
Abstract
Background:
While some studies have failed to reveal any significant relationship between magnetic resonance imaging (MRI) grading and return to sports after bone stress injuries, others have reported either a linear or nonlinear relationship.
Purpose:
To evaluate the prognostic value of MRI grading for time to return to sports and rate of return to sports after bone stress injuries.
Study Design:
Systematic review and meta-analysis.
Methods:
A systematic search was performed in PubMed, Web of Science, SPORTDiscus, and Google Scholar. Studies reporting return to sports data after bone stress injuries using MRI grading systems were included in this review. The risk of bias was evaluated using the Quality in Prognosis Studies tool. Meta-analyses were performed to summarize the mean time to return to sports. The Pearson correlation was used to determine the relationship between time to return to sports and MRI grade. A meta-analysis of proportions was conducted to determine the percentage of athletes who successfully returned to sports.
Results:
A total of 16 studies with 560 bone stress injuries met inclusion criteria. Higher MRI-based grading was associated with an increased time to return to sports (P < .00001). Pooled data revealed that higher MRI-based grading correlated with a longer time to return to sports (r = 0.554; P = .001). Combining all anatomic locations, the mean time to return to sports was 41.7 days (95% CI, 30.6-52.9), 70.1 days (95% CI, 46.9-93.3), 84.3 days (95% CI, 59.6-109.1), and 98.5 days (95% CI, 85.5-112.6) for grade 1, 2, 3, and 4 injuries, respectively. Trabecular-rich sites of injury (eg, pelvis, femoral neck, and calcaneus) took longer to heal than cortical-rich sites of injury (eg, tibia, metatarsal, and other long-bone sites of injury). Overall, more than 90% of all athletes successfully returned to sports.
Conclusion:
The findings from this systematic review indicate that MRI grading may offer a prognostic value for time to return to sports after the nonsurgical treatment of bone stress injuries. Both MRI grade and location of injury suggest that individually adapted rehabilitation regimens and therapeutic decisions are required to optimize healing and a safe return to sports.
Keywords
Bone stress injuries are overuse injuries resulting from repetitive loads that exceed bone-loading capacities. 41 These injuries are common and account for up to 20% of all sports injuries.14,15,17,23,54 Although most injuries heal with nonsurgical treatment, bone stress injuries can result in a significant absence from training and competition.2,30,34 Across the types of overuse injuries, bone stress injuries may take the longest time to return to sports. 55
Advances in imaging have suggested that bone stress injuries can be detected more accurately and before the presence of a fracture line.16,29,48,51,61 Magnetic resonance imaging (MRI) is considered the gold standard in the assessment of bone stress injuries.4,19,29,36,61 More than 25 classification systems, including several MRI-based classification systems, have been introduced to differentiate the severity of bone stress injuries. 43 The report by Fredericson et al 16 was among the first to describe an MRI classification system for tibial bone stress injuries. Grade 1 was defined as mild or moderate periosteal edema on T2-weighted images but normal bone marrow on T1 and T2. Grade 2 was defined as moderate to severe periosteal edema on T2 and marrow edema on T2 only. Grade 3 was defined as moderate or severe periosteal edema on T2 as well as marrow edema on T1 and T2. Grade 4 (the highest grade) was defined as moderate or severe periosteal edema on T2 and marrow edema on T1 and T2 with a fracture line present. The Fredericson classification corresponded with clinical features (pain with hop test, percussion, and palpation) and a greater time to return to sports in higher grade injuries. 16 Since then, further MRI grading criteria with a generalization to other skeletal injury sites have been introduced. For instance, modified classification systems were introduced by Arendt et al, 2 Kaeding and Miller, 31 and Nattiv et al. 48 While many classification systems include 4 grades of bone stress injuries, a differentiation between a low- and high-grade injury is commonly seen (in the past, often referred to as “stress reaction” and “stress fracture”).12,50,51 Recognition for the mechanism that causes a bone stress injury suggests that identifying the severity of injury may be used clinically to estimate the time to return to sports. An early report suggested a return to sports in 3 weeks after a grade 1 injury compared with >16 weeks after a grade 4 injury. 3 While some studies failed to reveal any significant relationship between grading and return to sports,4,8,62 other reports suggested a relationship particularly in the prognosis of low-grade bone stress injuries.3,16,29,48 Therefore, the purpose of this systematic review and meta-analysis was to examine whether MRI grading offers a prognostic value in the prediction of the time to return to sports and rate of return to sports after the nonsurgical treatment of bone stress injuries.
Methods
The methodology of this systematic review and meta-analysis followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 45 Before starting the literature search, all authors agreed on a study protocol that was published online (PROSPERO CRD42020168575).
Search Strategy
A systematic search was performed in PubMed, Web of Science, and SPORTDiscus. Studies from the earliest record up to February 25, 2020, were retrieved using the following search terms: (“stress injur*” OR “stress fractur*”) AND (“MRI” OR “magnetic resonance” OR “grading” OR “grade” OR “return to” OR “absence”). In addition, a “cited-by” analysis (forward search) and “reference” analysis (backward search) of all included studies were performed in Google Scholar and Web of Science.
Selection Criteria
To be included in this systematic review, articles needed to compare return to sports data after bone stress injuries of varying degrees of severity as determined by MRI (Appendix 1, available in the online version of this article). All MRI grading scales were eligible in this review. However, only comparable classification systems (grades 1-4; low vs high) were included in the meta-analysis (Figure 1). Additional inclusion criteria were the following: original research; English, German, or Spanish language; recreational athletes, competitive athletes, or military recruits; and nonoperative (nonsurgical) treatment. Exclusion criteria were the following: athletes with chronic underlying health conditions; studies that did not provide data for ≥2 MRI grades; and non–peer reviewed articles, newspapers, opinion pieces, reviews, meta-analyses, case reports, anecdotal studies and case studies with fewer than 10 cases, editorials, commentaries and letters to the editor, conference proceedings/abstracts, and book chapters. Articles were also excluded if the injury was attributed to trauma or occurred outside of movement-related activities.

Magnetic resonance imaging classification systems for bone stress injuries. STIR, short tau inversion recovery.
Study Selection
Two reviewers (T.H., T.R.) independently performed the systematic search. All identified articles were screened by title and abstract. The full texts of the remaining studies were obtained and checked against the selection criteria.
Data Extraction and Synthesis
In addition, 2 reviewers (T.H., K.H.) independently extracted the data of eligible studies. Initial disagreements for inclusion were resolved through a discussion to achieve a consensus. In the event of further disagreements, a third reviewer (A.S.T.) was available to reach a final decision. The following data were extracted: author(s), year of publication, country, study directionality, study design, number of patients/cases (male and female), classification, anatomic location(s), return to sports definition, return to sports time (for each grade), and return to sports rate (for each grade). Whenever possible, the corresponding authors of included studies were requested to provide missing data.
Quality Assessment
The risk of bias was evaluated using the Quality in Prognosis Studies (QUIPS) tool. 24 This tool was developed to assess the risk of bias in prognostic factor studies. It consists of 6 domains: (1) study participation, (2) study attrition, (3) prognostic factor measurement, (4) outcome measurement, (5) study confounding, and (6) statistical analysis and reporting. A study was judged as having a low risk of bias when all domains were rated low (or up to 1 domain rated moderate). A study was judged as having a high risk of bias when ≥1 domains were rated high. All in-between studies were judged as having a moderate risk of bias in accordance with recent recommendations. 21 There were 2 authors (T.H., K.H.) who independently assessed the risk of bias. Initial disagreements for inclusion were resolved through a discussion to achieve a consensus. In the event of further disagreements, a third reviewer (A.S.T.) was available to reach a final decision.
Statistical Analysis
The data from 9 studies were used for meta-analysis.1,2,4,22,34,39,48,50,51 A further 7 studies were included in the systematic review but not meta-analysis, as specific return-to-sports data for each injury grade were missing.8,13,16,37,44,49,62 Meta-analyses were performed to summarize the mean time to return to sports for MRI grades 1 to 4 (7 studies) and to compare low- with high-grade injuries (8 studies). Further, a meta-analysis of proportions was conducted to determine the percentage of athletes who successfully returned to sports (5 studies). Data were entered and analyzed for summary effects using Review Manager 5.4 software (Cochrane Collaboration) and StatsDirect software (StatsDirect). The main outcome was time to return to sports with adjustments for MRI grade (1-4; low vs high). Grading to predict return to sports was divided into trabecular-rich sites of injury (eg, pelvis, femoral neck, and calcaneus) and cortical-rich sites of injury (eg, tibia, metatarsal) whenever possible. Grade 1 and grade 2 were defined as low-grade injuries, and grade 3 and grade 4 were defined as high-grade injuries.12,48 The mean difference and 95% CI for all studies were calculated, and a random-effects model was used. 28 The pooled return to sports rate and 95% CI were calculated for the total cohort. For each outcome, the heterogeneity of results was tested across the studies using the I2 statistic to quantify the degree of heterogeneity. Values of 25%, 50%, and 75% corresponded to predefined limits for low, medium, and high degrees of heterogeneity, respectively. 25 Means and variances that were not provided were estimated by the median, range, and sample size. 26 Finally, the Pearson correlation was used to examine the relationship between time to return to sports and MRI grade using SPSS Statistics 25 for Windows (IBM). A P value <.05 was considered significant.
Results
Literature Search
Initial search terms yielded 2893 potentially relevant articles (PubMed: n = 1259; SPORTDiscus: n = 437; Web of Science: n = 1197). Each was reviewed, and 16 met criteria for inclusion in the qualitative analysis (Figure 2). A forward (“cited-by”) and backward (“reference”) search through Google Scholar and Web of Science yielded 1834 potentially relevant articles, none of which were included for qualitative analysis. Ultimately, 2583 articles were excluded based on titles and abstracts. The full texts of 286 articles were screened.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart. MRI, magnetic resonance imaging.
Study Characteristics
There were 16 studies that reported MRI grading for a total of 560 bone stress injuries. Of the included studies, 14 were retrospective studies, and 2 were prospective studies. While the vast majority of studies were chart reviews (10 studies) or case series (1 study), 4 cohort/follow-up studies (1 prospective cohort study) and 1 cross-sectional study were included. The most common MRI grading system reported was the Arendt classification (7 studies). The Fredericson classification was used by 4 studies. The remaining 5 studies used classification systems other than the ones by Arendt and Fredericson. There were 9 studies that limited their evaluation to one anatomic region (eg, tibia, femoral neck). The characteristics and outcomes of all included studies are listed in Table 1 (see Appendix 2, available online, for extended data).
Characteristics of the Included Studies a

MR, magnetic resonance; N/A, not available; STIR, short tau inversion recovery.
Data are shown as the mean, mean (median), or mean ± SEM (median).
Value indicates approximate data, which may or may not represent the whole cohort.
Discharge rate.
Assessment of Risk of Bias
The QUIPS tool revealed 4, 3, and 9 studies to have a low, moderate, and high risk of bias, respectively (Figure 3). The overall judgment was based on all 6 domains: study participation (low: 13 studies; moderate: 1 study; high: 2 studies), study attrition (low: 5 studies; moderate: 7 studies; high: 4 studies), prognostic factor measurement (low: 11 studies; moderate: 4 studies; high: 1 study), outcome measurement (low: 5 studies; moderate: 9 studies; high: 2 studies), study confounding (low: 3 studies; moderate: 8 studies; high: 5 studies), and statistical analysis and reporting (low: 4 studies; moderate: 7 studies; high: 5 studies).

Assessment of risk of bias.
Time to Return to Sports
A total of 13 of 16 studies supported the hypothesis that MRI-based grading is a prognostic factor for time to return to sports. ¶ Pooled data from 8 studies showed that MRI-based grading correlated with time to return to sports (r = 0.554; P = .001).1,2,4,34,39,48,50,51 The mean time to return to sports was 41.7 days (95% CI, 30.6-52.9), 70.1 days (95% CI, 46.9-93.3), 84.3 days (95% CI, 59.6-109.1), and 98.5 days (95% CI, 85.5-112.6) for grades 1, 2, 3, and 4, respectively (Table 2).
Meta-analysis of Time to Return to Sports per MRI Grade a

Data are shown as the mean ± SEM (in days) unless otherwise indicated. MRI, magnetic resonance imaging.
A similar result was shown for high- versus low-grade injuries. High-grade injuries led to a longer time to return to sports of 24.8 days (95% CI, 12.3-37.2) and 47.6 days (95% CI, 17.8-77.5) for predominantly cortical and predominantly trabecular high-grade injuries, respectively. Combining all anatomic locations, high-grade injuries required a significantly longer time to recover (mean, 29.7 days [95% CI, 41.2-18.3]; P < .00001).
Rate of Return to Sports
A total of 10 of 16 studies reported data on the rate of return to sports. # There were 5 studies that were eligible for the meta-analysis of proportions.1,2,4,39,50 The rates of athletes who returned to sports varied from 61.9% to 100%. In particular, 4 studies reported a 100% rate of return to sports for all MRI grades of injury,1,4,22,50 and 2 studies (participants were military recruits) reported a subset of the population that did not return to their preinjury status.8,51 Specifically, no correlation between injury grade and return to sports was observed by Chalupa et al. 8 In contrast, Rohena-Quinquilla et al 51 reported a significantly higher discharge rate in high-grade femoral neck stress injuries (grade 1: 2.7%; grade 2: 3.7%; grade 3: 10%; grade 4: 38.1%). Among studies that primarily investigated an athletic population, Lee et al 37 reported 1 athlete and Arendt et al 2 reported 2 athletes who were unable to return to sports. Overall, >90% of athletes returned to sports (Figure 4).

Meta-analysis of rate of return to sports.
Discussion
The purpose of this systematic review with meta-analysis was to determine the role of MRI grading to predict return to sports and understand the overall proportion of athletes who are able to continue sports participation. The findings from our review of 16 studies may suggest that MRI grading offers a prognostic value in predicting the time to return to sports after the nonsurgical treatment of bone stress injuries. A greater time to return to sports was seen in higher grades of injury (P < .00001). The bone anatomy and injuries at trabecular-rich sites (eg, pelvis, femoral neck, and calcaneus) took longer to heal than other cortical-rich sites of injury. Overall, most athletes returned to sports (94%) including those with stress fractures (grade 4).
Our findings suggest that MRI grading is important to guide athlete expectations on a typical safe return to sports. These findings are important, given earlier studies proposing that there is insufficient evidence to confirm the prognostic value of MRI grading for return to sports.2,8,12,34,48,50 This suggests that bone stress injuries of different grades should not be considered identical because of their presence in similar anatomic locations. Nevertheless, it should be emphasized that imaging findings should be associated with the clinical signs and symptoms of pain and overuse. Notably, studies have revealed that imaging findings of bone edema, used in the MRI grading scale, have no prognostic significance in asymptomatic patients.5,35,56 Furthermore, the MRI grade of injury is part of many factors that contribute to clinical decision making of when an athlete can return to sports. Freedom from pain 33 is important to consider, and repetitive imaging10,42 may be required.
This review comprises data from 560 bone stress injuries in a variety of anatomic sites. Several studies identify that the anatomic site of injury may influence the rate of healing.6,43,48 Nattiv et al 48 showed a longer time to return to sports after high-grade injuries at trabecular-rich sites compared with cortical-rich sites of injury. This classification is frequently used to distinguish between bone sites thought to have greater trabecular (eg, femoral neck, sacrum, calcaneus) versus cortical bone (eg, femoral shaft, metatarsals, tibia).38,40,48 Classifying bone stress injuries by anatomic location may be important to understand differences in expected times to return to sports and the relative association to impaired bone health. Each bone may include differences in relative components of trabecular and cortical bone that affect the risk for injuries and the rate of healing. Trabecular-rich sites of injury have been associated with a higher risk for low bone mineral density.40,48,58,59 The mechanism for this is unknown but may represent differences in the hormonal sensitivity of bone or potential differences in the biological risk factors for an injury.40,48,59 It was therefore presumed that bone disorders are more severe and more pronounced at predominantly trabecular bone sites.27,48 This is in line with our finding from subgroup analysis that tended to show different healing rates between low- and high-risk injuries in a predominantly cortical versus trabecular bone site. Although not evaluated using statistical measures, this may be because of longer healing times in predominantly trabecular bone sites (Figure 5). An isolated evaluation of each anatomic site was not feasible because of study heterogeneity and the inclusion of rare injury sites. By considering the distribution of anatomic sites included for meta-analysis, this review comprises the best evidence for tibial, metatarsal, and femoral neck bone stress injuries. There is no clear evidence of whether the generalization of our findings to other anatomic sites is possible.
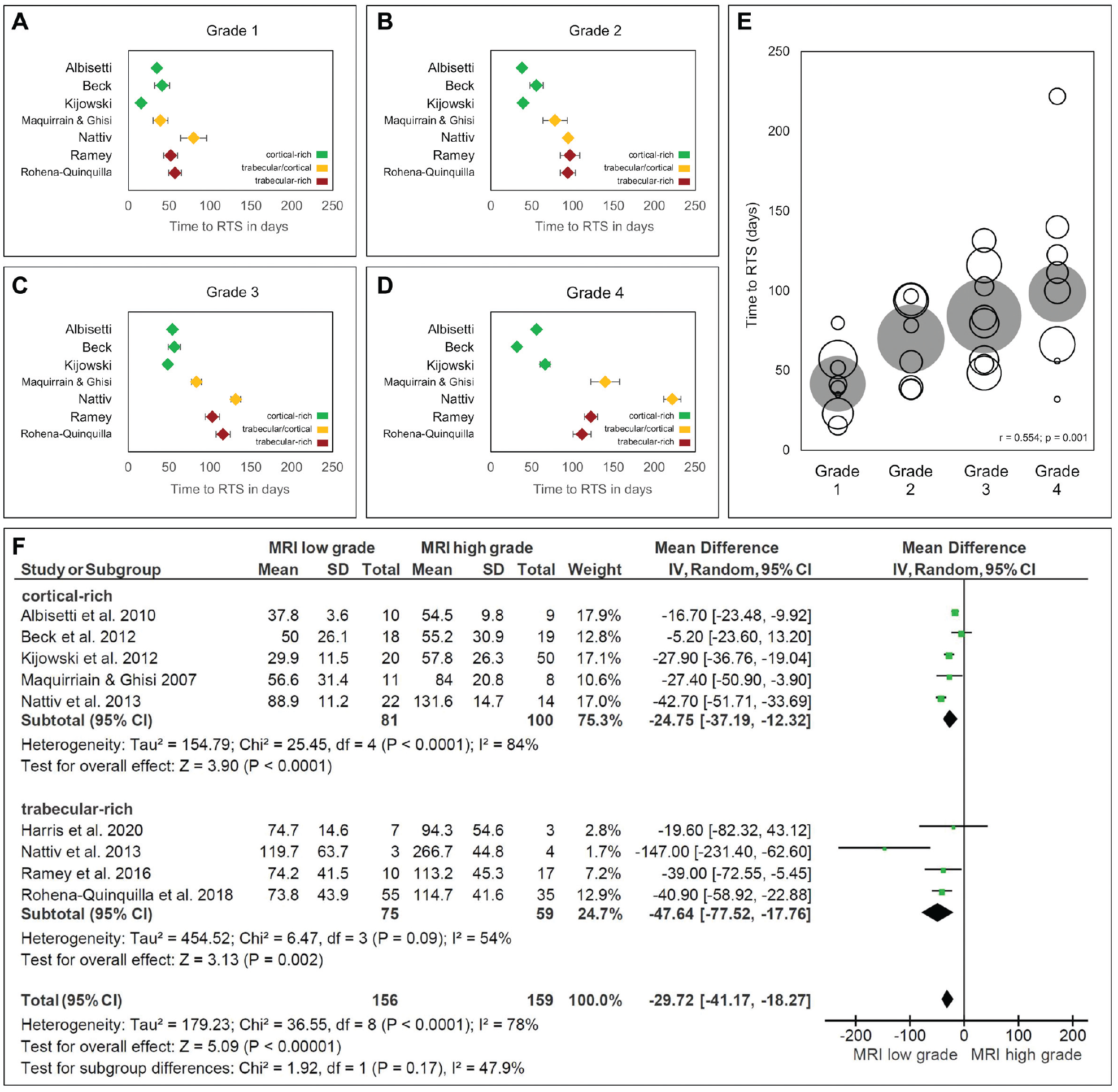
Meta-analysis of time to return to sports. (A-D) Time to return to sports for grades 1 to 4. (E) Pooled data for time to return to sports. (F) Forest plot of differences in means (with 95% CIs) for time to return to sports in patients with low-grade injuries compared with high-grade injuries. IV, inverse variance; MRI, magnetic resonance imaging; RTS, return to sports.
Anatomic location and injury grade are considered the 2 most important factors when planning treatment. 32 Other prognostic factors for return to sports should, however, not be ignored. 48 A multifactorial approach by Nattiv et al 48 proposed that bone mineral density serves as an independent predictor for time to return to sports. Treatment requires addressing aspects of nutrition including energy availability, as identified in the female athlete triad and the relative energy deficiency in sport model.11,47,57 Further, impaired calcium homeostasis due to vitamin D deficiency is known to be associated with bone quality 52 and the occurrence of bone stress injuries. 9 Other aspects of treatment including medications, ultrasound, and electromagnetic field stimulation have been proposed to each influence time to return to sports.7,20,53
Our findings suggest that identifying bone stress injuries by early MRI grading may reduce the time to return to sports. A well-established fact is that early presentation and low-grade bone stress injuries are often missed on plain radiographs.48,49,61 Bone scintigraphy, computed tomography and ultrasonography may also be used to identify bone stress injuries, but major limitations apply to each (eg, ionizing radiation and/or limited probability of detection).4,18,19,46 Providing a sensitivity of 68% to 100% and a specificity of 84% to 100%, MRI is usually considered the method of choice for the diagnosis of bone stress injuries.3,13,46,61 Studies included in this systematic review used several different MRI classification systems based on T1-weighted, T2-weighted, and short tau inversion recovery images. In this review, the most common classification systems were those proposed by Arendt and Fredericson (7 studies and 4 studies, respectively).
Our review suggested that nearly all athletes with bone stress injuries will return to sports. The meta-analysis showed that, with all grades combined, more than 90% of athletes returned to sports. Our findings are consistent with the majority of studies that suggested that a higher grade of injury may have a slightly lower rate of return to sports.2,39,51 One study in skeletally immature patients showed the opposite association. 49 The study demographics may limit understanding the factors that contribute to this association, such as young athletes choosing a different sport after sustaining a bone stress injury. In accordance with previous statements,8,12,34,48,50 this review identifies gaps in knowledge and the need for prospective research.
Strengths and Limitations
The strengths of this systematic review and meta-analysis include the broad scope of review of MRI grading and bone stress injuries in different athlete populations and separated by anatomy. Although the number of studies included in the meta-analysis is limited, the results can be considered valid. 60 Further limitations of this review should be noted. First, a high proportion of studies had a moderate or high risk of bias (75%). In particular, statistical analysis and reporting as well as study confounding were judged inappropriate in 12 studies (5 high, 7 moderate) and 13 studies (5 high, 8 moderate), respectively. Moreover, 11 studies provided insufficient data regarding study attrition. This is probably because, in most circumstances, only retrospective studies were available. Another limitation is the heterogeneity across included studies. However, after performing subgroup analysis (trabecular- vs cortical-rich sites of injury), we were able to reduce the heterogeneity among the studies. It should also be mentioned that, despite a high rate of return to sports, no conclusion can be made regarding postinjury levels of performance. This may be further characterized in future investigations to help advance patient care. The risk of publication bias is another limitation. Furthermore, only studies with comparable MRI grading data were eligible to be included. For instance, data from studies exclusively reporting on return to sports after a stress fracture were excluded from this systematic review. This was done because the aim of this review was to determine the predictive value of MRI grading. However, clinicians seeking to discover the most likely length of time for an athlete to be absent after a bone stress injury should include data from large epidemiological studies in their considerations. This is especially important, as included studies of this systematic review are characterized by nonnegligible variability regarding the study design, participants, anatomic locations, and treatment regimen. Not only for this reason, further investigations on predicting factors other than grading on return to sports are highly recommended.
Conclusion
Our findings indicate that MRI grading may offer a prognostic value in the prediction of return to sports after the nonsurgical treatment of bone stress injuries. These results suggest that bone stress injuries of varying degrees should not be considered identical. Patients need an individually adapted treatment and rehabilitation regimen, and therapeutic decisions ought to be made with consideration given to MRI-based injury severity. A prolonged time to return to sports may be avoided if bone stress injuries are detected early.
Supplemental Material
sj-pdf-1-ajs-10.1177_0363546521993807 – Supplemental material for Does Magnetic Resonance Imaging Grading Correlate With Return to Sports After Bone Stress Injuries? A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-ajs-10.1177_0363546521993807 for Does Magnetic Resonance Imaging Grading Correlate With Return to Sports After Bone Stress Injuries? A Systematic Review and Meta-analysis by Tim Hoenig, Adam S. Tenforde, André Strahl, Tim Rolvien and Karsten Hollander in The American Journal of Sports Medicine
Footnotes
Submitted July 13, 2020; accepted December 12, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.