
Abstract
According to the Center for Disease Control (CDC), the proportion of acquired immunodeficiency syndrome (AIDS) diagnoses among women in the United States has more than doubled between 1984 and 2019 and rates of sexually transmitted diseases (STDs) in all individuals increased 30% between 2015 and 2019. Further, the CDC has designated women ages 13 to 44 years as a group vulnerable to human immunodeficiency virus (HIV) and STD infection, in part due to frequency of engaging in sexual risk behaviors. Sexual self-efficacy is associated with decreased sexual risk behaviors and counters norms that emphasize passivity and compliance as traditional sexual behavior in women. In the current study, we assessed knowledge of HIV and STD transmission and risk factors, sexual self-efficacy, and frequency of sexual risk behaviors in 281 woman-identified respondents aged 18–44 years in an online survey. Knowledge of HIV and STDs was low (averages of 63.3% and 49.9%, respectively). Younger women, and women who identified as single, White, and/or LGBTQ+ reported more sexual risk behaviors. HIV knowledge and sexual self-efficacy were independently associated with fewer risk behaviors and significantly interacted to predict sexual risk behaviors. STD knowledge and sexual self-efficacy were independently associated with fewer sexual risk behaviors. These findings highlight the need for comprehensive, widespread, and identity-inclusive sexual health education.
According to recent reports from the Center for Disease Control (CDC), the proportion of acquired immunodeficiency syndrome (AIDS) diagnoses among women in the United States (U.S.) has more than doubled since the early years of the AIDS epidemic, from 8% in 1984 to 18% in 2019 (Bosh et al., 2021) and rates of sexually transmitted diseases (STDs) in all individuals increased 30% between 2015 and 2019 (CDC, 2022c). In 2020, more than half (57%) of new human immunodeficiency virus (HIV) and AIDS diagnoses were in individuals aged 13 to 34 years (CDC, 2022a). The CDC (2022c) estimates that individuals between the ages of 15 to 24 years acquire half of all new STD diagnoses each year, and approximately 1 in 5 sexually active people have an STD. The CDC has designated women ages 13–44 years as a particularly vulnerable group and identified the continued increase of STDs in the U.S. an epidemic. Given the rates of STDs and HIV infection in the U.S. it is important to understand women's sexual health knowledge and how this knowledge may be associated with sexual risk behaviors. Sexual risk behaviors are activities, such as unprotected sexual intercourse, sexual activity with multiple partners, or intercourse with an intravenous drug user, that increase risk of contracting sexually transmitted infections (Chawla & Sarkar, 2019).
It is also critical to identify potential protective factors that may decrease sexual risk behaviors. For example, there is a growing body of literature that suggests sexual self-efficacy is associated with fewer sexual risk behaviors (e.g., Devieux et al., 2002; Reising et al., 2005). Focusing on women's sexual self-efficacy offers an important feminist counter perspective to ideology or ideas and norms that emphasize passivity and compliance as traditional, normative, and acceptable female behavior (Curtin et al., 2011). Schick et al. (2008) note that many aspects of engaging in safe sex (e.g., negotiating that a male partner wear a condom) require women to advocate for themselves in direct contrast to traditional norms of passive female sexuality. Further, women advocating for safe sex practices may be interpreted as being sexually promiscuous (e.g., if women assert the protection is for both parties) rather than “chaste” from the perspective of traditional gender norms. In contrast, sexual self-efficacy frames engaging in safe sex practices as acting to ensure one's well-being. In addition, sexual self-efficacy provides an alternative to sexual scripts that position women to serve as responsible “gate keepers” (by refusing sex) by promoting women taking steps to enhance their sexual satisfaction and well-being while using safe sex practices.
This study assessed HIV and STD knowledge and sexual risk behaviors in individuals who identify as women aged 18 to 44 years, extending our understanding of sexual health knowledge and risk behaviors beyond college student samples. Further, we examined the extent to which women's sexual self-efficacy is associated independently with decreased sexual risk behaviors and moderates the relation between sexual knowledge of HIV and STDs and risk behaviors.
HIV and STDs in Women
HIV is a virus that attacks an individual's immune system. If untreated, HIV can cause damage to the immune system resulting in AIDS. Approximately 10 in 100 HIV positive women are unaware of their HIV status (CDC, 2022b). In 2019, an estimated 263,900 women in the U.S. had HIV with heterosexual contact serving as the primary form of transmission of infection (86%; CDC, 2022b). A woman is more likely to contract HIV from an infected partner during heterosexual vaginal intercourse (e.g., receptive sex) than a male counterpart. For women ages 13–26 years and women of color, heterosexual transmission rates are even higher at around 90%. In 2020, Black women accounted for 55% of all new HIV diagnoses, despite accounting for only 13% of the U.S. population (CDC, 2022a). HIV infections were next most common in Latina women (21%) while about 16% of women with HIV were White. Poverty is also a social factor linked to HIV vulnerability. For example, one study with 9,078 participants reported the prevalence of HIV among individuals living in poverty was nearly 20 times the national average in the U.S. (Denning & DiNenno, 2017).
STDs represent a broad range of infections that can be transmitted person-to-person through sexual contact. This may include kissing, oral-genital contact, genital-genital contact, use of sexual toys, as well as penetrative sexual contact (CDC, 2021). Within the U.S., human papillomavirus (HPV, 42.5 million), chlamydia (2.4 million), HIV (984,000), gonorrhea (209,000), and syphilis (156,000) are the most common STDs (CDC, 2020c). Similar to the disproportionately higher rates of HIV among women of color, STDs such as chlamydia, gonorrhea, and syphilis are 5 to 7 times higher among Black women and 1.4 to 2.2 higher in Latina women than White women (CDC, 2020a, 2020b).
In addition, compared to men, women disproportionately bear the long-term consequences of STDs (CDC, 2019). Several types of STDs cause pelvic inflammatory disease (PID), which leads to infertility for an estimated 24,000 women in the U.S. each year. Thousands more will experience ectopic pregnancy as a consequence of PID. Finally, HPV, which can lead to cervical cancer in women, is the most common STD (i.e., up to 85% of sexually active adults will contract it in their lifetimes).
HIV and STD Knowledge and Risk Behaviors
Given the rates of HIV and STDs, it is important to understand women's knowledge of STD and HIV risk factors for transmission. However, it is unclear to what extent sexual health information is routinely provided in the U.S. A 2018 review of nationwide school curriculums found that fewer than half (43%) of high schools and 18% of middle schools teach key CDC-identified topics for sexual health education (National Health Education Standards, 2019). Next, data on women's knowledge of HIV/AIDS is sparse. Research in the past decade suggests that young adults have lower levels of HIV knowledge compared to older samples (Haile et al., 2017; Shiferaw et al., 2015). In addition, pervasive misconceptions about HIV transmission continue to exist among young adults, such as the belief that sharing utensils or a bathroom with a person with HIV can lead to contraction of HIV (Demmer & Caroleo, 2001), or that spermicidal jellies or foams prevent sexual transmission of HIV (Lewis et al., 2009).
In addition to understanding current levels of knowledge of HIV and STD risk factors for transmission, it is important to assess the frequency and range of sexual risk behavior among young adult women. In a recent study with 1,534 college women, the most common sexual risk behaviors reported were using alcohol prior to sex in the last 6 months (52.1%), sex with someone who has had many sexual partners (35.5%), sexual contact with someone who is not well-known (28.6%), and sex without discussing sexual history (26.2%, Rudolph et al., 2020). However, there are comparatively few studies assessing women's sexual risk behaviors in the U.S., particularly with samples recruited outside of college.
Sexual Self-Efficacy
One variable that may reduce sexual risk behaviors is women's sexual self-efficacy. A number of feminist theorists have noted the key role of feminist and sex positive approaches that reject sexual scripts of female passivity in sexual roles and instead promote sexual agency and choice as avenues to increase women's sexual health (Bay-Cheng & Zucker, 2007; Eisele & Stake, 2008). Bay-Cheng and Zucker note common sexual scripts stigmatize and restrict women's sexual agency by emphasizing female subordination. In contrast, sexual self-efficacy provides an alternative framework that positions women as sexual decision makers.
In the context of sexual education, social cognitive theory (Bandura, 2001) posits that individuals must understand themselves to be self-efficacious agents, who feel competent in sexual health knowledge and are able to incorporate this information despite individual, partner, or structural-level challenges (DiClemente & Wingood, 1995). Given that social cognitive theory posits that both knowledge and perceptions of competency are necessary ingredients for engaging in health promotive behaviors, we anticipated that engagement in risk behaviors would vary depending on the level of knowledge and self-efficacy. Utilizing a definition of sexual self-efficacy as the belief in one's ability to successfully accomplish behaviors and manage affective responses in a sexual context (Bailes et al., 1998), we anticipated the fewest risk behaviors would be reported at high levels of knowledge and sexual self-efficacy.
From a feminist perspective, sexual self-efficacy offers an alternative to traditional social and gendered norms of women as passive and agreeable in sexual interactions and instead positions women to be agentic actors who engage in negotiation to ensure their sexual wellbeing (Schick et al., 2008). Hewitt-Stubbs et al. (2016) discussion of girls’ sexuality offers an important conceptualization of girls as sexual subjects (rather than sexual objects) and draws on the literature to provide a description of sexual subjectivity that includes feeling entitled to experience sexual pleasure and agency to make sexual health decisions. They describe findings of qualitative studies that suggest women report more difficulty communicating their sexual desires and needs than men and assert that developing a sense of oneself as a sexual subject who makes active sexual choices is key for sexual pleasure and safety.
Similarly, Bowleg et al. (2000) note that sexual self-efficacy requires cooperation between partners and found that in a sample of predominantly women of color, relationship power, or the ability to communicate directly about sexual needs and wants with a partner, was significantly associated with sexual self-efficacy. Additional research has demonstrated that women with self-efficacious communication skills are better able to negotiate with sexual partners on sexual preferences as well as safety precautions (Valera et al., 2017). In addition, HIV sexual knowledge is positively associated with women's self-efficacy for condom use (Curtin et al., 2011), higher sexual self-efficacy is associated with fewer HIV risk behaviors (Devieux et al., 2002), and numerous studies have identified low sexual self-efficacy as a predictor of risky sexual practices in undergraduate populations (e.g., Reising et al., 2005). Finally, drawing on data from the U.S. National Longitudinal study Adolescent Health Survey, Cheng et al. (2014) found that girls with higher sexual self-efficacy reported greater well-being as well as more condom use and lower rates of teen pregnancy.
Much of the existing literature on sexual self-efficacy focuses on assessing agency for engaging health-protective behaviors (wearing condoms, discussing sexual histories prior to sex, etc., Rocha-Rdz et al., 2017). However, recent efforts in sexual self-efficacy have broadened assessment to include satisfaction in sexual relationships, preventing sexual assault, and sexual equality/diversity (Koch et al., 2004). This broader definition is consistent with feminist calls for including women's sexual well-being and satisfaction in assessments of sexual self-efficacy (e.g., Hewitt-Stubbs et al., 2016) rather than narrowly focusing on safe sex practices.
Current Study
Although STD and HIV rates in women are rising, women's knowledge of specific precautions and risk factors for HIV and STD infection is unclear. In the current study, we explored women's sexual health knowledge and engagement of risk behaviors and evaluated the relation between sexual health knowledge and sexual risk behaviors among woman-identified individuals between the ages of 18–44 years. We also examined the extent to which individuals’ demographic characteristics and social identities were associated with HIV knowledge, STD knowledge, sexual self-efficacy, and risk behaviors. These analyses were exploratory given the limited literature focused on women's sexual knowledge, sexual self-efficacy, and sexual risk behaviors. Identifying social identities or demographic characteristics associated with sexual knowledge or risk behaviors could serve to inform prevention and sexual health education outreach. Next, we evaluated the potential moderating effect of sexual self-efficacy between sexual health knowledge and risk behaviors. We hypothesized that sexual self-efficacy would interact with HIV and STD knowledge to predict decreased risk behaviors, such that higher levels of respective knowledge and higher self-efficacy would be associated with fewer risk behaviors, and lower knowledge and lower self-efficacy would be associated with a greater number of risk behaviors. The expectation that self-efficacy would interact with HIV and STD knowledge level was based on prior findings that HIV knowledge and sexual self-efficacy were associated (Curtin et al., 2011) and the social cognitive theory argument that both sexual health knowledge and self-efficacy are necessary to engage in behaviors to promote sexual health.
Method
Participants
Power analyses were conducted via G*Power (Faul et al., 2009). For a linear multiple regression, in order to detect a moderate effect (0.15) with up to seven predictors, with alpha set to 0.05 and at 95% power, a sample size at least 153 was required for the proposed analyses. To improve the validity of online platform data collection, four attention check questions (i.e., “Please select answer ‘C’”) and one seriousness check (i.e., “I have taken part seriously”) question were included in line with Aust et al.'s (2013) recommendations. Eleven participants were excluded due to failing one or more attention checks, three participants were excluded due to failing the seriousness check, and five participants were excluded for selecting “married” on the demographics questionnaire, leaving a final N of 281 (Mage = 29.71, SDage = 6.16).
Participants reported a wide range of employment statuses, education levels, and annual incomes (see Table 1). The majority of the sample (n = 179, 63.7%) were currently single, and 105 (37.2%) were in a relationship. Next, 72.2% of the sample identified as heterosexual, and 72.6% of the sample identified as White. Last, 96.8% of this sample was assigned female at birth.
Sample Characteristics.
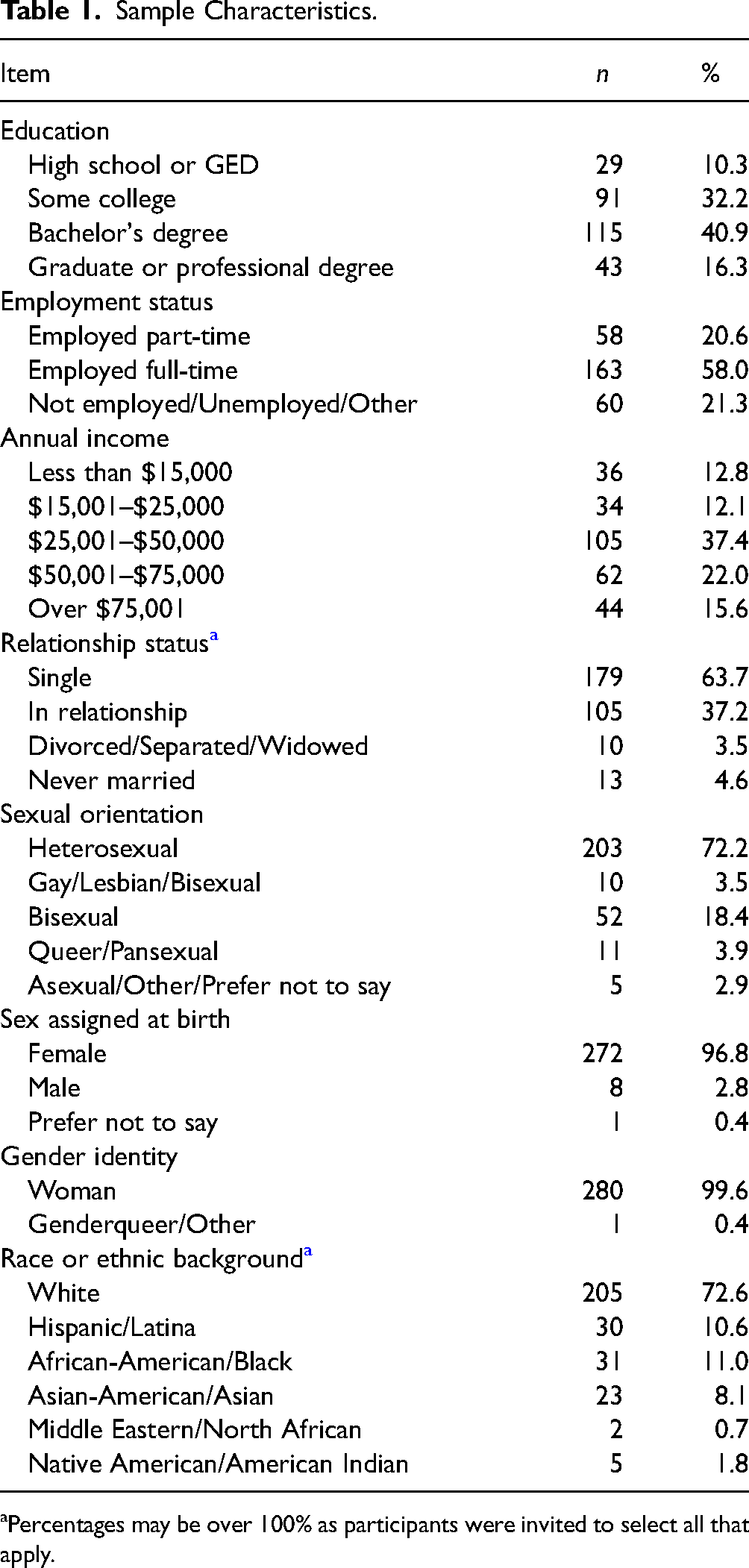
Percentages may be over 100% as participants were invited to select all that apply.
Measures
Sexual Health and Behavior Survey
There is a notable dearth of standardized measurements for condom usage, STD, and HIV-risk behaviors (Noar et al., 2006; Schroder et al., 2003). Fonner et al. (2014) made recommendations for measures to include items in three key areas: (1) condom use at last sex, (2) consistent condom use, and (3) number of protected and unprotected sex acts. Type of sex (i.e., vaginal, oral, or anal) should also be specified, and response choices should avoid dichotomous responses (Fonner et al., 2014). These recommendations were incorporated into this study's measure. Consistent with the United Nations General Assembly Special Session guidelines, condom usage and HIV risk behaviors were assessed through 27 questions adapted from the CDC (2011) Sexual Behavior Questionnaire. Questions assessed number of sexual partners, frequency of sexual acts, frequency of condom usage, current or past risk behaviors (i.e., drug use, tattooing, etc.), and sexual contact with others who have risk factors. The time frame for this measure was modified from the past one year to past two years, based on the timing of the COVID-19 pandemic and the potential impact of significantly reduced social contact for many people. The following is an example item from the measure: “To the best of your knowledge, how many times in the last 24 months (2 years) did you have sexual intercourse with partners who injected non-prescription drugs?” In line with the CDC's scoring of this measure, for the purposes of this study, endorsement of each sexual risk behavior was summed for a total possible score of 22. Chronbach's alpha was 0.89.
The HIV Knowledge Questionnaire-18 (HIV-K-Q)
General knowledge regarding aspects of HIV infection was assessed with the HIV Knowledge Questionnaire-18 (Carey & Schroder, 2002). This is an 18-item measure of knowledge about sexual transmission (e.g., vaginal, oral, or anal), prevention (e.g., condom use, monogamy, etc.), and consequences (e.g., treatment, disease course) of HIV infection. For example, items include “A woman cannot get HIV if she has sex during her period,” and “Showering, or washing one's genitals/private parts after sex keeps a person from getting HIV.” Participants may respond with true, false, or don’t know, to statements in these areas. Total scores are obtained by summing the total correct items (0–18 range) with higher scores reflecting greater knowledge. Carrey et al. provided support for internal consistency reliability (α’s ranged from 0.75 to 0.89 across three samples) and test-retest reliability over one (r = .94) and three (r = .76) week intervals. The subscales of this briefer version of the HIV-K-Q correlate highly (.93 to .97) with the validated 45-item HIV-K-Q, suggesting it assesses the same dimensions of knowledge. For the current study, Chronbach's alpha was 0.86.
STD Knowledge Questionnaire
The STD Knowledge Questionnaire (STD-K-Q; Jaworski & Carey, 2007) measures general knowledge about transmission, prevention, and causes of the six most common STDs (i.e., chlamydia, genital herpes, gonorrhea, hepatitis B, HIV, and human papillomavirus) within the U.S. with 27 items. Example items include “A man must have vaginal sex to get genital warts” and “Having anal sex increases a person's risk of getting Hepatitis B.” Like the HIV-K-Q, respondents indicate true, false, or don’t know. Total correct responses are summed [0 to 27 range] and higher scores reflect greater STD knowledge. Jaworski and Carey (2007) provided support for internal consistency (r = .86), test-retest reliability over a 2-week period (r = .88), and construct validity via sensitivity to change following an educational STD program. Given that no other broad assessment of STD knowledge exists, convergent validity was assessed via the HIV-K-Q 18, with a Pearson correlation coefficient of 0.64. For the current study, Chronbach's alpha was 0.91.
Sexual Health Practices Self-Efficacy Scale
Sexual self-efficacy was assessed via the Sexual Health Practices Self-Efficacy Scale (SHPSES; Koch et al., 2004; as cited in Fisher et al., 2010). The SHPSES consists of 20 items representing a variety of sexual health practices in six subscale areas: sexual relationships, sexual health care, sexual assault, safer sex, sexual equality/diversity, and abstinence. Respondents indicate their confidence in performing these practices, on a scale from 1 (not at all confident) to 5 (extremely confident). Confidence is defined as having the knowledge, skills, practice, and comfort necessary to carry out the sexual health practice (Fisher et al., 2010). Example items include “Talking with a (prospective) sexual partner about your sexual histories,” and “Negotiating with a sexual partner to practice safer sex.” Total scores for this measure are obtained by summing the individual items and range from 20 to 100 (highest self-confidence). Chronbach's alpha for the current study was 0.92.
This measure demonstrates good convergent validity with other measures of sexual self-efficacy (e.g., the Sexual Risk Behavior Beliefs and Self-Efficacy Scales; Basen-Engquist et al., 1999). Among university samples, this measure has also demonstrated the ability to discriminate between participants that have taken sexual health classes and those who have not, and has shown positive correlation with actual practice of safer sexual behaviors in the month following its administration (Milstein, 2006). Koch et al. reported a Chronbach's alpha of 0.89. For the current study, alpha was 0.92.
Procedure
Participants were eligible for the study if they identified as a woman, were between the ages of 18–44 years, were not currently married, and had been sexually active, in-person, with at least one other person in the past 2 years. We recruited participants from Amazon's Mechanical Turk (MTurk) internet-based platform. This sample was restricted to U.S. participants only. Individuals elect to participate in surveys and other tasks in a “crowdsourcing marketplace” for compensation. Extant data indicate that MTurk participants offer a broad range of sociodemographic diversity for researchers that can exceed convenience sampling, while allowing for more efficient and cost-effective data collection (Buhrmester et al., 2017). In line with recommendations from other MTurk research, participants were required to have at least a 95% approval rating on MTurk as these workers score better on measures of attentiveness compared to those with a < 94% approval ratio (Peer et al., 2017). Workers who have completed at least 100 tasks and have had completion approved for 95 or more tasks are given this rating. Participants were compensated $0.50 for completing the survey.
Participants completed the survey measures via Qualtrics in March and April 2021. All questionnaires and attention checks were administered in randomized order, with the exception of a seriousness check that was administered at the end of participation. Four attention-check questions were inserted randomly throughout the survey (Aust et al., 2013). Participants were required to score 100% on all the attention and seriousness items. In addition, participants were required to take more than 7 min to be over the minimum seconds-per-item response time (Cobanoglu et al., 2021). The average time for completion in this sample was 28 min, 31 s. Additionally, participants were required to use a unique IP address within the U.S. (Aguinis et al., 2021; Cobanoglu et al., 2021). Finally, consistent with the Transparency and Openness Promotion guidelines, we report all excluded data, total and final sample size, and measures used to test the study hypotheses. The research hypotheses were pre-registered. The data is available via the Open Science Framework at https://osf.io/pxq82.
Results
Descriptive Statistics
With regard to sexual health history, 47.3% (n = 133) of participants had ever been tested for HIV/AIDS, and 155 (55.2%) had been tested for STDs/STIs. Within the total sample, seven participants (4.9%) reported that they were HIV positive. Additionally, the following lifetime positive results were reported for the following STDs/STIs: chlamydia (n = 32, 11.3%), gonorrhea (n = 10, 3.6%), genital herpes (n = 14, 5.0%), genital warts or HPV (n = 18, 6.4%), hepatitis B (n = 6, 2.1%), and syphilis (n = 6, 2.1%).
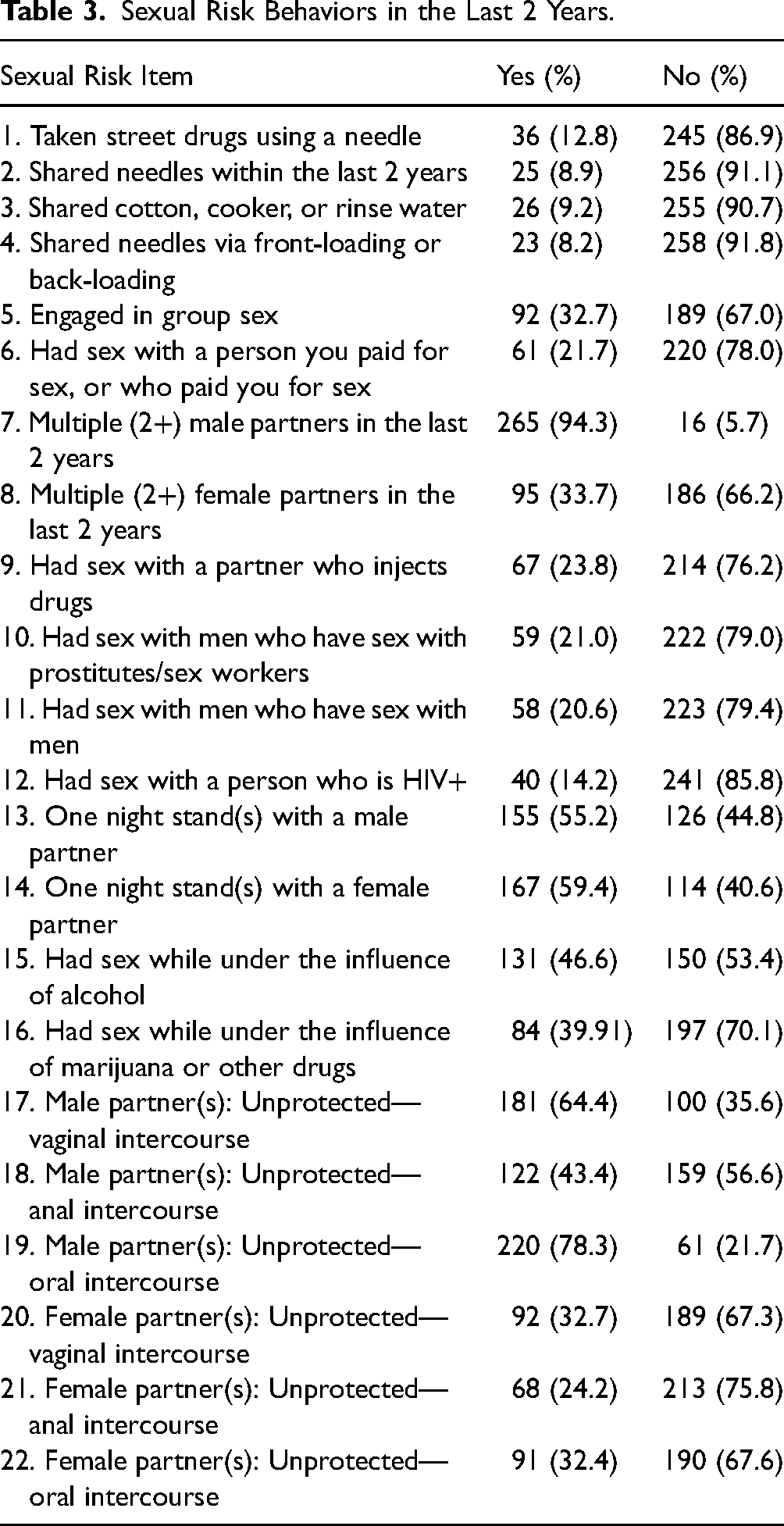
Correlations among study variables and means and standard deviations are provided in Table 2. On the Sexual Health and Behavior Survey, participants reported a mean of 7.68 sexual risk behaviors (SD = 5.08) within the last 2 years. Consistent with previous research, the most common risk behaviors within this sample were sex with multiple (i.e., 2 or more) male partners (n = 265, 94.3%), and unprotected oral sex (n = 220, 78.3%) and vaginal sex (n = 181, 64.4%) with male partners. See Table 3 for incidence rates of all risk behaviors.
Descriptive Statistics and Correlations Among Key Variables (N = 281).
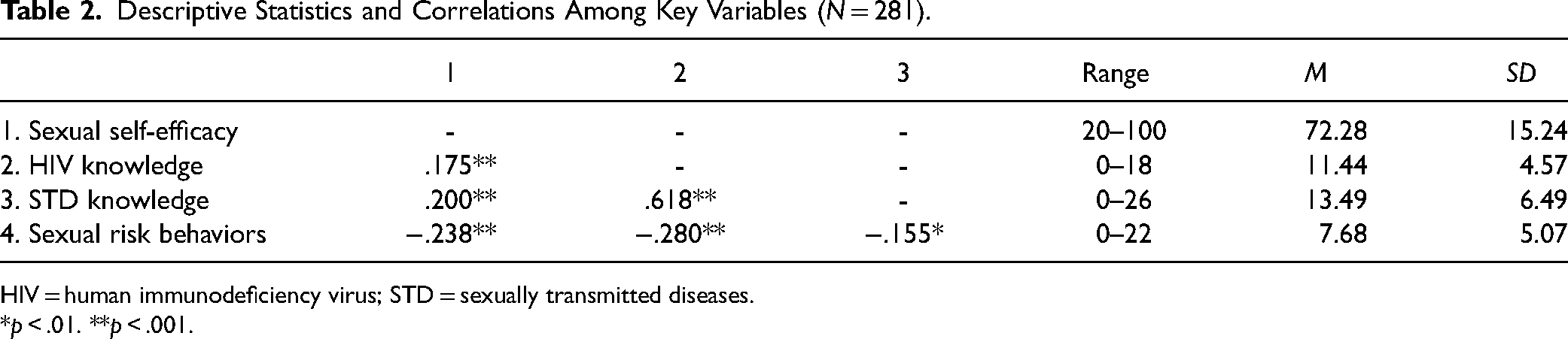
HIV = human immunodeficiency virus; STD = sexually transmitted diseases.
*p < .01. **p < .001.
Sexual Risk Behaviors in the Last 2 Years.
Next, participants reported an average age of initial sexual contact at 16.33 years (SD = 4.19), and 169 (60.1%) reported using a condom when they had sexual intercourse for the first time. Over the last 2 years, 35.2% (n = 99) reported “never” carrying condoms. For participants who had sexual intercourse with a new partner in the last 2 years, 36.3% (n = 102) did not discuss sexual histories. Given this data was collected during the COVID-19 pandemic, participants reported the following regarding their current in-person sexual activity compared to prior to the pandemic: greatly increased (8.2%), somewhat increased (15.7%), stayed the same (37.7%), somewhat decreased (19.9%).
Knowledge about HIV and STDs was generally low within this sample. On the HIV-K-Q, respondents scored an average of 11.44 (SD = 4.58) items correctly, corresponding to a score of 63.3% on the measure. Eleven (3.9% of sample) respondents received a score of 100% on this measure. Knowledge about STDs was lower. Respondents scored an average of 13.49 (SD = 6.48, 49.9%) items correctly on the STD-K-Q. Six (2.1% of sample) scored above a 90%.
Associations Between Demographic and Identified Variables
Age was significantly correlated with STD knowledge (r = .186, p = .002) as well as HIV knowledge (r = .140, p = .019) such that older participants indicated greater knowledge. Race was significantly associated with sexual risk behaviors, such that White women (M = 8.22, SD = 5.35) had significantly higher numbers of sexual risk behaviors than women on color, M = 6.55, SD = 4.25, t(279) = 2.61, p = .005. Relationship status was related to several variables, such that individuals who were single reported a greater number of sexual risk behaviors, t(253) = 3.13, p = .002, lower sexual self-efficacy, t(252) = −2.19, p = .03, and lower STD knowledge, t(253) = −2.10, p = .04, than individuals in a relationship. Sexual orientation was significantly associated with STD knowledge as well as sexual risk behaviors, such that individuals who identified as heterosexual had fewer sexual risk behaviors, t(279) = −4.16, p < .001, and lower STD knowledge, t(279) = −2.06, p = .02, compared to individuals who identified with other sexual orientations.
Primary Analyses
Moderation analyses were selected a priori to data collection. The hypothesized models were evaluated using SPSS statistical software, version 23 (IBM, 2015) and the PROCESS macro version 3.5.3 (Hayes, 2017) with 10,000 bootstrap confidence intervals. PROCESS is a regression path analysis modeling tool that is widely used to test moderation models.
HIV Knowledge
First, a model with HIV knowledge, sexual self-efficacy, and the interaction of HIV knowledge and sexual self-efficacy predicting sexual risk behaviors was tested. Race/ethnicity, relationship status, and sexual orientation were included as covariates. Given the limited research in this area, covariates were identified and included on the basis of the preliminary analyses. The full model was significant, F(6, 247) = 14.19, p < .0001, R2 = .256. The main effect of HIV knowledge on sexual risk behaviors was significant, ß = −0.296, t(247) = −4.62, p < .0001, 95% CI [−0.422, −0.170], such that for every one standard deviation increase in HIV knowledge, there was a decrease of 0.296 sexual risk behaviors. The main effect of sexual self-efficacy on sexual risk behaviors was also significant, ß = −0.063, t(247) = −3.37, p = .0009, 95% CI [−0.101, −0.027]. Sexual orientation ß = 3.56, t(247) = 5.47, p < .0001, 95% CI [2.28, 4.85], relationship status ß = −1.45, t(247) = −2.35, p = .019, 95% CI [−2.68, −0.237], and race/ethnicity ß = −1.75, t(247) = −2.84, p = .0009, 95% CI [−2.96, −0.542] were all significant covariates in the model. The interaction of sexual self-efficacy and HIV knowledge was significant, ß = 0.0076, t(247) = 1.95 p = .05, 95% CI [0.0001, 0.0152], change in R2 = .0115, indicating that the moderation model was supported (see Figure 1). Figure 1 illustrates that at low levels of HIV Knowledge and low levels of self-efficacy, we see the highest rates of risk behaviors, and at high levels of sexual self-efficacy and HIV knowledge, we see the lowest levels of risk behaviors, as predicted.
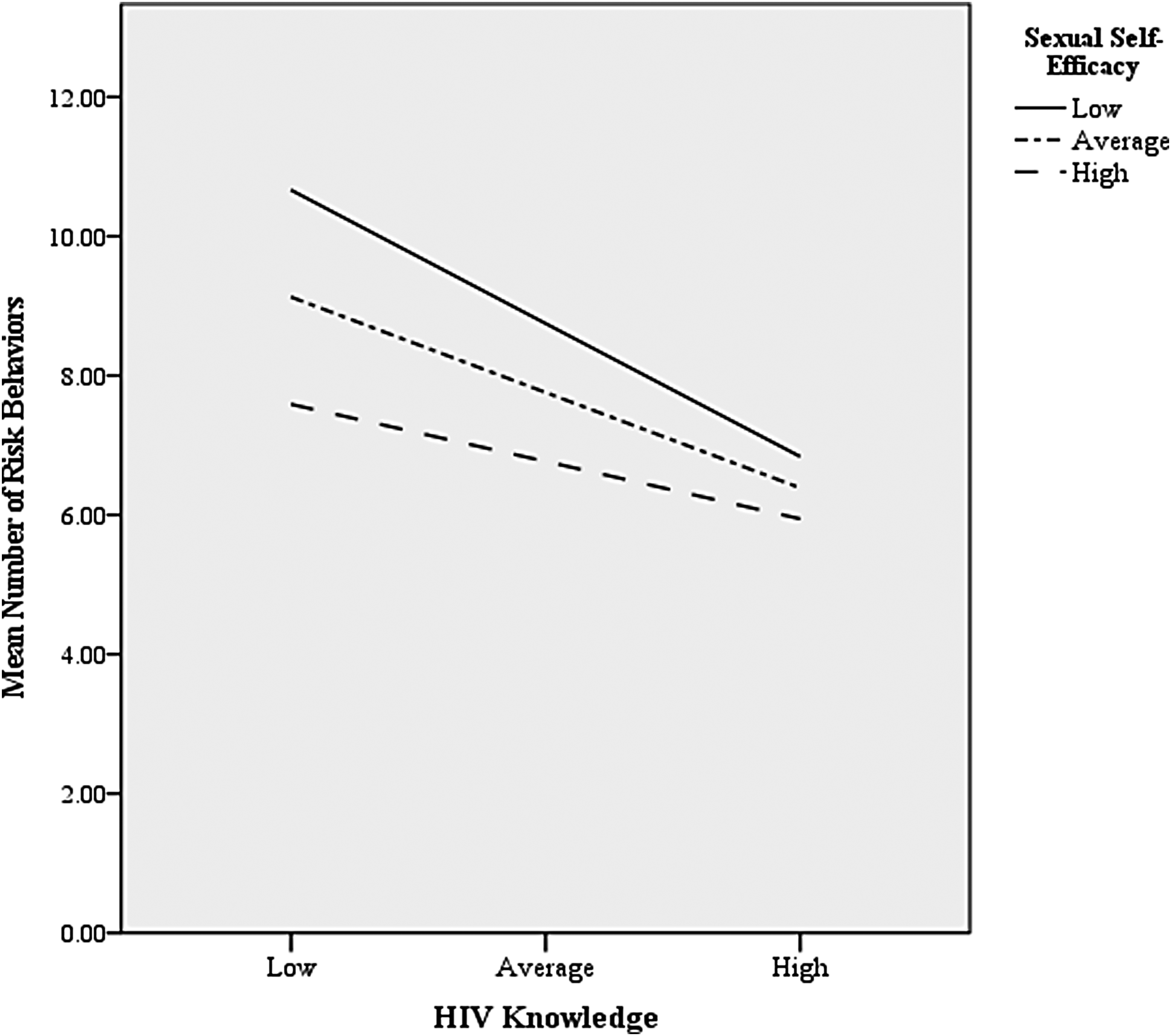
Interaction of HIV Knowledge and Sexual Self-Efficacy Predicting to Sexual Risk Behaviors.
STD Knowledge
Second, we examined STD knowledge, sexual self-efficacy, and the interaction of STD knowledge and sexual self-efficacy as predictors of sexual risk behaviors. Race/ethnicity, relationship status, and sexual orientation were included as covariates. The full model was significant, F(6, 247) = 10.27, p < .0001, R2 = .199. The main effect of STD knowledge on sexual risk behaviors was significant, ß = −0.107, t(247) = −2.24, p = .03, 95% CI [−0.202, −0.013]. For every one standard deviation increase in STD knowledge, there was a 0.107 unit decrease in sexual risk behaviors. Similarly, sexual self-efficacy had a significant effect on sexual risk behaviors, ß = −0.072, t(247) = −3.66, p = .0003, 95% CI [−0.111, −0.033], such that for every one standard deviation increase in sexual self-efficacy, there was a 0.072 unit decrease in sexual risk behaviors. Sexual orientation ß = 3.32, t(247) = 4.91, p < .0001, 95% CI [1.989, 4.652], relationship status ß = −1.59, t(247) = −2.46, p = .014, 95% CI [−2.863, −0.319], and race/ethnicity ß = −1.89, t(247) = −2.95, p = .003, 95% CI [−3.152, −0.630] were all significant covariates in the model. The interaction between STD knowledge and sexual self-efficacy was not significant, ß = −0.0004, t(247) = −2.46, p = .89, 95% CI [−0.006, 0.005]. Thus, while STD knowledge and sexual self-efficacy were independently related to sexual risk behaviors, there was not support for the hypothesized moderation.
Discussion
The current study examined HIV and STD knowledge, sexual self-efficacy, and their relations with sexual-risk behaviors among woman-identified individuals aged 18 to 44 years. HIV knowledge and sexual self-efficacy independently were associated with fewer risk behaviors as well as significantly interacted to predict fewer sexual risk behaviors whereas STD knowledge and self-efficacy were related to fewer risk behaviors independently. Novel to this study were the inclusion of a non-college sample, evaluation of a breadth of sexual risk behaviors, and assessment of sexual self-efficacy as a predictor of a range of sexual risk behaviors. Additionally, the measure of sexual self-efficacy used in this study captured women's sexual health practices across multiple domains. This broader assessment of sexual self-efficacy includes recognition of women's agency related to their sexual satisfaction and equity in relationships as well as sexual safety and reflects feminist calls to change how we conceptualize and discuss women's sexual behaviors (Bay-Cheng & Zucker, 2007).
Sexual Health and Risk Behaviors
Assessment of sexual risk has most frequently focused on unprotected sex and condom use as this provided a concrete and measurable way to address transmission via bodily fluids (Fonner et al., 2014). However, scholars have lamented the lack of data surrounding broader sexual risk behaviors, particularly as condoms may not be fully effective against STDs that can be contracted via other means of contact (CDC, 2021). In the current study, we aimed to address this gap in the literature by measuring a broader range of sexual risk behaviors within the last 2 years.
The Sexual Health and Behavior survey used in our study assessed incidence of 22 sexual risk behaviors in the last two years, with participants reporting engaging in more than seven behaviors on average (M = 7.7). It is important to acknowledge that engagement in any one of these behaviors does not inherently mean risk of HIV/STD contraction. For example, unprotected sex with a partner in the past 2 years may indeed be safe if both parties have been monogamous and have been negative for HIV/STDs during this time. Similar precautions could be utilized for many of the items on this survey, the depth of which was not the focus of this study. Yet, it is also critical to note that only three participants did not have any risk behaviors in the past 2 years, over half (57.1%) had engaged in six or more, and 15% engaged in 15+ risk behaviors.
The CDC (2021) cites engagement in risk behaviors as one of the primary contributors to increased risk of HIV/STD contraction for women under the age of 45 years. Yet, studies on female risk behaviors often only evaluate one or a few risk behaviors in isolation (e.g., sex under the influence of substances, sex without condom use). When restricted to the most common risk behavior(s), such as unprotected sex, risk behavior rates in previous studies (e.g., Duncan et al., 2006) were similar to those reported in the current study. Of note, the timing of data collection (March-April 2021) occurred approximately 1 year into the COVID-19 pandemic in the U.S. Importantly, over one-third of respondents indicated their sexual behavior stayed about the same while 24.1% indicated increased sexual activity compared to prior to the pandemic. Thus, for many participants, sexual activity was not restricted during COVID-19.
Generally speaking, the results corroborate previous research indicating that women under the age of 44 years engage in a variety of risk behaviors (Rudolph et al., 2020). Further, based on participants’ average HIV and STD knowledge scores, it appears likely that many individuals may not know what constitutes self/partner risk behaviors (Majer et al., 2016). Rates of self-reported testing in this sample were also low, with 47.5% reporting lifetime HIV testing and 55.3% reporting lifetime STI/STD testing. Given this, it is perhaps unsurprising that reported rates of STDs in this sample were lower than rates reported by CDC. While speculative, participants' lower knowledge regarding what constitutes risk behavior may be related to reduced rates of testing. Additionally, some STDs, such as HPV, may begin to show a cohort effect in reduction of prevalence, as the first HPV vaccine that targeted several strains of HPV was approved by the U.S. Food and Drug Administration (FDA) in 2006, and has since been expanded to be offered to individuals 9–45 years of age (FDA, 2018).
Social Identities Related to Sexual Risk Behaviors
Within the current sample, individuals who identified as single, White, and who were of a sexual minority status reported significantly more sexual risk behaviors. That women who were single engaged in a greater number of risk behaviors is perhaps unsurprising given prior reports of sexual activity among this demographic. For example, in the National Survey of Family Growth, with 6,493 single, married, and cohabitating women (Lindberg & Singh, 2008), single women had sex with more than one partner at higher rates (22%) than married (8%) and cohabitating (9%) women.
The finding that White women in this sample reported more risk behaviors is consistent with the current literature that suggests that women of color engage in fewer sexual risk behaviors (e.g., Smith, 2015) even while epidemiological research indicates that women of color are at disproportionally high risk of contracting HIV and other STDs (CDC, 2022a). For example, Smith (2015) found that Latino/a/x and Asian-identified respondents were consistently less likely than White respondents to have multiple sex partners, one-night stands, and sex while under the influence of drugs. The higher risk of contracting HIV and other STDs among women of color may reflect the ongoing disparities in HIV/STD prevention, health promotion, and access to care for women of color within the U.S. (Prather et al., 2018). It is plausible that women of color engage in fewer risk behaviors, but are subject to a variety of micro- and macro-level disparities that elevate their risk for contraction.
Women of minority sexual identities were also significantly more likely to report engaging in risk behaviors compared to women who identified exclusively as heterosexual. Roughly 28% (n = 78) of this sample identified as gay/lesbian, bisexual, pansexual, queer, asexual, or another sexual identity. While the majority of research in this area has focused on LGBQ+ adolescents and youth, the results of the current study are consistent with previous literature. Studies of adult women who have sex with women note earlier onset of sexual activity, more frequent unprotected sex, and that women who have sex with women more often trade sex for money (Morgan, 2014; Scheer et al., 2002).
As with racial identity, significant individual and societal level factors have been tied to greater likelihood of risk behaviors among sexual minority women. For example, LGBTQ+ women are more likely to experience a number of correlates for risk behaviors, including poverty, abuse and/or trauma exposure, sexism, societal stigma about sexual relationships, and greater frequency of substance use (Ecker et al., 2019). Importantly, less information about sexual risk and prevention-specific materials are available to LGBTQ+ women. While men who have sex with men have been a notable and prominent target of HIV/AIDS and other STD information campaigns, women who have sex with women and individuals with other marginalized sexual identities have been largely overlooked. According to the Sexuality Information and Education Council of the U.S., only seven states currently have policies that include affirming sexual orientation instruction on LGBTQ+ identities, or discussion of sexual health for this population.
HIV and STD Knowledge
As a whole, this sample had low levels of HIV and STD knowledge. Respondents had mean scores of 63.3% on the HIV-K-Q, and 49.9% on the STD-K-Q. Jaworksi and Carey (2007), the authors of the STD-K-Q, reported similar results, with over half of participants scoring 50% or below on the measure. These low levels of HIV and STD knowledge are gravely concerning. Many health campaigns and education initiatives shifted their focus to HIV prevention beginning in the 1980s. This emphasis on HIV may come at the expense of STD education. HIV prevention education does incorporate important information that applies to other STDs, but knowledge of HIV alone is insufficient (CDC, 2021). In a 2014 compendium of state statues explicitly related to STDs other than HIV, the department of Public Health Law Research and CDC note that existent state statues largely focused on establishment of clinics, mandatory testing and/or treatment, and confidentiality of STD-related records. That is, the most notable efforts to date regarding STDs emphasize post-contraction care, rather than sexual health education or dissemination of sexual health knowledge.
According to the Sexuality Information and Education Council of the U.S. (2023) report, 29 states and the District of Columbia currently mandate any form of sex education to be taught in schools, though there is generally some form of opt-in sexual education offered in every state. However, even when primary education features STDs in teaching, the depth and breadth of information is (generally) limited. Thirty-eight states currently include information on HIV in sexual education curricula, and the majority of this information emphasizes the importance of not sharing bodily fluids (i.e., a precaution that is necessary for HIV, but insufficient for other STDs). Thirty states are required to “stress” abstinence for HIV/STD prevention. However, scholars and advocates have argued that abstinence-only sexual education disproportionately harms and disadvantages girls by perpetuating gender stereotypes (e.g., emphasizing females as the gatekeepers of male sexuality), and places girls at increased risk of consequences (e.g., pregnancy and/or higher likelihood of contracting HIV or STDS; Woebse, 2013).
Sexual Self-Efficacy
Few studies to date have explicitly examined sexual self-efficacy and broad arrays of sexual risk behaviors, and most of these studies exclusively examined undergraduate samples (e.g., Reising et al., 2005). By including a broader study sample of individuals who identify as women, this study expands our knowledge of demographic groups that can benefit from targeted increases in sexual self-efficacy.
The mean score on SHPSES was 72.28 (SD = 15.46), with scores ranging from 20–100. “Typical” levels of sexual self-efficacy have yet to be established within the literature. However, the current findings are similar to those of Charest et al. (2016), who reported a mean total score of 70.7 (SD = 12.9) on the SHPSES in a sample of 386 heterosexual and LGBTQ+ adults.
Sexual self-efficacy, as measured by the SHPSES in this study, encompasses health-protective behaviors (wearing condoms, discussing sexual histories prior to sex, etc.) but also includes items on sexual satisfaction, addressing sexual assault situations, and sexual equality/diversity, among others. Therefore, the construct of sexual self-efficacy here was broader than simply physical-based sexual health protection. This conceptualization of sexual self-efficacy offers an important alternative to traditional, gendered expectations of women as passive recipients of sex. Instead, women are positioned as agentic sexual actors and deserving of sexual safety and well-being (Bay-Cheng & Zucker, 2007; Eisele & Stake, 2008; Schick et al., 2008).
Previous studies focus on reporting sexual self-efficacy in one or few specific situations (e.g., percentage of respondents who would say no to a partner whose sexual health history is unknown; Rocha-Rdz et al., 2017). In contrast, the SHPSES provides a more global view of women's perception of their ability to navigate sexual situations and act to enhance their sexual well-being and satisfaction. This broader definition of sexual self-efficacy is more consistent with feminist work emphasizing women's sexual subjectivity, including satisfaction and pleasure in relationships and communication skills as well as sexual safety, as predictors of decreased sexual risk behaviors and well-being (Bowleg et al., 2000; Hewitt-Stubbs et al., 2016). Further, it is critical to note that sexual self-efficacy offers an alternative to sexual scripts that position women as gate keepers and idealize chastity (Schick et al., 2008). Conceptualizations of sexual self-efficacy that normalize expectations of equality, sexual well-being, and negotiation skills are critical to changing the current discourse and norms on women's sexual roles.
HIV Knowledge, Sexual Self-Efficacy, and Risk Behaviors
HIV knowledge and sexual self-efficacy were significantly related to fewer sexual risk-behaviors. Additionally, as hypothesized, there was a moderating effect of sexual self-efficacy and HIV knowledge on sexual risk behaviors. In other words, when sexual self-efficacy was lower, HIV knowledge was more strongly associated with fewer sexual risk behaviors. In contrast, at higher levels of self-efficacy, higher level of knowledge was not as strongly associated with reduced risk behaviors.
From an education standpoint, these results make intuitive sense. As sexual self-efficacy increases, the need for HIV knowledge in order to also influence/reduce risky sexual behavior decreases. When interpreted via the lens of Bandura's (2001) social-cognitive theory for HIV, the initial development of self-efficacy is cited as the point at which actual behavior change is most substantial. That is, as individuals obtain knowledge, they then begin to develop their self-efficacy and understand themselves to be agents capable of acting in sexual situations. Then, they are more likely to act with this novel information by understanding that they can do so. As this process is reinforced, health-promotive behavior can be sustained on continued feelings of self-efficacy, empowerment, fewer health consequences, etc. rather than on the initial receipt of knowledge (Coleman & Ball, 2009).
STD Knowledge, Sexual Self-Efficacy, and Risk Behaviors
The finding that STD knowledge was related to reductions in sexual risk behaviors is notable in light of the dearth of literature in this area. Less attention has been given to STD knowledge and its sexual health benefits. Three studies to date have examined STD knowledge as it related to sexual risk behaviors, all finding that increases in knowledge were associated with fewer risk behaviors (Downs et al., 2004; Gaydos et al., 2008; Jemmott et al., 2011). All of these studies focused on outcomes following various combined HIV/STD knowledge intervention programs. While information on HIV can be relevant for STDs, HIV and STD prevention are not synonymous.
Next, while it was proposed that sexual self-efficacy would interact with STD knowledge to reduce sexual risk-taking, this relation was not supported in this study. Given that STD knowledge was low in this study, it may be that knowledge was not sufficient to influence development of sexual self-efficacy as proposed by social cognitive theory. The findings of this study do suggest that both sexual health knowledge and self-efficacy are independently associated with reduced risk behaviors, supporting the implementation of educational programs that include information about risk and strategies and skills training that empower women to make their own (ideally health promotive) sexual decisions.
Limitations and Future Directions
This study should be evaluated in light of several limitations. Due to the cross-sectional nature of the data, cause and effect relationships cannot be determined. This study also utilized a convenience sample of MTurk workers. Recruiting participants via this platform strengthened the study by allowing for a more diverse and nationally-representative sample of women, though the results may not be fully generalizable to women whose identities were underrepresented in this sample.
In addition, modifications to the timeframe for the Sexual Health and Behavior Survey and the timing of this study during the COVID-19 pandemic could have influenced the results. Public and private life looked very different for many Americans beginning in early 2020. Recall of the previous 2 years of sexual activity may have been limited by memory, distress, or other external factors related to the COVID-19 pandemic, and the results here may not be generalizable to a “normal” year. Further, the use of a 2-year time frame limits comparisons of these findings with sexual risk behavior collected utilizing a more typical 1-year time frame. In addition, equal weight was given to each risk behavior. Future research will ideally advance our understanding of the relative risk of different sexual behaviors (e.g., getting a tattoo vs. sharing needles vs. multiple partners) and include assessment of frequency of behavior(s) as well. Finally, sexual self-efficacy may have been impacted by the nature of some of the risk behavior items assessed such as sexual interactions under the influence of alcohol or marijuana. Future research should more closely examine the association between sexual self-efficacy and different types of risk behaviors.
Practice Implications
Few studies have explicitly measured sexual self-efficacy as a mechanism for risk-reduction. Findings from this study support the inclusion of sexual self-efficacy materials in conjunction with presentation of HIV and STD information in school based sexual education programs. The findings from this study also support the aim of incorporating comprehensive HIV and STD knowledge and self-efficacy training in risk-reduction programs. Notably, including sexual self-efficacy training as a typical component of sexual health education also has the potential to change current traditional sexual scripts and instead promote views that engaging in sexual self-efficacy is normative and leads to improved sexual health, equity, and well-being (e.g., Bay-Cheng & Zucker, 2007).
Efforts in this direction are starting. The American College of Obstetricians and Gynecologists (2016) recommends that comprehensive sexual health education be medically-accurate and culturally inclusive and include topics on prevention of HIV/STDs and unintended pregnancy, forms of sexual expression, healthy sexual and nonsexual relationships, gender identity and sexual orientation and questioning, communication, recognizing and preventing sexual violence, consent, and decision making. Next, in late 2020, the CDC released its first-ever National Strategic Plan for Sexually Transmitted Infections, offering a roadmap to develop, enhance, and expand STD education and prevention. Some programs specifically targeting women (albeit with heavier focus on HIV than broader STDs) currently incorporate sexual health knowledge and self-efficacy in their curricula (e.g., Sisters Informing Sisters about Topics on AIDS, DiClemente & Wingood, 1995; Project POWER, Fogel et al., 2015). These recommendations offer important and needed guidance to policy makers and educators in this field.
The findings from this study also lend themselves to clinician efforts. Experiences of sexual assault, sexual health concerns, and need for relationship skills are common presenting concerns among women-identified individuals seeking mental health treatment. Many empirically-supported treatment modalities feature direct or indirect components of self-efficacy and could be adapted to include sexual health knowledge and sexual self-efficacy content.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.