
Abstract
Background:
Meniscal allograft transplant (MAT) is an effective treatment for relieving symptoms and improving knee function in patients who experience symptomatic unicompartmental knee pain after a previous meniscectomy. However, the literature contains a paucity of studies assessing the survival rate and prognostic factors of soft tissue MAT.
Purpose:
To report the survivorship of a large, single-center cohort of consecutive patients treated with arthroscopic MAT using soft tissue technique and to investigate variables that could potentially influence failures and outcomes.
Study design:
Case series; Level of evidence, 4.
Methods:
Consecutive MAT procedures totaling 364 performed in a single institution between June 2004 and April 2019 were screened and assessed for eligibility. Subjective clinical scores (Lysholm score, Tegner activity scale, and visual analog score) were collected preoperatively and at 2, 5, 7, and 10 years of follow-up. Two survival analyses were performed using Kaplan-Meier curves, with surgical failure (defined as any graft revision) and clinical failure (defined as a Lysholm score <65 points) used as endpoints. Univariate analyses were performed using reoperations, surgical failure, clinical failure, and different demographic and surgical characteristics as endpoints.
Results:
A total of 324 consecutive patients were evaluated at a mean follow-up 5.7 ± 3.0 years. Of these, 189 (58%) underwent an associated surgical procedure. A total of 22 patients (6.8%) were considered to have experienced surgical failure, and no predictors of surgical failure were identified based on the relevant variables. When all patients were considered, a significant improvement in all of the patient-reported outcome measures was present between the preoperative assessment and the last follow-up (P < .001), with no significant decrease over time. Moreover, 70 (21.6%) patients were considered to have experienced clinical failure; the need for concurrent cartilage procedures (odds ratio, 0.16; P = .001) and anterior cruciate ligament (ACL) reconstruction (odds ratio, 0.40; P = .059) were predictors of failure. Finally, a lower survival rate was reported in female patients compared with male patients (49% vs 69%, respectively; P = .007) and in patients who required cartilage surgery (P = .014). In particular, patients who required cartilage surgery showed nearly half the survival rate compared with those with required no cartilage procedures at 10-year follow-up (36.4% vs 71%, respectively; P = .029).
Conclusion:
Female sex and the need to combine MAT with a cartilage procedure or ACL reconstruction could result in an increased rate of clinical failure at midterm follow-up.
Meniscal allograft transplant (MAT) is an effective treatment for postmeniscectomy syndrome, which entails a symptomatic noncompartmental pain in the meniscus-deficient knee without significant articular cartilage wear. 5 The aim of MAT is to reestablish meniscal functional status, providing protection and stability to the joint. 2 Many reviews have shown that MAT provides good clinical results at short- and midterm follow-up, especially pain relief and mechanical function.6,22 In a meta-analysis of 3157 MAT procedures, investigators reported a significant improvement in clinical outcomes at both medium- and long-term follow-up (5-15 years) across all outcome measures and good patient satisfaction at long-term follow-up. 4 Novaretti et al 19 reported reasonable long-term survivorship, with 73.5% and 60.3% of allografts remaining functional after 10 and 15 years, respectively. However, the current knowledge of MAT survivorship is limited, the main limitation being the small cohorts studied, which rarely exceed 100 patients. 26 A few larger case series reported survival analysis and outcome, especially of the bony fixation technique.17,25 The mean survival rates ranged from 11 years24,28 to 16.1 years, 26 and each study proposed different criteria to define failure 18 : some definitions were based on clinical outcome and knee function alone, and others relied on a patient’s need for reoperation, although without consensus on the kind of outcomes considered to indicate failure.
Another controversial issue involves the identification of failure predictors, especially concerning the role of concurrent procedures associated with MAT.14,29 The acceptable threshold of articular cartilage damage is currently not known, and the majority of surgeons report moderate or severe degeneration to be an exclusion criterion. However, some evidence indicates that chondral damage identified and treated at the time of MAT may not affect the clinical outcomes of MAT. 23
Considering this background, the principal aim of the present study was to report the survivorship of a large cohort of MAT procedures performed in a single center using a soft tissue technique, according to clinical outcomes and surgical revisions. The secondary aim was to investigate the potential predictors of MAT survivorship and assess the trend of clinical outcomes over time. The hypothesis was that a progressive decrease in survival rate would occur between short- and long-term follow-up and that the complexity of cases (eg, concurrent procedures, advanced chondral damage) could affect the survival probability.
Methods
All MAT procedures performed in a single institution (Rizzoli Orthopaedic Institute) between June 2004 and April 2019 (n = 364) were screened and assessed for eligibility. Indications for MAT were unicompartmental pain due to a previous total or subtotal meniscectomy, with osteoarthritis grade 1 to 3 according to the Kellgren-Lawrence 10 radiographic evaluation, no signs of contralateral compartment or patellofemoral compartment damage, and <5° of coronal malalignment. A corrective osteotomy was performed in patients who had >5° of malalignment. A concurrent anterior cruciate ligament (ACL) reconstruction was performed in cases of anteroposterior knee laxity and patient-reported subjective instability. In patients with focal Outerbridge 20 grade 4 chondral lesions <2 cm2, microfractures were performed, whereas in cases of larger focal Outerbridge grade 4 lesions, a scaffold was implanted. All patients undergoing MAT were adequately counseled regarding the risks and benefits of the procedure and surgical alternatives. Inclusion criteria for the present study were both medial and lateral MAT that reached the minimum follow-up of 2 years, with no limits regarding age or concurrent procedures. No other exclusion criteria were applied.
Surgical Technique
Fresh-frozen (−80°C) nonirradiated and non–antigen matched allografts were used. The meniscal allografts were provided by the regional tissue bank and were matched to the patients using the anthropometric method. 27
All patients underwent MAT with soft tissue fixation, without any bone plugs or bone bridge. The original surgical technique required a single-tunnel fixation on the posterior horn with a suture secured to the periosteum. More recently, a double-tunnel technique was developed with 2 separate sutures for the anterior and the posterior horn that are tied together. However, the single-tunnel technique is still performed in the presence of graft size mismatch.8,16 Peripheral suturing to the capsule was performed with all-inside stitches (nonabsorbable Ultrabraid No. 0 wire and poly-
The postoperative rehabilitation protocol started with a 2-week period of immobilization and no weightbearing, followed by toe-touch weightbearing for the following 2 weeks, restriction of range of motion (ROM; 0°-90° during weeks 3-4 and then free ROM), isometric exercises, and closed kinetic chain strengthening. At week 4 postoperatively, partial weightbearing was allowed, and at week 6 postoperatively, progression to full weightbearing was started; full flexion of the knee was also allowed. Sport-specific exercises were started after 3 months, whereas return to noncontact activities was not allowed until the fourth month. Patients were advised not to resume demanding sports activities before 8 months postoperatively. Because of the cautious nature of the rehabilitation protocol regarding knee mobilization and weightbearing, no substantial differences were present in cases of concurrent ACL reconstruction, osteotomy, or cartilage procedures.
Patient Evaluation
Patient details were extracted from medical records, including the number of years from the first meniscectomy, cartilage status, and details of the surgical intervention and concurrent procedures. All patients were contacted by telephone by 2 investigators (I.R., V.C.), who interviewed the patients and administered questionnaires.31,32 The preoperative evaluation was performed with the Lysholm score, the Tegner activity scale, and a 0- to 100-point visual analog score (VAS). The same scores were repeated at 2, 5, 7, and >10 years of follow-up. All of the procedures performed during the follow-up period were recorded.
Based on these data, 2 different criteria for failure were used. Surgical failure was considered to have occurred when patients required revision procedures related to the initial MAT, such as total knee arthroplasty, unicompartmental knee arthroplasty, meniscectomy due to graft tear, or revision MAT. In cases of surgical failure, clinical scores were not gathered at the time of the interview, and the time from MAT to revision surgery was noted and used for survival analysis. Clinical failure was considered to have occurred when patients required the revision procedures listed previously and when patients had a poor Lysholm score (<65 points) 3 at final follow-up. In cases of clinical failure, the survival time was considered to be the time when follow-up was collected, and this temporal landmark was used as the time to failure in the survival analysis.
Ethics
The study (prot. gen. No. 0021258) was approved by the institutional review board of the Rizzoli Orthopaedic Institute, Bologna, Italy.
Statistical Analysis
Statistical analysis was performed with SPSS software (IBM). Continuous parametric variables were expressed as mean ± SD, the Tegner score was expressed as median with interquartile range, and categorical variables were expressed as number and percentage. The Student t test was used to compare continuous variables, the Wilcoxon test to compare Tegner scores, and the chi-square test to compare categorical variables.
Survival analyses were performed using the Kaplan-Meier method. Survival proportions at 2, 5, 7, and 10 years and mean survival time were calculated. Univariate analyses were performed using surgical failure, clinical failure, and reoperations as endpoints; the independent variables used were sex, age, graft side (medial vs lateral), body mass index (≤25 vs >25), time from first meniscectomy, time from last meniscectomy, Outerbridge grade (0-2 vs 3-4), type of MAT (isolated vs combined), concurrent ACL reconstruction, concurrent osteotomy, and concurrent cartilage procedure. The patients obtaining a Lysholm score <65 at the follow-up interview were considered to have experienced clinical failure. The time of surgical failure, when available, was retrieved so as to not overestimate the survival time. Variables that had a P value <.10 in the univariate analysis were used in a multivariate regression analysis and chosen as factors for the Kaplan-Meier survivorship analysis using the log-rank test. The presence of generic concurrent procedures (ie, either ACL reconstruction, osteotomy, or cartilage) was also investigated as a relevant factor in the survivorship analysis. Differences were considered significant with P < .05.
Results
A total of 364 patients received a MAT within the considered period and were thus included in the present study (Figure 1). After the telephone interview, the data of 324 patients (89%) were obtained at a mean follow-up of 5.7 ± 3.0 years (Table 1). Among these, 182 (56%) underwent medial MAT, and 142 (44%) underwent lateral MAT. At the time of the index procedure, chondral damage was present in 130 patients (40%) and grade 1 chondromalacia was present in 12 patients (4%), grade 2 in 63 patients (19%), grade 3 in 61 patients (19%), and grade 4 in 58 patients (18%). Thus, 63% of patients were considered to have no or mild chondral damage, whereas 37% had moderate to severe chondral damage. A total of 189 patients (58%) underwent ≥1 concurrent procedure: 76 (23%) underwent high tibial or distal femoral osteotomy, 81 (25%) underwent primary or revision ACL reconstruction, and 57 (18%) underwent at a cartilage procedure (Table 2).
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) diagram. MAT, meniscal allograft transplant.
Patient Characteristics a
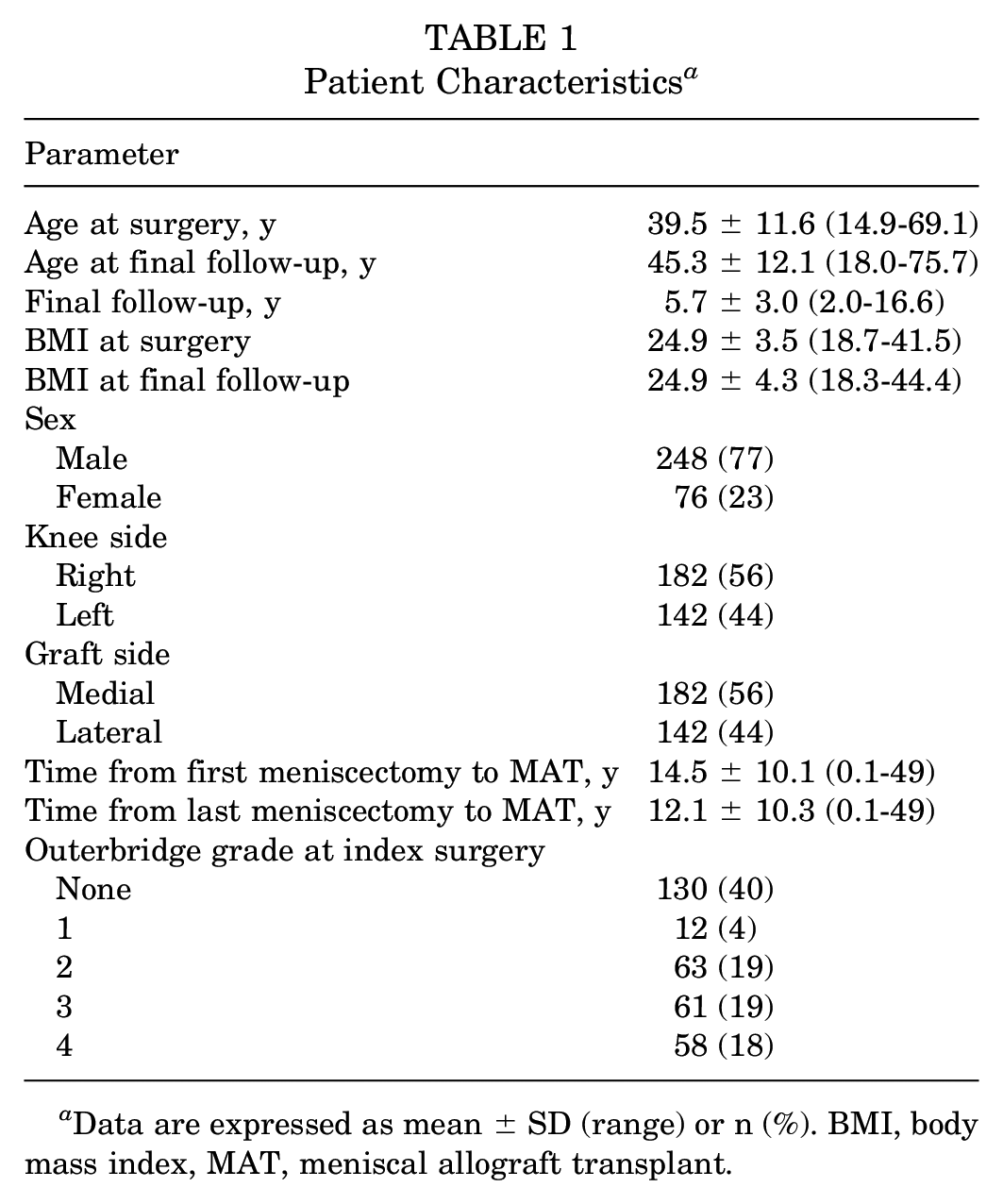
Data are expressed as mean ± SD (range) or n (%). BMI, body mass index, MAT, meniscal allograft transplant.
Concurrent Procedures Performed in Association With MAT at the Time of the Index Surgery a
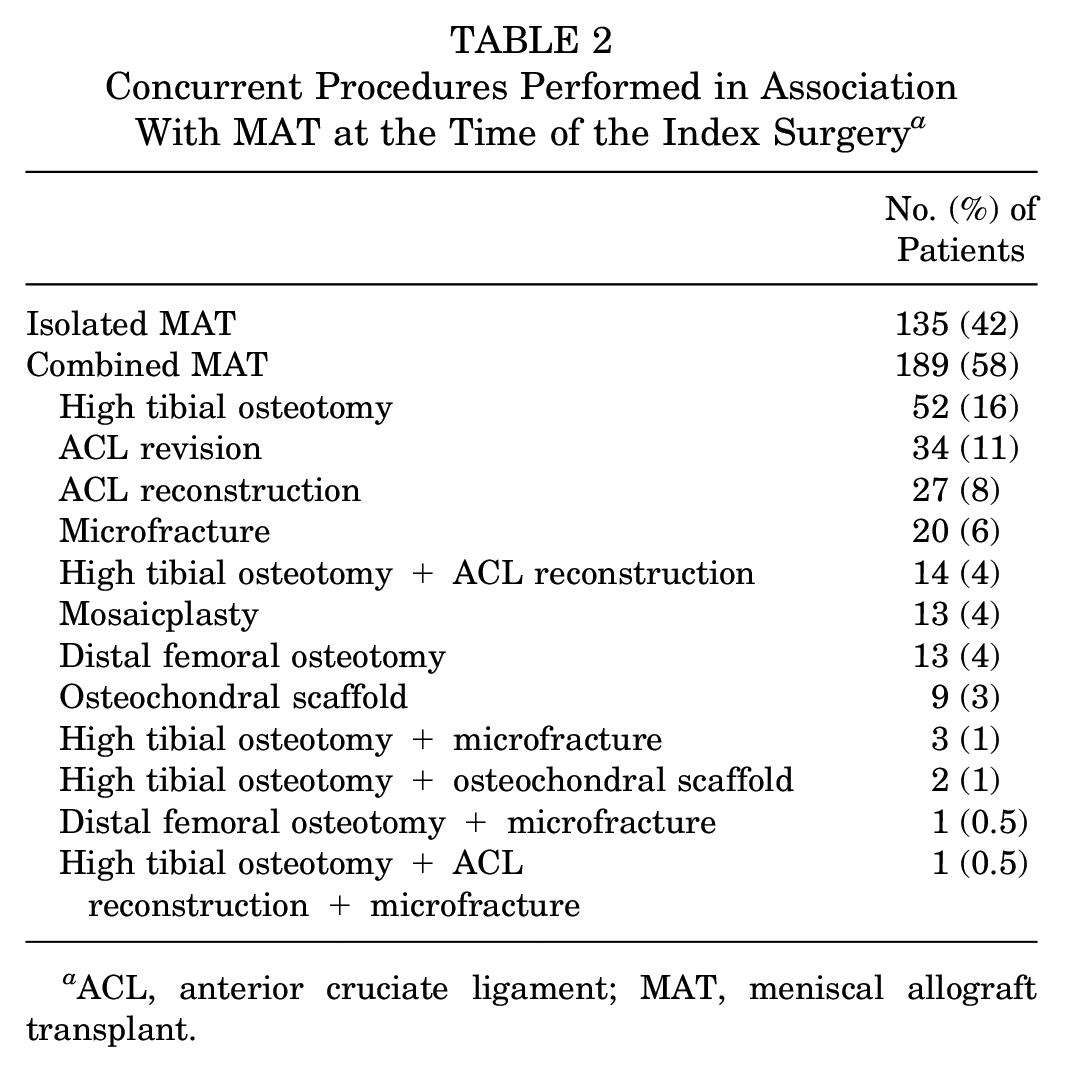
ACL, anterior cruciate ligament; MAT, meniscal allograft transplant.
Reoperations and Surgical Failures
Overall, 62 patients (19%) underwent a surgical procedure during the considered follow-up; thus, the survivorship from all reoperations was 87.5% at 2 years, 82.3% at 5 years, 78.2% at 7 years, and 74.1% at 10 years. No predictors of reoperations were identified with univariate and multivariate analyses. No differences in survivorship from reoperations were reported based on the relevant variables (Figure 2; Table 3). The clinical outcomes were similar among the 2 fixation groups, and no difference was reported between the single-tunnel and double-tunnel techniques in terms of surgical failures (6.3% vs 6.8%, respectively; P = .91) and clinical failures (18.9% vs 16.9%; P = .75).
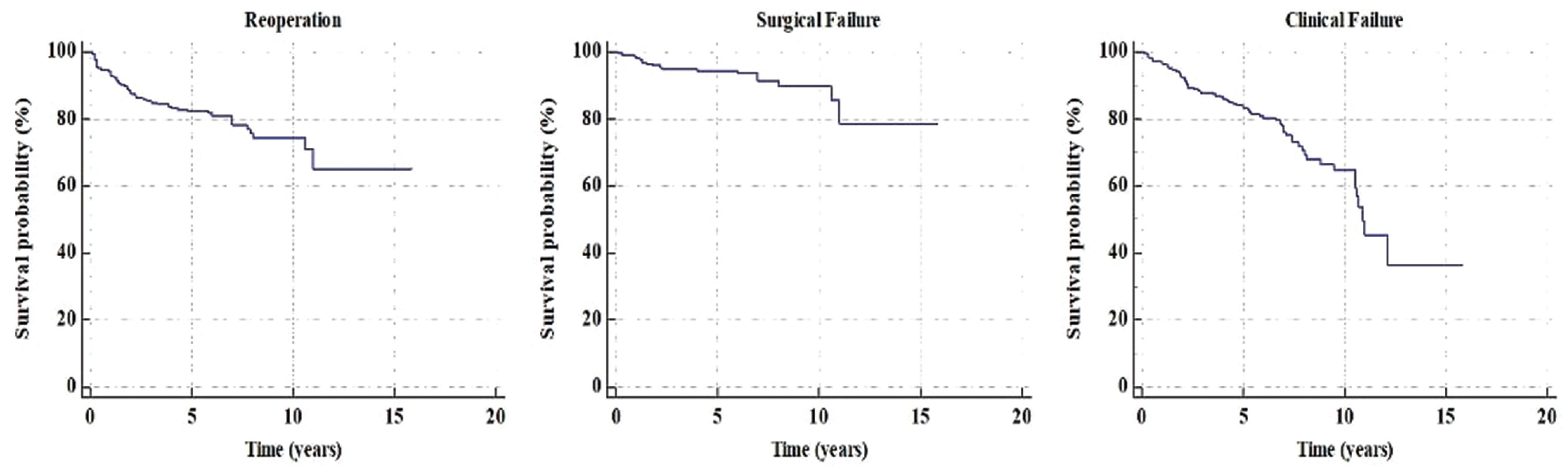
Survival rates according to different endpoints.
Type, Cause, and Timing of Reoperations Performed Over the Follow-up Period a
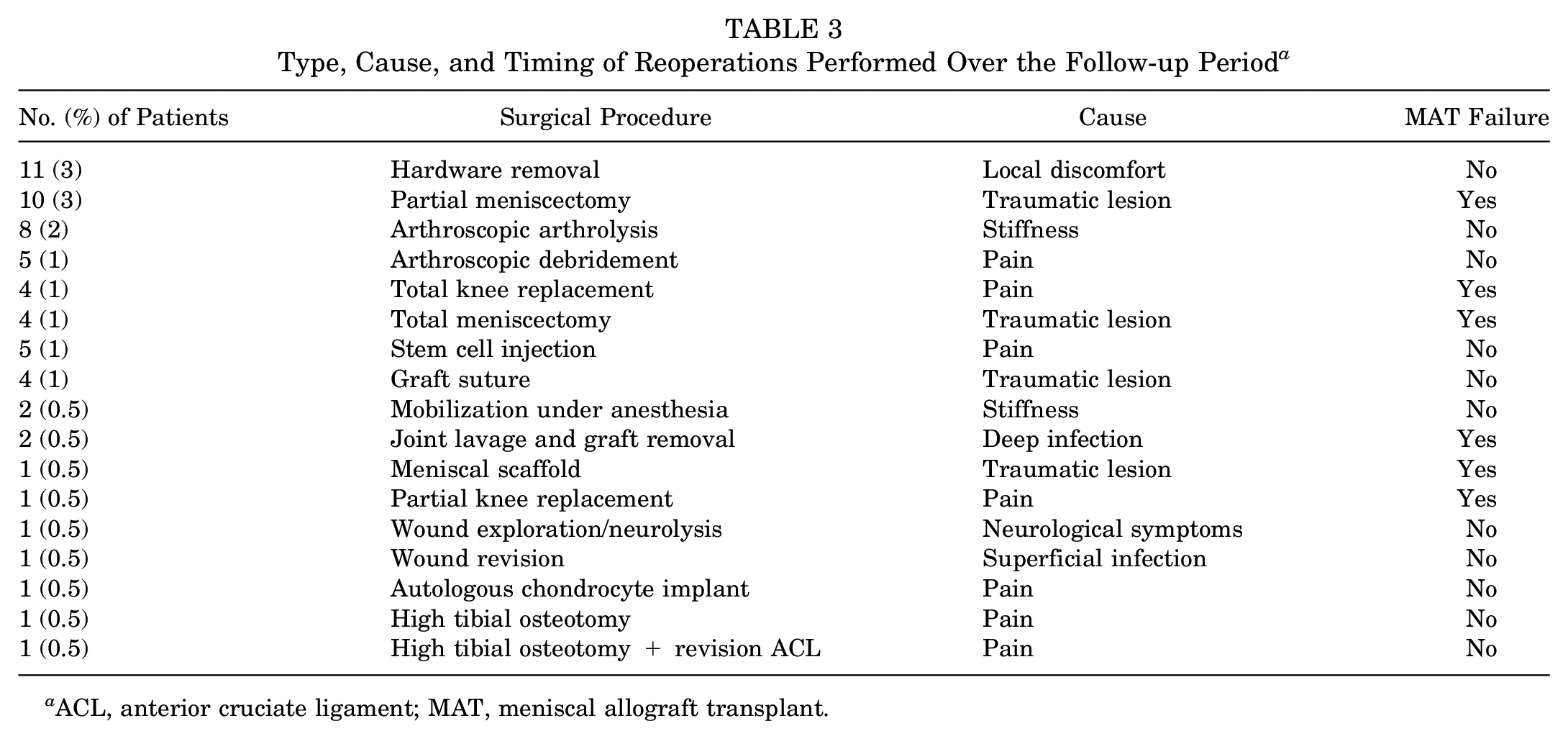
ACL, anterior cruciate ligament; MAT, meniscal allograft transplant.
In total, 22 procedures (7%) were considered surgical failures (Table 4); therefore, the survival rate from surgical failure was 96.1% at 2 years, 94.3% at 5 years, 91.4% at 7 years, and 89.6% at 10 years. No predictors of surgical failures were identified with univariate and multivariate analysis (Figure 3). In addition, no differences in survivorship from surgical failure were reported based on the relevant variables.
Survival Rates From Surgical Failures According to Different Variables a
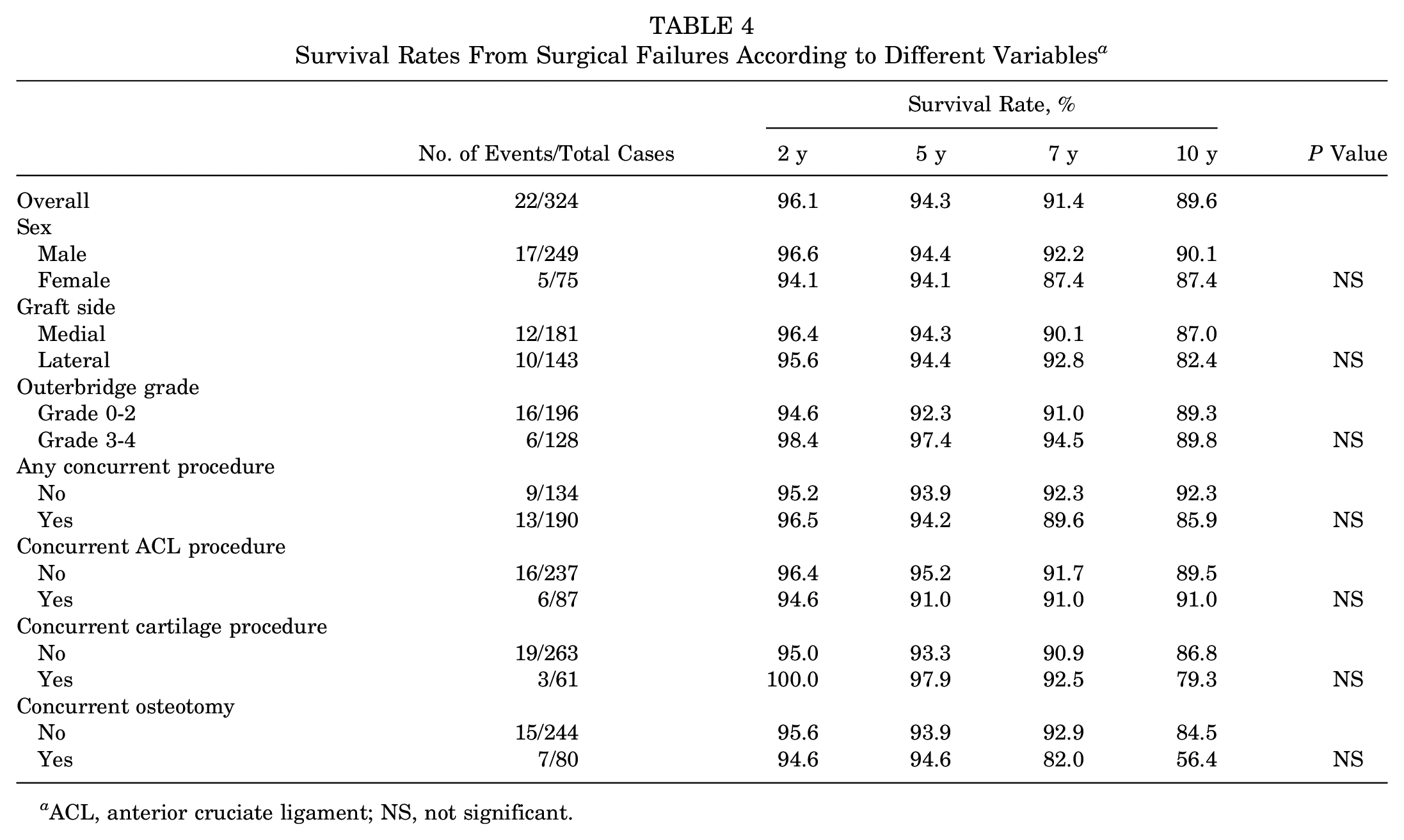
ACL, anterior cruciate ligament; NS, not significant.
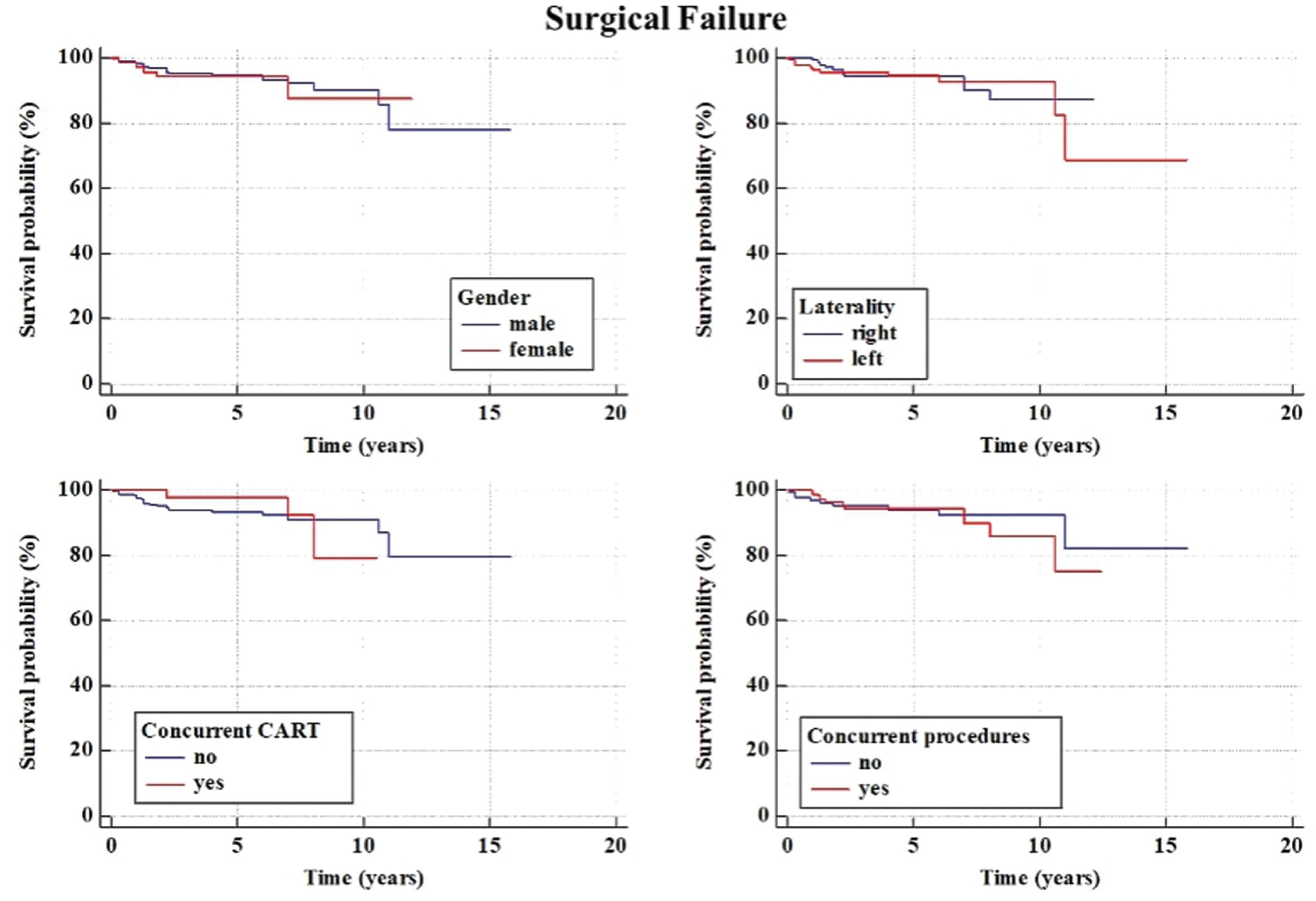
Kaplan-Meier survival curves for surgical failure and subgroup analysis based on graft side (medial vs lateral). CART, cartilage procedure.
The remaining 40 reoperations (12%), mostly hardware removal and arthroscopic arthrolysis due to stiffness, were not related to the failure of the graft and were thus not considered surgical failures.
Clinical Scores
Significant improvements of Lysholm score, VAS score for pain, and Tegner activity score were present between the preoperative assessment and the last follow-up at a mean of 5.7 ± 3.0 years (P < .001). The clinical scores were stable over time, as no significant differences were found between the 2, 5, 7, and >10-year follow-up points (Table 5; Figure 4). A total of 48 patients (15%) had a poor Lysholm score and were thus considered to have experienced clinical failure.
Patient-Reported Outcomes at the Different Follow-up Points a
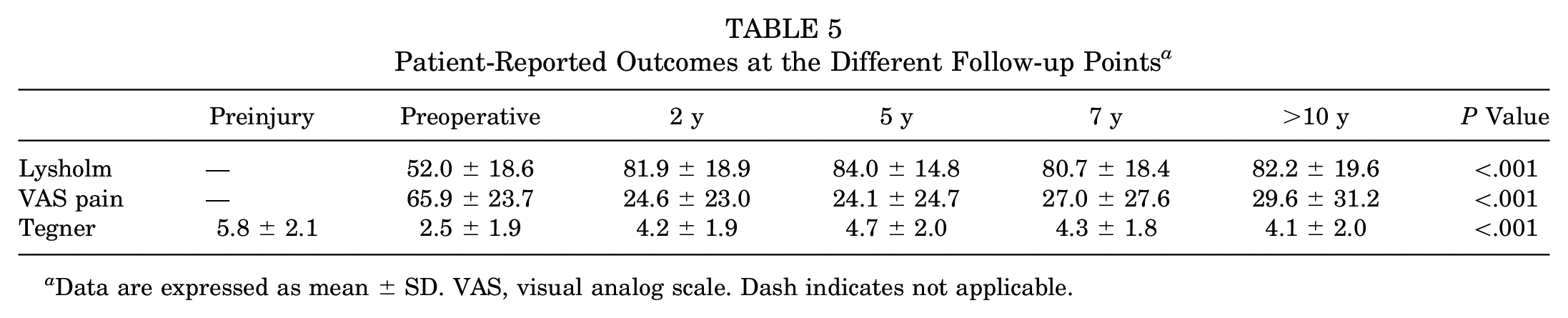
Data are expressed as mean ± SD. VAS, visual analog scale. Dash indicates not applicable.
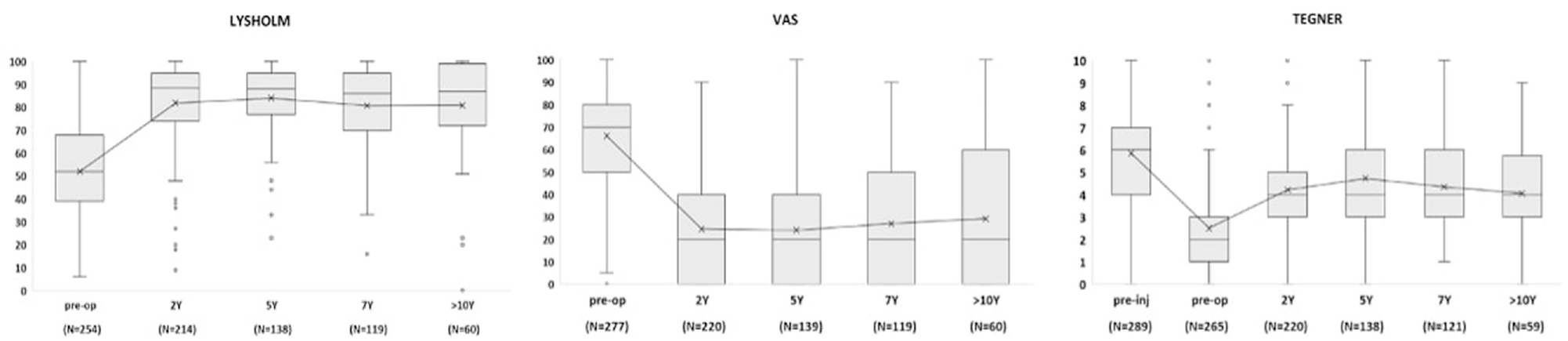
Mean values of the clinical scores and the number of patients included in the analysis at the various follow-up points. Pre-Inj, preinjury; Pre-op, preoperative; VAS, visual analog scale.
Clinical Failures
Given that 48 patients had a poor Lysholm score and 22 patients experienced surgical failure, a total of 70 patients (22%) were identified as having experienced clinical failure (Figure 5). Overall, the survival rate from clinical failure was 92.2% at 2 years, 83.3% at 5 years, 76.0% at 7 years, and 64.5% at 10 years (Figure 5; Table 6). The univariate analysis identified the presence of a concurrent cartilage procedure (odds ratio [OR], 0.16; P = .001) and the presence of concurrent ACL reconstruction (OR, 0.40; P = .059) as predictors of failure (Table 7). The multivariate analysis identified the presence of a concurrent cartilage procedure as the only predictor of failure (OR, 6.4; P = .01). Moreover, a lower survival rate was reported in female patients compared with male patients (P = .007) and in patients who underwent concurrent procedures compared with those who had isolated MAT (P = .014). Specifically, patients who underwent a concurrent cartilage procedure had nearly half the survival rate at 10-year follow-up compared with patients who had no cartilage procedure (P = .029) (Figure 5; Table 7).
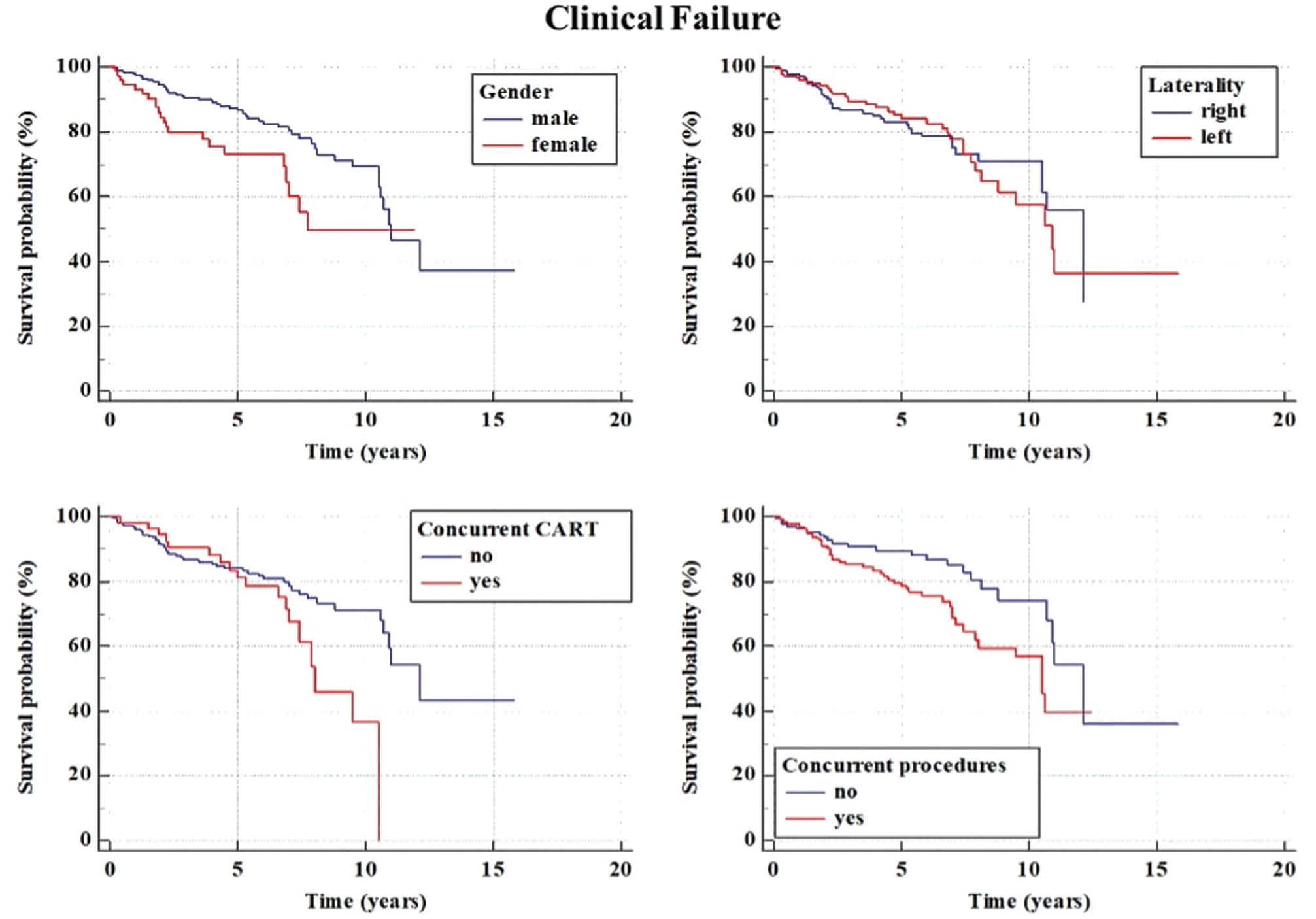
Kaplan-Meier survival curves for clinical failure, which was defined as surgery for graft removal or poor Lysholm score (<65 points), and subgroup analysis based on graft side (medial vs lateral). CART, cartilage procedure.
Survival Rates From Clinical Failure According to Different Variables a
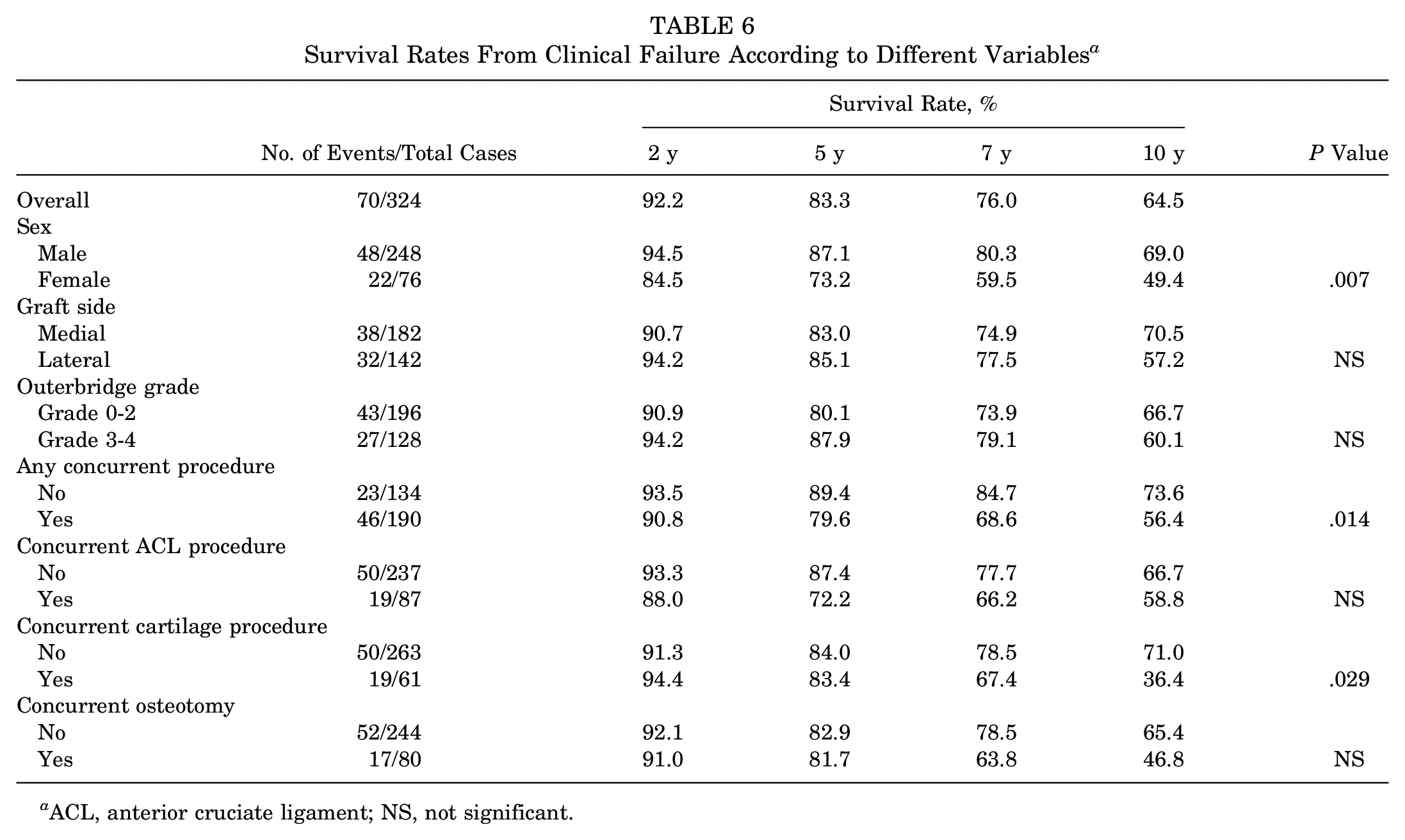
ACL, anterior cruciate ligament; NS, not significant.
Univariate Regression for the Outcomes Associated With Surgical and Clinical Failure a
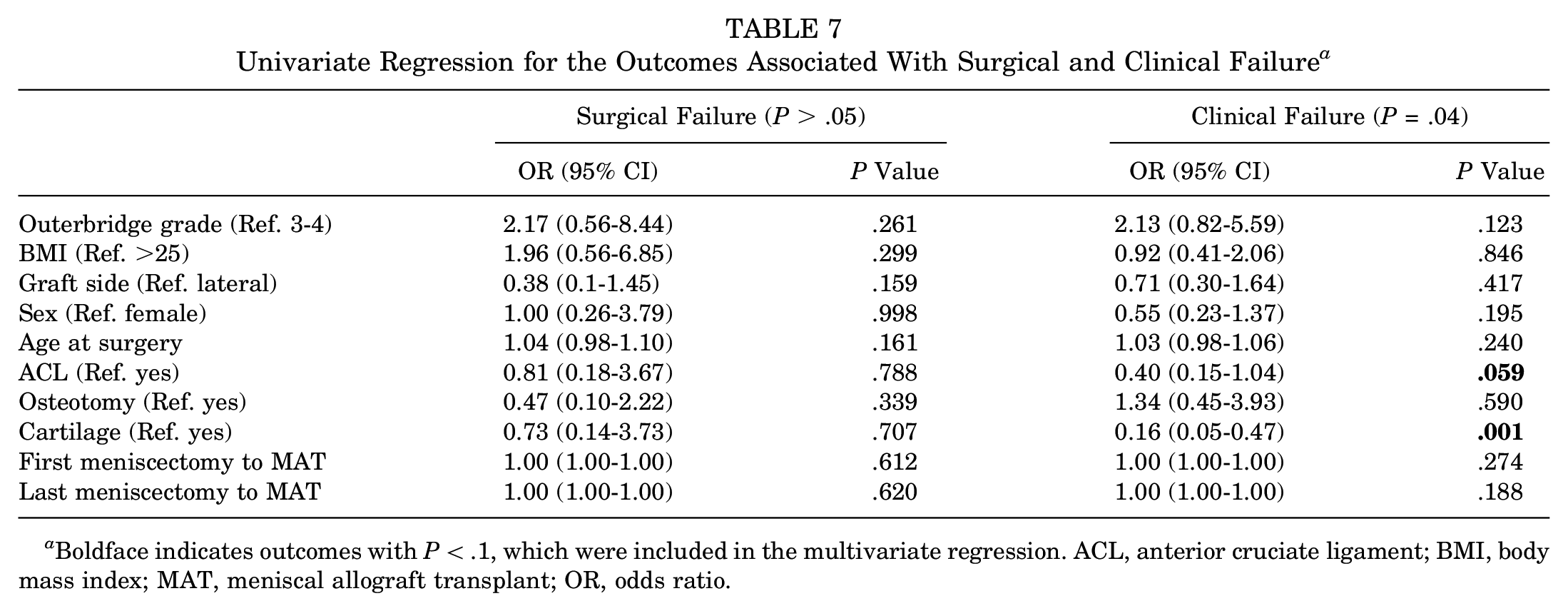
Boldface indicates outcomes with P < .1, which were included in the multivariate regression. ACL, anterior cruciate ligament; BMI, body mass index; MAT, meniscal allograft transplant; OR, odds ratio.
Discussion
The most important finding of the present study was that a satisfactory survival rate and subjective clinical outcomes of up to 10 years could be obtained with MAT performed with soft tissue fixation, both as an isolated procedure and in the case of combined surgeries. However, a concurrent cartilage procedure and female sex appeared to be correlated with inferior outcomes. The present study has several strengths that highlight its results in the panorama of MAT. To our knowledge, the present study is the largest single-center case series in the literature to date, entailing >320 MAT procedures performed with a modern arthroscopic technique and soft tissue fixation. This aspect is crucial because most of the larger case series published so far involve bony fixation techniques, and it is still controversial whether one technique is superior to the others. The present study reported survival rates of 94% at 5 years and 89% at 10 years, rates that are comparable with other large case series that involved bone plug fixation techniques.12,17 This finding contrasts the results of a recent meta-analysis by Ow et al, 21 who found a lower reoperation rate with the bone plug fixation technique. Interestingly, those investigators did not specify whether the reoperations were related to the MAT procedure, and the rate of second surgery was not weighted based on the percentage of concurrent procedures. In contrast, considering only the graft failures, the suture technique (6.9%) showed similar results to the bone plug techniques (6.2%) and a lower failure rate compared with the bone bridge techniques (9.3%).
Extreme care should be used when comparing failure rates across various MAT series because the criteria for failure are controversial; multiple criteria are used, including knee replacement, graft removal, poor clinical outcomes, and magnetic resonance imaging (MRI) evidence of graft tears.12,19,25,30
Another strength of the present series is the inclusion of a heterogeneous population of patients regarding age, graft side, cartilage status, and presence of concurrent procedures that closely resembles the common clinical practice; in fact, no particular exclusion criteria were applied for this study. This, coupled with a large number of patients, allowed a solid statistical analysis aimed at detecting predictors of failures. Interestingly, multivariate analysis did not reveal age to be a significant factor with regard to failure, whereas the main factor correlated with the worst results was the need for a concurrent cartilage procedure. The threshold of cartilage degeneration allowed for MAT is still controversial, even though the worst outcomes have been reported in cases of advanced chondropathy.
Saltzman et al 23 did not report significant differences between MAT full-thickness cartilage lesions and those with no chondral defects. In contrast, Kempshall et al 11 reported a higher failure rate in patients with advanced chondral damage. Interestingly, in the present study, the degree of chondral damage did not seem to affect the rate of surgical or clinical failure, whereas a concurrent cartilage procedure did. This could be because we used a high threshold for cartilage treatment, and only the more severe, grade 4 lesions were managed operatively. Of note, the failure rate of patients who underwent a concurrent cartilage procedure was nearly double compared with patients who had diffused mild or moderate chondromalacia of the affected compartment not amenable for a focal treatment. The results of our study appear different from a previously reported investigation, 23 in which procedures such as osteochondral allografts, microfractures, autologous chondrocyte implantation, and mosaicplasty appeared effective to guarantee clinical outcomes similar to cases with intact cartilage. However, that research had a follow-up of <4 years, whereas the present study showed an abrupt decrease of surgical success at 5 years and beyond, according to survival analysis and Kaplan-Meier curves. Thus, based on these findings, it could be hypothesized that combined MAT and cartilage procedures can be effective at midterm, whereas outcomes tend to decline with time more rapidly with respect to isolated MAT.
The higher failure rate in female patients is another interesting finding. A similar result was reported by Frank et al, 7 who demonstrated that female patients were more likely to undergo revision surgery than male patients. Unfortunately, in both the Frank et al study and our study, the causes of such disparity were not characterized, which should be investigated in future studies in order to confirm the finding that female patients experience a higher rate of failure.
The present study has several limitations. It is a retrospective study. Moreover, apart from assessing failures and reoperations, we used patient-reported outcome measures (PROMs) as the only subjective evaluation, and the patient’s scores were excluded from the analysis in the presence of a surgical failure. Thus, this approach in the definition of endpoint could have overestimated positive results. However, failure criteria, including low subjective scores, were introduced to mitigate this limitation, as already performed by many authors. 9 Clinical scores collected via telephone interviews could introduce some reporting and recall bias. However, a previous study demonstrated that clinical scores could be reliably collected through telephone interview. 13
Graft removal and PROMs are the most commonly used criteria for failure, given the lack of a universally accepted definition of MAT failure. Graft extrusion and shrinkage are common findings on MRI after MAT, but their clinical relevance seems marginal, and a mismatch between the MRI appearance of a graft and clinical status has already been reported in the literature. 23 Another limitation is that the inclusion criteria allowed a broad spectrum of cartilage degeneration (Kellgren-Lawrence grade 1-3) and many patients underwent associated surgeries combined with MAT, including different cartilage restoration procedures. However, a heterogeneous population with multiple knee comorbidities requiring associated surgeries is a typical patient profile referred to high-level sports medicine centers that perform MAT. 1 Another limitation is related to the surgical procedure, because the present analysis included patients who underwent single-tunnel MAT fixation as well as patients who had double-tunnel MAT fixation. Nevertheless, this study aimed to present the clinical results of a large series of patients who underwent soft tissue fixation, and subsequent analysis revealed no difference in surgical failures between these 2 types of fixations.
Another limitation is that not all patients completed every follow-up assessment; thus, for each time point, PROMs could be evaluated in only in a subset of patients. However, every patient included in the study had PROM evaluation at least at 1 time point, which was used to determine the presence or absence of clinical failure. Moreover, the main purpose of the study was to perform a survival analysis and identify predictors of failure, not to precisely assess the trend in clinical status at each time point. We conducted a broad follow-up, ranging from 2 to 16 years, which prevented us from collecting the 2, 5, 7, and >10-year assessments for all patients, but allowing us to include a vast number of patients.
The lack of objective MRI evaluation leaves some questions unanswered regarding the status of the transplanted meniscus, cartilage wear, and the potential chondroprotective effect of the MAT. The last limitation of the study is related to the assessment of clinical failure in the survivorship analysis. Because of the study protocol, the time of the clinical failure could have been underestimated.
Conclusion
MAT had a surgical failure rate of 7% and a clinical failure rate of 22% at an average follow-up of 5.7 years. Good outcomes were reported for both medial and lateral MAT and for both isolated and combined MAT with an overall survival rate of 90% from surgical failure and 65% from clinical failure at 10 years of follow-up. However, slightly inferior outcomes were reported in female patients and in cases of combined cartilage treatments, especially after 5 years from surgery.
Footnotes
Submitted March 29, 2022; accepted August 29, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.Z. is a consultant for Smith & Nephew and DePuy Synthes. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.