
Abstract
Purpose:
To make a diagnosis of cancer with BDORT (resonance test), we can choose two methods. One is to use a chemical agent like Integrin α5β1 or Oncogene C-fos Ab2, the other is to use microscopic cancer slides. These two methods were originally introduced by Prof. Omura of New York. The former is sensitive but not specific and the latter is not so sensitive but is specific. It is useful to investigate the diagnostic sensitivity of the microscopic cancer slide and the specificity of it to the type and differentiation of the cancer in order to utilize them to detect the presence of cancer tissue in clinical medicine.
Methods and Materials:
78 patients, made diagnosis of cancer, (gastric cancer: 30, colon cancer: 22, hepatocellular carcinoma (HCC): 5, Gall Bladder carcinoma: 1, Cholangiocarcinoma: 2, Pancreas carcinoma: 7, Breast cancer: 11) were analyzed. The cancer slides used were as follows.
Used slides to detect the Cancer
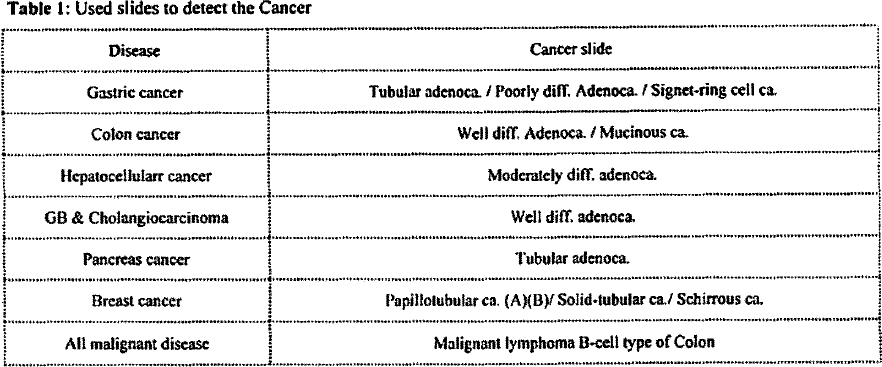
| Disease | Cancer slide |
|---|---|
| Gastric cancer | Tubular adenoca. / Poorly diff. Adenoca. / Signet-ring cell ca. |
| Colon cancer | Well diff. Adenoca./ Mucinous ca. |
| Hepatocellularr cancer | Moderately diff. adenoca. |
| GB & Cholangiocarcinoma | Well diff. adenoca. |
| Pancreas cancer | Tubular adenoca. |
| Breast cancer | Papillolubular ca. (A)(B)/ Solid-tubular ca./ Schirrous ca. |
| All malignant disease | Malignant lymphoma B-cell type of Colon |
Result:
Diagnostic rates were as follows.
Diagnostic rate of the Cancer by corresponding cancer slides
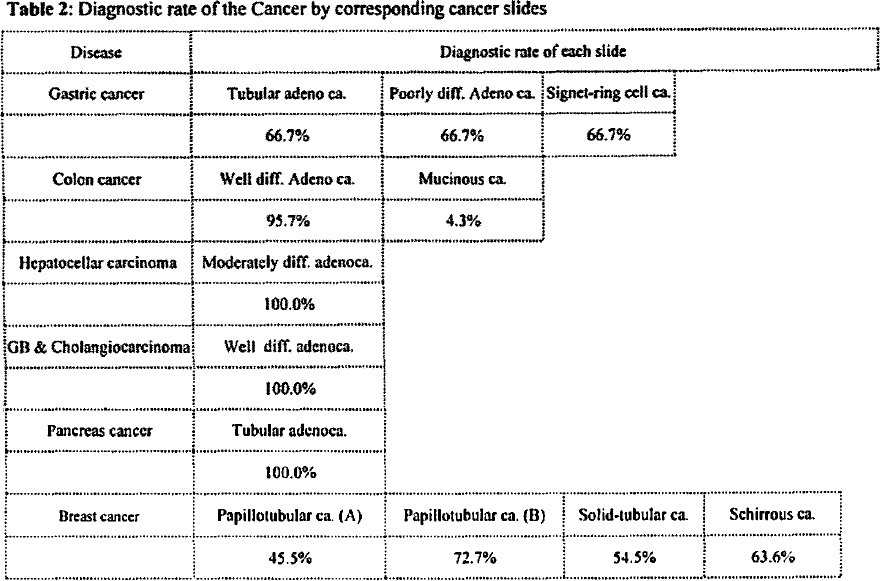
| Disease | Diagnostic rate of each slide | |||
|---|---|---|---|---|
| Gastric cancer | Tubular adeno ca. | Poorly diff. Adeno ca. | Signet-ring cell ca. | |
| 66.7% | 66.7% | 66.7% | ||
| Colon cancer | Well diff. Adeno ca. | Mucinous ca. | ||
| 95.7% | 4.3% | |||
| Hepatocellar carcinoma | Moderately diff. adenoca. | |||
| 100.0% | ||||
| GB & Cholangiocarcinoma | Well diff. adenoca. | |||
| 100.0% | ||||
| Pancreas cancer | Tubular adenoca. | |||
| 100.0% | ||||
| Breast cancer | Papillotubular ca. (A) | Papillotubular ca. (B) | Solid-tubular ca. | Schirrous ca. |
| 45.5% | 72.7% | 54.5% | 63.6% | |
No. of cancer resonance test positive slides
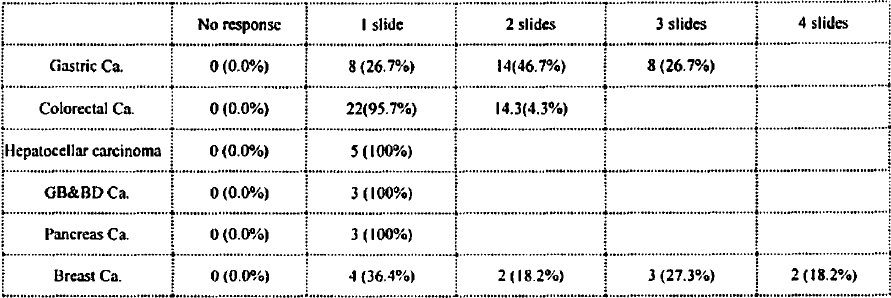
| No response | 1 slide | 2 slides | 3 slides | 4 slides | |
|---|---|---|---|---|---|
| Gastric Ca. | 0(0.0%) | 8(26.7%) | 14(46.7%) | 8(26.7%) | |
| Colorectal Ca. | 0(0.0%) | 22(95.7%) | 14.3(4.3%) | ||
| Hepatocellar carcinoma | 0(0.0%) | 5(100%) | |||
| GB&BD Ca. | 0(0.0%) | 3(100%) | |||
| Pancreas Ca. | 0(0 0%) | 3(100%) | |||
| Breast Ca. | 0(0.0%) | 4(36.4%) | 2(18 2%) | 3(27.3%) | 2(18.2%) |
To make diagnosis of cancer completely (100%), gastric cancer needed 3 slides, colon cancer did 2 slides, Hepatoceller, GB & Cholangiocarcinoma, and Pancreas cancer did only 1 slide, and breast cancer did 4 slides.
Diagnostic rate of the Cancer by B-cell Malignant lymphoma slide
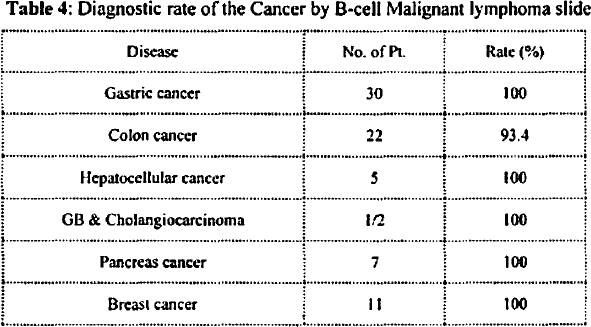
| Disease | No. of Pt. | Rate (%) |
|---|---|---|
| Gastric cancer | 30 | 100 |
| Colon cancer | 22 | 93.4 |
| Hepatocellular cancer | 5 | 100 |
| GB & Cholangiocarcinoma | 1/2 | 100 |
| Pancreas cancer | 7 | 100 |
| Breast cancer | 11 | 100 |
Discussion:
There was no correlation between the cancer tissue type, differentiation and tissue type of microscopic cancer slides. To make diagnosis of the cancer with the microscopic slides, several samples should be added by repeating the examination with trial and error, because of the specificity of resonance cannot be obvious. Diagnostic rate of the Cancer by B-cell Malignant lymphoma slide is very high but isn’t reach 100%. It is useful to screen cancer, because the response has less effect of tissue volume or concentration, different from chemical agent like Integrin α5β1 or Oncogene C-fos Ab2. Further examination is needed to make diagnostic rate to 100%, utilizing T-cell Malignant lymphoma slide or others.
Get full access to this article
View all access options for this article.