
Abstract
Background:
A 2015 study of platelet-rich plasma (PRP) for groin injuries in National Football League (NFL) players alerted the authors to the possibility that PRP is associated with heterotopic ossification (HO). The current study of athletes seen between 2014 and 2019 provides a more comprehensive analysis of that observation.
Purpose/Hypothesis:
This report describes the early results of groin surgery for athletes who had experienced failed PRP therapy performed by different practitioners and with an assortment of PRP techniques. The primary goal of this cohort study was to determine short-term clinical outcomes after surgery of PRP-treated patients. It was hypothesized that previous PRP treatment would be associated with the presence of HO among patients with core muscle injuries (CMIs).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All athletes seen at 1 institution and identified at their first visit as having received PRP for a CMI were followed and compared with patients with a CMI who had not previously received PRP. Although in many cases HO was observed on clinical examination or imaging, HO was identified intraoperatively in all surgical cases and confirmed pathologically. Successful surgery was defined as return to play at previously high levels of performance or greater as determined by the athletes’ own assessments. All patients who had received PRP were followed for ≥2 years.
Results:
Among 3642 patients with a new CMI seen between 2014 and 2019, 68 (1.9%) patients developed HO within the core muscles and/or adjacent soft tissues. Of the 68 patients, 60 (88.2%) were men, and the mean age was 34.5 years. Of the 68 patients, 62 (91.2%) were athletes and 44 (64.7%) had been treated previously with PRP. HO was observed in 24 (0.7%) patients without previous PRP treatment. Three athletes who received PRP retired early from sports because of HO and scar issues. In total, 22 of 28 (78.6%) NFL players who received PRP developed HO, compared with 0 (0%) of 28 randomly selected, age-, position-, and injury-matched NFL players. After surgical repair, 3-month success rates were 67.9% and 96.4%, respectively, in the PRP and non-PRP groups (P = .006). By 6 months postoperatively, PRP-treated patients were back to similarly high success rates compared with the non-PRP cohort. Scar tissue issues played a prominent role in the relative delay in definitive success.
Conclusion:
The present, more comprehensive study confirms the previous preliminary analysis that treating CMIs with PRP may be associated with HO.
The purpose of this review is to follow up on a smaller study, presented at the 2018 AOSSM annual meeting, that investigated the phenomenon of heterotopic ossification (HO) among patients with core muscle injuries (CMIs). 11 CMI refers to damage to any skeletal muscle within the area between the chest and midthigh. By 2014, platelet-rich plasma (PRP) was becoming a popular treatment option for a variety of orthopaedic and other disorders.6,12 During the same time frame, HO was an uncommon but seemingly increasingly frequent finding among athletes referred with a suspected CMI. 3 The latter observation prompted a deeper look into the connection between PRP and HO. 7
Here, we report on a larger cohort of patients with a CMI followed for ≥2 years to determine more definitively whether HO is associated with previous PRP treatment. Some of these data were presented at the 2022 AOSSM annual meeting. 13 Because all of the patients were referred and had received previous attempts at definitive therapy, these patients must be considered highly selected, so no definitive statement concerning cause and effect would be possible. However, this lack of a prospective nature for studying effects of PRP would not prohibit establishment of an association of that treatment with subsequent surgical findings and outcomes. All of the PRP administrations in this study were performed by other treating physicians before evaluation by the authors (A.E.P. and W.C.M.).
Methods
A total of 3642 patients with a CMI seen by 2 surgeons at a single institution between 2014 and 2019 were entered into a database and followed postoperatively for ≥2 years. All patients had a CMI involving the rectus abdominis, pectineus, adductor longus, adductor brevis muscles, and/or pubic fibrocartilage. Diagnosis required pain and/or weakness upon resistance testing of the involved muscles plus corresponding undermining or detachment of the caudal rectus abdominis, adductor longus origin, and pubic fibrocartilage on magnetic resonance imaging (MRI). 15 That cohort was segmented by age, sex, athletic status, and whether they had received PRP injections before their visits. Patients who had HO with or without PRP were analyzed according to the same criteria.
Before the initial clinical examinations, all patients referred for a suspected CMI completed a standardized data form that included demographic characteristics, sport profile, and clinical information.
The largest player group treated with PRP came from the National Football League (NFL). The initial analysis of this group prompted a random selection of non–PRP treated NFL players for comparison who were matched for age, position, injury site, and severity over a similar time frame.
For both the full patient cohort and the NFL cohorts, comparisons between groups were made using chi-square or Fisher exact tests. All P values were 2-tailed, and P values <.05 were considered statistically significant. Relative risk represented a measure of association between PRP and HO, postoperative “untoward events,” or surgical success.
Heterotopic Ossification
HO was established by the presence of calcification of the fibrocartilage and/or skeletal muscle as detected by gross and/or microscopic pathology. In patients with a CMI who did not receive surgery, HO was determined by the combination of direct palpation and radiographic calcification. All patients underwent MRI studies. To assess hip pathology, radiographs were obtained in some cases. Ultrasonography was also performed for a variety of reasons. The HO occurred in patterns: distinct lumps measuring <1 to 9 cm in size, multiple lumps, diffuse or tiny nodules, or a combination of those findings. Extensive fibrosis was defined by fascial thickening and scarring of the muscle beyond what is expected for the type and severity of injury. This was determined by the operating surgeon and was recorded in the operative note.
PRP Treatment
Patients were categorized as having received previous PRP treatment based on official reports or responses in the standard questionnaire, plus statements made by the patients during the history examination. In all cases, phone calls were made directly to PRP providers in attempts to document details of the treatment. Patients who received PRP injections outside the core musculature (eg, joint space, high chest, or below the thigh) were not included for analysis, nor were 2 patients who received non-PRP, stem cell injections.
Severity of Injury
Each muscle involved in the CMI was graded intraoperatively by the attending surgeon using a previously published grading system. 8 The grading system is based on the percentage of the muscle footprint that has dislodged from the pubic fibrocartilage. Grade 1 denotes an injury involving <30% of the footprint, grade 2 represents an injury involving 30% to 95%, and grade 3 designates 96% to 100% detachment.
Outcomes
Outcomes were determined as previously published.8,10 Patients self-reported using a 5-level scale: 5, at or above preinjury level of performance, no discomfort; 4, at or above preinjury level of performance, still with mild symptoms; 3, better, but not at preinjury level of performance; 2, no better; 1, worse than preoperatively. “Surgical success” included both levels 4 and 5. 9 Assessments were performed at 3, 6, 12, and 24 months. Additional measures included hematomas, scar complications, skin indentations, need for percutaneous procedures such as dry needling or corticosteroid injections, and delays in rehabilitation progression.
NFL Medical Staff Interviews
To understand how often PRP was being used for these injuries and what might have been a success rate with this form of treatment, we retrospectively interviewed head team physicians and head or associate head athletic trainers covering all 32 NFL teams during the study interval. They were asked to estimate the number of players treated with PRP annually for those specific injuries, anatomic locations of those treatments, and observations about possible successes. Additionally, they estimated the number of cases of symptomatic HO in the core region they had seen annually.
The study was approved by the institutional review board at Jefferson Medical College (IRB control No. 06U.300).
Results
Between 2014 and 2019, a total of 3642 patients with a new CMI were seen. Of these, 3012 (82.7%) were men.
Heterotopic Ossification
Among 3642 patients with a new CMI seen between 2014 and 2019, a total of 68 (1.9%) patients developed HO within the core muscles and/or adjacent soft tissues. Of the 68 patients, 60 (88.2%) were men, and the mean age was 34.5 years. Further, 62 (91.2%) of the 68 patients were athletes, and 44 (64.7%) had been treated previously with PRP. HO was observed in 24 (0.7%) patients without previous PRP treatment. Of the patients previously treated with PRP into the core muscles, 64 (59.3%) had no evidence of HO. In other words, HO was observed in 44 of 108 (40.7%) patients with previous PRP treatment and 24 of 3534 (0.7%) patients without previous PRP treatment.
Platelet-Rich Plasma
Among the entire cohort of 3642 patients with new CMI seen between 2014 and 2019, a total of 108 (3.0%) patients had previously received PRP into the core musculature. In total, 125 patients stated that they had previously received PRP somewhere in their body; 17 of the 125 had received injections outside the core musculature and so did not qualify for the analysis. Determining the exact location of PRP injections within the core musculature was not possible with the documentation and verbal reports obtained.
The 108 patients received PRP therapy from 94 different practitioners or practice groups. Seven patients had received >1 injection, and all were found to have HO. A total of 21 practitioners indicated preferences for leukocyte-poor preparations for muscle and tendon injuries, and 2 practitioners indicated preferences for leukocyte-rich plasma. 4 Timing of therapy ranged from 2 to 19 months before evaluation.
Twelve patients had also undergone previous core muscle surgery. Ossification was observed between 3 weeks and 26 months after PRP administration.
The 108 patients had a mean age of 34.6 years (range, 16-78 years), and 97 (89.8%) were men. All had persistent symptoms and signs of CMI, limitations in their abilities to perform sports, and MRI findings 14 of CMI.
As mentioned, professional football players predominated as the largest identifiable group of patients who had received PRP (Table 1). In total, 27 (67.5%) of the 40 football athletes played in the NFL when they received PRP. Two of the other 13 joined the NFL the year after receiving treatment in college and are included as NFL players. The other 11 football players were high school or collegiate athletes.
Sports of 108 Patients With Previous Platelet-Rich Plasma Treatment
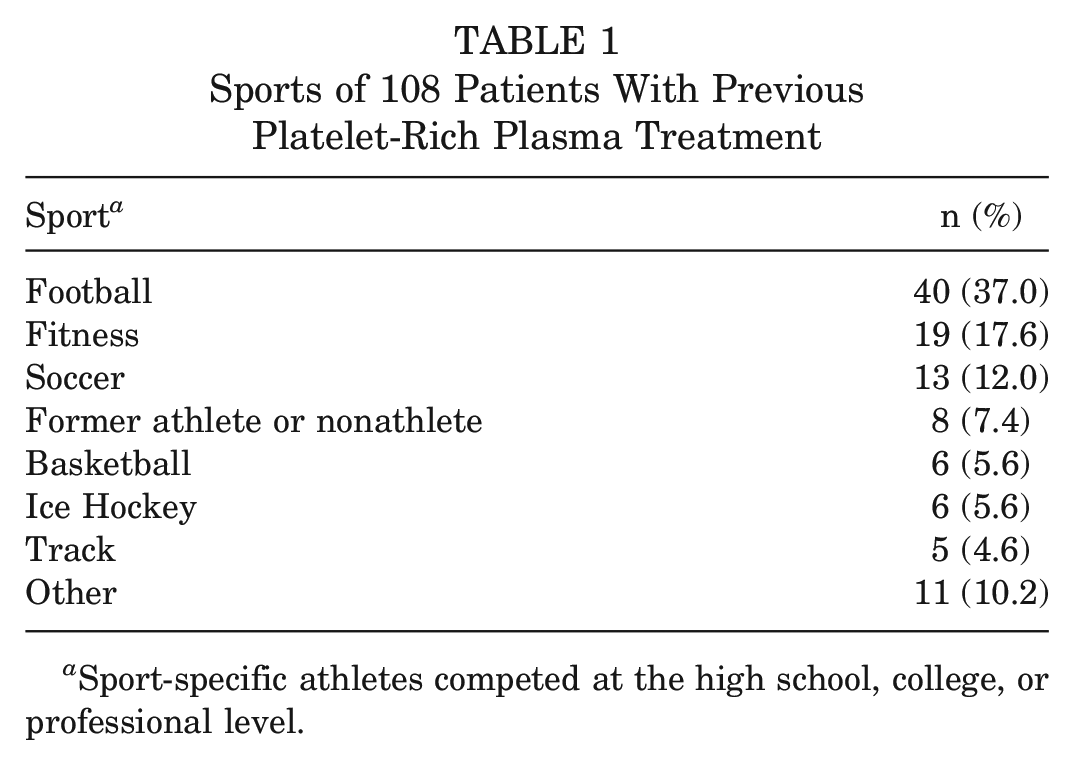
Sport-specific athletes competed at the high school, college, or professional level.
The second largest group to receive PRP was so-called fitness athletes, who were not professional or otherwise high-level, single-sport athletes and who were linked by a strong desire to stay in shape. This group included amateur runners, recreational athletes in various sports, and regular visitors to gyms. Those 2 largest groups were followed in number by soccer players, former athletes or nonathletes, and basketball, ice hockey, and track athletes. Of the 108 patients, 99 (91.7%) underwent CMI repair surgery. Five (5.0%) of the 99 also had combined femoroacetabular impingement surgeries (ie, performed under the same anesthetic). The 9 PRP patients who did not have core muscle surgery all chose nonoperative treatments. Seven of the 9 nonoperative patients came from the fitness group.
Operative Findings After PRP
At surgery, 73 (73.7%) of the 99 PRP patients had grade 2 or 3 injuries of ≥1 core muscle (Table 2). At surgery, 43 (43.4%) patients had HO involving the adductor and/or rectus abdominis muscles (Figure 1). The HO often involved the periosteum of the pubic bone and distinct branches of inguinal, femoral, or obturator nerves, suggesting that calcifications were associated with pain.
Operative Findings Among 99 Surgical Patients With Previous Platelet-Rich Plasma Treatment a
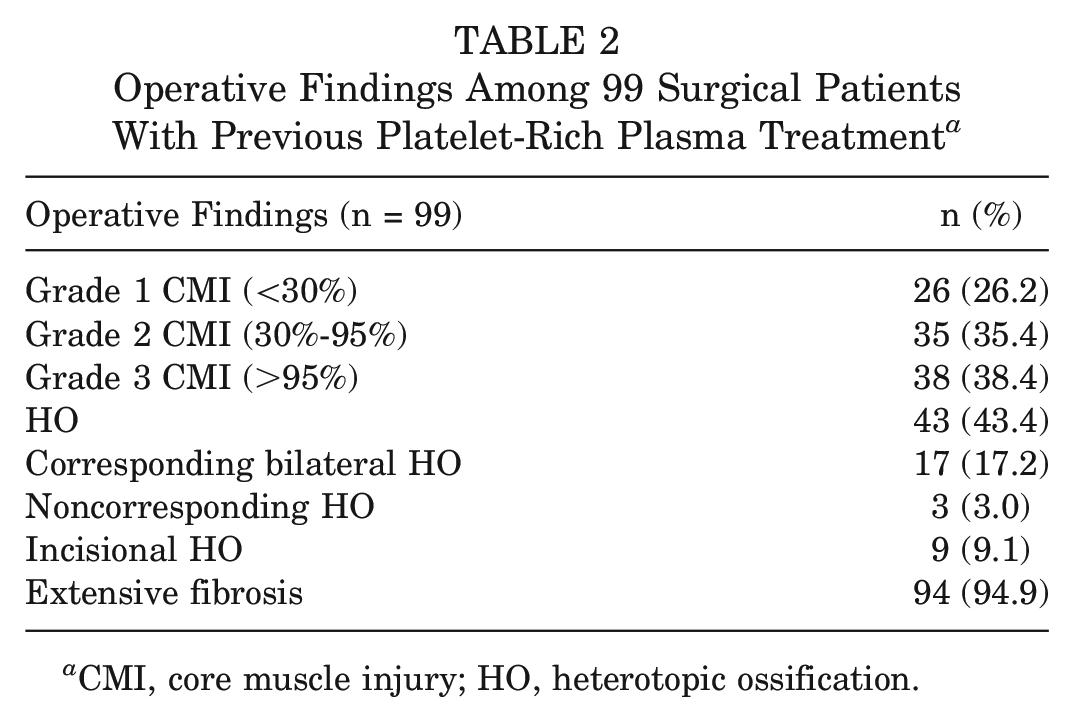
CMI, core muscle injury; HO, heterotopic ossification.
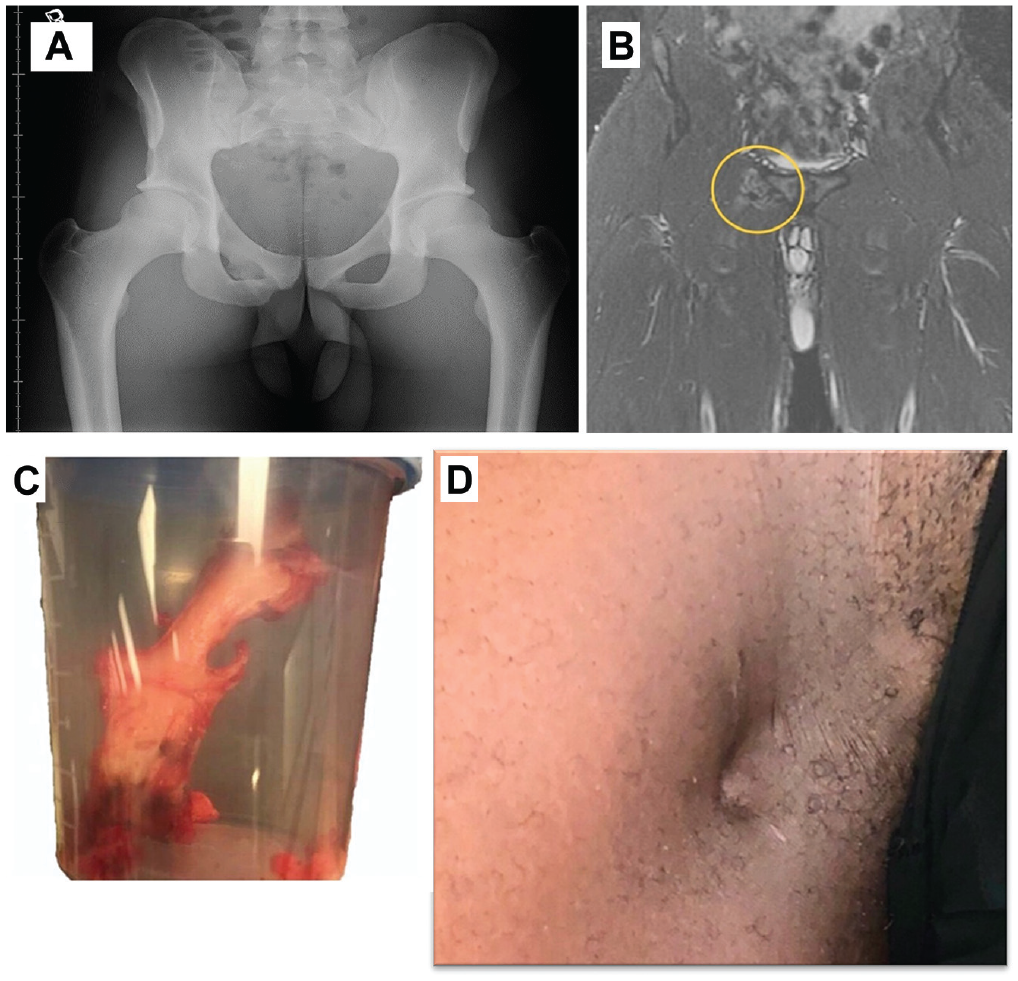
(A) Radiograph of a National Football League (NFL) player with heterotopic ossification (HO) of the pectineus and adductor longus muscle that was palpable on physical examination. (B) Coronal stir magnetic resonance image of the same NFL player with HO. The gnarled lesion adjacent to the right pubic body appears irregular and multishaded, like tissues tied in a knot. (C) Surgical specimen of sharp, spiculated HO removed from the adductor muscles of the same NFL player. (D) Heterotopic bone-related thigh indentation, 2 inches below the inguinal incision, noticed by this NFL player several months after definitive surgical core muscle repair and previous PRP.
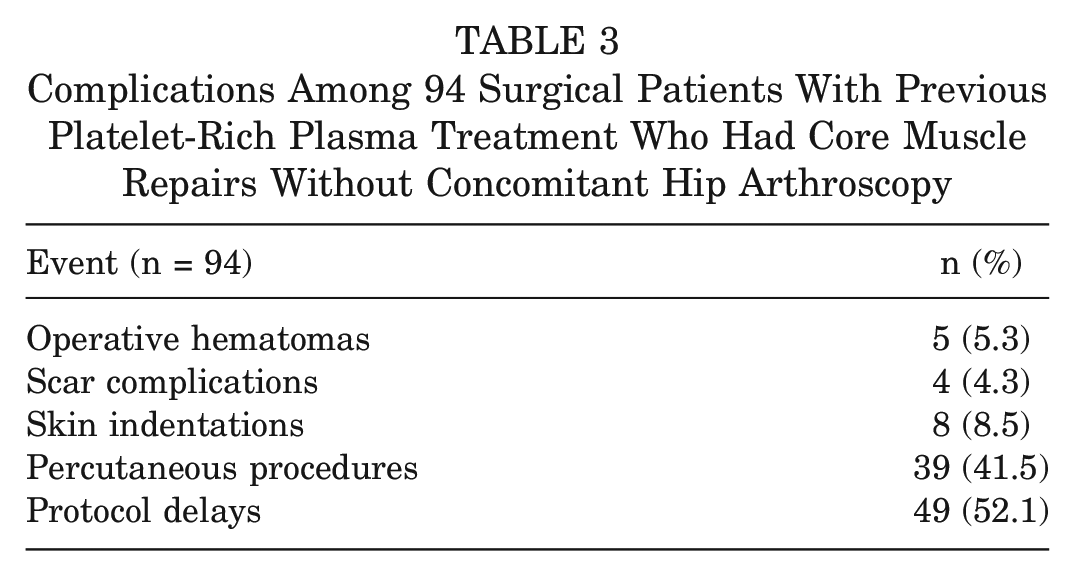
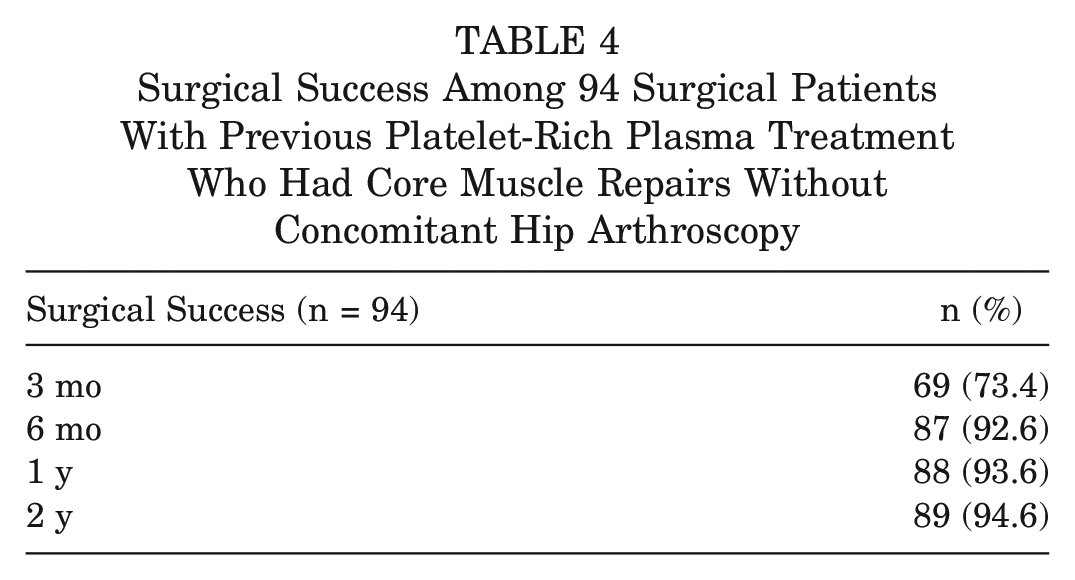
All 17 patients who were known to have received bilateral PRP injections had bilateral HO. Interestingly, 3 of the 43 patients found to have HO intraoperatively had HO not only on the side where the PRP had been injected but also on the opposite side, where PRP had not been injected. In 2 of those 3 patients, HO occupied the skin of otherwise well-healed, bilateral inguinal incisions from unsuccessful hernia surgery after failed unilateral PRP treatment. Extensive fibrosis was noted in the muscles of 94 (94.9%) of the 99 operated patients who had received PRP (Table 2). There were delays in the 6-week postoperative rehabilitation progression in 52.1% of the surgical patients who had core muscle repairs without hip arthroscopy (Table 3). The 3 month success rate after surgery among this group was 73.4% and increased to 92.6% at 6 months (Table 4). Three athletes who received PRP retired early from sports and, in part, attributed it to HO.
Complications Among 94 Surgical Patients With Previous Platelet-Rich Plasma Treatment Who Had Core Muscle Repairs Without Concomitant Hip Arthroscopy
Surgical Success Among 94 Surgical Patients With Previous Platelet-Rich Plasma Treatment Who Had Core Muscle Repairs Without Concomitant Hip Arthroscopy
NFL Player Analysis
The 29 NFL players with previous PRP treatment had a mean age of 26 years (range, 21-33 years). Among them there were 7 cornerbacks, 6 wide receivers, 5 linebackers, 3 safeties, 3 defensive ends, 3 kickers, 1 defensive tackle, and 1 running back. Of these 29 players who had previously received PRP, 28 underwent CMI surgery. Of those 28 patients, 24 patients (85.7%) had grade 2 or 3 injuries of ≥1 core muscle, and 22 patients (78.6%) had HO. Of the 3 patients who had bilateral ossification despite only 1 side having been injected, 2 patients were NFL players, and both had calcified skin scars bilaterally. Extensive fibrosis was noted at surgery in 26 (92.9%) of 28 players. None of the 28 operated patients had CMI surgery combined with femoroacetabular impingement surgery.
Seventeen (60.7%) of the 28 players who underwent surgery had complications, including 2 postoperative hematomas (ie, within 24 hours of surgery) and 2 delayed muscular hematomas that required surgery; all 17 players had delays in completion of rehabilitation protocols. Twelve (42.9%) patients had postoperative, percutaneous, ultrasound-guided needling and corticosteroid injections in response to delayed rehabilitation progression due to restrictive scarring over the adductors and/or rectus abdominis muscle. 5 Of the 28 players, 19 (67.9%) had success at 3 months, 25 (89.3%) at 6 months, and 26 (92.9%) at 1 year. Two players retired because they could “no longer compete.”
Seven patients who had surgery during the season and remained eligible to return were included in a return-to-play analysis. Five of the 7 patients made it back fully (at 6, 7, 9, 10 and 11 weeks). One NFL player made it back at 7 weeks and then required surgery again at 9 weeks because of a severe scar breakup episode; he returned to play fully again at 3 weeks after the second surgery and played the remainder of the season, plus 4 more seasons, without further event. Six of the 8 patients with skin indentations were NFL players. Five of the 6 reported no association of the indentations with performance. The sixth player reported ipsilateral thigh weakness. A single NFL player did not undergo surgery. He had an obvious, palpable, radiograph-documented HO deposit in the pectineus muscle 6 cm distal to the pubis and was successfully treated by percutaneous hematoma aspiration, dry needling, and steroid injections. He was still playing at 2 years without further limitation.
Comparison With Non-PRP, Matched Controls
As mentioned, a pool of NFL players who had never received PRP was developed from the database. These players were matched with the 28 NFL players who had undergone surgery and PRP treatment according to type of surgery, age, position, the involved muscles, and severity of injury. From that pool, 28 players were randomly selected for comparative analysis (Table 5).
Comparison of 28 NFL Athletes With Previous PRP Treatment and 28 Non-PRP, Matched Controls a
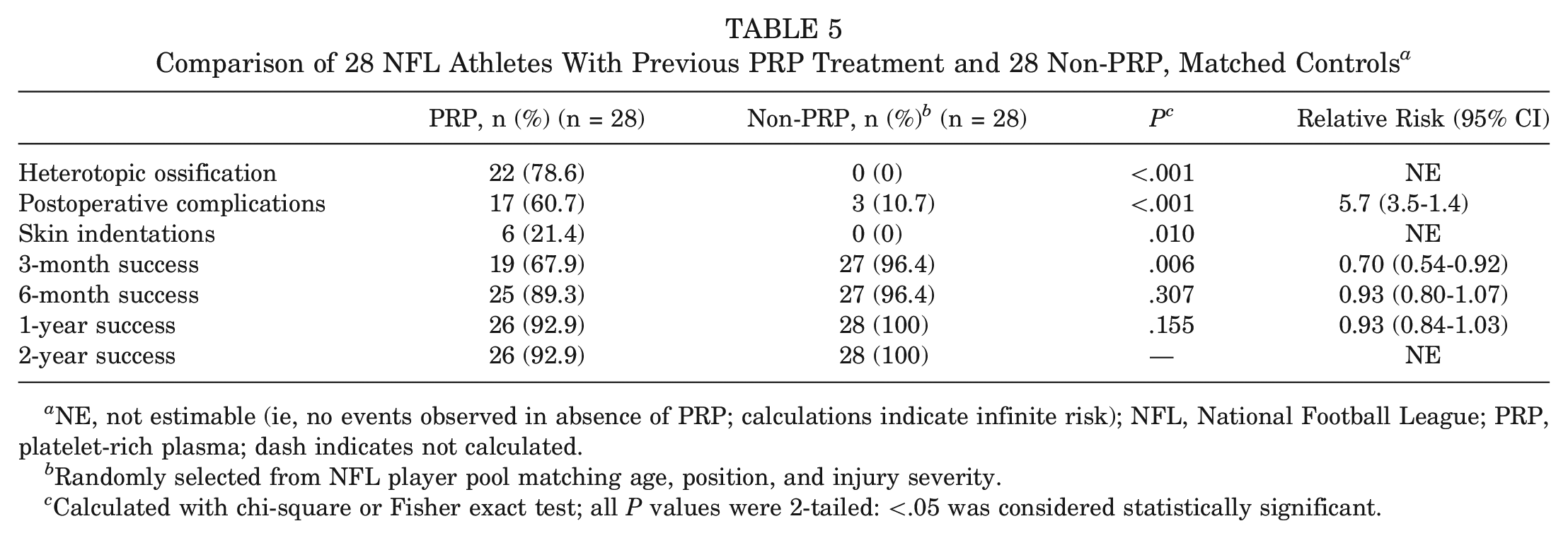
NE, not estimable (ie, no events observed in absence of PRP; calculations indicate infinite risk); NFL, National Football League; PRP, platelet-rich plasma; dash indicates not calculated.
Randomly selected from NFL player pool matching age, position, and injury severity.
Calculated with chi-square or Fisher exact test; all P values were 2-tailed: <.05 was considered statistically significant.
None of the patients in the matched, comparative set developed HO, although 2 patients had notable fibrosis at surgery. Three (10.7%) of the 28 matched control players had complications. One had an early postoperative hematoma. Another underwent adductor surgery 6 weeks after surgery for new symptoms on the opposite side of the original adductor surgery. The third player was limited by pain past his rehabilitation protocol timeline and needed postoperative percutaneous steroid injections to get him back to full play. There were no infections.
Of the 28 matched comparative players, 27 (96.4%) reported success at 3 months and 6 months postoperatively, and all 28 reported success by 1 year (Table 5). One player retired after 1 year because of an elbow injury. Six (85.7%) of 7 players who underwent surgery during the season returned to play within 8 weeks of surgery. No subsequent scar or other relevant issues occurred in any of the patients over that first year, nor did any player report skin indentations. Two-year outcome analysis did not alter the 1-year findings in either the PRP or the control group.
NFL Medical Staff Interviews
Based on estimates from team medical staff members, the number of groin injuries in the league between 2014 and 2019 ranged roughly between 89 and 204 per year (or 534 to 1224 total during the time period). Of the 3642 patients included in the database for this study, 310 were NFL football players. This means that roughly 25% to 60% of NFL players with groin injuries between 2014 and 2019 were included in this study.
Eighteen (56%) of the team representatives said they never used PRP for groin injuries, and 3 of the other 14 teams abandoned PRP for this indication during the study period. Three team physicians reported observing HO after PRP administration within the same time frame. With regards to other injuries, 30 of the 32 team physicians still used PRP.
The 14 physicians who reported at least some PRP use during the time period estimated that a mean of 12% (range, 10%-75%) of their players with groin injuries were treated with PRP. Applying these percentages to the estimated number of NFL athletes with groin injuries results in approximately 28 to 64 players receiving PRP for groin injuries between 2014 and 2019. These estimates suggest that the 29 NFL players included in this study comprise about 45% to 100% of that population.
Discussion
Among 3642 patients with a new CMI seen between 2014 and 2019, 68 (1.9%) patients developed HO within the core muscles and/or adjacent soft tissues. Of these 68 patients, 44 (64.7%) had been treated previously with PRP. Among the entire cohort, 108 patients were treated with PRP injections into the core muscles. HO was observed in 44 of 108 (40.7%) patients with previous PRP treatment and 24 of 3534 (0.7%) patients without previous PRP treatment. These results suggest an association between PRP injections into the core musculature and HO.
In this study, previous treatment with PRP was associated with a 52% rate of rehabilitation delays (Table 3). The early delay in return to preinjury level of performance dissipated over the first 6 months of the 2-year follow-up. Many of the rehabilitation delays developed from fascial thickening, muscle scarring, and HO, which occurred in 43% of the athletes who had PRP versus 0.7% who did not receive PRP. In NFL athletes, this ratio was even more profound: 79% versus 0% in injury-, age-, and position-matched controls. One might postulate that the present observations about groin injuries and PRP parallel some lessons learned in combat casualties, where it has been observed that enhanced systemic inflammation increases the risk of HO.1,2 In the current study, the finding that 3 patients developed calcification at sites distant from where the PRP was administered also suggests a systemic process contributing to the formation of HO.
Likewise, this study suggests that local wound characteristics play a role in the development of HO. Although less frequent, when new bone formations did occur in the absence of PRP, nearly all those were in the setting of chronic, untreated large-gap muscle avulsions.
Although the results of this study raise a red flag for 1 PRP indication (ie, central CMIs), we do not condemn the overall use of PRP based on this study. Thirty of the 32 team physicians still used PRP “regularly” and “without apparent complication” for selected joints and other muscles or tendons. A recent study, also presented at the 50th anniversary meeting of the AOSSM, showed an increased chance of HO around the hip joint in patients given PRP during hip arthroscopy. 14
The current study was limited to a single-arm assessment of outcomes after failed PRP at a single institution that specializes in treating core injuries. All patients had received their PRP treatments elsewhere and in a variety of settings. 12 The data suggest an association between PRP and HO. The study design does not yield definitive answers to either (1) direct causation of HO by PRP or (2) whether initial treatment with PRP for acute groin injuries might sometimes be beneficial.
This study is from a referral practice and therefore probably includes a selection bias of patients with unfavorable outcomes who were referred for further treatment. We do not know how many patients might have benefited from PRP administered by the outside physicians. One possible exception to the last statement is the NFL players. We were able to retrospectively obtain firm estimates from team physicians and head athletic trainers of PRP use for these injuries during the same time period. This information was based on estimates and is therefore anecdotal and subject to recall bias.
Based on the interviews with NFL team representatives, this study includes roughly 25% to 60% of NFL athletes with groin injuries. It is reasonable to conclude that a significant proportion of NFL athletes with groin injuries were included in this study. The number of NFL athletes who were treated with PRP but not included in this study remains uncertain. The selection bias inherent in this study (ie, including only PRP treatment failures) means that definitive conclusions about potential harmful effects of PRP treatment cannot be made. However, the fact that the majority of team physicians stopped using PRP for this indication implies that the answer to the second question (whether PRP treatment for acute groin injuries might sometimes be beneficial) is no.
Going back to the first question, PRP may have contributed to the formation of heterotopic bone. All referring physicians reported that the HO was not noted on examinations before PRP administration; therefore, it is unlikely that the HO preexisted. However, patients often did not have previous imaging. Therefore, we cannot say with certainty that none of the cases of HO observed in this study were present before PRP treatment. Independently, 3 team physicians stopped using PRP after they directly and independently observed HO occurrence in the core muscles after PRP. They had not previously been told the results of the present analysis.
Conclusion
The present, more comprehensive, study confirms the previous preliminary analysis that treating CMIs with PRP may be associated with HO. 11
Footnotes
Presented at the 2018 AOSSM annual meeting in San Diego, California, and the 2022 AOSSM annual meeting in Colorado Springs, Colorado.
Submitted January 13, 2023; accepted September 11, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.