
Abstract
Background:
Femoroacetabular impingement (FAI) has been extensively investigated and is strongly associated with athletic participation.
Purpose:
To assess (1) the prevalence of cam-type FAI across various sports; (2) whether kinematic variation among sports influences hip morphology; and (3) whether performance level, duration, and frequency of participation or other factors influence hip morphology in a sporting population.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic search of Embase, PubMed, and the Cochrane Library was undertaken following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Prospective and retrospective case series, case reports, and review articles published after 1999 were screened, and those that met the inclusion criteria decided a priori were included for analysis.
Results:
The literature search identified 58 relevant articles involving 5683 participants. A total of 49 articles described a higher prevalence of FAI across various “hip-heavy” sports, including soccer, basketball, baseball, ice hockey, skiing, golf, and ballet. In studies including nonathlete controls, a greater prevalence of FAI was reported in 66.7% of studies (n = 8/12). The highest alpha angle was identified at the 1-o’clock position (n = 9/9) in football, skiing, golf, ice hockey, and basketball. The maximum alpha angle was located in a more lateral position in goalkeepers versus positional players in ice hockey (1 vs 1:45 o’clock). A positive correlation was also identified between the alpha angle and both age and activity level (n = 5/8 and n = 2/3, respectively) and between prevalence of FAI and both age and activity level (n = 2/2 and n = 4/5).
Conclusion:
Hip-heavy sports show an increased prevalence of FAI, with specific sporting activities influencing hip morphology. There is some evidence to suggest that a longer duration and higher level of training also result in an increased prevalence of FAI.
Registration:
CRD4202018001 (PROSPERO).
Femoroacetabular impingement (FAI) is a common cause of intra-articular hip pain and is a precursor to the development of idiopathic osteoarthritis of the hip. 22 There are 3 types of FAI: cam, pincer, and a mixed type with features of cam and pincer. Cam-type FAI describes an abnormality of the femoral head-neck junction with a decreased head-neck offset that generates excess shear forces on the acetabulum. 22 Pincer type is conversely due to acetabular overcoverage, which leads to damage of the labrum secondary to repeated linear contact in hip flexion, thereby leading to calcific changes in the labrum. 22
Cam FAI has an increased prevalence in the athletic population, where repetitive impact and increased stress on the physis may cause the development of abnormal joint morphology. From a young age, the frequency and intensity of training in this population are far greater than in recreational athletes or the general population. 43 High levels of athletic activity at a young age have been proposed to lead to developmental abnormalities in growth from the proximal femoral physis, resulting in the development of cam morphology; it has also been proposed that different movement patterns can lead to sport-specific variations in cam morphology.8,51 Sporting activities can be broadly divided into categories depending on the type of movement, as shown in Table 1. 43
Sports Categories
The aim of this systematic review therefore is to assess (1) the prevalence of cam-type FAI across various sports; (2) whether kinematic variation among sports influences hip morphology; and (3) whether performance level, duration, and frequency of participation or other factors influence hip morphology in a sporting population.
Methods
Our systematic review and meta-analyses were conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The study protocol is registered with PROSPERO (CRD4202018001).
Search Strategy
The search process is displayed in Figure 1 and the search strategy in Appendix A (available in the online version of this article). Inclusion criteria were studies in the English language in which cam FAI was measured via the alpha angle in patients aged ≤30 years and those investigating an association between cam and sporting activities. Articles were excluded if they were nonoriginal, technical notes, editorials, commentaries, or conference abstracts or they were published before 1999. Two reviewers (C.D., M.P.) independently screened titles and abstracts. Full texts were assessed by 3 authors (C.D., M.P., Y.S.). Included articles underwent validity assessment by 3 authors (C.D., M.P., Y.S.) using the appropriate Joanna Briggs Institute critical appraisal checklist. 13 Articles scoring <50% were excluded. Disagreements were settled by majority opinion, and the senior author (V.K.) was involved if a majority opinion could not be reached.
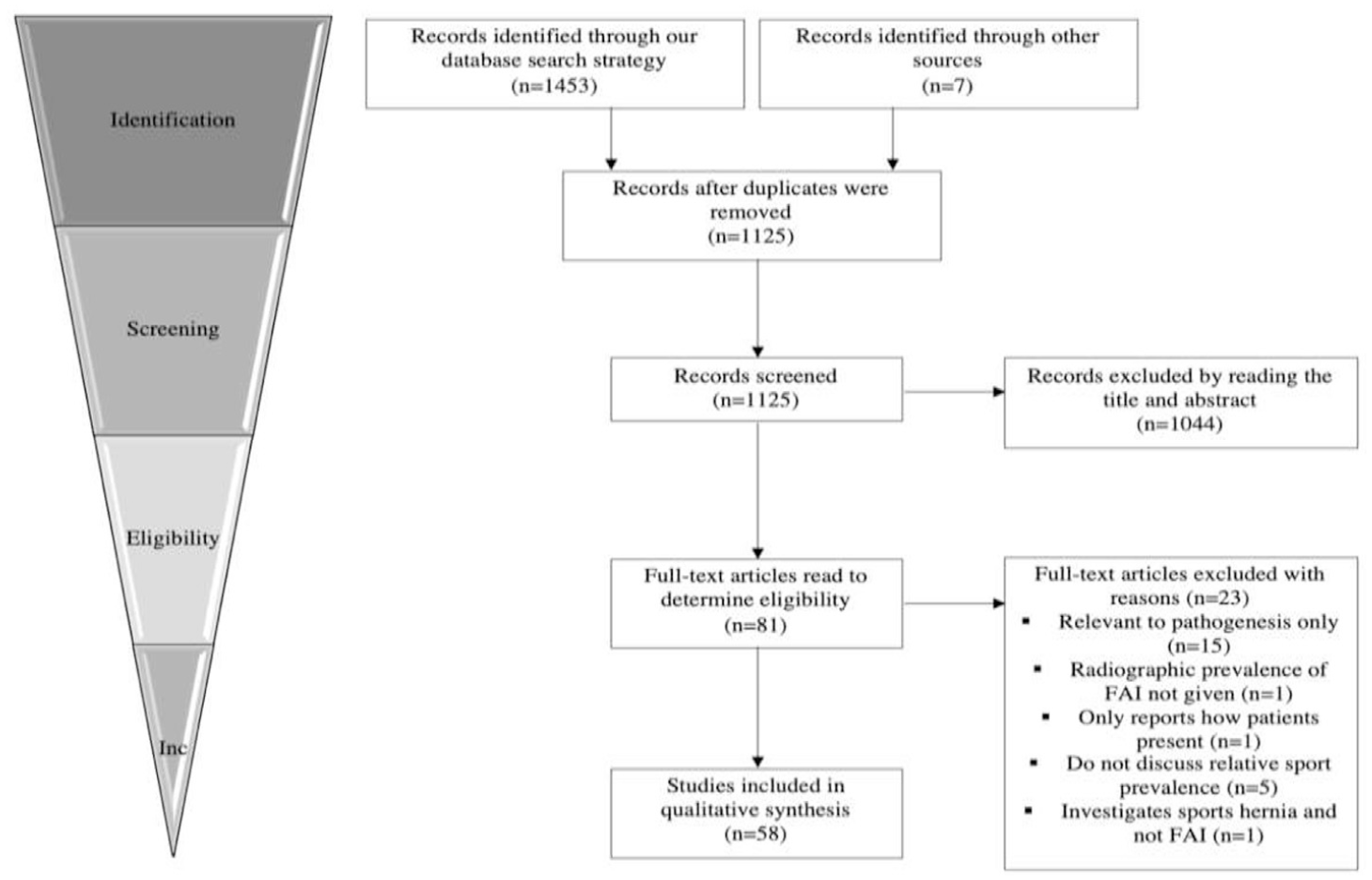
Search process. FAI, femoroacetabular impingement.
Data Analysis
Meta-analyses were performed to compare alpha angle measurements between athletes and controls. In addition, the difference in prevalence of FAI across various sports, training durations, and frequencies was analyzed.
All meta-analyses were conducted using Review Manager 5.3 (Nordic Cochrane Centre; Cochrane Collaboration). Heterogeneity was assessed using the I2 statistic, and random-effects modeling was used for pooling of heterogeneous data. When random effects modeling was employed, weights were assigned using the Mantel-Haenszel method for pooling of prevalence odds ratios and the inverse variance method for standardized mean difference calculations. If studies did not report standard deviation, this was estimated using the formula provided by Higgins et al. 14 Statistical significance was defined by P≤ .05.
For data extraction and quantitative synthesis, (1) if mean alpha angle was not reported, alpha angles in the anterosuperior region or at the 1-o’clock position were used; (2) if open and closed physis groups existed, alpha angles from closed physis groups were used; (3) if standard deviations for right and left hip alpha angles were listed, only right hip values for alpha angle and standard deviation were used to create the forest plots; and (4) lateral view alpha angles were preferable, although anterior-posterior values were used if lateral angles were not listed. The values for epiphyseal extension listed in Table 2 were extracted from the 1-o’clock position since they correlated with alpha angle (P < .001 in the anterosuperior quadrant for all angles and P < .006 for alpha angles >55°). 52
Comparison of Hip Morphologies Reported in Athletes vs Controls a
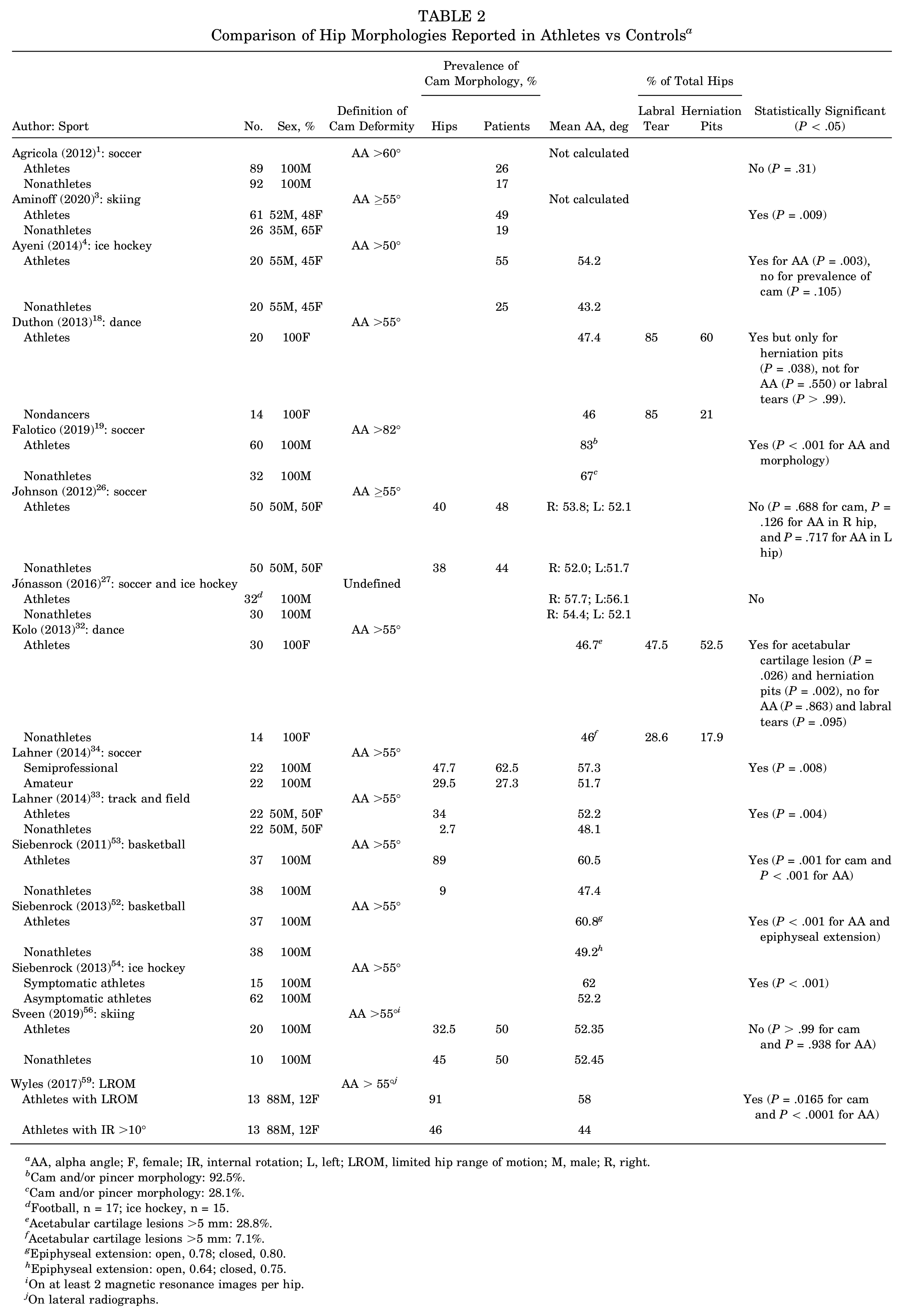
AA, alpha angle; F, female; IR, internal rotation; L, left; LROM, limited hip range of motion; M, male; R, right.
Cam and/or pincer morphology: 92.5%.
Cam and/or pincer morphology: 28.1%.
Football, n = 17; ice hockey, n = 15.
Acetabular cartilage lesions >5 mm: 28.8%.
Acetabular cartilage lesions >5 mm: 7.1%.
Epiphyseal extension: open, 0.78; closed, 0.80.
Epiphyseal extension: open, 0.64; closed, 0.75.
On at least 2 magnetic resonance images per hip.
On lateral radiographs.
Results
The initial literature search identified 1453 studies and 7 through other sources. In total, 58 studies were finally included in the qualitative and quantitative analyses, with 5683 participants (Figure 1).
Prevalence of Cam-Type FAI
A total of 49 texts described a higher prevalence of cam-type FAI in athletes than in an asymptomatic general population. 49 Twelve studies included nonathletic controls and compared the prevalence of FAI morphology between athletes and controls, of which 8 demonstrated statistical significance (Table 2).
Pooled analysis of the results revealed a higher prevalence of FAI per individual in athletes as compared with nonathletes, who are 1.83 times more likely to be diagnosed (95% CI, 1.12-3.01; P = .02) (Figure 2), and a similar trend in prevalence per hip, which did not reach significance (odds ratio, 5.51; 95% CI, 0.48-62.72; P = .17) (Figure 3).
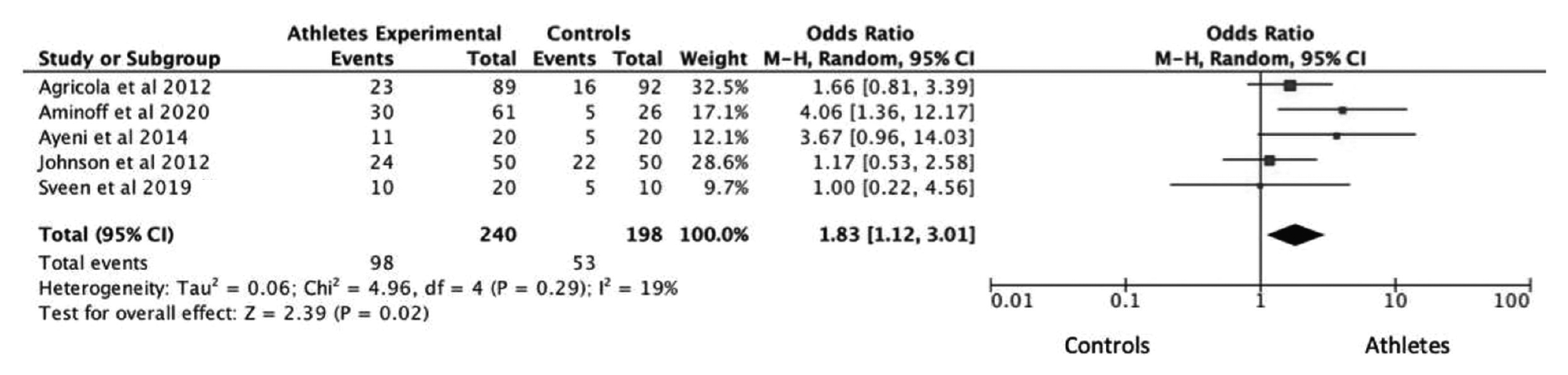
Prevalence of cam-type FAI per individual in athletes vs controls. The term events here refers to the occurrence of cam morphology in athletes and controls. For example, in the 2012 study by Agricola et al, 1 23 experimental events implies that 23 athletes were reported to have cam morphology out of the 89 athletes studied. Of the 92 controls assessed, 16 had cam-type FAI. FAI, femoroacetabular impingement; M-H, Mantel-Haenszel.
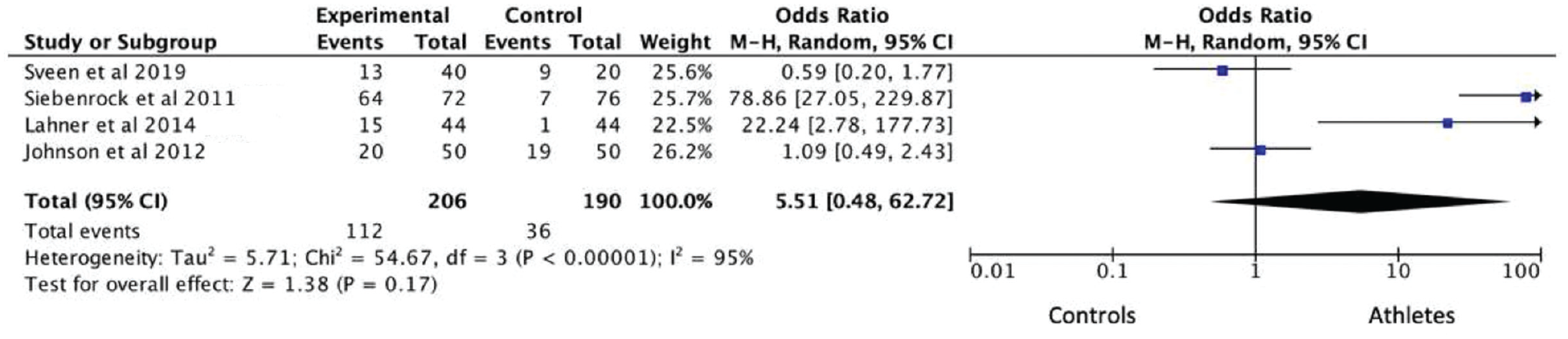
Prevalence of cam-type FAI per hip in athletes vs controls. The term events here refers to the occurrence of cam morphology per hip in athletes and controls. For example, in the 2019 study by Sveen et al, 56 13 experimental events implies that 13 hips had cam morphology out of the 40 hips assessed. Of the 20 assessed control hips, 9 had cam-type FAI. FAI, femoroacetabular impingement; M-H, Mantel-Haenszel.
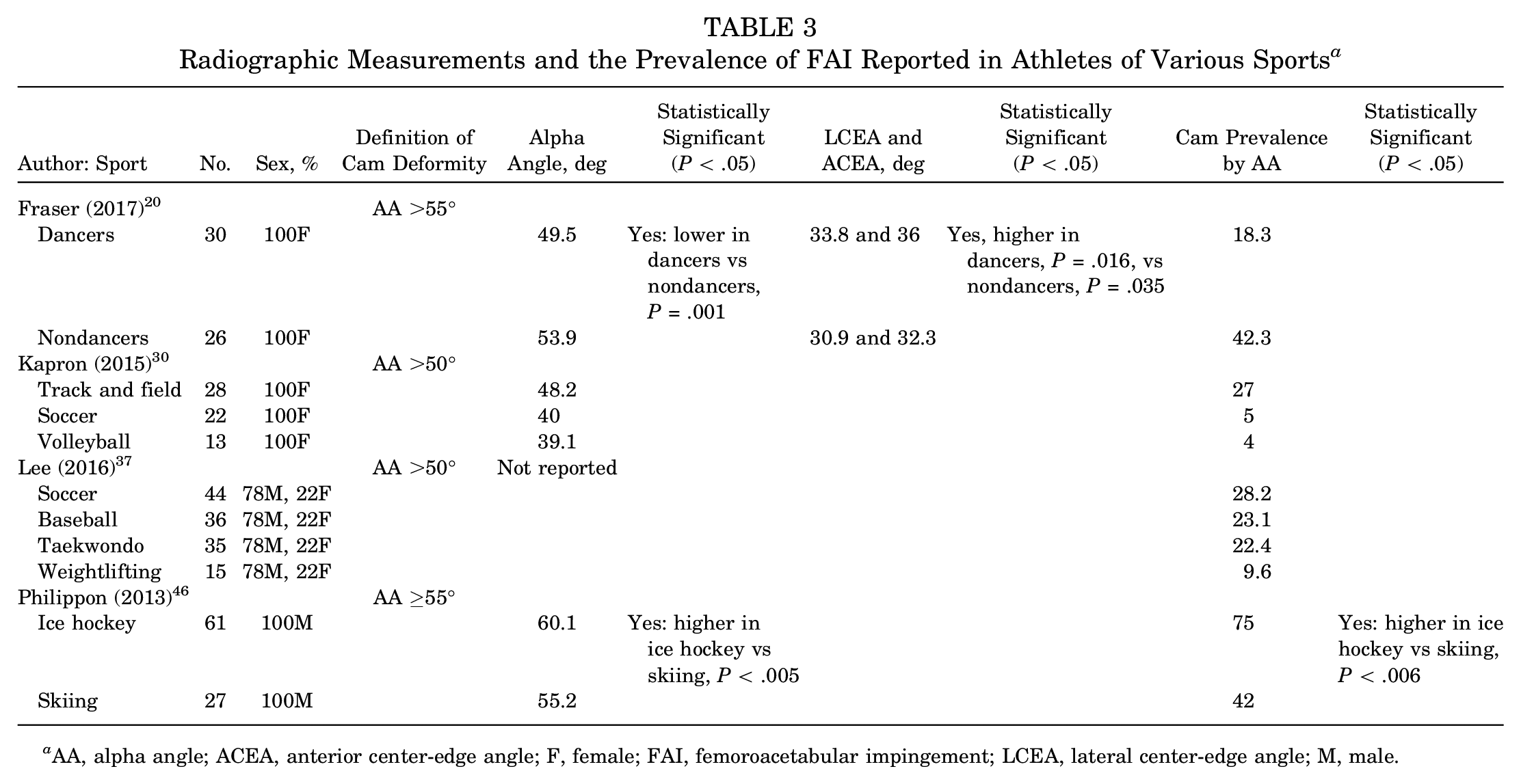
When athletes of various sports were compared, impingement sports tended to show the highest prevalence of cam FAI, with cutting and contact sports also frequently reporting high prevalence. Ice hockey players had the highest prevalence of cam-type FAI 46 (Table 3).
Radiographic Measurements and the Prevalence of FAI Reported in Athletes of Various Sports a
AA, alpha angle; ACEA, anterior center-edge angle; F, female; FAI, femoroacetabular impingement; LCEA, lateral center-edge angle; M, male.
Of 10 studies, 9 reported a higher alpha angle in athletes versus nonathletes (Table 2, Figure 4), with 5 citing statistical significance. Pooled analysis showed that athletes had a significantly higher mean alpha angle than controls (95% CI, 0.27-1.40; P = .004). We were unable to calculate standardized mean difference values from Jónasson et al, 27 so their values are not included in this synthesis.
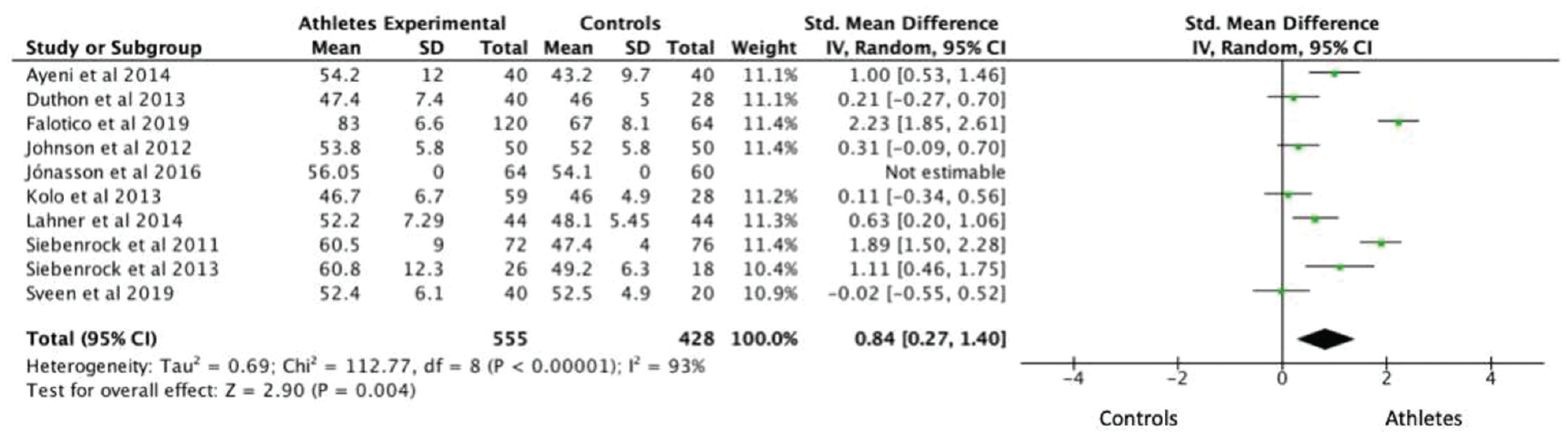
Standardized mean difference in alpha angle of athletes vs controls. IV, inverse variance.
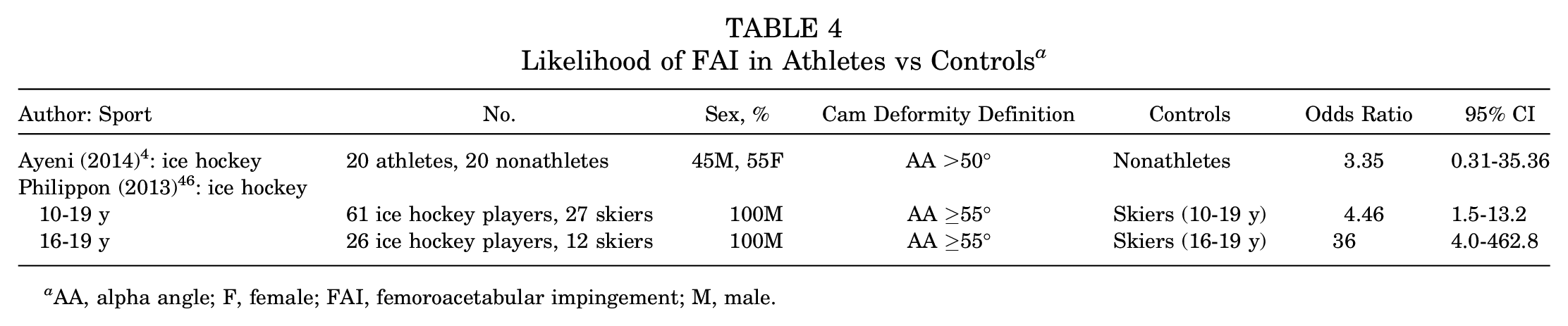
Specifically, ice hockey, an impingement sport, is one of the most reported sports in the literature (see Table 1). Elite ice hockey players are >3 times more likely to develop cam morphology than the general population. 38 Moreover, significantly greater alpha angles are recorded in ice hockey players. 4 Ice hockey players are also >4 times more likely than skiers to have an alpha angle >55° (Table 4), and 79% of ice hockey players showed cam impingement as opposed to 40% of skiers. 46
Likelihood of FAI in Athletes vs Controls a
AA, alpha angle; F, female; FAI, femoroacetabular impingement; M, male.
Cam Morphology and Hip Kinematics
The position of a cam deformity is described across a radial clock face at the femoral head-neck junction on magnetic resonance images, where superior is 12 o’clock and anterior 3 o’clock. Nine studies reported a maximum alpha angle in athletes in the anterosuperior quadrant, with 6 studies specifically mentioning the 1-o’clock position (Table 5).
How the Location of Maximum AA Compares Among Sports a
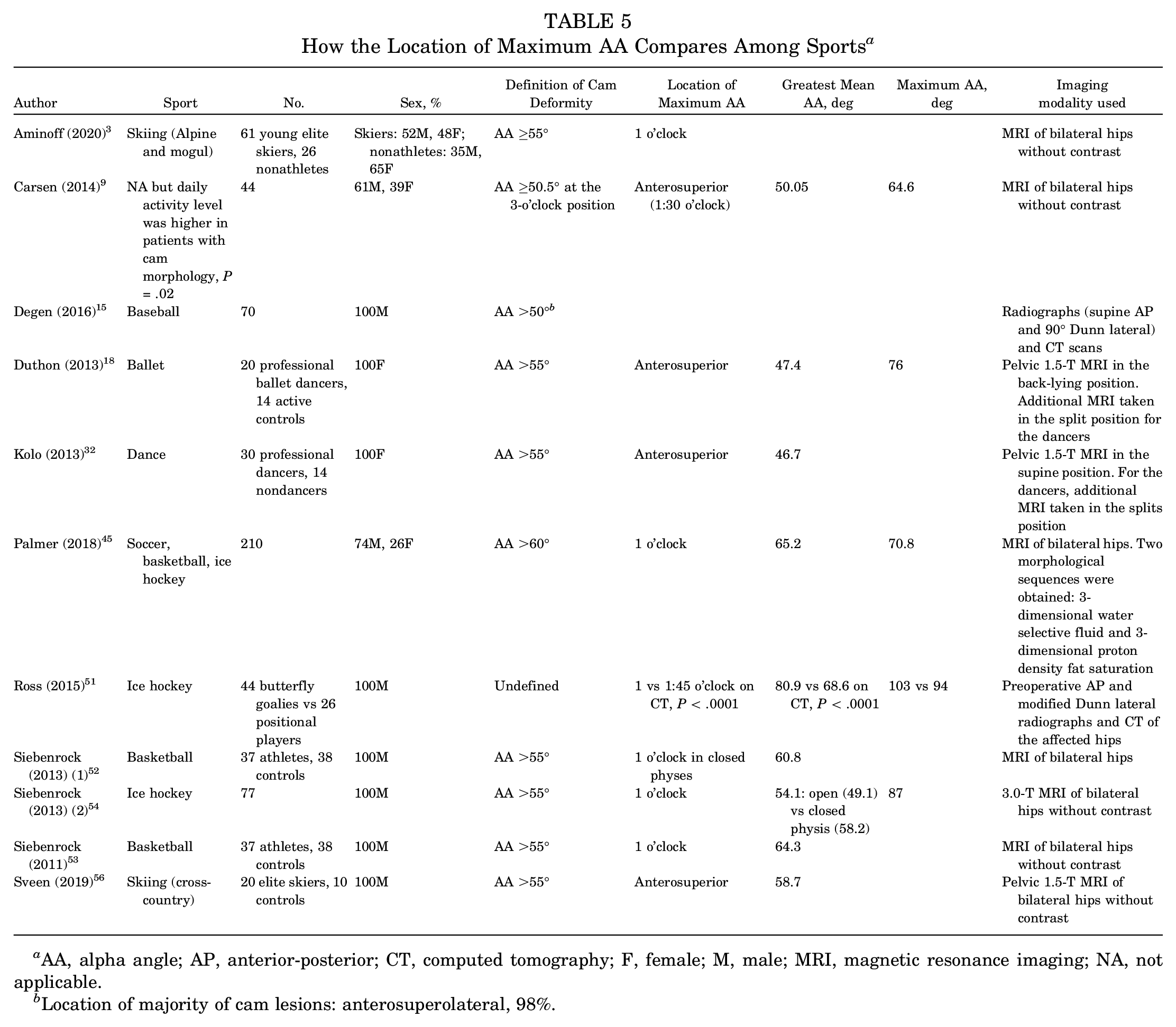
AA, alpha angle; AP, anterior-posterior; CT, computed tomography; F, female; M, male; MRI, magnetic resonance imaging; NA, not applicable.
Location of majority of cam lesions: anterosuperolateral, 98%.
In studies that compared hips subjected to different kinematic conditions, certain “at risk” movements conferred a risk for a higher prevalence of a cam deformity and affected the 3-dimensional morphology of the cam deformity. The location of the maximum alpha angle is different in positional players versus goalkeepers in ice hockey, 1:45 versus 1 o’clock, respectively 51 (Table 5). This same study also found a significantly higher alpha angle on the anterior-posterior view in goaltenders versus positional players (Table 6). Two studies identified asymmetry in morphology among hips exposed to different kinematic parameters in sporting activity, with a lower alpha angle (P < .01), lower prevalence of cam (P = .026), but greater pain in golfers’ lead versus trail hips.16,17
How Morphology and Radiographic Angles Vary Among Positions Within Sports a
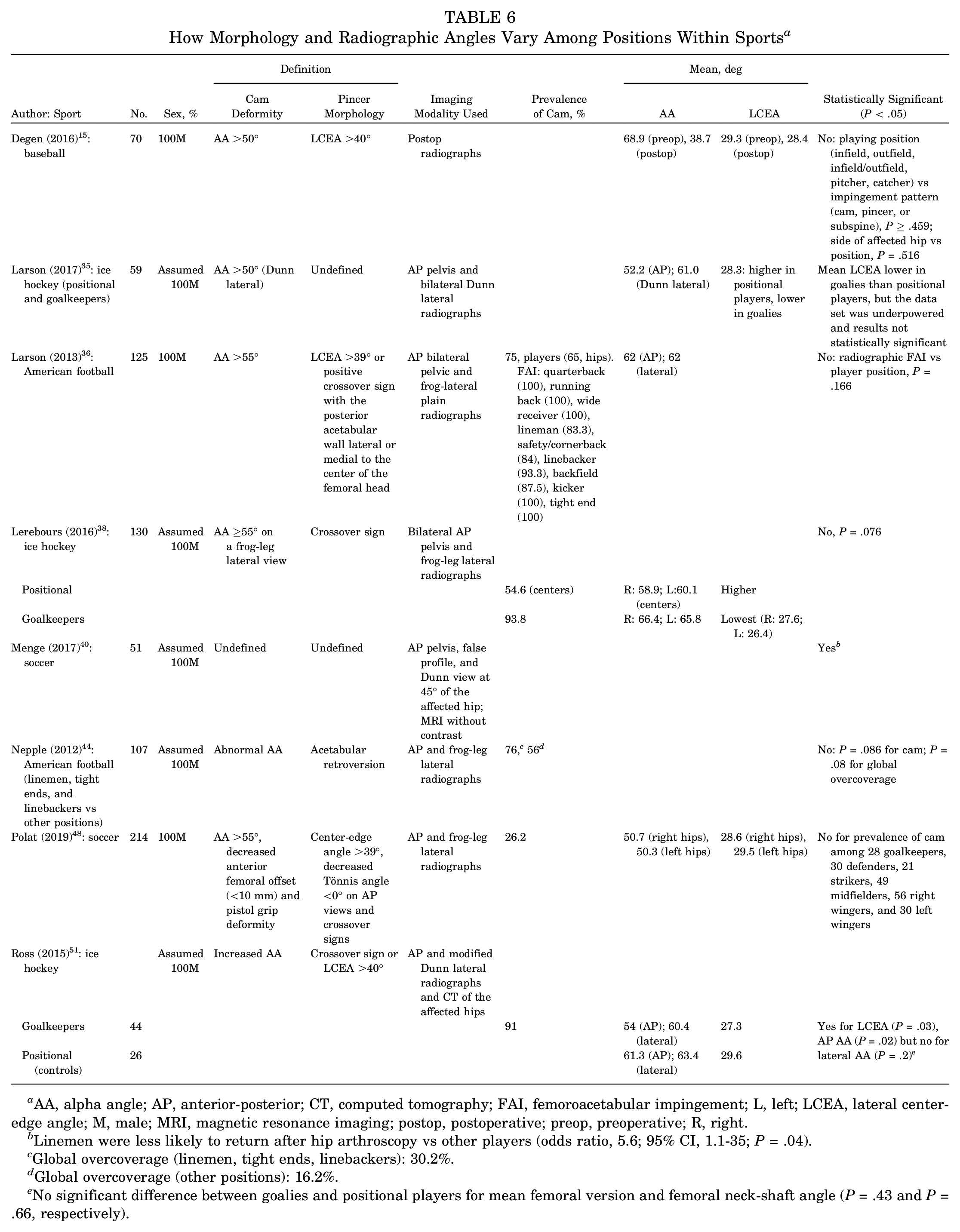
AA, alpha angle; AP, anterior-posterior; CT, computed tomography; FAI, femoroacetabular impingement; L, left; LCEA, lateral center-edge angle; M, male; MRI, magnetic resonance imaging; postop, postoperative; preop, preoperative; R, right.
Linemen were less likely to return after hip arthroscopy vs other players (odds ratio, 5.6; 95% CI, 1.1-35; P = .04).
Global overcoverage (linemen, tight ends, linebackers): 30.2%.
Global overcoverage (other positions): 16.2%.
No significant difference between goalies and positional players for mean femoral version and femoral neck-shaft angle (P = .43 and P = .66, respectively).
Other Factors Influencing Cam Morphology
Five studies reported significant associations between the prevalence of cam morphology and (1) the level at which athletes were competing and (2) the frequency and/or duration of training (Table 7).19,34,43,48,57
Relationship Between the Level, Frequency, and/or Duration of Training and Prevalence of Cam Morphology a
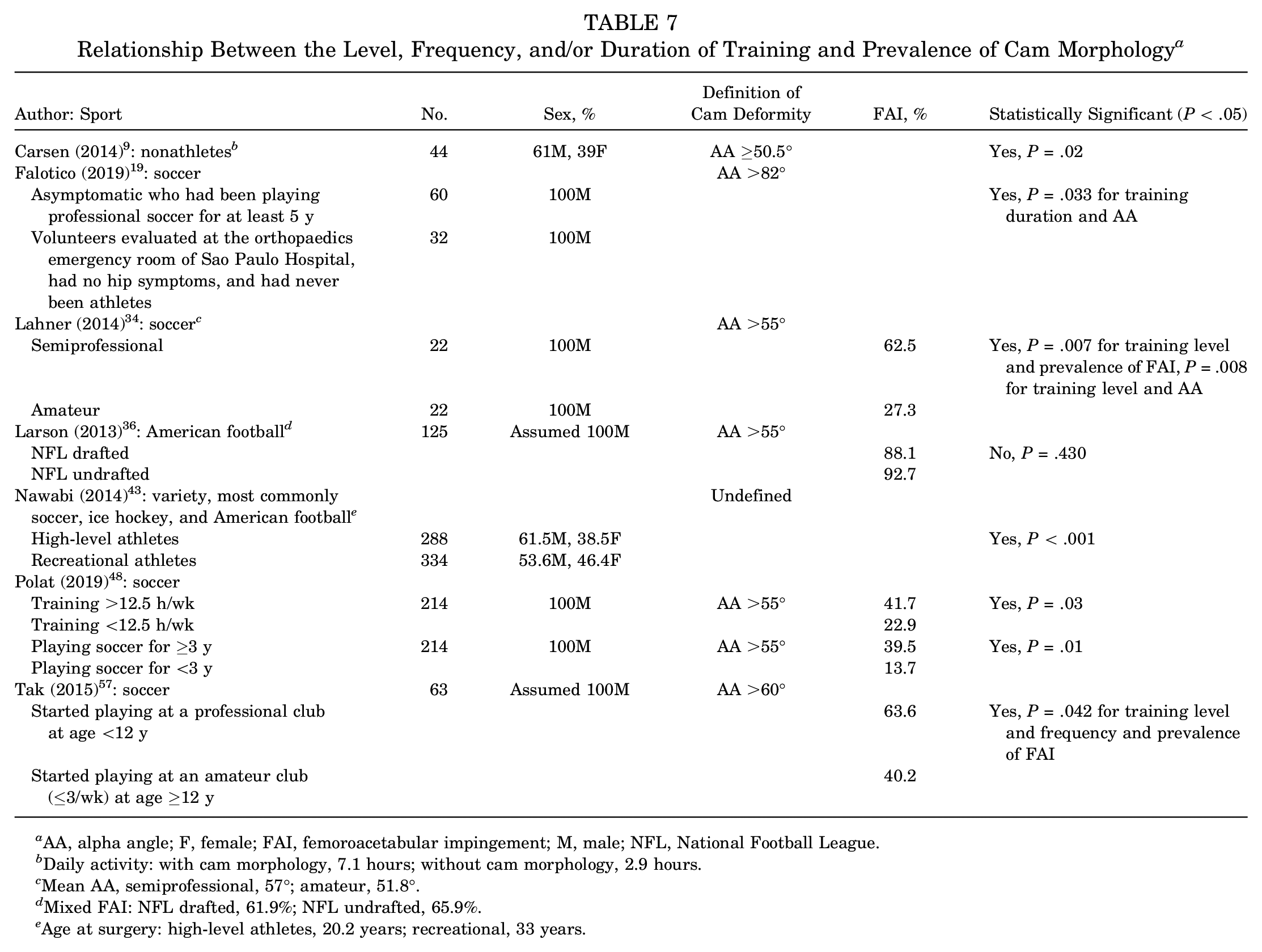
AA, alpha angle; F, female; FAI, femoroacetabular impingement; M, male; NFL, National Football League.
Daily activity: with cam morphology, 7.1 hours; without cam morphology, 2.9 hours.
Mean AA, semiprofessional, 57°; amateur, 51.8°.
Mixed FAI: NFL drafted, 61.9%; NFL undrafted, 65.9%.
Age at surgery: high-level athletes, 20.2 years; recreational, 33 years.
Athletes who trained at a higher frequency were 2.59 times more likely to develop FAI (95% CI, 1.49-4.51; P < .001) (Figure 5).
Increased age was associated with increased prevalence of cam (n = 2/3; P < .05) and increased alpha angle (n = 4/5; P < .05). Few studies reported the association between the age at which athletes started training and their alpha angle (n = 1/2; P < .05) (Table 8).
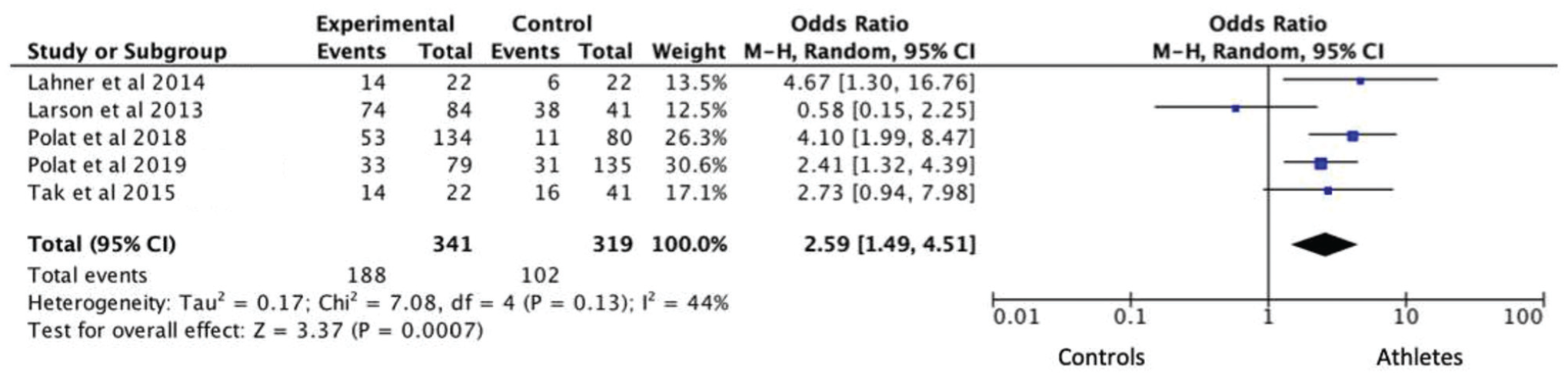
Effect of increased frequency and/or duration of training on cam morphology. M-H, Mantel-Haenszel.
Relationship Between the Age of Athletes and Prevalence of FAI/AA a
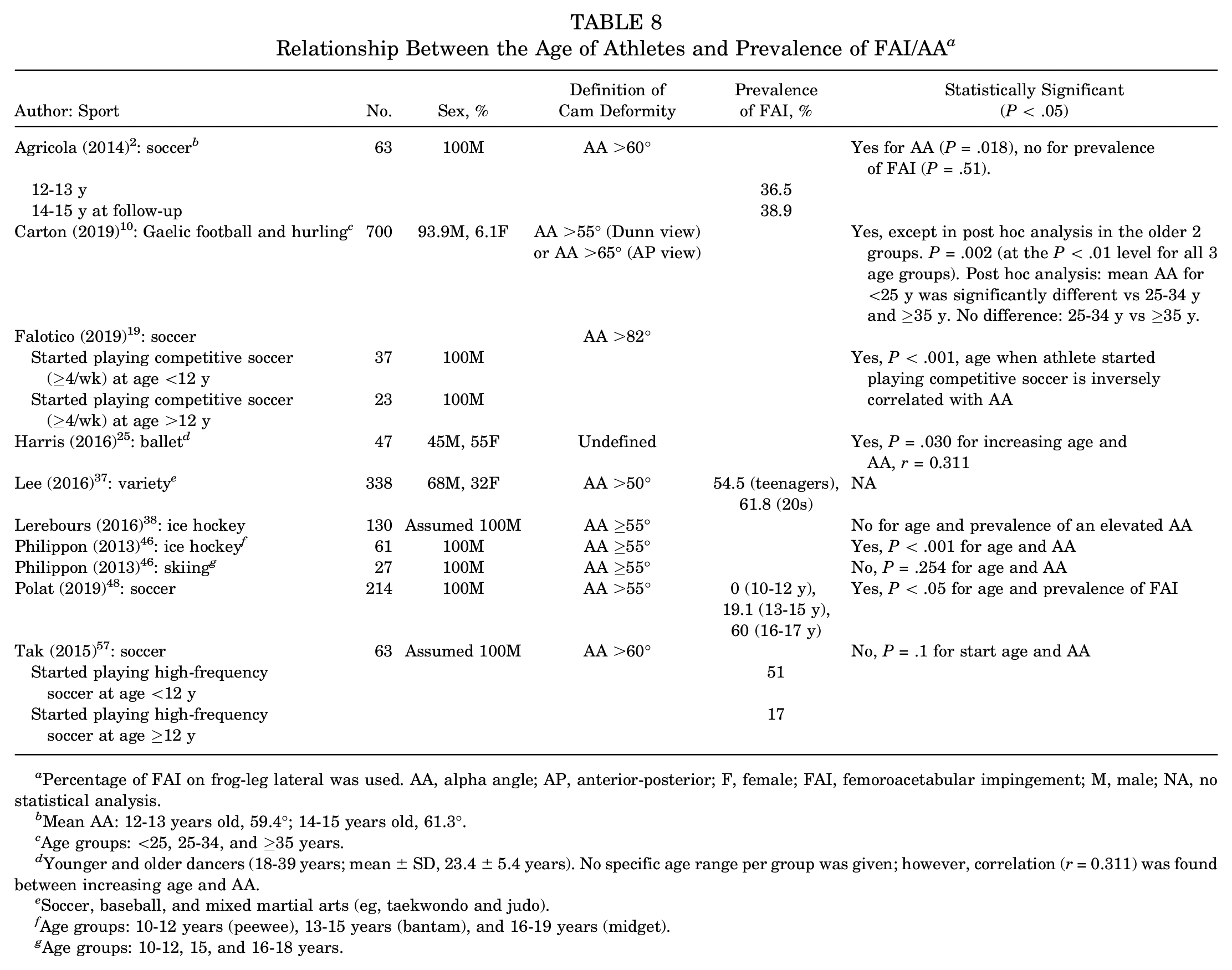
Percentage of FAI on frog-leg lateral was used. AA, alpha angle; AP, anterior-posterior; F, female; FAI, femoroacetabular impingement; M, male; NA, no statistical analysis.
Mean AA: 12-13 years old, 59.4°; 14-15 years old, 61.3°.
Age groups: <25, 25-34, and ≥35 years.
Younger and older dancers (18-39 years; mean ± SD, 23.4 ± 5.4 years). No specific age range per group was given; however, correlation (r = 0.311) was found between increasing age and AA.
Soccer, baseball, and mixed martial arts (eg, taekwondo and judo).
Age groups: 10-12 years (peewee), 13-15 years (bantam), and 16-19 years (midget).
Age groups: 10-12, 15, and 16-18 years.
Ethnicity was assessed in 2 studies.21,42 No significant differences were found between the hips of Asian and non-Asian players in the Japanese baseball league. 21 In soccer, however, East Asian athletes had the lowest prevalence of cam (19%; P < .032) when compared with their White, Black, and Arabic counterparts, who displayed a similar prevalence of 60% to 72%. 42 Similarly, large pathological cam lesions (>78°) were absent in East Asian players and most commonly seen in White players (P = .041).
Pincer and Its Relation to Cam-Type FAI
Pincer morphology is less frequently discussed in relation to sporting activity than cam morphology in the literature; however, it has been noted to be relatively more prevalent in athletes participating in Gaelic football and hurling, baseball, ballet and American football (Table 9).
Comparing Pincer, Mixed, and Cam Morphology in a Variety of Sports a
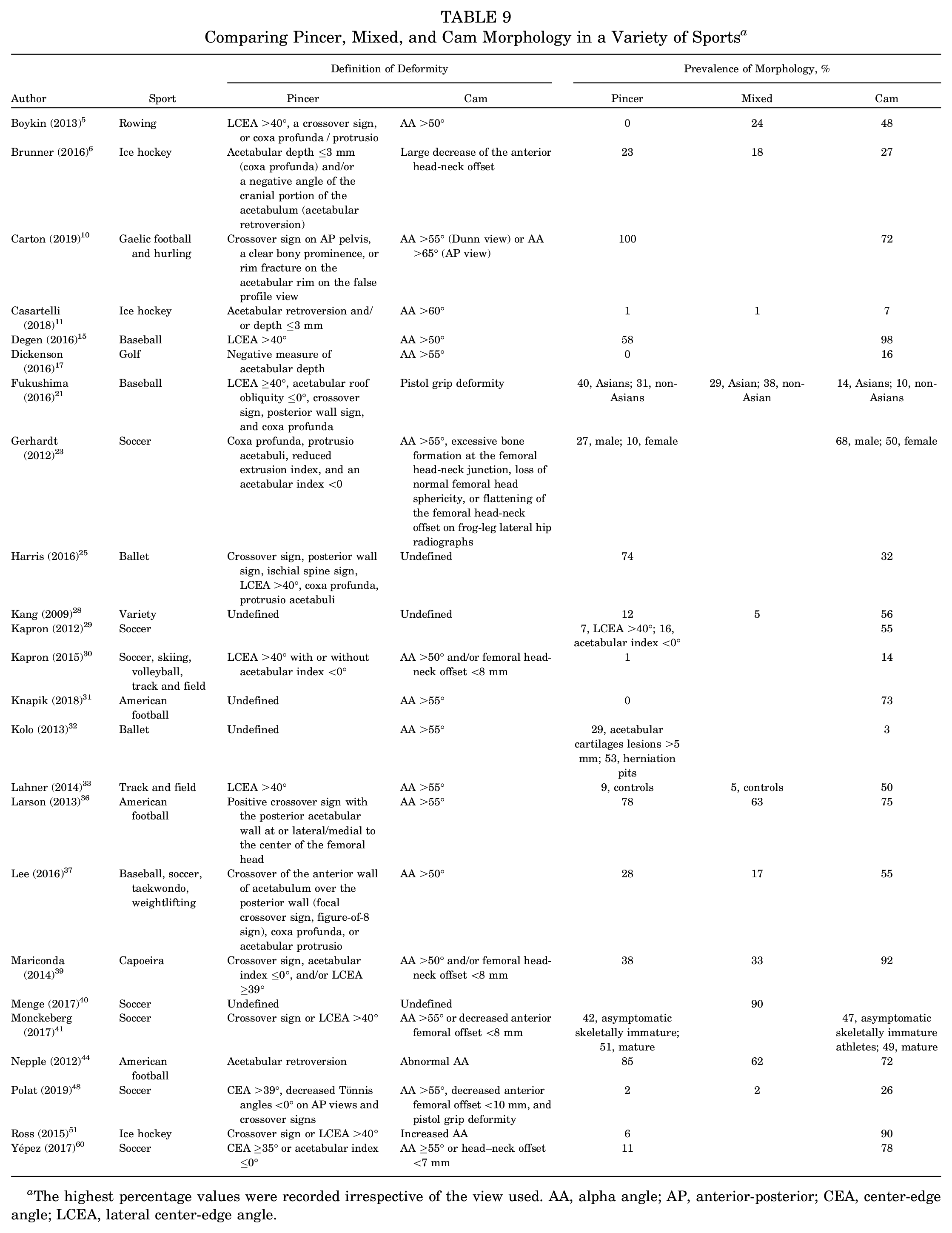
The highest percentage values were recorded irrespective of the view used. AA, alpha angle; AP, anterior-posterior; CEA, center-edge angle; LCEA, lateral center-edge angle.
Discussion
The purpose of this review was to determine the effect of sport on hip morphology and whether the kinematic conditions to which the hip is exposed influences the development of the cam deformity. In addition, we sought to identify factors that may influence cam development. Increased athletic activity is associated with a higher prevalence of cam and a greater alpha angle. The greatest alpha angles are in the anterosuperior quadrant, specifically at the 1-o’clock position. Sports can be categorized according to biomechanical similarities, which show differences in FAI prevalence and/or alpha angles, and these categories reflect differing risks for cam development, with impingement, cutting, and contact sports most likely predisposing an athlete to cam morphology (see Table 1). Similarly, there are positional differences in the cam morphology in ice hockey players. This suggests that different kinematic conditions may result in different femoral head-neck morphological abnormalities. However, there is a paucity of data for the female athletes, with only 15 of the 34 studies listed in Tables 2 to 8 including female data. Much of the current literature also focuses on a small variety of sports, such as ice hockey or soccer.
Hip Morphology Across Sporting Populations
Our results depict that contact sports and sports that involve deep flexion and rotation (impingement) have a higher prevalence of cam morphology in comparison with endurance, flexibility, and cutting sports. 43 Therefore, as expected, the alpha angles in athletes engaged in sports involving impingement are higher than in the athletes engaged in cutting sports. This provides strong support in favor of different sporting loads leading to a variation in the pathology of the hip.
The high frequency of FAI among ice hockey players may be due to the repetitive stress placed on the hip as a result of the unique impinging skating motion and position employed, suggesting that the type of sport influences morphology. 55 This is in comparison with skiers, for example (Table 4), for which the snow could attenuate the impact on landing and the forces transmitted across the hip. This would reduce the cumulative stress placed on the physis of skiers. This implies a model wherein reduced impact stresses lead to the development of less severe cam morphology. In accordance with this, no significant difference in the prevalence of cam was found between cross-country skiers and nonathletes. 56 In contrast, mogul and Alpine skiers reported a significantly higher prevalence of cam versus controls. 3 Alpine and mogul skiing involves high ground-reaction forces, and in the mogul discipline, 2 acrobatic jumps will result in high-impact landings. Competitions are additionally often held on hard and uneven snow, meaning that the snow will offer less impact protection to these skiers than to cross-country skiers.
A higher incidence of cam deformity was found in patients participating in martial arts—for example, taekwondo or hapkido—as compared with those whose primary sport was not a martial art. 28 As with Alpine and mogul skiing, martial arts involve sudden shocks applied to the acetabular rim. It is not unfeasible that sports that involve high ground-reaction forces, in addition to those involving the “at risk” impinging movements, confer a risk for the development of cam morphology.
Dancers more commonly have pincer morphology than cam morphology, with the alpha angle being significantly lower in dancers than nondancers 20 (see Table 3). Kolo et al 32 discovered the presence of cam morphology in only 1 of 30 dancers. No significant difference was found in alpha angle or labral tears between dancers and nonathletes, although statistically significant differences were recorded for acetabular cartilage lesions and herniation pits between the groups (see Table 2). Pincer impingement with subluxation-associated acetabular labral and cartilage lesions and herniation pits is therefore far more prevalent in dancers than cam-type FAI. Additionally, the lateral and anterior center-edge angles of dancers are significantly higher than those of nondancers. This supports the premise of dancers’ having a higher prevalence of pincer morphology and elevated lateral center-edge angles and lower alpha angles than single-sport athletes who are nondancers, 20 and it suggests a difference in radiological presentation and FAI types among sports.
Overall, cam morphology tends to be more frequent in other sports—for example, ice hockey, soccer, basketball, golf, track and field, and rowing. A high prevalence of mixed morphology was also noted in soccer, baseball, and American football players (Table 9), implying that the kinetics and kinematics involved in many sports predispose to cam and pincer and not necessarily isolated morphology.
Positional Differences
Ice hockey butterfly goalkeepers are suggested to be most at risk of cam-type FAI owing to the biomechanical demands of flexion and internal rotation, similar to the flexion, adduction, internal rotation impingement test.43,47,58 Similar demands of extreme internal rotation are placed on athletes in ballet 12 and golf. 24 Indeed, butterfly goalkeepers have a significantly higher alpha angle in comparison with outfield players, and the maximum alpha angle is located in a more lateral position in goalkeepers (1 vs 1:45 o’clock). Anterosuperior impingement may be related to end-range internal rotation. 58 Siebenrock et al 54 noted higher alpha angles in symptomatic versus asymptomatic ice hockey players at 1-, 2-, and 12-o’clock. At these positions, a negative correlation was reported between alpha angle and internal rotation. This suggests that symptomatic cam is associated with functional deficits relating to the “at risk” positions, including decreased internal rotation. However, it is not known whether the relationship between cam deformity and internal rotation relationship is functional and a result of osseous impingement or a consequence of the symptomatic pain experienced. Kinematic exposure through positional differences may affect not only the development of the deformity itself and the associated symptoms but also the outcomes of treatment. In soccer, linemen were less likely to return to play after hip arthroscopy in comparison with other positions (odds ratio, 5.6; 95% CI, 1.1-35; P = .04) (Table 6). This has been attributed to the additional movement and rapid changes of direction required in this position, which may result in more severe morphology.
Ballet dancers more frequently display pincer morphology rather than cam deformity. These athletes typically perform 6 movements: arabesque, développé devant, développéà la seconde, grand écart facial, grand écart latéral, and grand plié. Such movements result in linear contact between the superior or posterosuperior rim of the acetabulum and the femoral head-neck junction. Furthermore, performing the splits results in direct contact between the acetabulum and the anterosuperior femoral head-neck junction. These movements all involve extremes of abduction, flexion, and rotation, once again suggesting that extreme stresses on the hip joint result in FAI syndrome. 32 It is unknown whether these stresses may contribute to the development of pincer deformity; however, interestingly, just as cam morphology is more commonly present in the anterosuperior aspects of the femoral neck, specifically the 1-o’clock position, pincer morphology targets the superior, posterosuperior, and anterosuperior portions of the femoral head-neck junction. In addition, in ballet, female dancers typically dance more en pointe, while male dancers are expected to perform bigger jumps, thereby placing the hips of each sex under different kinematic conditions. This may partially explain the marked sex differences observed in cam prevalence in ballet dancers, with Harris et al 25 reporting a greater prevalence of cam morphology in male dancers (P = .01).
Other Factors Influencing Cam Development
Intense exercise from a young age places increased stresses on the hip joint, and repetitive microtrauma associated with sport predisposes athletes to hip pathology that would not exist or remain asymptomatic otherwise. 7 Tak et al 57 found a significant dose-response relationship between the frequency of training among adolescent soccer players and the development of cam, supporting the notion that high-impact activity during skeletal immaturity can lead to cam development. The prevalence of cam was significantly lower in soccer players playing for an amateur club from the age of 12 years onward than those who started playing for a professional club before 12 years (P = .042). In the same age groups, a significant difference in the prevalence of a pathological cam deformity was found (alpha angle >78°) (P = .038). However, there was no statistical significance between the age at which athletes started playing soccer and the prevalence of FAI in athletes competing at the same level (P = .1). This suggests that the frequency and intensity of training could have a greater effect on the development of FAI than the age at which training began.
A significant positive correlation between age and alpha angle has, however, been identified in ice hockey players throughout adolescence. Philippon et al 46 found that 37% of peewee players, 63% of bantam players, and 93% of midget players had alpha angles ≥55°. In fact, ice hockey players in the midget group (16-19 years) were 36 times more likely than skiers to have an alpha angle >55° (Table 4). Agricola et al 2 showed that cam develops during skeletal immaturity in soccer players and likely remains stable after. As age increases, so does the cumulative duration of training and skill level, implying that age, frequency, duration, and level of training all correlate with alpha angle and cam morphology.
Finally, it was interesting to observe an ethnic difference in the prevalence of cam deformity across athletes competing in the same sport at the same level. 42 While it is impossible in this observational study to control the activity in adolescence exactly, this points to a role of genetic factors in the development of cam deformity. Indeed, Pollard et al 50 noted an increased prevalence of cam deformity in the siblings of those treated for FAI.
Although the relative contributions of these disease-modifying factors still must be established, early screening in those at risk will allow for preventive strategies to be developed, thereby promoting joint and sporting longevity.
Strengths and Limitations
This systematic review is the first to establish the types of sport that are associated with a higher prevalence of cam deformity, and so are hip heavy, and to examine kinematic demands that are related to morphological characteristics at the femoral head-neck junction. Additionally, the methodology encompasses a broad and comprehensive systematic literature search of multiple databases, which allowed us to capture the majority of the existing literature.
However, there are some limitations to this review. We included reviews published in the English language and may have missed data published in other languages. Data were recorded heterogeneously across studies, and for complete data extraction and estimation of mean population values, we were required to use assumptions and compare heterogeneous data. Further limitations of quantitative synthesis are discussed in the Methods section.
Conclusion
Athletic activity affects the hip joint and predisposes to cam-type FAI. Cam deformity is most commonly associated with sports that include repetitive movements demanding levels of internal rotation as well as impact, in particular impingement, followed by cutting and contact sports. Athletes of these sports have higher alpha angles than less athletic controls, with the highest prevalence of cam morphology among ice hockey players. Cam morphology most frequently occurs at the 1-o’clock position of the radial clock face at the femoral head-neck junction on magnetic resonance imaging, with the position potentially being influenced by the kinematic demands of the sport. Dance sport does not fit this trend, however, and is associated with pincer morphology and subluxation. There is a positive correlation seen in some studies between the alpha angle and both age and activity level and between prevalence of FAI and both age and activity level.
With increased awareness of the positive correlation between athletic activity and FAI among clinicians, physiotherapists, athletes, and coaches, as well as greater radiographic and clinical screening, we hope that athletes will be diagnosed, managed better, and be able to return to play far sooner than is currently possible.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211023500 – Supplemental material for Does the Type of Sport Influence Morphology of the Hip? A Systematic Review
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211023500 for Does the Type of Sport Influence Morphology of the Hip? A Systematic Review by Chantelle Doran, Matthew Pettit, Yash Singh, Karadi Hari Sunil Kumar and Vikas Khanduja in The American Journal of Sports Medicine
Footnotes
Submitted August 16, 2020; accepted January 28, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: V.K. has received education support from Smith & Nephew and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.