
Abstract
Background:
The pathology of dorsal wrist pain in gymnasts without abnormal radiographic findings remains unclear.
Purpose/Hypothesis:
The purpose of this study was to identify abnormal wrist sagittal kinematics in gymnasts with dorsal wrist pain. It was hypothesized that gymnasts with dorsal wrist pain would show abnormal sagittal kinematics with reversible hypermobility of the intercarpal joint.
Study Design:
Controlled laboratory study.
Methods:
Participants included 19 wrists in male gymnasts with dorsal wrist pain, 18 wrist in male gymnasts without wrist pain, and 20 adult men without a history of wrist pain. Magnetic resonance imaging (T2-weighted sagittal images) findings at 0°, 30°, 60°, and 90° of wrist extension were used in kinematic analysis. The angles and translations of the radiolunate, capitolunate, and third carpometacarpal joint were measured and compared between the 3 groups.
Results:
At 90° of wrist extension, gymnasts with dorsal wrist pain had a significantly lower radiolunate joint angle (28.70°± 6.28° vs 36.19°± 7.81°; P = .020) and a significantly higher capitolunate joint angle (57.99°± 6.15° vs 50.50°± 6.98°; P = .004) and distal translation (1.17 ± 0.50 mm vs 0.46 ± 0.62 mm; P = .002) than gymnasts without dorsal wrist pain.
Conclusion:
Gymnasts with dorsal wrist pain showed abnormal wrist sagittal kinematics. These novel findings may facilitate understanding of dorsal wrist pain, which can be recognized as a new syndrome termed “gymnast’s lunate dyskinesia.”
Gymnastics has the highest prevalence14,24 and incidence9,25 of wrist injury from overuse among all sports with a focus on wrist loading. 28 Overall, 75% of male gymnasts and 33% of female gymnasts experienced wrist pain for ≥4 months, 32 and the wrist is the most affected joint among male gymnasts. 55 In fact, 47% of gymnasts have limited performance 19 and 21% miss ≥1 practice per month 15 because of this pain. One of the most common wrist injuries is the distal radial physeal injury, termed “gymnast’s wrist.”3,16,36 Other disorders that present with dorsal wrist pain include wrist capsulitis, dorsal wrist impingement, and occult dorsal ganglion cysts, which exhibit abnormal radiological findings. However, in clinical practice, many gymnasts complain of dorsal wrist pain without abnormal radiological findings, restriction of range of motion, or inflammatory signs, including local swelling or warmth. Additionally, it is characterized by reversible pain that is often relieved by nonoperative treatment. This pain is often problematic at the moment of hyperextension while the wrist joint is load bearing during pommel horse or floor exercises.15,32 From a kinetic perspective, these loading parameters are comparable with those encountered at heel strike during running. 34 However, from a kinematic perspective, the mechanism remains unclear. We speculate that strong axial pressure applied during wrist extension causes hypermobility in the sagittal plane at the intercarpal joint. Because sagittal plane motion is nearly uniplanar 47 and frontal and horizontal intercarpal motions are minimal in this plane, 26 wrist extension can be validly evaluated using a 2-dimensional sagittal scan. 49 Yet, treatment of dorsal wrist pain with these characteristics is challenging because the cause of pain remains unclear. Understanding the mechanism of this pain is crucial, as it can serve as a strategy for finding the most appropriate treatment. Therefore, this study aimed to determine if there is a significant association between wrist sagittal kinematics and dorsal wrist pain in gymnasts using magnetic resonance imaging (MRI). We hypothesized that gymnasts with dorsal wrist pain would show abnormal sagittal kinematics with reversible hypermobility of the intercarpal joint.
Methods
Ethics Statements
This study was approved by the institutional ethics committee, and all study participants signed a consent form before enrollment in the study. Before study commencement, informed consent was obtained from the parents or guardians of participants who were underage.
Study Design and Population
This study included 40 wrist joints of 20 high school male gymnasts who participated in the national competition and 20 wrist joints of 20 healthy adult men with no history of wrist pain. The patient selection process for this study is summarized in Figure 1. The wrist joints were classified into 3 groups: 40 wrist joints of gymnasts were classified into pain and painless groups, and 20 wrist joints of healthy men were classified as the control group. The selection criteria were MRI scans with no abnormal findings and passive wrist extension excursion >90°, which were common for all groups. In cases where fracture or bone deformity, arthritis or osteoarthritis, soft tissue inflammation or injury, or nodules or tumors were observed on sagittal MRI, we excluded participants.
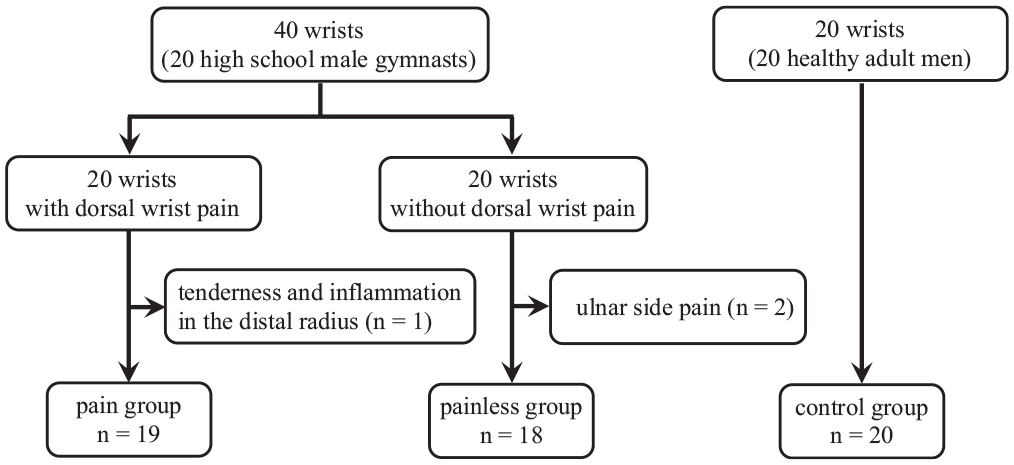
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) diagram showing the patient selection process. Of the 40 wrists in 20 gymnasts, 10 wrists in 5 gymnasts with bilateral pain, 10 wrists in 5 gymnasts with bilateral painless, 9 wrists in 9 gymnasts with unilateral pain, and 8 wrists in 8 gymnasts with unilateral painless.
The pain group consisted of 20 male gymnasts who had dorsal wrist pain at the moment of performance with hyperextension of the wrist during load bearing. The pain was located in the middorsal wrist joint, and no patient had scaphoid pain. After excluding 1 wrist joint because of the presence of tenderness and inflammation in the distal radius, 19 wrists were finally included in the pain group: 10 wrists in 5 gymnasts with bilateral pain and 9 wrists in 9 gymnasts with unilateral pain. The painless group consisted of 20 wrists with no history of wrist pain in the previous 3 months. All participants in the painless group had a history of dorsal wrist pain. After excluding 2 wrists with ulnar side pain without dorsal wrist pain, 18 wrists were included in the painless group: 10 wrists with bilateral painless (5 patients) and 8 wrists with unilateral painless (8 patients).
The control group comprised 20 adult male wrists; we recruited the youngest adult men who worked at the author's facility and were nongymnasts with no history of wrist pain.
Imaging Method
An MRI scanner (AIRIS II Confort 0.3T; Hitachi Medical) was used to visualize the radiolunate, capitolunate, and third carpometacarpal joints, and all imaging was performed at our institution. Sagittal images of the wrists (T2-weighted; slice thickness, 3 mm; imaging time, 60 seconds) and a neck coil were used. The imaging position is shown in Figure 2A. Measurement in the prone position is stable and reproducible, generalized as the standard imaging method of the wrist joint, and excellent for comparative assessment. 39 The wrist joint was fixed using originally designed equipment made of styrene foam, in which the angle of the wrist can be set at 30° intervals from 0° to 90° of wrist extension (Figure 2B). The fixation requirements were as follows: 3 points on the proximal forearm, distal forearm, and back of the hand were fixed with an elastic band, and the palm surface was made to adhere to the fixation device. For the adhesion requirement, the pisiform was in contact with the fixation device. We also confirmed that there was no pain in the wrist joint during imaging in all participants. After MRI, it was confirmed that the radial and third metacarpal axes were aligned from the frontal plane. In addition, because some gymnasts were <20 years, we checked that the carpals were sufficiently ossified to ensure that the results would not be affected. 23
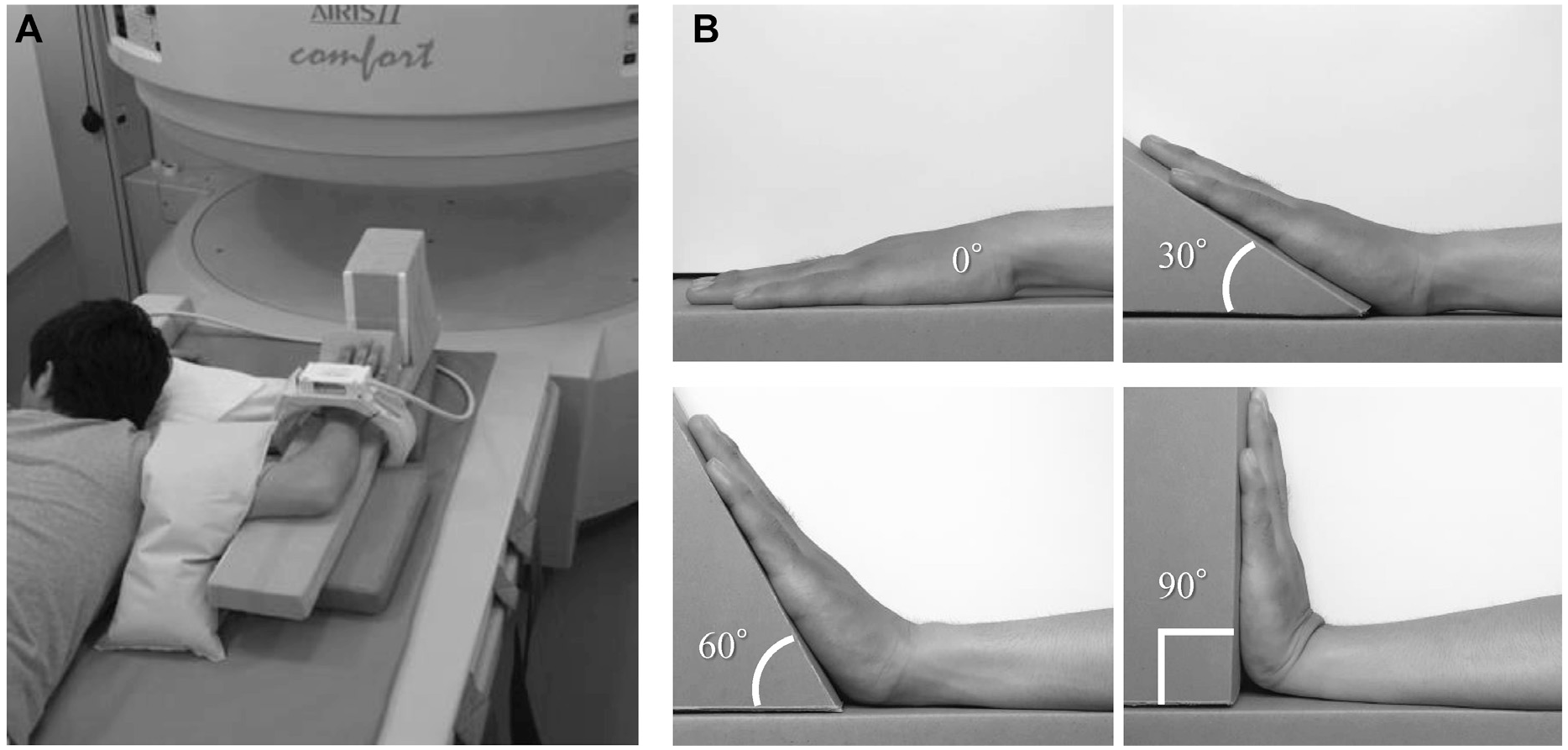
Magnetic resonance imaging method. (A) Imaging was performed with the participant in the prone position at 90° of shoulder abduction, 90° of elbow flexion, neutral position of the wrist radial/ulnar deviation, and neutral position of forearm pronation/supination. (B) Imaging of the wrist joint was performed in 4 positions, in which the angles made by the forearm ventral surface and palm surface were at 0°, 30°, 60°, and 90° of wrist extension.
MRI Analysis
The kinematics of the wrist joints were analyzed by measuring the joint angles and translations of the radiolunate, capitolunate, and third carpometacarpal joints using sagittal MRI (1520 × 1930 pixels; pixel size, 0.103 × 0.103 mm). Using National Institutes of Health ImageJ Version 1.45, we measured the coordinates of 14 marks (Figure 3) for the joint angle measurement and 16 marks (Figure 4) for the joint translation measurement from 11 images of the sagittal plane at 0°, 30°, 60°, and 90° of wrist extension, with the upper-left corner of the image as the origin (0, 0). For all marks, 11 sagittal slices were selected, respectively, that met the definition, and the coordinates were measured from those slices. All measured coordinates were transformed with the distal palmar edge of the radius as the origin (0, 0) to produce the kinematics of the rigid body, as shown in Figure 5. The angles and translation of the radiolunate, capitolunate, and third carpometacarpal joint (2-dimensional distances and x- and y-axis directions between the center marks of each articular surface) were calculated from the coordinate system obtained by coordinate transformation. The center coordinates of the articular surface were calculated using the least squares method of the circle, as the center coordinates of the approximate circle of the articular surface. The x-axis was the radial axis (plus on the x-axis indicates the distal direction), and the y-axis was the vertical axis to the x-axis through the distal volar edge of the radius (plus on the y-axis indicates the dorsal direction).
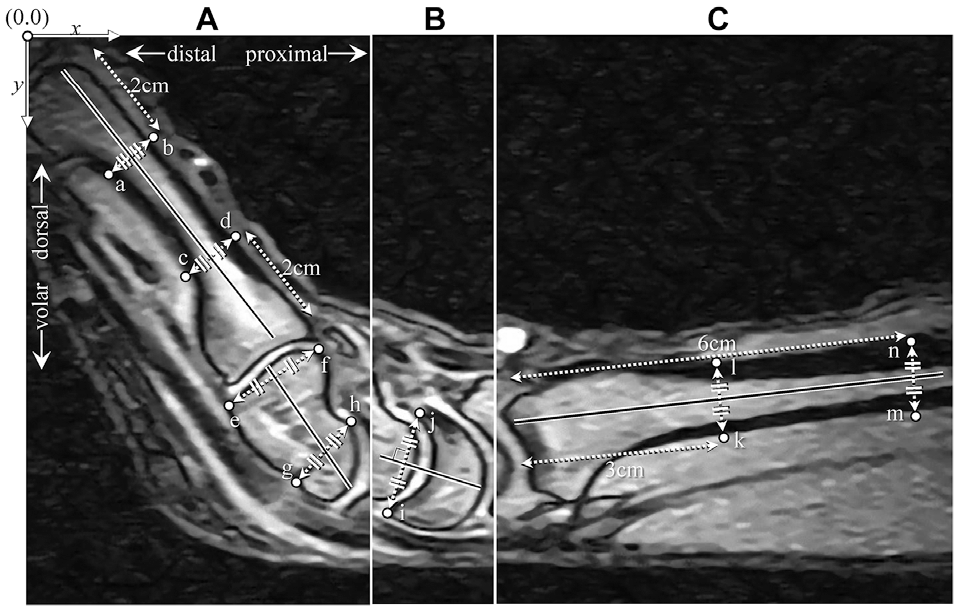
Magnetic resonance imaging measurement method for analyzing the joint angles of the radiolunate, capitolunate, and third carpometacarpal joints. (A) The angle of the third metacarpal was defined as the inclination of the line connecting the midpoints of marks a and b to c and d. Marks a, b, c, and d are the superficial surfaces of the third metacarpal bodies. The angle of the capitate was defined as the inclination of the line connecting the midpoints of marks e and f to g and h. Marks e and f are the most dorsal and volar points of the capitate distal articular surface, and marks g and h are the most dorsal and volar points of the capitate proximal articular surface. (B) The lunate angle was defined as the inclination of the vertical axis passing through the midpoint of marks i and j. Marks i and j are the most dorsal and volar points of the lunate distal articular surface, respectively. (C) The radius angle was defined as the angle of the line connecting the midpoints of marks k and l to m and n. Marks k, l, m, and n are the superficial surfaces of the radius shafts.
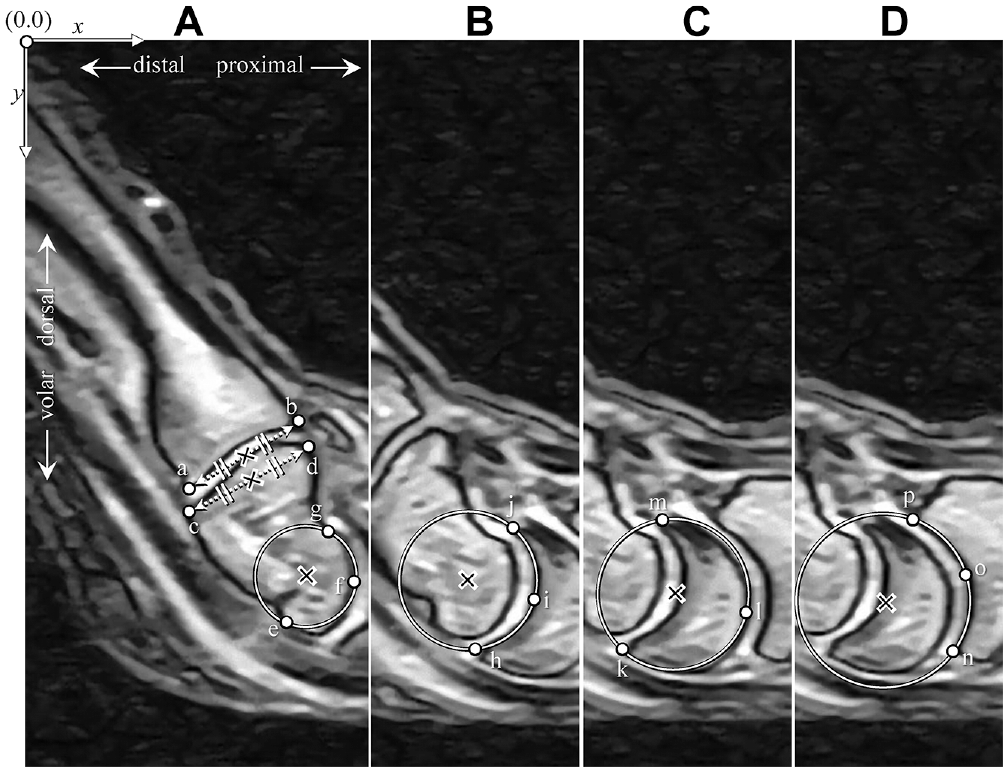
Magnetic resonance imaging measurement method for analyzing joint translation of the radiolunate, capitolunate, and third carpometacarpal joints. (A) The center of the third metacarpal, indicated by a cross, was defined as the midpoint of the line connecting marks a and b. Marks a and b are the most dorsal and volar points of the third metacarpal proximal articular surface, respectively. The center of the capitate distal articular surface, indicated by a cross, was defined as the midpoint of the line connecting marks c and d. Marks c and d are the most dorsal and volar points of the capitate distal articular surface, respectively. The center of the capitate proximal articular surface, indicated by a cross, was defined as the center of the approximate curvature of a circle calculated from marks e, f, and g. Marks e, f, and g are the most volar, middorsal, and most dorsal points of the capitate proximal articular surface, respectively. (B) The center of lunate distal articular surface, indicated by a cross, was defined as the center of the curvature approximate of a circle calculated from marks h, i, and j. Marks h, i, and j are the most volar, middorsal, and most dorsal points of the lunate distal articular surface, respectively. (C) The center of the lunate proximal articular surface, indicated by a cross, was defined as the center of the curvature approximate of a circle calculated from marks k, l, and m. Marks k, l, and m are the most volar, middorsal, and most dorsal points of the lunate proximal articular surface, respectively. (D) The center of the radius of the distal articular surface, indicated by a cross, was defined as the center of the curvature approximate of a circle calculated from marks n, o, and p. Marks n, o, and p are the most volar, middorsal, and most dorsal points of the radius distal articular surface, respectively.
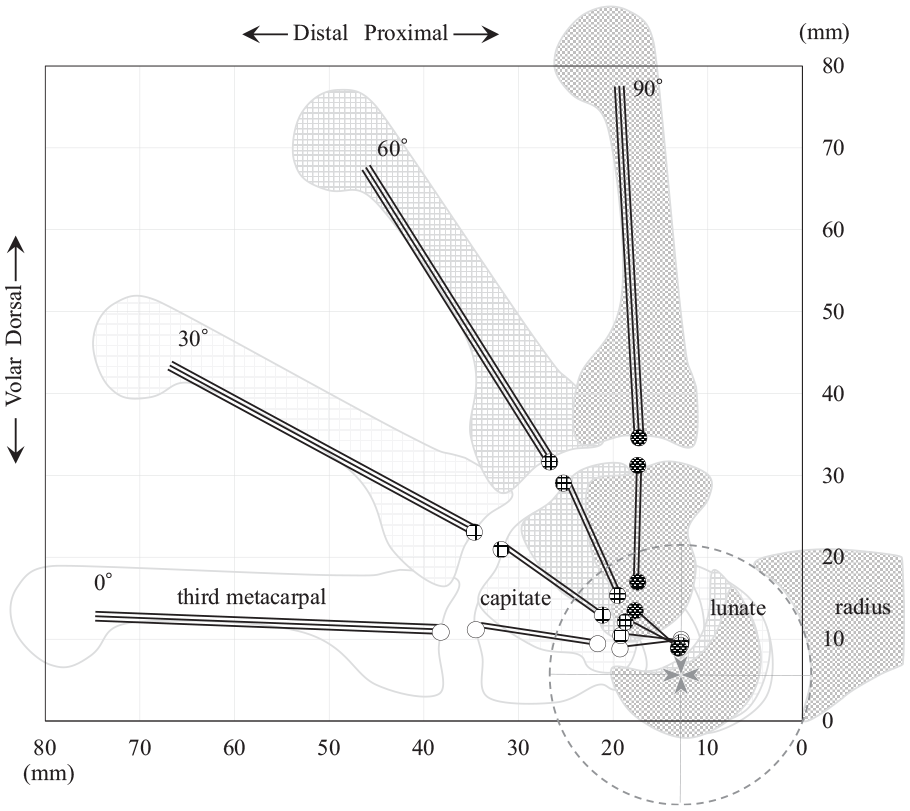
Rigid body model of wrist sagittal kinematics. The coordinates from the magnetic resonance imaging analysis were transformed so that the origin (0, 0) was the volar end of the distal articular surface of the radius, and the radius shaft was parallel to the x-axis to create the sagittal kinematics of the rigid body model. The tips of the 4 arrows indicate the center of the distal articular surface of the radius, commonly at 0°, 30°, 60°, and 90° of wrist extension. The triple line is the third metacarpal, the double line is the capitate, and the single line is the lunate. The inclination of all lines indicates the angle of each bone. The starting point indicates the center of the proximal articular surface, and the endpoint indicates the center of the distal articular surface.
Statistical Analysis
Descriptive statistics are reported as means, standard deviations, and ranges. One-way analysis of variance (ANOVA), Welch ANOVA, or the Kruskal-Wallis test were used to compare clinical and morphological characteristics, as well as angles and translations of the radiolunate, capitolunate, and third carpometacarpal joints at 0°, 30°, 60°, and 90° of wrist extension between the pain, painless, and control groups. When significant differences were observed, the Games-Howell, Tukey, or Steel-Dwass test was used to perform multiple comparisons. Because the pain and painless groups included bilateral cases, independence was confirmed by examining the correlation between the left and right wrists. In this study, the total sample size was 57 participants. A post hoc power analysis revealed that the study was 80% powered to detect an effect size >0.40. Statistical significance was set at P < .05. Data were analyzed using R Version 4.1.2 (CRAN).
In total, 26 images were measured twice by a single rater (physical therapist, T.S.) at an interval of 6 months to validate the relative and absolute reliability assessments. Moreover, a single rater (physical therapist) measured once to validate interobserver reliability. This was achieved by calculating 2 separate measures of agreement: the intraclass correlation coefficient 27 (ICC) and the Bland-Altman 95% limit of agreement (LOA). 6
Results
Comparison of Clinical and Morphological Features
Age, height, and body weight were significantly higher in the control group than in the pain and painless groups, and there were no significant differences in body mass index between the groups. The control group had significantly lower palmar tilt than the pain and painless groups. However, there were no significant differences in palmar tilt between the pain and painless groups (Table 1).
Comparison of Clinical and Morphological Features a
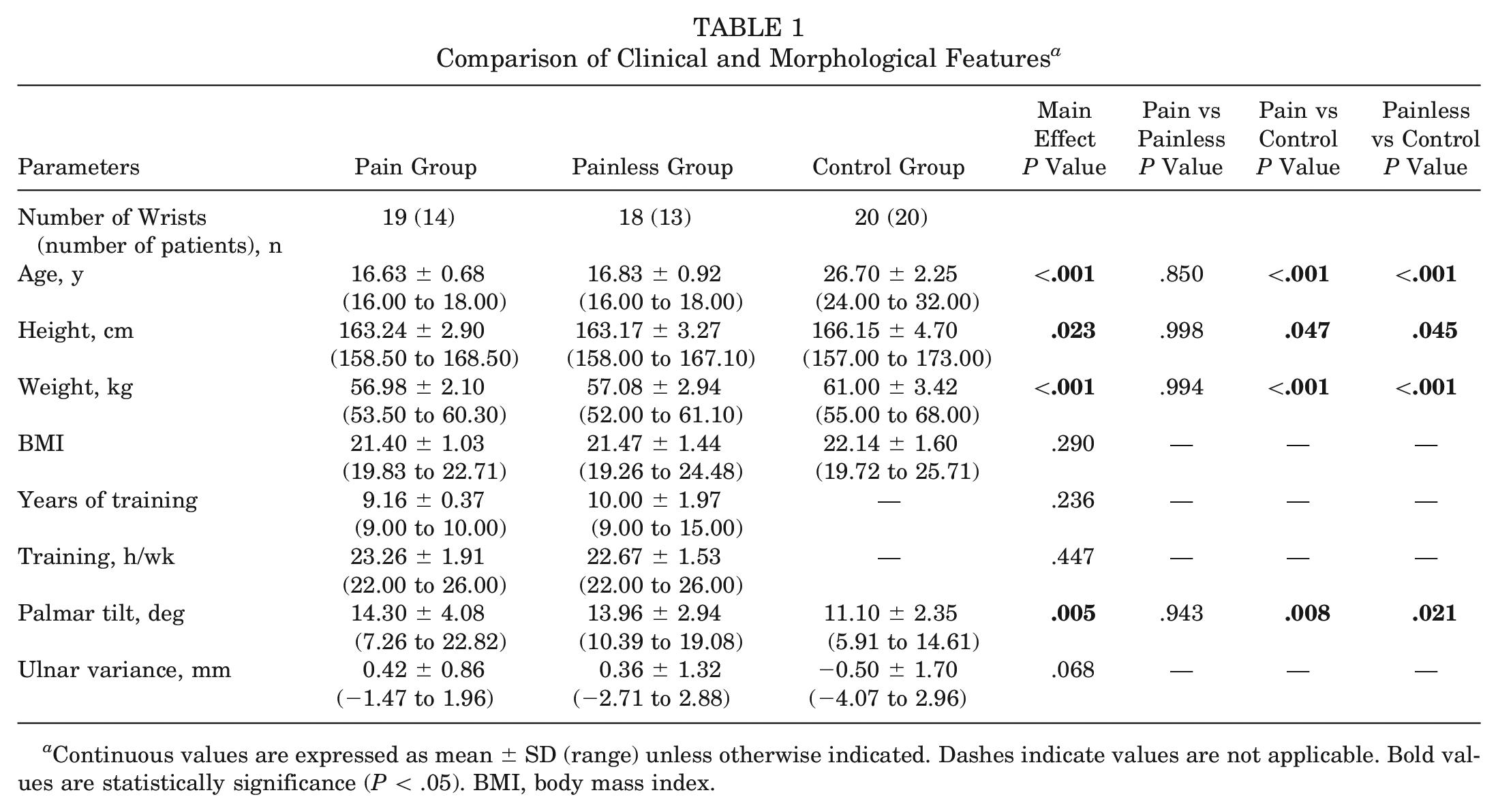
Continuous values are expressed as mean ± SD (range) unless otherwise indicated. Dashes indicate values are not applicable. Bold values are statistically significance (P < .05). BMI, body mass index.
Comparison of the Radiolunate Joint Angle and Translation
The angle of the radiolunate joint at 90° of wrist extension was significantly lower in the pain group than in the painless and control groups (P = .020 and P < .001, respectively). The 2-dimensional radiolunate translation at 0° of wrist extension was significantly higher in the pain group than in the control group (P = .032) (Table 2).
Comparison of Radiolunate Joint Angle and Translation a
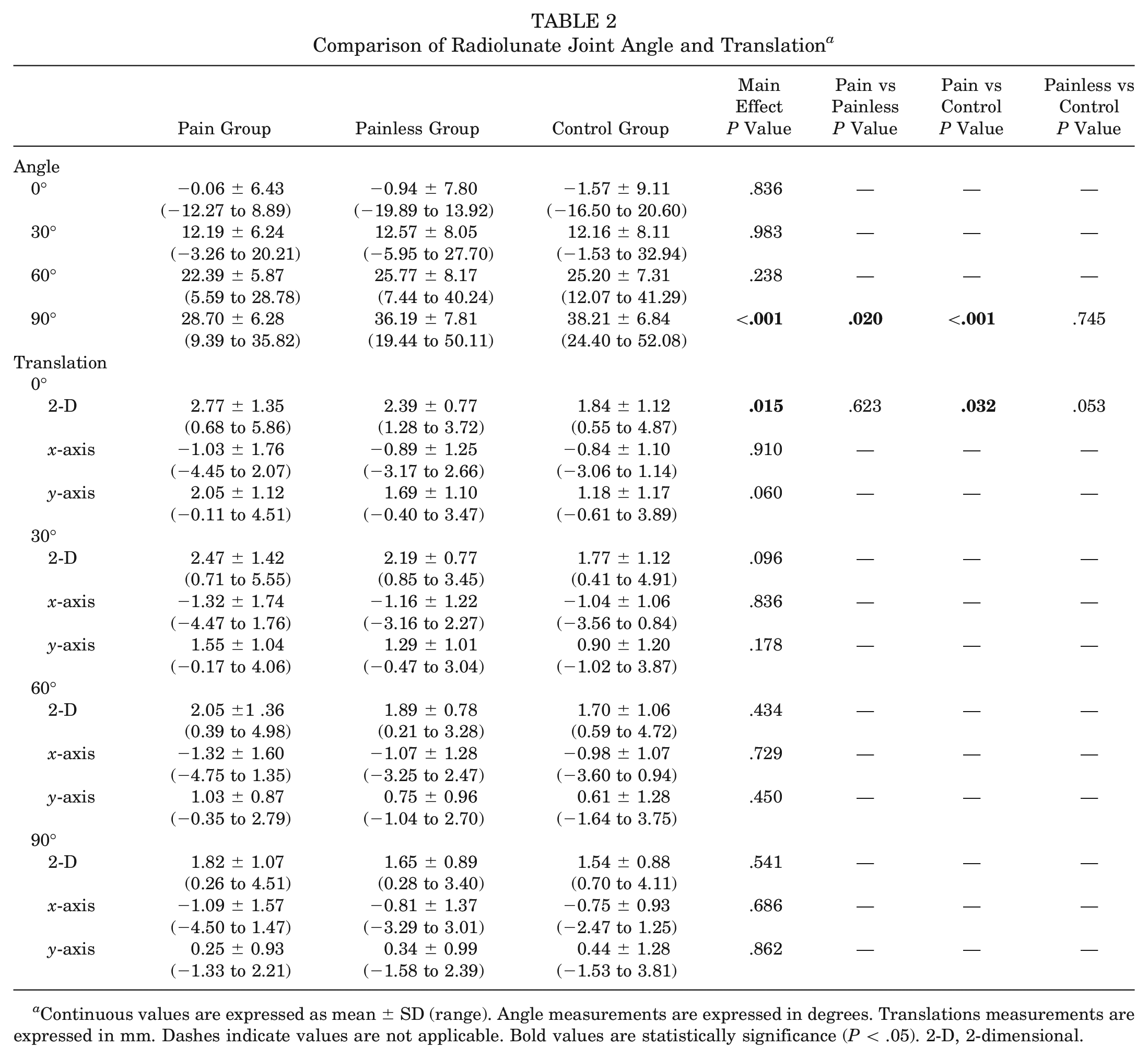
Continuous values are expressed as mean ± SD (range). Angle measurements are expressed in degrees. Translations measurements are expressed in mm. Dashes indicate values are not applicable Bold values are statistically significance (P < .05). 2-D, 2-dimensional.
Comparison of the Capitolunate Joint Angle and Translation
The capitolunate joint angles at 30° and 60° of wrist extension were significantly higher in the pain group than in the control group (P = .038 and P = .004, respectively). The angle at 90° of wrist extension was significantly higher in the pain group than in the painless and control groups (P = .004 and P < .001, respectively). The 2-dimensional and y-axis translations at 90° of wrist extension were significantly higher in the pain group than in the control group (P = .006 and P = .046, respectively). The x-axis translation at 90° of wrist extension was significantly higher in the pain group than in the painless group (P = .002) (Table 3).
Comparison of Capitolunate Joint Angle and Translation a
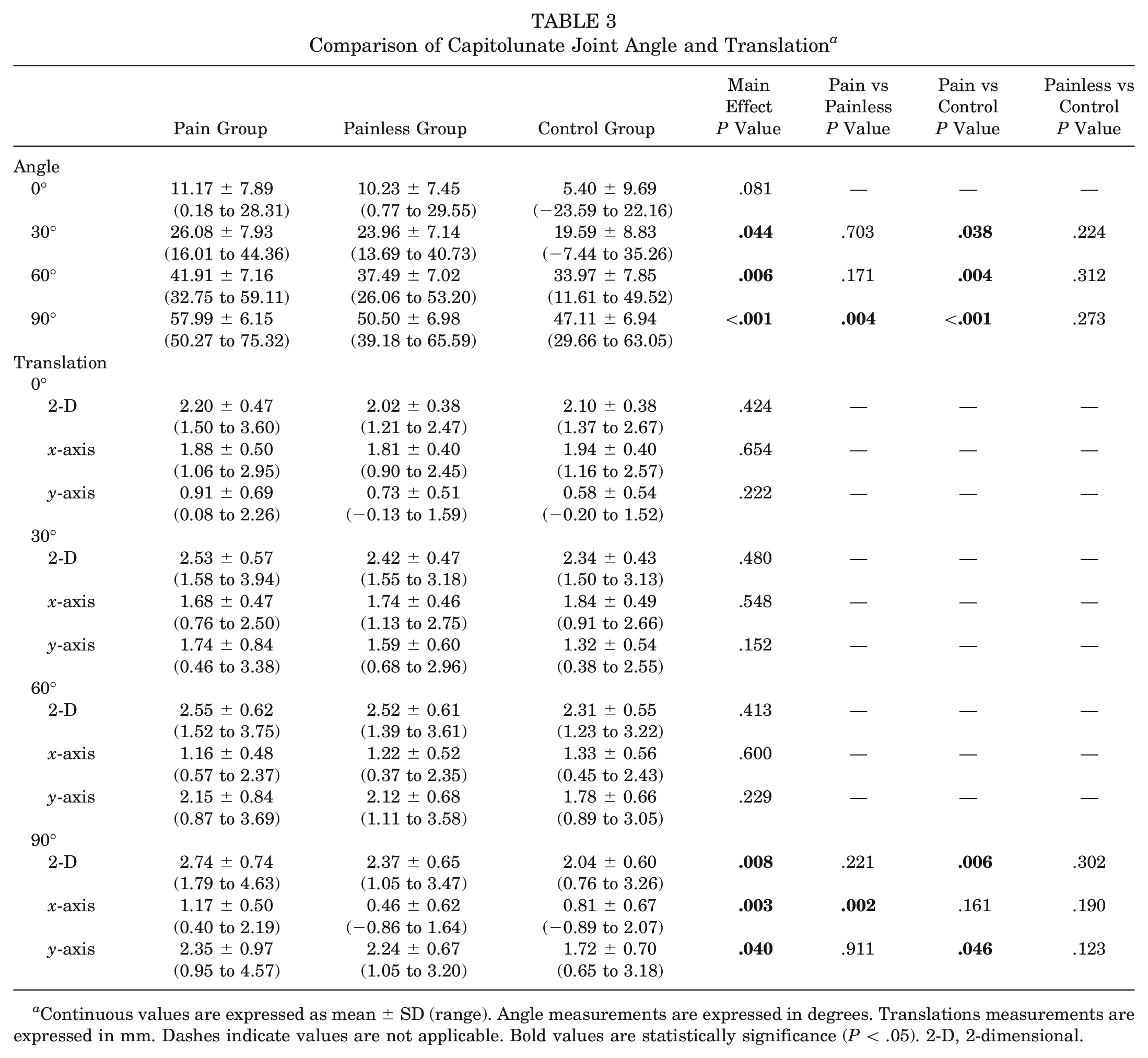
Continuous values are expressed as mean ± SD (range). Angle measurements are expressed in degrees. Translations measurements are expressed in mm. Dashes indicate values are not applicable. Bold values are statistically significance (P < .05). 2-D, 2-dimensional.
Comparison of the Third Carpometacarpal Joint Angle and Translation
The third carpometacarpal joint angles at 0°, 30°, and 60° of wrist extension were significantly higher in the control group than in the pain and painless groups (0°: P < .001 and P = .003; 30°: P < .001 and P = .005; and 60°: P < .001 and P = .018). The y-axis translation at 90° of wrist extension was significantly higher in the pain group than in the control group (P = .034) (Table 4).
Comparison of Third Carpometacarpal Joint Angle and Translation a
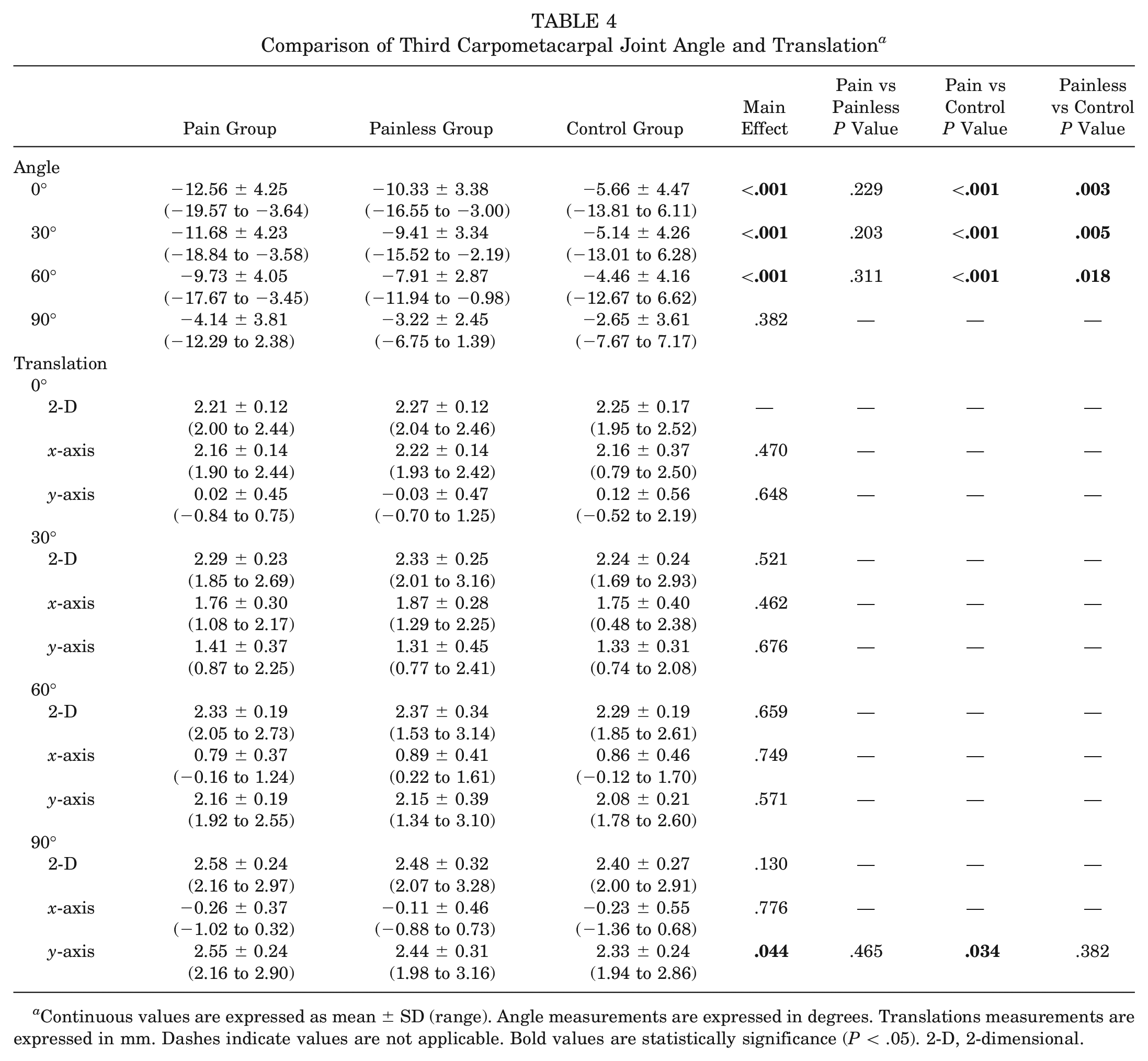
Continuous values are expressed as mean ± SD (range). Angle measurements are expressed in degrees. Translations measurements are expressed in mm. Dashes indicate values are not applicable Bold values are statistically significance (P < .05). 2-D, 2-dimensional.
Relative Reliability Assessments and Absolute Reliability Assessments
The ICC was moderate to excellent for all the findings. The 95% LOA was lower than all significantly different findings. Therefore, we interpreted the significantly different findings as being outside the error range. The ICC and LOA for the radiolunate, capitolunate, and third carpometacarpal joints are shown in Appendix Table A1 (available in the online version of this article).
Discussion
In this cross-sectional, case-control study of wrist kinematics in gymnasts with dorsal wrist pain, the most important finding was that gymnasts with dorsal wrist pain showed abnormal sagittal kinematics, including a decrease in the angle of the radiolunate joint, an increase in the angle of the capitolunate joint, and an increase in the distal translations of the capitolunate joint with a wrist extension of 90°. To our knowledge, this is the first study to report abnormal kinematics in patients with dorsal wrist pain.
Although the pathology of dorsal wrist pain is controversial, several studies have reported that the pain originates in the capitolunate joint, which is consistent with our results. Terng et al 51 reported that wrist hyperextension results in entrapment of excess subcapsular soft tissue in the midcarpal joint, resulting in dorsal wrist pain. Sgromolo et al 48 reported that excision of the posterior interosseous nerve, innervating the midcarpal joint and within the wrist capsule, 7 improves dorsal wrist pain. Furthermore, there is a case report in which wrist pain was intensified by wrist hyperextension, and dorsal lunocapitate impingement was found on imaging. 1
Previous reports on the relationship between wrist pain and an increased angle of the capitolunate joint are consistent with the results of our pain group. Beuckelaers and Hollevoet 5 reported that the angle of the capitolunate joint of the wrist with ganglion, one of the pathologies associated with dorsal wrist pain, was increased compared with that of the control group. In gymnasts with wrist pain evaluated with necrosis of the capitate, the articular surface of the capitate to the lunate was irregular and the capitolunate joint was enlarged. 37 Johnson and Carrera 22 reported that young patients with wrist extension trauma and subsequent chronic wrist pain showed instability of the capitolunate joint under a fluoroscopic stress test. Although these reports included individuals with evident abnormal imaging findings, they cannot be interpreted as having the same pathology, as none of the participants in the current study had abnormal imaging findings.
To the best of our knowledge, there have been no studies measuring capitolunate joint translation. Recently, case-control studies of distal radioulnar joint instability, 42 rotator cuff tears, 44 and acetabular dysplastic hips 2 showed greater symptomatic joint translation in the pain group than in the control group, indicating the importance of joint translation evaluation. Furthermore, a new pathology of hip joint disability due to structural and functional abnormalities, termed “microinstability,” 11 has been gaining interest, and our observation of the distal translation of the capitolunate joint in the pain group in this study could be similar to this pathology. In wrist hyperextension, the force of the capitate is concentrated on the dorsal prominence of the lunate. 30 Therefore, the distal translation of the capitate can be interpreted as abnormal sagittal kinematics resulting from the dorsal prominence of the lunate being the fulcrum and the distal capitate being the point of load. In other words, capitolunate joint distal translation is a disability of joint centralization that occurs at 90° of wrist extension, and we speculate that the pain point of dorsal wrist pain is the capitolunate joint.
The abnormal kinematics of the capitolunate joint at 90° of wrist extension can be interpreted to originate from lunate dyskinesia. Lunate dyskinesia is speculated to be transient or reversible, because all participants in the painless group were without dorsal wrist pain at the time of the MRI scan, although they had a history of dorsal wrist pain. The lunate is termed the “intercalated segment” 54 and functions as a bearing between the radius and the capitate. During wrist hyperextension, the contribution of the capitolunate joint is reported to be greater than that of the radiolunate joint, 43 with the lunate extending further and functioning as a bearing to support the capitate joint. In other words, when the lunate is unable to perform the bearing function required for wrist hyperextension, the decrease in the angle of the radiolunate joint and the increase in the angle of the capitolunate joint are 2 sides of the same coin.
The third carpometacarpal joint is reported to be involved in wrist extension in addition to the range of motion of the radiolunate and capitolunate joints, and a small amount of mobility has been observed in this joint. 43 However, there are also reports of its being tightly bound, which contradicts its mobility.38,40 Thus, there is inconclusive evidence regarding its presence or absence, and to the best of our knowledge, no reports have shown a relationship between the range of motion of the third carpometacarpal joint and wrist pain or age. In our study, all participants had mobility of the third carpometacarpal joint, with a high flexion range of motion at 0° to 60° of wrist extension in the pain and painless groups, which is a characteristic of gymnasts. However, at 90° of wrist extension, there was no significant difference in kinematics between the 3 groups. Therefore, we conclude that the third carpometacarpal joint is not affected by lunate dyskinesia and is not a point of dorsal wrist pain.
In our study, gymnasts exhibited an increased palmar tilt compared with healthy adults, regardless of dorsal wrist pain, which could be related to abnormal wrist sagittal kinematics in gymnasts. To our knowledge, reports on the relationship between increased palmar tilt and wrist pain in gymnasts are limited and, therefore, inconclusive. Guerra et al 19 found a trend of increased palmar tilt of the radius in gymnasts with wrist pain. However, our results did not find such a trend in the pain and painless groups. The reason for this is that the participants in the previous study were aged, on average, 13 years, which is different from the age of our participants (16-18 years), suggesting that in the earlier study the participants’ bone structure was still developing. In hyperextension during load bearing, the lunate is in extension and palmar translation, and stress is concentrated on the palmar side of the distal end of the radius, 10 causing premature closure of the growth plate. 18 The result is an increased palmar tilt, one of the findings of Madelung-like deformity.12,53 Although we cannot conclude that our participants had Madelung-like deformity, it has been reported that lunate extension is decreased in Madelung deformity compared with that in healthy individuals, 41 which is consistent with our pain group results. The reason lunate extension did not decrease, even though an increase in palmar tilt was also observed in the painless group, is assumed to be that only the pain group showed an abnormal lunate position at 0° of wrist extension compared with the control group. In other words, abnormal sagittal kinematics at 90° of wrist extension might be influenced by the lunate position in the neutral position. However, the pain group also showed good centralization of the radial and lunate at 90° of wrist extension, and we believe the radiolunate joint is not a pain point for dorsal wrist pain.
Overall, the new findings showed that the sagittal kinematics of the lunate in gymnasts with dorsal wrist pain were different from those of gymnasts without dorsal wrist pain. This finding is important as it shows that gymnast's lunate dyskinesia syndrome is a newly described syndrome. There are many different diseases that cause dorsal wrist pain. 20 In particular, it is difficult to accurately differentiate between dorsal impingement syndromes,13,45 dorsal wrist capsular impingement, 35 dorsal wrist impingement,4,21 wrist capsulitis, 50 and extensor retinaculum impingement, 52 as these conditions are assigned confusing terminologies and often include mixed pathologies in their reporting. However, the clear difference from gymnasts with dorsal wrist pain, as defined in this study, is the absence of tenderness, limitations of wrist movement, and imaging findings such as osteophytes and inflammation. Therefore, we conclude that dorsal wrist pain in gymnasts with normal MRI findings is different from or may have irreversible prepathology compared with these previously described pathologies.
Wrist pain in gymnasts is treatable with physical therapy that corrects improper biomechanics 4 and treats key musculoskeletal impairments and movement deficiencies, 8 which the authors support. Our results highlight that the assessment and functional improvement by physical therapy in gymnasts with dorsal wrist pain must be considered in cases of a decrease in the angle of the radiolunate joint, an increase in the angle of the capitolunate joint, and an increase in the distal translations of the capitolunate joint with wrist extension of 90°. Furthermore, understanding that this new syndrome is a reversible pathology could assist gymnasts in self-management of it.
The present study has several limitations. First, this was a retrospective case-control study that did not explain the causality of dorsal wrist pain. Therefore, future interventional studies are warranted. Second, because of the small number of participants studied, data may have been collected from a specific population or period. The training intensity of the participants was equivalent to previous studies and was appropriate.19,29,31,46 Third, we could not include gymnasts without a history of dorsal wrist pain in the painless group of this study. Thus, this group was not a true painless group, as we could not identify athletes with no previous incidents, particularly among elite gymnasts with extensive competitive experience. Therefore, the painless group may have exhibited transient abnormal wrist sagittal kinematics. Fourth, the control group had a mean higher age, height, and weight than the other groups, which may have affected the results. However, the carpals of the pain and painless groups were sufficiently ossified, and there was no evidence of a correlation between palmar tilt and age 33 ; therefore, the results were less affected by age differences. Furthermore, to the best of our knowledge, height and weight have not been reported as confounding factors for intercarpal joint mobility, so these also had fewer effects. Fifth, in the present analysis, the features of the 2-dimensional evaluation were observed in only the sagittal plane. Occult ganglion cysts may be overlooked by only imaging in the sagittal plane. Because we found no dorsal wrist tenderness in any participant, we do not believe that the lesion was present. Although no 3-dimensional evaluation was performed, radial and ulnar deviation, pronation, and supination were performed under the same conditions in all participants, and all conditions that affected the results of the 2-dimensional evaluation were eliminated. Last, because no load bearing was applied during MRI at 90° of wrist extension, it was impossible to capture the actual phenomenon at the time of occurrence of dorsal wrist pain. Research has been conducted to analyze the impact strength of gymnastic techniques,17,34 and it is necessary to study dynamic wrist kinematics synchronized with actual gymnastic movements, not static movements, as in our study.
Conclusion
Gymnasts with dorsal wrist pain showed abnormal sagittal kinematics with reversible hypermobility, as hypothesized. The findings of this study suggest the existence of a new previously unrecognized syndrome, gymnast's lunate dyskinesia, within a group of diseases currently termed “gymnast’s wrist.” We defined this new syndrome as dorsal wrist pain in gymnasts at hyperextension while load bearing without abnormal imaging findings, restriction of range of motion, and inflammatory symptoms such as local swelling, heat sensation, or tenderness. Understanding these kinematic abnormalities may help therapists treat gymnasts. These abnormalities in kinematics may be transient and reversible and need to be validated in future physical therapy intervention studies.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465231204361 – Supplemental material for Abnormal Wrist Sagittal Kinematics in Gymnasts With Dorsal Wrist Pain: A New Syndrome
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231204361 for Abnormal Wrist Sagittal Kinematics in Gymnasts With Dorsal Wrist Pain: A New Syndrome by Takahiro Sekiguchi, Shinobu Saito, Takahiro Ogura, Akihiro Tsuchiya and Hideaki Shiratsuchi in The American Journal of Sports Medicine
Footnotes
Submitted January 20, 2023; accepted August 23, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.