
Abstract
Background:
Previous biomechanical studies have identified capsular closure, labral repair or reconstruction, and osteochondroplasty as important surgical interventions to improve hip stability.
Purpose:
To investigate the outcome metrics used to quantify hip stability and assess and measure the relative contributions of the labrum, capsule, and bone to hip stability through a quantitative analysis.
Study Design:
Systematic review and meta-analysis; Level of evidence, 4.
Methods:
PubMed and Embase databases were searched using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Included studies evaluated cadaveric hip biomechanics related to capsular, labral, and bony management during hip arthroscopy. Studies were assessed for distraction force and distance, fluid measures, and contact forces used to quantify the suction seal. Exclusion criteria included open surgery, arthroplasty, reorientation osteotomy, or traumatic dislocation.
Results:
A total of 33 biomechanical studies comprising 322 hips that evaluated 1 or more of the following were included: distraction force or distance (24 studies), fluid measures (10 studies), and contact forces (6 studies). Compared with a capsulotomy or capsulectomy, capsular repair or reconstruction demonstrated greater resistance to distraction (standardized mean difference [SMD], 1.13; 95% CI, 0.46-1.80; P = .0009). Compared with a labral tear, a labral repair or reconstruction demonstrated less resistance to distraction (SMD, −0.67; 95% CI, −1.25 to −0.09; P = .02). Compared with a labral debridement, repair or reconstruction demonstrated greater resistance to distraction (SMD, 1.74; 95% CI, 1.23 to 2.26; P < .00001). No quantitative analysis was feasible from studies evaluating the effect of osseous resection due to the heterogeneity in methodology and outcome metrics assessed.
Conclusion:
Most biomechanical evidence supports capsulotomy repair or reconstruction to improve hip distractive stability at the end of hip arthroscopic surgery. While the repair of a torn labrum does not improve distractive resistance, it is superior to labral debridement in most biomechanical studies.
Procedural volumes for hip arthroscopy continue to increase globally as the field advances in both diagnostic and therapeutic capacities.4,49 Despite recent interest in the biomechanical consequences of soft tissue and bony management in hip arthroscopy, it is unclear how certain aspects of surgical correction of capsular, labral, and bony pathology influence joint mechanics and stability. The labrum, capsule, and bony congruity of the femoral head and acetabulum are important contributors to hip stability. Biomechanical evidence suggests that normal, intact hip anatomy provides the greatest joint stability, and the introduction of bony or soft tissue pathology decreases stability.7,22,46,54 The presence of pathology, or treatment thereof, can contribute to microinstability, which is symptomatic excessive motion of the femoral head within the acetabulum leading to altered joint loading and concordant pain, dysfunction, and osteoarthritis.31,40,48,52 This has led to an increased focus on refining surgical techniques to restore normal joint anatomy and enhance surgical outcomes. Many techniques for capsular closure, labral preservation or restoration, and femoral cam and acetabular rim resection have been supported by biomechanical studies and are used in hip arthroscopy procedures based on patient indications.10,21,44,47
Multiple biomechanical outcome metrics have been used to quantify hip stability in the setting of bone and soft tissue pathology. The hip suction seal has been established as a reproducible measure of hip stability, particularly in the setting of labral pathology.6,17,51 However, the contributions of the capsule and bone to the suction seal have not been well-defined. Other outcome metrics such as hip range of motion, contact forces, joint loading, and translations between the femoral head and acetabulum have been used to quantify the capsular and bony contributions to hip stability.28,45-47,58 The relationship between different outcome metrics to quantify hip stability is still largely unknown. The purpose of this review was to investigate the outcome metrics used to quantify hip stability and assess and measure the contributions of the labrum, capsule, and bone in different conditions to hip suction seal mechanics in in vitro biomechanical studies through a quantitative analysis. We hypothesized that a capsular repair or reconstruction would improve stability compared with a capsulotomy or capsulectomy, that a labral repair or reconstruction would improve stability compared with a labral tear, and that a femoral cam and acetabular rim resection would improve stability compared with the abnormal bone morphology in femoroacetabular impingement syndrome (FAIS).
Methods
Study Registration
This study was registered in the international prospective register of systematic reviews (ID: CRD42022372625). No ethics or institutional review board approval was required.
Search Strategy
Two online databases (Embase and PubMed) were searched from database inception until October 30, 2022, for literature that investigated the contribution of the hip labrum, capsule, or bony structure to the suction seal in biomechanical cadaveric studies. The search included broad terms such as “hip arthroscopy,”“cadaver,” and “labrum” (Appendix 1, available in the online version of this article) and was completed using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and checklist.
Assessment of Study Eligibility
The research question and study eligibility criteria were established a priori. The inclusion criteria were English-language studies, the biomechanical evaluation of human cadaveric hip specimens, and an assessment of the contribution of the labrum, capsule, or bone to the hip suction seal and stability metrics. Exclusion criteria were animal studies; reviews; technique reports; editorials; opinion articles; clinical studies; abstracts; studies that concerned open surgery, arthroplasty, reorientation osteotomy, or traumatic dislocations; and studies that focused on patient-reported outcome scores.
Study Screening
All titles, relevant abstracts, and full-text articles were screened by 2 orthopaedic surgeon reviewers independently (A.J.H. and W.B.). Any disagreements were deliberated between the 2 reviewers, and a senior author (R.M.D.) was consulted if a consensus could not be obtained. The references of the included studies were manually screened for any articles that were not included in the initial search strategy.
Data Abstraction
Data were collected and recorded in an Excel spreadsheet (Version 16.66; Microsoft Corporation). Abstracted data included the manuscript title, author(s), year of publication, study design, number of cadaveric specimens, cadaver age, cadaver handling, hip structures assessed, and stability metric outcomes. The data were extracted by a single reviewer (A.J.H.) and checked by a second reviewer (W.B.). Disagreements were deliberated between the 2 reviewers, and a senior author (R.M.D.) was consulted if a consensus could not be obtained. Missing data were excluded from the analysis. Study investigators were contacted for additional details and raw data as necessary.
Data Synthesis
The biomechanical cadaveric studies were assessed for several hip stability metrics including the distractive force and distance required to rupture the suction seal, the peak negative pressure and change in volume in the central compartment associated with disruption of the suction seal, and the change in contact area, force, and pressure between the femoral head and acetabulum in different soft tissue and bony structural states.
Statistical Analysis
Weighted means and standard deviations were calculated for continuous variables using IBM SPSS Statistics Version 23 (IBM Corp). Standardized mean differences (SMDs) were calculated between the capsulotomy or capsulectomy and capsular repair or reconstruction groups in the native capsule studies. SMDs were calculated between the labral tear or labrectomy and labral repair or reconstruction groups in the native labrum studies. Review Manager (RevMan) Version 5.4.1 (Cochrane) was used for data analysis. Forest plots were created for the distractive force and distance comparing the capsulotomy or capsulectomy and capsular repair or reconstruction states and for comparing the labral tear or labrectomy and labral repair or reconstruction states. The I2 index was used to measure the heterogeneity of the included studies. 23 Effect sizes were calculated using a random-effects model with the DerSimonian-Laird estimator, because high heterogeneity precluded the use of a fixed-effects model. 12 An SMD score of 0.2 to 0.49 was considered weak, a score of 0.5 to 0.79 was moderate, and a score of 0.8 or greater was considered large. 9
Results
Search Strategy
The initial search of online databases identified 2307 studies. A systematic screening and assessment of eligibility identified 33 articles that satisfied the inclusion criteria (Figure 1).
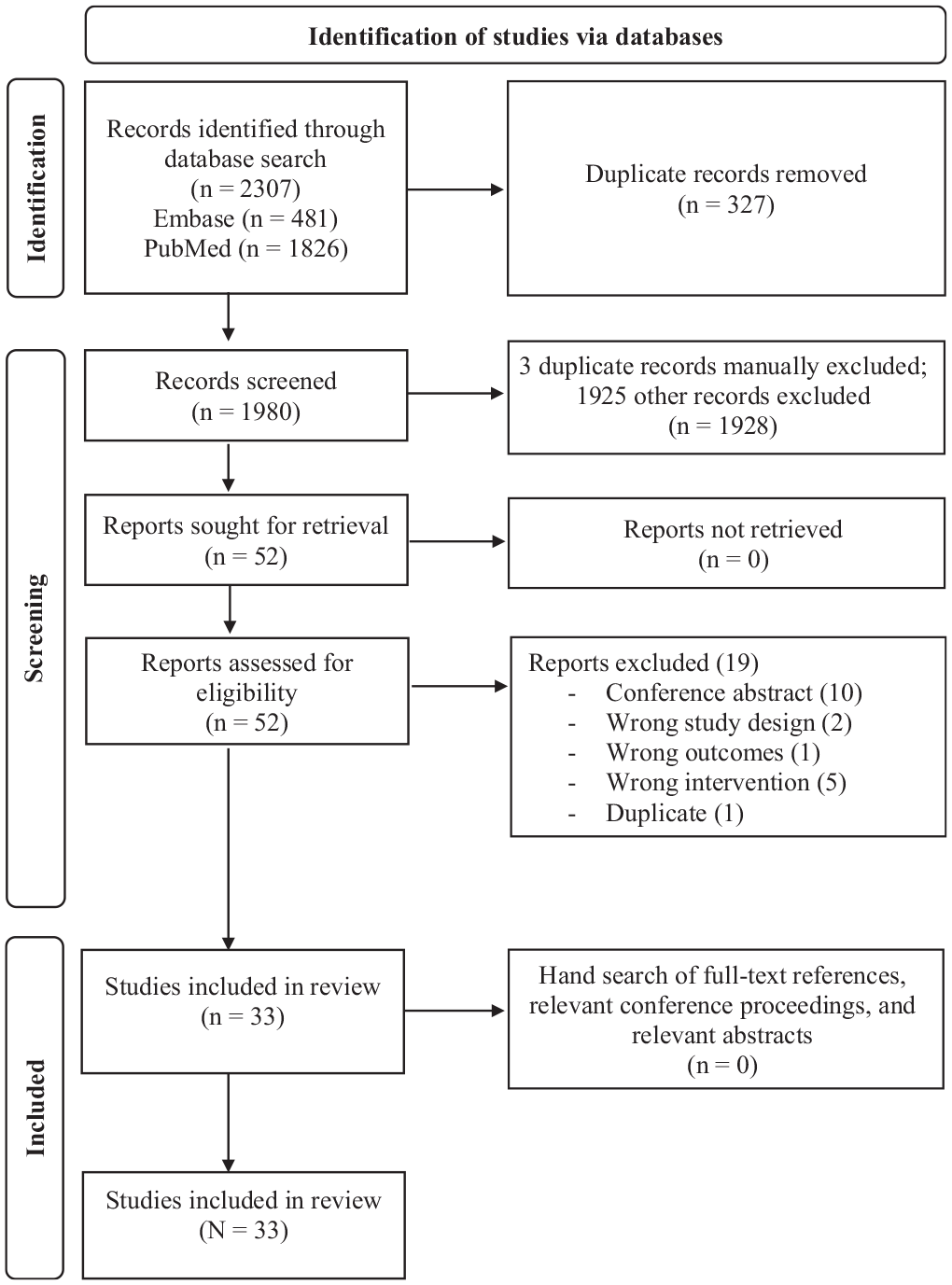
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of study selection.
Study Characteristics
The studies comprised 259 specimens (322 hips) with a mean age of 51.5 years (range, 18-85 years). A total of 24 studies evaluated distraction force or distance to quantify the suction seal. ‖ Ten studies evaluated fluid parameters including peripheral and central compartment intracapsular pressure or volume during or without joint compression or distraction, ¶ and 6 studies evaluated contact forces.3,8,36,56,57,65 A summary of the characteristics of each study is shown in Table 1 and Appendix 2 (available online).
Study Characteristics a
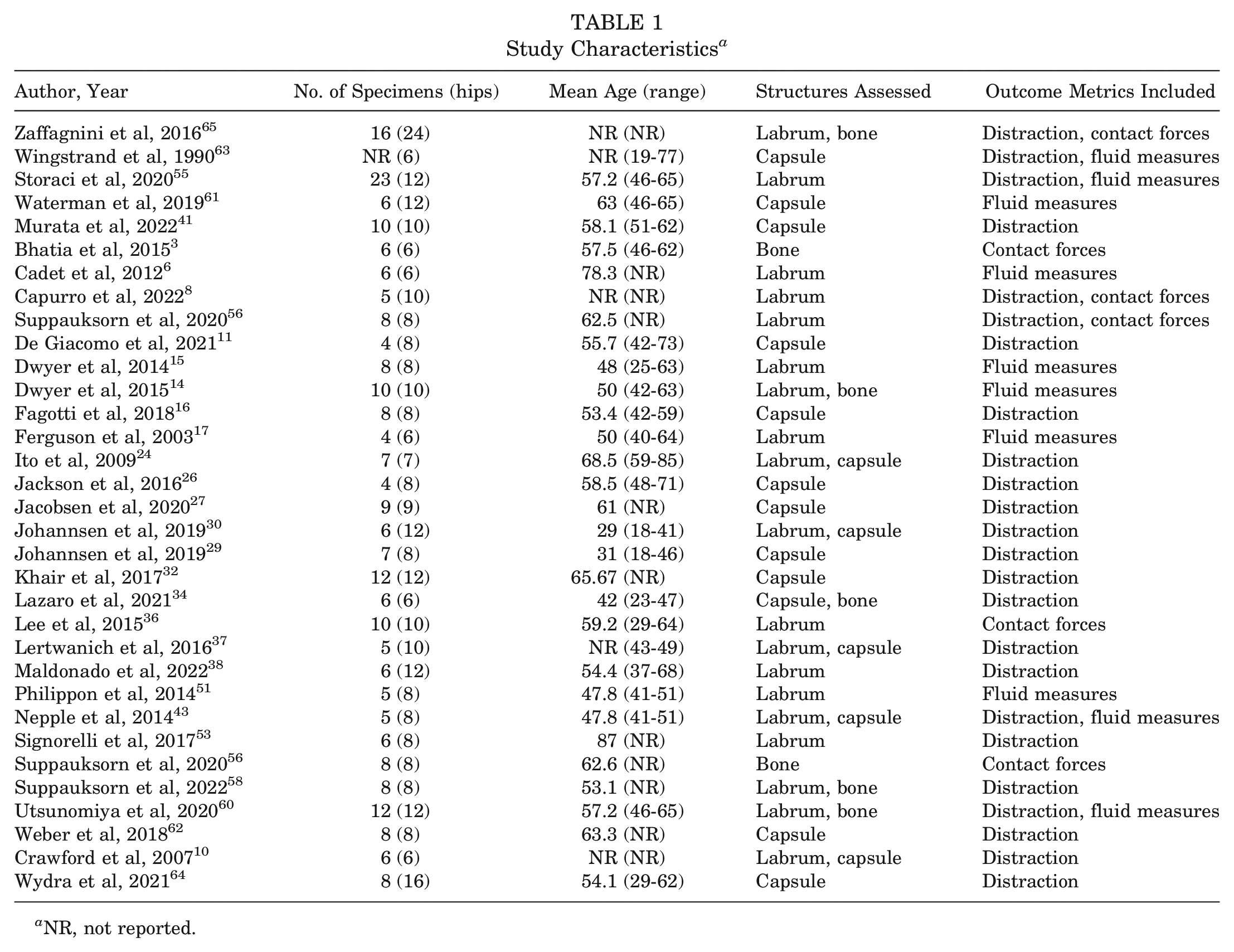
NR, not reported.
Capsule
The capsular contribution to hip stability was quantified using both distraction and fluid outcome metrics in 17 biomechanical cadaveric studies. # Multiple capsular states were investigated including intact, iatrogenic laxity, capsulotomy, repair, reconstruction, and capsulectomy conditions.
Fluid Outcome Metrics
Three studies quantified the capsular contribution to stability through fluid outcome metrics.43,61,63 Two studies measured the negative intra-articular pressure within the central compartment while distracting or rotating the hip joint with an intact capsule.43,63 Waterman et al 61 compared the reduction in central compartment volume after interportal capsular shift or T-capsulotomy plication. Wingstrand et al 63 found no change in intracapsular pressure while rotating the hip about the femoral neck axis. Nepple et al 43 found no correlation between peak intra-articular fluid pressurization and maximal distraction force with an intact capsule, and concluded these 2 functions of the fluid seal may be independent. 51 Waterman et al 61 found similar decreases in intracapsular volume after interportal capsular shift and T-capsular plication compared with baseline. They concluded that both repair strategies result in a decreased capsular volume.
Distraction
Four studies created a capsular laxity model to assess microinstability.26,29,30,41 Two studies simulated iliofemoral ligament laxity by stretching the capsule in extension under 35 N·m of extension torque for 1 hour.26,41 Two studies created capsular laxity by first administering 30 N·m of external rotation torque in a maximally extended hip for 100 cycles at 0.5 Hz, followed by a second round of 1000 cycles of repeated external rotation to the position achieved at the end of the first 100 cycles.29,30 All 4 studies measured the distraction distance under a load control condition from 40 to 200 N to quantify hip stability, and all demonstrated increased femoral head translation in the laxity state compared with an intact capsular state, suggesting decreased stability.
Six biomechanical studies that compared a capsular repair or reconstruction to capsulotomy or capsulectomy were included in a quantitative analysis.16,26,27,32,62,64 All these used similar experimental conditions including an interportal capsulotomy or small capsulectomy with subsequent repair or reconstruction. Two studies added a T-capsulotomy and subsequent repair in addition to the interportal capsulotomy and repair.62,64 Fresh-frozen cadaveric hips were dissected down to the capsule, mounted onto custom testing systems, and assessed for their distractive stability of the hip joint. One study assessed the distraction distance under load control conditions of 40 and 80 N, 26 while the other 5 studies assessed the force required to rupture the suction seal or to distract the hip joint a predetermined distance.16,27,32,62,64 The standardized effect size for distraction between experimental (capsular repair or reconstruction) and control (capsulotomy or capsulectomy) was 1.13 (95% CI, 0.46-1.80; P = .0009; I2 = 55%). The forest plot for distraction in the capsular repair or reconstruction and capsulotomy or capsulectomy settings is demonstrated in Figure 2.
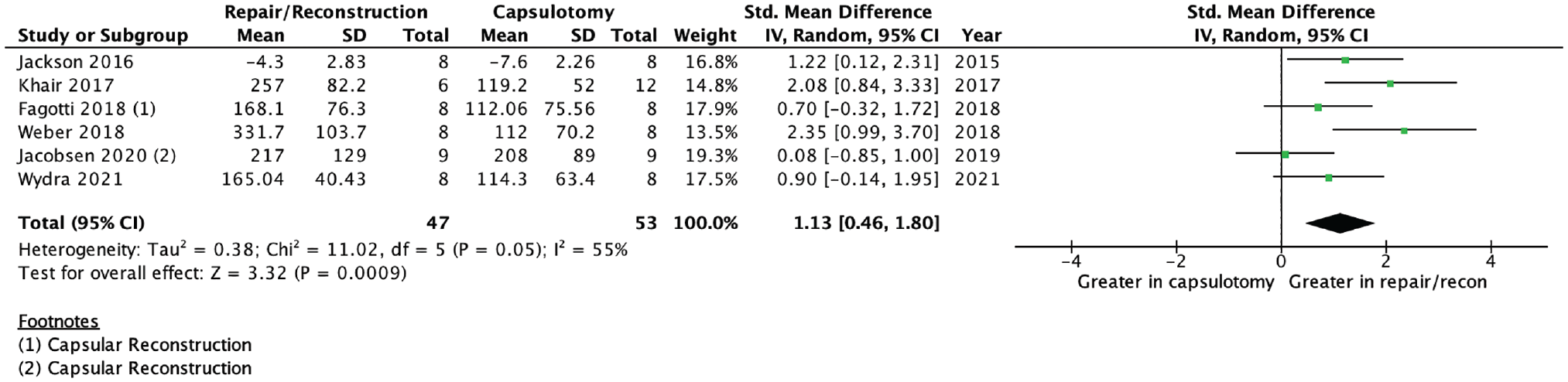
Forest plot demonstrating capsular repair or reconstruction versus capsulotomy or capsulectomy. IV, inverse variance; recon, reconstruction; Std, standardized.
Labrum
The labral contribution to hip stability was quantified using distraction, contact forces, and fluid outcome metrics in 19 biomechanical cadaveric studies. ** Multiple labral states were investigated including intact, tear, repair, augmentation, partial and complete labrectomy, and reconstruction conditions.
Fluid Outcome Metrics
Five studies quantified the labral contribution to stability through fluid outcome metrics only.6,14,15,17,51 Three studies quantified the fluid seal by measuring the fluid efflux from the central compartment during fluid infusion in several conditions and hip positions.6,14,15 Two studies quantified the fluid seal by measuring the fluid pressure within the central compartment in different labral conditions.17,51 Additionally, Ferguson et al 17 also measured the cartilage creep consolidation in intact and labrectomy states to quantify the contribution of the central compartment hydrostatic fluid pressure to cartilage health. All 5 studies confirmed the importance of an intact labrum to the resistance of fluid transport between the central and peripheral compartments. These studies also reproduced an increase in fluid efflux in labral pathology states and pivoting positions involving terminal flexion and internal rotation.6,14,15,17,51
Contact Forces
Three studies quantified the labral contribution to stability through contact forces by inserting a Tekscan pressure sensor between the femoral head and acetabulum to compare the contact pressure, area, and peak force after a labrectomy and labral reconstruction.8,36,56 Capurro et al 8 used a Model 4400 hip-specific Tekscan pressure sensor, while Lee et al 36 and Suppauksorn et al 56 used Model 5101 large Tekscan pressor sensors. Two studies compared a partial labrectomy to a segmental labral reconstruction using a polyurethane scaffold, iliotibial band autograft, or semitendinosus allograft.8,36 Suppauksorn et al 56 compared labral tear and repair conditions with a 270° labral reconstruction using iliotibial band allograft. Two studies also made a qualitative assessment of the suction seal during distraction for each tested condition.8,56 Two studies found increased contact pressure and decreased contact area after partial labrectomy with at least partial restoration of normal acetabular contact areas and pressures after segmental labral reconstruction with a polyurethane scaffold, iliotibial band, or semitendinosus allograft.8,36 Suppauksorn et al 56 reported decreased contact area and increased contact force after a labral reconstruction compared with a labral repair. While Capurro et al reported reestablishment of the suction seal after segmental labral reconstruction in 80% of specimens, Suppauksorn et al 56 reported restoration of the suction seal after 270° labral reconstruction in only 12.5% of specimens. These studies concluded that while a labral reconstruction improves hip stability compared with a labrum-deficient state, it may not restore normal contact forces, areas, and pressures in the hip joint as well as a labral repair.
Distraction
Six of the 19 biomechanical studies that assessed the contribution of the labrum to hip stability were included in quantitative analyses.38,43,53,58,60,65 Five studies that compared a labral repair or reconstruction to a labral tear made up the primary quantitative analysis.43,53,58,60,65 All these studies used similar experimental conditions, including the creation of a labral tear with subsequent repair or reconstruction. Two studies additionally removed abnormal bone morphology via a femoral cam resection or acetabular osteochondroplasty.58,60 Fresh-frozen cadaveric hips were dissected down to the capsule, mounted onto custom testing systems, and assessed for their distractive stability of the hip joint. Two studies assessed the distraction distance under a load control condition,43,53 while the other 3 studies assessed the force required to rupture the suction seal or to distract the hip joint a predetermined distance.58,60,65 The standardized effect size for distraction between experimental (labral repair or reconstruction) and control (labral tear) was −0.67 (95% CI, −1.25 to −0.09; P = .02; I2 = 49%). The forest plot for distraction in the labral repair or reconstruction and labral tear settings is demonstrated in Figure 3.
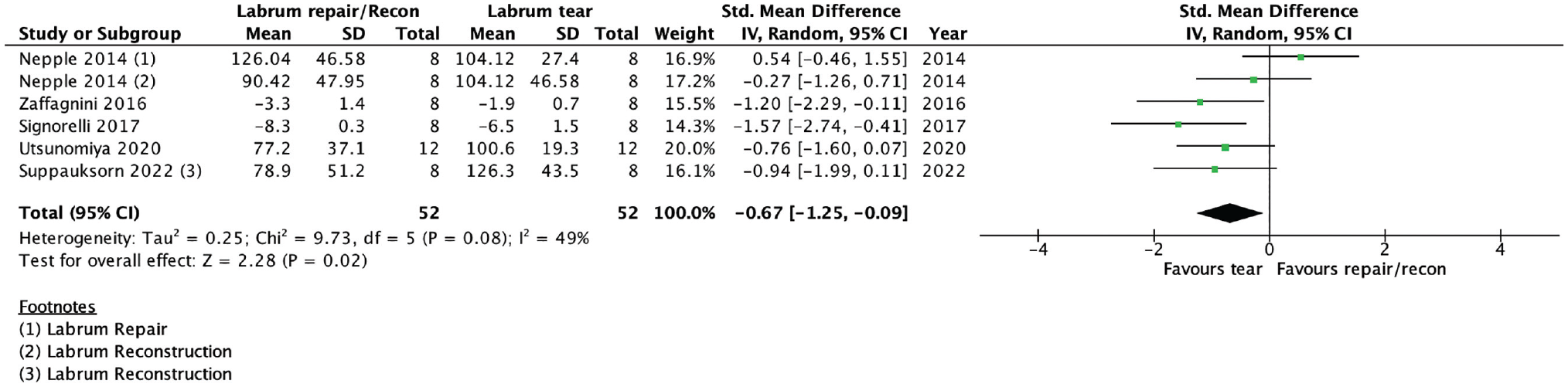
Forest plot demonstrating labral repair or reconstruction versus labral tear. IV, inverse variance; recon, reconstruction; Std, standardized.
A secondary analysis included 4 studies that compared a labral repair or reconstruction to a labrectomy.38,43,53,65 All these studies used similar experimental conditions. Three studies included partial labrectomy and labral repair conditions,43,53,65 and 2 studies included labral reconstruction and complete labrectomy condition.38,43 Fresh-frozen cadaveric hips were dissected down to the capsule, mounted onto custom testing systems, and assessed for their distractive stability of the hip joint. Two studies assessed the distraction distance under a load control condition,53,65 while the other 2 studies assessed the force required to rupture the suction seal or to distract the hip joint a predetermined distance.38,42 The standardized effect size for distraction between experimental (labral repair or reconstruction) and control (labrectomy) was 1.74 (95% CI, 1.23-2.26; P < .00001; I2 = 0%). The forest plot for distraction in the labral repair or reconstruction and labral tear settings is demonstrated in Figure 4.
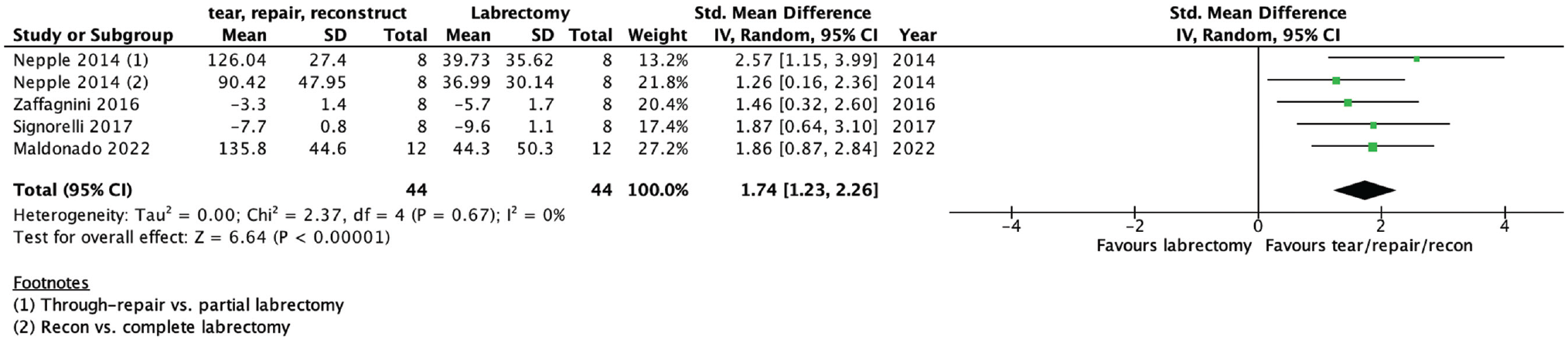
Forest plot demonstrating labral repair or reconstruction versus labrectomy. IV, inverse variance; Std, standardized.
Bone
The bony contribution to hip stability was quantified using distraction, contact forces, and fluid outcome metrics in 7 biomechanical cadaveric studies.3,14,34,57,58,60,65 Multiple bony states were investigated including normal hip congruency, femoral cam morphology with and without acetabular pincer morphology, partial cam resection, complete cam resection, cam overresection, and various degrees of acetabular osteochondroplasty. Two studies assessed native FAIS morphology specifically.14,57 Four studies quantified the contribution of different bony states to hip stability using distraction outcome metrics.34,58,60,65 Both the purpose and the conditions tested in these studies varied broadly.
Fluid Outcome Metrics
Two studies quantified the contribution of different bony states to hip stability using fluid outcome metrics.14,60 Dwyer et al 14 assessed the effect of FAI-induced labral pathology on hip central compartment pressure, and Utsunomiya et al 60 assessed the central compartment pressure in different combined acetabular osteochondroplasty and labral conditions.
Contact Forces
Three studies considered the contribution of different bony states to hip stability using contact stress, contact area, and peak force between the femoral head and acetabulum.3,57,65 Zaffagnini et al 65 found that a hyperextended, externally rotated hip position localizes the contact area to the posterior-superior acetabulum. Bhatia et al 3 reported increased contact area after 4 mm of acetabular rim resection and increased contact pressure and peak force after 6 mm of resection. Suppauksorn et al 57 found a 6.4% and 17.4% decrease in contact pressure after incomplete and complete femoral cam resections, respectively. No quantitative analysis was completed to assess the bony contribution to hip stability secondary to the large variability in the methodology and reporting between included studies.
Outcome Metric Comparison
Four studies assessed both distraction and fluid measures to quantify hip stability.43,55,60,63 Three studies measured the intra-articular pressure and distractive strength in a series of labral, capsular, and bony conditions.43,55,60 Nepple et al 43 found a moderate correlation between peak intra-articular pressure and distractive strength for a series of labral conditions but no correlation between peak pressurization and distractive strength (r = 0.005; not significant) for intact-state specimens. Utsunomiya et al 60 found similar decreases in intra-articular pressure and distractive resistance after labral repair and refixation compared with intact conditions. Storaci et al 55 found a strong correlation between maximum distraction force and peak negative intra-articular pressure (r = −0.83; P = .001) when comparing the suction seal in hips with different labral heights. Wingstrand et al 63 measured changes in intra-articular pressure in different hip positions and completed a separate analysis that measured the maximal distraction force in different capsular conditions.
Three studies assessed both distraction and contact forces to quantify hip stability.8,56,65 Two studies compared the contact stress, contact area, and peak force between the femoral head and acetabulum in different labral states in addition to completing a dichotomous analysis of the suction seal for each state.8,56,65 Capurro et al 8 found lower contact areas, higher contact forces, higher peak forces, and loss of the suction seal with the segmental labrectomy state, while greater contact areas, lower contact forces, lower peak forces, and restoration of the suction seal occurred after segmental labral reconstruction. Suppauksorn et al 56 found greater contact areas and restoration of the suction seal after labral repair compared with lower contact areas and restoration of the suction seal in only 12.5% of specimens after labral reconstruction. Zaffagnini et al 65 compared the distractive distance between multiple labral states and in a separate analysis assessed the contact area between the femoral head and acetabulum during 3 clinical examination maneuvers.
Discussion
There were 2 main findings in this study. First, a capsular repair or reconstruction improved hip stability compared with a capsulotomy or capsulectomy state, respectively. Second, a labral repair or reconstruction did not improve hip stability compared with a labral tear state but did improve stability compared with a labrectomy state. Notably, no quantitative analysis was feasible from studies evaluating the effect of osseous resection on hip stability due to the heterogeneity in methodology and outcome metrics assessed.
Two of the 6 studies included in the capsular quantitative analysis assessed capsulectomy and capsular reconstruction conditions.16,27 It was appropriate to combine the capsular repair and reconstruction states and compare them with the capsulotomy and capsulectomy states for 2 reasons. First, there are similar structural changes between repair and reconstruction, as well as capsulotomy and capsulectomy. An interportal capsulotomy violates the iliofemoral ligament, one of the primary stabilizing structures of the hip capsule, by cutting it perpendicular to its fibers. 50 Both studies that investigated a capsulectomy state created a capsular defect by removing an approximately 20 × 30–mm portion of capsule at the proximal and anterior aspect of the capsule, effectively producing a defect in the iliofemoral ligament.16,27 Second, the relationship between a capsulotomy and capsular repair exhibited the same pattern as a capsulectomy and capsular reconstruction. The improved stability identified in this biomechanical systematic review, paired with supportive clinical evidence suggesting improved clinical outcomes with complete capsular closure, emphasizes the importance of capsular closure in routine hip arthroscopy cases. 2
Labral tear management has been a highly debated topic in hip arthroscopy over the past 20 years. A labral tear may occasionally be an incidental finding, but more commonly it is associated with underlying pathology such as FAIS and contributes to the clinical presentation with groin pain and mechanical symptoms.20,35 The labrum is an important contributor to the suction seal and hip stability, and great focus has been directed toward restoring its function when injured or damaged, with an emphasis on repair, or reconstruction when repair is not feasible. 5 This review suggests that repairing a labral tear does not always restore its normal suction seal function. In fact, in the presence of cam morphology, an isolated labral repair may increase strain in the cartilage at the chondrolabral junction. 59 The labral repair strategy also has a biomechanical effect on the suction seal. A vertical mattress repair fixes the base of the labrum back to the acetabular rim while leaving the outer edge free to potentially contribute to the suction seal during distraction. In contrast, a simple suture repair strategy cinches the labrum circumferentially, resulting in less contact area between the labrum and femoral head. Signorelli et al 53 and Zaffagnini et al 65 both showed greater resistance to distraction after a vertical mattress labral repair compared with a simple suture repair. However, previous research has found no difference in patient-reported outcomes based on repair technique. 25 Last, labrectomy significantly decreases the distractive strength of the hip compared with either labral tear or repair. If a labral tear is symptomatic and must be addressed, our findings suggest that it is most important to avoid excision of the torn labrum, and that either a labral repair or reconstruction would be a better option to maintain at least partial hip stability.
A third finding of this study was that there may be a correlation between distraction, intra-articular pressure, and contact forces as outcome metrics for hip stability, but further investigation is needed. The correlation between distractive strength and intracapsular pressure may be hypothesized based on the law of Boyle: P∝ 1/V, where P is the pressure and V is the volume. 18 If it is assumed that an intact hip capsule is fluid-tight and maintains a constant temperature, then when the intracapsular volume increases during hip distraction, the pressure must decrease. This finding was replicated in all 3 studies that reported both intra-articular pressure and distractive strength.43,55,60 Nepple et al 43 found a moderate correlation between peak intra-articular pressure and distractive strength for a series of labral conditions but no correlation between peak pressurization and distractive strength (r = 0.005; not significant) for intact-state specimens. They concluded that the distractive stability and fluid pressurization functions of the labrum may be independent because of the lack of correlation. Fluid pressurization (intra-articular fluid and interstitial fluid within articular cartilage during compressive loads) 51 is not equivalent to intra-articular pressure and may have a different relationship to distraction than intra-articular pressure.
A relationship between contact area, contact force, peak contact pressures, and distraction strength may also exist. Capurro et al 8 reported restoration of the suction seal, higher contact areas, lower contact forces, and lower peak forces after a labral reconstruction compared with a partial labrectomy. Similarly, Suppauksorn et al 56 reported restoration of the suction seal and greater contact areas after a labral repair compared with a labral reconstruction. It may be that soft tissue and bony conditions that increase contact areas and decrease contact forces between the femoral head and acetabulum also contribute to greater distractive strength. However, no study in this review compared these 2 outcome measures on continuous scales. Further investigation is warranted to identify this potential relationship.
Strengths
This review considered the contribution of several anatomic structures through multiple outcome metrics to add to our current understanding of hip stability, how it differs in pathologic states, and how it changes with surgical intervention. We used rigorous methods with predetermined objectives, strict inclusion and exclusion criteria, and a standardized method of assessment a priori to carry out a reproducible search and report relevant results. This review also strengthens the biomechanical evidence underlying current trends in the management of FAIS and other hip pathology. Gupta et al 21 reported that 100% of hip arthroscopy surgeons perform a labral repair when a labral tear is present and 88.9% perform a capsular closure at the end of surgery in most cases. Five-year patient-reported outcomes, patient satisfaction, rate of revision surgery, and conversion to hip arthroplasty after hip arthroscopy favor complete capsular repair.13,19 Additionally, patients who undergo labral repair are less likely to be converted to THA within 10 years compared with those who undergo labral debridement. 33 This review supports avoiding labral debridement when managing symptomatic labral tears and performing interportal capsulotomy repair to restore stability during hip arthroscopy.
Limitations
The heterogeneity among included studies in this systematic review limited the ability to complete large comparative analyses. The variability in methodology including biomechanical setup, surgical technique, and outcome measures limited our quantitative analyses to comprise less than half of all available biomechanical studies included in our systematic review. Second, the mean age of the cadavers was 51.5 years, and most studies only included hips with normal morphology. This demographic does not accurately reflect the young hip with FAIS that most commonly undergoes hip arthroscopy. Third, the in vitro setting of the included studies introduced multiple limitations. In most studies, the surrounding soft tissues were dissected down to the level of the capsule, so any synergistic stability normally afforded by those tissues was removed. Furthermore, the instability states created were iatrogenic in nature, dissimilar to the clinical pathology generally seen in patients. For example, iatrogenic labral tears were mostly a single, longitudinal, full-thickness incision, usually at the chondrolabral junction, without the associated fraying, cartilage extension, and unstable flaps commonly seen in vivo. 20 Additionally, the in vitro surgical correction was mostly completed in an open fashion, as opposed to an in vivo setting where surgery is done arthroscopically. Last, changes in range of motion secondary to applied rotational forces was not included as an outcome measure in our review. This decision was made in the context of a previous systematic review completed by Jimenez et al, 28 which assessed predominantly the rotational differences after capsular repair compared with capsular release.
Future Directions
A comparison of different outcome metrics used to assess hip stability will help define new soft tissue and bony stabilizer functions. Understanding the relationship between these outcome metrics will also help make further conclusions about previously completed biomechanical research. An inverse relationship between intra-articular pressure and distraction strength likely exists and deserves further study. Second, a comparison of the relative contributions of the labrum, capsule, and bone to hip stability would help clinicians understand what the most important aspects of the hip are and how to address them to maximize stability and patient function. It may be that the native conchoidal shape of the femoral head is essential to maintain the labral seal and distribute load, and the optimal degree of cam resection should be individualized based on underlying femoral head and labral anatomy.39,46 Third, a biomechanical assessment of the suction seal strength after a vertical mattress labral repair compared with a labral tear would be interesting to determine whether the labral fixation strategy was a contributing factor to the findings of this study. Last, the effective management of loss of the suction seal and instability secondary to iatrogenic cam overresection is a relatively understudied area. The hip remplissage is a suggested solution but does not have the same underlying biomechanical principles as a remplissage for anterior shoulder instability, and current evidence is limited to a level 4 small-sample case series. 1 Future investigation using multiple outcome metrics regarding techniques to restore hip stability after cam overresection is warranted.
Conclusion
Most biomechanical evidence supports capsulotomy repair or reconstruction to improve hip distractive stability at the end of hip arthroscopic surgery. While the repair of a torn labrum does not improve distractive resistance, it is superior to labral debridement in most biomechanical studies.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465231208193 – Supplemental material for The Contribution of Soft Tissue and Bony Stabilizers to the Hip Suction Seal: A Systematic Review of Biomechanical Studies
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231208193 for The Contribution of Soft Tissue and Bony Stabilizers to the Hip Suction Seal: A Systematic Review of Biomechanical Studies by Alexander J. Hoffer, Wouter Beel, K.C. Geoffrey Ng and Ryan M. Degen in The American Journal of Sports Medicine
Footnotes
Submitted May 3, 2023; accepted August 30, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at https://education.sportsmed.org/Public/Catalog/Home.aspx?CourseSearch=1&Criteria=9&Option=25. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.