
Abstract
In this study, we examined active-duty women's experiences with gender microaggressions in the U.S. military and their associations with depressive symptoms. We also tested if rank and coping strategies would moderate the link between gender microaggressions and depressive symptoms. Participants comprised 682 self-identified women from the U.S. Air Force, Army, and Navy. Results from an online survey indicated that active-duty women's experiences with gender microaggressions were positively and significantly associated with their scores on a measure of depressive symptoms. Military rank moderated this association but coping strategies did not. Specifically, among those in lower military ranks (i.e., enlisted service members) we found a stronger association between gender microaggressions and depressive symptoms, whereas higher rank (i.e., officers) served as a buffer. Our results suggest that clinicians should be aware of the potential effects of gender microaggressions on active-duty women's mental health, especially among enlisted women. Commanding officers and military policymakers should consider potential implications of gender microaggressions on unit cohesion, unit performance, and mission effectiveness.
Recent data indicate 8.4% of active-duty women experienced unwanted sexual contact and 29% experienced sexual harassment in 2021 (Department of Defense [DOD], 2022). The DOD attributes this violence to what the American Psychological Association (APA) in its 2018 Guidelines for Psychological Practice with Boys and Men termed traditional masculinity or what we might designate as the toxic masculinity that permeates the military services (e.g., misogyny, homophobia, and transphobia; Christensen & Kyed, 2022; Christensen & Rasmussen, 2018; Doan & Portillo, 2022) and other hegemonically homosocial spaces (Lipman-Blumen, 1976; Wadham, 2013). Controlling for paygrade (i.e., military rank), branch of service, and deployment status, the 2018 DOD Workplace and Gender Relations Survey among 115,884 active-duty service members identified sexual harassment and gender discrimination as leading factors in perceptions of unit climate. The report's authors concluded, “Women consistently rated unit climate lower and workplace hostility higher than men” (Breslin et al., 2019, p. xiii).
As such, what active-duty military women report about sexual harassment and the gender discrimination they experience with co-workers, peers, and acquaintances is crucial to understanding the contexts in which military women serve. Sexual harassment is a gender-related form of workplace hostility that Fitzgerald et al. (1999) differentiated in four separate dimensions as sexist behavior, sexual hostility, unwanted sexual attention, and sexual coercion. Sexual harassment in organizations also has been referred to as workplace incivility (i.e., low-level injustices that can accumulate over time to have a significant negative impact on targets; Cortina et al., 2017). Regarding the military context, Calkins et al. (2021) defined gender discrimination in a military workplace as comments, insults, or other behaviors that target service members based on their gender that negatively affect their careers. For example, the Breslin and colleagues' (2019) report on gender relations in the workplace included the following as examples of gender discrimination and sexual harassment in the military: telling sexual jokes, objectifying women's appearance, inviting women to unwanted relationships, and commenting about how women should act.
Gender Microaggressions: A Form of Covert Discrimination
Although researchers have addressed how women experience overt sexual harassment and gender discrimination in the military (Bell et al., 2018; Breslin et al., 2019), far less research has been conducted on covert forms of discrimination in this context. In the current study, we were interested in one form of covert discrimination in the U.S. military—gender microaggressions that target self-identified women (also referred to as sexist microaggressions; Cherry & Wilcox, 2021). Scholars have addressed gender microaggressions in a variety of contexts, such as undergraduate education (Gartner, 2021), medical school (Struble et al., 2022), and the workplace (Basford et al., 2014). With the notable exception of a technical report (Brown, 2011), gender microaggressions have not yet been addressed in the military. Sue and Spanierman (2020) defined microaggressions as “verbal and nonverbal interpersonal exchanges in which a perpetrator causes harm to a target, whether intended or unintended … [They] communicate hostile, derogatory, and/or negative slights to the target” (p. 8). Moreover, researchers have posited gender microaggressions as a gateway to sexual harassment and sexual assault (Gartner & Sterzing, 2016). Similar to how workplace incivility can lead to psychological distress (Jeong & Lee, 2022), gender microaggressions may also negatively affect women's mental health (Nadal & Haynes, 2012). Given that gender microaggressions have the potential to cause harm and that service women suffer greater psychological distress than active-duty men (Meadows et al., 2018), in the current study we explored whether experiences with gender microaggressions among women in the military are associated with depressive symptoms.
Initial scholarship on gender microaggressions used qualitative approaches to develop taxonomies of microaggressive themes (Capodilupo et al., 2010; Nadal & Haynes, 2012). Researchers put forth taxonomies of gender microaggressions for both higher education (Capodilupo et al., 2010; Nadal, 2010) and workplace contexts (Basford et al., 2014). Among higher education participants, Capodilupo et al. (2010) identified gender microaggressions themes that include: assumptions of traditional gender roles, sexual objectification, second-class citizenship, assumptions of inferiority, sexist language, and denial of sexism. Drawing from these taxonomies and a review of the gender microaggressions literature, Miyake (2018) developed the Female Microaggressions Scale (FeMS). The FeMS broadened Capodilupo et al’s (2010) taxonomy by employing their themes (e.g., traditional gender roles), updating them (e.g., invalidation of the reality of sexism), and adding new themes (e.g., implicit threatened physical safety and explicit threatened physical safety). In the current study, we used the FeMS (Miyake, 2018) to assess active-duty women's experiences with gender microaggressions in the military.
Although there has been little empirical research on gender microaggressions in the military, service women have detailed their experiences in media. A woman soldier and cultural support team member embedded with special operators in Afghanistan, for instance, recounted an example of a traditional gender roles microaggression: A male soldier asked her, “You guys nurses?” She went on to explain how cultural support team women were “used to being sized up as nurses or members of a softball team” (Lemmon, 2015, p. 146). In another example, the U.S. Navy veteran Stephanie Flores (2021) described her experiences in a CNN opinion editorial: “I can clearly remember, for example, a supervisor asking what my ‘Latina stripper name’ would be … I remember questions about supposed sexual favors … I ‘must have given’ to earn the qualifications I worked hard to achieve.” Widely reported incidents of men posting military women's naked photos on social media provide evidence of the sexual objectification gender microaggressions theme (Broadwell & Thomas, 2017; Katzenberg, 2019). Extending these anecdotal accounts, we sought to investigate gender microaggressions empirically among active-duty women.
Subsequent research has documented the associations between gender microaggressions and women's mental health including depression, anxiety, low self-esteem, and post-traumatic symptoms (Cherry & Wilcox, 2021; Gartner, 2019; Williams & Lewis, 2019). For example, among a sample of undergraduate women, Gartner (2019) found that experiences with gender microaggressions were significantly and positively related to depressive and post-traumatic symptoms. In another example among 370 adult cis-gender women, Cherry and Wilcox (2021) found sexist microaggressions positively predicted trauma symptomology, and this association was partially mediated by self-compassion. In the current study, we were interested in exploring the link between gender microaggressions and depressive symptoms, which has implications for active-duty women's mental health as well as unit cohesion, morale, mission readiness, and performance (Armistead-Jehle et al., 2011; Gaddes et al., 2017; Pflanz & Ogle, 2006).
Potential Moderating Role of Military Rank and Coping Strategies
To understand the link between gender microaggressions and depression, we examined the potential moderating role of military rank (i.e., a military-specific factor not yet examined in the microaggressions literature) and coping strategies (i.e., a factor with robust empirical evidence in the context of minority stress theory; Brooks, 1981; Meyer, 1995, 2003). Although we examined individual women's coping strategies, like Brooks (1981), we acknowledge the crucial need for structural changes to address the power imbalances that enable oppression. We do not wish to place the onus on women to be complacent with an unjust system.
Military rank refers to a command hierarchy of enlisted and officer categories with increasing levels of authority, power, and responsibility for personnel, equipment, and mission (DOD, n.d.-b; Department of Veterans Affairs, 2021; Mattila et al., 2017). Bonnes (2021) highlighted the role of rank as a “military specific factor [that shapes] sexual violence vulnerability and experiences” (p. 7). Prior research has found enlisted women (i.e., women in lower military ranks) were more likely to experience sexual harassment and abuse (Antecol & Cobb-Clark, 2001; DOD, 2019) and related mental health concerns (Buchanan et al., 2008) than officers (i.e., women in higher military ranks). Most closely aligned with our study, Buchanan et al. (2008) found a significant interaction with various forms of sexual harassment and rank on psychological distress. In other words, the link between sexual harassment and psychological distress was stronger for enlisted women than for officers. Because little research has addressed gender microaggressions in the military, we sought to investigate if military rank (i.e., enlisted vs. officers) moderated the link between gender microaggressions and depressive symptoms.
To understand the impact of gender microaggressions on mental health and possible mitigating factors, we employed minority stress theory (Brooks, 1981; Meyer, 1995, 2003). Minority stress theory posits that individuals with stigmatized social identities chronically experience additional stress because they encounter prejudice (Brooks, 1981; Meyer, 1995, 2003). Moreover, minority stress theory suggests coping strategies can moderate the association between microaggressions and mental health outcomes. Thus, in the present study, we examined whether coping strategies influence the link between gender microaggressions and depressive symptoms among active-duty women.
We drew from Lazarus and Folkman's (1984) transactional theory of approach and avoidance coping. According to Lazarus and Folkman (1984), coping strategies for stress-inducing situations are categorized as (a) problem-focused (i.e., managing the stress-inducing situation) or emotion-focused (i.e., regulating emotional responses to the problem) and (b) engagement (i.e., confronting stressors) or disengagement (i.e., avoiding stressors). Prior qualitative research on women's coping responses to gender microaggressions has found that responses to microaggressions varied from avoiding the situation to confronting the perpetrator (Nadal et al., 2013). Although there is some debate on the effectiveness of coping strategies against discrimination (Pascoe & Smart Richman, 2009; Schmitt et al., 2014), some studies have suggested that problem-focused engagement buffered the association between discrimination and depressive symptoms (Noh & Kaspar, 2003; West et al., 2010), whereas disengagement strategies exacerbated this association (Schmitt et al., 2014; West et al., 2010). To our knowledge, no research has explored the moderating effect of coping strategies on the association between gender microaggressions and depressive symptoms.
The Current Study
The purpose of the current study was to investigate active-duty women's experiences with gender microaggressions in the U.S. military, the link between gender microaggressions and depressive symptoms, and possible protective or detrimental factors on this association. Because women in lower military ranks have been identified as more vulnerable to psychological distress from sexual harassment (Buchanan et al., 2008), we investigated whether rank moderated the link between experiences with gender microaggressions and depression. Additionally, guided by minority stress theory (Brooks, 1981; Meyer, 2003), we examined whether coping strategies moderated the link between microaggressions and depression. Findings have implications for active-duty women's mental health, as well as for unit cohesion, morale, mission readiness, and performance (Armistead-Jehle et al., 2011; Gaddes et al., 2017; Pflanz & Ogle, 2006).
As such, we developed three hypotheses. First, we hypothesized that gender microaggressions would be positively associated with depressive symptoms. Second, we predicted that rank would moderate the association between gender microaggressions and depressive symptoms. Specifically, we hypothesized that the lower the rank, the stronger the link between gender microaggressions and depressive symptoms. Third, we anticipated that coping strategies would moderate the association between gender microaggressions and depressive symptoms. Specifically, we expected higher frequency of engagement coping styles would buffer the link between gender microaggressions and depressive symptoms. We also predicted higher frequency of disengagement coping styles would exacerbate the association between gender microaggressions and depressive symptoms.
Method
Participants
Participants included 682 active-duty self-identified women (
Participant Demographic Characteristics (N = 682).
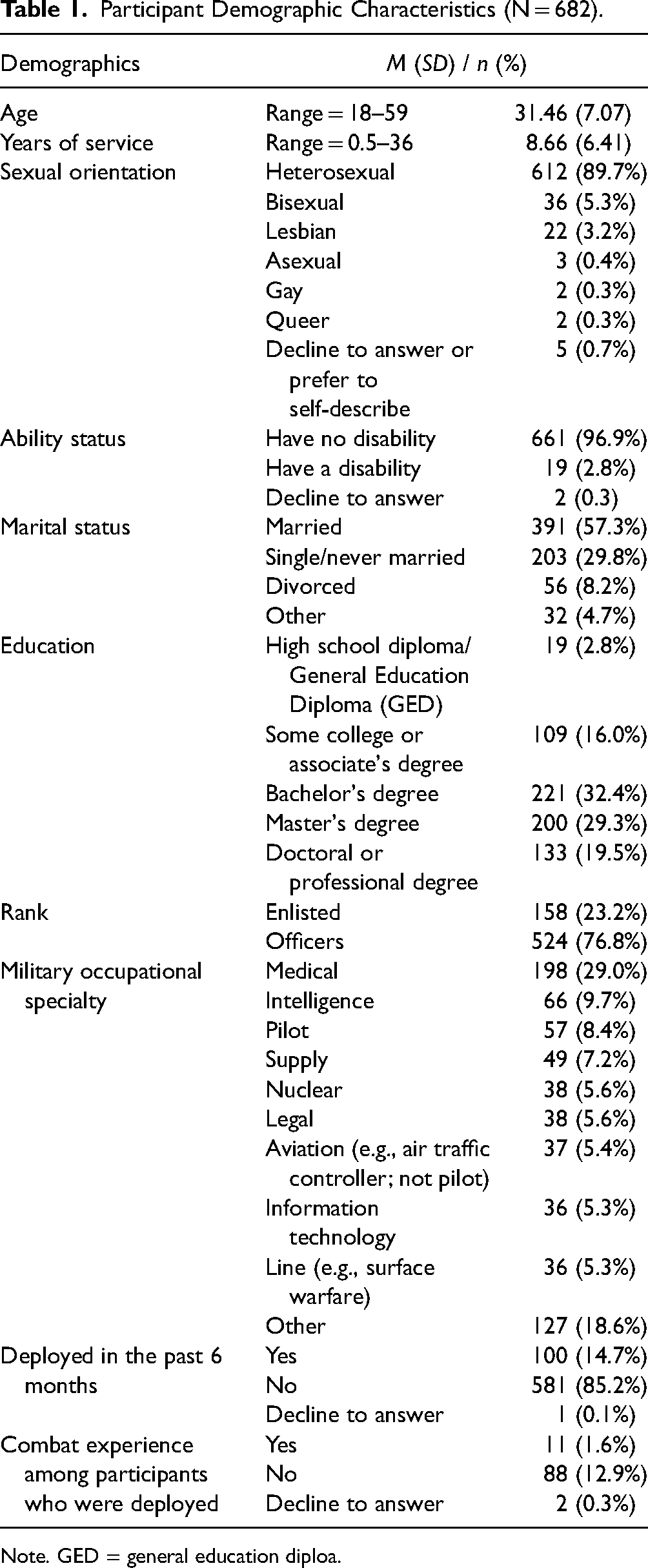
Note. GED = general education diploa.
Measures
Gender Microaggressions That Target Women. We used the FeMS (Miyake, 2018) to assess frequency of women's experiences with gender microaggressions. Although the original scale instructions asked about lifetime experiences, to maximize participant recall of recent military experiences, we modified the instructions to ask participants about their experiences within the past 6 months. The FeMS is a four-point Likert-type scale ranging from 1 (never) to 4 (often/frequently), with higher scores indicating more experiences with gender microaggressions. The FeMS comprises 34 items with eight subscales: sexual objectification (4 items; “I observed someone staring at a woman's body”), assumptions of inferiority/second-class citizen (5 items; “Someone assumed that I am not intelligent because of my gender”), assumptions of traditional gender roles (4 items; “Someone assumed that I am nurturing because of my gender”), invalidation of the reality of sexism (5 items; “Someone told me that sexism is no longer an important social issue”), sexist language (4 items; “Someone called me a ‘bitch’”), implicit threatened physical safety (4 items; “Someone told me not to walk alone because I might be raped or assaulted”), explicit threatened physical safety (4 items; “Someone touched me without my consent”), and environmental (4 items; “I observed in the media that women are not believed when they report being sexually harassed”). Miyake (2018) reported internal consistency estimates for each subscale (α's = .71–.84) among a sample of adult women in the U.S., and she specified the total score could be used. Accordingly, in the present study, we utilized the total scale score (α = .95). Additionally, Miyake found support for construct and criterion-related validity of scores on the FeMS via positive correlations with both sexist discrimination and body surveillance and by demonstrating that FeMS scores predicted body surveillance above and beyond the variance explained by sexist discrimination.
Depressive Symptoms. We used the Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001) to measure the severity of participants’ depressive symptoms. Participants responded to nine items using a four-point Likert-type scale ranging from 0 (not at all) to 3 (nearly every day). To align with 6-month participant reports on the gender microaggressions scale, we adapted the PHQ-9 instructions to consider the past 6 months instead of 2 weeks. Example items include “Little interest or pleasure in doing things” and “Trouble concentrating on things, such as reading the newspaper or watching television.” The internal consistency for scores on the PHQ-9 was .92 for a prior sample of military personnel (Bryan et al., 2014), and internal consistency in the current study was .88. Prior research supported the construct and criterion validity of scores on the PHQ-9. For example, scores were correlated with a major depression diagnosis via structured mental health professional interviews (Kroenke et al., 2001), and PHQ-9 scores predicted general health survey scores (Kroenke et al., 2001; Stewart et al., 1988).
Coping Strategies. We used the Coping Strategies Inventory-Short Form (CSI-SF; Speyer et al., 2016) to assess participants’ frequency of using certain coping strategies in response to stress. The response format is a five-point Likert-type scale ranging from 1 (never) to 5 (almost always). The CSI-SF includes 14 items with four subscales: emotion-focused engagement (EFE; 4 items; “Let my feelings out to reduce the stress”), problem-focused engagement (PFE; 4 items; “Make a plan of action”), emotion-focused disengagement (EFD; 2 items; “Tend to blame myself”), and problem-focused disengagement (PFD; 4 items; “Hope the problem will take care of itself”). Previous research found EFE and PFE positively correlated with wellbeing, whereas EFD and PFD were negatively correlated with wellbeing (Yeh & Chiao, 2013). Prior research provided internal consistency estimates for U.S. adults receiving hemodialysis (EFE α = .78, PFE α = .77, EFD α = .74, and PFD α = .62; Speyer et al., 2016). In the current study, Cronbach's alphas were .78 for EFE, .69 for PFE, .85 for EFD, and .60 for PFD. We excluded the PFD scale from further analysis due to the low alpha. Structural validity of scores on the CSI-SF was supported in prior research by exploratory and confirmatory factor analyses (Speyer et al., 2016).
Procedure
Our university's institutional review board approved the study procedures. We used several recruitment approaches: military-related organization listservs (e.g., APA Society for Military Psychology listserv), Facebook groups (e.g., Female Navy Officers, Army Women's Foundation, and Female Air Force Officers), and the second author's personal Facebook page. To enhance participation, we also employed snowball sampling (Heckathorn, 2011), in which we asked participants to share the survey link with their networks. We offered participants the opportunity to enter a raffle and win one of seventy-two $25 gift cards. We also asked participants to vote for a military organization and donated $100 to the one with the most votes (i.e., American Women Veterans Foundation).
The Qualtrics online survey comprised an informed consent form, demographic questionnaire, FeMS, PHQ-9, and CSI-SF. Out of 918 responses, we excluded participants who did not meet inclusion criteria (i.e. did not have at least 6 months of full-time active duty; n = 34), answered one or more of the attention questions incorrectly (e.g., “Please select ‘never’ if the sky is blue”; n = 187), or answered age inaccurately (n = 2); two participants reported age as 71 and 95 when mandatory retirement age ranges from 62 to 68. We also excluded one participant who self-identified as transgender and did not self-identify as a woman. Additionally, due to their low numbers, we excluded the following from our analyses: Marine Corps (n = 10), Coast Guard (n = 1), and Chief Warrant Officer (n = 1). Thus, the final sample size was 682 participants.
Data Analytic Plan
We used multiple linear regression to test the association between gender microaggressions and depressive symptoms, and we used separate equations to test the role of each moderator on this association. These separate analyses allowed us to focus on specific relations for each moderator and interpret the moderations with clarity. Next, we used SPSS PROCESS macro (Model 1) to test rank and coping strategy as potential moderators of the link between microaggressions and depression (Hayes, 2013). We used 10,000 bootstrap samples to examine p-values and 99% confidence intervals. The bootstrap confidence intervals are statistically significant if the upper and lower intervals do not include zero (Wood, 2005). To reduce the risk of Type I error, we utilized a Bonferroni correction. We analyzed a priori power analysis for interaction effects to assess needed sample size using G*Power version 3.1, which recommended a sample size of 583 based on a .02 effect size (Cohen, 2013), a .01 error probability, and .80 power, and total four predictors (i.e., gender microaggressions, rank, coping style, and interaction term).
Results
We used SPSS 26 to perform data screening and analyses. Missing data were less than 5%, and we used pairwise deletion for participants who did not complete at least 80% of each scale (Schlomer et al., 2010). Per Lorah and Wong's (2018) recommendation, we mean-centered scores on the gender microaggressions scale (FeMS) and our viable coping scales (EFE, PFE, and EFD).
Preliminary Analyses
All variables’ absolute skewness and kurtosis values were below three and 10, respectively, indicating normal distributions. See Table 2 for descriptive statistics and correlations among study variables.
Correlations, Means, and Standard Deviations Among Study Variables.
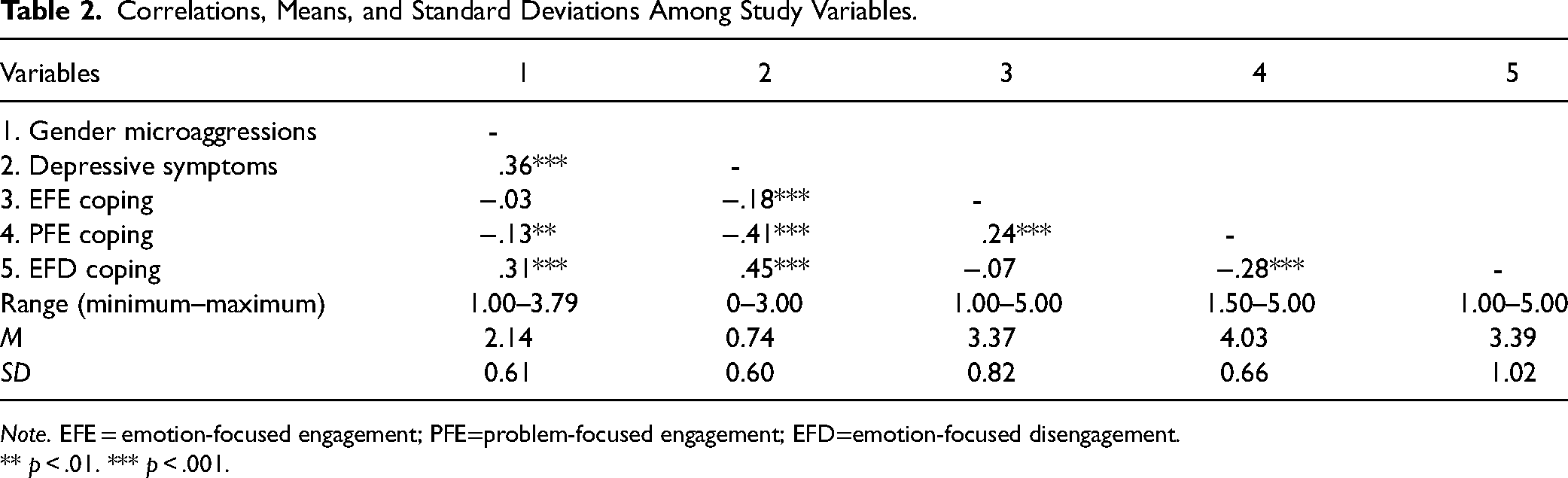
Note. EFE = emotion-focused engagement; PFE=problem-focused engagement; EFD=emotion-focused disengagement.
** p < .01. *** p < .001.
Given the exploratory nature of our study and desire to inform future research in this area, we examined group differences in gender microaggressions and depressive symptoms. We found significant differences on gender microaggressions and depressive symptoms by sexual orientation, branch, and rank. We did not find significant differences by race (see Table 3).
Group Differences in Gender Microaggressions and Depressive Symptoms.
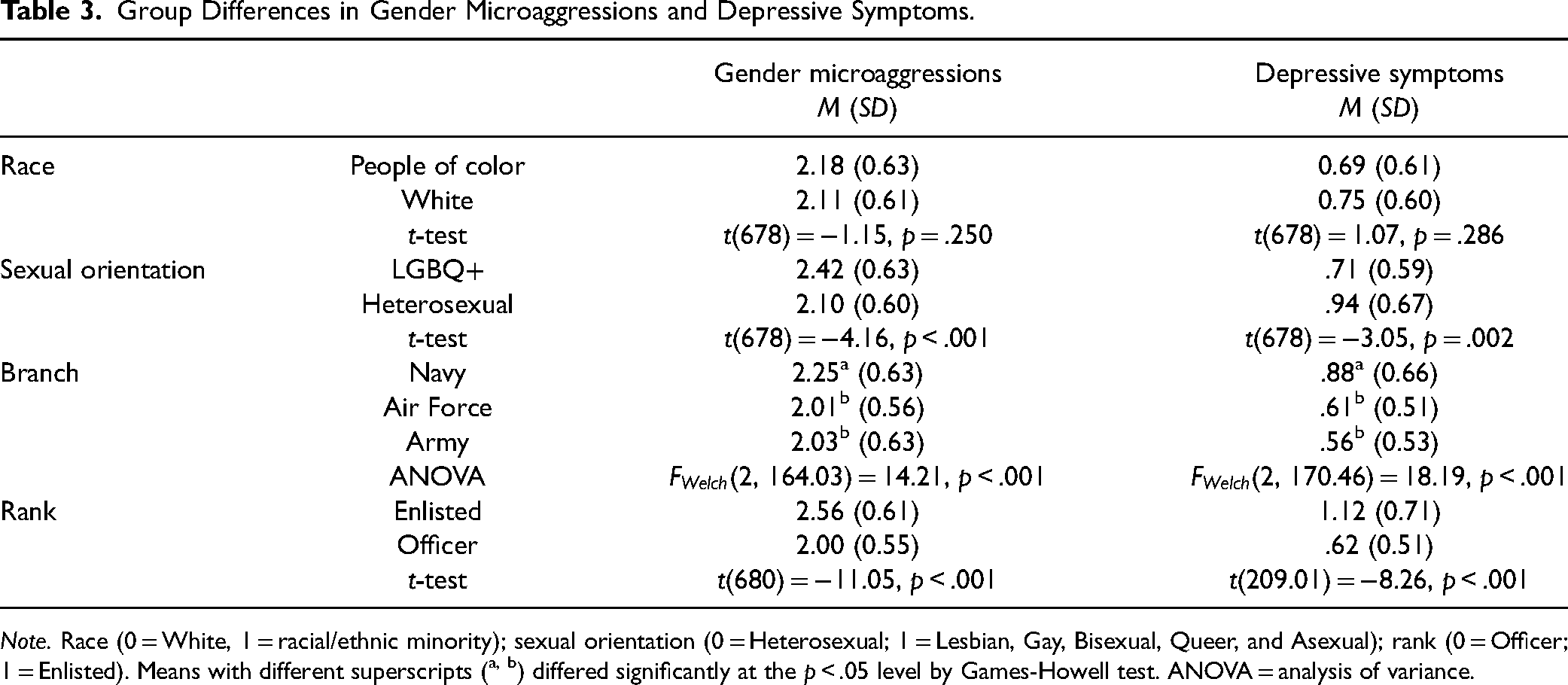
Note. Race (0 = White, 1 = racial/ethnic minority); sexual orientation (0 = Heterosexual; 1 = Lesbian, Gay, Bisexual, Queer, and Asexual); rank (0 = Officer; 1 = Enlisted). Means with different superscripts (a, b) differed significantly at the p < .05 level by Games-Howell test. ANOVA = analysis of variance.
Link Between Gender Microaggressions and Depressive Symptoms
We used multiple linear regression analysis to test the first hypothesis if gender microaggressions predict depressive symptoms. Because the literature suggests the importance of rank in the context of military sexual harassment (Bonnes, 2021), we included rank as a covariate. The model was significant,
Moderating Role of Military Rank
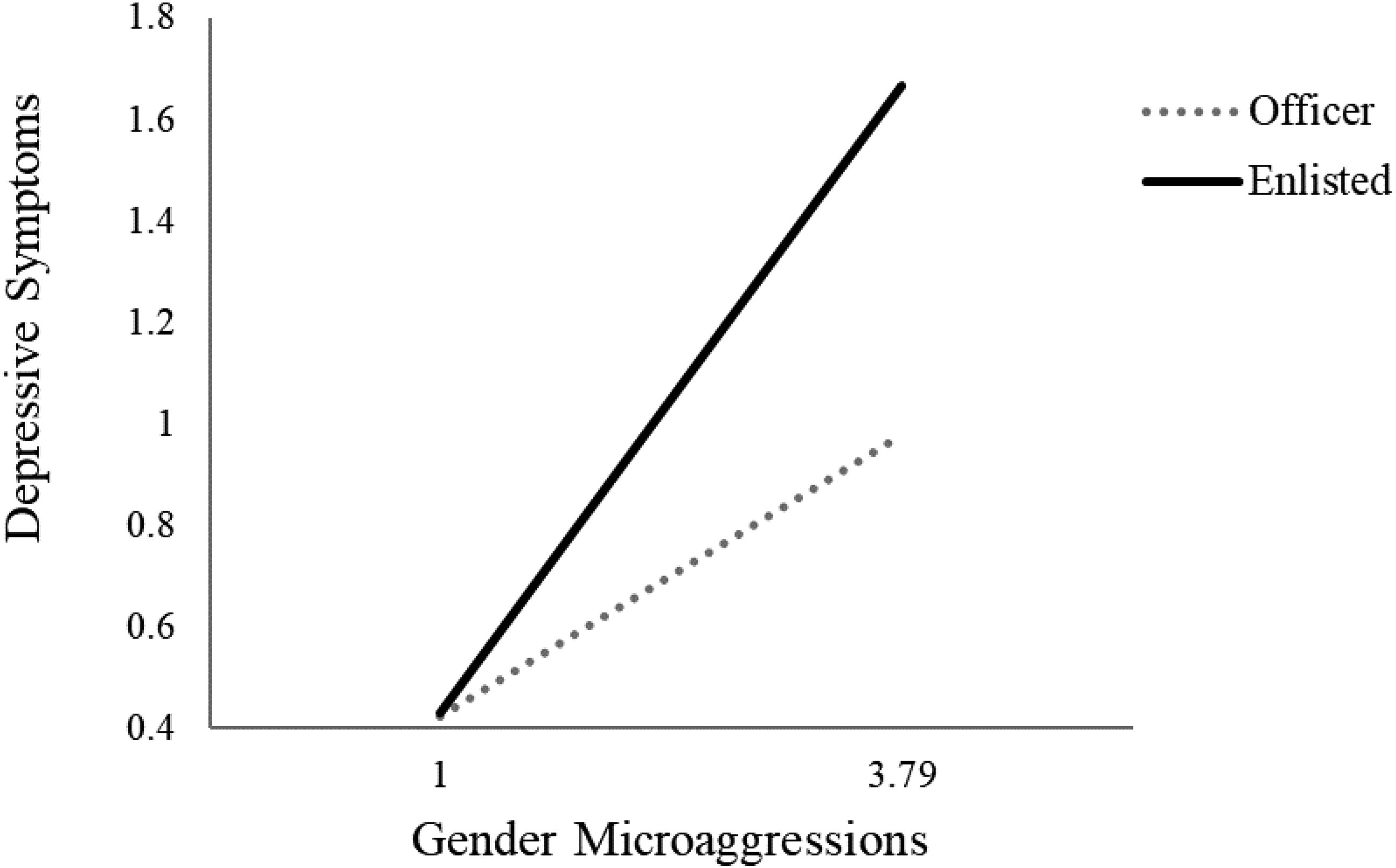
We conducted simple moderation of the PROCESS macro Model 1 (Hayes, 2013) to test our second hypothesis that rank moderated the link between gender microaggressions and depressive symptoms. The model was significant,
Military Rank as Moderator on the Association Between Gender Microaggressions and Depressive Symptoms.
Rank as a Moderator on the Link Between Gender Microaggressions and Depressive Symptoms.
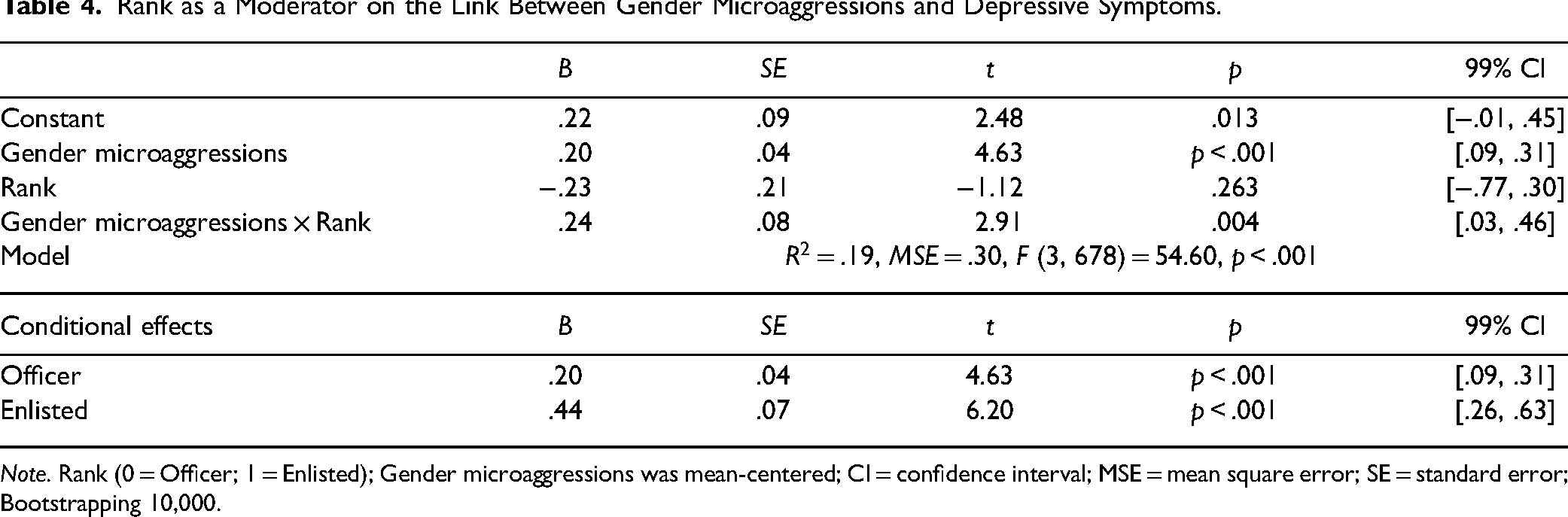
Note. Rank (0 = Officer; 1 = Enlisted); Gender microaggressions was mean-centered; CI = confidence interval; MSE = mean square error; SE = standard error; Bootstrapping 10,000.
Moderating Role of Coping Strategies
We conducted simple moderation of the PROCESS macro Model 1 (Hayes, 2013) to test the third hypothesis that coping strategies would moderate the link between gender microaggressions and depressive symptoms. We included rank as a covariate and conducted separate analyses for each of the three coping moderators.
In the model with EFE as a moderator on the link between gender microaggressions and depressive symptoms, the model was significant,
Coping Strategies as Moderators on the Link Between Gender Microaggressions and Depressive Symptoms.
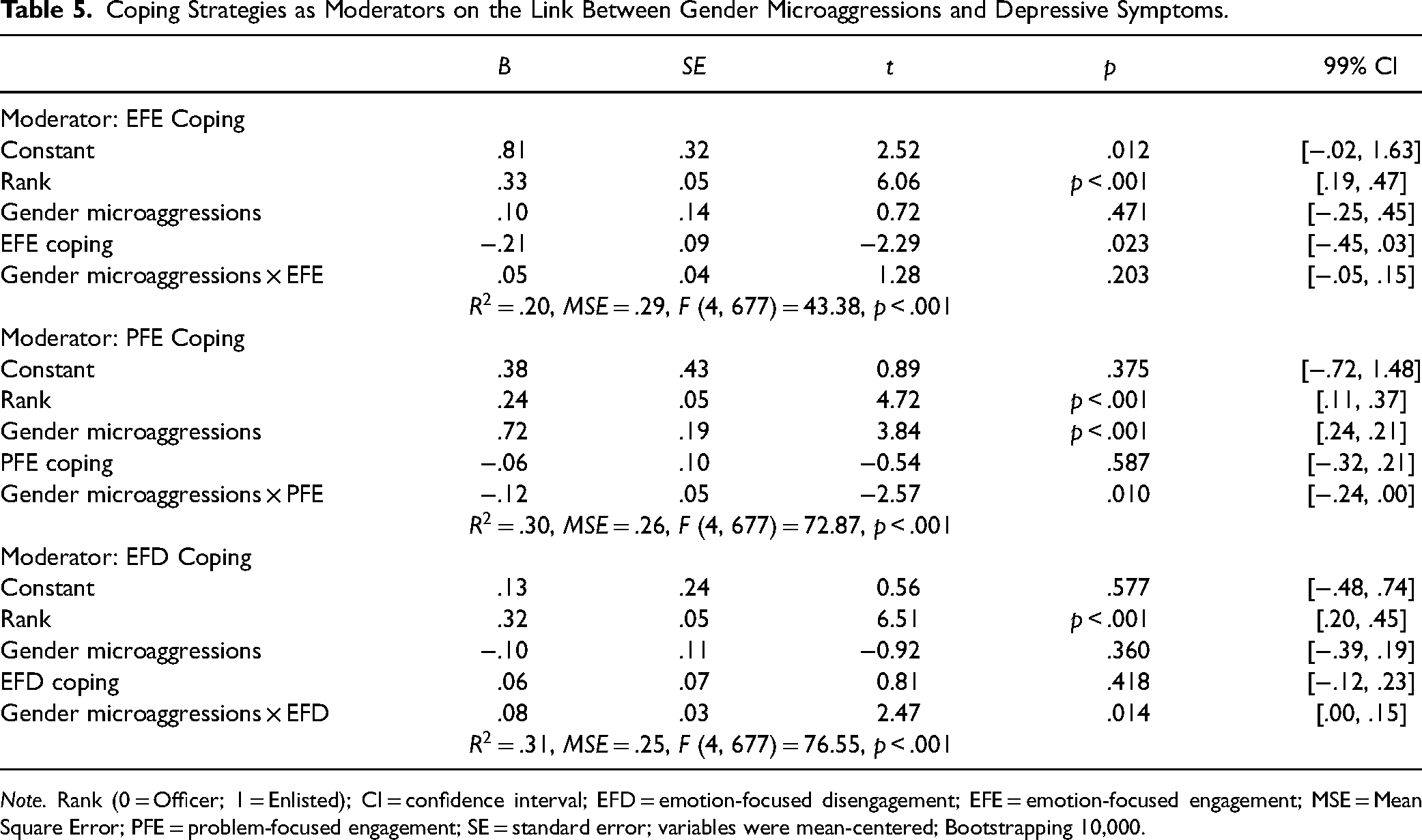
Note. Rank (0 = Officer; 1 = Enlisted); CI = confidence interval; EFD = emotion-focused disengagement; EFE = emotion-focused engagement; MSE = Mean Square Error; PFE = problem-focused engagement; SE = standard error; variables were mean-centered; Bootstrapping 10,000.
When testing PFE as a moderator on the link between gender microaggressions and depressive symptoms, the model was significant,
When testing EFD as a moderator between gender microaggressions and depressive symptoms, the model was significant,
Discussion
This study is among the first to examine active-duty women's experiences with gender microaggressions in the U.S. military. Adding empirical evidence to anecdotal accounts (e.g., Broadwell & Thomas, 2017; Katzenberg, 2019), our results indicate that active-duty women in this sample experienced gender microaggressions in the military workplace. However, mean FeMS scores in the current study (M = 2.14, SD = 0.61) were lower than those in Miyake's (2018) original sample of civilian women (M = 2.69, SD = 0.53). One possible explanation for the lower mean scores is that women in a hypermasculine environment such as the military might need to desensitize themselves to be able to do their jobs. Nevertheless, across these two studies, participants’ mean scores fell between 2 (a little/rarely) and 3 (sometimes/a moderate amount). Additionally, our exploratory analysis of group differences indicated that gender microaggressions scores differed significantly by sexual orientation, branch, and rank. As we hypothesized, greater experiences with gender microaggressions in the military were associated significantly with higher reports of depressive symptoms. This finding aligns with previous studies among civilian samples (Gartner, 2019; Williams & Lewis, 2019). Moreover, we found the link between gender microaggressions and depression was moderated by military rank. Findings have implications for active-duty women, unit cohesion, morale, mission readiness, and performance (Armistead-Jehle et al., 2011; Gaddes et al., 2017; Pflanz & Ogle, 2006).
The Moderating Effect of Military Rank
In the present study, we found that military rank mattered. Specifically, our findings indicated that enlisted (i.e., the lower rank in our sample) experienced greater levels of gender microaggressions and depressive symptoms than officers. This aligns with prior research that junior enlisted military personnel experienced the highest level of depressive symptoms (Bachynski et al., 2012). We also found the link between gender microaggressions and depressive symptoms was significantly stronger among enlisted personnel than among officers. This result is consistent with prior research that found a stronger association between experiences with sexual harassment and psychological distress among lower ranking enlisted women (Buchanan et al., 2008). Enlisted women in our study may have experienced a double stigma of gender and rank (Buchanan et al., 2008). It is also possible that service women in higher ranks might have encountered types of microaggressions that were not captured in our gender microaggressions measure. For example, male subordinates might question or undermine women officers’ leadership (Bagilhole, 2014), which was not captured by the FeMS. Additionally, male subordinates might deliver microaggressions behind women officers’ backs, fearing repercussions due to the power differential.
The Moderating Effect of Coping Strategies
Contrary to our hypothesis grounded in minority stress theory (Brooks, 1981; Meyer, 2003), we did not find a significant moderating effect of any of the coping strategies (PFE, EFE, and EFD) on the link between gender microaggressions and depressive symptoms among active-duty women. When we conducted analyses with a less stringent alpha (.05), we found that problem-focused engagement buffered the association between gender microaggressions and depressive symptoms, whereas EFD exacerbated the link. Because effect sizes for moderators generally are small (Aguinis et al., 2005; Aiken & West, 1991), power to detect such effects is a relevant concern (see Lorah & Wong, 2018). Although we met the terms of our power analysis, future research might seek larger samples to detect moderator effects. As such, the moderating role of coping strategies still might be important to consider further in future research. Because our coping measure was designed for medical patients and did not focus specifically on coping with discrimination, the items we assessed may not be relevant for coping with gender microaggressions. Future research would benefit from using discrimination-specific coping measures.
Limitations and Future Research Directions
Although our findings add to feminist science and the larger gender microaggressions literature by exploring active-duty military women's experiences in a largely unexamined and hypermasculine context, there are several limitations. First, our sample may not be generalizable to all U.S. military women. Our sample was 78.6% White active-duty women, whereas population estimates are 56.7% (DOD, n.d.-a). Additionally, 81.3% of our sample had a college degree or higher, compared to 27.3% of all active-duty women (DOD, n.d.-a). Officers were also overrepresented in our sample (i.e., nearly 75% compared to 19.2% nationally; DOD, n.d.-a). It is possible that our approach to participant recruitment by a U.S. Navy officer influenced the composition of our sample. Because enlisted women were most vulnerable to the negative effects of gender microaggressions, future research would benefit from greater focus on this population. Due to low numbers, we were unable to include Marine Corps and Coast Guard women in our analyses. Because DOD reports indicate that Marines lead all branches in sexual harassment and assault and is the branch with the lowest percentage of women service members (DoD, n.d.-a), we recommend future research includes Marines. Also notable, most of our participants had not been deployed and had not experienced combat. Gender microaggressions may be experienced differently in overseas military operations and combat environments. Finally, we speculate the more masculinized military roles (e.g., Army Rangers, Marine scout snipers, Navy SEALS, and so forth) may situate women in more unwelcoming, hostile, and sexist contexts. Future research should seek more representative samples for those populations.
Future research might also examine how demographic characteristics (e.g., race, sexual orientation, and gender identity) influence the experiences with and effects of gender microaggressions. As Gartner et al. (2020) recommended, future studies may utilize microaggression scales that capture population-specific adaptations (e.g., gendered racial microaggressions; Keum et al., 2018; Lewis & Neville, 2015).
Noted above, our coping strategies measure also presented some limitations. We could not use PFD due to low internal consistency. Moreover, our general measure may not have captured the more specific ways military women cope with gender microaggressions. Thus, we recommend employing additional coping measures and/or using qualitative methods to gain a deeper understanding of coping strategies active-duty women use in response to gender microaggressions. Finally, our focus on individual-level responses to gender microaggressions may not capture collective forms of coping or acknowledge how gender microaggressions are linked to structural oppression (Sue & Spanierman, 2020). Therefore, future research might consider examining community-level coping strategies and collective forms of resistance to gender microaggressions.
Regarding our outcome variable, we only assessed depressive symptoms. Because other psychological (e.g., trauma) and physiological (e.g., sleep disturbances) outcomes may pose challenges to unit cohesion, unit performance, and mission readiness, we recommend future research that assesses a range of outcomes.
Practice Implications
Our results suggest that clinicians should consider the harmful effects of gender microaggressions in the U.S. military. Due to the hypermasculine military culture that minimizes microaggressions and mental health issues, it is possible that active-duty women might not disclose their experiences with microaggressions or their depressive symptoms to their superiors. Clinicians can assist service women in naming their experiences with gender microaggressions and validating their detrimental effects. Support groups might provide a therapeutic setting where women could validate each other. Importantly, because we found enlisted women to be more vulnerable to the effects of gender microaggressions, clinicians should be aware of the potential double stigma these women face (Buchanan et al., 2008). In addition, military policymakers should establish policies and procedures that enable enlisted women to report diverse types of sexist discrimination including gender microaggressions (Rea, 2020) along with other types of sexual harassment, without fear of retaliation.
Although sexual assault and prevention training is required for U.S. service members (DOD Sexual Assault Prevention and Response Office, 2021), gender microaggressions have not been addressed. Certified trainers have been service members who may know little about gender microaggressions theory and research. Therefore, we recommend clinicians work collaboratively with sexual assault and prevention trainers to provide psychoeducation on microaggressions and their adverse effects. Military policymakers involved in sexual assault prevention should consider gender microaggressions, as these subtle forms of sexism reflect underlying cultural issues that can contribute to sexual assault (Gartner & Sterzing, 2016).
Finally, and consistent with Brooks (1981), we do not wish to place the onus on the targets for simply coping with subtle forms of sexism in the military. As the military continues to transition to an increasingly gender-inclusive force, leadership training at every level needs to draw on feminist science to heighten knowledge, awareness, and skills in ways that explicitly respond to gender microaggressions to best support women service members.
Conclusion
The present study is one of the first to document empirically active-duty U.S. military women's experiences with gender microaggressions. Our findings indicate that service women's experiences with microaggressions were associated with depressive symptoms. Additionally, results suggested that the link between gender microaggressions and depressive symptoms was moderated by military rank. Our findings have important implications for active-duty women's individual mental health and likely have implications for unit cohesion, unit performance, and mission effectiveness (Armistead-Jehle et al., 2011; Gaddes et al., 2017; Pflanz & Ogle, 2006).
Footnotes
Author Note
This study is based on Sierra K. Dimberg's doctoral dissertation under the direction of Lisa B. Spanierman at Arizona State University. The views presented are those of the authors and do not necessarily represent the views of the Department of Defense or any of its components. We would like to thank Alisia Tran for her thoughtful feedback on an earlier draft of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.