
Abstract
Background:
The preoperative number of dislocations has been previously proved to be a major factor influencing the results after Bankart repair with more preoperative dislocations correlated with higher recurrence rates and more reoperations. This could possibly be because of the lower quality of the tissue repaired during the procedure after multiple dislocations. On the other hand, the Latarjet procedure does not “repair” but rather reconstructs and augments the anterior glenoid.
Purpose/Hypothesis:
The main objective was to report the clinical outcomes of patients undergoing a Latarjet procedure after 1 dislocation versus multiple (≥2) dislocations. The hypothesis was that the preoperative number of dislocations would not influence clinical results.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients older than 18 years who had undergone a primary Latarjet procedure for shoulder instability with at least 2 years of follow-up were included. Three different techniques were used: a mini-open technique using 2 screws, an arthroscopic technique using 2 screws, and an arthroscopic technique using 2 cortical buttons. Patients were evaluated and answered a questionnaire to assess the number of episodes of dislocation before surgery, the time between the first dislocation and surgery, recurrence of the dislocation, revision surgery, the Walch-Duplay score, the Simple Shoulder Test score, and the visual analog scale (VAS) score for pain.
Results:
A total of 308 patients were included for analysis with a mean follow-up of 3.4 ± 0.8 years. Of that, 83 patients were included in the first-time dislocation group and 225 in the recurrent dislocation group. At last follow-up, the rates of recurrence and reoperation were not significantly different between groups: 4.8% in the first-time dislocation group versus 3.65% in the recurrent dislocation group and 6.1% versus 4.0%, respectively. The overall Walch-Duplay scores at last follow-up were also comparable between the 2 groups, 67.3 ± 24.85 and 71.8 ± 25.1, even though the first-time dislocation group showed a lower pain subscore (15.0 ± 8.6 vs 18.0 ± 7.5; P = .003). The VAS for pain was also significantly higher in the first-time dislocation group compared with the recurrent dislocation group (1.8 ± 2.3 vs 1.2 ± 1.7; P = .03).
Conclusion:
The number of episodes of dislocation before surgery does not affect postoperative instability rates and reoperation rates after the Latarjet procedure. However, patients with first-time dislocations had more postoperative pain compared with patients with recurrent dislocations before surgery.
The shoulder is the most unstable joint in the human body, and anterior shoulder dislocation has been reported to have an incidence of around 42 in 100,000 people/year. 11 Each anterior dislocation of the shoulder increases the risk of soft tissue and bony lesions with a subsequent higher risk of recurrence.9,15,32 Bankart lesions have been reported in up to 95% of shoulders after dislocation. 27 The other main types of lesions are bony lesions; they appear in a mirror position on the anteroinferior part of the glenoid and the posterosuperior part of the humerus. Humeral lesions as described by Malgaigne occur in 47% to 90% of dislocated shoulders.4,27
Several surgical options have been described to prevent recurrent anterior dislocations. These include both soft tissue and bony procedures. The 2 most commonly performed surgeries are (1) repair of the Bankart lesion and (2) reconstruction with a coracoid bone block. 20 Both of these can be performed open or arthroscopically. Worldwide, the Bankart repair is currently the most popular surgery and represents almost 90% of primary surgeries for anterior instability.3,6 In Europe, however, and especially in France where it was described originally, 72% of surgeons choose the Latarjet as a primary surgery for instability. 28
In high-risk populations, the rate of recurrent shoulder instability can exceed 70% after a primary episode of traumatic anterior dislocation treated nonoperatively. 21 Surgical stabilization of the shoulder has been shown to significantly decrease the recurrence rate after a single episode of traumatic anterior dislocation from 71.3% to 17.5%. 21 Additionally, only 50% to 56% of the patients treated nonoperatively were able to return to sports compared with 71% to 93% after surgical treatment.14,25
The preoperative number of dislocations has been previously proved to be a major factor influencing the results after Bankart repair, with a 4 times higher recurrence rate and 6 times more reoperations in patients operated after multiple dislocations versus those with first-time dislocations. 22 This could possibly be because of the lower quality of the reattached labrum after multiple episodes of dislocation. On the other hand, the Latarjet procedure does not “repair” the anatomic structures but rather reconstructs and augments the anterior glenoid, stabilizing the shoulder with both the so-called “sling effect” of the subscapularis or conjoint tendon7,31 and the “bone-block effect.”2,23 To our knowledge, the effect of the number of dislocations on the clinical results of the Latarjet procedure has never been evaluated.
The main objective of this study was to report the clinical outcomes of patients undergoing a Latarjet procedure after 1 dislocation versus patients undergoing the same procedure after multiple (≥2) episodes in a large series of patients. The hypothesis was that the preoperative number of episodes of dislocation would not influence clinical results after a Latarjet procedure.
Methods
A retrospective study was conducted and approved by the local institutional review board. All patients who were included had undergone a primary Latarjet procedure for recurrent anterior glenohumeral joint instability between 2013 and 2015 in 1 of 5 institutions. Patients older than 18 years at the time of surgery with a minimum 2-year follow-up were identified using a computerized database that contains files of all patients who underwent surgery for shoulder instability in these 5 different institutions. Patients were excluded if they had additional shoulder pathology at the time of surgery including posterior or multidirectional instability, pathological involvement of the long head of the biceps, rotator cuff tear, or symptomatic acromioclavicular joint pathology. Patients were also excluded if they could not speak or read French. The initial research found 441 patients. Twelve were excluded because they were not able to understand the survey properly, leaving 429 patients available for study. Medical records of all the eligible patients were reviewed by 3 independent reviewers (A.H., V.S., P.L.) to collect the following data: patient characteristics, number of episodes of dislocation prior to surgery, arm dominance, shoulder hyperlaxity, level of sport, type of sport, and Instability Severity Index Score. Shoulder hyperlaxity was defined as described by Balg and Boileau 1 and Coudane et al 8 as passive external rotation ≥85° or a Gagey test result >95°. 12 An episode of dislocation was defined as a glenohumeral dislocation that required reduction by someone else. The level of sport was categorized as “competitive,”“recreational,” or “none.” The type of sport was categorized as “contact/collision,”“throwing sports,” and “other.” Standard anteroposterior preoperative radiographs of the shoulder were reviewed to determine if a Hill-Sachs lesion was visible in external rotation and if a loss of contour of the glenoid was present as described by Balg and Boileau. 1
Surgical Procedure
All the surgeries were performed by fellowship-trained senior shoulder surgeons (P.H.). Three different techniques were used depending on the surgeon’s choice and habits:
•A mini-open technique using a drill guide (Arthrex) and two 4-mm cannulated cancellous screws based on the surgical technique of the modified Latarjet procedure as described by Walch 30
•An arthroscopic technique as described by Lafosse et al 19 using a specific guide (DePuy Mitek) and two 3.5-mm cannulated cancellous screws
•An arthroscopic technique using 2 cortical buttons (Tightrope; Arthrex) placed through a custom-made posterior drill guide with a fixed 7-mm offset (Vims) with concurrent Bankart repair 29
Postoperative Management
All patients had a similar postoperative protocol and wore a sling for the first week postoperatively. At the beginning of the second week, patients were encouraged to start self-assisted rehabilitation for 3 weeks. After 1 month postoperatively, the patients were referred to a physical therapist to start active mobilization in elevation and external rotation.
Assessment at Latest Follow-up
After the initial chart review, all remaining eligible patients were contacted via phone and mailed/emailed a questionnaire to assess shoulder function and instability. Patients were given a month to respond from the time that the initial questionnaire was mailed before being contacted again by a member of the study team via phone. The questionnaire assessed the number of episodes of dislocation before surgery, the time between the first dislocation and surgery, recurrence of dislocation, revision surgery, the Walch-Duplay score, 30 the Simple Shoulder Test (SST) score, and the visual analog scale (VAS) score.
Statistical Analysis
Categorical variables were summarized using percentages and continuous variables using means and standard deviations. Chi-square or Fisher exact tests, depending on the sample size, were used to compare categorical variables, and the Student t test was used for continuous variables.
Recurrence and reoperation were estimated using the Kaplan-Meier method, and curves were compared using the log-rank test. All statistical analyses were performed with SAS software version 9.4 (SAS Institute). P values were assessed at the level of 5%.
Results
Patient Characteristics
A total of 308 (71.8% [95% CI, 67.5%–76.1%]) shoulders of eligible shoulders were included for analysis with a mean follow-up of 3.4 ± 0.8 years (Figure 1).
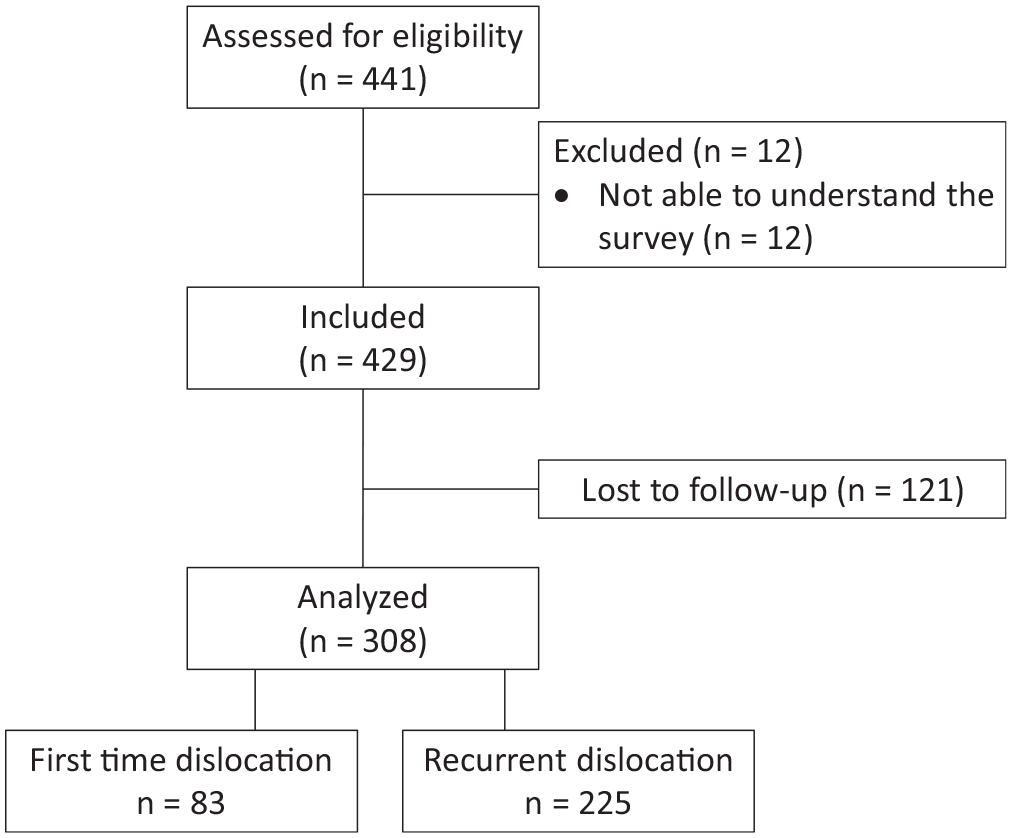
Flowchart.
Global results regarding the population in this series are detailed in Table 1.
Patient Characteristics a
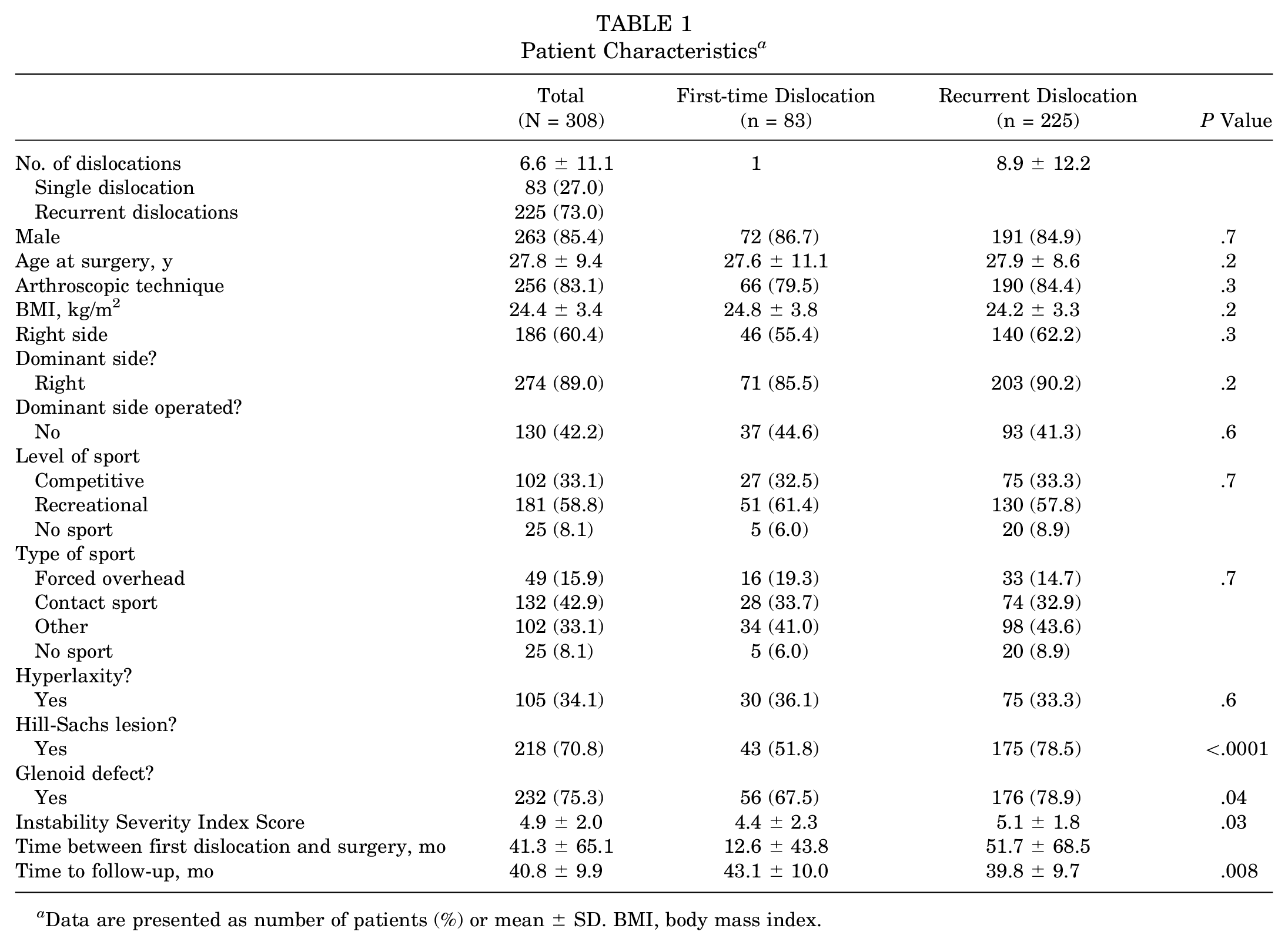
Data are presented as number of patients (%) or mean ± SD. BMI, body mass index.
Patients were predominantly young (27.8 years) males (85.4%) who were involved in a sport activity at either the competitive level (33.1%) or recreational level (58.8%). The types of sports practiced were contact sports in 42.9% of cases or forced overhead sports in 15.9% of cases. A high rate of bony lesions was observed on either the humeral side (70.8%) or glenoid side (75.3%). The mean Instability Severity Index Score was 4.9 ± 2.0 points. Patients waited an average of 41.3 ± 65.1 months between the first dislocation and surgery.
Concerning the 2 groups, 83 patients were included in the first-time dislocation group and 225 in the recurrent dislocation group. In the recurrent dislocation group, the mean number of episodes of dislocations reported by the patients before surgery was 8.9 ± 12.2. Both groups were comparable regarding the affected side, the surgical technique used, sex, body mass index (BMI), type of sport, and level of participation in sports. Higher rates of bony lesions were found in the recurrent dislocation group on either the humeral side (78.5% vs 51.8%; P < .001) or the glenoid side (78.9% vs 67.5%; P = .04), as well as a higher Instability Severity Index Score (5.1 ± 1.8 vs 4.4 ± 2.3; P = .03). The delay between the first episode of dislocation and surgery was longer in the recurrent dislocation group (51.7 ± 68.5 months vs 12.6 ± 43.8 months). However, even in the first dislocation group, surgery was never performed in an acute setting (minimum delay between first episode of dislocation and surgery, 2 months).
Recurrence, Reoperation, Functional Scores, and Complications
At last follow-up, the rate of recurrence or reoperation was not significantly different between groups: 4.8% (n = 4) in the first-time dislocation group versus 3.7% (n = 8) in the recurrent dislocation group (P = .8), and 6.1% (n = 5) in the first-time dislocation group versus 4.0% (n = 9) in the recurrent dislocation group, respectively (P = .5), with a mean delay of 20.3 ± 12.9 and 12.5 ± 13.7 months.
The main reason for reoperation was hardware removal in 57.1% of cases. The overall Walch-Duplay scores at last follow-up were also comparable between the 2 groups: 67.3 ± 24.85 for the first-time dislocation group versus 71.8 ± 25.1 in the recurrent group (P = .2), even though the first-time dislocation group showed a significantly lower pain score (15.0 ± 8.6 vs 18.0 ± 7.5; P = .003). The SST scores at last follow-up were similar in the 2 groups.
Pain VAS was also significantly higher in the first-time dislocation group compared with the recurrent dislocation group (1.8 ± 2.3 vs 1.2 ± 1.7; P = .03). Follow-up was also longer in the first-time dislocation group compared with the recurrent dislocation group (43.1 ± 10.0 months vs 39.8 ± 9.7 months; P = .008). All results are detailed in Table 2.
Clinical Results at Last Follow-up a
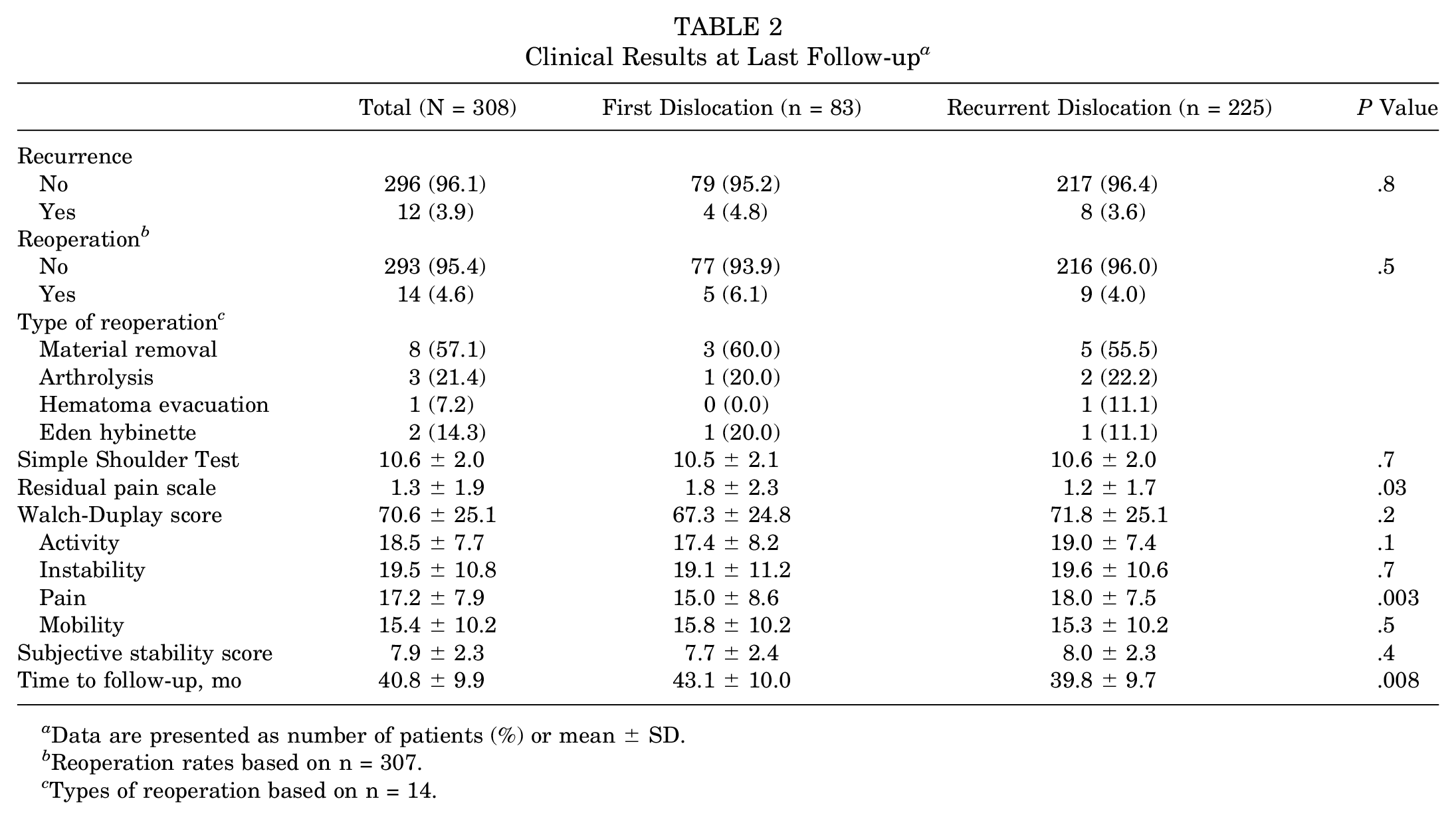
Data are presented as number of patients (%) or mean ± SD.
Reoperation rates based on n = 307.
Types of reoperation based on n = 14.
Discussion
The main finding of the current study is that the preoperative number of episodes of dislocation does not influence recurrence rates after a Latarjet procedure as opposed to what has been previously demonstrated after arthroscopic Bankart repair. 22 The recurrence 13 and reoperation 17 rates found in this study are consistent with the recent literature regarding arthroscopic or open Latarjet procedures.5,17
This innocuity of multiple preoperative dislocations after a Latarjet procedure was found in the present study even though these multiple dislocations had created greater bony lesions and therefore had led to higher Instability Severity Index Scores. This confirms the findings from Balg and Boileau 1 and later from Phadnis et al, 26 who recommend performing a Latarjet procedure rather than an arthroscopic Bankart repair in patients with higher Instability Severity Index Scores. Indeed, as the Latarjet is not an anatomic procedure, its stabilization mechanism does not rely on the preoperative status of the anteroinferior capsuloligamentous complex, which is likely to be severely damaged after multiple episodes of dislocation.
The second important finding of this study was the lower residual pain found in patients in the recurrent dislocation group compared with those in the first-time dislocation group on the VAS and the Walch-Duplay scores. However, the clinical significance of the difference in VAS scores (1.8 ± 2.3 vs 1.2 ± 1.7) should be questioned. Indeed, smaller glenoid bony defects were observed in the patients with first-time dislocations, and this could be a hypothesis for increased postoperative pain. Several studies have shown that the coracoid bone block remodels to restore the initial glenoid shape10,18,24 under the effect of biomechanical loading according to Wolff’s law. Following this hypothesis, patients in the first-time dislocation group with less glenoid bone loss may have undergone greater remodeling of the coracoid bone block and greater osteolysis. Even though some studies have described osteolysis as a possible cause of pain, 18 it has never been proved. However, osteolysis may lead to prominence of the screws and create a painful impingement with the subscapularis. In this study, hardware removal was the most common cause (57.1%) for reoperation. The study was not designed to properly investigate the extent of osteolysis, and additional investigations are warranted. However, this study suggests that Latarjet procedures should be proposed with caution in patients after a first episode of dislocation with an intact glenoid. Indeed, outcomes in terms of recurrence, reoperation, and complications are not negatively affected by the number of preoperative episodes of dislocation, and on the contrary, this could lead to greater postoperative pain possibly because of excessive remodeling of the bone block.
The main limitation of our study is its retrospective design and the fact that patients were evaluated through a questionnaire sent by mail or by email. It remains possible that patients lost to follow-up may have had a different recurrent instability rate; however, this cohort remains large and similar stability was documented in both primary and salvage Latarjet procedures. Preoperative computed tomography scans were not obtained for all patients, and therefore we were unable to precisely quantitate humeral and glenoid bone loss, which may have affected the rate of recurrent instability. Furthermore, the study was not designed to evaluate graft osteolysis or graft positioning; therefore, no computed tomography scans or radiographs were analyzed. In addition, although our study shows no influence of the number of preoperative dislocations on recurrence and reoperation rates, it has been demonstrated by Hovelius and Saeboe 16 that long-term osteoarthritis was more frequent in patients with multiple episodes of dislocation. We did not perform any radiographic analysis, and therefore this could not be evaluated in our study. Finally, our definition of dislocation (defined as a glenohumeral dislocation that required reduction by someone else) can be considered too narrow as it does not take into account subluxation. However, this definition was the same for both groups, which could therefore be compared. This study also has some strengths. It evaluates a large number of patients. Several different techniques were included in the analysis with both open and arthroscopic approaches, with different means of fixation (screws and cortical buttons) and performed by 5 surgeons included in the study, enhancing the generalizability of our findings.
Conclusion
The number of episodes of dislocation before surgery does not affect lower postoperative instability rates and reoperation rates. However, patients with first-time dislocations had higher postoperative pain compared with patients with recurrent dislocations before surgery. Further studies are warranted to determine whether this higher postoperative pain can be explained by increased remodeling of the bone graft in patients with first-time dislocations with no glenoid bone loss.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Submitted April 11, 2019; accepted August 20, 2019.