
Abstract
Background:
Proximal full-thickness free hamstring tendon injury (ie, tendon avulsion or rupture) is a severe injury. Treatment decision making relies on clinical factors and magnetic resonance imaging (MRI) variables; it specifically relies on which tendons are injured as well as the extent of tendon retraction. According to a worldwide evaluation of current practice, discontinuity of both proximal tendons and retraction of >2 cm are used as surgical indications. However, both the diagnosis and the use of MRI variables in decision making may be fraught with uncertainty in clinical practice. A reliable standardized MRI assessment is required.
Purpose:
To propose an MRI assessment for acute proximal full-thickness free hamstring tendon injury and to evaluate its interater reliability.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
We included 40 MRI scans of patients with acute (≤4 weeks of injury) proximal full-thickness free hamstring tendon injury. Three musculoskeletal radiologists assessed proximal full-thickness free hamstring tendon discontinuity using the novel “dropped ice cream sign” and tendon retraction (in mm). Quantification of tendon retraction (in mm) was performed using 2 different methods: (1) a direct (ie, shortest distance between the center of the hamstring origin and the tendon stump) method and (2) a combined craniocaudal/mediolateral measurement method. Absolute and relative interrater reliability were calculated.
Results:
We found an almost perfect interrater agreement (kappa = 0.87) for assessment of full-thickness tendon discontinuity using the dropped ice cream sign. Interrater agreement for the direct and craniocaudal retraction measurements was good for both the conjoint (intraclass correlation coefficient [ICC], 0.88 and 0.83) and the semimembranosus tendons (ICC, 0.81 and 0.79). The mediolateral retraction measurement yielded only moderate to poor reliability for the conjoint (ICC, 0.53) and semimembranosus tendons (ICC, 0.41).
Conclusion:
The standardized MRI assessment to identify proximal hamstring tendon discontinuity and quantify tendon retraction is reliable. We recommend using the novel dropped ice cream sign and the direct retraction measurement in clinical practice and research.
Keywords
Acute proximal full-thickness free hamstring tendon injury (ie, tendon avulsion or rupture) is a severe injury that can result in persisting symptoms and dysfunction.3,4,16 Treatment delay may negatively affect the outcome4,6; thus, a timely diagnosis and adequate treatment decision making are essential. Magnetic resonance imaging (MRI) plays a pivotal role in both diagnosis and treatment decision making.2,5,12,15 MRI is considered the gold standard for diagnosis2,5,12 because of its superior sensitivity.
After a diagnosis, MRI is additionally used for treatment decision making, as identification of involved tendons and assessment of tendon retraction on MRI are widely used as decision modifiers.12,15 Specifically, injuries involving both the conjoint and semimembranosus tendons and retraction of >2 cm are used to support the choice for operative treatment. 15 Additionally, MRI is valuable for preoperative planning. However, both the diagnosis and the use of MRI variables in decision making may be fraught with uncertainty in clinical practice.
Alaia et al 1 conducted a survey among radiologists to identify the preferred ischial tuberosity landmark and perceived difficulties in quantifying tendon retraction. They concluded that substantial variability in tendon retraction measurements can be expected because of the differences in choosing a proximal landmark from which to measure and the perceived difficulties in precisely locating the proximal tendon stump.
An MRI assessment of the proximal hamstring complex after injury that is to be used for decision making in clinical practice should be reliable. However, based on the aforementioned work of Alaia et al, 1 we currently cannot assume that such assessment is done reliably without evaluation of measurement reliability. In a previous study, Six et al 13 evaluated the reliability of the proximal hamstring tendon assessment on MRI without a standardized approach or a previous calibration session to evaluate the routine, unmodified reliability in our current clinical practice. They found a substantial interrater agreement for tendon discontinuity, but only a moderate agreement for tendon retraction. We hypothesized that, in accordance with the work of Alaia et al, this resulted from the lack of a standardized approach. Studies reporting hamstring tendon retraction have not included measurement methods.
In this study, we present a standardized assessment for (1) proximal free tendon discontinuity using the novel “dropped ice cream sign,” and (2) tendon retraction for acute (≤4 weeks from onset of injury) proximal full-thickness free hamstring tendon injury on MRI. We subsequently evaluated interrater reliability. Our hypothesis was that this standardized assessment can be used to reliably evaluate tendon discontinuity and the extent of tendon retraction on MRI.
Methods
Participants
A total of 40 eligible participants were included between January 2013 and February 2019 as part of an ongoing prospective study on the outcome of operative and nonoperative treatment of proximal full-thickness hamstring tendon injury. This study was exempted from ethics review by the institutional review board (Medisch Ethische Toetsings Commissie, Amsterdam UMC, Amsterdam, the Netherlands, No. W17_231). All patients gave informed consent.
Patients included in the current study had an acute proximal full-thickness hamstring tendon injury that was confirmed by MRI acquired ≤28 days after injury. Eligibility criteria are shown in Table 1.
Eligibility Criteria of Participants a
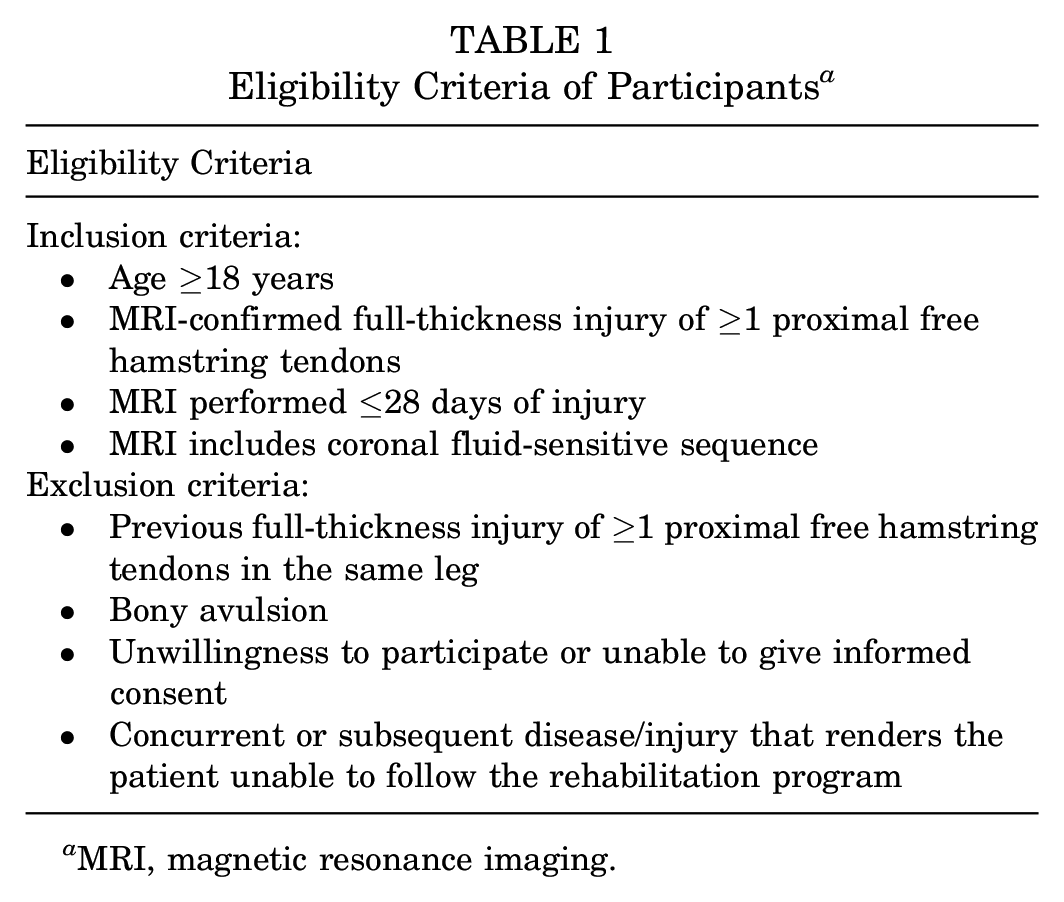
MRI, magnetic resonance imaging.
MRI Protocol
The initial MRI was done at the referring center or in the study center. In the latter, images were acquired with a 3T magnet system (Ingenia System; Philips) and a body matrix coil. Coronal Dixon T2-weighted images (repetition time/echo time [TR/TE], 2000-6000/60 ms; field of view [FOV], 450 × 450; slice thickness, 4 mm; matrix, 820 × 651) were obtained. Subsequently, axial T2-weighted turbo spin echo images (TR/TE, 2500-6000/70 ms; FOV, 450 × 250; slice thickness, 2.5 mm; matrix, 900 × 360) and axial Dixon proton density–weighted images (TR/TE, 2000-3500/shortest possible time; FOV, 400 × 450; slice thickness, 3.5 mm; matrix, 800 × 699) were obtained.
Standardized MRI Assessment
The MRI assessment was performed using a standardized scoring form by 3 raters, who were musculoskeletal radiologists (F.F.S., C.F.B., M.M.) with between 5 and 29 years of experience. All raters were blinded to patient data and clinical findings. The order in which MRI scans were assessed was randomized. Before the assessment, a calibration session was held to make sure all raters understood the measurements and were able to perform them independently. All raters were instructed using an identical slideshow (see Appendix, available in the online version of this article) with illustrated measurement methods, along with 3 exemplary cases.
All raters assessed tendon discontinuity (ie, free tendon avulsion or rupture of the conjoint tendon, the semimembranosus tendon, or both) using the novel dropped ice cream sign and they quantified tendon retraction (in mm) using the craniocaudal, mediolateral, and direct methods.
Proximal Full-Thickness Free Tendon Discontinuity
To assess proximal full-thickness free tendon discontinuity, we introduced the dropped ice cream sign (Figure 1). On axial sequences, the ischial tuberosity resembled a tilted ice cream cone. The 2 hamstring tendon attachments then represented 2 scoops of ice cream: the conjoint tendon attached on the medial facet and the semimembranosus tendon attached on the lateral facet. 17 In case of a proximal hamstring tendon avulsion, it appeared as if 1 or both of the “scoops” had fallen off the ice cream cone. A “single dropped ice cream sign” could be noted in case of proximal tendon avulsion of a single tendon. A “double dropped ice cream sign” was seen in case of avulsion of both the conjoint and the semimembranosus tendons. The remainder of the proximal free tendon distal to the ischial tuberosity was subsequently assessed for full-thickness rupture.
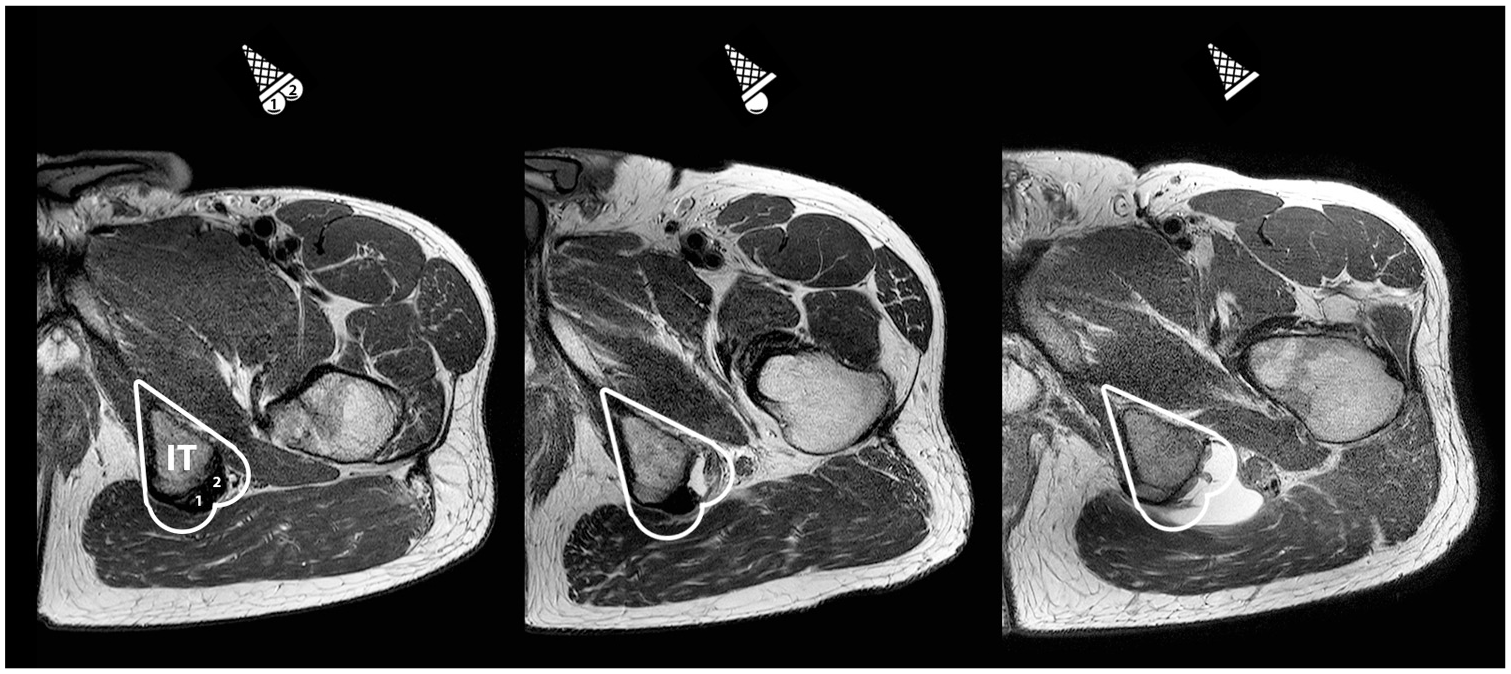
The dropped ice cream sign to assess if and which proximal tendons are avulsed. On an axial magnetic resonance sequence depicting a left pelvic area, the ischial tuberosity (IT) resembles an ice cream cone. The 2 scoops represent the proximal tendons: (1) the conjoint tendon medially and (2) the semimembranosus tendon laterally. Depending on whether 1 or both proximal hamstring tendons are avulsed, there is a single (middle) or double dropped ice cream sign (right). The ice cream flavors
Tendon Retraction
The extent of tendon retraction (in mm) was measured on coronal fluid-sensitive sequences using 2 separate methods. Multiple plane reconstruction was not allowed as this is not typically employed in assessing anisotropic MRI sequences. The first method was the direct (ie, shortest) distance between the anatomic footprint and the most proximal part of the tendon stump (Figure 2). For the proximal landmark, the footprint of the proximal hamstring complex, the center of the upper region of the ischial tuberosity 17 can was taken. In the coronal plane, the lateral outline of the ischial tuberosity was divided into 2 slopes with differing angles. The upper region was the superior/steeper slope (Figure 2; dotted line). The most proximal part of the tendon stump was defined as the most proximal point of low signal intensity that could be confidently identified as part of the hamstring tendon.
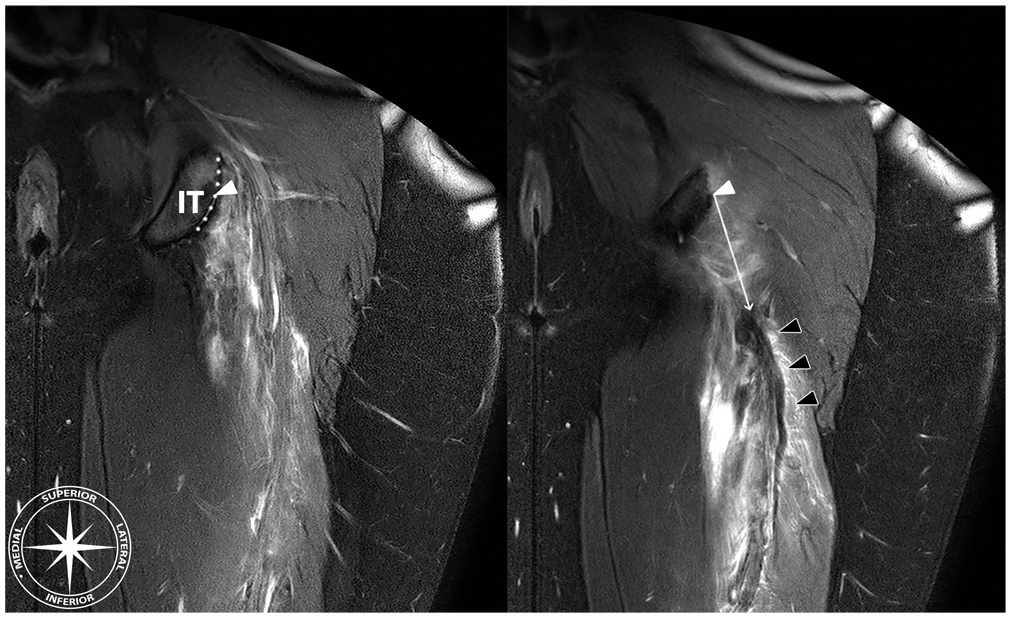
Direct retraction measurement. First, the point representing the center (white triangle) of the proximal hamstring complex origin on the upper region (dotted line) of the ischial tuberosity (IT) is determined. From this point, the direct (ie, shortest) distance (white arrow) to the most proximal part of the hypointense tendon stump (black triangles) was measured (in mm). Note that determining the anatomic landmarks is done on different images within 1 magnetic resonance imaging sequence.
The second method comprised purely craniocaudal and mediolateral distances between the ischial tuberosity and proximal tendon stump (Figure 3). The craniocaudal distance between the most distal margin of the ischial tuberosity and the most proximal part of the hypointense tendon stump and the mediolateral distance between the most lateral margin of the ischial tuberosity and the most medial part of the proximal tendon stump were measured separately. As a result of these landmarks, a tendon stump that is located proximal to the most distal margin of the ischial tuberosity would result in a “negative” retraction. The same applied to a tendon stump that was positioned medial to the most lateral margin of the ischial tuberosity. Although this method did not respect the anatomic tendon footprint and could be considered more abstract because of the possibility of negative retraction, it was included because these anatomic landmarks hypothetically left little room for interpretation and could therefore yield higher reliability than the direct measurement.
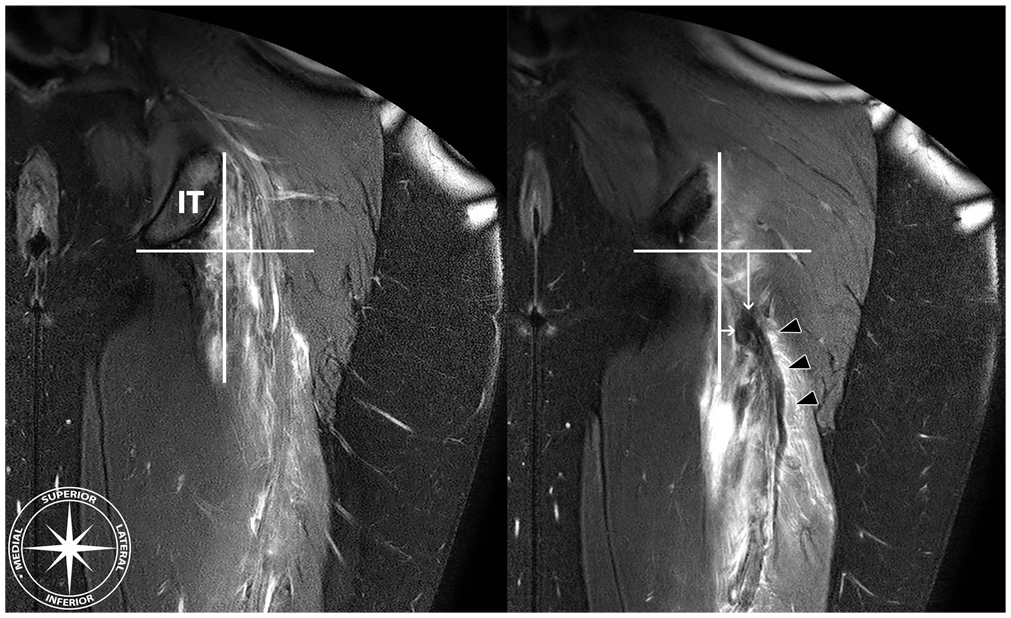
Craniocaudal and mediolateral retraction were quantified by drawing reference lines at the level of the most inferior (horizontal line) and the lateral border (vertical line) of the ischial tuberosity (IT). The craniocaudal (vertical white arrow) and the mediolateral (horizontal white arrow) distances between the reference lines and the most superior and medial margins of the hypointense tendon stump (black triangles) were measured (in mm).
Statistical Analysis
Statistical analysis was performed using SPSS (Version 25.0; SPSS Inc). With an expected intraclass correlation coefficient (ICC) of 0.8 and a 95% CI of ±0.1, the calculated sample size was determined to be 40 participants. 7 A descriptive analysis was used to present demographic data of the study participants and to present outcome of the MRI assessment. The approximate normal distribution of data was evaluated using a qualitative graphical assessment, and descriptive data were presented as mean ± SD or median (interquartile range [IQR]) as appropriate.
Interrater reliability was evaluated using the ICC for continuous variables and the Fleiss kappa (κ) for categorical variables as ≥2 raters carried out the measurements. ICC values, calculated using a 2-way random effects model with the agreement definition (ICC2,1), were used to determine whether there was poor (<0.50), moderate (0.50-0.75), good (0.76-0.90), or excellent (>0.90) reliability. 9 Additionally, we calculated the SEM and the minimal detectable change (MDC). The SEM was calculated as √(MSw) and MDC as 1.96 x √(2) x SEM. Kappa values were used to determine whether there was poor (<0.00), slight (0.00-0.20), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), or almost perfect (0.81-1.00) agreement. 10
Results
The 40 participants (Figure 4) included 17 women and 23 men with a mean age of 49 ± 9.9 years. A total of 24 (60%) MRI scans were performed at the study center and 16 (40%) at the referral center. The injury involved the right leg in 15 (37.5%) and the left leg in 25 (62.5%) participants. The median time between injury and MRI was 7.5 (IQR, 4.5-16.5) days.
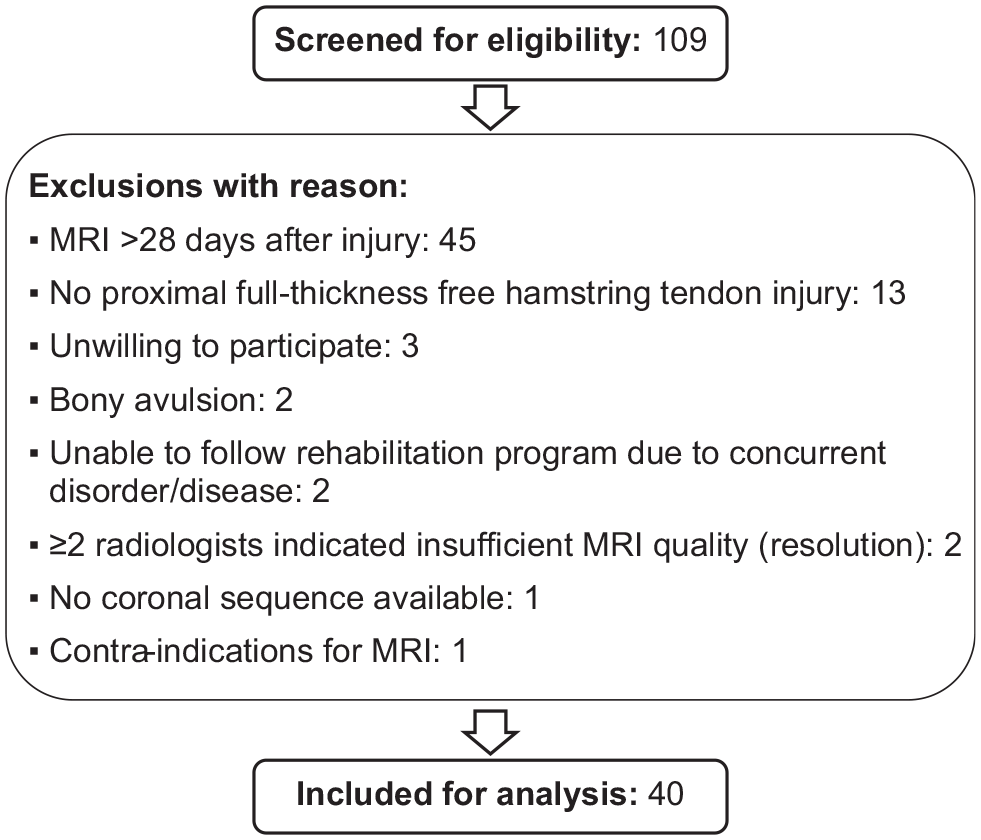
Flowchart of the inclusion process. MRI, magnetic resonance imaging.
The outcomes of the standardized MRI assessment and interrater reliability are provided in Tables 2 and 3.
MRI Assessment of Tendon Discontinuity and Retraction Per Rater in Acute Proximal Full-Thickness Free Hamstring Tendon Injury a
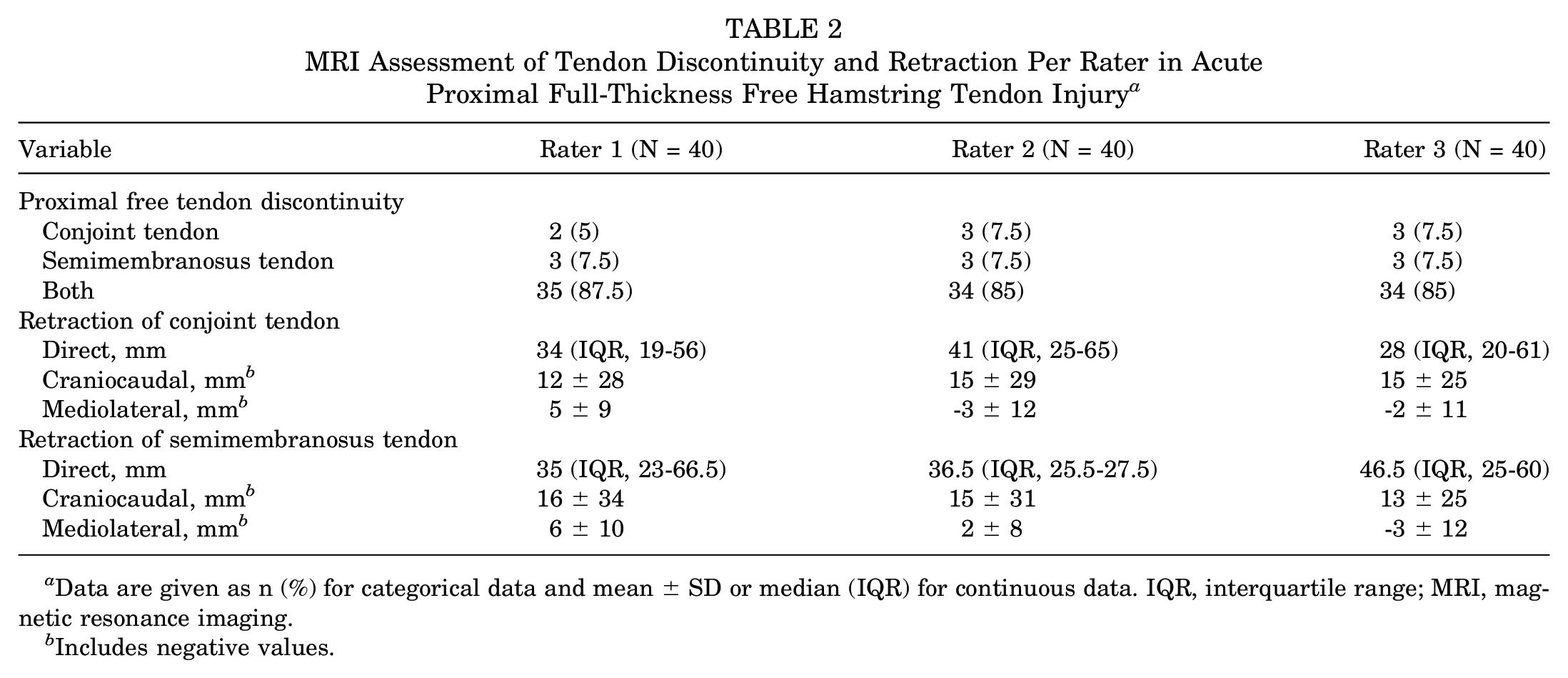
Data are given as n (%) for categorical data and mean ± SD or median (IQR) for continuous data. IQR, interquartile range; MRI, magnetic resonance imaging.
Includes negative values.
Interrater Reliability of Free Tendon Discontinuity and Quantification of Tendon Retraction on MRI in Acute Proximal Full-Thickness Hamstring Tendon Injury a
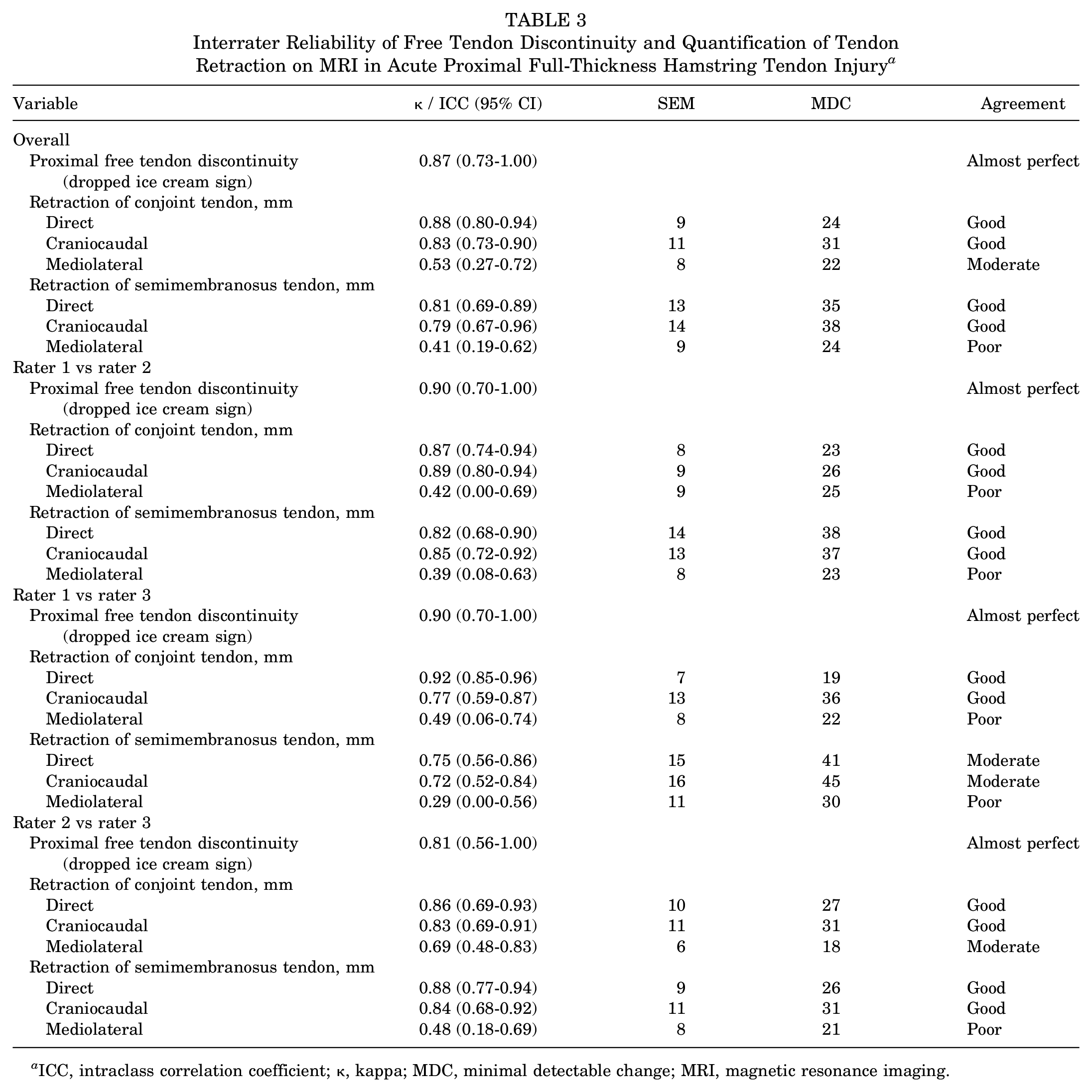
ICC, intraclass correlation coefficient; κ, kappa; MDC, minimal detectable change; MRI, magnetic resonance imaging.
There was an almost perfect interrater agreement for the assessment of tendon discontinuity using the dropped ice cream sign. The raters unanimously reported tendon avulsion of both the conjoint and semimembranosus tendons in the 19 patients who were treated operatively. This was confirmed during operative repair.
For tendon retraction, using the direct and craniocaudal measurements, we noted a good interrater agreement for both the conjoint and the semimembranosus tendons. The mediolateral measurement was not reliable, with only moderate and poor agreement for the conjoint and the semimembranosus tendons, respectively.
Discussion
The most important finding from this study is that the standardized MRI assessment of acute proximal full-thickness free hamstring tendon injury is interrater reliable. We found an almost perfect agreement for assessing proximal free tendon discontinuity using the novel dropped ice cream sign. We noted good agreement for quantifying tendon retraction using the direct and craniocaudal measurements. The direct measurement had superior absolute reliability (ie, SEM/MDC) compared with the craniocaudal measurement and is thus the preferred method.
Little research has been done on the reliability of tendon retraction measurements on MRI after hamstring avulsion or rupture. This is surprising considering that such data are essential to determine clinical utility of a variable or a measurement. Alaia et al 1 conducted a survey among musculoskeletal radiologists and predicted that substantial variability in tendon retraction can be expected due to differences in choosing proximal and distal landmarks for the measurements. The proximal landmark used was either the origin of the conjoint tendon (47%), the origin of the semimembranosus tendon (39%), or the posterior-inferior edge of the ischial tuberosity (14%). Almost half (44%) of the radiologists expressed difficulty in determining the location of the retracted tendon stump. Six et al 13 evaluated the reliability of proximal hamstring tendon assessment on MRI without a standardized scoring method to evaluate routine, unmodified reliability in current clinical practice. A standardized MRI assessment was recommended, mainly because of lower interrater agreement for tendon retraction measurements than was acceptable for use in clinical practice. Six et al found substantial agreement for identifying tendons with a full-thickness injury (κ = 0.77) and moderate/moderate agreement for quantifying retraction of the conjoint/semimembranosus tendons (ICC, 0.73/0.57; MDC, 38/57 mm). Such issues have also been found in other muscle groups. Several studies noted substantial interrater variability of MRI measurements after rotator cuff injury. Interrater reliability for assessing the number of involved rotator cuff tendons and determining the amount of retraction in qualitative manner demonstrated only a moderate agreement (κ, 0.40-0.55 and κ, 0.44-0.58).8,11,14
Using the proposed standardized assessment in the current study, we found an almost perfect and good/good interrater agreement. Using standardized assessments, absolute and relative reliability are substantially more favorable compared with the study by Six et al. 13 Corresponding SEM/MDC values for the quantification of tendon retraction were nonnegligible but arguably acceptable. Yet, the MDC values should be taken into account when using retraction beyond a certain cutoff value as an indication for operative repair. We found that the direct method to quantify tendon retraction is the most reliable. The alternative method comprising craniocaudal and mediolateral distances was less reliable and is therefore not preferred. However, the craniocaudal distance may be used to correlate physical examination findings with imaging findings, as the inferior margin of the ischial tuberosity is an easily palpable landmark. Interrater reliability for the craniocaudal distance was rated as good, but mediolateral distances cannot be reliably measured. The mediolateral distance was part of the combined craniocaudal/mediolateral measurement method to ensure a more complete description of tendon retraction rather than craniocaudal distance alone, but we argue that it likely has no clinical relevance in isolation. We hypothesize that the mediolateral displacement, often due to hematoma formation resulting from tendon avulsion or rupture, is reversible upon hematoma resorption.
Limitations
The main limitation of this study was that not all MRI scans were performed in the study center. Identical MRI protocols would have potentially further increased reliability. Heterogeneity in imaging protocols and quality reflects clinical practice and increases its external validity. Also, no gold standard (eg, intraoperative findings and measurements) was available to draw conclusions regarding the measurement validity of quantifying tendon retraction.
Recommendations for Clinical Practice and Research
This study presents a reliable MRI assessment for proximal free tendon discontinuity and quantifying tendon retraction in acute proximal full-thickness free hamstring tendon injury. We recommend that the MRI assessment of acute proximal hamstring injury includes the dropped ice cream sign and the direct retraction measurement. The measured extent of retraction depends on the measurement method used and on the precise landmarks employed in the measurement (Table 2). Therefore, we recommend that MRI reports and studies using this variable should be explicit in how the measurement was performed. Ideally, the anatomic landmarks used to measure retraction should be reported. We propose the center of the upper region of the ischial tuberosity 17 and the most cranial extent of clearly identifiable (PD/T2) hypointense tendon stump as standardized landmarks.
Tendon discontinuity and tendon retraction are important factors for treatment decision making.12,15 Although the development of a reliable MRI assessment is a vital step in the right direction, additional data are needed to assess clinical utility. For one, further validity testing is necessary to investigate whether tendon retraction on MRI correlates with intraoperative findings to ensure accurate preoperative planning. With regard to using retraction as an indication for operative repair, the association between tendon retraction and outcome after nonoperative treatment needs to be examined. After all, retraction is only useful for decision making if there is a retraction threshold beyond which nonoperative treatment results in poorer outcomes. Such research efforts should also include analyses to determine whether 2 cm is an appropriate cutoff value, ideally employing the standardized and reproducible measurements outlined in this study.
Conclusion
The standardized MRI assessment to identify full-thickness free tendon injury and to quantify tendon retraction in acute (≤4 weeks of injury) proximal hamstring tendon injury was reliable. We recommend using the novel dropped ice cream sign and direct retraction measurement (ie, the shortest distance between the center of the proximal hamstring complex origin and the proximal tendon stump) in clinical practice and research.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211021612 – Supplemental material for Good Interrater Reliability for Standardized MRI Assessment of Tendon Discontinuity and Tendon Retraction in Acute Proximal Full-Thickness Hamstring Tendon Injury
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211021612 for Good Interrater Reliability for Standardized MRI Assessment of Tendon Discontinuity and Tendon Retraction in Acute Proximal Full-Thickness Hamstring Tendon Injury by Anne D. van der Made, Frank F. Smithuis, Constantinus F. Buckens, Johannes L. Tol, Willem R. Six, Kenny Lauf, Rolf W. Peters, Gino M. Kerkhoffs and Mario Maas in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank Ms Iris Kilsdonk for her contribution to improving the dropped ice cream sign concept and Mr Cas Edo Dahmen for his help with preparation of the figures.
Submitted October 28, 2020; accepted March 1, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.