
Abstract
Background:
Anterior cruciate ligament (ACL) reconstructions (ACLRs) with graft diameters <8mm have been shown to have higher revision rates. The 5-strand (5S) hamstring autograft configuration is a proposed option to increase graft diameter.
Purpose:
To investigate the differences in clinical outcomes between 4-strand (4S) and 5S hamstring autografts for ACLR in patients who underwent ACLR alone or concomitantly with a lateral extra-articular tenodesis (LET) procedure.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Data from the STABILITY study were analyzed to compare a subgroup of patients undergoing ACLR alone or with a concomitant LET procedure (ACLR + LET) with a minimum graft diameter of 8mm that had either a 4S or 5S hamstring autograft configuration. The primary outcome was clinical failure, a composite of rotatory laxity and/or graft failure. The secondary outcome measures consisted of 2 patient-reported outcome scores (PROs)—namely, the ACL Quality of Life Questionnaire (ACL-QoL) and the International Knee Documentation Committee (IKDC) score at 24 months postoperatively.
Results:
Of the 618 patients randomized in the STABILITY study, 399 (228 male; 57%) fit the inclusion criteria for this study. Of these, 191 and 208 patients underwent 4S and 5S configurations of hamstring ACLR, respectively, with a minimum graft diameter of 8mm. Both groups had similar characteristics other than differences in anthropometric factors—namely, sex, height, and weight, and Beighton scores. The primary outcomes revealed no difference between the 2 groups in rotatory stability (odds ratio [OR], 1.19; 95% CI, 0.77-1.84; P = .42) or graft failure (OR, 1.13; 95% CI, 0.51-2.50; P = .76). There was no significant difference between the groups in Lachman (P = .46) and pivot-shift (P = .53) test results at 24 months postoperatively. The secondary outcomes revealed no differences in the ACL-QoL (P = .67) and IKDC (P = .83) scores between the 2 subgroups.
Conclusion:
At the 24-month follow-up, there were no significant differences in clinical failure rates and PROs in an analysis of patients with 4S and 5S hamstring autografts of ≥8mm diameter for ACLR or ACLR + LET. The 5S hamstring graft configuration is a viable option to produce larger-diameter ACL grafts.
Keywords
Hamstring autografts are widely used for anterior cruciate ligament (ACL) reconstructions (ACLRs). A recent systematic review has shown comparable outcomes and failures with bone–patellar tendon–bone autografts when using independent femoral tunnel drilling techniques. 5
The 4-strand (4S) hamstring autograft comprising doubled semitendinosus and gracilis tendons is the most frequently used hamstring autograft configuration. 20 Mean graft diameter in this configuration is variable, 17 and the predictability of hamstring tendon diameter12,13,33 and length9,14 has been researched to aid in surgical planning for graft preparation. Magnussen et al 20 have suggested that the use of hamstring autografts of an ≤8mm diameter in patients <20 years is associated with higher revision rates after ACLR. Many studies have correlated larger graft sizes with better patient outcomes and smaller graft sizes with increased failure.6,22,26,31 However, obtaining a graft size with a ≥8mm diameter can be challenging, especially in patients with a shorter stature and female patients. 6
The 5-strand (5S) hamstring autograft configuration has been suggested as a mechanism to increase overall graft diameter.3,17-19 This configuration is obtained by tripling the semitendinosus tendon alongside a doubled gracilis tendon. In doing so routinely, Krishna et al 17 have demonstrated achieving graft sizes >8mm in 75% of patients.
Equally important to graft choice is restoring a rotationally stable knee, a goal that conventional ACLR was unable to achieve as consistently as desired, thus renewing an interest in the anterolateral ligament (ALL). Historical procedures focused on anterolateral capsular reconstruction to address ACL-deficient knees with lateral extra-articular tenodesis (LET), which is similar to the ALL in function with some anatomic differences.10,29 Cadaveric studies have supported augmentation of ACLR with an extra-articular reconstruction when both the ACL and ALL are sectioned, and furthermore, the addition of LET has outperformed an ALL reconstruction biomechanically. 32 A meta-analysis performed by Hewison et al 10 found that combining an ACLR with an LET procedure significantly reduced rotational laxity. Getgood et al 8 recently published the STABILITY study, concluding that the addition of LET to hamstring autograft ACLR reduced graft rupture and rotatory laxity at 2 years postoperatively in young patients at high risk of failure.
The purpose of this study was to perform a subgroup analysis of the STABILITY study cohort to compare the efficacy of 4S and 5S hamstring autograft configurations for ACLR in patients who underwent ACLR alone or concomitantly had an LET procedure performed. We hypothesized that there would be no difference in outcomes with respect to graft rupture, rotatory laxity, and patient-reported outcome scores (PROs) between 4S and 5S autografts ≥8mm in diameter.
Methods
This study was a post hoc subgroup analysis of the data collected in the STABILITY study, which was a pragmatic, parallel-groups, multicenter, randomized clinical trial comparing ACLR alone versus ACLR with LET (ACLR + LET). 8 The patients in the study had a higher than normal risk of graft failure.7,8 The inclusion criteria for this subgroup analysis were patients undergoing either an ACLR or an ACLR + LET who had a graft diameter of ≥8mm and had one of the configurations (either 4S or 5S) for a hamstring autograft. We excluded patients with grafts <8mm and any other configurations of hamstring autograft (such as 6-strand).
The detailed method has been previously published.7,8 All patients underwent an anatomic ACLR in a standardized fashion using hamstring autograft. The standard method was using a 4S configuration unless the graft diameter was <8mm, in which case the semitendinosus was tripled and sutured to itself to create the 5S configuration and increase the graft diameter. The maximum final graft diameter was recorded. Femoral tunnels were drilled using an anatomic transportal drilling technique. Femoral fixation was performed with cortical suspensory fixation (Endobutton CL, Smith & Nephew; Exobutton, Conmed), and tibial fixation was performed with an interference screw with or without a backup screw/staple. Of the patients who were randomized to the LET, the modified Lemaire technique was used.7,8,23 This was a standardized technique across all clinical sites.
Outcome Measures
Similar to the original STABILITY study, the primary outcome was defined as ACLR clinical failure. This was a composite of 3 scenarios: persistent (detected at ≥2 visits) mild asymmetric pivot shift (grade 1), a moderate or severe (grade 2 or 3) asymmetric pivot shift at any follow-up visit, or a graft rupture confirmed as a tear of the graft on magnetic resonance imaging or arthroscopic examination. Hence, the primary outcome was a combination of rotatory stability and graft integrity. For the purposes of this subgroup analysis, patient evaluations at 24 months postoperatively were used for outcome measures.
The secondary outcome measures consisted of PROs, including the ACL Quality of Life Questionnaire (ACL-QoL) and International Knee Documentation Committee (IKDC) subjective score. The ACL-QoL score consists of 5 domains relating to physical symptoms and complaints, work-related concerns, recreational activities and sports participation or competition, lifestyle, and social and emotional well-being. The responses are recorded on a 100-mm visual analog scale, and a total average score out of 100% is calculated. 25 The subjective IKDC score is composed of 18 items containing questions about symptoms, function, and sports activities with responses in Likert scales and dichotomies. 11
Statistical Analysis
Patient characteristics, recorded in Table 1, were stratified by 4S and 5S with an ≥8mm graft diameter and by ACLR alone and ACLR + LET groups, using means, standard deviations, and counts. Five univariate binary logistic regression models were used to assess the association between the primary outcome and the use of 5S versus 4S graft configurations. The associations between clinical stability (0 = stable or 1 = failure) and the use of 4S versus 5S grafts with a minimum 8mm diameter were examined in the following:
Patients undergoing ACLR
Patients undergoing ACLR + LET
All patients (ACLR and ACLR + LET)
Characteristics of Patients With 4-Strand and 5-Strand Hamstring Autografts a
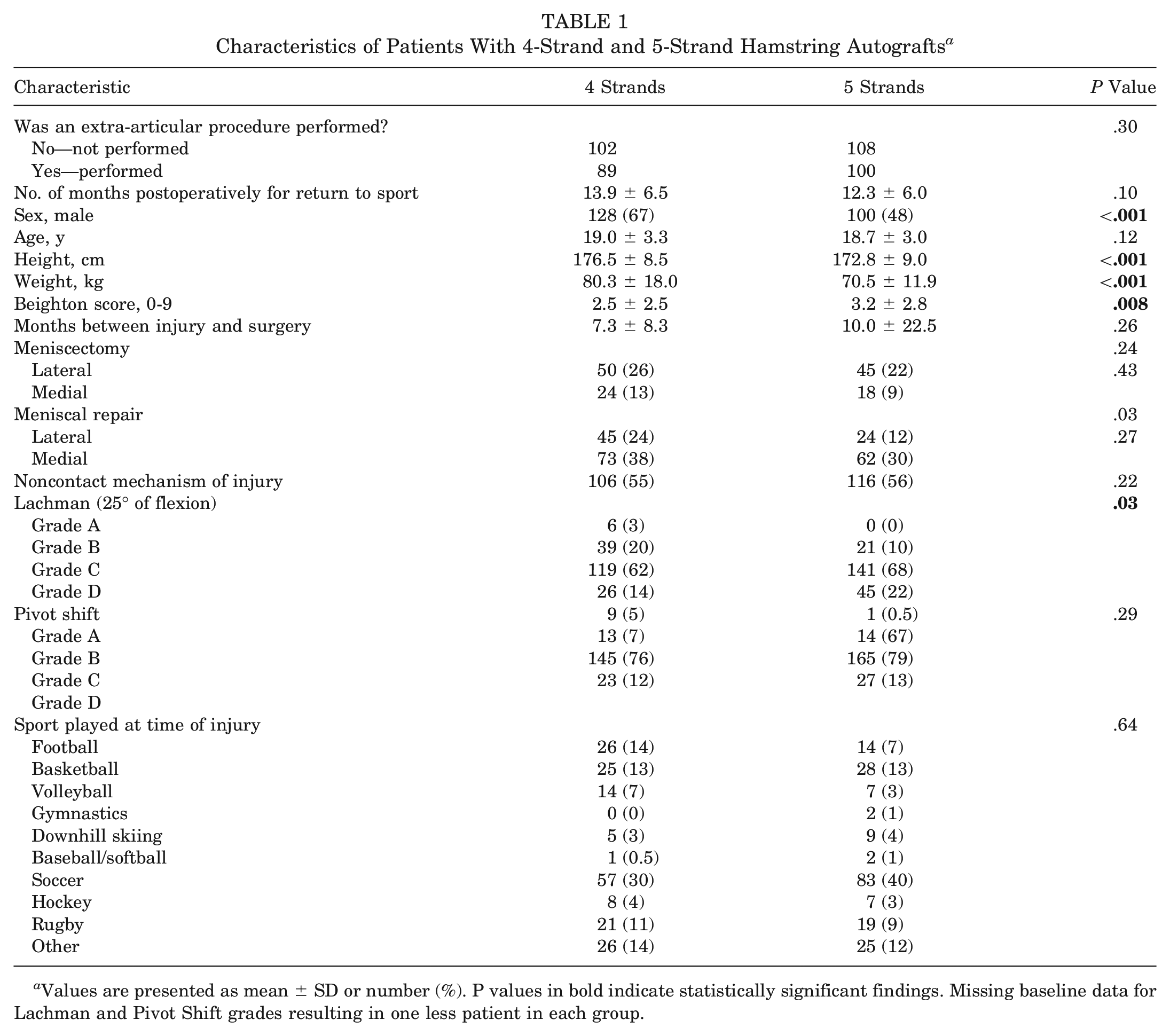
Values are presented as mean ± SD or number (%). P values in bold indicate statistically significant findings. Missing baseline data for Lachman and Pivot Shift grades resulting in one less patient in each group.
The process was repeated for graft integrity (0 = intact or 1 = rupture). All P values were 2-tailed, and significance was defined as P < .05. Analyses were performed in SPSS Version 26 for Windows (SPSS, Inc).
The measures of clinical stability were evaluated at the 24-month (final) follow-up for all (ACLR and ACLR + LET) patients and compared between the 4S and 5S groups using 2 binary logistic regression analyses to assess the following:
Association between the Lachman grades (A vs B, C, D) and the graft configuration (4S vs 5S)
Association between the pivot-shift grades (A vs B, C, D) and the graft configuration (4S vs 5S)
In addition, the means, standard deviations, and levels of statistical significance (P value) of the 2 PROs (ACL-QoL and IKDC) at the 24-month follow-up for all patients (ACLR and ACLR + LET) were calculated.
Results
Patient Characteristics
Table 1 displays the patient characteristics stratified by 4S and 5S hamstring autograft configuration. Of the 618 patients randomized in the STABILITY study, 399 (228 male; 57%) fit the inclusion criteria for this study (Figure 1). There were 191 (128 male; 67%) and 208 (100 male; 48%) patients in the 4S and 5S groups, respectively. The 5S subgroup had significantly (P < .001) fewer male patients compared with the 4S subgroup. In addition, the 5S subgroup of patients had shorter height (P < .001) and lower weight (P < .001), delineating the importance of these anthropometric factors in predicting the likelihood of smaller-diameter hamstring tendons and thereby a need for 5S grafts to obtain graft diameters of ≥8mm. The mean Beighton score was significantly higher (P = .008) in the 5S subgroup compared with the 4S subgroup. The grades of Lachman test were significantly higher (P = .03) in the 5S subgroup compared with the 4S subgroup at baseline.
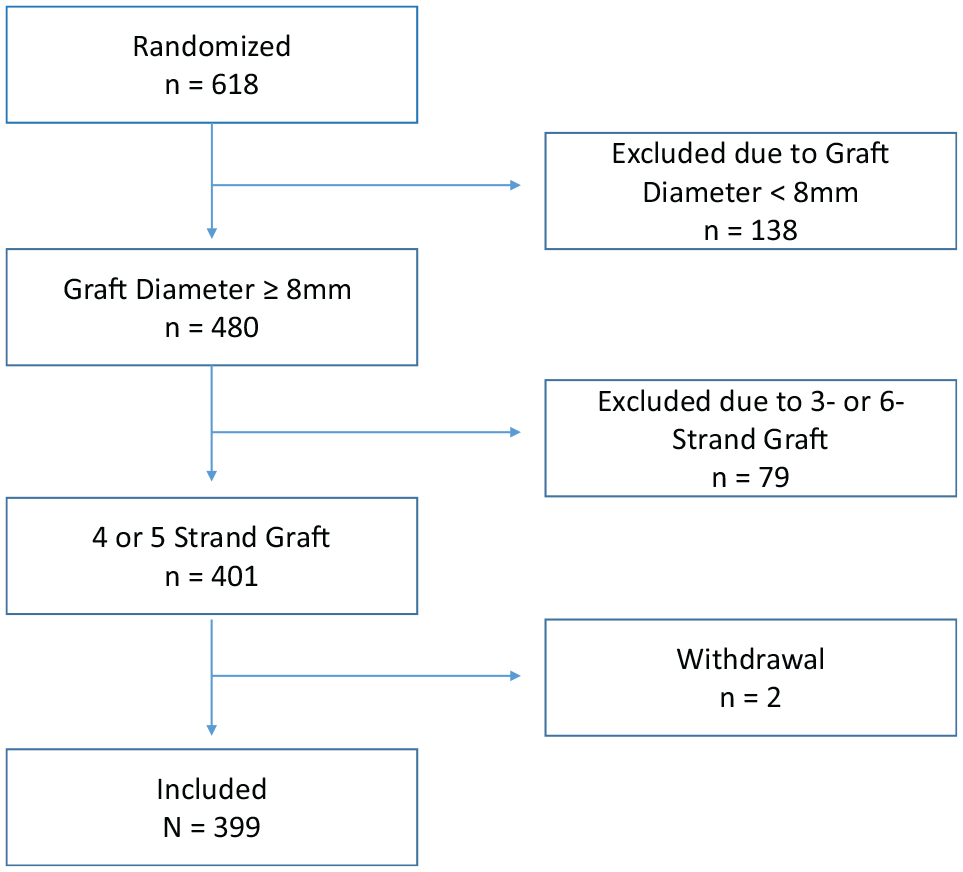
Flowchart demonstrating the inclusion and exclusion criteria.
Table 2 further stratifies the patient characteristics based on ACLR and ACLR + LET, with the same trends as Table 1.
Patient Characteristics With 4 and 5 Strands Separated by ACLR vs ACLR + LET Groups a
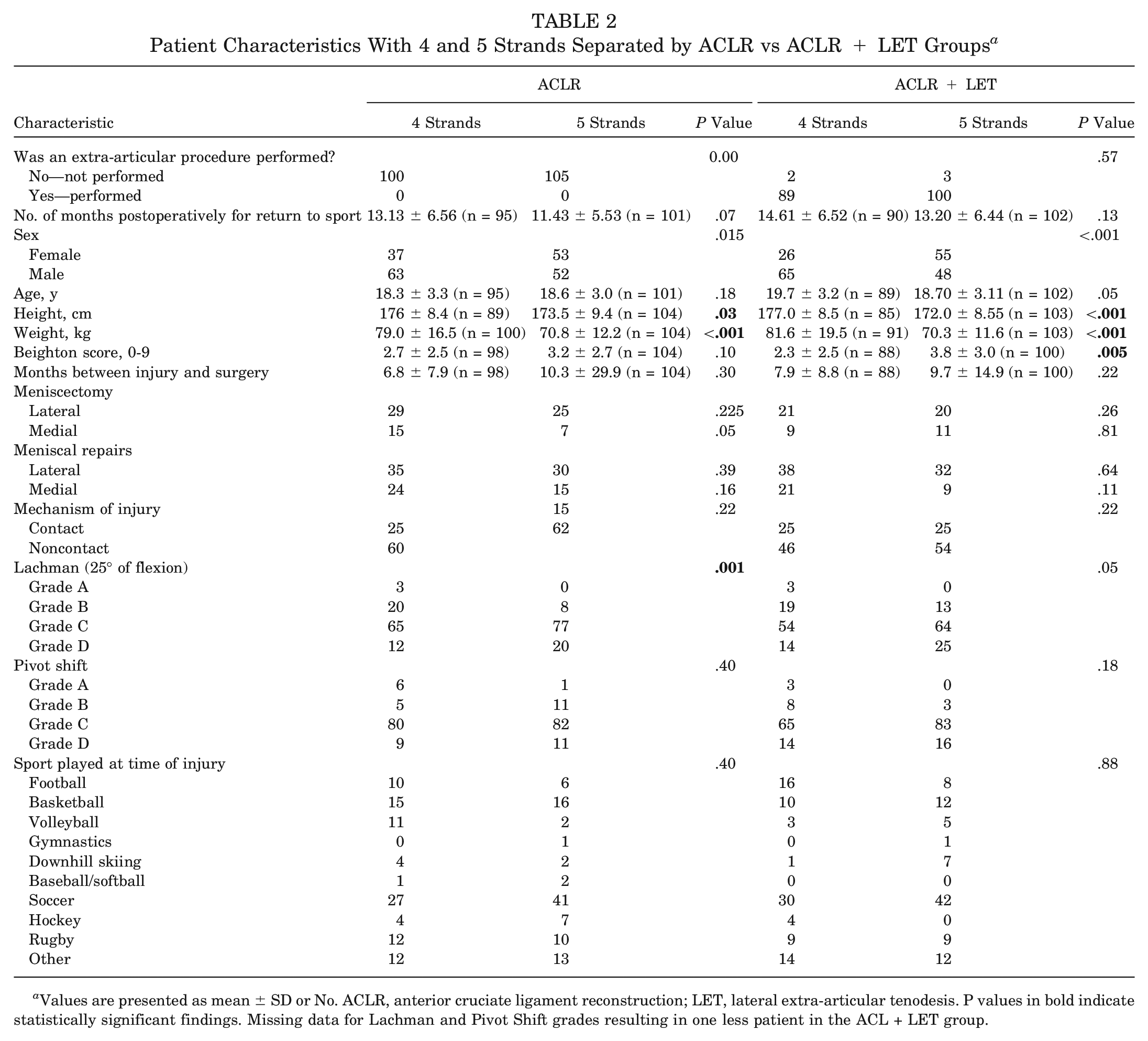
Values are presented as mean ± SD or No. ACLR, anterior cruciate ligament reconstruction; LET, lateral extra-articular tenodesis. P values in bold indicate statistically significant findings. Missing data for Lachman and Pivot Shift grades resulting in one less patient in the ACL + LET group.
Table 3 displays the association between the primary outcome and the use of 4S versus 5S and the groups. There were no associations between the primary outcome in terms of rotatory stability (0 = stable or 1 = failure) and the use of 4S versus 5S in patients undergoing ACLR alone (P = .84), in patients undergoing ACLR with the addition of LET (P = .10), or in all combined patients (P = .42).
Association of Primary Outcomes to 5-Strand vs 4-Strand Hamstring Grafts a
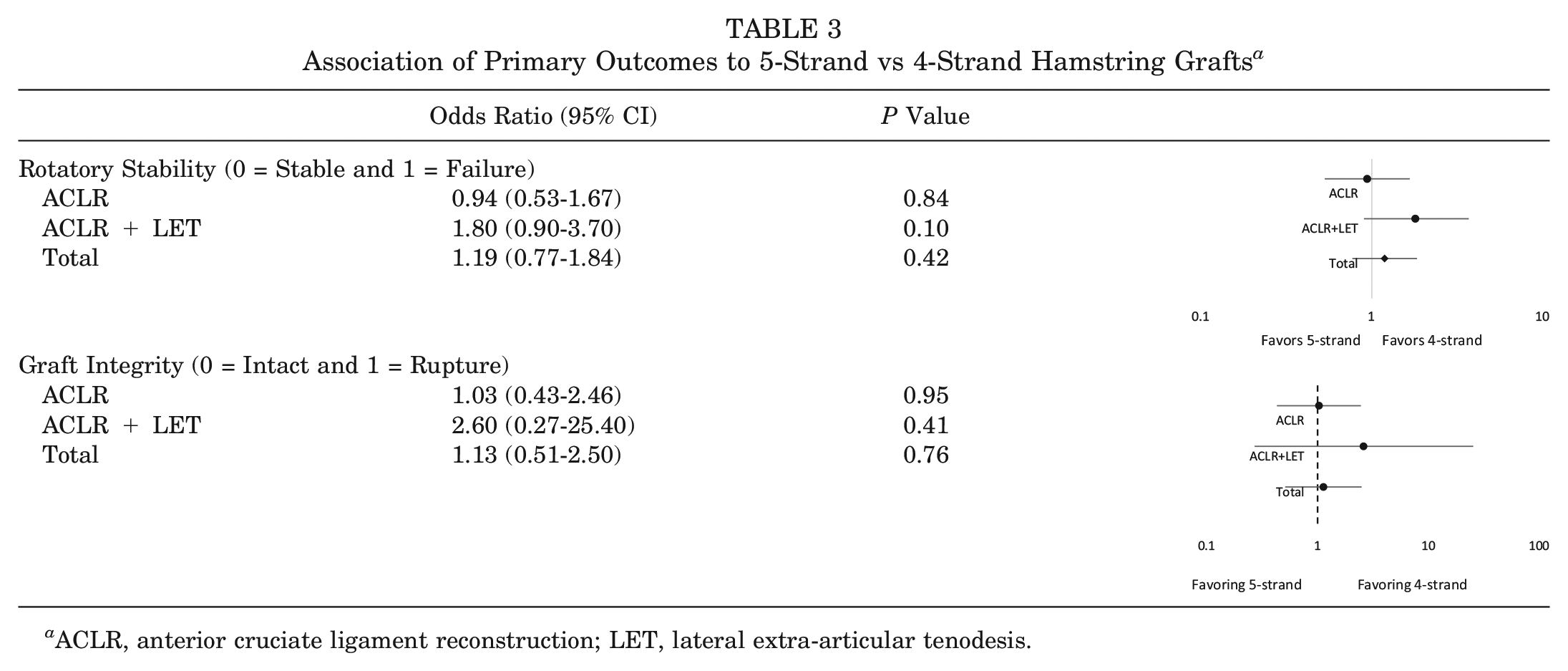
ACLR, anterior cruciate ligament reconstruction; LET, lateral extra-articular tenodesis.
Similarly, there were no associations between the graft integrity (0 = intact or 1 = rupture) and the use of 4S versus 5S grafts in patients undergoing ACLR alone (P = .95), in patients undergoing ACLR with the addition of LET (P = .41), or in all combined patients (P = .76).
When examining the physical examination differences between the use of 4S and 5S autografts in all patients, there was no statistically significant difference for the Lachman (P = .46) and pivot-shift (P = .53) tests (Table 4).
Lachman and Pivot-Shift Tests at 24-Month Follow-up for All Patients Undergoing 4-Strand and 5- Strand Hamstring ACLR With and Without LET a
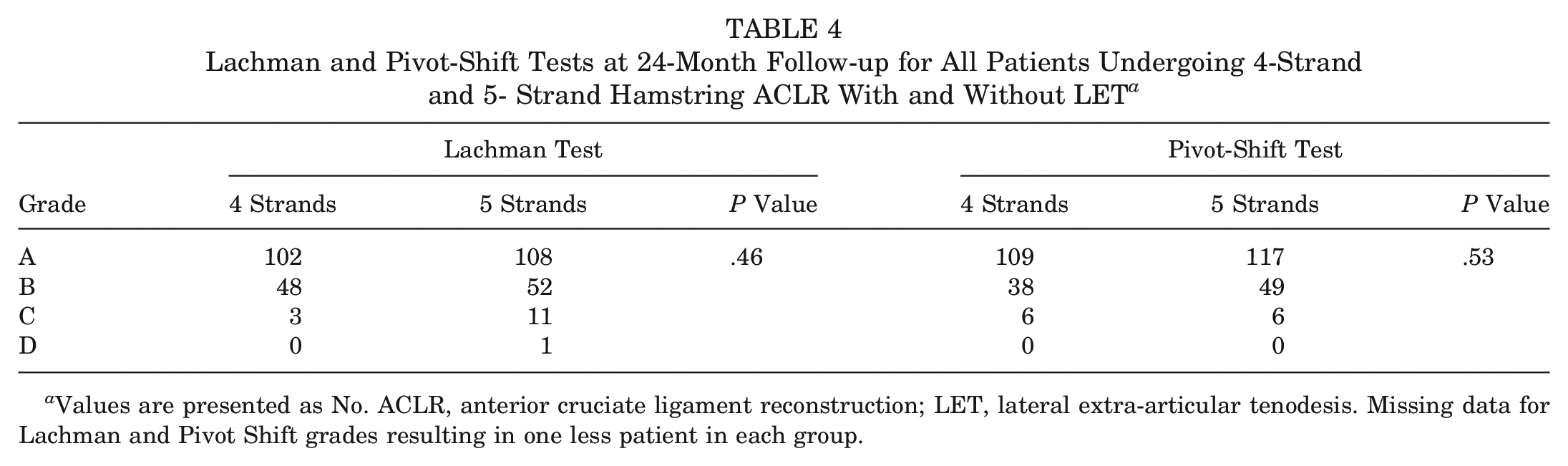
Values are presented as No. ACLR, anterior cruciate ligament reconstruction; LET, lateral extra-articular tenodesis. Missing data for Lachman and Pivot Shift grades resulting in one less patient in each group.
The secondary outcome measures were evaluated in terms of PROs at 24-month follow-up (Table 5). There were no statistically significant differences between all patients with 4S and 5S autografts for ACL-QoL (P = .67) and IKDC (P = .83) scores.
Association of Secondary Outcomes to 5-Strand and 4-Strand Hamstring Grafts at 24-Month Follow-up a
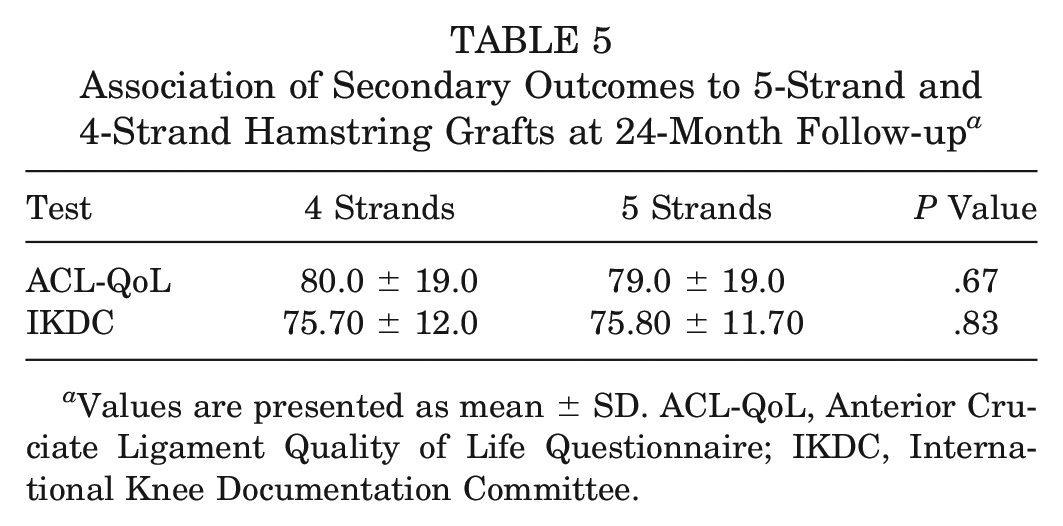
Values are presented as mean ± SD. ACL-QoL, Anterior Cruciate Ligament Quality of Life Questionnaire; IKDC, International Knee Documentation Committee.
Discussion
The most important question this study sought to answer was whether 5S hamstring graft configuration works as well as a 4S configuration of the same diameter. The most important finding of this study was that there was no difference between patients in the 4S and 5S groups with or without LET with respect to rotatory stability, graft integrity, or PROs at 24-month follow-up. Patients requiring 5S hamstring autografts to achieve an ≥8mm graft diameter for ACLR were more likely to be female, have a shorter stature and weigh less, and have a higher Beighton score compared with those with 4S autografts. While this difference was statistically significant, <1 absolute point on the Beighton score may be questionable for its clinical significance, particularly when it has been shown to have moderate intra- and interexaminer reliability. 21 Furthermore, the Lachman test at baseline differed significantly between the 4S and 5S groups. Despite the differences at baseline (favoring the 4S group), there was no difference between the 4S and 5S groups with respect to rotatory stability, graft integrity, or PROs at 24-month follow-up.
Prodromos and Joyce 28 first reported the technique and long-term outcomes of 5S hamstring autograft for ACLR. They reported that patients with 5S autografts had better stability based on KT-1000 arthrometer side-to-side testing when comparing 18 consecutive patients undergoing 5S hamstring ACLR to 133 patients treated with 4S hamstring ACLR. However, the predominant need to consider the 5S graft configuration became more apparent in the past decade, as studies have shown an effect of graft size on outcomes of ACLRs.6,20,22,26,31 There is also an increased failure of ACLR in select populations with allograft augmentation of hamstring grafts to upsize the autograft intraoperatively. 27 Biomechanically, increased tensile strength has been reported with increasing hamstring graft diameter in human cadaveric specimens. 1 However, no statistically significant differences have been identified between 4S and 5S configurations with respect to mean failure load, stress relaxation, stiffness, and graft displacement in ovine and human cadaveric models.2,34
Krishna et al 17 recently published a randomized control trial (RCT) comparing 32 patients with 4S and 32 patients with 5S hamstring autograft ACLRs. The authors showed a mean 1.4-mm increase in graft diameter with the 5S configuration compared with 4S. Interestingly, 75% of patients in the 5S group exceeded the 8mm graft diameter compared with only 28% in the 4S group. In a follow-up study by Krishna et al, 16 the authors followed patients in the original RCT and found no difference except Knee injury and Osteoarthritis Outcome Score Symptoms score between the 4S and 5S groups. All other PROs (Lysholm knee score, IKDC subjective knee score, 36-Item Short Form Health Survey, and Tegner Activity Scale), objective tests (KT-2000 measurements, Lachman test, pivot-shift test, and hop test), and rerupture rates showed no statistically significant difference between the 2 groups. The results of our study concur with these findings. While the current study did not record the size of the 4S configuration before modifying it to 5S to understand the increase in size that the 5S configuration provides, the authors’ experiences show it tends to be a 1-mm increase in diameter from 4S to 5S constructs.
Sideris et al 30 recently published their experience with the 4S and 5S graft configurations in 18 and 10 patients, respectively. The authors found a greater decrease in side-to-side difference in the 4S group at 6 weeks and a greater increase in laxity in the 5S group at 12 weeks, concluding that there was no benefit to using a 5S group compared with the 4S group. These findings contrast with our study, which showed no statistically significant differences in Lachman or pivot-shift testing between the groups at 2 years postoperatively. However, their small sample size limits interpretation and is inconsistent with the rest of the literature. Our study was significantly larger (399 vs 28 patients).
Finally, sex-based and anthropometric differences between patients and their effect on ACL injuries and prediction of hamstring graft size for ACLR are important to consider when planning for surgery. Chandrashekar et al 4 performed a cadaveric study revealing that the ACL in female patients was smaller in length, cross-sectional area, volume, and mass but not different in mass density compared with that in their male counterparts. The authors postulated the smaller size may contribute to the higher rate of ACL injuries in female patients. Moghamis et al 24 studied the effect of anthropometric factors on hamstring graft size in ACLR in male patients and identified a positive correlation between patient height and thigh length with gracilis and semitendinosus graft length. This study, along with others,9,12 demonstrated the importance of anthropometric factors in predicting hamstring graft sizes. Furthermore, a minimum length of 240 mm of semitendinosus and 160 mm of the gracilis tendon is required to prepare the 5S configuration. 17 Ilahi et al 15 noted that abnormally distal musculotendinous junctions of hamstring tendons can cause shorter grafts in the absence of technical error and affect the ability to employ a particular graft preparation technique, thus increasing uncertainty of graft utilization. Our study showed a preponderance of female patients and those of shorter stature and with lower weight undergoing the 5S graft configuration. The 5S configuration still compensated for the negative risk factors that face patients who otherwise may have had an inferior outcome with a 4S graft, which would have been a smaller-diameter graft. Anthropometric factors such as the higher Beighton score, sex, height, and weight could have been negative risk factors but still showed comparable outcomes with patients with the 4S graft, who may not have been faced with those factors. These findings further strengthen the need to consider patient sex and anthropometric factors when planning for ACLR, as some patients may require the surgeon to be proficient in 5S graft configuration if hamstring autograft is chosen.
There are several limitations in this study. First, this is a post hoc subgroup analysis of the STABILITY study and hence was not adequately powered to analyze differences between 4S and 5S hamstring autograft ACLR. As such, these findings are at a higher risk of being inaccurate. The STABILITY study was predominantly powered for detecting differences between patients randomized to ACLR with concurrent LET or ACLR alone with hamstring autograft. However, its large number of participants allowed the sample size of 4S (191 patients) and 5S (208 patients) graft configurations to be larger than other studies reporting on the same concept and perhaps may carry some scientific rigor nonetheless. Second, there was no randomization based on graft configuration, as the purpose was to see if the modification in graft preparation could mitigate the risks of failure in a smaller-diameter graft. Third, patients with grafts that were <8mm diameter after graft preparation were excluded. Any differences between patients with 4S and 5S graft configurations when the graft is <8mm remain unknown. In addition, whether patients with a graft <8mm benefit from the addition of LET or not also remains unknown. Fourth, the increase in size from 4S to 5S was not recorded at the time of the STABILITY study. This makes it difficult to predict the augmentation effect of the 5S configuration in these patients. Finally, the comparison in this study is between 4S and 5S hamstring ACLR of similar diameters. Therefore, while the results show no difference between 4S and 5S configurations for ACLR, they may not accurately depict any advantage a 5S graft of higher diameter may have in a patient whose tendons, if used in a 4S configuration, would have yielded a graft <8mm. The choice of converting a hamstring autograft from a 4S to 5S configuration is made primarily because the 4S graft configuration in a particular patient is <8mm. Hence, a pragmatic comparison would have been between 5S grafts ≥8mm and 4S grafts <8mm to replicate a common clinical scenario that surgeons are faced with when deciding to use a 5S configuration. Based on our results, it appears that once a 5S graft reaches an 8mm diameter, it clinically behaves similar to a 4S graft of the same diameter. These findings may be limited to the graft fixation and tunnel creation techniques used in this investigation. Investigating the effects of surgical technique on results is beyond the scope of this study.
Conclusion
There were no significant differences in clinical failure and PROs in an analysis of patients with 4S and 5S hamstring autografts of ≥8mm diameter for ACLR or ACLR + LET at a 24-month follow-up. The 5S hamstring graft configuration is a viable option to produce larger-diameter ACL grafts.
Authors
Parth Lodhia, MD (University of British Columbia, New Westminster, Canada); Goris Nazari, PhD (Canadian Institutes of Health Research, Ottawa, Ontario, Canada); Dianne Bryant, MSc, PhD (The University of Western Ontario, London, Ontario, Canada); Alan Getgood, MD (Western Ontario University, London, Ontario, Canada); Robert McCormack, MD (University of British Columbia, New Westminster, Canada); and the STABILITY Group (Alan M.J. Getgood, MD, Dianne M. Bryant, MSc, PhD, Robert Litchfield, MD, Kevin Willits, MD, Trevor Birmingham, PhD, Chris Hewison, MD, Andrew D. Firth, MSc, Stacey Wanlin, Ryan Pinto, MSc, Ashley Martindale, MSc, Lindsey O’Neill, MSc, Morgan Jennings, MSc, Michal Daniluk, MSc [London Health Sciences Centre, Western University, Fowler Kennedy Sport Medicine Clinic, London, Canada]; Robert G. McCormack, MD, Dory Boyer, MD, Mauri Zomar, CCRP, Karyn Moon, Raely Moon, Brenda Fan, Bindu Mohan, Kyrsten Payne [Fraser Orthopaedic Institute, New Westminster, Canada]; Mark Heard, MD, Gregory M. Buchko, MD, Laurie A. Hiemstra, MD, PhD, Sarah Kerslake, MSc, Jeremy Tynedal, MPH [Banff Sport Medicine, Banff, Canada]; Peter B. MacDonald, MD, Greg Stranges, MD, Sheila Mcrae, PhD, LeeAnne Gullett, Holly Brown, BHK, Alexandra Legary, Alison Longo, Mat Christian, Celeste Ferguson [Pan Am Clinic, Winnipeg, Canada]; Alex Rezansoff, MD, Nick Mohtadi, MD, Rhamona Barber, Denise Chan, MSc, Caitlin Campbell, Alexandra Garven, BSc, Karen Pulsifer, Michelle Mayer [Sport Medicine Centre, University of Calgary, Calgary, Canada]; Devin Peterson, MD, Nicole Simunovic, MSc, Andrew Duong, MSc, David Robinson, David Levy, Matt Skelly, BSc, Ajaykumar Shanmugaraj, BSc [McMaster University, Hamilton, Canada]; Davide Bardana, MD, Fiona Howells, BPharm, Murray Tough [Queens University, Kingston, Canada]; Tim Spalding, Pete Thompson, Andrew Metcalfe, Laura Asplin, Alisen Dube, Louise Clarkson, Jaclyn Brown, Alison Bolsover, Carolyn Bradshaw, Larissa Belgrove, Francis Milan, Sylvia Turner, Sarah Verdugo, Janet Lowe, Debra Dunne, Kerri McGowan, Charlie-Marie Suddens [University Hospitals Coventry Warwickshire NHS Trust, Coventry, UK]; Peter C.M. Verdonk, MD, PhD, Geert Declerq, MD, Kristien Vuylsteke, Mieke Van Haver [Antwerp Orthopaedic Center, Ghent, Belgium]).
Footnotes
Submitted December 31, 2021; accepted July 28, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.G. has received consulting fees from Smith & Nephew, Ossur, Olympus, Graymont, precision OS, and Xiros Ltd; research support from Smith & Nephew and Ossur; speaking fees from Conmed; and royalties from Smith & Nephew and Graymont. R.M. has received financial support from Canadian Olympic Committee, Canadian Football League, Whitecaps Football Club, BC Lions Football Team, Curling Canada, Softball Canada, and Canadian Premiere League. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.