
Abstract
Background:
Recently, interest in anterior cruciate ligament (ACL) preservation and repair after proximal ACL tears has been resurrected. Although good clinical outcomes have been reported in the literature with adequate patient selection, to date detailed scientific evidence for the functional benefit of primary ACL repair with ligament augmentation is scarce.
Purpose:
To compare patient-reported, clinical, and functional outcomes in patients 2 years after ACL repair and InternalBrace augmentation (ACL-IB) with age- and sex-matched patients 2 years after ACL reconstruction (ACL-R) and with matched healthy controls.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
In total, 29 patients 2 years after ACL-IB, 27 sex- and age- matched patients 2 years after ACL-R (hamstring autografts), and 29 matched healthy controls were included. Patient-reported outcomes were assessed using the International Knee Documentation Committee score, Knee injury and Osteoarthritis Outcome Score, EQ-5D-5L, Tegner Activity Scale, and Anterior Cruciate Ligament Return to Sports after Injury scale. Surgery time was recorded. For clinical outcomes, range of motion and thigh and shank circumference were measured, and passive anterior translation was determined using the Rolimeter. Isokinetic muscle strength was measured using a Biodex dynamometer. The limb symmetry index (operated/contralateral or nondominant/dominant × 100), side-to-side differences (operated – contralateral, nondominant – dominant), and hamstring-quadriceps ratios were calculated for functional parameters. Failure and reoperation rates were not compared.
Results:
Two years after surgery, patients treated with ACL-IB showed good to excellent patient-reported outcomes comparable with those of patients after ACL-R. Surgery time, including concomitant surgeries, was significantly shorter in the ACL-IB group (mean, 81 minutes) compared with the ACL-R group (mean, 97 minutes) (P = .024). Isokinetic muscle strength was comparable between patient groups without significant differences in extensor and flexor strength or in hamstring-quadriceps ratios.
Conclusion:
These results suggest that ACL-IB achieves comparable patient-reported, clinical, and functional outcomes with ACL-R at 2 years postoperatively and, after careful patient selection, should be considered as a valuable early treatment alternative for proximal ACL tears.
Registration:
NCT04429165 (ClinicalTrials.gov identifier).
Anterior cruciate ligament (ACL) tears are among the most common injuries of the knee, leading to pain, effusion, instability, and significant limitations in activities of daily living and sports. 33 Furthermore, an increased risk for early onset of osteoarthritis has been reported in chronic ACL-deficient knees. 30 Early attempts to repair and preserve the ruptured ACL have shown highly dissatisfying results with persisting tibiofemoral instability, reinjury rates of 50%, and significant impairment in range of motion (ROM).16,46 Consequently, primary repair surgery was abandoned in the 1980s and replaced by arthroscopic ACL reconstruction (ACL-R) using autologous grafts, which is still considered the surgical gold standard treatment of ACL ruptures. 10
However, advocates of primary repair surgery emphasize its potential advantages, including a less invasive (smaller drilling tunnel) and more soft tissue-sparing approach (no morbidity at the harvest site because no graft is harvested), faster return to full ROM, less daily awareness of the operated knee, fewer complications, and, if necessary, less complicated revision surgery.53,57,59 Moreover, preservation of the native ACL likely preserves nerve endings, blood supply, and proprioception, which contributes to normal joint function, including stiffness and stability. 40 Ultimately, the abovementioned factors combined could result in less postoperative tissue swelling and effusion, faster return to full ROM, faster postoperative rehabilitation, better preservation/restoration of muscle strength, and earlier return to work and sports compared with ACL-R.3,17,36,52
The remarkable evolution of arthroscopic techniques and devices along with recently published promising clinical results have resurrected interest in primary repair of proximal ACL tears.17,25,28,61 Several approaches have been reported with or without reinforcement of the native ACL,31,53,62 and improved outcomes, including a significantly lower failure rate, have been reported. 28
A frequently used technique in ACL repair and augmentation for proximal ACL ruptures is the InternalBrace (ACL-IB; Arthrex Inc). To date, several case-control studies and systematic reviews have shown favorable clinical outcomes after ACL repair surgery. # However, although various studies have reported biomechanical and functional parameters in patients after ACL-R12,19,37 and results of gait analysis and functional hop testing after dynamic intraligamentary stabilization (Ligamys; Mathys),8,43 such evaluations for ACL-IB are scarce. Because still increased failure rates after primary repair compared with ACL-R have been reported 61 and scientific evidence for functional outcome is limited, many surgeons are hesitant to consider ACL-IB as an alternative treatment option for proximal ACL tears. Therefore, the aim of this study was to compare detailed patient-reported, clinical, and functional outcomes in patients 2 years after ACL-IB with age- and sex-matched patients 2 years after gold standard ACL-R (using autologous hamstring tendons) and matched healthy, noninjured controls.
Methods
Patients and Controls
This nonrandomized single-center comparative study with prospective data collection was approved by the regional ethics board (Ethics Committee Northwest Switzerland EKNZ 2019-00491 and EKNZ 2020-00551), and the study is registered at clinicaltrials.gov (NCT04429165). The detailed study protocol including all performed analyses has been previously published. 34
After careful evaluation of inclusion and exclusion criteria (Table 1), the following groups were included in our study:
ACL-IB: consecutive patients 2 years after primary ACL repair and ligament augmentation operated at our institution and checked for inclusion and exclusion criteria (Table 1 and Figure 1) (n = 29).
ACL-R: patients 2 years after ACL-R with autologous hamstring grafts were selected on the basis of sex and age from all patients treated in our clinic to obtain a sex- and age-matched comparison group (n = 27).
Controls: sex- and age-matched participants with healthy knees (n = 29).
Inclusion and Exclusion Criteria for Patients After ACL-IB and ACL-R and Healthy Controls a
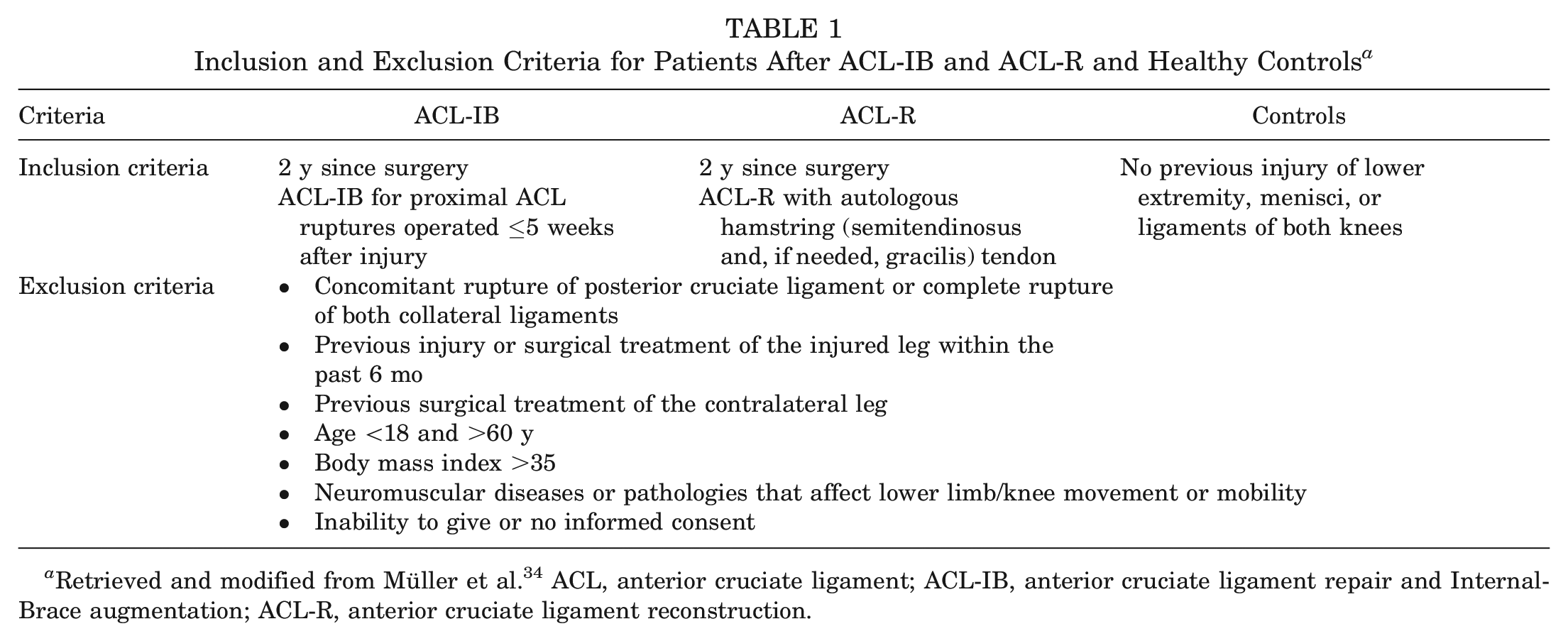
Retrieved and modified from Müller et al. 34 ACL, anterior cruciate ligament; ACL-IB, anterior cruciate ligament repair and InternalBrace augmentation; ACL-R, anterior cruciate ligament reconstruction.
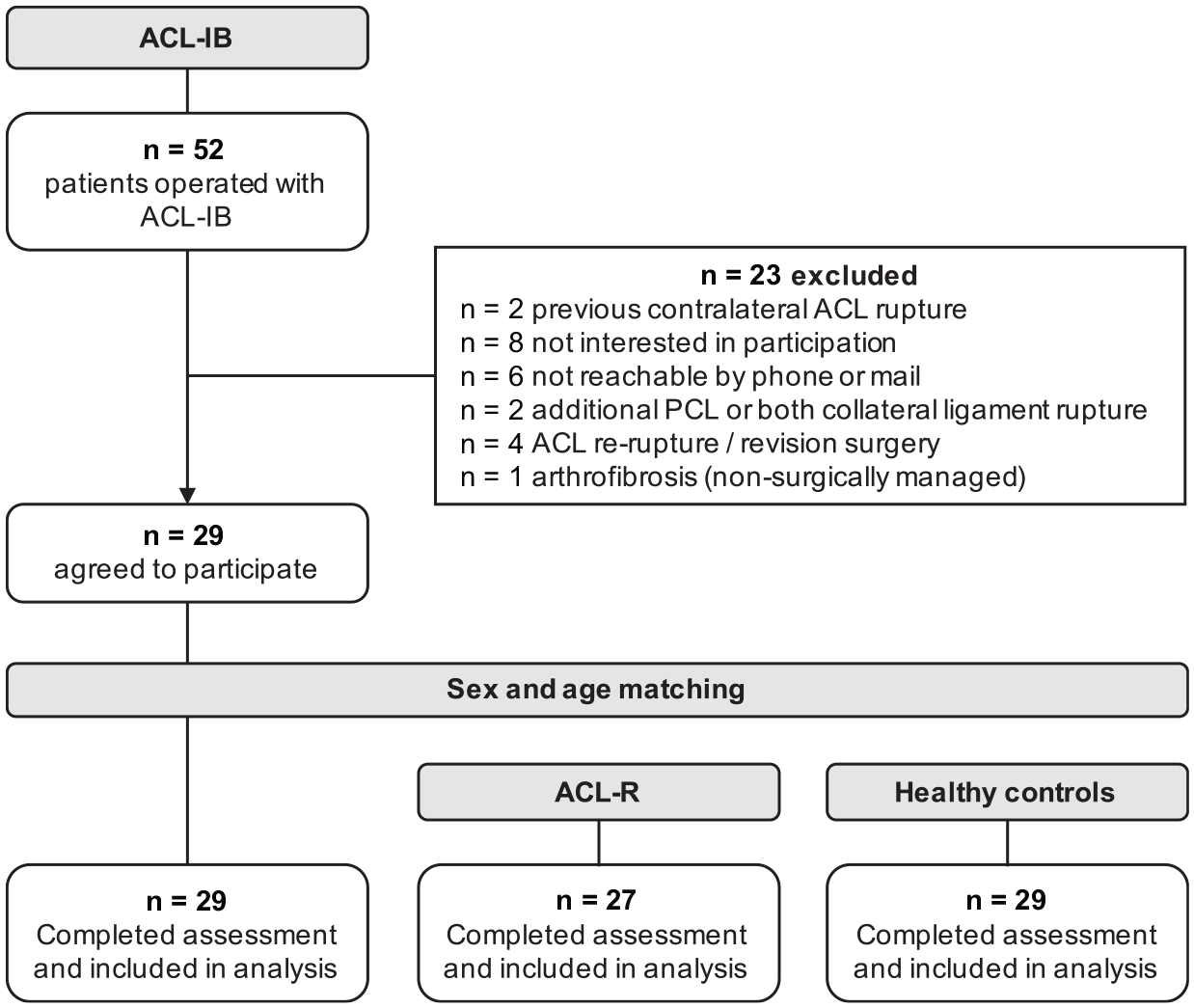
Flowchart of patient selection and matching procedure. ACL, anterior cruciate ligament; ACL-IB, anterior cruciate ligament repair and InternalBrace augmentation; ACL-R, anterior cruciate ligament reconstruction; PCL, posterior cruciate ligament.
All patients had full-thickness ACL tears verified via preoperative magnetic resonance imaging and arthroscopy. Surgeries in patients of both groups were performed between May 2016 and April 2020, and patients were enrolled in our study 2 years after surgery if they met our inclusion criteria. Healthy controls were recruited via flyers in the local area and announcements on online platforms. Figure 1 depicts the detailed patient selection and matching procedure.
Surgical Procedure and Rehabilitation Protocol
The same board-certified senior orthopaedic surgeons (S.M., G.P, C.E.) performed the ACL-IB and ACL-R surgeries.
ACL Repair and InternalBrace Augmentation
ACL-IB was performed within a maximum of 5 weeks after a patient sustained a proximal ACL tear (Sherman types 1 and 2). 46 The procedure was performed as previously described in detail. 34 Depending on the tissue quality, the torn ACL was stitched in the proximal portion with 1 or 2 sutures (eg, FiberLink; Arthrex) to obtain secure fixation. Through use of conventional tibial and femoral ACL targeting devices, surgeons placed 4.5-mm drill holes in the tibial and femoral footprints. The suturing fibers were then passed through the femoral tunnel along with an augmenting FiberTape (ie, the InternalBrace) and a flip button device for femoral fixation (eg, ACL Tight Rope; Arthrex). After reattachment of the ACL to the femoral footprint, the 2 ACL repair sutures were firmly tied down to the button. Distally, the augmenting suture tape was fixed to the tibia with an interference screw (eg, SwiveLock; Arthrex) or button (eg, EndoTack; Karl Storz SE and Co KG) with the knee in a position near extension (0°-20°).
ACL Reconstruction
Autologous hamstring tendons (semitendinosus and/or gracilis) were harvested for ACL-R. Drill holes with diameters corresponding to the size of the graft were placed in the femoral and tibial footprints. Femoral fixation was realized by using a flip button (eg, Rigidloop; DePuy Synthes, Mitek Sports Medicine), and tibial fixation was performed using an interference screw (eg, MILAGRO; DePuy Synthes, Mitek Sports Medicine).
Postoperative Rehabilitation
For both patient groups (ACL-IB and ACL-R), the same rehabilitation protocol was prescribed. Partial weightbearing (touch-toe, 10-15 kg) was advised, and knee flexion was limited to 90° using a knee brace for 6 weeks. Full weightbearing was allowed and active strength and proprioceptive training started from week 7. After 12 weeks, guided 3-month strength training (medical training therapy) was prescribed. Thereafter, rehabilitation was individually adapted according to patient need. The rehabilitation process after 12 weeks was not strictly monitored.
Study Procedures
Two years after index surgery, written informed consent was obtained before patients and controls were asked to complete several questionnaires, undergo a standardized clinical examination, and perform instrumented functional muscle strength tests.
Patient-Reported Outcome Measures
Health and knee-related outcomes, such as symptoms, pain, function, and everyday activity levels, were assessed using the following: International Knee Documentation Committee (IKDC) score, 26 Knee injury and Osteoarthritis Outcome Score (KOOS), 41 Anterior Cruciate Ligament Return to Sports after Injury (ACL-RSI) scale, 35 EQ-5D-5L, 20 and the Tegner Activity Scale (TAS). 51
Clinical Examination
Maximum circumference of the thigh and shank was measured in both legs. Knee stability in anterior-posterior translation (drawer test; knee flexion, 20-30°) was assessed bilaterally using the Rolimeter 39 (Aircast Europe GmbH) with manual maximum anterior force to the tibia, 50 and the ROM of both knees was measured using a goniometer. Outcomes are presented as the side-to-side difference (SSD; operated – contralateral, nondominant – dominant).
Isokinetic Muscle Strength Testing
All participants first completed a 5-minute warm-up on a treadmill at a self-selected walking speed. After randomization to determine the leg to be tested first in all assessments, we measured isokinetic muscle strength bilaterally using a dynamometer (Biodex Medical Systems). Alignment of the dynamometer axis of rotation and the knee axis (femoral transepicondylar line) was verified. To restrict movements to the knee only, the upper body and the thigh of the tested leg were fixed using straps (Figure 2). To get accustomed to the setting and movements, participants performed 3 to 4 full flexion and extension movements with submaximal intensity before testing. The test protocol consisted of 4 reciprocal active flexion and extension movements with maximum effort at an angular velocity of 60 deg/s to evaluate isokinetic knee flexor and extensor strength. Maximum torques were recorded for each movement and leg as absolute values and normalized to body mass. For further analysis, the limb symmetry index (LSI; operated/contralateral or nondominant/dominant × 100), SSD, and hamstring/quadriceps (H/Q) ratio were calculated.
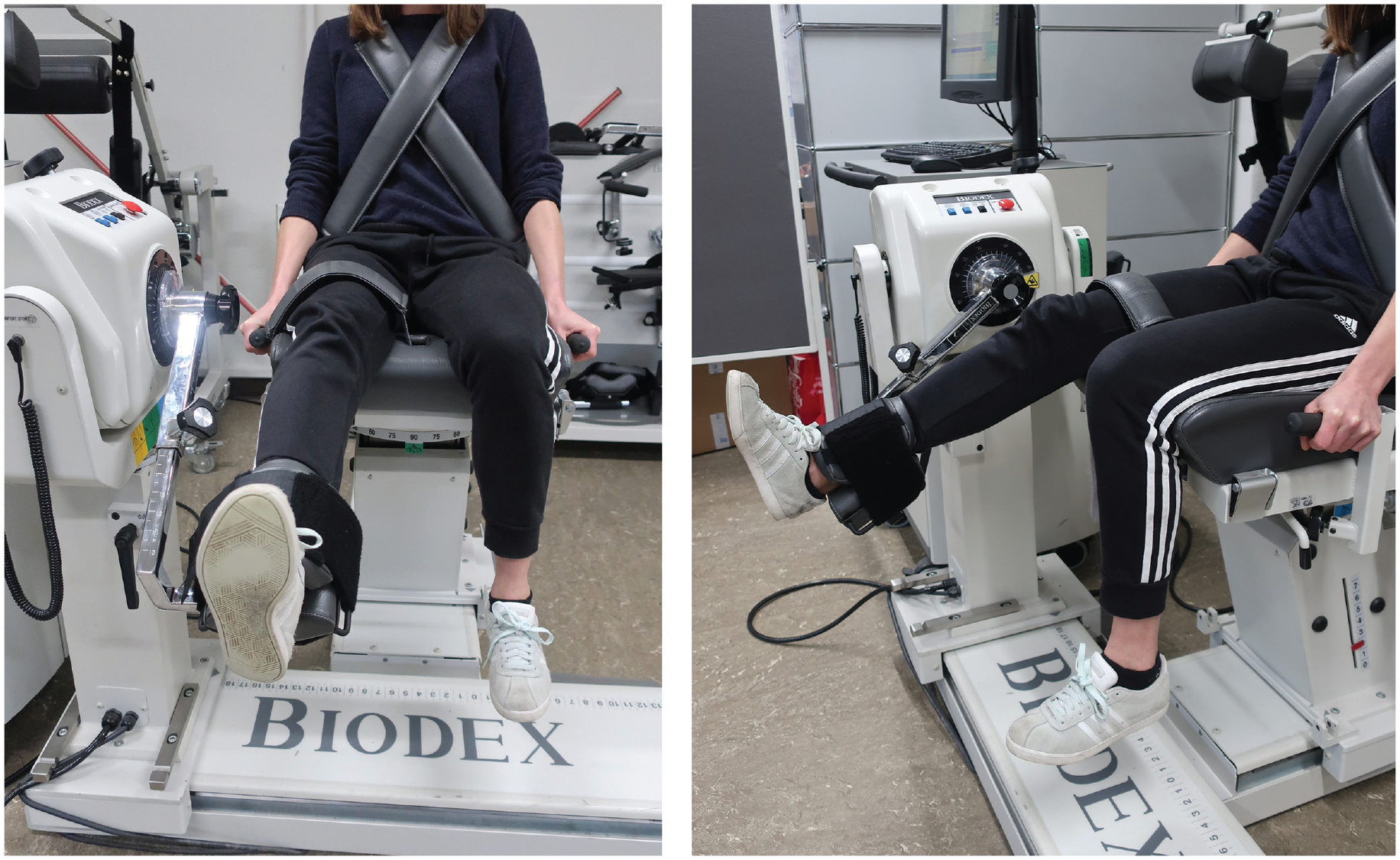
Isokinetic muscle strength measurement (extensor and flexor peak torque at 60 deg/s).
Statistical Analysis
According to our sample size calculation based on balance parameters, joint position sense, and the IKDC score, 34 28 participants per group were required to detect a statistically significant difference with a power of 80% and a significance level of 5%. Statistical analysis was performed using SPSS Version 28.0.1.0 (IBM Corp). All data were evaluated for normal distribution using the Shapiro-Wilk test. Normally distributed values (patient characteristics, surgery time, circumference, ROM, anterior tibial translation [ATT], and isokinetic strength) are presented as mean and standard deviation and were analyzed using 1-way analysis of variance with post hoc Bonferroni tests or t test for independent samples. Clinical and nonnormally distributed parameters are presented as median (25th and 75th percentiles) and were analyzed using Kruskal-Wallis test. Differences in distributions of concomitant injuries were tested using chi-square test. The level of significance was set to 5% for all tests.
Results
Demographic, Anthropometric, and Surgery- and Injury-Related Outcomes
Overall, 29 patients 2 years after ACL-IB, 27 patients 2 years after ACL-R, and 29 healthy controls met our inclusion criteria and participated in the present study. To ensure best-possible age and sex matching, we recruited 5 patients after ACL-R from 2 other medical centers. However, all included patients were treated with the same surgical technique, and the same postoperative rehabilitation was prescribed.
Patient characteristics did not differ between groups (Table 2). Time from injury to surgery was shorter in the ACL-IB group (median, 20 days) than in the ACL-R group (median, 28 days) (P = .026). Although follow-up time and numbers of concomitant injuries and surgeries were comparable between the 2 intervention groups, patients undergoing ACL-IB had a significantly shorter surgery time (mean, 81 minutes) than those undergoing ACL-R (mean, 97 minutes) (P = .024) (Table 2). Four patients in the ACL-IB group experienced ACL rerupture (Figure 1). The 4 patients with re-ruptures were excluded from the 52 patients treated with ACL-IB. We had to exclude 23 patients: 52-23 = 29. All patients included in the study completed all testings as described.
Demographic, Anthropometric, and Surgery- and Injury-Related Outcome Data of Patients After ACL-IB and ACL-R and Healthy Controls a
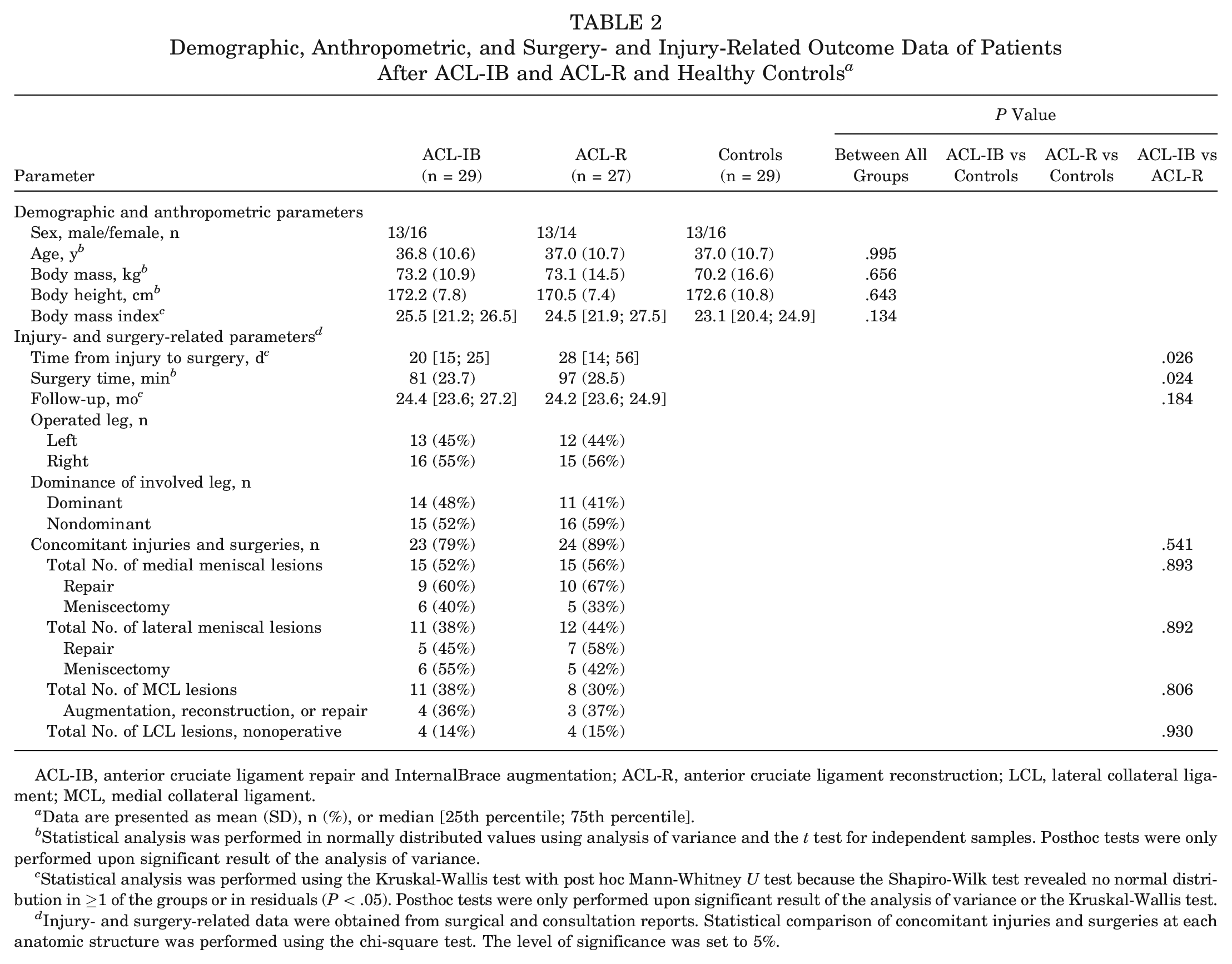
ACL-IB, anterior cruciate ligament repair and InternalBrace augmentation; ACL-R, anterior cruciate ligament reconstruction; LCL, lateral collateral ligament; MCL, medial collateral ligament.
Data are presented as mean (SD), n (%), or median [25th percentile; 75th percentile].
Statistical analysis was performed in normally distributed values using analysis of variance and the t test for independent samples. Posthoc tests were only performed upon significant result of the analysis of variance.
Statistical analysis was performed using the Kruskal-Wallis test with post hoc Mann-Whitney U test because the Shapiro-Wilk test revealed no normal distribution in ≥1 of the groups or in residuals (P < .05). Posthoc tests were only performed upon significant result of the analysis of variance or the Kruskal-Wallis test.
Injury- and surgery-related data were obtained from surgical and consultation reports. Statistical comparison of concomitant injuries and surgeries at each anatomic structure was performed using the chi-square test. The level of significance was set to 5%.
Patient-Reported Outcome Measures
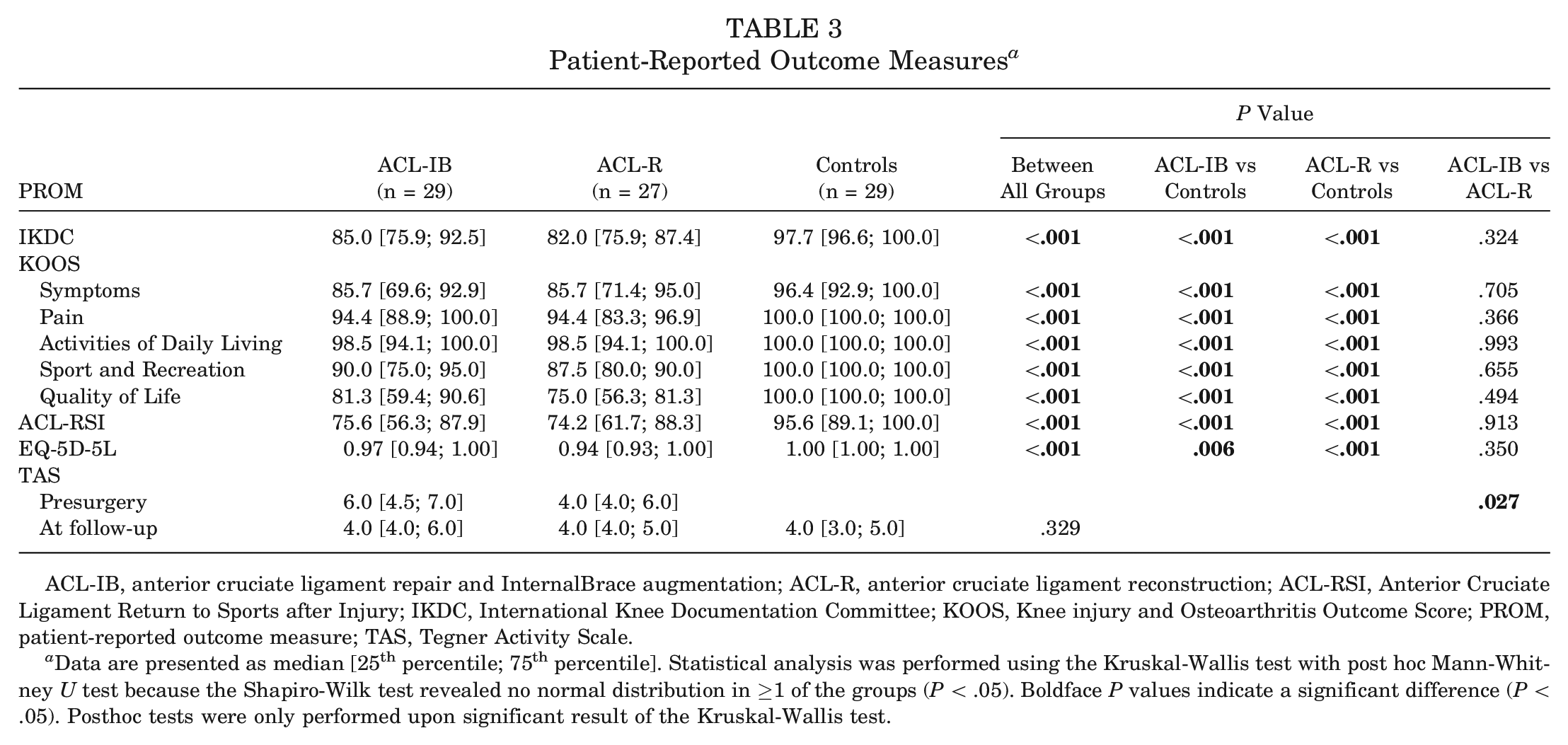
Both intervention groups (ACL-IB and ACL-R) had inferior outcomes compared with controls in all evaluated scores (Table 3). Two years postoperatively, the ACL-IB group had comparable outcomes with the ACL-R group (Table 3). The TAS showed the same activity level for the ACL-IB and ACL-R groups after 2 years (both TAS 4).
Patient-Reported Outcome Measures a
ACL-IB, anterior cruciate ligament repair and InternalBrace augmentation; ACL-R, anterior cruciate ligament reconstruction; ACL-RSI, Anterior Cruciate Ligament Return to Sports after Injury; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PROM, patient-reported outcome measure; TAS, Tegner Activity Scale.
Data are presented as median [25th percentile; 75th percentile]. Statistical analysis was performed using the Kruskal-Wallis test with post hoc Mann-Whitney U test because the Shapiro-Wilk test revealed no normal distribution in ≥1 of the groups (P < .05). Boldface P values indicate a significant difference (P < .05). Posthoc tests were only performed upon significant result of the Kruskal-Wallis test.
Clinical Examination
Thigh and shank circumferences did not differ between all groups when comparing the operated or contralateral side (Table 4). Postoperative flexion was comparable between the ACL-IB group and controls but significantly lower in the ACL-R group compared with controls (P < .001). We found both intervention groups had a significantly greater SSD in passive anterior translation than controls but no differences between the ACL-IB and ACL-R groups (Table 4). A more detailed analysis of ATT revealed that 8 patients after ACL-IB and 1 patient after ACL-R had an SSD >3 mm.
Results of Clinical Examination and Isokinetic Muscle Strength Test of Knee Flexion and Extension in Patients After ACL-IB and ACL-R and Healthy Controls a
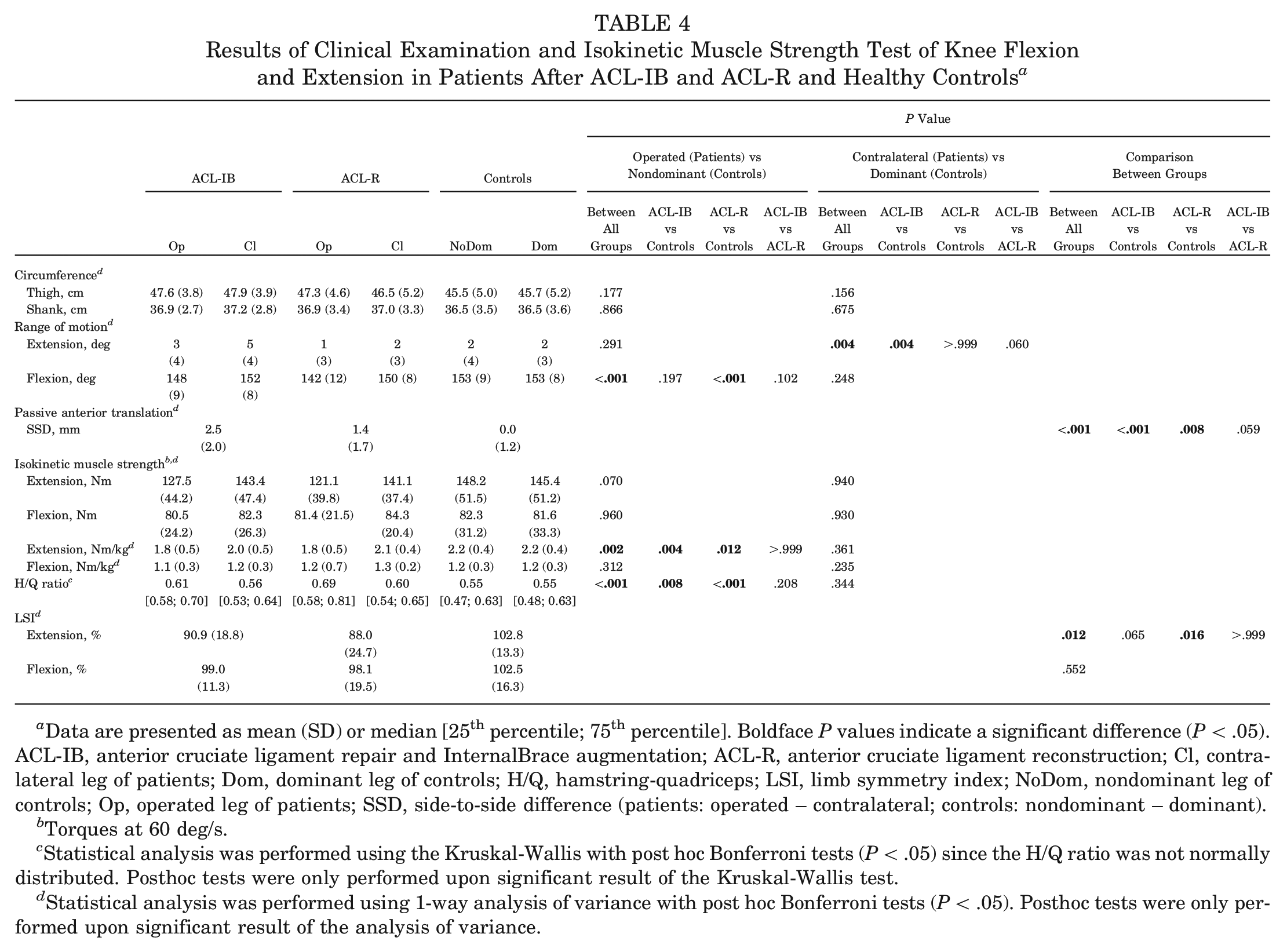
Data are presented as mean (SD) or median [25th percentile; 75th percentile]. Boldface P values indicate a significant difference (P < .05). ACL-IB, anterior cruciate ligament repair and InternalBrace augmentation; ACL-R, anterior cruciate ligament reconstruction; Cl, contralateral leg of patients; Dom, dominant leg of controls; H/Q, hamstring-quadriceps; LSI, limb symmetry index; NoDom, nondominant leg of controls; Op, operated leg of patients; SSD, side-to-side difference (patients: operated – contralateral; controls: nondominant – dominant).
Torques at 60 deg/s.
Statistical analysis was performed using the Kruskal-Wallis with post hoc Bonferroni tests (P < .05) since the H/Q ratio was not normally distributed. Posthoc tests were only performed upon significant result of the Kruskal-Wallis test.
Statistical analysis was performed using 1-way analysis of variance with post hoc Bonferroni tests (P < .05). Posthoc tests were only performed upon significant result of the analysis of variance.
Isokinetic Muscle Strength
Absolute isokinetic muscle strength for extensor and flexor muscles of both legs did not differ between all groups (Table 4). Normalized isokinetic extensor muscle strength was significantly lower in the operated leg in both the ACL-IB and the ACL-R groups than in controls (strength deficit, 14% for ACL-IB vs 18.3% for ACL-R) but not different between the ACL-IB and ACL-R groups. Correspondingly, the H/Q ratio was higher in both the ACL-IB and the ACL-R groups than in controls but not different between the ACL-IB and ACL-R groups. The LSI for extensor muscles revealed significantly lower values for the ACL-R group compared with controls but not for the ACL-IB group (Table 4).
Discussion
The most important finding of our study is that we provide new scientific evidence for the patient-reported, clinical, and functional benefits of primary ACL repair with augmentation for treatment of proximal ACL tears. Treatment with ACL-IB resulted in good to excellent clinical outcomes 2 years postoperatively that were comparable with the gold standard ACL-R. Patient-reported outcomes were comparable for both patient groups, but surgery time was 16 minutes shorter for the ACL-IB group. In contrast to patients after ACL-R, patients after ACL-IB did not have reduced knee flexion ROM or a significantly different extensor LSI compared with healthy controls. These results add to the scientific evidence for the patient-reported, clinical, and functional benefits of ACL-IB and will help in clinical decision-making and establishing of this procedure as a valuable treatment alternative for proximal ACL tears.
Overall, the included participants did not show differences regarding demographic or injury-related (for patients) data. As expected, time from injury to surgery was significantly shorter in the ACL-IB group, as primary repair of the torn ACL is best performed within a time frame of approximately 3 weeks before circulation of the stump is compromised and advanced scar tissue formation of the torn ligament is present. 53 Interestingly, even if concomitant injuries and surgeries performed along with the ACL surgery did not differ among both groups, the overall surgery time was significantly shorter for the ACL-IB group. To the best of our knowledge, to date no other study comparing ACL-IB and ACL-R investigated this aspect. A shorter surgery time not only is beneficial in terms of reduced operating room time and hence treatment costs but also reduces the risk of adverse events after ACL surgery. 4
Several studies have reported clinical outcomes after ACL-IB with follow-up times ranging from 12 months to 6 years postoperatively. ** In our study, both the ACL-IB and the ACL-R groups had lower patient-reported outcomes than healthy controls, whereas no differences between both intervention groups were found. To our knowledge, no previous study reported patient-reported outcome measures from age- and sex-matched healthy controls, and to date only 3 studies have directly compared the patient-reported outcome measures of ACL-IB and ACL-R.17,32,48 Mattiassich et al 32 presented 12- to 18-month outcomes comparing 27 patients after ACL-IB with 23 patients after ACL-R. The mean overall KOOS after ACL-IB was 83.3 versus 83.0 points after ACL-R, without significant differences between these groups. Szwedowski et al 48 reported comparable Lysholm scores 14.8 months after ACL-IB compared with ACL-R 13.6 months postoperatively. Recently, Ferreira et al 17 reported 30-month clinical outcomes (IKDC score, KOOS, and ACL-RSI) comparing ACL-IB with ACL-R (75 patients per group; age, 40.0 vs 37.6 years). Except for KOOS Symptoms scores, our 2-year results are in agreement with those of Ferreira et al, who also reported comparable or nonsignificantly better outcomes for ACL-IB compared with ACL-R. However, direct comparison is limited because our data were not normally distributed and we hence present median and not mean values.
Several clinical outcomes after ACL-IB have been summarized in a recent systematic review by Wilson et al 61 comprising 347 patients. The mean follow-up was 2.7 years (range, 1-5 years) with a mean overall KOOS of 87.7, IKDC score of 88.5, and TAS score of 6.1. Although the IKDC score and KOOS in our study are in line with those in the systematic review, the TAS score in our cohort was lower than the reported TAS score that remained unchanged compared with preoperative baseline (6.1 after 2.7 years vs 6.3 preoperatively). In our study, the activity level was comparable for both patient groups 2 years postoperatively as well as for the included healthy controls (TAS, 4 each). Hence, all patients and participants were well matched in terms of activity, and reliable outcomes for this specific cohort may be expected.
Passive ATT is considered an indicator for postoperative knee stability, 13 with SSDs reported as outcome measures in most studies.17,45,61 In our study, ATT was significantly higher in patients after ACL-IB or ACL-R than in healthy controls but did not differ between patient groups. However, SSDs of 2.5 mm in ATT after ACL-IB and 1.4 mm after ACL-R are higher than those reported in other publications. Ferreira et al 17 observed an SSD of 1.1 mm for ACL-IB and 0.6 mm for ACL-R, whereas Wilson et al 61 reported a mean SSD of 1.2 mm for ACL-IB in their systematic review. In contrast, Severyns et al 45 reported a residual side-to-side laxity of 1.6 mm after single-bundle ACL-R, which is comparable with that in our cohort. In our study, each patient was asked for subjective symptoms of instability before testing, and none of the included patients reported such symptoms or had symptomatic instability during testing. Although the overall SSD remained below the reported threshold of 3 mm at which knee laxity may be assumed,5,13,42,45 some patients after ACL-IB had an SSD in ATT >3 mm. However, because ATT measurements using a Rolimeter only allow determination of 2-mm increments, this accuracy may not allow us to define a clear cutoff of 3 mm as reported in the literature. To account for this potential limitation and to rule out that a higher ATT had an effect on the results presented, we performed a subgroup analysis comparing patients who underwent ACL-IB with an SSD in ATT >3 mm with those with values <3 mm. None of the statistical tests revealed a significant difference in clinical and functional outcomes among both groups (all P > .05), suggesting that ATT measured with a Rolimeter during a Lachman test may not be determinative of clinical and functional outcomes, at least at the follow-up reported in this study. Whether an increased postoperative SSD in ATT may be an influencing factor for long-term clinical and functional outcomes, especially after ACL-IB, needs to be investigated in long-term studies.
Loss of extensor and flexor strength and the physiological balancing of these muscles are a common concern after ACL surgery. In particular, a persisting quadriceps deficit—a risk factor for early onset of knee osteoarthritis 49 —has been reported after ACL-R.7,11,29,38 For instance, Chung et al 11 reported a persisting quadriceps strength deficit of 17% 2 years after ACL-R using hamstring grafts compared with matched healthy controls, which is in line with our own findings. Although absolute strength values did not differ between groups in our study, normalizing these values to body mass revealed significantly impaired extensor strength for the ACL-IB and ACL-R groups compared with the healthy controls. However, no significant differences were found for flexor and extensor strength when comparing ACL-IB and ACL-R, with nonsignificantly higher absolute extensor strength in the ACL-IB group. This is corroborated by the only study published to date that directly compared strength measurements between ACL-IB and ACL-R. Ferreira et al 17 reported no significant differences between groups regarding extensor muscle strength 6 months postoperatively, although strength deficits after ACL-IB were less pronounced (–23.1%) compared with ACL-R (–28.2%). The reestablished extensor muscle strength after ACL-IB is also demonstrated when analyzing the LSI: compared with the noninjured reference extremity of each patient, only patients who underwent ACL-IB were, on average, able to pass the critical threshold of 90%, which must be met for a safe return to sports after ACL surgery. 6
The H/Q ratio is often reported and describes the muscle balancing of each leg. Depending on age and angular velocity, the physiological range of the H/Q ratio is specified between 0.50 and 0.75,1,22 indicating that physiologically the quadriceps muscle is up to twice as strong as the hamstring muscles. Even though we did not observe significant differences between both patient groups, our findings indicate an improved postoperative muscle balancing in the patients who underwent ACL-IB, as these ratios were closer to those of the matched healthy controls.
A particular strength of our study is that we report comprehensive patient-reported, clinical, and functional comparative analysis 2 years after ACL-IB and ACL-R and include healthy controls. Furthermore, this is a single-center study with well-defined inclusion and exclusion criteria; all groups were matched for age and sex and did not differ in their knee-specific activity level. In particular, we focused on recreational athletes and nonathletes, for whom scientific evidence is especially scarce, and hence were able to present a range of outcome parameters for this particular cohort. Demographic, anthropometric, and surgery-related parameters did not differ between groups. Hence, the observed differences in the outcome parameters between groups cannot be attributed to differences in patient characteristics between groups but indeed represent differences in function between groups. Overall, the results will be helpful in understanding potential functional and physiological benefits of primary augmented ACL repair and in finding the optimal treatment strategy for future patients (including optimized patient selection) as well as for optimizing the rehabilitation of patients after ACL rupture treated with ACL-IB or ACL-R.
Potential limitations of our study include the fact that our approach of matching all groups for sex and age and not comparing consecutive patients in both patient groups precluded reporting and comparison of failure or reoperation rates. Recruitment of consecutive patients in both patient groups could have resulted in differences in patient characteristics and activity levels between groups, and potential differences in outcomes could not have been attributed to the surgical technique. In addition, we did not obtain preoperative or follow-up data beyond 2 years. However, according to Janssen et al, 27 the remodeling of hamstring grafts used for ACL-R is completed 2 years after surgery at the earliest. Hence, only after this period should a meaningful examination of function in daily life and sports be carried out, which is why we decided to focus particularly on the 2-year outcomes, as did other studies on ACL repair with augmentation.23,28 For a direct comparison of ACL-IB and ACL-R, it would have been interesting to include isolated ACL injuries. However, isolated ACL injuries only account for approximately 10% of cases. 47 Limiting a study to these 10% of patients with ACL injuries would have severely compromised the relevance of the results to typical clinical populations and would require very long recruitment periods or multicenter trials (including multiple surgeons) to achieve the required sample size. Importantly, both patient groups were comparable in terms of concomitant injuries and surgeries, and the secondary injuries included reflect very well what is seen in clinical practice on a daily basis. In addition, both patient groups (and the control group) were comparable in age and sex distribution. Hence, the results presented here can be considered a realistic reflection of the majority of patients evaluated in outpatient clinics and thus may be of great importance for the orthopaedic community. As the mean age of the patients included in our study was between 36 and 37 years, the results presented here may not be fully applicable to younger patients, in whom poorer outcomes and higher rates of rerupture have been reported after ACL-IB. 18
Postoperative magnetic resonance imaging scans or arthroscopic follow-up that would have allowed assessment of ACL healing (or graft integrity) and whether the InternalBrace was still intact 2 years after surgery were not available. Hence, it is not possible to answer whether the InternalBrace is still functioning as a load-sharing device at the time of publishing. Moreover, randomization of patients evaluated with proximal ACL tears (Sherman types 1 and 2) to an ACL-IB, ACL-R, or nonoperative treatment group was not possible in this study design. However, considering that according to van der List et al 56 only 16% of all ACL ruptures qualify as Sherman type 1 (proximal avulsion of ACL with distal ligament remnant >90%) and a maximum of 27% as the already less suitable for repair type 2 (ligament remnant, 75%-90%), it would have been impossible to carry out this study with an adequate number of patients within an appropriate time frame. Finally, 14 patients eligible for ACL-IB were either not reachable or not interested in participating, thus introducing the possibility of selection bias.
In summary, the presented results support the clinical and functional benefit of ACL-IB and add to the scientific evidence supporting this technique. However, further comparative studies and randomized controlled trials with larger patient cohorts, including other tendon grafts commonly used for ACL-R (bone–patellar tendon–bone, quadriceps, and allografts), are needed to confirm these findings.
Conclusion
ACL-IB achieves comparable patient-reported, clinical, and functional outcomes with ACL-R, including improved postoperative leg symmetry. Based on these results, ACL-IB can be considered a valuable and reliable alternative early treatment option for proximal ACL tears for a carefully selected patient population.
Footnotes
Acknowledgements
The authors express their gratitude to Prof. Dr Anja Hirschmüller and Dr Bertram Rieger (both Altius Swiss Sportmed Center AG, Rheinfelden, Switzerland) for referring patients after ACL-R to our investigation.
Submitted February 6, 2023; accepted July 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Deutsche Arthrose-Hilfe e.V. (P486-A1195; Saarlouis, Germany), Swiss Orthopaedics, and the Department of Orthopaedics and Traumatology of the University Hospital Basel, Basel, Switzerland. The funding sources were involved neither in the study design, collection, analysis, or interpretation of data nor in the writing of the manuscript or in the decision to submit the manuscript for publication. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.