
Abstract

Cristina Tassorelli1,2, Rebecca L. Robinson3, Carlos Vallarino3, Lars Viktrup3, Maurice Vincent3 and Daisuke Danno4,*
1Department of Brain and Behavioral Sciences, University of Pavia, University of Pavia, Pavia, Italy
2Headache Science and Neurorehabilitation Centre, IRCCS Mondino Foundation, Pavia, Italy
3Eli Lilly and Company, Indianapolis, USA
4Tominaga Hospital Headache Center/Department of Neurology, Osaka, Japan
Objective
To compare the 3-month responder rate between galcanezumab (a CGRP mAb), and amitriptyline, topiramate, and the broader subset of traditional oral migraine preventive medications (TOMP), classified as drugs having evidence of established or probable efficacy per American Headache Society guidelines (a key secondary objective of the TRIUMPH Study).
Methods
TRIUMPH, an ongoing, international observational study, included patients with a diagnosis of migraine who initiated or switched to a preventive medication. The current analysis used data collected between 25 February 2020 and 9 February 2023 for patients with ≥4 migraine headache days reported within 30 days before baseline and taking galcanezumab or a TOMP (beta blockers, anticonvulsants, tricyclic antidepressants, calcium channel blockers, angiotensin II receptor antagonists). The established/probable efficacy TOMP subset included patients taking medications with established (topiramate, sodium valproate/valproic acid, metoprolol, propranolol) or probable (amitriptyline, candesartan, atenolol, nadolol) efficacy. Responders at 3-months included those with reduction from baseline in monthly migraine headache days of ≥50% in episodic and ≥30% in chronic migraine. The difference in the proportion of responders between the treatments was assessed using weighted Chi-squared tests. The weights were derived from a least absolute shrinkage and selection operator model fit of propensity scores using 65 baseline covariates. Study outcome was compared between the cohorts at 5% alpha level (two-sided). Prior assessment of 3-month effectiveness of galcanezumab versus TOMP (TRIUMPH’s primary objective) found significantly greater proportions of patients receiving galcanezumab responded at 3-months than those receiving TOMP allowing key secondary endpoints to be formally tested. Galcanezumab comparisons with amitriptyline and topiramate were not allocated alpha.
Results
A total of 2879 patients from the United States (46.3%), Japan (22.7%), Germany (14.3%), Italy (6.9%), the United Arab Emirates (5.6%), the United Kingdom (2.3%) and Spain (1.8%) were analyzed. Baseline characteristics of patients are presented in Table 1. The two most commonly used TOMP medications were amitriptyline (n = 243) and topiramate (n = 350). At 3-months, galcanezumab cohort (n = 1083) had substantially greater weighted proportion of responders than in the amitriptyline (49.5% and 24.3% respectively, p < 0.0001) and topiramate subsets (48.8% vs. 37.0% respectively, p = 0.0014). Additionally, galcanezumab users had significantly greater weighted proportion of responders (47.9%) than in the established/probable efficacy TOMP subset (n = 932, 35.2%; p < 0.0001).
Conclusion
Baseline characteristics of patients before switching from or initiating Galcanezumab, and TOMP.

Abbreviations: MSQ-RFR, Migraine-Specific Quality of Life Questionnaire, version 2.1 Role Functioning Restrictive; SD, standard deviation; TOMP, traditional oral migraine preventives.
Disclosure of Interest
Cristina Tassorelli has received consulting fees from Abbvie, Lundbeck, Dompé, Eli Lilly, Teva, Pfizer; honoraria: Abbvie, Lundbeck, Dompé, Eli Lilly, Teva, Pfizer; travel support: Lundbeck, and is the president of IHS. Maurice Vincent, Carlos Vallarino, Lars Viktrup and Rebecca Robinson are full-time employees and shareholders at Eli Lilly and Company. Medical writing support was provided by Priyanka Bannikoppa, Eli Lilly Services India Private Limited.
Marte-Helene Bjørk1,2, Solveig Borkenhagen3, Francisco Oteiza3, Erik Magnus Sæther3, Christoffer Bugge3 and Aud N Dueland4,5
1Dept of Clinical Medicine, University of Bergen, Bergen, Norway
2Dept of Neurology, Haukeland University Hospital, Bergen, Norway
3Oslo Economics, Oslo, Norway
4Sandvika Neuro Centre, Oslo, Norway
5Dept Neurology, Oslo University Hospital, Norway
Background
While many new migraine preventive drugs have become available in recent years, little is known about their comparative retention and effectiveness in a real-world setting.
Aim
We aimed to estimate treatment retention and effectiveness of a range of migraine preventive drugs in a nationwide registry-based cohort study of migraine patients in Norway treated with preventive drugs between 2010 and 2020.
Methods
Migraine patients were identified based on triptan prescriptions (Anatomical Therapeutic Chemical classification codes (ATC N02CC), and drug reimbursement codes for migraine. Patients with comorbid cluster headache or age <2 years or >99 years were excluded. Migraine preventive drugs were identified based on ATC codes. Retention was defined as the number of uninterrupted days of preventive migraine treatment. Effectiveness was defined as the reduction in prescriptions of triptans the first year after initiating preventive medication compared to the 90-day baseline period before the first preventive medication prescription fill. The follow up period was divided into four subsequent 90-day periods. Retention and efficacy rates for the different preventive drugs were compared against those for beta blockers. The primary outcomes were retention rate and 30% effectiveness for the following migraine preventive drug groups: beta blockers (propranolol and metoprolol), candesartan, lisinopril, topiramate, calcitonin gene-related peptide (CGRP) antibodies (erenumab, fremanezumab, galcanezumab), botulinum toxin A, clonidine, and simvastatin. Covariates included patient age, county of residence, selected comorbidities: acute myocardial infarction, congestive heart failure, hypertension, heart rhythm disorders, renal disease, depression, anxiety disorder, nicotine replacement products, epilepsy, mood disorders, type 2 diabetes and asthma (based on reimbursement codes), year of treatment start, previous or simultaneous use of other migraine preventive drugs, and overuse of triptans. Comparative retention was adjusted for covariates using Cox regression, and effectiveness using adjusted logistic regression to calculate odds rates (ORs). To further account for differences in patient characteristics across drug types, we applied propensity score weighting. Several sensitivity analyses were done to test the robustness of our estimates across migraine subgroups, drug use indications, comorbidities and treatment patterns.
Results
The study population consisted of 104,072 patients, 81,890 female (78.69%), mean age 44.60 (SD = 15.61). Compared to beta blockers, botulinum toxin A (HR = 0.43, 95% CI 0.42–0.44) and CGRP- antibodies (HR = 0.63, 95% CI 0.59–0.66) were the least likely to be discontinued, while clonidine (HR = 2.95, 95% CI 2.88–3.02) and topiramate (HR = 1.34, 95% CI 1.31–1.37) were the most likely to be discontinued. Patients on simvastatin, CGRP antibodies, and amitriptyline were more likely to achieve a clinically significant reduction in triptan use during the first 90 days of treatment, with propensity score-adjusted ORs of 1.28 (95% CI 1.19–1.38), 1.23 (95% CI 0.79–1.90), and 1.13 (95% CI 1.08–1.17), respectively. Sensitivity analyses did not change estimates much.
Conclusion
Overall, the results showed favorable response of CGRP antibodies, amitriptyline, and simvastatin over beta blockers, while topiramate and clonidine were associated with poorer outcome
Disclosure of Interest
Novartis Norway AS contributed to the funding of this study . Dr Bjørk reported receiving speakers honoraria from Teva, Eisai, and Lilly; advisory board honoraria from Jazz Pharmaceuticals, Angelini Pharma, Lundbeck, Pfizer and Eisai; consultancy honoraria from Novartis, and institutional grants from Sanofi for the conduction of a post authorization safety study. Aud N. Dueland reported receiving speakers honoraria from AbbVie, Lilly, Lundbeck, Novartis, Roche, and Teva, advisory board honoraria from Lilly, Lundbeck, Pfizer, and Teva, and consultancy honoraria from AbbVie and Novartis The other authors reported no conflicts of interests
Sanjay Rao Kordcal, Debashish Chowdhury, Rahul Nagane, Ashish Duggal and Headache Group
G B Pant Institute of Post Graduate Medical Education and Research (GIPMER), Delhi, India
Background
The long-term efficacy and safety of GONB for the preventive treatment of episodic cluster headaches (ECH) remains unknown.
Objectives
To study the long-term efficacy and safety of GONB in patients of ECH following a double-blind treatment phase (DBTP).
Methods
We conducted a randomized, double-blind, placebo-controlled, parallel-group trial that included ECH patients diagnosed by ICHD-3 criteria, aged 18–65, with 1 or more attacks per 24 h for 7 days before randomization. DBTP lasted for 4 weeks, following which a long-term open label study was undertaken for 52 weeks. ECH patients were either not on any preventive medications or on stable doses for at least 3 months Concurrent oral preventive drugs were allowed or escalated after Week 1 during the DBTP in patients with persistent attacks. In the open-label treatment phase (OLTP), patients who continued to have attacks and opted out of the study and those who continued to have attacks at the end of Week 4 were offered GONB with 2ml methylprednisolone (80mg) and 2ml of 2% lignocaine. The efficacy and safety of the 2nd GONB during the OLTP were assessed at Week 8 and 12. Oral, intramuscular, or intravenous steroids were not allowed during OLTP. Remission was defined as attack-free state at the time of last evaluation. The patients were then followed up to 52 weeks (physically or telephonically) and recurrence of cluster period (CP) and its treatment was recorded. Descriptive summaries were provided. Data were reported as observed, without imputation for missing data. The trial was registered with the Clinical Trials Registry of India (CTRI/2021/21/038397).
Results
During the DBTP, out of 20 patients who received the active GONB, one patient exited the study the day after randomization and was lost to follow-up as he shifted to another city. Of the remaining 19 patients, 3 patients opted out of the study. Among the 20 patients who received placebo, 2 patients opted out of the study. Thus, of 34 patients who completed the DBTP, 5 patients from the placebo group and none from the active group required a repeat GONB (27.8% vs. 0%; p = 0.022). There was a significant difference in the time to remission between the active and the placebo groups (9.0 ± 2.6 days vs. 16.2 ± 7.7 days; p = 0.002) following the 2nd GONB. The distribution and the outcome of ECH patients during the OLTP is shown in Table 1. 80% of patients in the active group achieved complete remission at Week 12 following a single GONB. Out of nine patients who entered the OLTP, seven (77.7%) achieved a complete remission at Week 8 and all (100%) at Week 12.
Mean long-term follow-up duration was 39.4 ± 12 weeks (median 43 weeks). Out of the 39 patients, thirty-two (82.1%) and twelve patients (30.8%) completed the 26-week and 52-week follow-up respectively. Seven patients (three from the active group and four from the placebo group) had fresh attacks of ECH. These new CPs occurred at a median of 46 weeks from the time of randomization (range: 30–51 weeks). All seven patients were treated with a 3rd GONB comprising 2ml methylprednisolone (80mg) and 2ml of 2% lignocaine. Six of these seven patients became attack free (median time to remission: 7 days) till the last evaluation. Repeat GONBs were well tolerated. and no new adverse effects were found.
Conclusion
A single GONB within 1 week of the start of CP along with oral preventives provided attack free state in 80% of patients with ECH for 12 weeks. In non-responders to the first GONB, a second block provided an attack free state for a median period of 46 weeks. The results of this study thus show that GONB is an effective and well tolerated treatment option for patients with ECH.
Disclosure of Interest
None Declared.
Distribution of and outcome of ECH patients during open-label treatment phase (OLTP)

Debashish Chowdhury, Sanjay Rao Kordcal*, Rahul Nagane and Ashish Duggal
G B Pant Institute of Post graduate Medical education and Research, New Delhi, Delhi, India
Background
There is poor evidence of greater occipital nerve blocks (GONB) for the preventive treatment of cluster headaches. (1)
Objectives
To study the efficacy and tolerability of GONB injections as a transitional preventive treatment for episodic cluster headaches (ECH).
Methods
This randomized, double-blind, placebo-controlled, parallel-group trial included ECH patients diagnosed by ICHD-3 criteria, aged 18–65, with 1 or more attacks per 24 h for 7 days before randomization (baseline). The patients needed to have a previous history of at least 1 prior cluster period (CP) and the current CP for no more than 2 weeks. At the time of randomization, ECH patients were either not on any preventive medications or on stable doses for at least 3 months.
ECH patients were randomized to receive active GONB [2ml methylprednisolone (80mg) and 2ml lignocaine (2%)] and placebo [(4 ml saline injections)]. Before giving GONB, lignocaine jelly was applied topically to mask the effect of numbness following the GONB. Patients with persistent attacks at the end of Week 1 had the option of preventive add-ons or escalation of existing doses. Acute treatment options like oxygen and triptans were allowed. The primary efficacy endpoint was the mean change in weekly attack frequency from baseline to Week 4. The key secondary endpoints were the mean change in weekly attack frequency from baseline to Weeks 1, 2, and 3 and the proportion of patients achieving complete remission (disappearance of attacks) from day 4 to Weeks 1, 2, 3, and 4.
Efficacy analyses were performed in a modified intention-to-treat population that included all patients who received at least 1 injection of GONB and had a follow-up for 1 week following GONB. A least-square-mean change from baseline was calculated using a linear mixed-effects model for repeated measures that included participants as a random effect and weekly baseline values (1-week pre-randomization) as covariates. The model included fixed categorical effects of the treatment group, sex (male vs. female), use of preventive medication during DBTP (yes vs. no), and week and week-by-treatment group interaction without any imputation for missing data. The proportion of patients achieving complete remission was compared by a Cochran Mantel-Haenszel test. A gatekeeping strategy maintained the overall type I error rate at a two-sided alpha level 0.05 for the primary and key secondary endpoints. Based on the estimates provided by a previous study (2) and keeping an alpha value of 5% with 80% power and a 10% attrition rate, the sample size was estimated to be 20 patients in each group. The trial was registered with the Clinical Trials Registry of India (CTRI/2021/21/038397).
Results
Forty ECH patients were randomized. Thirty-nine patients (19 in the active group & 20 in the placebo group) were available for efficacy analysis. The change in weekly attack frequency from baseline to Week 4 was −11.1 (95% CI: −8.5 to −4.4) for the active group compared to −7.7 (95% CI: −11.8 to −9.8) for placebo [mean difference −3.4 (95% CI: −5.2 to −1.7, p < 0.001)]. The mean difference between the two groups in weekly attack frequency from baseline to Weeks 1, 2, and 3 were −3.4 (95% CI: −5.2 to −1.7; p < 0.001), −5.1 (95% CI: −6.8 to −3.3; p < 0.001), and −4.1 (95% CI: −5.9 to −2.3; p < 0.001) respectively. Ten patients (52.6%) from the active group achieved complete remission in Week 1 compared to 4 (20%) in the placebo group (OR = 4.4, 95% CI = 1.1 – 18.4, p = 0.039). Fourteen patients in the active group (73.7%) achieved complete remission in Week 2 compared to 6 (30%) in the placebo group (OR = 6.5, 95% CI = 1.6–26.5, p = 0.009). No significant differences were found in Weeks 3 and 4. GONB was well tolerated in both groups. At least 1 treatment-emergent adverse effect (TEAE) was complained equally by the patients in each group (18 each). TEAEs were, however, mild and transient. No serious adverse events were reported.
Conclusion
This study found that GONB injection with methylprednisolone and lignocaine, compared to a placebo, significantly reduced the weekly attack frequency from baseline to Week 1 through Week 4 in ECH patients. At Weeks 1 and 2, a significantly higher proportion of patients receiving active GONB achieved complete remission than those receiving placebo.
Disclosure of Interest
None Declared.
Footnotes
Doga Vuralli1, Merve Ceren Akgor2, Saliha Ilbasmis2, Bahar Tasdelen3, Fatih Gultekin4 and Hayrunnisa Bolay1
1Gazi University Faculty of Medicine, Department of Neurology and Algology, Neuropsychiatry Center, NÖROM, Ankara, Turkey
2Gazi University Faculty of Medicine, Department of Neurology, Ankara, Turkey
3Mersin University Faculty of Medicine, Department of Biostatistics and Bioinformatics, Mersin, Turkey
4Lokman Hekim University Faculty of Biochemistry, Ankara, Turkey
Methods
1118 participants that filled the online survey were included in the study. Age, gender, presence of chronic disease, medications used, presence of headache, the clinical features of headache according to ICHD3 criteria, presence of irritable bowel disease symptoms, consumption behavior of patients regarding 125 food/food additives and whether or not these food/food additives trigger headache and/or abdominal pain were asked in the questionnaire. The participants were diagnosed as migraine and medication overuse headache according to ICHD3 criteria.
Results
88% of the participants had migraine and 32% of the participants had MOH. 63.9% of the MOH patients and 52% of migraine patients had irritable bowel disease whereas only 31.3% of the participants without headache had irritable bowel disease. Specific food triggers for MOH patients were, banana, apple, cherry, apricot, watermelon, olive, ice cream and yogurt. The common characteristics of food triggers such as banana, apple, cherry, apricot, watermelon specific to MOH are that they are healthy fruits and frequently consumed in daily life. Another common feature of these food triggers of MOH is that they are dopaminergic foods. Whereas migraine-specific food triggers were peanut butter, chocolate, cacao, coffee cream, milk powder, fish, red wine, white wine, mayonnaise, deserts with syrup, gateau and foods containing red food dye. Migraine specific triggers consisted of histaminergic foods and processed foods containing food additives. Food trigger specific to irritable bowel disease was red grape which is also dopaminergic. Tomato juice and spinach were common triggers of both MOH and irritable bowel disease. Cream cheese, custard, milk, potato, onion, garlic, bulgur wheat, bagel, citrus fruits, cabbage, canned foods, soy sauce and beer were among the shared triggers between migraine, MOH and irritable bowel disease.
Conclusion
This was the first study to investigate the frequency of irritable bowel disease symptoms and food triggers among medication overuse headache patients. The frequency of irritable bowel disease symptoms was higher in MOH patients compared to migraine patients. MOH specific triggers were mostly dopaminergic foods whereas migraine specific food triggers were mostly histaminergic and processed foods. It is important to raise awareness about food triggers in headache patients. Individuals with migraine and MOH must add diet diaries to their headache diaries. Migraine, MOH and irritable bowel disease patients should be aware of their food triggers and the treatment plan of these patients must include appropiate and personalized diets with the avoidance of those triggers.
Disclosure of Interest
None Declared.
Laura Papetti1, Federica Del Chierico1, Francesca Toto1, Matteo Scanu1, Ilaria Frattale2, Stefano Levi Mortera1, Fabiana Ursitti1, Giorgia Sforza1, Gabriele Monte1, Massimiliano Valeriani1 and Lorenza Putignani1
1IRCCS Bambino Gesù, rome, Italy
2Tor Vergata University, Rome, Italy
Objective
Primary: to verify if gut microbiota in children with migraine shows differences in the profiling when compared with age-matched controls.
Secondary
to verify if different migraine phenotype (aura or not aura; presence of nausea/vomiting during the attacks; duration of disease and frequency of monthly days with headache) are associated with differences in the profiles of gut microbiota.
Methods
Patients aged between 6 and 18 years were recruited by the headache center of bambino Gesù children hospital; informed consent was obtained by each participant. Migraine diagnosis was made according the criteria of third version of the international classification of headache disorders.
The gut microbiota profiling was obtained by the 16S rRNA region sequencing from faecal samples of migraine patients (n = 98) and of healthy subjects (n = 100, HCs).
QIIME2 v2022.2 software was used to obtain Amplicon Sequence Variants (ASV) with 99% of identity and taxonomic assignations by the sequence matching with Greengenes database (v13.8, ![]() ). Alpha and beta diversity analyses and multivariate (unsupervised Principal Component Analysis [PCA] and the supervised Partial Least Square Discriminant Analysis [PLS-DA]) and univariate (Linear Discriminant analysis [LDA] effect size [LEfSe]) tests were applied to compare the gut microbiota profiles between migraine and HC groups by R v4.0.2.
). Alpha and beta diversity analyses and multivariate (unsupervised Principal Component Analysis [PCA] and the supervised Partial Least Square Discriminant Analysis [PLS-DA]) and univariate (Linear Discriminant analysis [LDA] effect size [LEfSe]) tests were applied to compare the gut microbiota profiles between migraine and HC groups by R v4.0.2.
Results
Alpha diversity, assessed by Shannon-Weiner and Simpson indexes, was not significantly different between patients with migraine and HC (Mann-Whitney test, p-value > 0.05). However, the median of these two indices were higher in patients respect to HC.
The analysis of β-diversity, which was performed by Bray-Curtis and Unweighted Unifrac algorithms, revealed a dissimilarity statistically significant among two groups (PERMANOVA, p-value = 0.001), suggesting a different gut microbiota profile of patients compared with HCs (Figure 1).
The PCA evidenced the presence of gut microbiota fingerprints specific of patients’ and HC (Figure 2A. Furthermore, the PLS-DA model confirmed the two differential profiles for migraine and HC cohorts, each characterized by different distribution of bacteria (Figure 2B). The low Root Mean Square Error value (RMSE = 0.347) and the high R2 (0.525) and Area Under the Receiver Operating Characteristics (AUROC = 0.87) values suggested a high accuracy of the model to predict the subject classification.
Finally, the LEfSe test confirmed the presence of features that characterize the gut microbiota composition of patients affected by migraine (Figure 2C). By matching the results from these different statistical approaches, we assigned, Bacteroides, Faecalibacterium, Butyricicoccuus, Lactobacillus and Enterobacteriaceae as biomarker of the patient’s microbiota, while Bifidobacterium, Akkermansia, Collinsella, Eggerthella, Clostridium, Erysipelotrichaceae, Mogibacteriaceae and Coriobacteriaceae to gut microbiota of HCs.
Conclusions
Our study shows that pediatric migraine patients have a very different GM composition compared to HCs. These differences do not appear to be related to disease characteristics such as duration, presence of aura, or neurovegetative or sensory symptoms. We are carrying out further analyses to determine whether these populations of bacteria may be responsible for the production of pro-inflammatory substances.
Figure 1. Comparison of the faecal microbiota profiles among patients and CTRL. Beta diversity was performed by Bray-Curtis algorithm and reported by principal coordinate analysis (PCoA) plots. PERMANOVA test were applied on β-diversity distance matrices, resulting statistically significant (p-value = 0.001).
Figure 2. Gut microbiota compositional analysis at genus level of MIMIC and CTRL. Results are reported in figure: unsupervised multivariate analysis (principal component analysis [PCA] plot) (A), supervised multivariate analysis plot (partial least squares discriminant analysis [PLS-DA] loading variables plot (B). LDA plots of LEfSe univariate analysis (B). Enriched bacterial taxa in MIMIC are represented by blue bars, and CTRL enriched bacterial taxa are represented by orange bars.
Disclosure of Interest
None Declared.
Roberto De Icco1,2, Marta Allena2, Michele Corrado1,2, Federico Bighiani1,2, Francescantonio Cammarota1,2, Carla Brancaccio1,2, Valentina Grillo1,2, Marianna Semprini3, Elena Fenoglio3, Grazia Sances2 and Cristina Tassorelli1,2
1Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy
2Headache Science & Neurorehabilitation Center, IRCCS Mondino Foundation, Pavia, Italy
3Rehab Technologies, Istituto Italiano di Tecnologia, Genova, Italy
Objectives
The pathophysiological mechanisms underlying episodic cluster headache (eCH), and shift between active and remission phases, are elusive. We aimed to study the internodal and internetworks connectivity patterns of the resting state networks in eCH patients, assessing brain connectivity by means of high-density EEG (HD-EEG).
Methods
We enrolled 24 patients with eCH and 19 healthy controls (HCs) (eCH: age: 41.4 ± 13.7 years, 87% males; HCs: age: 34.3 ± 12.1 years, 73.7% males; p = 0.085 for age, and p = 0.432 for sex). eCH patients reported a mean of 2.2 ± 1.2 attacks per day, in 58.3% of them attacks occurred preferentially during night-time. The active phases recurred on average every 16.3 ± 13.5 months. Eight eCH patients were investigated only during an active phase (T0), 10 only during a remission phase (T1) and 6 on both phases. The default mode network (DMN) areas of interest were the right and left angular gyrus (RANG and LANG), the medial pre-frontal cortex (MPC) and the posterior cingulate cortex (PCC).
Results
In eCH patients, we found a lower internodal brain connectivity of the DMN at T1 (remission phase) when compared to T0 (active phase) between PCC and MPC (T0 = 0.078 ± 0.009 vs. T1 = 0.049 ± 0.006, p = 0.022) and between PCC and RANG (T0 = 0.076 ± 0.008 vs. T1 = 0.052 ± 0.005, p = 0.024). At T1, the DMN connectivity between PCC and MPC areas was lower in eCH group when compared to HCs (CHe-T1 = 0.049 ± 0.005 vs. HS = 0.067 ± 0.005, p = 0.028).
Conclusion
eCH patients evaluated during a remission phase of disease showed lower brain connectivity within specific areas of the DMN when compared with either eCH patients tested during an active phase and HCs. This finding may represent a biological marker of disease, while the fluctuation in PCC connectivity may reflect pathophysiological mechanisms involved in the shift from one phase of disease to the other.
Disclosure of Interest
RDI has received speaker honoraria form Eli Lilly, TEVA and Lundbeck. GS has received personal fees from Eli Lilly, Lundbeck, Novartis, and Teva. CT has received personal fees for the participation in advisory boards and/or scientifc symposia from Abbvie, Dompé, Eli Lilly, Novartis, Lundbeck and Teva. The other authors have no conficts of interests to declare.
Berkay Alpay1, Bariscan Cimen1, Elif Akaydin1, Hayrunnisa Bolay2 and Yildirim Sara1
1Hacettepe University, Ankara, Turkey
2Gazi University, Ankara, Turkey
Objective
Migraine is a type of primary headache, disabling millions worldwide. In one third of the patients transient, fully reversible neurological impairments called migraine auras are experienced. Canonically, migraine auras are speculated to arise as a result of an electrophysiological phenomenon called spreading depression (SD). So far, only levcromakalim (LVC) was able to induce both aura and headache in migraineurs with aura, rest of the migraine-provoking drugs, including nitroglycerine (NTG), were unable to induce aura. The objective of this work is to compare LVC effects on acute pain-related behaviors and SD with the other established headache inducing agent, NTG.
Methods
Periorbital and hind paw mechanical thresholds were tested with von Frey filaments. Anxiety-like behaviors, photophobia, and locomotion were evaluated with elevated plus maze (EPM), dark-light box (DLB) and open field arena (OFA). Effects of LVC and NTG on SD were investigated in rats under urethane anesthesia with in vivo electrophysiology.
Results
LVC significantly decreased mechanical thresholds in a shorter time with respect to NTG. LVC- and NTG-injected rats spent a shorter time in the open arms of EPM than the control group. LVC and NTG significantly reduced the time spent in the bright compartment of DLB. LVC group, in contrast with NTG group, travelled a significantly shorter distance in OFA. NTG administration reduced the SD threshold while LVC had no effect.
Conclusion
LVC reduced mechanical thresholds and induced pain-related behaviors within a shorter timeframe but otherwise effects were similar to that of NTG, however, as opposed to NTG, LVC did not alter SD parameters.
Disclosure of Interest
None Declared.
Messoud Ashina1,2, Ravinder Phul3, Melanie Khodaie3 and Ioana Florea3
1Department of Neurology, Danish Headache Center, University of Copenhagen, Glostrup, Denmark
2Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Glostrup, Denmark
3H. Lundbeck A/S, Copenhagen, Denmark
Objective
This proof-of-concept trial of Lu AG09222 (HOPE) was designed to assess the efficacy, safety, and tolerability of a single intravenous infusion of Lu AG09222 for migraine prevention in adults with migraine who had 2–4 unsuccessful prior preventive treatments.
Methods
HOPE was an interventional, randomized, double-blind, parallel-group, placebo-controlled Phase 2 trial (NCT05133323). Participants were 18–65 years of age, diagnosed with migraine (episodic or chronic), with documented failure of 2–4 previous preventive migraine treatments. The trial consisted of a 4-week double-blind treatment period and an 8-week double-blind follow-up period. Participants recruited from specialist settings in Europe and North America were randomly allocated (2:1:2) to one of three treatment groups: Lu AG09222 high dose, Lu AG09222 low dose, or placebo. The primary efficacy endpoint was the mean change from baseline in the number of monthly migraine days (MMDs) over weeks 1–4 for the high dose of Lu AG09222.
Results
A total of 237 participants were randomized in this trial (Lu AG09222 high dose, 97; Lu AG09222 low dose, 46; and placebo, 94). Participants were 87.8% female with a mean age of 42.5 and 16.7 MMDs at baseline. The change from baseline over weeks 1–4 in mean MMDs was −6.2 (standard error [SE] 0.66) with Lu AG09222 high dose and −4.2 (SE 0.67) with placebo. This trial met the primary endpoint; the difference from placebo in mean change in MMDs from baseline was significant with the Lu AG09222 high dose (−2.0 [90%CI −3.5; −0.6]; one-sided p = 0.01). Lu AG09222 was generally well tolerated.
Conclusions
This proof-of-concept trial demonstrated that Lu AG09222 can be a potential treatment for migraine prevention. In this trial, Lu AG09222 was well tolerated.
Disclosure of Interest
None Declared.
Giada Giuliani1, Gianfranco De Stefano1, Chiara Zilli1, Marta Altieri1, Francesca Caramia1, Giulia Di Stefano1, Andrea Truini1 and Vittorio Di Piero1,2
1Department of Human Neurosciences, Sapienza University of Rome, Rome, Italy
2University Consortium for Adaptive Disorders and Head Pain (UCADH), Pavia, Italy
Objective
We compared neuroradiological findings in two couple of patients with the same structural abnormalities but with different clinical pictures. Two patients presented a short-lasting unilateral neuralgiform headache attacks with conjunctival injection (SUNCT) while the others were affected by trigeminal neuralgia (TN). Our aim was to identify any difference in neuroradiological picture that could influence clinical presentation.
Methods
The first couple presented a pontine lesion involving trigeminal root entry zone, due to multiple sclerosis. First patient was a 68-years-old man who developed a SUNCT syndrome, characterized by shooting pain in the orbital region associated with prominent ipsilateral autonomic symptoms. Attacks, that were both spontaneous and triggered by tactile stimulation, disappeared after the introduction of lamotrigine. The second MS patient, with an indistinguishable lesion at MRI, reported electric shock like triggered pain in the maxillary region, with occasional ipsilateral autonomic symptoms, that responded to carbamazepine. In the second couple, brain magnetic resonance imaging (MRI) showed a neurovascular contact in which the superior cerebellar artery dislocated the fifth nerve without clear signs of atrophy; brainstem lesions were absent. Patients developed two different clinical pictures, consistent respectively with a SUNCT syndrome and a trigeminal neuralgia.
Results
Routine neuroradiological exams of our cases showed no apparent difference between SUNCT and TN patients.
Conclusion
SUNCT and TN significantly overlap. Both conditions are characterized by similar pain pattern, typically very short lasting and strictly unilateral. Presence of pain paroxysms triggered by innocuous stimuli is a hallmark of TN and it is also reported in SUNCT; autonomic symptoms, characteristic of SUNCT, are commonly present in TN patients, mainly when V1 territory is involved. These craniofacial syndromes may share a damage in the trigeminal primary afferents at the root entry zone, justifying the strong similarities. On the contrary, slight clinical differences could be explained by the additional role of hypothalamus in SUNCT.
Although SUNCT and TN are traditionally considered as different disorders, shared neuroradiological and clinical features suggest a common pathophysiological mechanism. To better understand the real nature of this link, future advanced neuroimaging studies are necessary.
Disclosure of Interest
None Declared.
Yue Xu1, Yi Qi2, Yichen Guo2, Xiangyu Lei2, Xiangqi Cao3 and Guogang Luo2
1Department of Neurology, Xi'an No.9 Hospital, Xi'an, China
2Department of Neurology, The First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China
3Department of Neurology, Tangdu Hospital of Air Force Medical University, Xi'an, China
Objective
The thickness of retinal nerve fiber layer (RNFL) may change in migraine patients, but it is not clear whether patent foramen ovale (PFO), which is highly associated with migraine, participates in the change process. This study aims to investigate the RNFL thickness and macular superficial blood flow density of migraine patients with PFO.
Methods
Patients with migraine who were admitted to the Headache Clinic of the First Affiliated Hospital of Xi'an Jiaotong University were included into this study. They were divided into a group with PFO and a group without PFO through contrast-transthoracic echocardiography (cTTE). Then the RNFL thickness, macular superficial vascular density (VD) and perfusion density (PD) were collected by optical coherence tomography (OCT).
Results
A total of 70 patients with migraine were included in this study. The RNFL temporal quadrant thickness and central VD in the superficial macular vascular plexus in the group with PFO were significantly increased compared to the group without PFO (p = 0.046, 0.048). Except for the RNFL nasal quadrant thickness, the other quadrant thicknesses and VD and PD in the superficial macular vascular plexus were higher in the group with PFO; Subgroup analysis showed that in the temporal quadrant thickness of RNFL, the spontaneous shunt group showed a significant increase compared to the induced shunt group and the non PFO group (p = 0.009).
Conclusions
Temporal RNFL thickening and increased central VD of the superficial macular vascular plexus were more pronounced in migraine patients with PFO and in migraine patients with spontaneous shunting PFO. It is suggested that PFO may affect RNFL thickness through right-to-left shunting.
Disclosure of Interest
None Declared.
Tiago Gomes de Paula*, Bruno Cristofolini, Caio Vieira Diniz, Alcides oliveira neto, Anelisa Bittencourt Campaner and Thais Rodrigues Villa
Headache Center Brasil, Sao Paulo, Brazil
Objectives
The objective of this case series was to assess the therapeutic effect of OnabotulinumtoxinA in female patients with chronic migraine and concurrent vasomotor symptoms, specifically hot flashes. The goal was to contribute to the understanding of the efficacy of OnabotulinumtoxinA in managing chronic migraine and vasomotor symptoms, thus improving the quality of life for affected.
Method
This case report series was based on the analysis of medical records of 8 outpatients from a private Headache Center in São Paulo, Brazil. All patients had chronic migraine and vasomotor symptoms, with 4 of them previously treated with hormonal therapy for vasomotor symptoms and the remaining 4 having received no treatment. All the patients received OnabotulinumtoxinA for chronic migraine prophylaxis and were asked about improvement in vasomotor symptoms after this treatment.
Results
Summary of patients analyzed in this case series.

| Patient | Age | Headache Days per Month | Migraine Days per Month | Hot Flash Symptoms | Hormonal Treatment | OnabotulinumtoxinA Cycle | Headache Days per Month | Migraine Days per Month | Hot Flash Symptoms |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 56 | 0 | 30 | Daily | Vaginal gel (estradiol) | 6 | 4 | 0 | 0 |
| 2 | 58 | 18 | 12 | Daily | Vaginal gel (estradiol) | 4 | 4 | 0 | 0 |
| 3 | 50 | 0 | 30 | Daily | Tibolone | 5 | 3 | 0 | 0 |
| 4 | 45 | 0 | 30 | Daily | Isoflavone | 4 | 10 | 3 | 3 |
| 5 | 47 | 20 | 10 | Daily | None | 4 | 6 | 0 | 0 |
| 6 | 51 | 0 | 30 | Daily | None | 7 | 4 | 0 | 0 |
| 7 | 46 | 8 | 22 | Daily | None | 8 | 7 | 0 | 0 |
| 8 | 44 | 9 | 21 | Daily | None | 3 | 9 | 0 | 0 |
The results presented promising results for patients who suffer from chronic migraine and hot flashes. OnabotulinumtoxinA was effective in reducing these vasomotor symptoms. It is also important to note that patients who were receiving hormonal treatment with estrogens for hot flashes also showed improvement of this symptoms even after the withdrawal of hormonal treatment, indicating that OnabotulinumtoxinA could be safe and effective alternatives for treating hot flash symptoms in patients with chronic migraine.
The improvement in vasomotor symptoms observed in this case series may be due to the indirect effect of OnabotulinumtoxinA on the sympathetic nervous system, which plays a role in both migraine and vasomotor symptoms.
The hypothalamus indeed plays a crucial role in regulating various bodily functions, such as sleep, pain processing and regulation, body temperature, and hormonal control. It is believed that the use of OnabotulinumtoxinA can help reduce excessive activation of the hypothalamus, which results in a decrease in symptoms of chronic migraine.
In the case of hot flashes, which are characterized by a sudden sensation of intense heat, sweating, and flushing of the face, abnormal activation of the hypothalamus is believed to be associated with the symptoms. Therefore, the hypothesis is that treatment with OnabotulinumtoxinA, by reducing hypothalamic activation, may have helped control hot flash symptoms as observed in patients.
Conclusion
This case series suggests that OnabotulinumtoxinA may be effective in patients with chronic migraine and vasomotor symptoms. However, further studies are needed to confirm these findings and explore potential underlying mechanisms. Identifying effective treatments for these conditions is important for improving the quality of life for affected individuals and reducing the risk of associated complications.
Disclosure of Interest
None Declared.
Rody El Nawar*, Michelle Miscala, Sawsan Alhashmi, Katarina Pasalic and Farrukh Hamid
Reem Hospital, Abu Dhabi, UAE
Objective
Reversible visual symptoms are one of the most commonly reported aura in migraine patients. Literature shows visual auras subdivided into elementary visual symptoms (EVS) such as scotomas, flashes, and zigzag lines [1,2]. The aim of this retrospective study is to analyze the correlation between 3 variables: the number of EVS, monthly attack migraine, and the duration of the headache phase.
Methods
From 222 migrainous patients, we included 52 who met the diagnostic criteria for migraine with visual aura evaluated within 4 months. We collected demographic data for each patient including age, sex, comorbidities, family history of migraine, type of aura, number of EVS, monthly attack of migraine (MAM), duration of the headache phase, previous medications, etc. We measured the linear correlation and the covariance between each of the 2 variables, among the ones noted above.
Results
A total of 52 consecutive outpatients, diagnosed with visual aura migraine, (average age 39 years, 19% male and 81% female) were enrolled in our retrospective study. The number of EVS was counted in each patient. Foggy/blurry vision was the most common visual aura reported by our patients (65%), followed by flashes of bright lights (34%) and tunnel vision (32%). The majority of the patients described one type of EVS (38.46%), 2 classes (28.85%), and 3 types (21.15%). There was a negative correlation and covariance between the MAM and the number of EVS experienced by the patient (r = −0.157, cov = −1.962) and the duration of the headache phase and the number of EVS (r = −0.329, cov = −4.837).
Conclusion
Our data suggests that the number of monthly days of migraine and the duration of the headache phase is not related to the number of EVS experienced in the patients, studied. Further studies are required to prove this negative correlation and covariance between the 3 factors.
Disclosure of Interest
None Declared.
Masayki Goto1,2, Yasushi Shibata1, Sumire Ishiyama3, Yuji Matsumaru4 and Eiichi Ishikawa5
1Department of Neurosurgery, Headache Clinic, Mito Medical Center, Mito Kyodo General Hospital, University of Tsukuba, Mito, Japan
2Seirei Memorial Hospital, Hitachi, Japan
3Ibaraki Prefectural University of Health Sciences, Ami, Japan
4Department of Stroke and Cerebrovascular Diseases, University of Tsukuba, Tsukuba, Japan
5Department of Neurosurgery, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan
Background
Space headache is an important health issue associated with future human spaceflight, but no studies have examined changes in brain microstructure and function in space headache. The most likely hypothesis for the cause of space headache is that the loss of hydrostatic pressure in microgravity causes a shift of body fluid toward the head and changes the intracranial environment. A well-established method to reproduce this phenomenon on earth is the head-down-tilted bed rest (HDBR), in which the head is lowered 6–10° from the horizontal position in the supine position. In recent studies of headache pathophysiology, magnetic resonance imaging (MRI) diffusion tensor imaging (DTI), and resting-state functional imaging (rsfMRI) can be used to noninvasively assess dynamic changes in brain microstructure and brain function in real-time. In this study, we used DTI and rsfMRI to analyze changes in brain microstructure and brain function during HDBR-induced headaches.
Subjects
Twenty-eight healthy adults (11 males, 17 females, mean age 47.7 ± 11.7 years) without chronic headache or intracranial disease.
Methods
DTI and rsfMRI were performed in the horizontal supine position and HDBR, and headache symptoms and intensity were evaluated. DTI is a method to analyze the amount and direction of water molecule diffusion by applying a 6-directional gradient magnetic field. Fractional anisotropy (FA), Axial Diffusivity (AD), Radial Diffusivity (RD), and Mean Diffusivity (MD) were calculated and compared in the headache and non-headache groups. RsfMRI is an imaging method that captures changes in the amount of oxidized hemoglobin with increased brain activity as changes in signal intensity. 30 regions of interest were analyzed for Functional Connectivity (FC), and correlation analysis between FC and headache intensity was performed.
Results
Headache occurred in 21 of 28 subjects. DTI analysis showed that AD, RD, and MD significantly increased after HDBR, rsfMRI analysis showed that FC significantly decreased after HDBR. FC was significantly higher in the headache group before HDBR between the right inferior frontal gyrus and left cerebellum, and after HDBR between the brainstem and left inferior frontal gyrus, left hypothalamus and left cerebellum. Correlation analysis showed a positive correlation between FC related to the hypothalamus and headache intensity before HDBR, and a negative correlation between FC related to the thalamus and cerebellum and headache intensity after HDBR.
Conclusion
We reproduced the pathophysiology of space headache using HDBR and revealed brain microstructure and functional brain changes using DTI and fMRI. These results may serve as biomarkers for the prediction of space headache onset, diagnosis, and treatment, and will contribute to human space exploration.
Disclosure of Interest
None Declared.
Jong-Hee Sohn1,2, Eungue Lee1 and Songyi Park2
1Department of Neurology, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea, Republic of
2Institute of New Frontier Research Team, College of Medicine, Hallym University, Chuncheon, Korea, Republic of
Background
Several animal models of migraine have been described, some of which have been valuable in the development of new therapeutic targets. While the pathophysiology of chronic migraine (CM) transformed from episodic migraine (EM) is not fully understood, it is still useful to make a clear distinction between these two conditions. Consequently, we developed a mouse model to simulate EM and CM-associated pain and examined the variations in neuropathology between the two models.
Methods
To create the EM and CM mouse models, we employed nitroglycerin (NTG), a known trigger for human migraines. We administered a single intraperitoneal injection of 10 mg/kg NTG to induce the EM model and repeated the injections every other day for a total of five times over nine days to establish the CM model. Mechanical hypersensitivity was evaluated using the von Frey filament test in each migraine model. Subsequently, we performed immunofluorescence co-staining with c-Fos and NeuN antibodies to compare neuronal activation. Additionally, we examined the relationship between EM and CM and the number and activity of microglia using the Iba1 marker.
Results
We observed no significant differences in mechanical threshold in the hindpaw between the NTG-injected EM and CM models. However, there were distinct neuropathological differences in the anterior cingulate cortex (ACC) and spinal trigeminal nucleus caudalis (Sp5C) regions of the brain tissue in the EM and CM models. In the ACC region, the expression of c-Fos and NeuN remained unchanged in the EM model but significantly increased in the CM model (p < 0.01). Conversely, in the Sp5C region, the EM model exhibited significantly increased expression of c-Fos and NeuN compared to the CM model of NTG-injected mice (p < 0.01). Furthermore, the expression of Iba1 in the Sp5C region significantly increased in the EM model, whereas in the ACC region, it increased in the CM model (p < 0.01).
Conclusions
These results demonstrate neuropathological changes in neurons and microglia in the Sp5C and ACC regions between the EM and CM models of NTG-injected mice. These changes may play a role in the pathogenesis of the transformation from EM to CM.
Disclosure of Interest
None Declared.
Jong-Hee Sohn1,2, Jong-Ho Kim3,2, Young-Suk Kwon3,2 and Eungue Lee1
1Department of Neurology, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea, Republic of
2Institute of New Frontier Research Team, College of Medicine, Hallym University, Chuncheon, Korea, Republic of
3Department of Anesthesiology and Pain Medicine, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea, Republic of
Methods
We collected clinical data from the SMART Clinical Data Warehouse over a 11-years. We assessed the nutritional status of patients using the Controlled Nutrition Status (CONUT) score and Prognostic Nutrition Index (PNI). A total of 20,714 patients with migraine and 333,610 control subjects were identified.
Results
The final analysis included 6,603 patients with migraine and 90,509 non-headache controls. Compared to individuals with normal nutritional status, those with mild, moderate, and severe malnutrition showed a significantly higher risk of migraine according to the CONUT score (adjusted odds ratio [aOR]: 1.72, 95% confidence interval [CI]: 1.63–1.82, P < 0.001; aOR: 4.80, 95% CI: 3.85–5.99, P < 0.001; aOR: 3.92, 95% CI: 3.14–4.89, P < 0.001). After adjusting for confounding variables, we observed that moderate (PNI 35–38) or severe malnutrition (PNI < 35) were associated with a higher prevalence of migraine (aOR: 4.80, 95% CI: 3.85–5.99, P < 0.001; aOR: 3.92, 95% CI: 3.14–4.90, P < 0.001) compared to normal nutritional status.
Conclusion
This study demonstrates an association between the CONUT and PNI scores and the risk of migraine, suggesting their potential utility as predictors of migraine risk. Furthermore, these results highlight the potential of nutrition-based strategies for the treatment of migraines.
Disclosure of Interest
None Declared.
Kimberly De Iaco - Mc Cord1, Sonia Di Ciaccio1, Carlotta Bianchini1, Joshua Brown2 and Gianluca Coppola3
1Department of Medical, Pfizer Italia, Rome, Italy
2Pfizer, Inc., New York, USA
3Sapienza University of Rome Polo Pontino ICOT, Department of Medico-Surgical Sciences and Biotechnologies, Latina, Italy
Objectives
Migraine headaches are a common ailment in Italy with a prevalence of 13%. Triptans are an important line of treatment for the acute migraine attacks; however, limitations related to their mechanism of action on the cardiovascular system greatly reduce the pool of patients that can safely utilize this medication. We wish to describe the migraine sufferers in an Italian retrospective cross-sectional database including self-reported migraine status and health risk factors. We aim to assess their metabolic and cardiovascular risk factors, as to determine the rate of contraindication to triptan treatment.
Methods
We descriptively analyzed a sample of the 2020 EU National Health and Wellness Survey (NHWS, Cerner Enviza)1, a European population survey with self-reported disease and health metrics. We focused on the Italian subset of the population, and labelled migraine sufferers only when a self-reported physician diagnosis was present. We defined three groups: 1) metabolic syndrome (respondents reporting type-2 diabetes or obesity - BMI ≥30), 2) cardiovascular (CV) risk factors, with ≥2 risk factors deemed “high-risk” (respondents reporting atherosclerosis, hypertension, hypercholesterolemia or actively smoking), and 3) absolute triptan contraindication as indicated by the Italian drug label (respondents reporting arrythmias, congestive heart failure, myocardial infarction (MI), left ventricular hypertrophy (LVH), transient ischemia attack (TIAs), peripheral vascular disease (PVD), stroke and unstable angina/chest pains). There was overlap in the three subgroups (i.e., respondents could be counted in all three instances).
Results
Within the survey respondents in Italy (10’026 total) the prevalence of diagnosed migraine sufferers was 12.8% (1’287 respondents). Of these respondents with migraine headaches, 66.4% had metabolic syndrome and/or CV risk factors and 27.2% could be considered as having a high CV risk. Furthermore, 19.6% had an absolute contraindication to triptans use, and 71.5% had a contraindication, CV risk factor or metabolic syndrome. The most frequent CV risk factors were currently smoking (39.4%), hypercholesterolemia (30.6%) and hypertension (19.4%). Type-2 diabetes and obesity were reported in 4.7% and 9.9% of migraine respondents, respectively. The most reported absolute triptan contraindications were arrhythmias (12.9%), TIAs (2.4%) and MIs (2.1%). Compared to the Italian non-migraine sufferers, respondents suffering with migraine headaches had significantly higher frequencies of arrhythmias, TIAs, PVD and unstable angina/chest pains. In terms of cardiometabolic risks, the migraine sufferers also reported significantly higher frequencies of hypercholesterolemia and current smoking status and lower frequency of obesity.
Conclusions
The cardiometabolic risk factors and triptans treatment contraindications are not equally distributed among the Italian migraine and non-migraine sufferers, the former generally reporting higher instances of contraindication and risk factors. Depending on the range or risk that can be accepted for triptan utilization, as many as 28.5% of migraine sufferers in Italy could be ineligible for this treatment. Even with absolute triptan contraindication definition, we found almost 20% of the population as not being able to receive triptan treatment. This highlights a need for alternative treatments, particularly in patients with cardiometabolic risk factors.
Disclosure of Interest
Pfizer is a contributor of this publication.
Nazia Karsan*, King's College London, London, United Kingdom. NIHR King's Clinical Research Facility, London, United Kingdom
Objectives
Migraine is a symptomatically heterogenous complex brain disorder. There is preclinical evidence for monoaminergic and peptidergic dysfunction, and suggestions of changes on human functional neuroimaging in brain areas involving such pathways, like dorsolateral pons, hypothalamus and basal ganglia. Spectroscopy has provided some insights about brain neurochemistry in migraine, but specific brain circuitry changes within different neurotransmitter networks have not been further explored. As well as dopamine, serotonin and noradrenaline, glutaminergic, GABA-ergic, opioid and cannabinoid systems may also be involved and could be exploited with novel therapeutics.
We aimed to use receptor target maps with resting state functional MRI data to identify which neurotransmitters may be modulating brain circuitry alterations in migraine with and without aura, and to compare these to healthy controls.
Methods
We used Receptor-Enriched Analysis of Functional Connectivity by Targets (REACT) to estimate and compare the molecular-enriched functional networks of healthy controls (HCs, n = 21) and patients with migraine (n = 25), both with (MwA n = 15) and without aura (MwoA, n = 10). For REACT, we employed receptor density templates of the transporters of dopamine (DAT), noradrenaline (NAT) and serotonin (SERT), as well as the GABA-A, mGlu5, NMDA and CB1 receptors, and estimated the subject-specific voxel-wise functional connectivity (FC) maps related to these molecular systems in a mixed model analysis. We also ran a supplementary analysis focused on serotonin, exploring FC related to SERT, 5-HT1B and 5-HT2A. For each system, we ran voxel wise independent samples t-tests (HC vs migraine and MwA vs MwoA), including framewise displacement as a covariate of no interest.
Results
The results revealed significant differences in the NAT-, SERT- (specifically 5HT2A) and NMDA-enriched functional networks between the migraine group and HC. Only the NAT-enriched network survived statistical significance following multiple comparison correction (P = 0.0008). In the NAT-enriched network, we found increased functional connectivity in migraine compared HCs in a cluster including the right-sided frontal pole, middle and inferior frontal gyri and the precentral gyrus. The analyses of the MwA and MwoA subgroups showed significant decreases in the mGlu5, CB1 and 5HT2A functional networks in MwA, which did not withstand statistical significance following multiple comparison correction.
Conclusions
Our results show that noradrenaline is involved in brain connectivity alterations in areas of the prefrontal cortex in migraine. This provides a feasible neural substrate for symptoms of migraine including cognitive change and emotional behaviour. Further studies of this type with larger sample sizes are warranted.
Disclosure of Interest
The study was partly funded by the Migraine Trust
Peter Goadsby1,2, Ipek Kizil3 and Francois Cadiou3
1King's College London, London, United Kingdom
2University of California, Los Angeles, Los Angeles, USA
3Healint, Singapore, Singapore
Objective
The rhythmicity of migraine attacks has been suggested to have a chronobiological basis (1). Limitations of previous studies have been retrospective reporting and small to modest size data sets. Patterns of attack onset have implications for understanding the influence of circadian biology and on clinical advice for management of migraine. Our objective was to estimate the distribution of migraine attacks throughout the day using a patient-reported big data approach.
Methods
Data (attacks = 1,847,456) from users (n = 153,802) of a migraine diary app (MigraineBuddy®) from one time zone (Eastern Seaboard) of the United States, determined by geolocation, which was degraded for this analysis, and who had consented for their entries to be used for research, were collated anonymously. Migraine diagnosis was self-reported, and verified with provision of canonical features of a migraine attack that users record. Users on a preventive treatment were excluded (2). Users reported onset of headache pain for their attack, which was time and date stamped. The periodicity of the data was assessed using Fourier analysis with two harmonics of the time of onset (x) collapsed to the nearest hour of 24: g(x) = a0 + a1*cos(x*w) + b1*sin(x*w) + a2*cos(2*x*w) + b2*sin(2*x*w); a0, constant term; a1, a2, b1, b2, coefficients; w, angular frequency, where frequency is 2*π/w (Matlab 2023A, Mathworks). The distribution of time of attack was modelled using circular statistics, and tested for uniformity with a Rayleigh test evaluated at P < 0.05 (Matlab Circular Statistics Toolbox and R 4.2.2, Circular package).
Results
The users were predominantly female (60.8%), with 30.4% unknown, and aged 41 ± 13 (mean ± SD) years.
For the Fourier model,
a0 = 7.83e+04 (7.171e+04, 8.489e+04); a1 = −3.998e+04 (−4.595e+04, −3.402e+04)
b1 = 6961 (−5430, 1.935e+04); a2 = −1.244e+04 (−2.069e+04, −4195);
b2 = −1.313e+04 (−2.284e+04, −3416); w = 0.2692 (0.2405, 0.298)
The cycling frequency of attacks was 23:20 hours:minutes (21:51, 26:08, 95% confidence interval). The distribution of attacks was non-uniform (P < 0.0001). Attacks tended to occur between 06:00 and 10:00 with a median time of 11:00.
Conclusions
Migraine attacks have a cycling behaviour over the day with a predilection for attacks in the morning. Understanding the influence of the cycling neurobiology of migraine has implications for its pathophysiology and for clinical practice offering a potential pathway to individualized treatment using machine learning approaches.
Disclosure of Interest
PJG reports, over the last 36 months, a grant from Celgene, and personal fees from Aeon Biopharma, Allergan/Abbvie, Amgen, CoolTech LLC, Dr Reddys, Eli-Lilly and Company, Epalex, GlaxoSmithKline, Lundbeck, Novartis, Praxis, Sanofi, Satsuma, Shiratronics, Teva Pharmaceuticals and Tremeau, and personal fees for advice through Gerson Lehrman Group, Guidepoint, SAI Med Partners, Vector Metric, and fees for educational materials from CME Outfitters, and publishing royalties or fees from Massachusetts Medical Society, Oxford University Press, UptoDate and Wolters Kluwer, and for medicolegal advice in headache, and a patent magnetic stimulation for headache (No. WO2016090333 A1) assigned to eNeura without fee. IK and FC are employees of Healint, Inc.
Wei Zhao*, Zhihua Jia, Zhao Dong and Shengyuan Yu
Chinese PLA General Hospital, Beijing, China
Background
The changes in medication overuse headache (MOH) have been a subject of debate. Orbitofrontal cortex (OFC) dysfunction has been reported in patients with chronic migraine and medication overuse headache, and several studies have explored the associations between OFC dysfunction and substance abuse.
Objective
To investigate changes in decision-making among MOH patients in China.
Methods
This cross-sectional study recruited 30 patients with chronic migraine (CM) and MOH, 29 patients with CM without MOH, 62 patients with episodic migraine (EM), and 60 healthy controls (HC) at the headache center of the Chinese PLA General Hospital from March 2022 to February 2023. The data collected included demographic information, headache characteristics, Generalized Anxiety Disorder-7 (GAD-7) scores, Patient Health Questionnaire-9 (PHQ-9) scores, Pittsburgh Sleep Quality Index (PSQI) scores, and Severity of Dependence Scale (SDS) scores. The Iowa Gambling Task (IGT) was used to conduct a neuropsychological assessment of changes in decision-making.
Results
The net scores of the Iowa Gambling Task (IGT) showed significant differences among the three groups (2.24 ± 12.68 vs 11.52 ± 14.22 vs 14.90 ± 11.19, p<0.001). Post hoc analysis revealed that the CM group exhibited poorer performance than the EM group and the HC group, while there was no significant difference between the EM group and the HC group. We also compared the net IGT scores between CM patients with and without MOH. We found that CM patients with MOH had negative net scores (−1.87 ± 12.84), while CM patients without MOH had positive net scores (6.48 ± 11.20), and these differences were significant (−1.87 ± 12.84 vs 6.48 ± 11.20, p = 0.01). We observed significant correlations between net IGT scores and clinical variables, including mean monthly migraine days (r = −0.27, p = 0.003), frequency of acute medication use (r = −0.21, p = 0.024), GAD-7 scores (r = −0.19, p = 0.012), PHQ-9 scores (r = −0.16, p = 0.035), and SDS scores (r = −0.26, p = 0.050).
Conclusion
The present findings suggested that MOH patients exhibited decision-making dysfunction, and we found a significant correlation between changes in decision-making and mean monthly migraine days, frequency of acute medication use, severity of dependence on acute medication, GAD-7 scores.
Disclosure of Interest
None Declared.
Seung Ae Kim1, Eunji Lee2, Soo Hyun Ahn1 and Mi Ji Lee1,3
1Department of Neurology, Seoul National University Hospital, Seoul, Korea, Republic of
2Soonchunhyang University, College of Medicine, Seoul, Korea, Republic of
3Seoul National University College of Medicine, Seoul, Korea, Republic of
Orthostatic headache is a hallmark symptom of spontaneous intracranial hypotension (SIH). However, SIH can manifest without headache, which can lead to a significant delay in treatment initiation. We hereby report a 70-year-old male with progressive gait disturbance and superficial siderosis. MR myelography showed an extensive extradural cerebrospinal fluid collection in the cervicothoracic spine. After a series of targeted epidural blood patch, the patient’s symptoms significantly improved. SIH should be considered as a potential cause of otherwise unexplained superficial siderosis to prompt an early diagnosis and treatment.
Disclosure of Interest
All the authors have no financial interests to disclose. We certify that all the authors have read and approved the submission of the abstract and the manuscript, and no work resembling the enclosed article has been published or is being submitted for publication elsewhere. We certify that we have each made a substantial contribution so as to qualify for authorship.
Cita Christine, Selviana Dian Pratiwi, Henry Riyanto Sofyan, Irma Savitri, Raymond Aris Nimrod Alvonsius Silalahi, Elizabeth Albertin and Tiara Aninditha*
Department of Neurology, Faculty of Medicine, Universitas Indonesia, Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Objective
This research aimed to assess the differences between knowledge, attitude, and practice among neurologists and general practitioners in Indonesia toward migraine patients.
Methods
We conducted an observational study among doctors attending a national neurology symposium. To gather data, we utilized a structured questionnaire consisting of nine items measuring knowledge, five items assessing attitude, and five items evaluating practice in relation to migraine. The collected data on knowledge, attitude, and practice were categorized into two groups: general practitioners (GPs) and neurologists. Analysis of the data was performed using SPSS version 26.
Results
The study involved 318 subjects, with neurologists having an average age of 42 years and GPs having an average age of 28 years. The majority of participants were women (65.4%). It was observed that neurologist significantly had better knowledge and practice related to migraine compared to GPs (PR > 1; p < 0.05). Regardless, there was no significant difference observed in knowledge, attitude, and practice regarding the use of headache diary (HD) for migraine patients (p > 0.05). A high percentage (77%) of subjects were familiar with HD, and all subjects agreed to use it when managing and evaluating migraine patients. However, only 24.2% of the subjects have utilized a headache diary in their daily practice. Both neurologists and GPs (94%) recognized the importance of administering abortive treatment early after the onset of migraine symptoms. Neurologists showed a moderately stronger association between attitude and practice (r = 0.461; p < 0.001) regarding the early use of abortive treatment for migraine symptoms compared to GPs (r = 0.184; p = 0.022). Moreover, 85.5% of doctors claimed to understand the diagnostic criteria for migraine, according to the International Headache Society (IHS). However, only 24.2% provided the correct answer regarding the diagnostic criteria for common migraine. Similarly, 99.1% of doctors agreed to prescribe prophylaxis for indicated migraine patients, yet only 12.9% demonstrated a better understanding of the indications for prophylaxis in migraine.
Conclusion
This study found that neurologists were more capable in knowledge and practice related to migraine management compared to GPs. However, no significant difference was observed in knowledge, attitude, and practice regarding the application of headache diary (HD) for migraine patients. Furthermore, the study revealed that more than half of the GPs and neurologists had inadequate knowledge of migraine diagnosis and prophylaxis administration indications. Additionally, there was a low rate of HD utilization in the daily practices of both GPs and neurologists. Regular education focusing on migraine diagnosis, HD implementation, and therapy is essential to enhance knowledge and awareness.
Abbreviation: General Practitioner (GP), Headache Diary (HD), International Headache Society (IHS)
migraine, knowledge, attitudes, practice, headache diary
Niamh Davies-Branch*, Greig Russell, Sean Lance, Pietro Cariga and Calvin Chan
Te Whatu Ora, Palmerston North Hospital, Palmerston North, New Zealand
Objective:
The greater occipital nerve block (GONB) is a recognised adjuvant treatment for prevention of primary headache disorders such as migraine and the trigeminal autonomic cephalagias. Palmerston North Hospital is a secondary centre with a newly established headache clinic offering this procedure. Outcomes of this pilot study included overall efficacy, side effects, and reduction in; severity, frequency, and number of severe headache days per month after GONB with 80mg methylprednisone and 2ml 2% lidocaine. The secondary aim was to establish which, if any, headache phenotypic features could predict GONB response.
Methods
A retrospective study was conducted of all patients with a diagnosis of migraine with or without aura who received a GONB. Patients were identified from clinic letters between December 2020 and May 2023. Statistical analysis was carried out using R Statistical Software (V2.18.1.1 R CoreTeam 2022). A p value of <0.05 was considered statistically significant and Chi-squared test with Yates continuity correction was used.
Results
A total of 78 patients were identified over the age of 16 with existing clinic follow-up post procedure, or with telephone follow-up. Median follow-up was 14 months. Of the patient cohort, the mean age was 42.4 years, and the female to male ratio was 60:16. 2 patients were male to female transitioned. Seven patients (9%) were of Maori descent. The median number of headache days per month and severe headache days per month was 30, and 14 days respectively. The most common associated symptoms were photosensitivity (88%) and nausea (79%). Forty-nine (63%) patients had medication overuse.
Fifty-six (72%) patients found the GONB effective, with a reduction in severity more common than frequency reduction (69% versus 47%). Rate of minor adverse events was 18% (n = 14) which included pain or lump at site of injection, or transient lightheadedness. 4 (5%) patients had worsening headache after the GONB. The median duration of relief post GONB was 8 weeks (range 0–80 weeks).
Nausea as an associated headache symptom was found to significantly reduce GONB benefit duration (mean 26.4 weeks versus 12.7 weeks, p = 0.04). There was also a trend towards nausea and reduced overall GONB effectiveness (p = 0.06). Other associated symptoms including photosensitivity, vertigo, cranial allodynia and movement sensitivity did not significantly affect outcome of a GONB (all p > 0.26).
Conclusion
GONB continues to be a useful intervention for chronic migraine headaches. 72% of our patients found overall relief after GONB and reported few side effects. We identified nausea as an associated headache symptom negatively predicting GONB efficacy. A larger study is required to further corroborate our findings and identify other associated symptoms that predict efficacy.
Disclosure of Interest
None Declared.
Laura Gómez-Dabó1, Alicia Alpuente1, Javier A Membrilla2, Javier Díaz de Terán2, Joana Rosell-Mirmi1, Marta Torres-Ferrus1, Edoardo Caronna1, Maria Arranz1 and Patricia Pozo-Rosich1
1Vall d'Hebron University Hospital, Barcelona, Spain
2La Paz University Hospital, Madrid, Spain
Objective
Patients presenting with headache who seek medical attention in the emergency room often encounter a hostile environment, experience extended waiting times for clinical care, and receive ineffective pain management. Considering these challenges, we have developed a Headache Protocol (HP) to enhance patient care and streamline the management of these patients. This study aims to evaluate adherence to the protocol and assess the impact of implementing the HP on attention timings, utilization of neuroimaging, and treatment outcomes.
Methods
Consecutive adult patients with headache who received medical care in the emergency room of a tertiary hospital between October 2022 and April 2023 were recruited. The HP involved providing patient care based on the urgency of the situation and the necessity for prompt diagnosis in cases of suspected life-threatening secondary headache disorders, as well as timely treatment for pain and associated symptoms in cases of suspected worsening of primary headache disorder. Existing red flags were categorized based on their level of urgency, leading to the development of three headache scales: HEAD1 (for emergent care), HEAD2 (for urgent care), and PEACE (for non-urgent care but requiring assessment for secondary headaches). These scales were designed to help assess and prioritize patients' conditions based on the severity of their symptoms and the presence of concerning signs, allowing for appropriate and timely medical intervention. Data were prospectively collected using a variable record sheet. The collected data included demographic information, time to diagnosis, utilization of neuroimaging, treatment administered, and scores on three headache scales. Compliance with regards to time to diagnosis, neuroimaging utilization, treatment, and scores on the three scales were analyzed.
Results
We included a total of 678 patients, of whom 66% were women, with a mean age 40.8 years. Data regarding the HEAD1 scale were obtained for 591 out of 678 (87.2%), with a score of ≥2 observed in 36 out of 591 cases (0.17%).In these patients, which indicated the need for emergent assessment and neuroimaging within 10 minutes, the mean attention time (MAT) was 82.2 minutes ( ± 61.04) and the mean neuroimaging time (MNT) was 213.6 minutes ( ± 58.7). Neuroimaging was performed in 19 out of 36 cases (52.78%), and pathological results found in 21% of these cases. Among the remaining 555 patients, 382 out of 555 (68.82%) obtained a score of ≥2 on the HEAD2 scale, indicating the need for assessment and treatment within 30 minutes. The MAT was 77.82 minutes ( ± 55.4) and the treatment time (TMT) was 111.9 minutes ( ± 50.7). PEACE data was obtained for 158 out of 555 (28.47%), and more than one criterion was met in 103 out of 158 cases (65.19%), suggesting the need for neuroimaging. Neuroimaging was performed in 42 out of 103 cases, with an MNT of 221.1 minutes if HEAD2≥2 and 197 minutes if HEAD2< 2.
Conclusions
During the initial 6-month period of implementation, there was a low level of adherence to the HP, leading to failure in meeting the established diagnostic and treatment objectives, despite efforts in clinical education. Enhancing the clinical care provided to these patients is crucial to enable early identification of secondary headaches and reduce the treatment duration for primary headaches.
Disclosure of Interest
None Declared.
Marta Torres-Ferrus1,2, Edoardo Caronna1,2, Alicia Alpuente1,2, Ruth Mas-de- les-Valls2, Eulalia Gine-Cipres1,2 and Patricia Pozo-Rosich1,2
1Vall d'Hebron University Hospital, Barcelona, Spain
2Vall d'Hebron Research Institut, Barcelona, Spain
Objective
To compare the response in terms of frequency reduction and change in patient-reported outcomes between erenumab (ERE) and onabotulinumtoxinA (OnabotA) after 6 months of treatment.
Methods
This prospective study included two parallel cohorts of patients with chronic migraine who were treated with ERE 140mg/month or OnabotA 195U/3 months. We included patients without other preventive treatments or psychiatric or chronic pain comorbidity. Baseline data, including demographic information, headache frequency (headache-migraine days per month – MHD, migraine days per month – MMD), impact scales (MIDAS, HIT-6, MSQ), and anxiety and depression levels (BAI, BDI-II) were collected at baseline and after 6 months of treatment. Baseline variables were balanced between the two treatment groups. The difference in efficacy between two groups was assessed using the ANOVA test for repeated measures and linear regression models in R.
Results
A total of 84 patients were included in the study (ERE = 42, BTX = 42) without significant differences in baseline variables between the groups. The baseline headache frequency was 18 (13–21) MHD for the ERE and 17 (15–20) MHD for OnabotA group. After 6 months of treatment, both groups showed a statistically significant reduction in headache frequency (ERE: −7.6 MHD, −5.1 MMD, p < 0.001; OnabotA: −4.93 MHD, −3.27 MMD, p < 0.001). There were no statistically significant differences in efficacy between the two treatment groups (p = 0.042). Significant reductions in HIT-6 and MSQ scores were observed in both groups (p < 0.05). Patients treated with ERE also showed significant improvements in MIDAS, BDI, and BAI scores (p < 0.05).
Conclusions
Erenumab and onabotulinumtoxinA are both effective preventive treatments for chronic migraine. However, patients treated with Erenumab demonstrated a higher reduction in headache frequency and significant improvements in disability, anxiety, and depression scales compared to those treated with OnabotulinumtoxinA.
Disclosure of Interest
MTF, EC, AA, EG, PPR reports personal fees and non-financial support from Allergan, Abbvie, Novartis, Eli&Lilly and/or TEVA
Hauke Basedau*, Kuan Po Peng, Marlene Schellong and Arne May
Department of Systems Neuroscience, University Medical Centre Hamburg-Eppendorf, Hamburg, Germany
Background
Monoclonal antibodies targeting calcitonin gene-related peptide (CGRP) or its receptor have been suggested to modify central processing of trigeminal nociception. However, it remains uncertain whether these effects are solely attributed to the longitudinal data collection process or if they can be attributed to the administration of a prophylactic agent known to be effective against migraine. This would mean that any changes are attributed to the overall improvement of migraine but not specific medication effects.
Methods
In order to address this uncertainty, we conducted a double-blind, randomized, placebo-controlled functional magnetic resonance imaging (fMRI) study with 40 participants diagnosed with migraine. We utilized an established trigeminal nociceptive paradigm involving the use of gaseous ammonia, similar to previous studies. Additionally, we employed an arterial spin labelling protocol to control for general medication induced blood flow changes. Participants were randomized by an independent investigator to receive either verum (erenumab 70 mg monthly for 2 months) or placebo (equivalent volume of saline solution). Baseline fMRI scans were conducted prior to the initiation of verum/placebo administration, and subsequent scans were performed after 4 weeks, followed by a second administration. Participants kept a headache diary throughout the study. Following previous studies using functional imaging, a clinical response was defined as a ≥30% reduction in headache frequency at follow-up.
Results
Twenty-one participants were randomized to the verum and the other 19 participants to the placebo group. Medications were well tolerated, none of the participants had to be excluded due to side effects. Analysis of the headache diaries after 2 months showed that 11 participants (27.5%, n = 40) experienced improvements in migraine activity, characterized by a minimum of 30% reduction in monthly headache frequency compared to baseline. Among these responders, seven were in the verum group (33.33% of the verum group) and four in the placebo group (21.05% of the placebo group).
Regarding the imaging outcomes, our preliminary findings indicate that the initiation of erenumab administration resulted in specific alterations in the ascending trigemino-nociceptive pathways, which were not observed in the placebo group.
Conclusion
Our study provides further evidence that monoclonal antibodies targeting the calcitonin gene-related peptide pathway modulates the central trigeminal pain processing. These changes were only seen in the erenumab verum group. It is important to note that the response rates to erenumab 70mg were not as substantial as anticipated in 2019, when this study was planned, resulting in a relatively small sample size for a subgroup analysis based on the responder status.
Disclosure of Interest
This study received an unrestricted grant from Novartis to the University Medical Centre Hamburg-Eppendorf. The funding sources did not influence study conduction in any way.
Victor Wang1, Michael Li2, J. Alex Wrem3, Mary Hopkins1 and Hsiangkuo Yuan1
1Jefferson Headache Center, Department of Neurology, Thomas Jefferson University, Philadelphia, USA
2Health Data Science, Information Services & Technology, Thomas Jefferson University, Philadelphia, USA
3Department of Family Medicine, Thomas Jefferson University, Philadelphia, USA
Objective
To assess the real-world medication usage and switch profile of Calcitonin Gene-Related Peptide Receptor (CGRP) monoclonal antibody (mAb) and antagonist (gepant) medications at a tertiary headache center. Patients with refractory migraine often undergo multiple unsuccessful medication treatments with limited improvement. To date, the efficacy of CGRP mAb and gepant medications has been established in both episodic and chronic migraine patients. However, data regarding these medications’ switch profiles and effects on patient headache burden remain limited and understudied.
Methods
This is a retrospective study conducted at Jefferson Headache Center (JHC), a tertiary headache facility. Electronic medical record data from patients with a diagnosis of migraine seen by JHC providers for at least two visits from December 1, 2018 to March 25, 2023 was analyzed with respect to patient demographics, ambulatory encounter diagnoses, medication orders, lab results, vital signs, patient problem lists, outcomes from patient surveys, inpatient admissions and discharge information. The following study is IRB exempt.
Results
We identified a total of 7,997 patients with migraine seen with an average and median age of 48 years, 6029 (75%) were female, 6,743 (84%) were white, and 658 (8%) were black. Of the total patients with migraine, 3,743 (46.8%) were ever prescribed at least 1 CGRP mAb: galcanezumab (980, 26.2%), erenumab (662, 17.7%), and fremanezumab (560, 15.0%). Of the mAb switch combinations, those involving erenumab and galcanezumab were the most common (302, 8.1%), followed by galcanezumab and fremanezumab (275, 7.3%), then by erenumab and fremanezumab (252, 6.7%). Of the total patients with migraine, 3,302 (41.3%) patients had been prescribed at least one gepant medication: ubrogepant (1,123, 32.5%), rimegepant (1,073, 32.5%), and atogepant (66, 2.0%). Of the gepant switch profiles, the preventive gepants atogepant and rimegepant had 54 patients (1.6%) on both medications, whereas the abortive gepants rimegepant and ubrogepant had 850 patients (25.7%) prescribed both medications. Patient outcome surveys revealed that the median headache days per month for patients in this study was 20 days, with a median intensity of 5 out of 10.
Conclusion
We describe the CGRP mAb and gepant medication usage and switch profiles at JHC. Many patients switched between CGRP mAb medications and between gepant medications. Further investigation into the reason for the switch and its effect on headache outcomes remains to be conducted.
Disclosure of Interest
Michael Li has received personal compensation for serving as an employee of Pascal Metrics. Michael Li has received stock or an ownership interest from Pascal Metrics. Hsiangkuo Yuan has the following disclosures: • Grants: NIH (R44NS115460, Drug-Free Nerve Block Device for the Relief of Pain and Symptoms in Migraines and Other Headaches) • Site investigators: Teva, Abbvie, Trillen, Thermaquil • Consultants: Silva, Clexio, Pfizer • Royalties: Cambridge University Press, Medlink
Norma Barajas1, Alexander Pabon Moreno1, Oscar Peñuela1 and Gustavo Gaitan Quintero2
1Hospital internacional de Colombia, Piedecuesta Santander, Colombia
2Universidad del Sinu, Cartagena Bolivar, Colombia
Case Report
Our patient, a 15-year-old adolescent, abruptly presented with blurred vision in her right eye and ocular pain. A few minutes later, a headache with migrainous characteristics on the same side occurred, accompanied by photophobia, nausea, and vomiting. Upon arriving at the emergency service, the patient showed normal vital signs, mydriasis, and anisocoria of 6/3 in the right eye. Neuroimaging tests and laboratory analyses were normal. Treatment with NSAIDs, flunarizine, and topiramate resulted in a quick improvement of the visual symptoms, although the anisocoria persisted for several months.
Conclusions
The ciliary ganglioplegic migraine is a benign cause of unilateral mydriasis. The duration of mydriasis can vary, ranging from hours accompanied by headache to several months. This condition responds well to cholinergic agents like pilocarpine. In relation to the pharmacological management of the migraine, conventional treatment is followed with positive results. It is always essential to carry out vascular neuroimaging and cranial nerve studies to rule out other causes such as tumors and aneurysms. Specifically, it has been reported that non-aneurysmatic vascular conflicts of the third pair can produce similar symptoms. Despite its benign nature, it is vital that physicians are familiar with this pathology in order to provide adequate management.
Disclosure of Interest
None Declared.
Jae-Moon Kim1 and Eunyoung Kim2
1Chungnam National University Hospital, Daejeon, Korea, Republic of
2Sejong Chungnam National University Hospital, Sejong, Korea, Republic of
Turtle headache is a rare headache syndrome of sleep-related headache and called as "clock-wise" or an "alarm clock" headache. Diagnostic criteria of turtle headache according to the ICHD-3 criteria, headache have to occur at least 10 days a month for greater than 3 months and last for 15 minutes up to 4 hours after waking. Unlike typical hypnic headache, headache onset started early in the morning just before awakening.
We report three patients with turtle headache. All the patients were female and onset-age was 62, 65 and 77 years each. Severity of headache was mild to moderate and Brain MRI revealed no abnormality related to headache. These patients were successfully treated with flunarizine and melatonin. All the patients wake up at 5 to 6 AM in the morning with tolerable headache. Characteristics of headache were dull in nature with minimal pounding nature, bilateral, no autonomic symptoms, and last 30 minutes to two hours.
Headache in these patients were different with typical hypnic headache as 1) headache onset was early in the morning just before awakening; 2) headache severity were mild to moderate; 3) headache was successfully treated with flunarizine and melatonin.
Disclosure of Interest
None Declared.
Song Guo1,2, Anders Hay-Schmidt2, Messoud Ashina1, Ayodeji Asuni3, Jes Olesen1 and Sarah Louise Christensen1
1Department of Neurology, Danish Headache Center, Copenhagen University Hospital – Rigshospitalet Glostrup, Copenhagen, Denmark
2Department of Odontology, Panum Institute, Faculty of Health, University of Copenhagen, Copenhagen, Denmark
3Department of Neuroscience, H. Lundbeck A/S, Copenhagen, Denmark
Objective
To increase our understanding of the mechanisms of how pituitary adenylate cyclase-activating peptide-38 (PACAP38) causes migraine-like hypersensitivity via its receptors VPAC1 and VPAC2 in a rodent model. A recent phase II trial using monoclonal antibodies (mAbs) to inhibit PACAP38 showed positive results in migraine prevention, whereas antibodies targeting the PAC1 receptor had previously failed. Better understanding of the PACAP-PACAP receptor interaction may identify more specific drug targets with better efficacy and fewer side effects.
Methods
We used an in vivo mouse model of provoked migraine-like hypersensitivity based on multiple PACAP38 injections and subsequent measurement of cutaneous tactile sensitivity response with von Frey filaments. PACAP38 response was tested in wildtype (WT) and two genetically modified strains of knockout (KO) mice lacking the respective PACAP-receptors: VPAC1 or VPAC2 (ntotal = 90). We also conducted ex vivo experiments in the same mice using myograph to test for vasoactivity and performed qPCR to confirm the lack of mRNA expression of the receptors.
Results
PACAP38 significantly induced hypersensitivity in both WT and KO mice (P < 0.009), and we found no significant difference in PACAP38 response between WT and VPAC1 or VPAC2 KO mice (P > 0.05). However, exploratory analyses using area under the curve showed a partial diminished PACAP38 response in VPAC1 and VPAC2 KO mice compared to WT (P < 0.05). Myograph experiments supported this finding and showed partial or compensated vasoactivity in KO mice.
Conclusion
This is the first study testing the effect of both VPAC1 and VPAC2-receptors on the same in vivo mouse model. The absence of VPAC1 and VPAC2 receptors in mice deficient of these receptors did not show a statistically significant reduction in the response to PACAP38, but we found a trend of partial diminished response. The findings suggest that these receptors may not be solely responsible for the induction of migraine-like pain but may instead act in conjunction. It is also possible that other receptors or compensatory mechanisms play a role in the genetically modified mice.
Disclosure of Interest
Jes Olesen owns the start-up company Cephagenics. MA is a consultant, speaker, or scientific advisor for AbbVie, Amgen, Eli Lilly, Lundbeck, Novartis, Pfizer and Teva; primary investigator for AbbVie, Amgen and Lundbeck ongoing trials. MA has no ownership interest and does not own stocks of any pharmaceutical company. MA serves as associate editor of Cephalalgia, associate editor of the Journal of Headache and Pain, and associate editor of Brain. All other authors report no competing interests.
Edoardo Caronna1, Victor José Gallardo1, Alicia Alpuente1, Marta Torres-Ferrus1, Mariano Huerta Villanueva2, Albert Muñoz2, Sergio Campoy2, Elisa Cuadrado Godia3, Laura Dorado4, Victor Obach5, Neus Fabregat5, Jaime Rodriguez Vico6, Javier Diaz de Teran7, Javier Membrilla7, Julio Pascual8, Gabriel Garate8, Ana Gago9, Angel Guerrero10, Jordi Sanahuja11, Antonio Sánchez Soblechero12, Alberto Lozano Ros12, Pablo Irimia Sieira13, Margarita Sanchez del Rio13, Amaya Echeverría Urabayen14, David Garcia Azorin10, Yesica Gonzalez Osorio10, Vicente Gonzalez Quintanilla8, Alba Lopez Bravo15, Iris Fernández Lázaro9, Sonia Quintas Gutierrez9, Alicia González-Martínez9, Belén Flores Pina4, Paula Manera Zorrilla-Lequerica3, Alex Jaimes Sanchez6, Andrea García Gómez6, Rocío Álvarez Escudero16, Agustín Oterino Durán16, Fernando Velasco Juanes17, Walter Sifontes17, Joana Rodriguez Montolio18, Candela Nieves Castellanos19, Marina Olivier19, Almudena Layos-Romero20, Alberto Andrés López20, Francisco Sánchez Caballero21, Isabel Beltrán Blasco22, Manuel Millán Vázquez23, Raquel Lamas Pérez23, Javier Viguera Romero21, Sonia Santos-Lasaosa18, Samuel Diaz Insa19, Carmen González Oria23, André Caetano24, Gonçalo Cabral24, Liliana Pereira25, Elisa Martins-Silva25, Isabel Luzeiro26, Catarina Fernandes26, Isabel Pavao Martins27, Beatriz Nunes Vicente27, Inês Marques28, Renato Oliveira28, Cem Thunstedt29, Andreas Straube29, Valeria Caponnetto30, Raffaele Ornello30, Gloria Vaghi31, Roberto De Icco31, Sabina Cevoli32, Paola Torelli33, Gabriella Egeo34, Christina Heidemann Sundal35, Marta Waliszewska36, Mona Ghadiri-Sani37, Ruth Ruscheweyh29, Raquel Gil-Gouveia28, Simona Sacco30, Cristina Tassorelli31, Piero Barbanti34 and Patricia Pozo-Rosich1
1Vall d´Hebron, Barcelona, Spain
2Hospital de Bellvitge - Hospital de Viladecans, Barcelona, Spain
3Hospital del Mar, Barcelona, Spain
4Hospital Universitario Germans Trias i Pujol, Barcelona, Spain
5Hospital Clinic, Barcelona, Spain
6Fundación Jiménez Díaz, Madrid, Spain
7Hospital La Paz, Madrid, Spain
8Hospital Univ. M. de Valdecilla, Santander, Spain
9Hospital La Princesa, Madrid, Spain
10Hospital Clínico Universitario de Valladolid, Valladolid, Spain
11Hospital Arnau de Villanova, Lleida, Spain
12Hospital Gregorio Marañon, Madrid, Spain
13Clínica Universidad de Navarra, Pamplona, Spain
14H Universitario de Álava (HUA), Alava, Spain
15Hospital Reina Sofia, Tudela, Spain
16Hospital Universitario Central de Asturias, Oviedo, Spain
17Hospital Universitario Cruces, Bilbao, Spain
18Hospital Lozano Blesa, Zaragoza, Spain
19Hospital Universitario La Fe, Valencia, Spain
20Hospital General Universitario de Albacete, Albacete, Spain
21Hospital Virgen de la Macarena, Sevilla, Spain
22Hospital General Universitario Dr. Balmis Alicante, Alicante, Spain
23Hospital Virgen del Rocío, Sevilla, Spain
24Centro Hospitalar de Lisboa Ocidental, Lisboa, Portugal
25Hospital Garcia Orta, Almada, Portugal
26Centro Hospitalar Universitário de Coimbra, Coimbra, Portugal
27Hospital de Santa Maria, Lisboa, Portugal
28Hospital da Luz Lisboa, Lisboa, Portugal
29Klinikum der LMU München, Munich, Germany
30Department of Biotechnological and Applied Clinical Sciences, University of L'Aquila, L' Aquila, Italy
31Fondazione Mondino, Pavia, Italy
32IRCCS Istituto delle Scienze Neurologiche, Bologna, Italy
33Unit of Neurology, Department of Medicine and Surgery, Headache Center, University of Parma, Parma, Italy
34Headache and Pain Unit, IRCCS San Raffaele Pisana, Rome, Italy
35Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
36Wrocław Medical University, Wroclaw, Poland
37THE WALTON CENTRE NHS FOUNDATION TRUST, Liverpool, United Kingdom
Objective
To describe the efficacy and safety of anti-CGRP monoclonal antibodies (mAbs) in real life in Europe.
Methods
Multicenter, observational study based on prospective registries of adult patients with high-frequency episodic (HFEM) or chronic (CM) migraine treated with anti-CGRP mAbs in Europe since January 2019. We collected demographic data, efficacy variables (headache days/month-HDM; migraine days per month-MDM, acute medication days/month-AMDM) and side effects. We analyzed efficacy (≥50%; ≥75% and 100% reduction in HDM) and safety at 6 months.
Results
35 European centers participated. We included a total of 5817 patients from Spain (63.9%), Italy (22.5%), Portugal (5.2%), UK (4.0%); Germany (2.1%), Sweden (1.6%) and Poland (0.6%). Demographics: Median age was 48.0 (40.0,55.0) years old, 82.3% (4785/5817) were women. 27.8% (1620/5817) had HFEM, 72.2% (4197/5817) had CM. Baseline headache characteristics: 20.0 (14.0, 28.0) HDM; 15.0 (10.0,20.0) MMD and 15.0 (10.0,24.0) AMDM. 62.5% (3153/5817) had medication overuse. Treatments prescribed: erenumab 46.4%; galcanezumab 28.1%, fremanezumab 25.6%. Outcomes: At 6 months (n = 4962), 56.5% (2803/4962) were ≥50% responders, 26.7% (1324/4962) ≥75% responders, and 2.1% (104/4962) 100% responders. There was a median reduction in HDM of −8.0 (−15.0,−3.0) days/month (p < 0.001). Side effects were reported in 19.8% (920/4962) patients, constipation being the most frequent (39.5%). 8.4% (462/5742) of patients discontinued treatment at 3 months, whereas 8.0% (369/4962) at 6 months (7.3% lack of efficacy; 0.5% lack of tolerability; 0.2% pregnancy).
Conclusion
the real-life data derived from this large European observational cohort show that anti-CGRP mAbs are effective, well tolerated, and safe in HFEM and CM, with response rates comparable to those found in clinical trials.
Disclosure of Interest
EC has received honoraria from Novartis, Chiesi, Lundbeck, MedScape; his salary has been partially funded by Río Hortega grant Acción Estratégica en Salud 2017–2020, Instituto de Salud Carlos III (CM20/00217). PPR has received, in the last three years, honoraria as a consultant and speaker for: AbbVie, Biohaven, Chiesi, Eli Lilly, Lundbeck, Medscape, Novartis, Pfizer and Teva. Her research group has received research grants from AbbVie, Novartis and Teva; as well as, Instituto Salud Carlos III, EraNet Neuron, European Regional Development Fund (001-P-001682) under the framework of the FEDER Operative Programme for Catalunya 2014–2020 - RIS3CAT; has received funding for clinical trials from AbbVie, Amgen, Biohaven, Eli Lilly, Novartis, Teva. She is the Honorary Secretary of the International Headache Society. She is in the editorial board of Revista de Neurologia. She is an associate editor for Cephalalgia, Headache, Neurologia, The Journal of Headache and Pain and Frontiers of Neurology. She is a member of the Clinical Trials Guidelines Committee of the International Headache Society. She has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. She is the founder of www.midolordecabeza.org. PPR does not own stocks from any pharmaceutical company.
Michael Lowe*, Laura Stobo, Anissa Benchiheub, George Gorrie, Sarah Miller, Alok Tyagi and Krishna Dani
Institute of Neurological Sciences, Glasgow, United Kingdom
Objective
The utility of switching between monoclonal antibodies to calcitonin gene-related peptide (CGRP-mAbs) in patients with chronic migraine who do not respond to, or develop adverse effects, with a first CGRP-mAb is uncertain.
We present our experience of switching between CGRP-mAbs in a tertiary headache service.
Methods
A retrospective case note review was undertaken as part of a clinical effectiveness evaluation. We identified 54 patients who had switched CGRP-mAb.
In our service all patients starting a CGRP-mAb are evaluated at baseline and 12 weeks with headache diaries in a nurse & pharmacist led CGRP clinic. Patients record headache duration, severity and medication used daily. We defined a severe headache day as a day with an average pain score of 7 or above on a scale of 0–10. For purposes of standardisation a month was considered a 4-week period. Data are recorded on a standardised proforma at each clinic visit and entered into a database. Positive response was defined as a 50% or greater reduction in severe headache days or a 30% or greater reduction in total headache days. We also assessed longer term outcomes from documentation in the electronic health record.
Patients who had not responded to a CGRP-mAb after 12 weeks, or reported loss of response on later follow up were offered treatment with a second or third CGRP-mAb. We targeted a washout period of 3 months between treatments, but this was not strictly adhered to.
Results
Most patients (50/54, 93%) had been given erenumab as the first CGRP-mAb. The reason for switching was lack of response in 28 patients (52%), loss of response over time in 16 patients (30%), adverse effects in 5 patients (9%) and rotation of treatment in 5 patients (9%). The gap between stopping the first CGRP-mAb and commencing the second was <3 months in 8 patients (15%), 3–6 months in 24 patients (44%) and >6 months in 22 patients (41%).
In patients who had switched CGRP-mAb due to lack of response or loss of response, evaluation of headache diaries at baseline and 12 weeks showed significant reductions in monthly headache days (mean reduction 5.8 days, p < 0.0001) and severe headache days (mean reduction 5.5 days, p < 0.0001). The overall response rate by the above definition was 58% in this group.
On extended follow up of the 44 patients switching CGRP-mAb due to lack of or loss of response, 10 patients (23%) had a positive response over at least 1 year of follow up. A further 5 patients (11%) had an ongoing positive response but had not yet reached 1 year of follow up.
16 patients who had not responded to a second CGRP-mAb were prescribed a third. The third CGRP-mAb was fremanezumab in 7 (44%) patients and galcanezumab in 9 (56%) patients. After 12 weeks there was no significant difference in headache days or severe headache days compared to baseline. 3 patients (19%) continue on treatment with a reported positive response, but none have reached 1 year of follow up. The remaining 13 patients discontinued treatment due to inefficacy.
Conclusion
We find that, in patients who did not respond to a first CGRP-mAb or lost response after an initial improvement, a trial of a second CGRP-mAb resulted in significant improvement in the first 12 weeks of treatment. A sustained response over time was seen in 34% of patients. Response to a third CGRP-mAb (after non-response to two prior treatments) was less promising.
The majority of patients in our cohort had used erenumab as the first treatment, as this was the first CGRP-mAb available for use in our centre. Erenumab targets the CGRP receptor, whilst fremanezumab and galcanezumab target the ligand. It is possible that the difference in mechanism may account for some of the difference in response between CGRP-mAb. Later cohorts of patients in our centre have been commenced on fremanezumab or galcanezumab first line and data from patients in these cohorts who have switched to a second CGRP-mAb after non-response may provide insight into this in future.
Disclosure of Interest
ML, LS & AB report no disclosures. AT has received grants for attending meetings, has attended advisory boards and participated in satellite symposia organised by Novartis, Teva, Eli Lilly & Lundbeck. He was a principle investigator in randomised clinical trials of erenumab, galcanezumab, fremanezumab & eptinezumab. GG was a sub-investigator in a randomised clinical trial of erenumab funded by AMGEN. SM has received speaker honoraria from Teva UK. KD has received travel and educational grants from Allergan and Novartis, received speaker fees from Lundbeck and participated in a Chronic Migraine Educational Steering committee sponsored by Allergan.
Edoardo Caronna1, Victor José Gallardo1, Alicia Alpuente1, Marta Torres-Ferrus1, Mariano Huerta Villanueva2, Albert Muñoz2, Sergio Campoy2, Elisa Cuadrado Godia2, Laura Dorado3, Victor Obach4, Neus Fabregat4, Jaime Rodriguez Vico5, Javier Diaz de Teran6, Javier Membrilla6, Julio Pascual7, Gabriel Garate7, Ana Gago8, Angel Guerrero9, Jordi Sanahuja10, Antonio Sánchez Soblechero11, Alberto Lozano Ros11, Pablo Irimia Sieira12, Margarita Sanchez del Rio12, Amaya Echeverría Urabayen13, David Garcia Azorin9, Yesica Gonzalez Osorio9, Vicente Gonzalez Quintanilla7, Alba Lopez Bravo14, Iris Fernández Lázaro8, Sonia Quintas Gutierrez8, Belen Flores Pina3, Paula Manera Zorrilla-Lequerica15, Alex Jaimes Sanchez5, Andrea García Gómez5, Alicia González-Martínez8, Rocío Álvarez Escudero16, Agustin Oterino Durán16, Fernando Velasco Juanes17, Walter Sifontes17, Joana Rodriguez Montolio18, Candela Nieves Castellanos19, Marina Olivier19, Almudena Layos-Romero20, Alberto Andrés López20, Francisco Sánchez Caballero21, Isabel Beltrán Blasco22, Manuel Millán Vázquez23, Raquel Lamas Pérez23, Javier Viguera Romero21, Sonia Santos-Lasaosa18, Samuel Diaz Insa19, Carmen González Oria23, André Caetano24, Gonçalo Cabral24, Liliana Pereira25, Elisa Martins-Silva25, Isabel Luzeiro26, Catarina Fernandes26, Isabel Pavao Martins27, Beatriz Nunes Vicente27, Inês Marques28, Renato Oliveira28, Cem Thunstedt29, Andreas Straube29, Valeria Caponnetto30, Raffaele Ornello30, Gloria Vaghi31, Roberto De Icco31, Sabina Cevoli32, Paola Torelli33, Gabriella Egeo34, Christina Heidemann Sundal35, Marta Waliszewska36, Mona Ghadiri-Sani37, Ruth Ruscheweyh29, Raquel Gil-Gouveia28, Simona Sacco30, Cristina Tassorelli31, Piero Barbanti34 and Patricia Pozo-Rosich1
1Vall d´Hebron, Barcelona, Spain
2Hospital de Bellvitge - Hospital de Viladecans, Barcelona, Spain
3Hospital Universitario Germans Trias i Pujol, Barcelona, Spain
4Hospital Clinic, Barcelona, Spain
5Fundación Jiménez Díaz, Madrid, Spain
6Hospital La Paz, Madrid, Spain
7Hospital Univ. M. de Valdecilla, Santander, Spain
8Hospital La Princesa, Madrid, Spain
9Hospital Clínico Universitario de Valladolid, Valladolid, Spain
10Hospital Arnau de Villanova, Lleida, Spain
11Hospital Gregorio Marañon, Madrid, Spain
12Clínica Universidad de Navarra, Pamplona, Spain
13H Universitario de Álava (HUA), Alava, Spain
14Hospital Reina Sofia, Tudela, Spain
15Hospital del Mar, Barcelona, Spain
16Hospital Universitario Central de Asturias, Oviedo, Spain
17Hospital Universitario Cruces, Bilbao, Spain
18Hospital Lozano Blesa, Zaragoza, Spain
19Hospital Universitario La Fe, Valencia, Spain
20Hospital General Universitario de Albacete, Albacete, Spain
21Hospital Virgen de la Macarena, Sevilla, Spain
22Hospital General Universitario Dr. Balmis Alicante, Alicante, Spain
23Hospital Virgen del Rocío, Sevilla, Spain
24Centro Hospitalar de Lisboa Ocidental, Lisboa, Portugal
25Hospital Garcia Orta, Almada, Portugal
26Centro Hospitalar Universitário de Coimbra, Coimbra, Portugal
27Hospital de Santa Maria, Lisboa, Portugal
28Hospital da Luz Lisboa, Lisboa, Portugal
29Klinikum der LMU München, Munich, Germany
30Department of Biotechnological and Applied Clinical Sciences, University of L'Aquila, L'Aquila, Italy
31Fondazione Mondino, Pavia, Italy
32IRCCS Istituto delle Scienze Neurologiche, Bologna, Italy
33Unit of Neurology, Department of Medicine and Surgery, Headache Center, University of Parma, Parma, Italy
34Headache and Pain Unit, IRCCS San Raffaele Pisana, Rome, Italy
35Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
36Wrocław Medical University, Wroclaw, Poland
37THE WALTON CENTRE NHS FOUNDATION TRUST, Liverpool, United Kingdom
Objective
To compare the efficacy and safety of anti-CGRP monoclonal antibodies (mAbs) in real life in Europe between women and men.
Methods
European multicenter, observational study based on prospective registries of adult patients with high-frequency episodic (HFEM) or chronic (CM) migraine treated with anti-CGRP mAbs since January 2019. We collected demographic data, efficacy variables (headache days/month-HDM; migraine days per month-MDM, acute medication days/month-AMDM) and side effects. We analyzed efficacy (≥50%; ≥75% and 100% reduction in HDM) and safety at 6 months, comparing women and men.
Results
We included a total of 5817 patients: median age was 48.0 (40.0,55.0) years old. 82.3% (4785/5817) were women, 17.7% (1032/5817) were men. There were significantly different proportions of women among recruiting countries: Sweden (91.5%), Germany (91.0%), Portugal (87.9%), Spain (83.4%), Italy (78.5%), UK (71.5%) and Poland (66.7%) (p = 0.0018). Women were statistically significantly younger than men (median: 47.0 (40.0, 55.0) vs. 49.0 (41.0, 57.0); p < 0.001), although the difference is not clinically relevant. There were no differences in the proportions of HFEM or CM between the two groups. Women had higher proportions of personal history of anxiety (35.4% vs. 31.2%; p = 0.024) and depression (30.6% vs. 26.3%; p = 0.035) compared to men. Baseline values were 20.0 (14.0,28.0) for HDM; 15.0 (10.0,20.0) for MMD and 15.0 (10.0,24.0) for AMDM, with no differences between the two groups. Women had higher proportions of allodynia (53.0% vs. 39.8%; p = 0.0018). At 6 months (n = 4962), there were no differences in proportions of ≥50% responders (56.3% vs. 57.2%; p = 0.628), ≥75% responders (26.4% vs. 28.2%; p = 0.284) and 100% responders (2.1% vs. 2.1%;p > 0.999) between women and men respectively. Overall side effects were reported in a slightly higher proportion of women compared to men (20.7% vs. 15.4%; p = 0.002), without differences in terms of constipation, or severe adverse events.
Conclusion
the real-life data derived from this large European observational cohort show that anti-CGRP mAbs are equally effective in both sexes, however women experience a slightly higher proportion of side effects, but no greater safety concerns.
Disclosure of Interest
EC has received honoraria from Novartis, Chiesi, Lundbeck, MedScape; his salary has been partially funded by Río Hortega grant Acción Estratégica en Salud 2017–2020, Instituto de Salud Carlos III (CM20/00217). PPR has received, in the last three years, honoraria as a consultant and speaker for: AbbVie, Biohaven, Chiesi, Eli Lilly, Lundbeck, Medscape, Novartis, Pfizer and Teva. Her research group has received research grants from AbbVie, Novartis and Teva; as well as, Instituto Salud Carlos III, EraNet Neuron, European Regional Development Fund (001-P-001682) under the framework of the FEDER Operative Programme for Catalunya 2014–2020 - RIS3CAT; has received funding for clinical trials from AbbVie, Amgen, Biohaven, Eli Lilly, Novartis, Teva. She is the Honorary Secretary of the International Headache Society. She is in the editorial board of Revista de Neurologia. She is an associate editor for Cephalalgia, Headache, Neurologia, The Journal of Headache and Pain and Frontiers of Neurology. She is a member of the Clinical Trials Guidelines Committee of the International Headache Society. She has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. She is the founder of www.midolordecabeza.org. PPR does not own stocks from any pharmaceutical company.
Dae Woong Bae1 and Jae young Ahn2
1St. Vincent's Hospital, Suwon, Korea, Republic of
2St. Vincetn's Hospital, Suwon, Korea, Republic of
Background
In clinical practice, migraine patients frequently describe a period of increased headache frequency and intensity in the few weeks preceding their next injections, as known as wear-off phenomenon. In one study, it was reported that about 60% of headache patients receiving onabotulinumtoxinA treatment had a wear-off phenomenon. There is no established bridging therapy to prevent wear-off phenomenon. In this study, we tried to explore the effectiveness of ultrasound guided peripheral nerve block as a preventive treatment to reduce the wear-off phenomenon of onabotulinumtoxinA.
Methods
This study was a retrospective chart & headache diary review of patients (n = 43) with chronic migraine initiated on onabotulinumtoxinA. A group of 43 patients enrolled from June 2021 to February 2023 was analyzed. The patient group was asked to keep a headache diary daily checking whether they had a headache day and whether they took acute pain relievers. Week 1 after OnabotA injection was defined to include days 1–7 after injection, week 2 days 8–14, and so on. The number of headache days per week was calculated. Wear-off was considered present If the number of headache days per week in week 9, 10, 11, 12 was ≥ 30% higher than mean headache days per week during week 5–8. There was no change in the existing migraine prophylaxis medication during the observation period. OnabotA treatment was performed by fixed site, fixed dose method, and 5 IU of only botox® was injected in each of the 31 designated sites. OnabotA treatment was performed strictly at intervals of 12 weeks (exactly 84 days). Ultrasound guided peripheral nerve block was performed on one day of week 8. Only 2% lidocaine was used without steroids, and it was injected under ultrasound guidance into both greater occipital nerve, auriculotemporal nerve and supraorbital nerves. Both OnabotA and peripheral nerve block procedure were performed by the same skilled operator. Medical records and headache diaries submitted for a total of 36 weeks until the end of the 3rd session of OnabotA treatment were reviewed.
Results
The results of descriptive statistics are as follows. Among the 43 patients enrolled, the proportion of women was 100%, the average age was 42.3 years, the average number of headache days per month was 22.5 days, and the average number of acute abortive medications used per month was 11.2 days. The number of patients with medication-overuse headache was 21 (48.8%), the number of patients with depression was 35 (81.4%), and the number of patients with anxiety was 24 (55.8%).
Among the 43 outpatients, wear-off was present in only 4 patients (9.3%) with a total of 5 events. All of wear-off occurred 2 weeks before the next OnabotA injection (in week 11 or 12). All wear-off phenomenon occurs only in the first or second session of OnabotA treatment. The point at which the first wear off occurred was 75% in session 1 and 25% in session 2.
Statistical analysis was performed to confirm the difference between the wear-off group and the no wear-off group. We compared numeric and atio data with means and standard deviations using an unpaired independent t-test. Statistical significance was defined as 2-tailed P value <.05. Patients age, medication overuse, depression, anxiety, headache days, frequency of abortive analgesic medication did not differ between the wear-off and no wear-off groups.
Conclusion
Preventive ultrasound guided peripheral nerve block can be the effective bridge therapy used in the wear-off period. In particular, when both GON, AT, and SO blocks were performed with ultrasound guidance, there was not a single wear-off phenomenon for at least 2 weeks after the nerve block procedure. Wear-off occurred only in OnabotA session 1 or 2 and was not observed in session 3. Factors that could discriminate the wear-off group and the no wear-off group were not identified. In the future, more large-scale RCT studies using various peripheral nerve block protocols will be needed.
Disclosure of Interest
None Declared.
Tiago Gomes de Paula* and Thais Rodrigues Villa
Headache Center Brasil, São Paulo, Brazil
Objective
The primary aim of this study is to assess the prevalence of hypothyroidism - be it idiopathic, induced by Hashimoto's disease, or secondary to Graves' disease treatment - in a cohort of 198 patients suffering from chronic migraine. By doing so, we seek to ascertain whether a meaningful association exists between these two conditions.
Results
In the study sample of 198 chronic migraine patients, 55 (27.8%) were concurrently diagnosed with hypothyroidism. Disaggregated by gender, 52 of these hypothyroidism diagnoses were females (representing 26.3% of all chronic migraine patients) and 3 were males (representing 1.5% of all chronic migraine patients). Thus, the incidence of hypothyroidism among chronic migraine patients was found to be notably higher than the reported prevalence in the general population, which is approximately 4.6% according to the American Thyroid Association.
Conclusion
This study revealed a high incidence of hypothyroidism among patients diagnosed with chronic migraines. In particular, females with chronic migraines were found to have a higher prevalence of hypothyroidism. It is possible that the physiological or hormonal changes associated with hypothyroidism may be a potential contributing factor to the development or severity of chronic migraines. However, further research is required to elucidate the exact relationship between these conditions and to validate these findings in a larger, more diverse population.
Despite the limitations, this study provides valuable insight into the intersection of chronic migraines and hypothyroidism, potentially enabling better understanding, diagnosis, and treatment of these interconnected conditions. Consequently, clinicians should consider evaluating patients with chronic migraines for hypothyroidism, particularly those of the female gender, to ensure comprehensive treatment and management.
Disclosure of Interest
None Declared.
Theresa Wodehouse1, Kavita Poply1, Anish Bahra2 and Vivek Mehta1
1Pain Research Centre & Barts Neuromodulation Unit, St Bartholomew’s Hospital, London, United Kingdom
2Department of Neurology, John Radcliffe Hospital, London, United Kingdom
Objective
Central sensitization and impaired conditioned pain modulation (CPM) response has been reported with migraine. Migraine patients can present with allodynia possibly attributed to increased sensitivity of peripheral ends of nociceptors with both peripheral and central sensitization. Occipital nerve stimulation (ONS) is an established neuromodulation procedure for selected patients with medically intractable chronic cluster headache and migraine with autonomic symptoms. Although clinically effective, there has been no long-term outcome data on its effect on central sensitisation.
Efficacy outcomes for ONS typically employ standardised headache questionnaire measures but objective tests of endogenous pain mechanisms such as Quantitative Sensory Testing (QST) are yet to be utilised to measure efficacy of ONS. Our group has published one- year outcomes in central sensitisation following ONS. (Wodehouse et al, 2020). The aim of this study was to evaluate whether QST detects change and provide more long-term outcome data in patients receiving ONS.
Methods
Six patients, 3 chronic migraine with autonomic symptoms (ICHD 1.3), 2 new persistent daily headache (ICHD 4.1) and 1 chronic cluster headache (ICHD 3.1) were implanted between 2014–2015 with percutaneous leads placed bilaterally parallel to the greater occipital nerve, IPG (Genesis/Prodigy St Jude Medical, Plano, TX, USA)/Medtronic ONS). Baseline QST and questionnaires were completed, and they were monitored up to a 12-month period and then annual review for 9 years (Local Clinical Effectiveness Approval, Barts Health NHS Trust)
Results
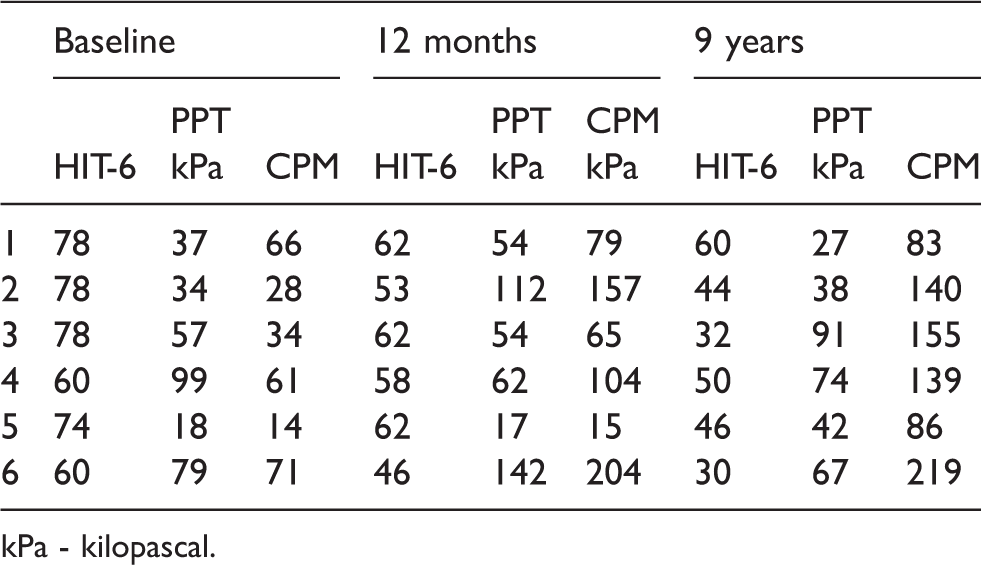
| Baseline |
12 months |
9 years |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| HIT-6 | PPT kPa | CPM | HIT-6 | PPT kPa | CPM kPa | HIT-6 | PPT kPa | CPM | |
| 1 | 78 | 37 | 66 | 62 | 54 | 79 | 60 | 27 | 83 |
| 2 | 78 | 34 | 28 | 53 | 112 | 157 | 44 | 38 | 140 |
| 3 | 78 | 57 | 34 | 62 | 54 | 65 | 32 | 91 | 155 |
| 4 | 60 | 99 | 61 | 58 | 62 | 104 | 50 | 74 | 139 |
| 5 | 74 | 18 | 14 | 62 | 17 | 15 | 46 | 42 | 86 |
| 6 | 60 | 79 | 71 | 46 | 142 | 204 | 30 | 67 | 219 |
kPa - kilopascal.
Conclusion
This is first long term follow up in our knowledge investigating the effect of central sensitisation following ONS. Responders showed substantial reductions in headache-related disability and improvements in conditioned pain modulation over 9-year duration.
Disclosure of Interest
VM Consultancy with Medtronic
Kyung Min Kim* and Min Kyung Chu
Yonsei University College of Medicine, Seoul, Korea, Republic of
Introduction
Headache is a prevalent condition that significantly impacts the daily life and social activities of individuals. However, studies focusing on the specific characteristics of activity limitations caused by headaches, compared to other diseases, are limited.
Methods
This study utilized data from the Seventh Korea National Health and Nutrition Examination Survey, a nationwide representative cross-sectional study conducted in 2016. We examined limitations in daily life and social activities resulting from current health problems or anticipated physical and mental conditions. The sample was divided into two groups: individuals reporting headaches as the reason for activity limitation and those with different reasons. We analyzed various variables, including sex, age, current smoking status, alcohol use, occupation, education level, body mass index, average sleep time, and depression.
Results
Among the Korean population, 9.0% experienced activity limitations, with 1.9% attributing them to headaches. Comparing activity limitations caused by headaches with those caused by other diseases, a significantly higher proportion of women experienced limitations due to headaches (86.7% vs. 58.3%, p = 0.040). However, no significant differences were observed in terms of age (years, 61.0 vs. 59.1, p = 0.759), smoking status (10.0% vs. 22.7%, p = 0.305), alcohol consumption (15.6% vs. 0%, p = 0.098), occupation (52.7% vs. 30.8%, p = 0.193), an education level (32.3% vs. 42.6%, p = 0.546), body mass index (kg/m2, 22.9 vs. 24.6, p = 0.233), average sleep time (hours, 7.2 vs. 7.2, p = 0.965), or depression (28.1% vs. 30.1%, p = 0.889).
Conclusions
Our findings highlight a significant sex difference in activity limitations specific to headaches. These results contribute to our understanding of the distinct impacts of headaches on individuals' daily life and social activities.
Disclosure of Interest
None Declared.
Jessica Ailani1, Richard B. Lipton2, Andrew M. Blumenfeld3, Molly Yizeng He4, Jonathan H. Smith5, Joel M. Trugman4, Rosa de Abreu Ferreira4 and Elimor Brand-Schieber4
1Georgetown University Hospital, Washington DC, USA
2Albert Einstein College of Medicine, Bronx, USA
3Headache Center of Southern California, Carlsbad, USA
4AbbVie, Madison, USA
5AbbVie, North Chicago, USA
Objective
Atogepant is a calcitonin gene-related peptide (CGRP) receptor antagonist approved in the U.S. for the preventive treatment of migraine in adults and ubrogepant is a CGRP receptor antagonist approved in the U.S. for the acute treatment of migraine with or without aura in adults. This study evaluated the safety and tolerability of ubrogepant for the acute treatment of migraine in participants taking atogepant for the preventive treatment of episodic migraine (EM).
Methods
TANDEM, a phase 4, two-period, multicenter, open-label study conducted in the U.S., enrolled adults with migraine, with or without aura, and <15 headache days/month. In Period 1, participants were treated with atogepant 60 mg once daily (QD) for 12 weeks. In Period 2, ubrogepant 100 mg as needed (PRN) was added to atogepant for the treatment of breakthrough migraine attacks (up to 8/month) for 12 weeks. In Period 2, an optional second ubrogepant dose or the participants’ own acute medication could be used to rescue headaches that did not resolve within 2–24 hours post dose. The primary endpoint was the safety and tolerability of atogepant and ubrogepant administered concomitantly.
Results
Of 263 participants enrolled, 262 were treated in Period 1 (Safety Population 1) and 218 continued and were treated in Period 2 (Safety Population 2). The mean number of ubrogepant use days was 6.6 (SD, 5.03; min, max, 1, 24) over the 12 weeks of Period 2 (n = 188). In Safety Population 1, 49.6% of participants experienced a treatment-emergent adverse event (TEAE) versus 43.1% in Safety Population 2. The most common TEAEs (≥5%) in Safety Populations 1 and 2 were COVID-19 (8.4%, 3.2%), fatigue (6.5%, 1.4%), nausea (6.1%, 0.9%), decreased appetite (5.7%, 0.9%), and constipation (5.3%, 0.9%), respectively. In Safety Population 2, no trend in TEAEs was identified in relation to the number of ubrogepant use days. 9.9% of participants discontinued any treatment due to TEAEs. There was 1 serious TEAE in each Period (Period 1, ureterolithiasis; Period 2, myelopathy), and both were considered not related to study treatment by the investigator. No hepatic safety issues or new safety signals were identified across the entire study.
Conclusions
The use of atogepant 60 mg QD for the preventive treatment of EM and ubrogepant 100 mg PRN for the acute treatment of migraine over 12 weeks was safe and well tolerated.
Disclosure of Interest
Jessica Ailani, MD, reports support for the present study from AbbVie, personal fees from AbbVie, Aeon, Amgen, Axsome, Biohaven, BioDelivery Sciences International, Eli Lilly, GlaxoSmithKline, Gore, Impel, Linpharma, Lundbeck, Miravio, Neso, Neurolief, Satsuma, Teva, and Theranica, clinical trial support from AbbVie, Biohaven, Eli Lilly, Satsuma, and Zosano, and stock options from CtrlM. She has provided editorial services to Current Pain and Headache Reports, Medscape, NeurologyLive, and SELF magazine. Richard B. Lipton, MD, has received research support from the National Institutes of Health, the FDA, and the National Headache Foundation. He serves as consultant for, advisory board member of, or has received honoraria or research support from AbbVie/Allergan, Amgen, Biohaven, Dr. Reddy’s Laboratories (Promius), electroCore, Eli Lilly, GlaxoSmithKline, Lundbeck, Merck, Novartis, Teva, Vector, and Vedanta Research. He receives royalties from Wolff’s Headache, 8th edition (Oxford University Press, 2009), and Informa. He holds stock/options in Biohaven and Manistee. Andrew M. Blumenfeld, MD, within the past 12 months, has served on advisory boards for, consulted for, and/or been a speaker or contributing author for Aeon, Allergan/AbbVie, Alder, Amgen, Axsome, BDSI, Biohaven, Eli Lilly, Impel, Lundbeck, Novartis, Revance, Teva, Theranica, and Zosano. He has received grant support from AbbVie and Amgen. Molly Yizeng He, PhD, Jonathan H. Smith, MD, Joel M. Trugman, MD, Rosa de Abreu Ferreira, MD, Elimor Brand-Schieber, PhD, are employees of AbbVie and may hold AbbVie stock.
Shuhua Zhang1, Zhao Dong1, Shengyuan Yu1, Suiyi Xu2, Chunfu Chen3, Zhanyou Xue4, Yuanrong Yao5, Hongrong Zhao6, Hongling Zhao7, Yabin Ji8, Dan Wang9, Dongmei Hu10, Kaiming Liu11, Jianjun Chen12, Sufen Chen13, Xiaoyu Gao14, Wei Gui15, Zhiliang Fan16, Dongjun Wan17, Xueqian Yuan18, Wensheng Qu19, Zheman Xiao20, Ming Dong21, Hebo Wang22, Chunyang Ju23, Huifang Xu24, Liang Zhang25, Zhonglin Liu26, Yanhong Wang27, Li Li28, Zhe Wang29 and Peng Xu30
1Department of Neurology, The First Medical Center, Chinese PLA General Hospital, Beijing, China
2Department of Neurology, Headache Center, The First Hospital of Shanxi Medical University, Taiyuan, China
3Department of Neurology, Shandong Provincial Hospital Afliated to Shandong First Medical University, Jinan, China
4Department of Rehabilitation, Suzhou BOE Hospital, Suzhou, China
5Department of Neurology, Guizhou Province People’s Hospital, Guizhou, China
6Department of Neurology, the First Affiliated Hospital of Soochow University, Suzhou, China
7Department of Neurology, Dalian Municipal Central Hospital, Dalian, China
8Department of Neurology, Nanfang Hospital, Southern Medical University, Guangzhou, China
9Department of Neurology, General Hospital of Northern Theatre Command, Shenyang, China
10Department of Neurology, The Second Affiliated Hospital of Shandong First Medical University, Shandong, China
11Department of Neurology, Second Affiliated Hospital, School of Medicine, Zhejiang University, Zhejiang, China
12Department of Neurology, LiShui Municipal Central Hospital, Lishui, China
13Department of Neurology, The Affiliated Changsha Central Hospital, Henyang Medical School, University of South China, Changsha, China
14DDepartment of Neurology, the Affiliated Yantai Yuhuangding Hospital of Qingdao University, Yantai, China
15Department of Neurology, The First Afliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, China
16Department of Neurology, Xingtai People's Hospital, Xingtai, China
17Department of Neurology, The 940th Hospital of Joint Logistic Support Force of Chinese People's Liberation Army, Lanzhou, China
18Department of Neurology, ZhengZhou People Hospital, Zhengzhou, China
19Tongji Medical Collage Huazhong University of Science & Technology, Shanghai, China
20Department of Neurology, Renmin hospital of Wuhan University, Wuhan, China
21Department of Neurology, Neuroscience Center, the First Hospital, JiLin University, Jilin, China
22Department of Neurology, Hebei General Hospital, Hebei, China
23Xuchang Central Hospital Affiliated to Henan University of Science and Technology, Xuchang, China
24Department of Neurology, Wuhan No.1 Hospital, Wuhan, China
25Department of Neurology, Affiliated Hospital of Qingdao University, Qingdao, China
26Department of Neurology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, China
27Department of Neurology, Changchun Traditional Chinese Medicine Hospital, Changchun, China
28Department of Neurology, Jincheng General Hospital, Jincheng, China
29Department of Neurology, The First Affiliated Hospital of Dalian University, Dalian, China
30Department of Neurology, Affiliated Hospital of Jining Medical University, Shandong, China
Background
Presently, the number of multicenter, multidimensional cohort studies available for cluster headache (CH), particularly in China, is insufficient. It is imperative to establish a representative and prospective cohort, for which we are undertaking the first Chinese Cluster Headache Register Individual Study (CHRIS) in China, aiming to provide valuable insights for further exploration.
Methods
The ongoing CHRIS is a comprehensive, multi-centered, prospective, and longitudinal cohort study being conducted across 31 provinces of China. It was started in January 2019 and formally established in August 2022. The study encompasses a broad array of multidimensional data, including demographic information, clinical characteristics, treatment history, imaging, electrophysiology, and biological samples, which were collected at baseline. Patient follow-up occurred every six months during both the cluster and non-cluster periods to capture outcomes, treatment patterns, and prognoses. The study protocol has been approved by the ethics committee of the Chinese PLA General Hospital. All patients are required to provide written informed consent.
Results
A total of 816 patients with CH were enrolled to date, 663 males and 153 females (a male-to-female ratio of 4.33:1), with a mean age of (35.05 ± 9.85) years and a mean age of onset of (24.93 ± 9.73) years. Of these patients, 19 (2.33%) were chronic CH, and only 57 (6.99%) patients had a family history of CH. The most common bout was found to occur 1–2 times per year (45.96%) and lasted form 2 weeks to 1 month (44.00%), frequently in spring (76.23%) and winter (73.04%). 68.50% of patients experienced 1–2 attacks per day, with the majority lasting 1–2 hours (45.59%). 85.54% of patients reported a circadian rhythm being from 9 AM to 12 PM (75.86%) and from 1 AM to 3 AM (43.48%). Most of the cluster episodes were observed to be strictly unilateral (94.00%), often having locations of retro-orbital (75.98%) and temporal (74.39%). There were 514 (62.98%) patients reported experiencing pre-attack symptoms (PAS), while 157 (19.19%) displayed pre- episode symptoms (PES). Lacrimation (78.80%) was the most common autonomic symptom seen in CH, followed by conjunctival injection (53.19%), rhinorrhea (49.63%), and nasal congestion (38.97%). The most common additional symptoms in CH included a sense of restlessness and agitation (55.88%), nausea (57.48%), photophobia (55.02%), and phonophobia (53.55%). Nearly half of the patients (39.22%) experienced a delay in receiving the correct diagnosis of 10 years or more. Only a small proportion of patients (11.89%) received a correct diagnosis of CH at the time of initial presentation. A total of 291 (35.67%) patients received common acute treatment, among which oxygen was the most frequently chosen (45.36%), followed by zolmitriptan orally (43.30%), zolmitriptan nasal spray (28.52%), rizatriptan orally (12.71%), lidocaine nasal drop (11.34%), and sumatriptan orally (1.37%). Of these, sumatriptan orally was the most effective (50.00% being >50% effective, 0 being 30%−50% and 50% being <30%, respectively). Only 198 (24.26%) had used common transitional or preventive treatments, namely oral glucocorticoid (45.96%), verapamil (21.73%), pregabalin (15.15%), subcutaneous glucocorticoid (18.18%), topiramate (13.14%), sodium valproate (4.55%), gabapentin (2.53%), lithium (2.02%), and calcitonin gene-related peptide pathway monoclonal antibodies (CGRP-mAb) (2.02%). CGRP- mAb was the most effective (50.00%, 0, 50%).
Conclusion
As the first Chinese CH registry study, we are establishing a representative, prospective longitudinal cohort to provide the world with valuable data from China. This study strives to enhance the management system for CH in China via a dynamic cohort woth long-term follow-up and multidimensional data.
Disclosure of Interest
None Declared.
Shu'hua Zhang*, Department of Neurology, The First Medical Center, Chinese PLA General Hospital, Beijing, China
Background and Objectives
Presently, the number of multicenter, multidimensional cohort studies available for cluster headache (CH), particularly in China, is insufficient. It is imperative to establish a representative and prospective cohort, for which we are undertaking the first Chinese Cluster Headache Register Individual Study (CHRIS) in China, aiming to provide valuable insights for further exploration.
Methods
The ongoing CHRIS is a comprehensive, multi-centered, prospective, and longitudinal cohort study being conducted across 31 provinces of China. The study encompasses a broad array of multidimensional data, including demographic information, clinical characteristics, treatment history, imaging, electrophysiology, and biological samples, which were collected at baseline. Patient follow-up occurred every six months during both the cluster and non-cluster periods to capture outcomes, treatment patterns, and prognoses.
Results
A total of 816 patients with CH were enrolled to date, 663 males and 153 females (a male-to-female ratio of 4.33:1), with a mean age of (35.05 ± 9.85) years and a mean age of onset of (24.93 ± 9.73) years. Of these patients, 19 (2.33%) were chronic CH, and only 57 (6.99%) patients had a family history of CH. The most common bout was found to occur 1–2 times per year (45.96%) and lasted form 2 weeks to 1 month (44.00%), frequently in spring (76.23%) and winter (73.04%). 68.50% of patients experienced 1–2 attacks per day, with the majority lasting 1–2 hours (45.59%). 85.54% of patients reported a circadian rhythm being from 9 AM to 12 PM (75.86%) and from 1 AM to 3 AM (43.48%). The most common autonomic symptom was lacrimation (78.80%), and nausea was reported by 57.48% of the patients. Nearly half of the patients (39.22%) experienced a delay in receiving the correct diagnosis of 10 years or more. Only 35.67% received common acute treatment and 24.26% have used common transitional or preventive treatments.
Discussion
As the first Chinese CH registry study, we are establishing a representative, prospective longitudinal cohort to provide the world with valuable data from China. This study strives to enhance the management system for CH in China via a dynamic cohort woth long-term follow-up and multidimensional data.
Disclosure of Interest
None Declared.
Jonathan J.Y. Ong1, Yingyi Liu2, Jonathan H. Smith2, Karen Carr2 and Peter J. Goadsby3,4
1Division of Neurology, Department of Medicine, National University Hospital, Singapore and Yong Loo Lin School of Medicine, National University Hospital, Singapore, Singapore
2AbbVie, North Chicago, IL, USA
3King's College, London, United Kingdom
4University of California, Los Angeles, CA, USA
Objective
To evaluate individual responses to atogepant among people with episodic and chronic migraine.
Methods
ADVANCE was a 12-week, double-blind, randomized, phase 3 trial evaluating atogepant 10 mg, 30 mg, and 60 mg once daily compared with placebo for the preventive treatment of episodic migraine. PROGRESS was a 12-week, double-blind, randomized, phase 3 trial evaluating atogepant 30 mg twice daily and 60 mg once daily compared with placebo for the preventive treatment of chronic migraine. In this post hoc analysis of data from the ADVANCE and PROGRESS trials, individual responses among participants who received either placebo or atogepant 60 mg were assessed. The proportions of participants who reported a given change in mean monthly migraine days (MMDs) across the 12-week treatment period were calculated. For ADVANCE, the categories were defined as an increase in MMDs, a reduction of ≥0 to <4 MMDs, and a reduction of ≥4 MMDs. For PROGRESS, the categories were defined as an increase in MMDs, a reduction of ≥0 to <5 MMDs, a reduction of ≥5 to <10 MMDs, and a reduction of ≥10 MMDs.
Results
For this post hoc analysis, 436 participants (placebo, n = 214; atogepant 60 mg, n = 222) in the modified intent-to-treat population (mITT) from ADVANCE were included and 502 participants (placebo, n = 246; atogepant 60 mg, n = 256) in the mITT population from PROGRESS were included. Mean (SD) MMDs at baseline in the ADVANCE trial were 7.5 (2.4) and 7.8 (2.3) for participants randomized to placebo and atogepant 60 mg, respectively. In the PROGRESS trial, mean (SD) MMDs at baseline were 18.9 (4.8) and 19.2 (5.3) for placebo and atogepant 60 mg, respectively. In the ADVANCE trial, 10.4% vs 18.2% of atogepant- vs placebo-treated participants experienced an increase in MMDs across the 12-week treatment period (nominal P = 0.03). Additionally, 54.1% vs 27.6% of atogepant- vs placebo-treated participants experienced a reduction of 4 or more MMDs (nominal P < 0.0001). In the PROGRESS trial, 11.7% vs 16.7% of atogepant- vs placebo-treated participants experienced an increase in MMDs across the 12-week treatment period (nominal P = 0.15). Additionally, 62.9% vs 48.7% of atogepant- vs placebo-treated participants experienced a reduction of 5 or more MMDs. A reduction of 10 or more MMDs was reported by 31.6% vs 21.5% of atogepant- vs placebo-treated participants (nominal P = 0.01).
Conclusion
Among participants with episodic or chronic migraine, more experienced an increase in migraine days on placebo than atogepant over the 12 weeks of the study. Ultimately, a higher proportion of participants had a reduction in MMDs on atogepant than placebo. These results further demonstrate the efficacy of atogepant 60 mg once daily, on a per patient basis, for the preventive treatment of episodic and chronic migraine.
Disclosure of Interest
Jonathan J. Y. Ong, MD, MBBS, FAMS, FRCP, reports participation in advisory boards and receiving honoraria from AbbVie (Singapore), DKSH, Lundbeck, Novartis, and Teva. Peter J. Goadsby, MD, PhD, DSc, reports, over the last 36 months, a grant from Celgene; personal fees from Aeon Biopharma, AbbVie, Amgen, CoolTech LLC, Dr Reddy’s, Eli Lilly and Company, Epalex, Lundbeck, Novartis, Pfizer, Praxis, Sanofi, Satsuma, Shiratronics, Teva Pharmaceuticals and Tremeau; personal fees for advice through Gerson Lehrman Group, Guidepoint, SAI Med Partners, and Vector Metric; fees for educational materials from CME Outfitters; and publishing royalties or fees from Massachusetts Medical Society, Oxford University Press, UptoDate, and Wolters Kluwer. Yingyi Liu, PhD, Jonathan H. Smith, MD, and Karen Carr, PhD, are employees of AbbVie and may hold AbbVie stock.
Hui Ching Ong1 and Mona Ghadiri-Sani2
1St Helens and Knowsley Teaching Hospitals NHS Trust, Liverpool, United Kingdom
2The Walton Centre NHS Trust, Liverpool, United Kingdom
Objectives
To assess the effectiveness and tolerability of Erenumab in migraine.
Methods
Retrospective evaluation of 195 patients on Erenumab from May 2019 to March 2023, including demographics, comorbidities, number of previous preventatives, discontinuation rate, monthly headache days (MHD) and severe headache days (SHD) at baseline (M0), 3 months (M3) and 6 months (M6).
Lifestyle compliance was addressed in all patients prior to starting Erenumab.
Results
Of 195 patients (F:M 144:51, 74%:26%) the mean age was 45 (range 19–88) with mean age of onset of 29 (range 3–63).
88 (45%) of patients had anxiety/depression, 25 (13%) restless legs, 23 (12%) hypertension, 15 (8%) obesity, 14 (7%) fibromyalgia, and 8 (4%) post-traumatic stress disorder.
The mean number of previously failed preventatives was 7 (range 3–24); 100 (51%) had received Botulinum toxin A, and 91 (47%) had another anti-CGRP therapy. They were 47% more likely to discontinue Erenumab compared to anti-CGRP naïve patients.
99 (51%) discontinued Erenumab, of which 64 (65%, n = 99; 33% overall, n = 195) stopped at M3; 81 (82%, n = 99) stopped due to inefficacy, 8 (8%) due to adverse effects and 7 (7%) cited both reasons. 2 (2%) stopped due to resolution of headaches after 15 months.
24 (12%) patients developed side effects, 8 constipation, 2 injection site reactions and 1 hypertension. Only 11 (6%) patients stopped due to the side effects.
131 patients had complete headache diaries; 43 (33%) of them stopped at M3. Of the remaining 88 patients, there was a mean reduction of 7 (95% confidence interval [CI] 5.0–8.3, n = 88) severe headache days (HDs) at M3 and 7 days at M6 (95% CI 3.2–10.6, n = 33). There was significant increase in zero HDs of 6 days (95% CI 3.6–7.4, n = 88) at M3 and 7 at M6 (95% CI 3.7–9.5, n = 33).
Conclusion
Erenumab is very well tolerated, however, its efficacy is moderate, particularly if there has been previous failure to other anti-CGRP treatments. In 50% of patients who respond, there is significant reduction in severe days and increase in zero days.
Disclosure of Interest
Dr Mona Ghadiri-Sani has received honorarium and hospital from Novartis.
Jennifer Fransen1, Nara Ikumi1, Angela Marti-Marca1, Victor J. Gallardo1, Adrià Vilà-Balló1, Edoardo Caronna2, Xim Cerda-Company1, Marta Torres2, Alicia Alpuente2 and Patricia Pozo-Rosich1,2
1Vall d'Hebron Research Institute, Barcelona, Spain
2Hospital Universitari Vall d'Hebron, Barcelona, Spain
Introduction
Alpha oscillations have been linked to cortical excitability, with lower amplitudes of alpha thought to reflect greater cortical excitability. Previous studies have examined the alpha frequency during resting state EEG in patients with migraine, however, these studies have mostly been done in patients with episodic migraine and have shown inconsistent results.
Objective
This study aimed to compare alpha activity between headache-free, healthy controls (HC), and patients with high-frequency episodic (HFEM) and chronic migraine (CM), both interictally and ictally. In addition, we assessed alpha oscillatory activity in these migraine patients (MP) before and after the treatment with Calcitonin Gene-Related Peptide monoclonal antibodies (CGRP-mAbs).
Methods
To study this, five minutes of resting state EEG were recorded during three sessions (two before and one after CGRP-mAbs treatment) in 66 MP (15.65 ± 5.1 headache days per month) and two sessions in 30 HC. The mean time between the first and second session was 10.4 ± 15.43 days, and for MP the mean time between the second and third session was 160 ± 55.9 days. Patients were diagnosed by a headache specialist with HFEM or CM according to the International Classification of Headache Disorders (ICHD-3) and had to fulfil the criteria for migraine with or without aura. Participants had to fill in a Digital Headache Diary daily, this diary was also used to confirm migraine phase. Only EEG recordings of MP in the interictal and ictal phase were used for the statistical analysis. Clinical and sociodemographic data were collected. The alpha frequency spectrum (8–13 Hz) of the occipito-parietal region was obtained to extract the relative alpha power amplitude and the individual alpha frequency (IAF). Mixed-effect linear regression models (LMM) and intraclass correlation (ICC) analyses were applied.
Results
EEG recordings of 63 MP (mean 15.79 ± 5.1 headache days per month, 54 females, and 40.1 ± 8.9 years old) and 25 gender- and age-matched HC (20 females, 38,6 ± 9.1 years old, p > 0.47) were included in the statistical analyses. An ICC analysis in HC confirmed the consistency of alpha power (ICC = 0.90) and IAF (ICC = 0.77) between the two EEG sessions. The results of the LMM showed no significant main effect of group (interictal MP, ictal MP and HC) (alpha power, p = 0.35; IAF, p = 0.21) or session (1 and 2) (alpha power, p = 0.68; IAF, p = 0.55) on alpha power and IAF. EEG recordings of 58 MP were collected after 160 ± 55.9 days of CGRP-mAbs treatment. 33 MP were categorized as responders (≥50% reduction in migraine headache days) and 25 as non-responders. We were unable to identify the response to treatment in five MP. Comparison of the alpha power (p = 0.13) and IAF (p = 0.06) between responders and non-responders to CGRP-mAbs treatment showed no significant differences.
Conclusion
Our results demonstrate that alpha activity does not differ between migraine patients (both interictally and ictally) and healthy controls in the occipito-parietal region. This activity is also similar before and after treatment with CGRP-mAbs. Therefore, we conclude that although individual alpha frequency and alpha power are reliable individual measurements of brain activity, they cannot be used as a biomarker of migraine or response to CGRP-mAbs treatment.
Disclosure of Interest
None Declared.
Areeba Nisar, Kareem El Neemani, Enchao Qiu, S. Omar Shah, Victor Romo, James Evans, Mark Moster, M. Reid Gooch and Hsiangkuo Yuan*
Thomas jefferson university, Philadelphia, USA
Objective
To investigate the venous manometry pressure waveform changes in patients evaluated for transverse sinus stenosis (TSS).
Methods
Clinical data from 4 patients evaluated for TSS were collected prospectively. During the venous manometry, pressure waveforms were captured using ICM+ software, and the trans-stenotic pressure gradient (TSPG) was assessed to determine the stenting eligibility (if TSPG ≥8 mmHg). Pressure waveforms were analyzed qualitatively, in particular, to look for 3 peaks (a, c, v) and 2 descents (x, y) that are typical for central venous pressure (CVP) waveforms. The differences between patients with or without TSS were compared.
Results
Venous pressure waveforms were captured from 4 patients (female 100%, age 36.3 ± 3.3, BMI 33.1 ± 6.8), where 3 were found to have TSPG ≥8 mmHg and received transverse sinus stents. Prior to stenting, TSS patients showed venous waveforms of a single ill-defined “plateau wave-like” pattern. In contrast, 1 patient without TSS (i.e., TSPG <8 mmHg) retained the 3 peaks and 2 descents CVP pattern. After the stent placement, the TSPG normalized, and the waveform changed drastically with the restoration of the CVP pattern.
Conclusion
Venous manometry pressure waveform analysis offers a way to assess the treatment response beyond pressure measurement. Our results suggest that the CVP pattern can be observed in patients without TSS or restored after venous stenting. Further quantitative waveform analysis may shed more light on the physiological impact of TSS or stenting.
Disclosure of Interest
Dr. Nisar, Dr. Neemani, Dr. Qiu, Dr. Shah, Dr. Romo, Dr. Evans, Dr. Moster do not have any disclosures. Dr. Yuan: past 24 months. Grants: NIH (R44NS115460, Drug-Free Nerve Block Device for the Relief of Pain and Symptoms in Migraines and other Headaches), Site investigators: Teva, Abbvie, Trillen, Thermaquil, Consultants: Silva, Clexio, Pfizer, Royalties: Cambridge University Press, Medlink. Dr. Gooch: Consultant for Stryker
Diallo Seybou Hassane1, Sakadi Foksouna2, Nderbe Melom Christelle2, Ngaleu Fallonne.C. T1, Traore Kankou1, Maiga Oumar1, Togo Maimouna1 and Maiga Youssoufa Mamadou1
1Neurology Department, CHU Gabriel Touré, Bamako, Mali
2Neurology Unit, CHU-RN, N'Djamena, Chad
Introduction
Headaches are the main reason for consultations in neurology departments and general medicine. We report on the experience of two days of free consultations in a province of Chad, with the aim of studying the burden of headache in a section of the Chadian population.
Results
In this study, we identified 61 patients with a 98.4% prevalence of headache in the last 12 months. The sex ratio was 1.03, with an average age of 38. Wage earners were the most common social strata with 31.1%. Headaches were responsible for almost a third of cases of absence from work, ranging from 1 to 5 days/month. More than half of headache sufferers received a monthly income below the minimum wage (60,000 FCFA). Around 1/3 were prepared to pay 25 to 2,500 FCFA/month for treatment.
Conclusion
Our work confirms the extent of headache and the burden it places on the population. Proper management of headaches will have a positive impact on the economic cost of this pathology.
Disclosure of Interest
None Declared.
Burden, Headache, Chad.
Rafiullah Khan1, Helen Delrosario2, Sophie Dorsey3, Aamir Ijaz3 and Fayyaz Ahmed3,4
1Hull University Hospital Nhs Trust, Hull, United Kingdom
2Hull University Hospitals Nhs Trust, Hull, United Kingdom
3Hull University Teaching Hospitals Nhs Trust, Hull, United Kingdom
4Hull York Medical School, Hull, United Kingdom
Objective
Galcanezumab is licensed as preventive treatment in those with > 4 days of headaches per month. We evaluated one year outcome on patients prescribed Galcanezumab for CM.
Methods
Adult CM patients attending the Hull Migraine clinic were prescribed Galcanezumab and followed up prospectively. Patients maintained a headache diary for at least 1 month prior to and continuously after commencing fremanezumab. All patients tried and failed at least 6 treatments with 93% failing OnabotulinumtoxinA. We measured monthly headache days (MHD), migraine days (MMD), headache-free days (HFD), analgesia medication (AMD) and triptan days (TD) and Headache Impact Test-6 (HIT6) scores at baseline and monthly during treatment for a year. The treatment was discontinued if they had < 30% reduction in either MHD, MMD at the end of three months. At one year, those that continued were asked to stop treatment for three months if they had < 4 headache days per month for the previous three months and treatment recommenced if any time in the subsequent three months, the headache days went above 4 per month.
Results
125 patients (98 F, 27 M), mean age 42.5 years (range 21–75), commenced Galcanezumab between January 2022– May 2022. 92 patients (76 F, 16 M) at 3-month follow-up had baseline MHD, MMD and HFD of 27, 17 and 3 days, improving to 15, 6 and 15 days respectively were classed as responders and continued treatment for one year. The remaining 33 patients (22 F, 11 M) stopped treatment due to lack of response. At one year 87 (94.5%) patients (73 F and 14 M) were still getting > 5 days of headaches per month and continued treatment and only 5 (5.5%) patients (3 F, 2 M) were able to stop treatment. All but 1 had to restart therapy as the headache days exceeded > 5 or more between in the month following stoppage and we await still await its outcome at month 3.
Side effects were observed in 15 (12F 3M) that included constipation, weight gain and a transient rash at the site of injection.
Conclusion
Even though many patients with CM are reverted to episodic migraine following Galcanezumab therapy, almost all (99%) patients are required to continue treatment for the second year.
Disclosure of Interest
Fayyaz ahmed has received honorarium for being on the advisory board of teva, abbvie, novartis, lundbeck, eli lilly and pfizer. he is a treasurer of the international headache society, council member of the british association for the study of headache, treasurer of anglo-dutch migraine association and headache advisory board member of the association of british neurologist Rafiullah Khan - none Helen Delrosario - none Sophie Dorsey - none Aamir Ijaz - none
Salma Mahamoud*, Grant O'Neil and Maciej Czachorowski
Pfizer, Surrey, United Kingdom
Background
Migraine is a highly prevalent disorder impacting a significant portion of the UK population. Whilst ethnic disparities in healthcare quality have been extensively documented, there is little effort to assimilate their implications on migraine care in England.
Objective
We aim to address this gap by conducting an analysis on the utilisation of migraine treatments across populations with differences in ethnic demographics.
Methods
We employed a mixed-method approach; Inequity of migraine care was analysed using NHS OpenPrescribing data for Sumatriptan prescriptions and nationally representative data for ethnic composition in Integrated Care Board (ICBs) regions in England. Scatter graphs and maps were plotted, and Pearson Correlation analysis was performed. A qualitative component in this research was also conducted to synthesise existing literature on ethnic disparities and health inequality utilising PubMed sources.
Results
There was marked variation in the prescribing of Sumatriptan across different demographics. There was significant positive linear association (r = 0.82, P < 0.001) between percentage of White population within an ICB and cost of Sumatriptan prescriptions per 1000 estimated migraine population. Contrastingly, there was significant negative correlations between Mixed, Asian, and Black populations and Sumatriptan prescription costs respectively (P < 0.001). ICBs with the highest proportion of White population (93.4%) received the greatest Sumatriptan prescription investment (£5732/1000 population), whilst ICBs with the largest Black population (17.60%) received amongst the lowest Sumatriptan prescription investment (£1981.149/1000 population).
Conclusion
These findings are consistent with other studies suggesting access to migraine treatment varies amongst ethnic groups. Interventions are required to reduce prescribing variations among ethnic communities suffering migraine. This study had the limitation that OpenPrescribing data is not matched to individual patient records. Additional studies are therefore needed to confirm these findings (e.g. utilising Clinical Practice Research Datalink (CPRD))
Disclosure of Interest
All Submitting authors are employed by and hold stock options from Pfizer Ltd.
Rafiullah Khan1, Helen Delrosario1, Modar Khalil1, Sophie Dorsey1, Aamir Ijaz2 and Fayyaz Ahmed1,3
1Hull University Teaching Hospitals Nhs Trust, Hull, United Kingdom
2Hull University Hospitals Nhs Trust, Hull, United Kingdom
3Hull York Medical School, Hull, United Kingdom
Background
OnabotulinumtoxinA is now a well established preventive option for Chronic Migraine (CM) since its approval by the Medicine and Healthcare Regulatory Agency (MHRA) in the United Kingdom and Food and Drug Administration (FDA) in the United States since 2010. In the United Kingdom (UK), it was recommended by the National Institute for health and Care Excellence in 2012 following failure of at least three first line preventive treatments and are appropriately addressed for medication overuse. The Hull Migraine Clinic in the UK was the first of its kind to offer treatment since July 2010.
Objective
To determine the long-term outcome of patients treated with OnabotulinumtoxinA in the prevention of CM.
Methods
Adult patients receiving OnabotulinumtoxinA for CM at the Hull Migraine Clinic were followed up prospectively. All patients had tried and failed at least one oral preventive migraine therapy. OnabotulinumtoxinA was delivered as per the PREEMPT study protocol. Patients were asked to maintain a headache diary throughout the treatment period. Data was extracted for headache days, migraine days, crystal clear (headache-free) days as a primary outcome measure. Responder rates were assessed using NICE criteria at cycle 2 (at least 30% reduction in headache days from baseline and treatment was continued if patients fulfilled the Hull Criteria described as a 50% reduction in either headache or migraine days or doubling of headache-free days from the baseline provided at least 6 such days are recorded post-treatment. Treatment was stopped at cycle 2 for lack of response (negative stopping rule) or when they achieved less than 8 days of headache per month for at least six months (positive stopping rule). Treatment was recommenced if the monthly headache days exceeded 10 for at least three consecutive months.
Results
337 (280F 57M) patients treated between July 2010 and May 2013 were followed up prospectively for 10 years from the start of their treatment. 202 (165F 37M) were responders and continued beyond cycle 2 while 135 (115F 20M) stopped treatment as per negative rule.
At the end of year 10 from receiving the 1st treatment, 51 (25.2%) (41F 10M) were still on treatment. Of these 30 (24F 6M) were on continuous treatment at 3–4 monthly intervals without stopping it. Additional 21 (17F 4M) patients had been recommenced on treatment following a successful stoppage during this period. 27 (22F 5M) patients had stopped treatment following initial response (development of resistance), 11 (All F) stopped treatment due to pregnancy and 8 (7F 1M) were lost to follow up. The remaining 105 (84F 21M), (51.9%) remained episodic following discontinuation of treatment.
Adverse events were reported by 18% of which 6% had mild to moderate but reversible ptosis, 7% had mild to moderate stiffness in the neck and less than 1% reported mild difficulty in swallowing. Following initial adverse events, the treatment was well tolerated throughout the treatment period.
Conclusion
We present the outcome data at year 10 on a large cohort of patients receiving OnabotulinumtoxinA as preventive therapy for CM. A quarter of the initial cohort were still on treatment although only half remained episodic following successful stoppage. OnabotulinumtoxinA was well tolerated and no long-term side effects were reported.
Disclosure of Interest
Fayyaz Ahmed has receivied honorarium for being on the advisory board of Teva, Novartis, Abbvie, Lunbeck, Eli Lilly And Pfizer. He is a treasurer of The International Headache Society, Treasurer of the Anglo-Dutch Migraine Association, Council Member of the British Association for the Study of Headache, Headache Advisory Board Member of the Association of British Neurologist. Rafiullah Khan - None Hele Delrosario - None Modar Khalil - None Sophie Dorsey - None Aamir Ijaz - None
Cristina Trevino-Peinado* and Paula Torres
Hospital Severo Ochoa, Leganés, Spain
Objectives
To assess the clinical characteristics of headache related to COVID-19 infection in healthcare workers, considering acute SARS-CoV-2 infection, vaccination status, and treatment modalities. Additionally, to investigate the waves of the pandemic associated with higher incidence of headache and evaluate persistent headache.
Methods
This descriptive cross-sectional study was primarily conducted in a single center. A 50-item survey was distributed to collect demographic information, headache characteristics, acute and preventive treatments, types of vaccines administered, and their relation to headache. Appropriate frequency measures were utilized for data analysis.
Results
A total of 392 healthcare professionals participated, with majority being female (71%). Headache associated with COVID-19 infection was predominantly described as frontal, bilateral, pressing, and of moderate intensity. Nonsteroidal anti-inflammatory drugs (NSAIDs) were the most commonly used acute treatment (43.8%), while antidepressants were the preferred choice for preventive treatment. Among the participants, 22 individuals experienced persistent headache, of which 18 were related to the infection, with an average HIT-6 score of 64. Comirnaty vaccine was administered in the highest proportion (64.6%), and it also showed the highest rates of headache occurrence (18/42 patients).
Conclusions
Headache related to vaccination was less frequent and persistent compared to headache related to SARS-CoV-2 infection, predominantly affecting female individuals. The waves of the pandemic associated with the highest number of headache cases were the first and sixth waves. The Comirnaty® (Pfizer/BioNTech) and Spikevax® (Moderna) vaccines have been associated with a higher percentage of headaches, primarily in women aged 25 to 35 years. Headaches typically occurred one day after vaccination
Disclosure of Interest
I have no conflicts of interest to declare regarding the presentation of this research.
Ian Finkelstein1, Rose Giammarco2 and Christie Tait3
1Toronto Headache & Pain Clinic, Toronto, Canada
2McMaster University, Department of Neurology, Hamilton, Canada
3Structure Clinic, Toronto, Canada
Background
Chronic migraine affects 1–2% of the population globally and is a highly disabling condition. Onabotulinum toxin A (Botox®) was the first treatment to be approved to treat Chronic migraine. The PREEMPT protocol consists of a fixed site-fixed dose injection paradigm with an optional follow-the-pain paradigm. As per the PREEMPT protocol, additional follow-the-pain injections can be utilized in the occipitals, temporalis, and trapezius regions when patients experience early wear off from treatment, have suboptimal control of their migraines or have areas of tenderness corresponding to areas of allodynia. Patients with Chronic migraine who suffer from peri-ocular pain do not benefit from the current PREEMPT injection protocol. We hypothesize that targeting these periocular areas of heightened localized pain with Onabotulinum toxin A injections will decrease peripheral sensitization within trigeminal nerve nociceptors and indirectly affect central sensitization in higher cortical regions of the brain.
Methods
An observational chart review of 51 patients was completed with 48 being female and 3 being male. The mean patient age was 45 years old. Patients had an ICHD-3 confirmed diagnosis of Chronic migraine and had associated complaints of peri-ocular pain. Patients had been receiving Onabotulinum toxin A according to the PREEMPT protocol for at least three treatments prior to the addition of follow-the-pain injections in the lateral orbicularis oculi regions. Using an on-line questionnaire, patients were asked to rate their pain scores (scale 1–10) in the peri-ocular area before and after injections in the lateral orbicularis oculi region, rate their response to the peri-ocular follow the pain injections on a 5-point Likert scale, rate the change in peri-ocular pain and overall migraine severity after injection over the lateral orbicularis oculi region, and finally, patients were asked if their overall migraine control had improved after lateral peri-ocular injections of Onabotulinum toxin A. Patients were also given the opportunity to provide subjective comments regarding noted changes in migraine symptoms with the addition of these peri-ocular injection sites.
Results
The average pain score reported prior to the lateral orbicularis oculi follow-the-pain treatment was 7.94/10. 42 of the respondents (82.4%) rated their pain between 7–10/10. The highest frequency pain scores were 8/10 for 21.6% of respondents and 9/10 for 29.4% of respondents. There was an overall reduction in the reported severity of localized pain around the eyes following the addition of injection sites in the lateral orbicularis oculi. Thirty-four of the 51 respondents (66.6%) reported pain intensity between 1–4/10 after the addition of follow-the-pain injection sites in the lateral orbicularis oculi. The number of respondents reporting pain intensities between 7–10/10 decreased from 82.4% in the pre-treatment rating to 11.7% of respondents in the post-treatment rating. The highest frequency pain scores in the post-treatment responses were 3/10 for 25.5% of respondents and 4/10 for 21.6% of respondents. On the 5-point Likert scale, 78.4% of the respondents indicated at least a very good or excellent response to treatment. Overall migraine severity improved in 25.5% of the respondents and was rated as excellent, 35.3% indicated a very good improvement, and 25.5% indicated good improvement. Finally, 92.2% of respondents found that the addition of these novel follow the pain sites around the eyes resulted in further improvement in migraine control.
Conclusion
Overall, the results suggest that Onabotulinum toxin A administration in the lateral orbicularis oculi may result in decreased localized symptoms of pain in the periocular area and an overall improvement in migraine control. Onabotulinum toxin A decreases the release of pro-inflammatory and excitatory neuropeptides involved in transmitting nociceptive pain and contributing to peripheral and central sensitization in migraine. Thus, targeting areas of heightened localized pain within the trigeminal nerve system is a treatment approach that warrants further investigation.
Disclosure of Interest
None Declared.
Jong-Geun Seo* and Sung-Pa Park
Department of Neurology, School of Medicine, Kyungpook National University, Daegu, Korea, Republic of
Objective
Apathy might be associated with poor quality of life (QOL) and poor response to treatment. However, the nature of apathy’s impact on migraine patients has not been highlighted. We aimed to investigate the correlation between apathy and associated factors in migraine patients, and the relationship between apathy and QOL.
Methods
We recruited migraine patients at a headache clinic, and age, gender, education-matched healthy controls. The subjects were evaluated by the Apathy Evaluation Scale-Self (AES-S), Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder-7 (GAD-7). Migraine patients were also assessed by the Migraine Disability Assessment Scale (MIDAS) and the Korean Migraine-Specific Quality of Life Questionnaire Version 2.1 (K-MSQ).
Results
The mean scores of the AES-S, PHQ-9, and GAD-7 were significantly higher in migraine patients than in controls. Migraine chronicity, duration of migraine, the MIDAS score, and the PHQ-9 score were significantly associated with the overall AES-S score. The strongest factor affecting the overall AES-S score was duration of migraine (β = −0.258, p < 0.001), followed by migraine chronicity (β = −0.233, p = 0.001) and the PHQ-9 score (β = 0.232, p = 0.001). The overall AES-S score was inversely proportional to the scores of the three K-MSQ dimensions (p < 0.001).
Conclusion
Apathy might be a common feature in CM patients or a longer duration of migraine patients, adjusted for coexisting depression. Clinicians need to treat migraine earlier to prevent the occurrence of apathy and poor QOL.
Disclosure of Interest
None Declared.
Amalie Kjerrumgaard, Jeppe Hvedstrup and Henrik Schytz*
Danish Headache Center, Department of Neurology, Rigshospitalet-Glostrup, University of Copenhagen, Copenhagen, Denmark
Objective
Headache calendars are essential tools in diagnosing and monitoring headaches. They are used in clinical practice for long-term monitoring, but their validation remains limited. Digital headache calendars have gained popularity due to several advantages over traditional paper diaries. The aim of this study was to validate the use of a digital calendar in monitoring patients with migraine and tension-type headache (TTH).
Methods
From July 2022 to February 2023, patients diagnosed with migraine and TTH were enrolled in this study. The validation of the digital calendar involved comparing self-reported single headache attacks in the digital calendar with the diagnostic headache diary based on the ICHD-3 criteria for migraine and TTH. Sensitivity and specificity were calculated to assess reliability, and the level of agreement was calculated using kappa-statistics.
Results
This study included 30 patients (41 ± 12 years, 87% women) diagnosed with migraine and TTH. The level of agreement in classification of a single headache attack as migraine revealed a sensitivity of 82% and a specificity of 78%, representing a substantial level of agreement (K = 0.60). The classification of a single headache attack as TTH revealed a sensitivity of 84% and a specificity of 72%, with a moderate level of agreement (K = 0.54).
Conclusion
The digital calendar proves effective in monitoring single headache attacks in patients with migraine and TTH. In clinical practice, we recommend using the digital calendar as a monitoring tool for headache patients, as they can accurately identify true migraine and TTH days.
Disclosure of Interest
None Declared.
Nur Ain Amir* and Wan Aliaa Wan Sulaiman
Universiti Putra Malaysia, Serdang, Malaysia
A migraine is one of the common disabling primary headache disorders, which is the most common disorders of the nervous system. Headache disorder is divided as primary headache or secondary to other diseases. Primary headache syndrome categorized into migraine, tension type headache (TTH) and cluster headache. They are often lifelong conditions, causing pain and inability, also reducing productivity (Rastenytė et al., 2017). The last study of prevalence of migraine in Malaysia was in 1996 which was 9%. Migraines are complex neurological disorders, and while the exact cause is still not fully understood, there are several recognized risk factors that can contribute to their development. The aim of this study was to get determine the risk of factors of migraine subjects in Malaysia population. A case and control study was done analyzed in 113 migraine patient and 163 control subjects. The questionnaire being distributed to migraine patient. The study reported that there were significant different between gender, education, job, salary, and marriage with migraine subject among Malaysian population, (p < 0.005). The study supports the list of risk factors found in migraine among Malaysia population.
Disclosure of Interest
None Declared.
Devi Ariani Sudibyo1, Isti Suharjanti2, M. Reza Fathoni3 and Nazla Ananda Rachmi Puti1
1Department of Neurology, Faculty of Medicine, Universitas Airlangga - Dr. Soetomo General Academic Hospital, Surabaya, Indonesia
2Department of Neurology, Faculty of Medicine, Universitas Airlangga - Dr. Soetomo General Academic Hospital, Surabaya, Indonesia, Indonesia
3Dr. Abdoer Rahem General Hospital, Situbondo, Indonesia
Introduction
Cervicogenic headache is one of the most disabling headaches that causes major physical dysfunction when compared to other headache disorder. Neuropathic and nociceptive pain component in cervicogenic headache are thought to have an impact on sufferers’ disabilities such as depression, anxiety and sleep disturbances which cause decreasing in the quality of life. This study aims to bear out association between pain type and quality of life in cervicogenic headache patients at Neurology Outpatient Clinic, Dr. Soetomo General Academic Hospital, Surabaya.
Material and Methods
This is an observational analytic study with cross-sectional design for patients with cervicogenic headache who met inclusion and exclusion criteria during the period June to August 2020 at Neurology Outpatient Clinic, Dr. Soetomo General Academic Hospital, Surabaya. Pain type examination was measured with painDETECT questionnaire and quality of life examination was measured using the 36-item short-form questionnaire and Health Survey (SF-36). Neuropathic pain was assessed if painDETECT score above 12 and poor quality of life was assessed if SF-36 score below 50.
Results
The sample size was 30 subjects. We found 13 subjects with poor quality of life (87%) and 2 subjects with good quality of life (13%) in neuropathic pain group, while in subjects with nociceptive pain, we found 1 subject with poor quality of life (7%) and 14 subjects with good quality of life (93%). Chi-square statistical analysis obtained p-value <0.01.
Conclusion
There was a significant association between pain type and quality of life in cervicogenic headache, meanwhile patients with neuropathic pain have a worse quality of life than nociceptive pain. This study provides insights on the importance of pain type evaluation to maintain good quality of life in cervicogenic headache.
Disclosure of Interest
None Declared.
cervicogenic headache, neuropathic pain, nociceptive pain, quality of life, SF-36, painDETECT
Scott Rosenthal, Angelina Koehler*, Elizabeth Ackley and Marcy Yonker
Children's Hospital Colorado, Aurora, USA
Background
Patients with severe and refractory headaches often have few options for treatment despite ongoing pain and significant disability. While intravenous dihydroergotamine (IV DHE), an ergot derivative with 5HT agonism, is often effective for the majority of pediatric patients presenting with status migrainosus and refractory headaches, a significant proportion of patients will fail to respond or cannot receive IV DHE due to intolerability/contraindications. Ketamine, a NMDA receptor antagonist, has emerged as potential therapeutic option for this population and has demonstrated benefit in other chronic pain syndromes and refractory mood disorders. Unfortunately, there is a paucity of literature available about the efficacy and tolerability of IV ketamine in the treatment of refractory pediatric headaches and status migrainosus.
Methods
We conducted a retrospective chart review of patients 5–21 years old, admitted to a tertiary pediatric referral center between 2019–2022 for the treatment of refractory headache with continuous intravenous ketamine. Patients were excluded if they received both ketamine and IV DHE in the same encounter, had a secondary etiology for headache, or had a pain score < 3 (on verbal analogue scale, 0–10) at presentation. Primary outcome measures were percent pain reduction at discharge ([Discharge Pain Score – Initial Pain Score]/Initial Pain Score*100), serious adverse events, medication side effects, headache recurrence within 72 hours, and headache recurrence within 30 days post-discharge. Recurrence was defined as phone call or re-presentation to care for headache requiring rescue therapy. Demographic variables were also collected.
Results
58 encounters comprised of 38 unique patients were included for analysis. The median age was 15.8 years (IQR 13.42–17.41) and 44/58 (76%) of patients identified as female. The most common diagnosis was chronic migraine without aura (45/58, 78%) and the median duration of headache or headache pain exacerbation at presentation was 10 days (IQR 3–26.5). The median maximum dose of ketamine was 0.28 mg/kg/hour (IQR 0.2–0.4) and the median duration of infusion was 3 days (IQR 2–3). The median percent pain reduction at discharge was 50% (IQR −67% to +25%). 37/58 (64%) of patients did not have headache recurrence or exacerbation with 1 month of discharge. Of those that recurred, the median time to recurrence was 7 days (IQR 3–12.5). 5/58 (9%) had recurrence with 72 hours of discharge. There were no serious adverse events. The most common side effects were dizziness (19%), nausea (12%), hallucinations (12%), blurry vision (12%), cognitive fog (9%), dysphoria (5%) and vomiting (4%). 4/58 (7%) encounters terminated therapy early due to side effects.
Conclusion
Intravenous ketamine is an effective, safe and well tolerated treatment option for refractory pediatric headaches and status migrainosus. There was a median pain reduction of 50% at discharge and nearly two-thirds of patients did not re-present for further rescue therapies within 1 month. There were no serious adverse events and side effects were very well tolerated.
Disclosure of Interest
None Declared.
Bettina Bjerring1, Stine Maarbjerg1, Lars Bendtsen1, Miki Nikolic2, Valentina Grillo3,4, Roberto De Icco3,4 and Henrik Schytz1
1Department of Neurology, Danish Headache Center, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
2Department of Clinical Neurophysiology, The Neuroscience Centre, Rigshospitalet, Copenhagen, Denmark
3Department of Brain and Behavioural Sciences, University of Pavia, Pavia, Italy
4Headache Science and Neurorehabilitation Center, IRCCS Mondino Foundation, Pavia, Italy
Objective
The blink reflex is useful to distinguish between primary and secondary trigeminal neuralgia and test the function of the trigeminal nerve. No prior studies have investigated whether the blink reflex could identify differences in electrophysiological responses between classical and idiopathic trigeminal neuralgia. The study investigated differences in latency and area under the curve in a cohort of classical and idiopathic trigeminal neuralgia patients.
Methods
Trigeminal neuralgia patients from the Danish Headache Center were consecutively enrolled in the study. According to degree of neurovascular contact assessed by magnetic resonance imaging findings, the patients were subtyped into either classical or idiopathic trigeminal neuralgia. The investigators and assessors of the blin reflex were blinded to the TN subtype and pain side. The blink reflex measured the R1 and R2 latencies as marker of nerve conductance, as well as the area under the curve as marker of the amplitude of the blink reflex.
Results
The study group constituted of 25 patients with classical trigeminal neuralgia and 30 patients with idiopathic trigeminal neuralgia. None of the blink reflex latencies (R1, R2) or the area under the curve significantly differed between the two TN subtypes when adjusted for age and sex (P > 0.05).
Conclusion
Our findings suggest that the blink reflex cannot be used as a diagnostic tool to differentiate between classical and idiopathic trigeminal neuralgia. The study also suggests that classical and idiopathic trigeminal neuralgia may share common pathophysiological mechanisms.
Disclosure of Interest
None Declared.
Mariano Huerta Villanueva1,2, Sergio Campoy1,2, Albert Muñoz-Vendrell2, Jaume Campdelacreu2 and Joan Prat2
1Hospital de Viladecans, Viladecans, Spain
2Unitat de Cefalees. Hospital Universitari de Bellvitge, L'Hospitalet de Llobregat, Spain
Background
Fremanezumab is a humanized monoclonal antibody targeting calcitonin gene-related peptide approved for the treatment of chronic and episodic migraine, with two dose regimens studied in clinical trials, 675 mg quarterly and 225 mg monthly. Patient and physician preferences play a role when different dose regimens are available.
Objective
To describe and compare the effectiveness, safety, and adherence to treatment with monthly or quarterly fremanezumab in a real-life cohort of patients with migraine.
Methods
Retrospective observational study with prospective data collection. Patients with migraine treated with fremanezumab followed for 3 or more months, and not previously treated with another anti-CGRP antibody, were included. Variables of effectiveness and safety were analyzed at 3 and 6 months. The primary endpoint was the mean change in the average number of migraine days per month (MMD) between the first 3 months after the first injection and baseline, comparing the two dosing regimens. As secondary endpoints the percentage of patients with reduction >50% in MMD, the percentage of adverse events, the withdrawals due to adverse events, changes in acute treatment consumption, and the percentage of patients continuing the treatment with fremanezumab after 6 months were evaluated.
Results
Sixty nine patients were included (26 monthly, 43 quarterly). Baseline characteristics did not differ significantly between the two groups. The baseline MMDs were 14 in monthly and 15,4 in quarterly group. In month 3, a reduction compared to the baseline of 4,3 and 5.2 MMD respectively was observed, 0,9 days in favor of the quarterly group (p = 0.56), and in month 6, of 5.8 and 6.2 days, 0.4 days in favor of quarterly group (p = 0.84).
The percentage of adverse events was the same at month 3 for both groups (30%) and it was 27% for the monthly and 19% for the quarterly regimen in month 6, with local reaction and constipation being the most frequents. Only one patient withdrew treatment due to adverse events (local reaction, in the monthly regimen and month 3). The percentage of patients with reduction >50% MMD for the monthly and quarterly group at month 3 was 42.3% and 44.2% respectively, and at month 6, 43,5% and 46,3%, not significantly different. At month 6, 87% of patients in monthly and 87,8% in quarterly group were continuing the treatment.
Conclusions
In the main efficacy, safety and adherence items analyzed, no statistically significant differences were observed between the two dosage regimens of fremanezumab in this real-life study.
Disclosure of Interest
MH-V has received honoraria for participating on advisory boards and for collaborations as consultant, scientific communications, speaker, research support as well as funding for travel and congress-attending expenses for Abbie-Allergan, Novartis, Lilly, Almirall, Chiesi, Esai, Exeltis, Kern Pharma, Menarini, TEVA, Lundbeck and Zambon. His research group has received research grants from Abbie-Allergan; and has received funding for clinical trials from Lilly, Novartis, TEVA. AMV, SC, JC and JP have received honoraria from Teva, Lilly, Roche, UCB, Bial, Chiesi, Allergan, Esai, Zambon, Kern Pharma, Pfizer, Biogen Idec, Novartis, TEVA, Merck, Janssen, Neuraxpharm, Genzyme, Sanofi, Bayer, Almirall and/or Celgene.
Soo Jin Cho1, Han Beet Kim2 and Hong-Kyun Park3
1Dongtan Sacred Heart Hospital, Hwaseung, Korea, Republic of
2Dongtan Sacred Heart Hospital, Hwaseung, Korea, Republic of
3Inje University Ilsan Paik Hospital, Goyang, Korea, Republic of
Background
Neck pain is one of burdensome symptom in the patients with headache. However, the frequency and severity of neck pain has not been well evaluated in medication-overuse headache (MOH). We investigated the frequency and severity of neck pain in a prospective registry of MOH. We hypothesize the neck pain can be improved with treatment of MOH.
Methods
We analyzed the data of on-going multicenter cooperative registry (Registry for Load and Management of MEdicAtion OveruSE Headache [RELEASE]) since April 2020. Treatment for MOH included withdrawal or tapering of overused medication and preventive medications based on the decision of investigators. Neck pain was assessed by the structured interview at baseline, 1, 3, 6, 12 months of follow-up. Neck pain was classified as mild or severe according to its association with high disability or functional limitation. The proportion of neck pain at baseline and 3 months of follow-up was compared by McNemar’s test and the association with MOH reversal at 3 months was assessed by Chi-square test.
Results
A total of 309 patients, 85.1% female, were enrolled. At baseline, 191 patients (61.8%) had neck pain and 78 patients were severe (25.3%). MOH patients with neck pain had more cutaneous allodynia (allodynia symptom checklist-12, 1.0 [0.0–4.0] vs. 0.0 [0.0–2.0], p = 0.007) and decrease quality of life (migraine-specific quality-of-life, 179.3 [116.0–218.8] vs. 187.9 [137.1–250.0], p = 0.036) compared to MOH patients without neck pain. A total of 228 patients returned for the 3 months visit and 118 patients (51.7%, p < 0.001) had neck pain and 24 patients (10.5%, p < 0.001) were severe. At 3 months follow-up, 138 (60.5%) patients were recovery from MOH. The proportion of severe neck pain were 6.5% in patients with recovery from MOH and 16.7% in patients without (p = 0.026).
Conclusions
About two-thirds of MOH patients had neck pain and one-fourth were severe. Treatment of MOH may reduce neck pain, especially severe neck pain, in patients with MOH.
Disclosure of Interest
None Declared.
Stefania Ferraroa,b,c, Anna Nigric, Maria Grazia Bruzzonec, Jean Paul Medinac, Davide Fedelic, Greta Demichelisc, Giuseppe Ciulloc, Luisa Chiapparinic, Alberto Proietti Cecchinid, Luca Gianie, Benjamin Beckera,b,f and Massimo Leoned
aCenter of Psychosomatic Medicine, Sichuan Provincial Center for Mental Health, Sichuan Provincial People's Hospital, University of Electronic Science and Technology of China, Chengdu, China
bSchool of Life Science and Technology, MOE Key Laboratory for Neuroinformation, University of Electronic Science and Technology of China, Chengdu, China
cDepartment of Neuroradiology, Fondazione IRCCS Neurologico ’Carlo Besta’, Milan, Italy
dDepartment of Neuroalgology, Fondazione IRCCS Neurologico ’Carlo Besta’, Milan, Italy
eDepartment of Neurology, Fondazione Maugeri, IRCCS, Milan, Italy
fState Key Laboratory of Brain and Cognitive Sciences, The University of Hong Kong, Hong Kong, China; Department of Psychology, The University of Hong Kong, Hong Kong, China
Background
The cyclic nature of cluster headache condition (circannual recurrence of cluster periods and the circadian onset of attacks) and the associated neuroendocrinological abnormalities have led to the hypothesis of the involvement of the ipsilateral-to-the-pain hypothalamus (Leone & Bussone, 1993). Although MRI findings point to abnormalities of the hypothalamus, inconsistencies among results do not allow a firm conclusion.
Objective
To confirm the ipsilateral to the cranial pain hypothalamic involvement and to clarify the nuclei involved in the cluster headache pathophysiology.
Methods
We used a state-of-the-art fully automated algorithm (Freesurfer v7.2) to extract the volumes of the hypothalamic subunits from 3D-T1 high-resolution images (acquired with Achieva 3 T, voxel size 1x1x1 mm) obtained from a large sample of 107 cluster headache patients (57 chronic and 50 episodic) and 59 healthy individuals, and we employed 3-block logistic regression models (p < 0.05) to verify the statistical association of the hypothalamic measures (normalized in respect to the intracranial volumes) with respect to (1) the cCH and CTRL diagnosis and (2) the eCH and CTRL diagnosis. In the 3-block logistic regression models, Model 1 comprised the demographic data, model 2 comprised the demographic data and the contralateral hypothalamic measures (null model = demographic data), model 3 comprised the demographic data, the contralateral hypothalamic measures and the ipsilateral hypothalamic measures (null model = demographic data and contralateral hypothalamic measures).
Results
After a careful check of biases determined by possible lateralization effects, our results showed that chronic cluster headache patients, but not episodic, in comparison to control individuals, present increased volume of the ipsilateral-to-the-pain anterior-superior hypothalamic subunit (MODEL 3: Χ2(101) = 11.74, p = 0.039, Nagelkerke R2 = 0.137; ipsilateral superior anterior subunit: OR = 1.159, p = 0.034; cCH: M = 25.91 ml range: 19–33.4, CTRL: M = 24.55 range: 15.6–33.7).
We did not find any correlation of the measures of this subunit with the years of chronicization of the disease neither an effect of the lithium therapy.
Interpretation
We confirmed abnormalities of the ipsilateral-to-the-pain hypothalamus, and we identified the anterior superior subunit as the key hypothalamic area of the pathophysiology of cluster headache.
Disclosure of Interest
None Declared.