
Abstract
Background:
Historically, symptomatic hip labral lesions were treated with arthroscopic debridement. Hip labral repair has become the standard treatment for labral pathology; however, to date, there are limited long-term studies regarding the outcomes of isolated labral debridement.
Purpose:
To (1) evaluate the long-term patient-reported outcomes of isolated labral debridement, (2) report reoperation and arthroplasty rates, and (3) identify risk factors contributing to reoperation or poor clinical outcomes.
Study Design:
Case series; Level of evidence, 4
Methods:
A retrospective review of a prospectively generated cohort of 59 hips in 57 patients from 1996 to 2010 who underwent hip arthroscopy with labral debridement was performed. Only patients with Tönnis grade <3 were included. Additionally, given the time period analyzed, resection of cam morphology was not performed, and the interportal capsulotomy was not repaired. The pre- and postoperative modified Harris Hip Score; Hip Outcome Score (HOS)-Activities of Daily Living and -Sports scores; and reoperation, conversion to total hip arthroplasty, and risk factors were analyzed.
Results:
In total, 48 hips in 47 patients (14 men, 33 women; mean age, 48.0 ± 12.9 years) met inclusion criteria and were followed for a mean of 17 ± 3 years (range, 13-27 years). The mean preoperative Tönnis grade was 1.3 ± 0.6 (range, 0-2), the mean chondral acetabular International Cartilage Regeneration & Joint Preservation Society (ICRS) grade was 1.7 ± 1.6 (range, 0-4), the mean chondral femoral ICRS grade was 0.9 ± 1.4, and the mean acetabular labral articular cartilage grade was 2.5 ± 1.2 (range, 0-4). At the final follow-up, mean the modified Harris Hip Score, HOS-Activities of Daily Living score, and HOS-Sports score were 82.2 ± 16.6, 81.9 ± 20.5, and 82.2 ± 20.5, respectively. Nineteen hips underwent subsequent reoperation at a mean of 5.5 ± 6.2 years (range, 0.5-21.2 years) postoperatively, including 16 hips (33% overall) being converted to total hip arthroplasty. Higher acetabular ICRS chondral grades at the time of surgery were observed in patients who went on to subsequent surgery compared with those who did not (2.3 ± 1.6 vs 1.1 ± 1.5; P = .02). In reoperation-free hips, Tönnis grade demonstrated a trend of increasing over time (1.4 preoperatively vs 1.7 at radiographic follow-up; P = .08). At the final follow-up, 19 hips (40%) had undergone reoperation, and 5 additional hips (10%) were rated as “abnormal” or “severely abnormal” in function, resulting in an overall clinical failure rate of 50%.
Conclusion:
Isolated labral debridement was found to result in high rates of failure and reoperation, with a third of patients being converted to arthroplasty and half of patients meeting criteria for reoperation or clinical failure. Of note, for patients remaining reoperation-free, satisfactory outcome scores were observed.
The hip labrum is a fibrocartilaginous lining of the acetabulum that confers additional coverage and stability of the femoral head and its interface with the acetabulum.2,6 The labrum can be traumatically or degeneratively damaged, with dysfunction of the labrum commonly caused by femoroacetabular impingement (FAI). 20 FAI is a structural hip disorder wherein an abnormally shaped femoral head/neck (cam impingement) or acetabular overcoverage (pincer impingement), or a combination of the 2, leads to abnormal contact and subsequent chondrolabral injury and early osteoarthritis via focal loading and subsequent delamination.7,16
Historically, labral lesions were treated with labral debridement, yielding modest results. 14 More recently, there has been an evolution of hip arthroscopic techniques and instrumentation, with a simultaneous increasing trend toward labral repair. 19 Such a shift in practice is supported by a prospective series published by Krych et al 12 that demonstrated superior improvements in functional outcomes after repair rather than debridement at a mean follow-up of 32 months. However, less is known regarding the long-term outcomes of isolated labral debridement. Previously, we reported on the short- to midterm follow-up of isolated labral debridement at a mean 5-year follow-up. Twenty percent of patients underwent subsequent hip surgery, and an additional 25% rated their hip function as “abnormal” or “severely abnormal.” 11 To date, there are few studies regarding the outcomes of labral debridement beyond 10 years of follow-up.13,23 Furthermore, even fewer studies have investigated the outcomes of isolated debridement without resection of cam or pincer morphology at long-term follow-up.3,18
Therefore, the purpose of this study was to (1) evaluate the long-term patient-reported outcomes of isolated labral debridement, (2) report reoperation and arthroplasty rates, and (3) identify risk factors contributing to reoperation or poor clinical outcomes. We hypothesized that a high rate of conversion to total hip arthroplasty (THA) and modest clinical outcomes would be observed.
Methods
After institutional review board (IRB No. 08-002259) approval, a retrospective review of a prospectively generated cohort of consecutive hips from 1996 to 2010 was performed. Inclusion criteria were (1) labral tear confirmed on magnetic resonance imaging scans, (2) patients >18 years of age who underwent isolated arthroscopic labral debridement without cam or pincer resection, (3) Tönnis grade <3, and (4) a lateral center-edge angle (LCEA) >25°. 5 Electronic medical records were reviewed, and patients were contacted by telephone or email to complete patient-reported outcome surveys.
Surgical Technique and Rehabilitation
All hip arthroscopies were performed by experienced hip arthroscopic surgeons (M.J.S., B.A.L.). Anterolateral and midanterior portals were used. Diagnostic arthroscopy of the labrum and cartilage was conducted in all patients. Subsequently, a capsulotomy was performed between the 2 portals to increase access to the hip joint. Labral debridement was performed, removing any unstable portions of labrum with the intention of preserving the remaining stable labral tissue. Given the time period analyzed, resection of cam morphology was not performed. The interportal capsulotomy was not repaired; that is, no patients underwent capsular closure. Postoperatively, patients used crutches for 2 weeks with foot-flat partial (25%) weightbearing restrictions. Patients were restricted from passive hip external rotation for 4 weeks. An institutional hip rehabilitation protocol was initiated postoperatively between days 7 and 10.
Reoperation and Failure
Reoperation was defined as subsequent hip surgery including revision arthroscopy, THA, or other ipsilateral hip surgeries. Failure was defined as reoperations or patient-reported hip function of “abnormal” or “severely abnormal.”
Data Collection
Patient data including age, sex, and time of surgery, as well as preoperative radiographic data including alpha angle, LCEA, and Tönnis grade, were collected. For patients not converted to THA, Visual Analog Scale (VAS), modified Harris Hip Score and Hip Outcome Score (HOS)-Activities of Daily Living and -Sports scores were collected at a mean follow-up of 5 years and at the final follow-up. Grading of acetabular and femoral head cartilage was conducted according to the International Cartilage Regeneration & Joint Preservation Society (ICRS) guidelines.1,21 The presence or absence of cam or pincer morphology, as well as the acetabular labral articular cartilage (ALAD)8,17 grade, was retrospectively determined. Measurements and grading were done by a board-certified orthopaedic surgeon (M.H.).
Statistical Analysis
Statistical analysis was performed using BlueSky Version 7.4.0 software (BlueSky Statistics Inc). Descriptive statistics are reported as number (percentage), and parametric variables are reported as mean ± standard deviation, with nonparametric variables reported as medians with ranges. The Pearson chi-square test was used for categorical variables. Kaplan-Meier analysis was used to evaluate the time-dependent rate of survival without reoperation or survival without conversion to THA. Paired t tests were used to compare baseline and final patient-reported outcomes. All statistical tests were 2-sided, with P < .05 considered statistically significant.
Results
Patient Characteristics
Of the original 59 hips in 57 patients, 11 hips (10 patients) were lost to follow-up, resulting in an 81% long-term follow-up. Therefore, 48 hips in 47 patients (14 men, 33 women; mean age, 48.0 ± 12.9 years; range, 18-73 years) met inclusion criteria and were followed for a mean of 17 ± 3 years (range, 13-27 years) postoperatively. The mean preoperative alpha angle was 58.8°± 13.0° (range, 45.0°-90.3°), with 56% of the cohort exceeding 50°, and the mean LCEA was 35.2°± 6.6° (range, 27.6°-40.0°). Of the cohort, 11% had no FAI morphology, 43% had cam morphology, 8% had pincer morphology, and 38% had mixed cam and pincer morphology. The mean preoperative Tönnis grade was 1.3 ± 0.6 (range, 0-2), the mean chondral acetabular ICRS grade was 1.7 ± 1.6 (range, 0-4), the mean chondral femoral ICRS grade was 0.9 ± 1.4, and the mean ALAD grade was 2.5 ± 1.2 (range, 0-4).
Clinical Outcomes
In patients who were not converted to THA, the mean modified Harris Hip Score, HOS-Activities of Daily Living score, and HOS-Sports score at the final follow-up were 82.2 ± 16.6, 81.9 ± 20.5, and 82.2 ± 20.5, respectively. Pairwise comparison of previously obtained midterm outcome scores at a mean of 5.5 ± 3.3 years of follow-up and long-term outcome scores at a mean of 16.6 ± 3.3 years of follow-up demonstrated no significantly different subjective outcomes over time (Table 1). The final mean visual analog scale pain scores at rest and with use were 1.6 ± 2.2 and 2.5 ± 2.7, respectively.
Pairwise Comparison of 5- and 17-Year Postoperative Outcomes a
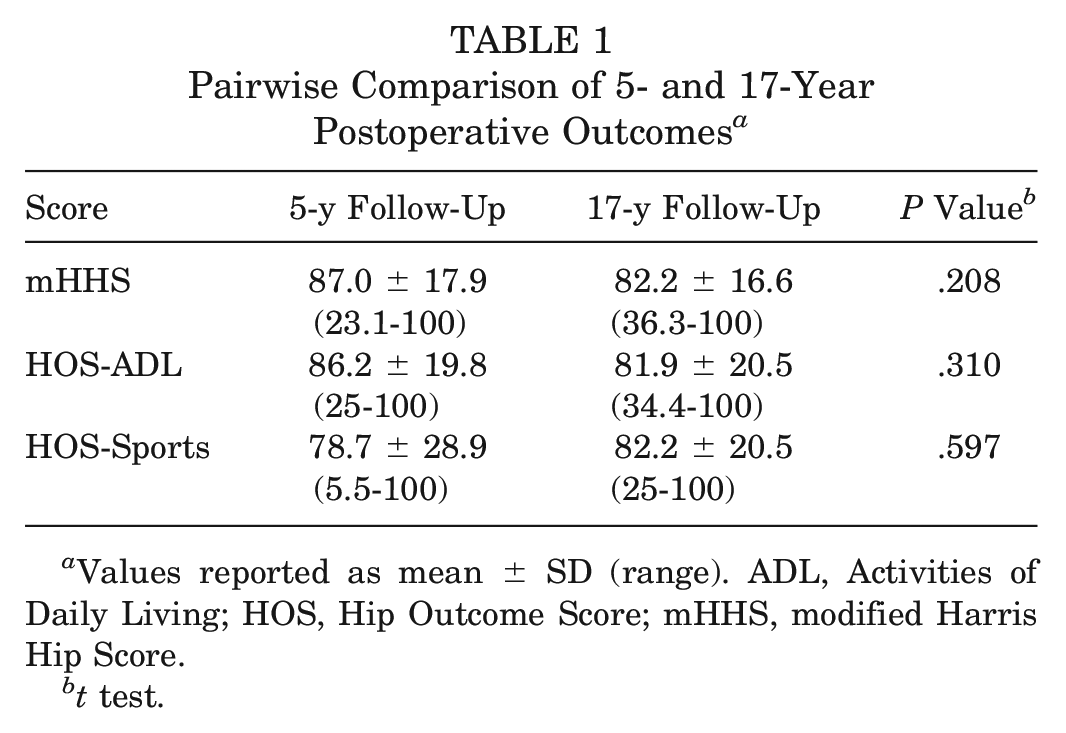
Values reported as mean ± SD (range). ADL, Activities of Daily Living; HOS, Hip Outcome Score; mHHS, modified Harris Hip Score.
t test.
At the final follow-up, the mean patient satisfaction on a scale from 1 to 10, with 1 being “not at all satisfied” and 10 being “most satisfied,” was 8.9 ± 2.1 (median, 10; range, 1-10), with 21 (78%) of those not converted to THA reporting a score 9 or 10. In subjective hip rating, 9 patients (36%) rated their hip as “normal,” 11 (44%) as “nearly normal,” 4 (16%) as “abnormal,” and 1 (4%) as “severely abnormal,” with 2 nonrespondents.
Reoperation and Conversion to Arthroplasty
At the final follow-up, 19 hips (40%) had subsequent surgical intervention at a mean of 5.5 ± 6.2 years (range, 0.5-21.2 years; interquartile range, 1.0-7.0 years). First-time reoperations consisted of 2 open revisions with complete labral excision, 3 arthroscopic revisions (1 cam resection alone, 1 cam resection with labral repair, and 1 cam and pincer resection with labral repair), and 14 THAs. Two arthroscopic revisions were converted to THA at 9 and 11 years after the initial surgery. Therefore, at the final follow-up, 16 hips (33%) had been converted to THA at a mean of 9.0 ± 7.7 years. In the 10 reoperation-free hips with retrievable pre- and postoperative radiographs, pairwise comparison of Tönnis grade demonstrated a trend toward increasing Tönnis grade over time: 1.4 preoperatively and 1.7 (P = .08) at a mean follow-up of 7.1 ± 3.6 years. Additionally, 2 patients (4%) were deceased at the final follow-up, both without having undergone subsequent reoperation. Rates of conversion to THA at 2, 5, 10, 15, and 20 years were 6.3%, 14.6%, 18.8%, 27.1%, and 29.2%, respectively (Figure 1).
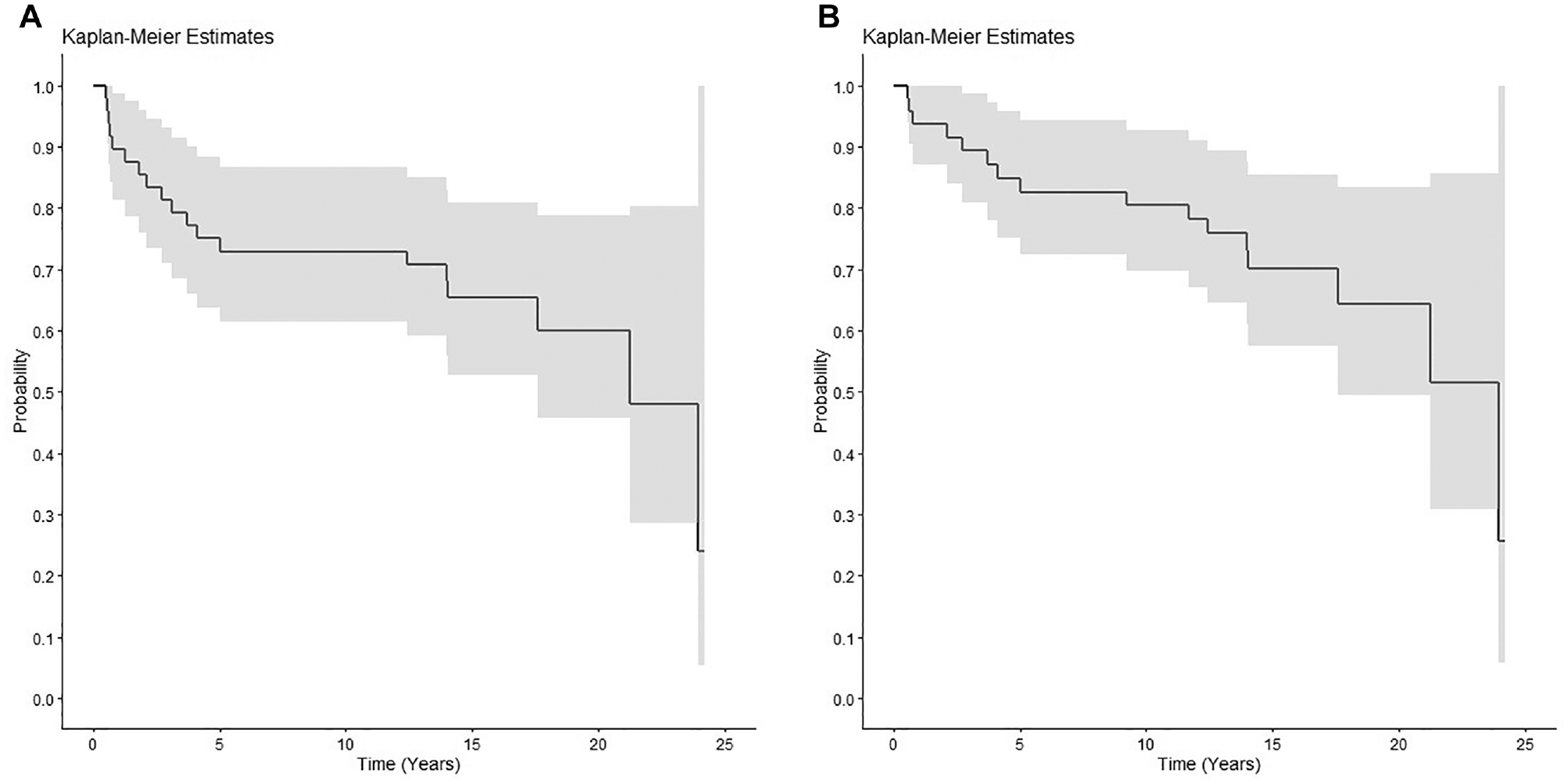
Treatment failure and risk factor analysis with (A) Kaplan-Meier estimator for all-cause failure and (B) Kaplan-Meier estimator for conversion to total hip arthroplasty.
At the final follow-up, 19 hips (40%) had undergone reoperation, and the subjective function of an additional 5 hips (10%) was rated as “abnormal” or “severely abnormal,” resulting in an overall failure rate of 50% at a mean of 17 years after isolated labral debridement. Univariate failure analysis demonstrated that patients who went on to subsequent surgery had higher mean acetabular ICRS chondral and ALAD grades at the time of surgery as compared with patients who did not go on to subsequent surgery (Table 2). No significant associations were observed between age, sex, Tönnis grade, or presence of subchondral cyst/edema on preoperative magnetic resonance imaging scans and at reoperation.
Comparison of Patients Who Did and Did Not Undergo Reoperation a
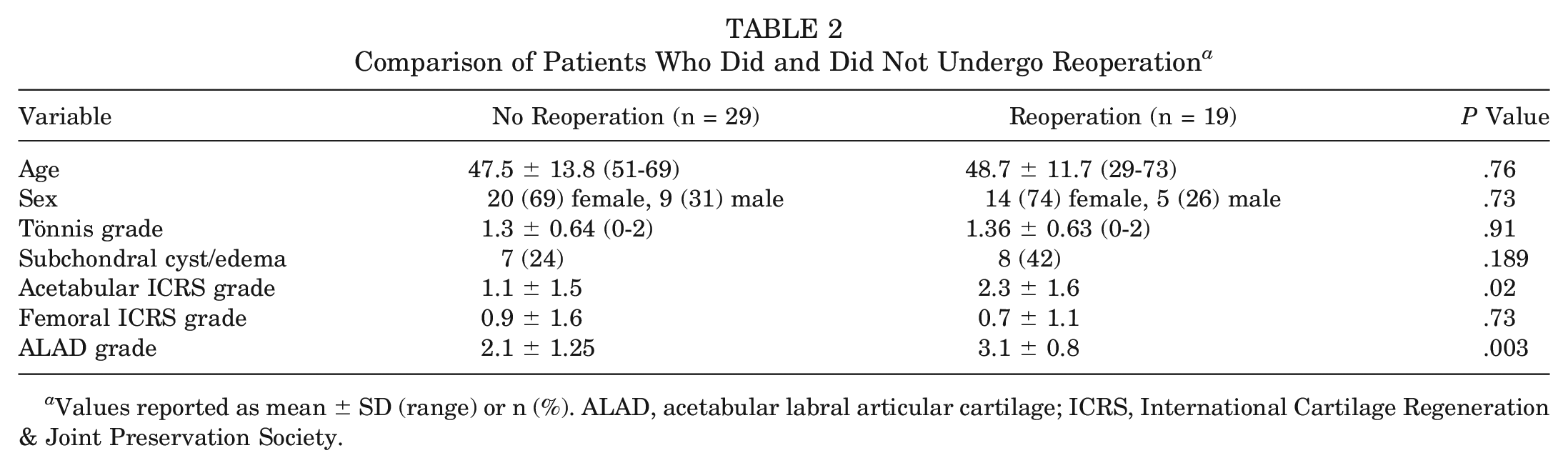
Values reported as mean ± SD (range) or n (%). ALAD, acetabular labral articular cartilage; ICRS, International Cartilage Regeneration & Joint Preservation Society.
Discussion
The main finding of this study was that at long-term follow-up, 1 in 3 patients had been converted to THA at a mean of just 9 years after isolated arthroscopic labral debridement. Furthermore, treatment in half of all patients treated with isolated arthroscopic labral debridement failed, as defined by reoperation or a self-reported subjectively abnormal hip rating. Of note, patients not undergoing subsequent surgery demonstrated modest but durable improvements in patient-reported outcomes at a mean of 17 years after the index surgery. These findings are clinically relevant as they highlight the overall modest outcomes and high rates of conversion to THA after isolated labral debridement.
In our previous series with a 5-year mean follow-up, only 7 patients (12%) had undergone THA. 11 Now, with 17-year mean follow-up, an additional 9 patients had been converted to arthroplasty, representing 33% of the patients eligible for inclusion. We found that preexisting high-grade acetabular chondromalacia and labral disruption significantly predicted conversion to THA; however, femoral head chondromalacia did not. This is likely, in part, due to the lower prevalence of intraoperatively visualized chondral damage of the femoral head. Our findings are similar to those of Byrd and Jones, 3 who observed a 23% THA conversion rate at 10 years in patients undergoing isolated labral debridement without bony resection, which is comparable to our 10-year rate of 19%. Similarly, the authors also demonstrated poorer outcomes and higher rates of conversion to THA in patients with preexisting arthritis.
A notable contrast is the growing body of literature on contemporary hip arthroscopy with labral repair, which has demonstrated overall improved patient-reported outcomes and lower failure rates compared with our historic cohort of labral debridement. At short-term follow-up, Krych et al 12 demonstrated superior clinical outcomes for patients undergoing labral repair as compared with labral debridement in a randomized controlled trial. Similarly, a recent systematic review by Hurley et al 10 reported superior outcomes in labral repair compared with debridement in nearly 700 patients across 8 studies with mean follow-ups of 32 to 120 months, although no difference in conversion to THA was observed. More recent studies focusing on the midterm outcomes of contemporary hip arthroscopy with labral repair and resection of cam and pincer morphology, such as those by Hevesi et al 9 and Lee et al, 15 have reported much lower rates of conversion to THA, ranging from 2.4% to 3.0% at a mean of 6 to 8 years of follow-up. The findings of these contemporary studies compare favorably to the long-term labral debridement data presented in the current study.
It is worth noting that the subjective patient-reported outcomes of patients who did not undergo reoperation or THA in our series were acceptable and similar at the final follow-up as compared with a previously reported midterm follow-up. Additionally, the average patient reported nearly a 9 of 10 for surgery satisfaction. This suggests that there is a subset of patients who, after isolated labral debridement, are not converted to THA and have relatively unchanged subjective function and satisfaction between mid- and long-term follow-up. These findings are supported by Chen et al, 4 who demonstrated at a minimum 5-year follow-up a matched cohort of “selective debridement with labral preservation” that produced comparable outcomes to labral repair. However, in our long-term series, even among this subcohort of patients who responded best to isolated debridement and did not undergo reoperation, the trend was for the Tönnis grade to increase over time, suggesting continued radiographic progression of hip degeneration.
The historic setting of this study is also worth discussing. Labral debridement was not chosen over repair; rather, debridement was chosen given that techniques, instrumentation, and the rationale for repair had yet to be developed. Similarly, cam decompression was not performed given that FAI was not yet well understood; Ganz et al 7 published their landmark paper “Femoroacetabular impingement: a cause for osteoarthritis of the hip” in 2003. Only 6 years later, near the end of the era being investigated (2009), is when bony resection and labral repair began to be implemented regularly at our institution. Understandably, the data presented in the current study are valuable and novel in the literature given the long-term longitudinal data regarding the outcomes of isolated labral debridement, which are unlikely to be otherwise replicated. Today, repair with labral preservation and addressing underlying components of FAI is desirable as we aim to restore and preserve the hip joint with modern biomechanical understanding and techniques. Given the rapid advancement of the field, the long-term outcomes of optimal hip arthroscopy and labral management continue to be investigated. 10 Therefore, these findings, akin to now-published long-term outcomes of the originally published Bernese periacetabular osteotomy cohort, 22 represent an important benchmark moving forward.
This study is not without limitations. First, although the follow-up was robust, the techniques for hip arthroscopy are changing rapidly; thus, a comparison across studies over the simultaneous global evolution of hip arthroscopy, techniques, and instrumentation is inherently challenging. Similarly, we cannot definitively attribute differential outcomes and rates of THA to labral debridement versus repair alone given the concomitant procedures that define modern hip arthroscopy (ie, cam or pincer resection and the transition to routine capsular closure). In parallel, indications for arthroscopy have changed over time, with many now considering Tönnis grade 2 changes a contraindication or relative contraindication to arthroscopic intervention. Additionally, as the mean age of this cohort was 48 years at the time of surgery and 65 years at the final follow-up, conversion to THA may reflect natural progression of disease rather than a result solely attributable to labral debridement rather than repair. Finally, no comparison cohort with more modern techniques, labral repair, and capsular closure was used given the lack of equivalent long-term follow-up for contemporary techniques.
Conclusion
Isolated labral debridement was found to result in high rates of failure and reoperation, with a third of patients being converted to arthroplasty and half meeting criteria for reoperation or clinical failure. Of note, for patients remaining reoperation-free, satisfactory outcome scores were observed.
Footnotes
Submitted March 1, 2023; accepted July 20, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: The authors acknowledge the support from the Foderaro-Quattrone Musculoskeletal-Orthopaedic Surgery Research Innovation Fund. This study was partially funded by the following: National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (T32AR56950). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. K.R.O. has received consulting fees from Arthrex, Smith + Nephew, and Endo Pharmaceuticals; support for education from Gemini Medical, Smith + Nephew, Pinnacle, and Medwest Associates; compensation for services other than consulting from Smith + Nephew; grants from Arthrex; and hospitality payments from Stryker, Wright Medical Technology, Medical Device Business Services, and Zimmer Biomet. M.J.S. has received royalties, consulting fees, and compensation for services other than consulting from Arthrex and research support from Stryker. B.A.L. has received royalties and consulting fees from Arthrex; stock or stock options in COVR Medical; consulting fees from Smith + Nephew; and education support from Linvatec. A.J.K. has received consulting fees from Arthrex, Joint Restoration Foundation, Responsive Arthroscopy, and Vericel; honoraria from Joint Restoration Foundation and Vericel; royalties from Arthrex and Responsive Arthroscopy; a grant from DJO; research support from Aesculap/B.Braun, Arthrex, Arthritis Foundation, Ceterix, and Histogenics; and hospitality payments from Gemini Mountain Medical and Smith + Nephew and serves on the medical board of trustees for the Musculoskeletal Transplant Foundation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.