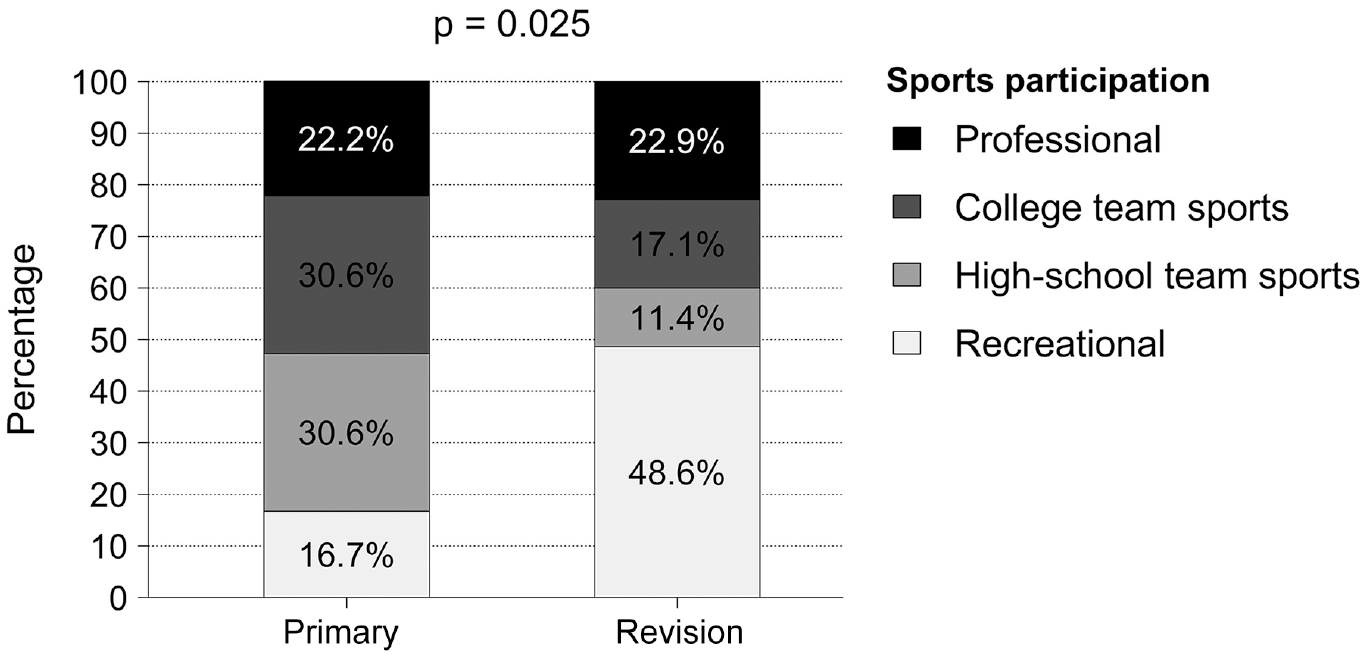
Postoperative sports participation between the study subgroups.
In the revision group, 30 shoulders (48.4%) revealed grade 1 osteoarthritis, 5 (8.1%) presented grade 2, and only 2 cases (3.2%) had grade 3 osteoarthritis. In the primary stabilization group, 6 shoulders (17%) showed grade 1 osteoarthritis, 2 shoulders (6%) had grade 2, and none had grade 3 according to the Ogawa et al18 osteoarthritis grading system. Differences between the study groups did not reach statistical significance (P = .214).
Complications were observed in 5 patients (8%) of the revision surgery group and in 2 of the primary group (5.7%), but the difference was not statistically significant (P = .695). There were 2 cases of graft fracture with no influence on shoulder stability, and no revision or repeated intervention was needed. Two cases of malunion were observed due to lateralized coracoid graft position with increased pain. No recurrent instability was noted, and pain was resolved with physical therapy in 1 case and screw removal in the second patient. There were no cases of osteolysis or nonunion. One patient in the revision and two in the primary group developed shoulder stiffness that resolved with structured rehabilitation.
Four recurrent dislocations (6.4%) were reported postoperatively in the revision surgery group and 1 in the primary group (2.8%), but no statistically significant difference was found at comparison (P = .140). In the revision group, the Eden-Hybinette procedure was conducted in 2 failed cases and in the remaining 2 patients anterior capsular reinforcement was performed. In the primary Latarjet group, arthroscopic revision Latarjet was indicated. No other cases of hardware complication such as screw bending, breakage, loosening, or humeral head erosion were detected. There were no deep infections or neurovascular complications identified in either cohort. No patients required further joint replacement for glenohumeral osteoarthritis.
It is noteworthy that 40 patients (out of 62) in the revision group and all 35 patients in the primary Latarjet group had an off-track glenoid defect, and the difference was significant at comparison (<.001). Because bone loss has been established as the most important factor in the failure of instability surgery, we conducted a subgroup analysis to minimize selection bias. Consequently, we removed all patients in the revision group who did not have an off-track lesion (n = 22), and the remaining 40 patients were compared with 35 patients in the primary Latarjet group as all had an off-track bone defect (Tables 5 and 6).
Comparison of Baseline Demographics and Patient Characteristics Between the Revision Arthroscopic Latarjet Group and Primary Arthroscopic Latarjet With an Off-track Glenoid Bone Defect a
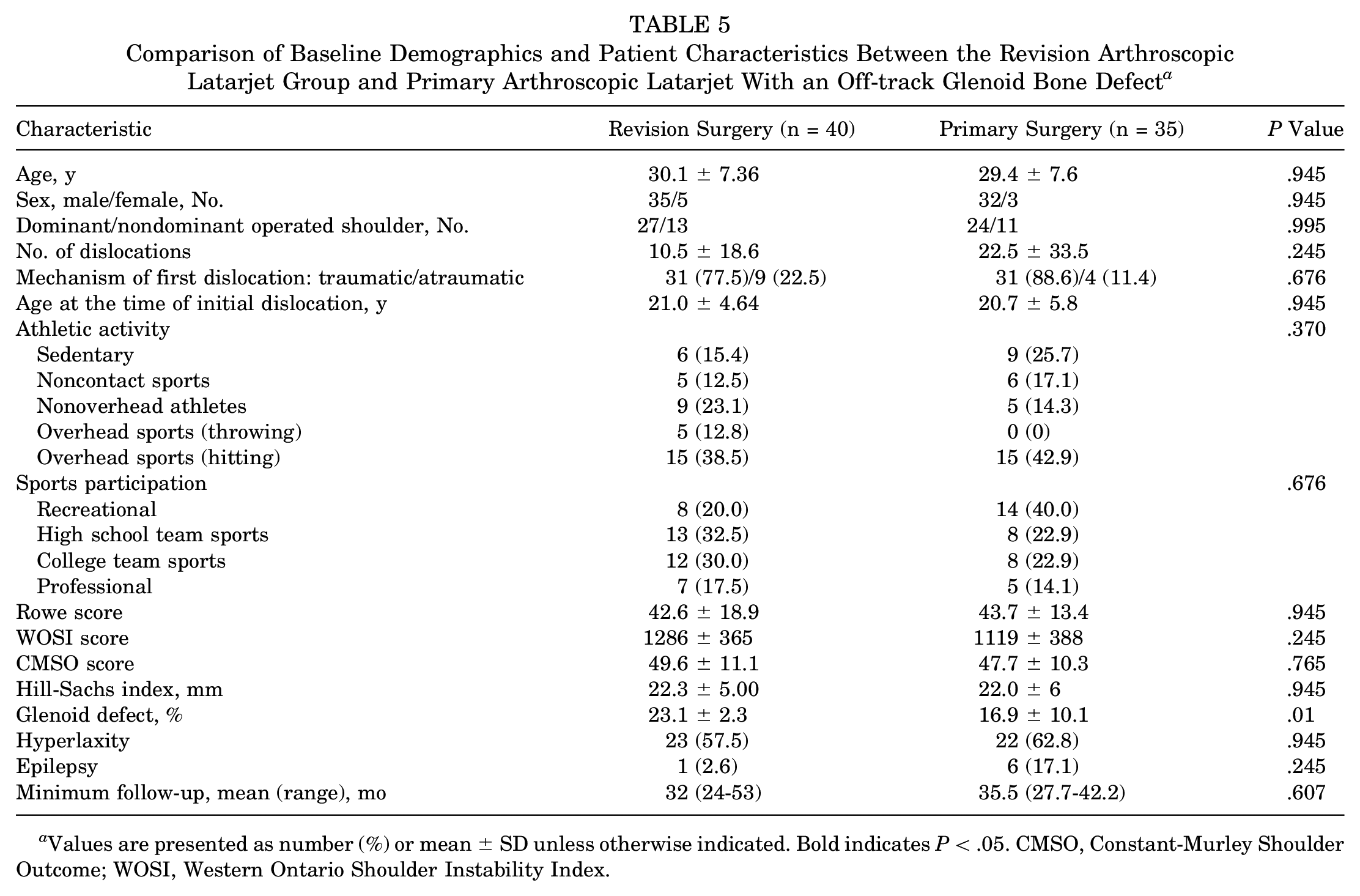
Values are presented as number (%) or mean ± SD unless otherwise indicated. Bold indicates P < .05. CMSO, Constant-Murley Shoulder Outcome; WOSI, Western Ontario Shoulder Instability Index.
Postoperative Functional Outcomes, Shoulder Range of Motion, Activity Level, and Sports Participation in Patients With an Off-track Glenoid Defect a
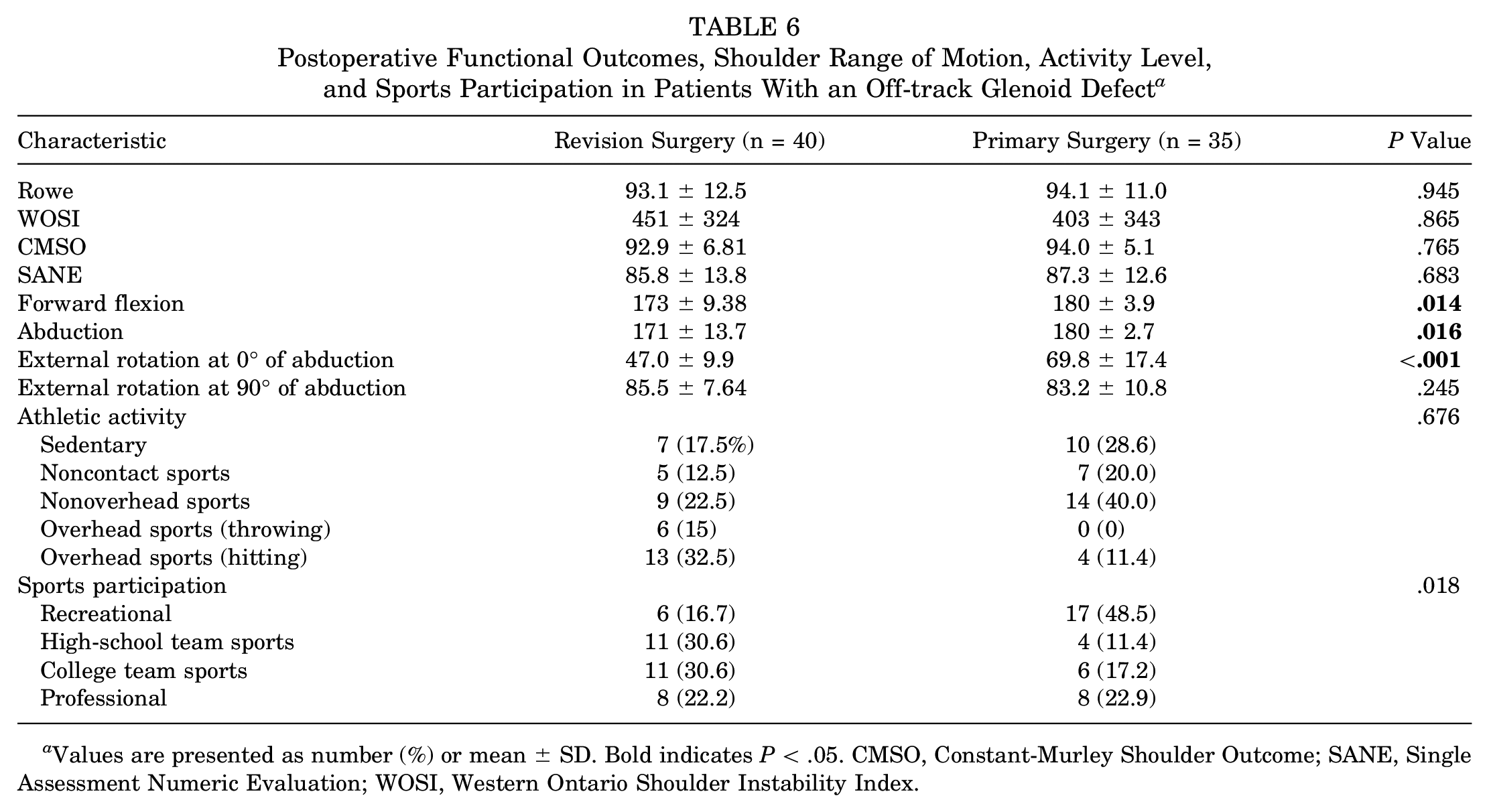
Values are presented as number (%) or mean ± SD. Bold indicates P < .05. CMSO, Constant-Murley Shoulder Outcome; SANE, Single Assessment Numeric Evaluation; WOSI, Western Ontario Shoulder Instability Index.
The revision subgroup demonstrated a significant decrease in postoperative sports participation compared with the primary Latarjet surgery group (Table 7). It appears both groups had an increase in Professional level, but the Primary group had a decrease in college and high school and an increase in recreational.
Comparison of Postoperative Functional Outcomes and Sports Participation between the study groups using the Benjamini-Hochberg correction method a
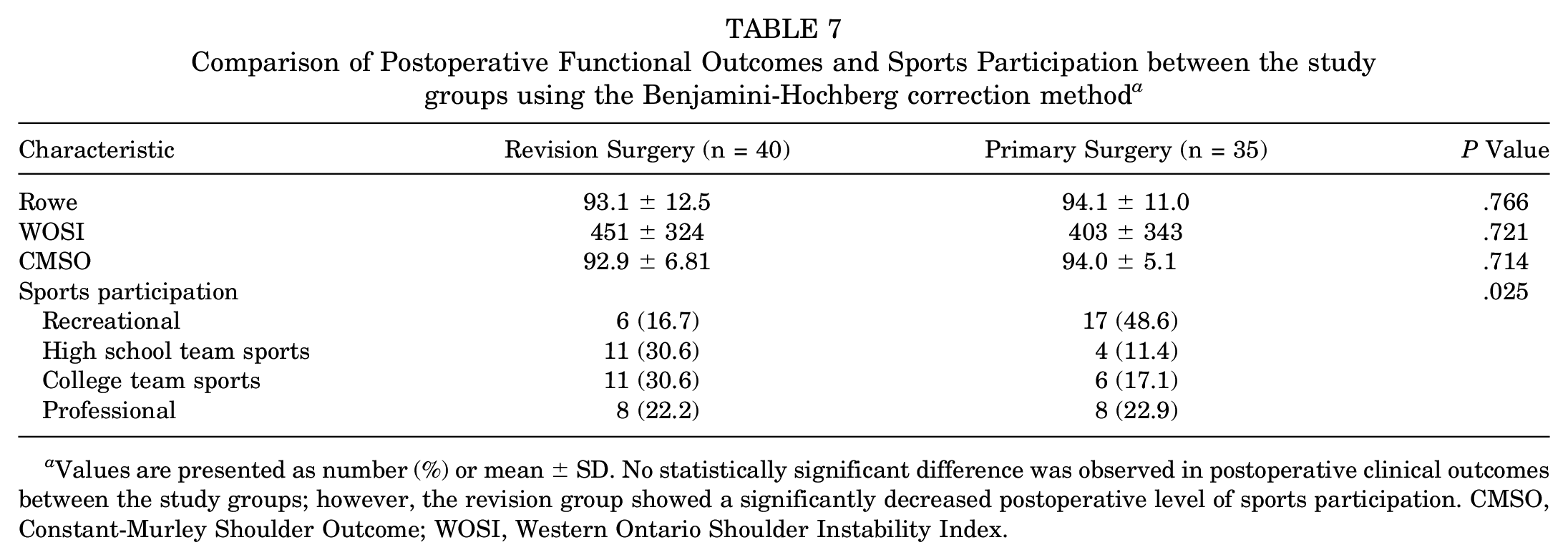
Values are presented as number (%) or mean ± SD. No statistically significant difference was observed in postoperative clinical outcomes between the study groups; however, the revision group showed a significantly decreased postoperative level of sports participation. CMSO, Constant-Murley Shoulder Outcome; WOSI, Western Ontario Shoulder Instability Index.
Discussion
The most important finding of this study was that the arthroscopic Latarjet procedure as a revision surgery can optimally restore glenohumeral stability in patients with failed arthroscopic Bankart repair. Satisfactory objective and subjective results were comparable with those who underwent primary Latarjet stabilization with no significant differences in terms of postoperative recurrence rate. Outcomes of the largest reported cohort of arthroscopic revision Latarjet in the literature are described in the current study.
Evidence from the current literature is still lacking on what should be our primary procedure in patients with recurrent anterior instability, with and without bone loss. In patients without bone defect and in those with subcritical bone loss (<15% of articular surface), primary or revision Bankart repair should be considered as arthroscopic Latarjet did not lead to superior results compared with repeated Bankart repair. 5 However, in patients with critical bone loss (>15%) and previous Bankart repair, arthroscopic Latarjet can be an option. Moreover, younger patient age (<28 years), ligamentous laxity, and participation in contact or overhead sports are associated with a higher risk of recurrence. 3 In addition, good to excellent clinical outcomes and recurrence rate are expected after arthroscopic Latarjet stabilization in patients with epilepsy compared with those without seizure. 9 To sum up, we have conducted primary arthroscopic stabilization in young patients with critical bone loss who participate in contact or overhead sports activities, as well as in those with epilepsy or hyperlaxity.
Reports in the literature comparing the clinical outcomes of open Latarjet as primary versus revision surgery are scant. While some studies suggested the worst results after revision surgery,10,22,30 others reported comparable outcomes between primary and revision surgery.23,32 Our findings regarding the recurrence after revision surgery are similar to those described in a recent study by Rossi et al, 23 who found equally satisfactory outcomes after the open Latarjet procedure as primary or revision surgery. Similarly, Ranalletta et al 21 found that the Latarjet procedure was equally efficient in revision and primary cases in rugby players with recurrent anteroinferior instability. It has been argued that the lack of differences between groups might be the consequence of using the Rowe score as a primary outcome measure, as it was previously reported21,23 to have a lower sensitivity than other subjective scores.10,21,23 On the contrary, Yapp et al 32 found no clinical differences and high levels of satisfaction when the open Latarjet was performed as a primary or revision procedure. In the current study, objective and subjective patient outcome measures were assessed to better support the validity of the conclusions.
Several studies have addressed the postoperative redislocation rate after open Latarjet in the scenario of previous failed surgery, ranging between 0% and 9%.1,4,11-13,28 This is similar to our series and to other comparative studies in which no differences between recurrence rates of open Latarjet as a primary or revision procedure have been reported.29,31 However, Yapp et al, 32 Flinkkilä et al, 10 and Rodkey et al 22 reported recurrence rates of 1%, 25%, and 20.7%, respectively, in patients who underwent an open Latarjet stabilization after failed Bankart repair. Significantly lower rates were found when the Latarjet procedure was carried out as a primary procedure.
Although there was a significant improvement in the postoperative subjective shoulder scores in our series, patients with revision surgery had a significantly decreased level of postoperative sports participation (P < .001). This is in accordance with a previous study by Privitera et al, 20 who evaluated return to play in contact and collision athletes after the open Latarjet procedure. They reported a lower return to play to a previous level when the Latarjet revision surgery was performed after ≥2 previous failed surgeries. In their series, patients with ≥2 previous stabilization procedures had 2.8 times the risk of decreased postoperative sports participation related to their shoulder condition. In our case series of 62 patients in the revision group, only 12 patients (19.3%) underwent 2 previous shoulder stabilization procedures, whereas 46 (74%) had only 1. It appears that there could have been other reasons for decreased postoperative return to play in patients with revision surgery. We documented a significantly decreased postoperative sports participation in the revision group (P = 0.008). However, no significant difference was found in the postoperative Rowe and CMSO scores between the study groups. It is noteworthy that most patients who changed or decreased their preinjury level of sports activity did so not because of shoulder problems; instead, they referred to their psychological readiness and fear of reinjury. Psychological readiness to return to sports is one of the underreported factors in the literature. The ability to deal with the fear of reinjury may highly govern patients’ readiness to return to their preinjury sports activities. Future efforts should focus on proper control and prevention of specific psychological traits to achieve improved postoperative outcomes.
Concerning postoperative range of motion, a significant reduction in forward flexion and external rotation with the arm at the side was found in the revision surgery group compared with the primary surgery group. This finding could be explained by surgical technique because the capsulolabral tissue was dissected from the anterior glenoid rim and reattached at the end of the procedure. Consequently, a significantly reduced postoperative range of motion could be related to the presence of an excessive fibrous remodeling of the capsulolabral tissue, resulting in decreased external rotation in the revision group, as recently stated. 33
Regarding postoperative osteoarthritis, we found an overall rate of glenohumeral osteoarthritis of 46.4%, which was higher in the revision surgery group, although differences were not significant. In our series, the rate of osteoarthritis was higher compared with other comparative studies with similar follow-ups22,23; however, in those studies, the severity of osteoarthritis was assessed using simple radiographs. On the other hand, Rossi et al 23 reported a 14% mild to moderate osteoarthritis rate using the Samilson and Prieto 25 evaluation system with a mean follow-up of 58 months. In this study, osteoarthritis assessment was conducted on a CT scan according to Ogawa et al, 18 which is more sensitive than the traditional system described by Samilson and Prieto, 25 and this might explain a higher rate osteoarthritis observed in our case series.
Several limitations of this study should be considered. First, it is a retrospective study of prospectively recorded data, and only results from patients with complete preoperative images and clinical evaluation (preoperative and postoperative) were collected, raising the possibility of selection bias. However, there might have been a risk of selection bias in those patients who underwent primary Latarjet surgery, leading to the decision of performing the Latarjet procedure instead of Bankart repair. One larger point for consideration is that the degree of bone loss in the study groups was different at baseline. Because bone loss has been established as the most important factor in the failure of instability surgery, we addressed this limitation by conducting a subgroup analysis of patients with an off-track glenoid lesion. Moreover, postoperatively, the difference in WOSI score outcome between the study groups was nearly significant (P = .05). Herein, we highlight a couple of interesting facts about the WOSI score. Shaha et al 27 reported outcomes in military patients after arthroscopic Bankart repair. The authors divided the cohort into 4 different quartiles based on bone loss. Quartile 1 (n = 18) had a mean bone loss of 2.8% (range, 0%-7.1%), quartile 2 (n = 19) had 10.4% (range, 7.3%-13.5%), quartile 3 (n = 18) had 16.1% (range, 13.5%-19.8%), and quartile 4 (n = 18) had 24.5% (range, 20.0%-35.5%). Interestingly, the mean WOSI score worsened as bone loss increased in each quartile. This is mirrored in our data: while good to excellent clinical and functional outcomes were observed in our cohort, the WOSI score presented a P value nearly not significant as all included patients in our study had critical bone loss. The question that might arise at this point is as follows: what is particular about the WOSI score that makes it difficult to achieve a significant postoperative improvement? One rationale might be related to the psychological readiness of the patients, who might fear reinjury and a return to the preoperative level of sports participation, as demonstrated in our study. Our hypothesis is based on our experience, as the justification for decreased postoperative activity (from competitive to recreational or sedentary) was not shoulder related but instead related to their psychological readiness and fear of reinjury, which would make them return to a lower preoperative level of sports participation. The WOSI score, unlike the Rowe and CMSO, possesses a strong psychological component that may reflect functional recovery after surgical treatment. The ability to deal with the fear of reinjury may highly influence patients’ reported postoperative subjective outcomes.
Even though the postoperative recurrence rates and patient outcome measures were reported with no significant differences between groups, the fact that a certain portion of the revision group eventually decreased their sports activity level, possibly meaning they decided to give up sports with high risks, might have led to decreased recurrent dislocation rates with comparable (acceptable) postoperative outcomes to the control primary group. Moreover, the lower number of postoperative recurrence cases could reduce the likelihood of detecting a true difference due to the sample size. Further follow-up in a larger sample size to decrease the probability of a type I error is warranted in the future.
Yet, this study has numerous strengths. To our knowledge, there are no reports of any comparative study on the outcome of the arthroscopic Latarjet as a revision surgery after failed arthroscopic Bankart repair. Only some authors have addressed the outcome of arthroscopic salvage or revision stabilization after open or arthroscopic primary surgery. The latest one is a multicenter retrospective comparative case-control study in 20 patients undergoing an open or arthroscopic Latarjet procedure for recurrent anterior shoulder instability after a failed arthroscopic Bankart repair versus primary Latarjet surgery (216 patients). 31 The study concluded that the assumption that a failed Bankart repair can be revised by a Latarjet technique with a similar result to a primary Latarjet appears to be incorrect. However, considering the sample size of the study (20 patients underwent revision surgery), we urge caution before drawing any conclusion.
To our knowledge, this study represents the largest reported case series of 62 patients undergoing an arthroscopic Latarjet procedure as a revision surgery after failed arthroscopic Bankart repair. It also provides objective and subjective patient-reported outcomes and postoperative imaging results in a consecutive series of patients operated on by the same senior surgeon at 1 institution. Surgical technique and postoperative management protocol were standardized for all included patients. Regarding bone defects, this is the first reported series of patients in whom the glenoid track was measured, taking into consideration the dynamic interaction of glenoid and humeral head defects.
Moreover, no study has addressed return to play after the arthroscopic Latarjet procedure. We observed that decreased postoperative sports participation can be expected in patients after the arthroscopic revision Latarjet procedure, and this finding should be of great interest to the readers. In addition, one of the major strengths of this study is its comparative nature, which enables it to generate a hypothesis. To sum up, the findings of this study enhance the hypotheses that the arthroscopic Latarjet remains an option when an arthroscopic Bankart repair fails, providing satisfactory patient-reported subjective outcomes with a lower rate of recurrence and complications.
Future research should focus on identifying risk factors for poor clinical outcomes after Latarjet revision surgery with the main goal to achieve improved patient selection.
Conclusion
Arthroscopic Latarjet as a revision surgery is a reasonable surgical option in failed Bankart repair cases. The decision to perform arthroscopic Latarjet stabilization as a revision surgery should not be influenced by the potential risk of future complications as it provides comparable clinical outcomes to the primary Latarjet procedure with a low postoperative recurrence rate. However, a decreased level of postoperative sports participation and external rotation with the arm by the side can be expected.
Footnotes
Submitted March 28, 2023; accepted September 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.C. has received consulting fees from DePuy Synthes, Smith & Nephew, and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.